
The Effectiveness of Robot- vs. Virtual Reality-Based Gait Rehabilitation: A Propensity Score Matched Cohort

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Methods
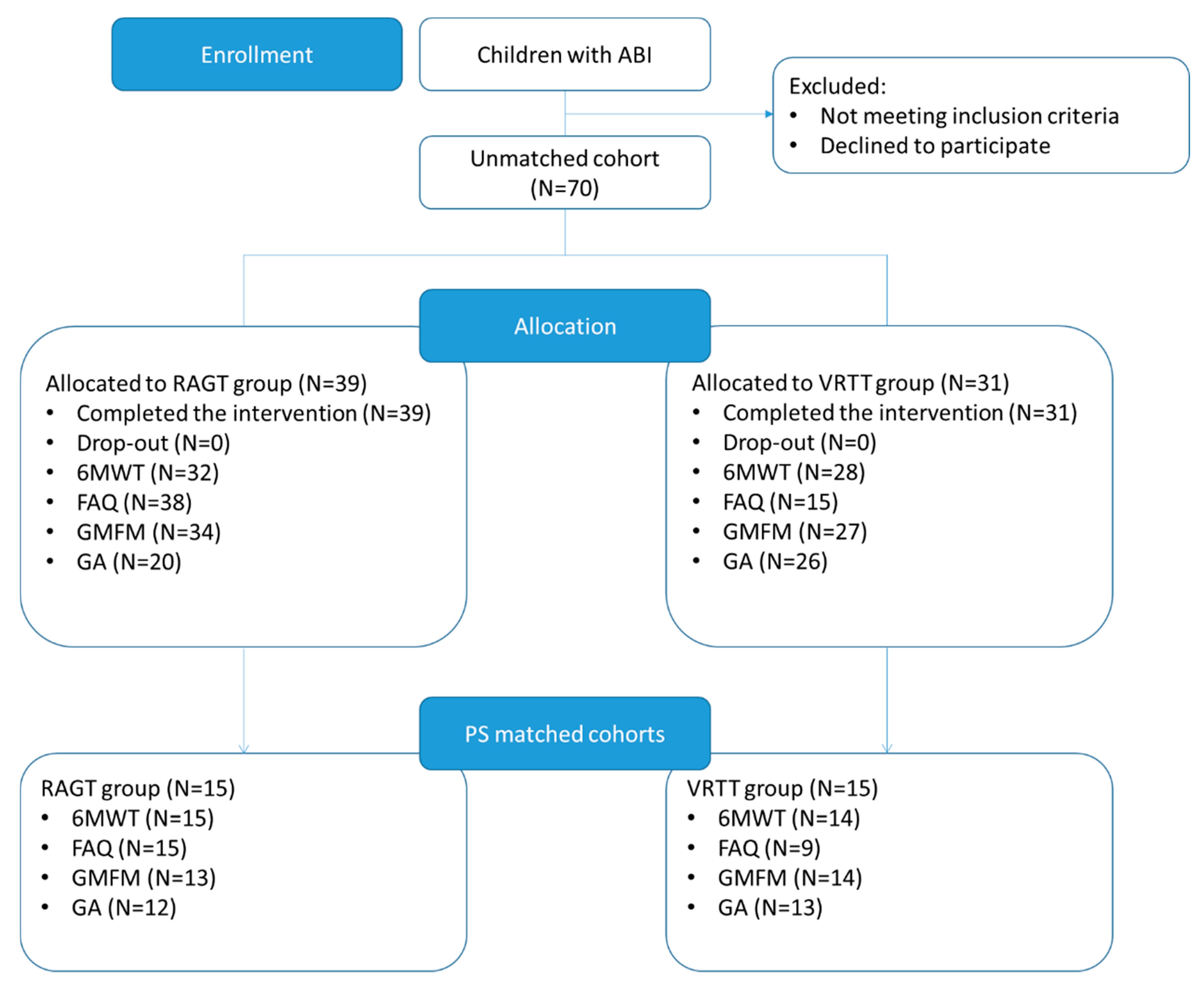
2.1. Participants
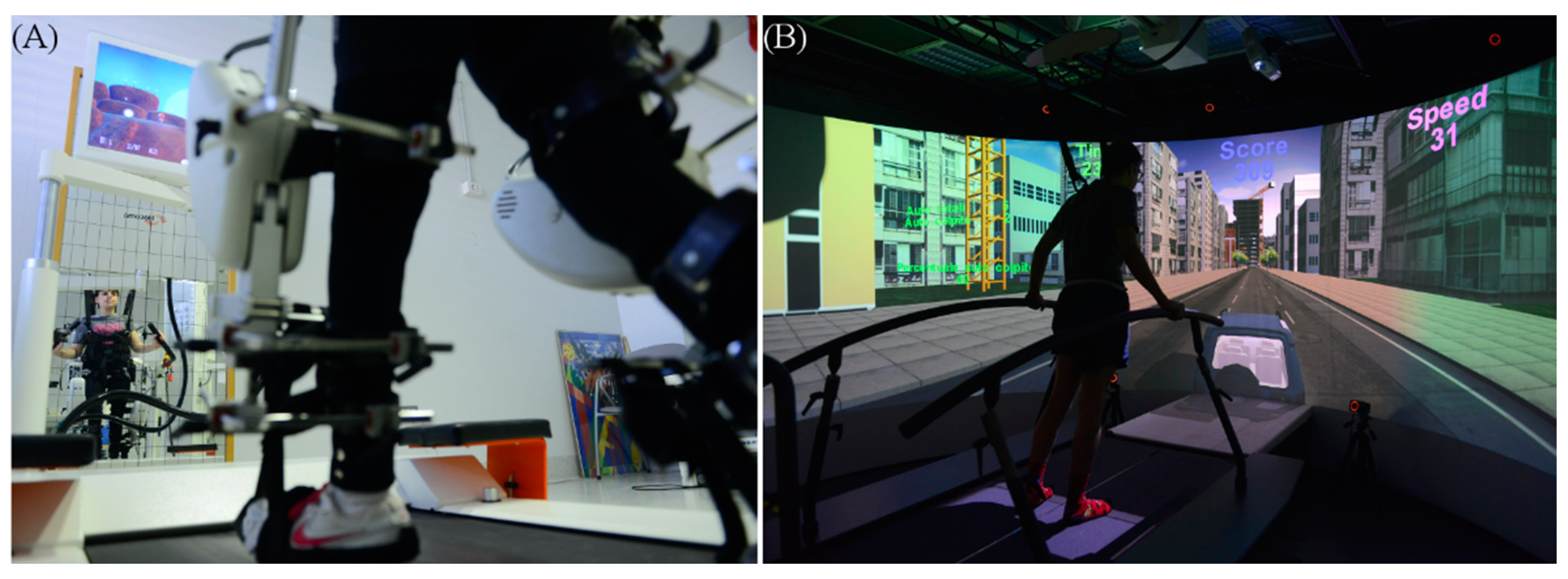
2.2. Intervention
2.2.1. Robot-Assisted Gait Training
2.2.2. Virtual Reality Plus Treadmill Training Gait Rehabilitation
2.3. Assessment
2.4. Data Analysis and Statistics
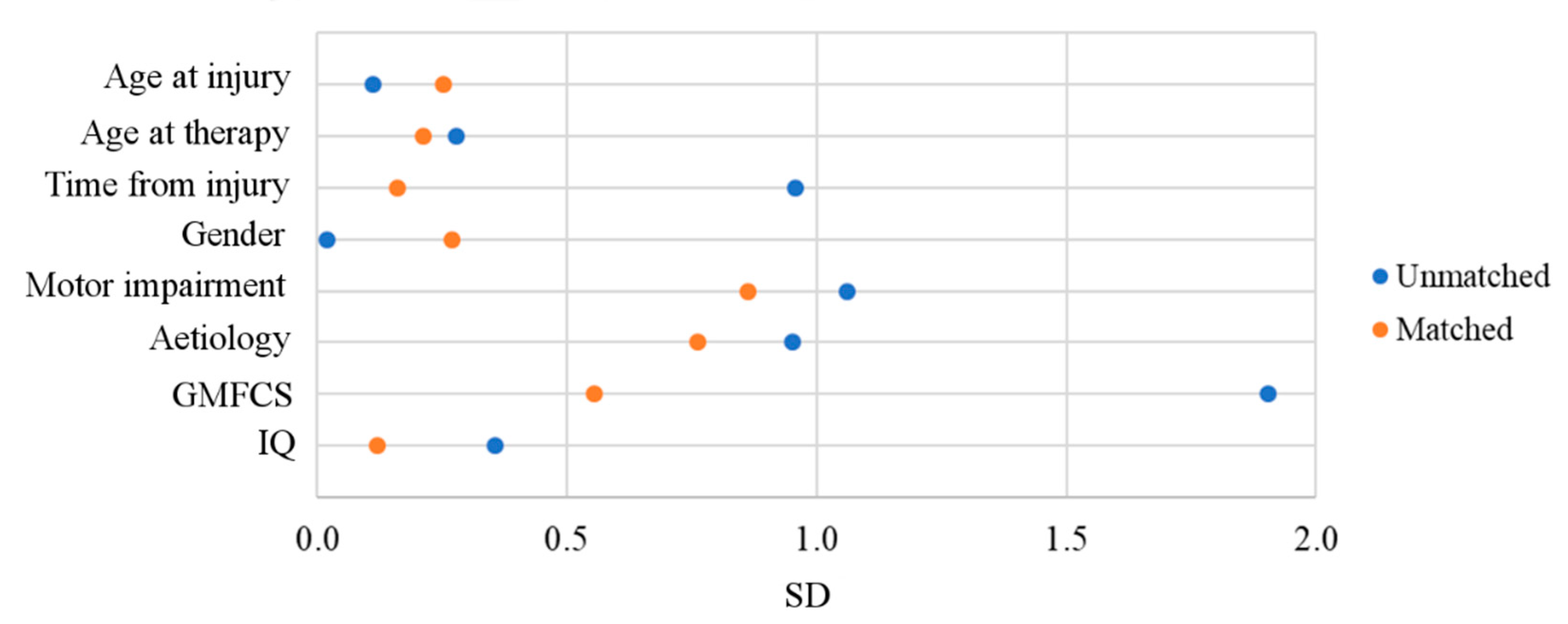
2.4.1. The Propensity Score Algorithm
2.4.2. Gait Parameters Extraction
2.4.3. Statistics
3. Results
3.1. Unmatched Cohort
3.2. Matched Cohorts
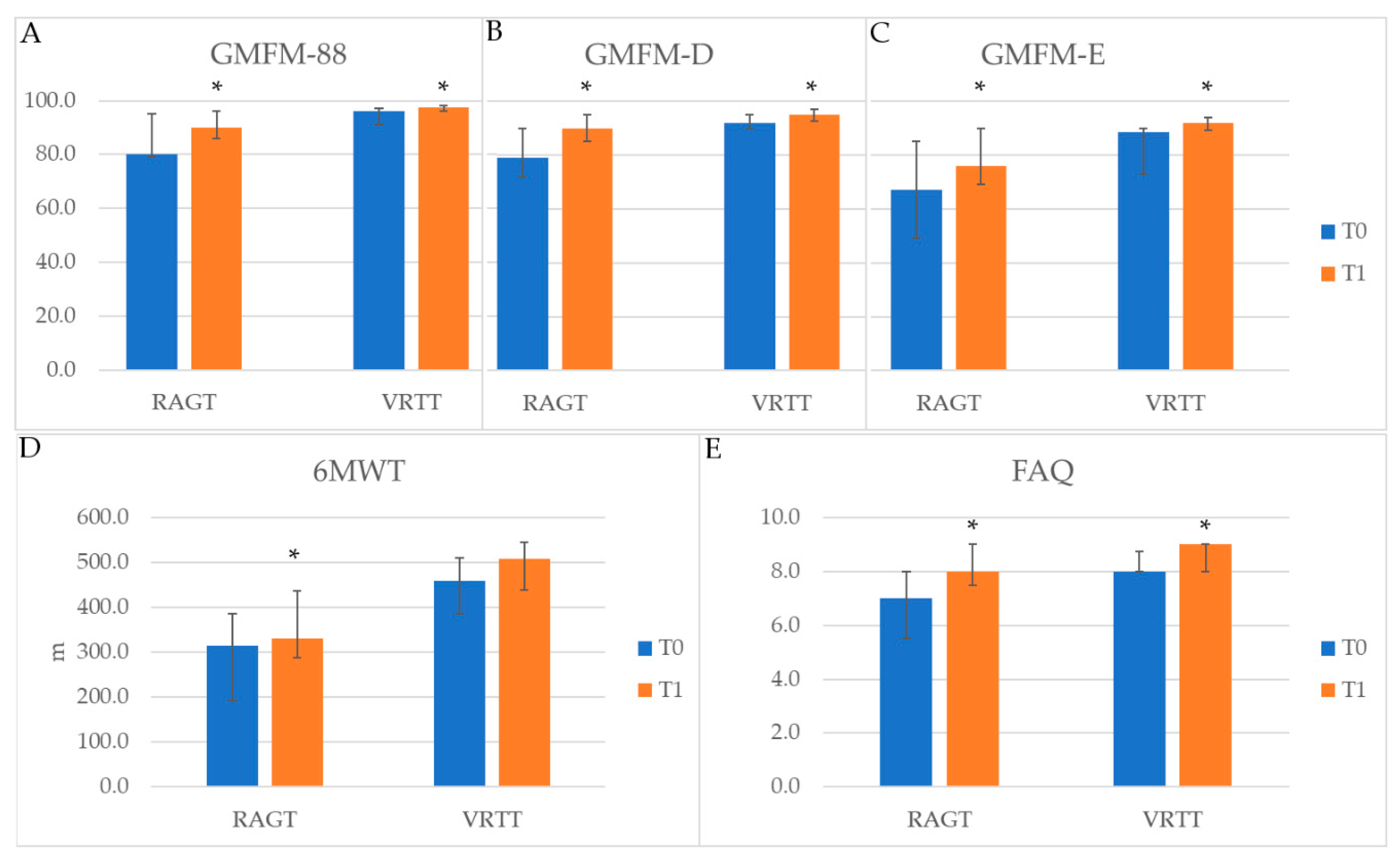
3.3. Outcomes in Matched Cohorts
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wong, C.P.; Forsyth, R.; Kelly, T.P.; Eyre, J.A. Incidence, aetiology, and outcome of non-traumatic coma: A population based study. Arch. Dis. Child. 2001, 84, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Gazzellini, S.; Strazzer, S.; Stortini, M.; Veredice, C.; Beretta, E.; Lispi, M.L.; Petacchi, M.E.; Menna, M.; Cipriani, P.; Zampolini, M.; et al. Pediatric rehabilitation of severe acquired brain injury: A multicenter survey. Eur. J. Phys. Rehabil. Med. 2012, 48, 423–431. [Google Scholar] [PubMed]
- Maranesi, E.; Riccardi, G.R.; Di Donna, V.; Di Rosa, M.; Fabbietti, P.; Luzi, R.; Pranno, L.; Lattanzio, F.; Bevilacqua, R. Effectiveness of Intervention Based on End-effector Gait Trainer in Older Patients With Stroke: A Systematic Review. J. Am. Med. Dir. Assoc. 2020, 21, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Thomas, S.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020. [Google Scholar]
- Yeh, S.; Lin, L.; Tam, K.; Tsai, C.; Hong, C.; Kuan, Y. Efficacy of robot-assisted gait training in multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2020, 41, 102034. [Google Scholar] [CrossRef]
- Fang, C.; Tsai, J.; Li, G.; Lien, A.S.; Chang, Y. Effects of robot-assisted gait training in individuals with spinal cord injury: A meta-analysis. BioMed Res. Int. 2020, 2020, 2102785. [Google Scholar] [CrossRef] [PubMed]
- Lefmann, S.; Russo, R.; Hillier, S. The effectiveness of robotic-assisted gait training for paediatric gait disorders: Systematic review. J. Neuroeng. Rehabil. 2017, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Jin, L.H.; Yang, S.-S.; Choi, J.Y.; Sohn, M.K. The Effect of Robot-Assisted Gait Training on Locomotor Function and Functional Capability for Daily Activities in Children with Cerebral Palsy: A Single-Blinded, Randomized Cross-Over Trial. Brain Sci. 2020, 10, 801. [Google Scholar] [CrossRef] [PubMed]
- Cherni, Y.; Ballaz, L.; Lemaire, J.; Maso, F.D.; Begon, M. Effect of low dose robotic-gait training on walking capacity in children and adolescents with cerebral palsy. Neurophysiol. Clin. 2020, 50, 507–519. [Google Scholar] [CrossRef]
- Carvalho, I.; Pinto, S.M.; Chagas, D.D.V.; Praxedes Dos Santos, J.L.; de Sousa Oliveira, T.; Batista, L.A. Robotic Gait Training for Individuals with Cerebral Palsy: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2017, 98, 2332–2344. [Google Scholar] [CrossRef]
- Petrarca, M.; Frascarelli, F.; Carniel, S.; Colazza, A.; Minosse, S.; Tavernese, E.; Castelli, E. Robotic-assisted locomotor treadmill therapy does not change gait pattern in children with cerebral palsy. Int. J. Rehabil. Res. 2021, 44, 69–76. [Google Scholar] [CrossRef]
- Druzbicki, M.; Rusek, W.; Snela, S.; Dudek, J.; Szczepanik, M.; Zak, E.; Durmala, J.; Czernuszenko, A.; Bonikowski, M.; Sobota, G. Functional effects of robotic-assisted locomotor treadmill thearapy in children with cerebral palsy. J. Rehabil. Med. 2013, 45, 358–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swinnen, E.; Lefeber, N. Benefits of robotic gait rehabilitation in cerebral palsy: Lessons to be learned. Dev. Med. Child Neurol. 2021, 63, 248–249. [Google Scholar] [CrossRef] [PubMed]
- Beretta, E.; Storm, F.A.; Strazzer, S.; Frascarelli, F.; Petrarca, M.; Colazza, A.; Cordone, G.; Biffi, E.; Morganti, R.; Maghini, C.; et al. Effect of Robot-Assisted Gait Training in a Large Population of Children With Motor Impairment Due to Cerebral Palsy or Acquired Brain Injury. Arch. Phys. Med. Rehabil. 2020, 101, 106–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beretta, E.; Molteni, E.; Biffi, E.; Morganti, R.; Avantaggiato, P.; Strazzer, S. Robotically-driven orthoses exert proximal-to-distal differential recovery on the lower limbs in children with hemiplegia, early after acquired brain injury. Eur. J. Paediatr. Neurol. 2018, 22, 652–661. [Google Scholar] [CrossRef]
- Beretta, E.; Romei, M.; Molteni, E.; Avantaggiato, P.; Strazzer, S. Combined robotic-aided gait training and physical therapy improve functional abilities and hip kinematics during gait in children and adolescents with acquired brain injury. Brain Inj. 2015, 29, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Karunakaran, K.K.; Ehrenberg, N.; Cheng, J.; Bentley, K.; Nolan, K.J. Kinetic Gait Changes after Robotic Exoskeleton Training in Adolescents and Young Adults with Acquired Brain Injury. Appl. Bionics Biomech. 2020, 2020, 8845772. [Google Scholar] [CrossRef] [PubMed]
- Ghai, S.; Ghai, I. Virtual Reality Enhances Gait in Cerebral Palsy: A Training Dose-Response Meta-Analysis. Front. Neurol. 2019, 10, 236. [Google Scholar] [CrossRef] [PubMed]
- Fandim, J.V.; Saragiotto, B.T.; Porfirio, G.J.M.; Santana, R.F. Effectiveness of virtual reality in children and young adults with cerebral palsy: A systematic review of randomized controlled trial. Braz. J. Phys. Ther. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, J.E.; McCoy, S.W. Virtual Reality and Serious Games in Neurorehabilitation of Children and Adults: Prevention, Plasticity, and Participation. Pediatr. Phys. Ther. 2017, 29 (Suppl. 3), S23–S36. [Google Scholar] [CrossRef] [PubMed]
- Peri, E.; Panzeri, D.; Beretta, E.; Reni, G.; Strazzer, S.; Biffi, E. Motor Improvement in Adolescents Affected by Ataxia Secondary to Acquired Brain Injury: A Pilot Study. BioMed Res. Int. 2019, 2019, 8967138. [Google Scholar] [CrossRef]
- Beretta, E.; Cesareo, A.; Maghini, C.; Turconi, A.C.; Reni, G.; Strazzer, S.; Biffi, E. An Immersive Virtual Reality Platform to Enhance Walking Ability of Children with Acquired Brain Injuries. Methods Inf. Med. 2017, 56, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Reiffel, J.A. Propensity-Score Matching: Optimal, Adequate, or Incomplete? J. Atr. Fibrillation 2018, 11, 2130. [Google Scholar] [CrossRef] [PubMed]
- Jupiter, D.C. Propensity Score Matching: Retrospective Randomization? J. Foot Ankle Surg. 2017, 56, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Jackman, M.; Novak, I.; Lannin, N. Effectiveness of functional hand splinting and the cognitive orientation to occupational performance (CO-OP) approach in children with cerebral palsy and brain injury: Two randomised controlled trial protocols. BMC Neurol. 2014, 14, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linder-Lucht, M.; Othmer, V.; Walther, M.; Vry, J.; Michaelis, U.; Stein, S.; Weissenmayer, H.; Korinthenberg, R.; Mall, V.; Validation of the Gross Motor Function Measure-Traumatic Brain Injury Study Group. Validation of the Gross Motor Function Measure for Use in Children and Adolescents With Traumatic Brain Injuries. Pediatrics 2007, 120, e880–e886. [Google Scholar] [CrossRef]
- Mossberg, K.A.; Fortini, E. Responsiveness and Validity of the Six-Minute Walk Test in Individuals with Traumatic Brain Injury. Phys. Ther. 2012, 92, 726–733. [Google Scholar] [CrossRef]
- Novacheck, T.F.; Stout, J.L.; Tervo, R. Reliability and validity of the Gillette Functional Assessment Questionnaire as an outcome measure in children with walking disabilities. J. Pediatr. Orthop. 2000, 20, 75–81. [Google Scholar] [CrossRef]
- Schwartz, M.H.; Rozumalski, A. The gait deviation index: A new comprehensive index of gait pathology. Gait Posture 2008, 28, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Storm, F.A.; Petrarca, M.; Beretta, E.; Strazzer, S.; Piccinini, L.; Maghini, C.; Panzeri, D.; Corbetta, C.; Morganti, R.; Reni, G.; et al. Minimum Clinically Important Difference of Gross Motor Function and Gait Endurance in Children with Motor Impairment: A Comparison of Distribution-Based Approaches. BioMed Res. Int. 2020, 2020, 2794036. [Google Scholar] [CrossRef]
- Schmid, S.; Romkes, J.; Taylor, W.R.; Lorenzetti, S.; Brunner, R. Orthotic correction of lower limb function during gait does not immediately influence spinal kinematics in spastic hemiplegic cerebral palsy. Gait Posture 2016, 49, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Flux, E.; van der Krogt, M.; Cappa, P.; Petrarca, M.; Desloovere, K.; Harlaar, J. The Human Body Model versus conventional gait models for kinematic gait analysis in children with cerebral palsy. Hum. Mov. Sci. 2020, 70, 102585. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Kim, J.; Arora, P.; Gaebler-Spira, D.J.; Zhang, Y. Effects of the Integration of Dynamic Weight Shifting Training Into Treadmill Training on Walking Function of Children with Cerebral Palsy: A Randomized Controlled Study. Am. J. Phys. Med. Rehabil. 2017, 96, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Harvey, R.L. Improving poststroke recovery: Neuroplasticity and task-oriented training. Curr. Treat. Options Cardiovasc. Med. 2009, 11, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Ishizuka, M.; Shibuya, N.; Takagi, K.; Hachiya, H.; Tago, K.; Sato, S.; Shimizu, T.; Matsumoto, T.; Aoki, T.; Kubota, K. Impact of anastomotic leakage on postoperative survival of patients with colorectal cancer: A meta-analysis using propensity score matching studies. Surg. Oncol. 2021, 37, 101538. [Google Scholar] [CrossRef] [PubMed]
- Stuart, E.A. Matching Methods for Causal Inference: A Review and a Look Forward. Stat. Sci. 2010, 25, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Evaluation Association. Using Propensity Scores with Small Samples; Annual Meetings of the American Evaluation Association; American Evaluation Association: San Antonio, TX, USA, 2010. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RAGT (N = 39) | VRTT (N = 31) | p-Value | |
|---|---|---|---|
| Age at injury, years * | 12.9 (8.6) | 10.6 (7.9) | 0.535 § |
| Age at therapy, years * | 13.5 (8.3) | 14.6 (5.8) | 0.295 § |
| Time from injury, years * | 0.5 (0.5) | 2.0 (3.0) | <0.001 § |
| Gender (male/female) * | 18/21 | 14/17 | 0.934 ‡ |
| Motor impairment (tetraparesis/R hemiparesis/L hemiparesis/ataxia/paraparesis/diplegia) | 13/11/7/8/0 | 4/2/6/18/1 | 0.004 ‡ |
| Aetiology (head trauma/stroke/tumour /encephalitis/AVM) * | 16/7/6/8/2 | 6/4/16/2/3 | 0.011 ‡ |
| GMFCS * | 1/13/14/11 | 4/27/0/0 | <0.001 ‡ |
| IQ * | 71.0 (21.8) | 77.0 (27.5) | 0.093 § |
| RAGT (N = 15) | VRTT (N = 15) | p-Value | |
|---|---|---|---|
| Age at injury, years * | 14.7 (9.7) | 9.5 (7.0) | 0.507 § |
| Age at therapy, years * | 15.0 (10.6) | 11.3 (5.2) | 0.604 § |
| Time from injury, years * | 0.5 (1.1) | 1.3 (1.3) | 0.351 § |
| Gender (male/female) * | 6/9 | 8/7 | 0.464 ‡ |
| Motor impairment (tetraparesis/R hemiparesis/L hemiparesis/ataxia/paraparesis/diplegia) | 1/7/4/3/0 | 2/2/4/7/0 | 0.194 ‡ |
| Aetiology (head trauma/stroke/tumour /encephalitis/AVM) * | 3/6/3/2/1 | 2/3/8/1/1 | 0.433 ‡ |
| GMFCS * | 1/13/1/0 | 0/15/0/0 | 0.343 ‡ |
| IQ * | 81.0 (18.0) | 87.0 (24.0) | 0.463 § |
| T0 | T1 | T0 vs. T1 | T1–T0 Change | |||
|---|---|---|---|---|---|---|
| Group | Median (IQR) | Median (IQR) | p-Value ~ (Time Effect) | Median (IQR) | p-Value ** (Group Effect) | |
| Velocity (ms−1) | RAGT | 0.55 (0.6) | 0.65 (0.35) | 0.112 | 0.1 (0.1) | 0.761 |
| VRTT | 0.7 (0.3) | 0.8 (0.2) | 0.165 | 0.1 (0.4) | ||
| Velocity/h (s−1) | RAGT | 34.76 (35.15) | 41 (22.02) | 0.117 | 2.48 (6.16) | 0.870 |
| VRTT | 55.08 (21.56) | 59.48 (16.29) | 0.279 | 5.68 (20.17) | ||
| Cadence (step·min−1) | RAGT | 92.1 (34.2) | 93 (21.9) | 0.423 | 0.6 (8.7) | 0.913 |
| VRTT | 108.6 (27) | 105.6 (22.2) | 0.624 | 4.2 (19.2) | ||
| Stride time (s) | RAGT | 1.31 (0.53) | 1.29 (0.30) | 0.505 | −0.01 (0.13) | 0.765 |
| VRTT | 1.12 (0.305) | 1.14 (0.24) | 0.363 | −0.04 (0.23) | ||
| Stance % (0–100) | RAGT | 66.01 (5.48) | 64.32 (3.08) | 0.099 | −1.26 (5.2) | 0.496 |
| VRTT | 62.84 (4.5) | 62.48 (3.83) | 0.249 | −0.9 (5.38) | ||
| GDI | RAGT | 81.9 (8.58) | 84.25 (9.11) | 0.158 | 0.83 (2.02) | 0.355 |
| VRTT | 85.82 (11.68) | 87.87 (11.94) | 0.028 | 3.33 (7.79) | ||
| Step width (m) | RAGT | 0.16 (0.05) | 0.14 (0.06) | 0.406 | −0.01 (0.04) | 0.913 |
| VRTT | 0.15 (0.04) | 0.15 (0.03) | 0.549 | 0.01 (0.03) | ||
| Step length (m) | RAGT | 0.38 (0.20) | 0.41 (0.19) | 0.020 | 0.028 (0.05) | 0.644 |
| VRTT | 0.41 (0.15) | 0.47 (0.09) | 0.108 | 0.06 (0.12) | ||
| Stride length (m) | RAGT | 0.76 (0.40) | 0.82 (0.39) | 0.023 | 0.05 (0.1) | 0.724 |
| VRTT | 0.82 (0.31) | 0.93 (0.17) | 0.124 | 0.11 (0.24) | ||
| T0 | T1 | T0 vs. T1 | T1–T0 Change | |||
|---|---|---|---|---|---|---|
| Group | Median (IQR) | Median (IQR) | p-Value ~ (Time Effect) | Median (IQR) | p-Value ** (Group Effect) | |
| Foot progression- Stance | RAGT | −19.5 (7.23) | −19.5 (11.35) | 0.695 | 0.06 (4.27) | 0.103 |
| VRTT | −20.05 (8.05) | −18.0 (11.34) | 0.033 | 3.45 (5.09) | ||
| Maximum ankle flexion a | RAGT | 11.6 (6.48) | 12.63 (7.96) | 0.875 | −0.33 (3.85) | 0.550 |
| VRTT | 7.45 (4.55) | 8.8 (6.65) | 0.701 | −0.40 (5.75) | ||
| Minimum ankle flexion b | RAGT | −12.9 (11.39) | −13.48 (7.79) | 0.388 | −2.4 (4.02) | 0.103 |
| VRTT | −17.85 (7.05) | −20.95 (10.4) | 0.009 | −4.0 (3.0) | ||
| ROM ankle flexion | RAGT | 16.08 (10.9) | 17.48 (9.55) | 0.432 | 0.6 (1.05) | 0.174 |
| VRTT | 14.8 (5.85) | 19.35 (5.65) | 0.023 | 3.4 (4.45) | ||
| Maximum knee flexion | RAGT | 48.15 (13.0) | 51.05 (12.08) | 0.388 | −0.01 (0.13) | 0.870 |
| VRTT | 52.6 (2.75) | 55.75 (6.1) | 0.753 | 2.5 (11.69) | ||
| Minimum knee flexion | RAGT | −5.95 (7.01) | −6.8 (4.15) | 0.433 | −0.48 (7.91) | 0.415 |
| VRTT | −4.7 (6.65) | −8.75 (10.05) | 0.023 | −2 (2.4) | ||
| ROM knee flexion | RAGT | 49.9 (15.8) | 55.93 (8.6) | 0.010 | 3.85 (4.43) | 0.480 |
| VRTT | 56.3 (8.75) | 58.95 (7.8) | 0.075 | 2.4 (3.1) | ||
| Maximum hip flexion | RAGT | 37.68 (4.29) | 38.3 (9.29) | 0.657 | 0.75 (4.7) | 0.355 |
| VRTT | 31.9 (9.85) | 32.05 (9.1) | 0.087 | −3.1 (3.3) | ||
| Minimum hip flexion | RAGT | 0.78 (13.3) | −8.93 (8.8) | 0.388 | −0.25 (11.9) | 0.913 |
| VRTT | −7.35 (13.1) | −10.45 (8.9) | 0.116 | −2.25 (5) | ||
| ROM hip flexion | RAGT | 38.15 (15.3) | 43.575 (9.7) | 0.034 | 3.3 (4.43) | 0.092 |
| VRTT | 41.8 (8.25) | 44.05 (6.6) | 0.875 | 0.5 (6.1) | ||
| ROM pelvic tilt | RAGT | 6.88 (3.88) | 7.5 (3.38) | 0.185 | 0.78 (1.01) | 0.901 |
| VRTT | 6.9 (3.15) | 7.55 (5.85) | 0.552 | 1.35 (4.15) | ||
| ROM pelvic obliquity | RAGT | 7.4 (3) | 9 (3.025) | 0.084 | 1.2 (2.8) | 0.327 |
| VRTT | 7.8 (3.3) | 9.1 (3.9) | 0.916 | 0.6 (4.3) | ||
| ROM pelvic rotation | RAGT | 0.44 (0.18) | 0.53 (0.16) | 0.041 | 0.12 (0.16) | 0.277 |
| VRTT | 0.5 (0.17) | 0.5 (0.16) | 0.650 | 0.02 (0.24) | ||
| RAGT (N = 15) | VRTT (N = 15) | p-Value ‡ | |
|---|---|---|---|
| 6MINWT | 8/6/1 | 6/8/0 | 0.463 |
| GMFM-88 | 7/6/0 | 3/11/0 | 0.081 |
| GMFM-D | 8/5/0 | 4/10/0 | 0.085 |
| GMFM-E | 9/4/0 | 7/7/0 | 0.310 |
| Step length | 1/11/0 | 1/12/0 | 0.953 |
| Maximum ankle flexion | 4/8/0 | 6/7/0 | 0.513 |
| Minimum ankle flexion | 3/9/0 | 4/9/0 | 0.748 |
| ROM ankle flexion | 2/9/1 | 3/10/0 | 0.545 |
| Maximum knee flexion | 4/6/2 | 1/11/1 | 0.168 |
| Minimum knee flexion | 1/7/4 | 0/11/2 | 0.284 |
| ROM knee flexion | 5/7/0 | 3/9/1 | 0.425 |
| Maximum hip flexion | 3/7/2 | 1/9/3 | 0.494 |
| Minimum hip flexion | 7/5/0 | 3/8/2 | 0.119 |
| ROM hip flexion | 4/7/1 | 3/9/1 | 0.838 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biffi, E.; Beretta, E.; Storm, F.A.; Corbetta, C.; Strazzer, S.; Pedrocchi, A.; Ambrosini, E. The Effectiveness of Robot- vs. Virtual Reality-Based Gait Rehabilitation: A Propensity Score Matched Cohort. Life 2021, 11, 548. https://doi.org/10.3390/life11060548
Biffi E, Beretta E, Storm FA, Corbetta C, Strazzer S, Pedrocchi A, Ambrosini E. The Effectiveness of Robot- vs. Virtual Reality-Based Gait Rehabilitation: A Propensity Score Matched Cohort. Life. 2021; 11(6):548. https://doi.org/10.3390/life11060548
Chicago/Turabian StyleBiffi, Emilia, Elena Beretta, Fabio Alexander Storm, Claudio Corbetta, Sandra Strazzer, Alessandra Pedrocchi, and Emilia Ambrosini. 2021. "The Effectiveness of Robot- vs. Virtual Reality-Based Gait Rehabilitation: A Propensity Score Matched Cohort" Life 11, no. 6: 548. https://doi.org/10.3390/life11060548