
Risk of Skin Cancer in Patients with Psoriasis: Single-Center Retrospective Study Comparing Anti-TNFα and Phototherapy
 ,
,
Abstract
:1. Introduction
1.1. Psoriasis and Skin Cancers
1.2. Relation between Psoriasis, Skin Cancers, and Exposome
1.3. Relation between Psoriasis, Skin Cancers, and Lifestyle
1.4. Aim of This Study
2. Materials and Methods
Statistical Analyses
3. Results
3.1. Phototherapy and Anti-TNFα
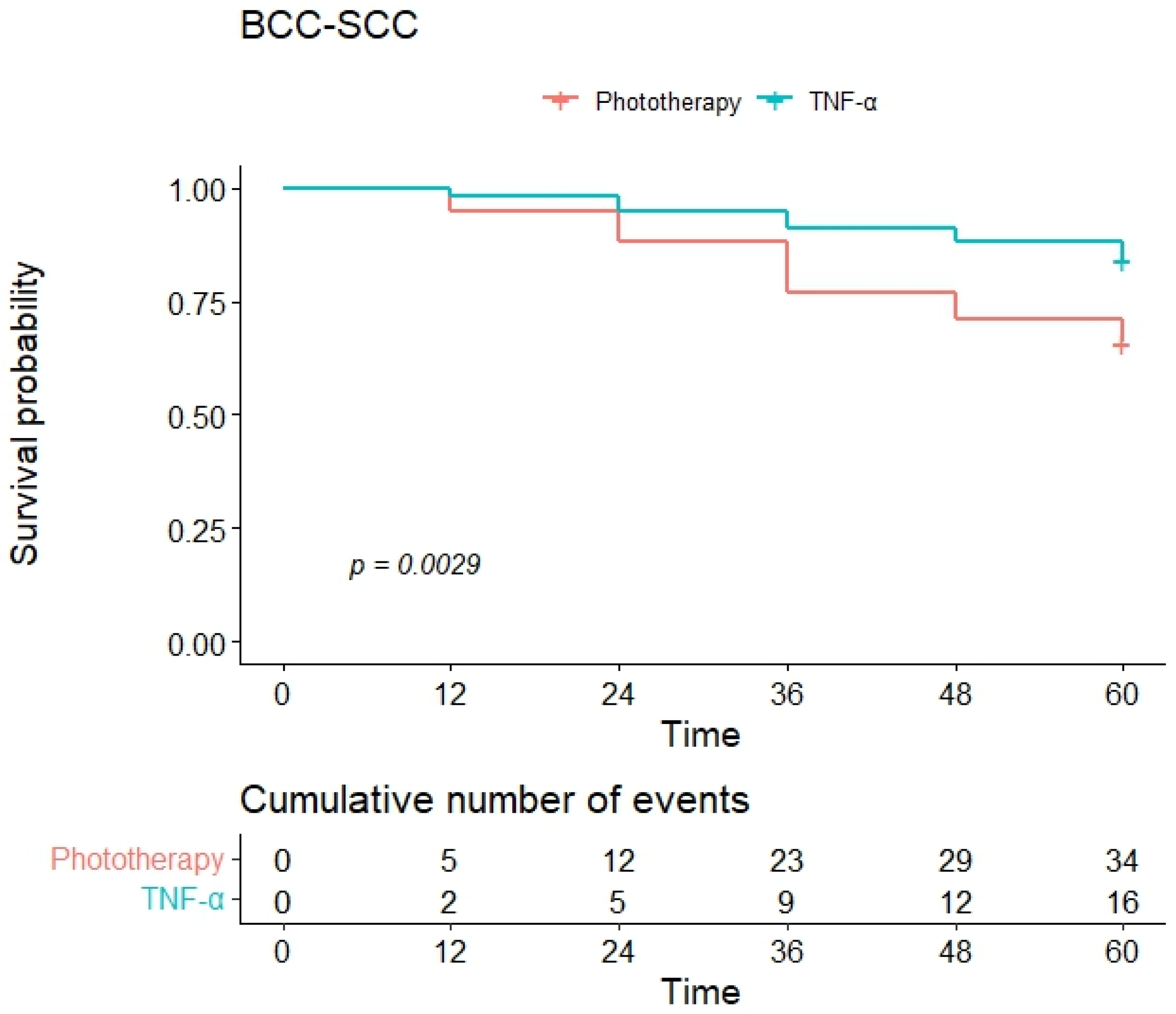
3.2. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trovato, E.; Cartocci, A.; Calabrese, L.; D’onghia, M.; Dragotto, M.; Capalbo, E.; Silvi, G.; Margiotta, F.M.; Pimpinelli, N.; Pellegrino, M.; et al. Pso-Reg: A web registry for psoriasis in real life. Ital. J. Dermatol. Venerol. 2023, 158, 249–254. [Google Scholar] [CrossRef]
- Boehncke, W.H.; Schon, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef] [PubMed]
- De Simone, C.; Calabrese, L.; Balato, A.; Cannavo, S.P.; Dattola, A.; Esposito, M.; Fargnoli, M.C.; Giuffrida, R.; Hansel, K.; Musumeci, M.L.; et al. Psoriasis and its management in women of childbearing age: Tools to increase awareness in dermatologists and patients. G. Ital. Dermatol. Venereol. 2020, 155, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Trovato, E.; Rubegni, P.; Cinotti, E. The Immunogenetics of Psoriasis. Adv. Exp. Med. Biol. 2022, 1367, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Chiricozzi, A.; Romanelli, P.; Volpe, E.; Borsellino, G.; Romanelli, M. Scanning the Immunopathogenesis of Psoriasis. Int. J. Mol. Sci. 2018, 19, 179. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, L.; Malvaso, D.; Antonelli, F.; Mannino, M.; Peris, K.; Chiricozzi, A. Investigational systemic drugs for moderate to severe plaque psoriasis: What’s new? Expert. Opin. Investig. Drugs 2023, 32, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Harden, J.L.; Krueger, J.G.; Bowcock, A.M. The immunogenetics of Psoriasis: A comprehensive review. J. Autoimmun. 2015, 64, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.M.; Clements, M.A.; Kwilasz, A.J.; Watkins, L.R. T cell transgressions: Tales of T cell form and function in diverse disease states. Int. Rev. Immunol. 2022, 41, 475–516. [Google Scholar] [CrossRef] [PubMed]
- Tokuyama, M.; Mabuchi, T. New Treatment Addressing the Pathogenesis of Psoriasis. Int. J. Mol. Sci. 2020, 21, 7488. [Google Scholar] [CrossRef] [PubMed]
- Fargnoli, M.C.; Bardazzi, F.; Bianchi, L.; Dapavo, P.; Fabbrocini, G.; Gisondi, P.; Micali, G.; Offidani, A.M.; Pellacani, G.; Skroza, N.; et al. Brodalumab for the Treatment of Moderate-to-Severe Psoriasis: An Expert Delphi Consensus Statement. J. Clin. Med. 2023, 12, 3545. [Google Scholar] [CrossRef] [PubMed]
- Caldarola, G.; Falco, G.M.; Calabrese, L.; D’Amore, A.; Chiricozzi, A.; Mariani, M.; Palmisano, G.; De Simone, C.; Peris, K. Drug survival of biologics and non-biologics in patients affected by palmoplantar psoriasis: A “real-world”, mono-center experience. Int. J. Dermatol. 2024, 63, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Read, C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA 2020, 323, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- D’Onghia, M.; Ursini, F.; Cinotti, E.; Calabrese, L.; Tognetti, L.; Cartocci, A.; Lazzeri, L.; Frediani, B.; Rubegni, P.; Trovato, E. Psoriasis and Fibromyalgia: A Systematic Review. J. Pers. Med. 2024, 14, 165. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, F. Psoriasis: Comorbidities. J. Dermatol. 2021, 48, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Ciazynska, M.; Kaminska-Winciorek, G.; Lange, D.; Lewandowski, B.; Reich, A.; Slawinska, M.; Pabianek, M.; Szczepaniak, K.; Hankiewicz, A.; Ulanska, M.; et al. The incidence and clinical analysis of non-melanoma skin cancer. Sci. Rep. 2021, 11, 4337. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.S.; Strange, R.C.; Lear, J.T. Basal cell carcinoma. BMJ 2003, 327, 794–798. [Google Scholar] [CrossRef] [PubMed]
- D’Orazio, J.; Jarrett, S.; Amaro-Ortiz, A.; Scott, T. UV radiation and the skin. Int. J. Mol. Sci. 2013, 14, 12222–12248. [Google Scholar] [CrossRef] [PubMed]
- Marks, R. Measurement of biological ageing in human epidermis. Br. J. Dermatol. 1981, 104, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Zafiriou, E.; Karampinis, E.; Roussaki-Schulze, A.-V. Psoriasis and Exposome: Unveiling the Inner and the External Contributors of Psoriasis Disease. In Psoriasis—Recent Advances in Diagnosis and Treatment; InterOpen: London, UK, 2023. [Google Scholar] [CrossRef]
- Villarreal-Martinez, A.; Gallardo-Blanco, H.; Cerda-Flores, R.; Torres-Munoz, I.; Gomez-Flores, M.; Salas-Alanis, J.; Ocampo-Candiani, J.; Martinez-Garza, L. Candidate gene polymorphisms and risk of psoriasis: A pilot study. Exp. Ther. Med. 2016, 11, 1217–1222. [Google Scholar] [CrossRef]
- Vorobjeva, N.; Prikhodko, A.; Galkin, I.; Pletjushkina, O.; Zinovkin, R.; Sud’ina, G.; Chernyak, B.; Pinegin, B. Mitochondrial reactive oxygen species are involved in chemoattractant-induced oxidative burst and degranulation of human neutrophils in vitro. Eur. J. Cell Biol. 2017, 96, 254–265. [Google Scholar] [CrossRef]
- Goldminz, A.M.; Au, S.C.; Kim, N.; Gottlieb, A.B.; Lizzul, P.F. NF-kappaB: An essential transcription factor in psoriasis. J. Dermatol. Sci. 2013, 69, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Cust, A.E.; Armstrong, B.K.; Goumas, C.; Jenkins, M.A.; Schmid, H.; Hopper, J.L.; Kefford, R.F.; Giles, G.G.; Aitken, J.F.; Mann, G.J. Sunbed use during adolescence and early adulthood is associated with increased risk of early-onset melanoma. Int. J. Cancer 2011, 128, 2425–2435. [Google Scholar] [CrossRef] [PubMed]
- Trovato, E.; Fiorani, D.; Cartocci, A.; Cinotti, E.; Rubegni, P. IGF1 synthesis after CO2 fractional laser resurfacing (FLR): New insights in the treatment of scalp actinic keratoses. Lasers Surg. Med. 2023, 55, 642–652. [Google Scholar] [CrossRef] [PubMed]
- Balda, A.; Wani, I.; Roohi, T.F.; Suman; Krishna, K.L.; Mehdi, S.; Nadiga, A.P.; Makkapati, M.; Baig, M.A.I. Psoriasis and skin cancer—Is there a link? Int. Immunopharmacol. 2023, 121, 110464. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Chen, H.; Qian, H.; Wang, F.; Xu, Y. Advances in the modulation of ROS and transdermal administration for anti-psoriatic nanotherapies. J. Nanobiotechnol. 2022, 20, 448. [Google Scholar] [CrossRef] [PubMed]
- Klisic, A.; Bakic, M.; Karanikolic, V. Comparative Analysis of Redox Homeostasis Biomarkers in Patients with Psoriasis and Atopic Dermatitis. Antioxidants 2023, 12, 1875. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Wu, W.; Fu, W.; Hu, Y. The effects of phototherapy and melanocytes on keratinocytes. Exp. Ther. Med. 2018, 15, 3459–3466. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Ranganathan, P. TNF-alpha antagonism and cancer risk in rheumatoid arthritis: Is continued vigilance warranted? Discov. Med. 2012, 13, 229–234. [Google Scholar] [PubMed]
- Bujoreanu, F.C.; Bezman, L.; Radaschin, D.S.; Niculet, E.; Bobeica, C.; Craescu, M.; Nadasdy, T.; Jicman, D.S.; Ardeleanu, V.; Nwabudike, L.C.; et al. Nevi, biologics for psoriasis and the risk for skin cancer: A real concern? (Case presentation and short review). Exp. Ther. Med. 2021, 22, 1354. [Google Scholar] [CrossRef]
- Paradisi, A.; Didona, B.; Tabolli, S.; Ricci, F.; Sobrino, L.; Panebianco, A.; Abeni, D. Reduced frequency of non-melanoma skin cancer in 72,739 patients with psoriasis: A retrospective study. Eur. J. Dermatol. 2017, 27, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Liu, Q.; Wu, L.; Nie, Z.; Mei, Z. Risk of non-melanoma skin cancer in patients with psoriasis: An updated evidence from systematic review with meta-analysis. J. Cancer 2020, 11, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Peleva, E.; Exton, L.S.; Kelley, K.; Kleyn, C.E.; Mason, K.J.; Smith, C.H. Risk of cancer in patients with psoriasis on biological therapies: A systematic review. Br. J. Dermatol. 2018, 178, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Woo, Y.R.; Park, C.J.; Kang, H.; Kim, J.E. The Risk of Systemic Diseases in Those with Psoriasis and Psoriatic Arthritis: From Mechanisms to Clinic. Int. J. Mol. Sci. 2020, 21, 7041. [Google Scholar] [CrossRef] [PubMed]
- Mason, K.J.; Burden, A.D.; Barker, J.; Lunt, M.; Ali, H.; Kleyn, C.E.; McElhone, K.; Soliman, M.M.; Green, A.C.; Griffiths, C.E.M.; et al. Characteristics and skin cancer risk of psoriasis patients with a history of skin cancer in BADBIR. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e498–e501. [Google Scholar] [CrossRef] [PubMed]
- deShazo, R.; Soltani-Arabshahi, R.; Krishnasamy, S.; Langley, R.G.; Kalia, S.; Stahle, M.; Langholff, W.; Goyal, K.; Fakharzadeh, S.; Galindo, C.; et al. Non-Melanoma Skin Cancer Risk Among Patients in the Psoriasis Longitudinal Assessment and Registry (PSOLAR). J. Drugs Dermatol. 2019, 18, 1059–1060. [Google Scholar] [PubMed]
- Pierard-Franchimont, C.; Pierard, G.E.; Quatresooz, P. Focus on skin cancer association and progression under TNF antagonist therapy. Expert. Opin. Biol. Ther. 2011, 11, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- D’Arcy, M.E.; Beachler, D.C.; Pfeiffer, R.M.; Curtis, J.R.; Mariette, X.; Seror, R.; Mahale, P.; Rivera, D.R.; Yanik, E.L.; Engels, E.A. Tumor Necrosis Factor Inhibitors and the Risk of Cancer among Older Americans with Rheumatoid Arthritis. Cancer Epidemiol. Biomark. Prev. 2021, 30, 2059–2067. [Google Scholar] [CrossRef] [PubMed]
- van Lumig, P.P.; Menting, S.P.; van den Reek, J.M.; Spuls, P.I.; van Riel, P.L.; van de Kerkhof, P.C.; Fransen, J.; Kievit, W.; de Jong, E.M. An increased risk of non-melanoma skin cancer during TNF-inhibitor treatment in psoriasis patients compared to rheumatoid arthritis patients probably relates to disease-related factors. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Crisafulli, S.; Bertino, L.; Fontana, A.; Calapai, F.; Ingrasciotta, Y.; Berretta, M.; Trifiro, G.; Guarneri, C. Incidence of Skin Cancer in Patients With Chronic Inflammatory Cutaneous Diseases on Targeted Therapies: A Systematic Review and Meta-Analysis of Observational Studies. Front. Oncol. 2021, 11, 687432. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Clinical and Demographic Characteristics | Phototherapy | Anti-TNF | p |
|---|---|---|---|
| N | 100 | 100 | |
| Gender = M (%) | 63 (63.0) | 61 (61.0) | 0.884 |
| Age (mean (SD)) | 55.06 (14.98) | 58.47 (12.27) | 0.080 |
| Positive family history_BCC_SCC = 1 (%) | 16 (16) | 11 (11) | 0.303 |
| BMI = obese (%) | 13 (13.0) | 8 (8.0) | 0.356 |
| Psoriatic arthritis = YES (%) | 12 (12.0) | 20 (20.0) | 0.177 |
| Nail psoriasis = YES (%) | 26 (26.0) | 36 (36.0) | 0.169 |
| Palms/soles = YES (%) | 34 (34.0) | 38 (38.0) | 0.659 |
| Scalp = YES (%) | 43 (43.0) | 53 (53.0) | 0.203 |
| Genitals = YES (%) | 19 (19.0) | 23 (23.0) | 0.602 |
| Variables | HR | 95% CI | p-Value |
|---|---|---|---|
| Male | 0.85 | 0.49, 1.50 | 0.58 |
| Age | 1.12 | 1.08, 1.15 | <0.001 |
| Familiarity per NMSC | 0.50 | 0.18, 1.40 | 0.19 |
| Obesity | 0.97 | 0.38, 2.43 | 0.94 |
| Arthritis | 1.47 | 0.75, 2.88 | 0.26 |
| Nail psoriasis | 1.06 | 0.58, 1.92 | 0.85 |
| Palms/soles | 1.20 | 0.68, 2.11 | 0.53 |
| Scalp | 0.51 | 0.28, 0.91 | 0.023 |
| Genitals | 0.58 | 0.26, 1.29 | 0.18 |
| Anti-TNF therapy | 0.42 | 0.23, 0.75 | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trovato, E.; Dragotto, M.; Capalbo, E.; Cartocci, A.; Rubegni, P.; Calabrese, L. Risk of Skin Cancer in Patients with Psoriasis: Single-Center Retrospective Study Comparing Anti-TNFα and Phototherapy. J. Clin. Med. 2024, 13, 2452. https://doi.org/10.3390/jcm13092452
Trovato E, Dragotto M, Capalbo E, Cartocci A, Rubegni P, Calabrese L. Risk of Skin Cancer in Patients with Psoriasis: Single-Center Retrospective Study Comparing Anti-TNFα and Phototherapy. Journal of Clinical Medicine. 2024; 13(9):2452. https://doi.org/10.3390/jcm13092452
Chicago/Turabian StyleTrovato, Emanuele, Martina Dragotto, Eugenio Capalbo, Alessandra Cartocci, Pietro Rubegni, and Laura Calabrese. 2024. "Risk of Skin Cancer in Patients with Psoriasis: Single-Center Retrospective Study Comparing Anti-TNFα and Phototherapy" Journal of Clinical Medicine 13, no. 9: 2452. https://doi.org/10.3390/jcm13092452