
Effect of Acupuncture on Functional Capacity in Patients Undergoing Hemodialysis: A Patient-Assessor Blinded Randomized Controlled Trial

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Settings
2.2. Participants
2.3. Intervention
2.4. Outcome Measurement
2.4.1. Six-Minute Walk Test (6MWT)
2.4.2. Thirty-Second Sit-to-Stand (STS-30) Test
2.4.3. Handgrip Strength (HGS) Test
2.5. Randomization and Blinding
2.6. Quality Control and Data Collection
2.7. Statistical Analysis and Sample Size
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Acupuncture Points | Location |
|---|---|
| KI3 (Taixi) | On the posteromedial aspect of the ankle, in the depression between the prominence of the medial malleolus and the calcaneal tendon. |
| SP6 (Sanyinjiao) | On the tibial aspect of the leg, posterior to the medial border of the tibia, 3 cun superior to the prominence of the medial malleolus. |
| ST36 (Zusanli) | On the anterior aspect of the leg, on the line connecting ST35 with ST41, 3 cun inferior to ST35, on the tibialis anterior muscle. |
| HT7 (Shenmen) | On the wrist, at the ulnar end of the transverse crease of the wrist, in the depression on the redial side of the tendon of m. flexor carpi ulnaris. |
| CV4 (Guanyuan) | On the lower abdomen, 3 cun inferior to the center of the umbilicus, on the anterior median line. |
| Non-Acupuncture Points | Location |
|---|---|
| Non-Acupuncture point 1 (NA1) | Located near KI3 (Taixi). On the posteromedial aspect of the ankle, at the midpoint of KI3 (Taixi) and KI7 (Fuliu). KI7 (Fuliu) is located on the posteromedial aspect of the leg, anterior to the calcaneal tendon, 2 cun superior to the prominence of the medial malleolus. |
| Non-Acupuncture point 2 (NA2) | Located near SP6 (Sanyinjiao). On the leg, at the midpoint of the medial side of the tibia, 1 cun distal from SP6 (Sanyinjiao). |
| Non-Acupuncture point 3 (NA3) | Located near ST36 (Zusanli). On the anterior aspect of the leg, at midpoint of ST37 (Shangjuxu) and the Gallbladder Meridian. ST37 (Shangjuxu) is located on the anterior aspect of the leg, on the line connecting ST35 with ST41, 6 cun inferior to ST35, on the tibialis anterior muscle. |
| Non-Acupuncture point 4 (NA4) | Located near HT7 (Shenmen). On the wrist, at the transverse crease of the wrist, at the midpoint of HT7 (Shenmen) and PC7 (Daling), between the Pericardium Meridian and Heart Meridian. |
| Non-Acupuncture point 5 (NA5) | Located near CV4 (Guanyuan). On the lower abdomen, 1 cun lateral from CV6 (Qihai). CV6 (Qihai) is located 1.5 cun inferior to the center of the umbilicus, on the anterior median line. |
| Screening | Baseline | Treatment Period | Follow-Up Period | ||||
|---|---|---|---|---|---|---|---|
| 0 Week | 1 Week | 3 Week | 9 Week | 12 Weeks after Treatment | |||
| Patient | Eligibility | X | |||||
| Informed Consent | X | ||||||
| Demographics and clinical data | X | ||||||
| Physical examination | X | ||||||
| Randomization Laboratorial data | X X | ||||||
| X | |||||||
| Intervention | Verum Acupuncture Subgroup A | 9 Acupuncture treatments (3 sessions per week for 3 weeks) | X | ||||
| Verum Acupuncture Subgroup B | 9 Acupuncture treatments (1 session per week for 9 weeks) | ||||||
| Comparison | Sham Acupuncture Subgroup A | 9 Acupuncture treatments in non-acupuncture points (3 sessions per week for 3 weeks) | X | ||||
| Sham Acupuncture Subgroup B | 9 Acupuncture treatments in non-acupuncture points (1 session per week for 9 weeks) | X | |||||
| Non-Acupuncture Group 0 | Non-Acupuncture Treatment | X | |||||
| Outcomes | 6MWT walked distance | X | X | X | X | ||
| Lower Limbs Strength | X | X | X | X | |||
| Handgrip Strength | X | X | X | X | |||
| Assessment of blinding success. | X | X | |||||
| Participant Safety | Adverse events | X | X | X | X | ||
References
- Wang, V.; Vilme, H.; Maciejewski, M.L.; Boulware, L.E. The Economic Burden of Chronic Kidney Disease and End-Stage Renal Disease. Semin. Nephrol. J. 2016, 36, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Elshahat, S.; Cockwell, P.; Maxwell, A.P.; Griffin, M.; O’Brien, T.; O’Neill, C. The impact of chronic kidney disease on developed countries from a health economics perspective: A systematic scoping review. PLoS ONE 2020, 15, e0230512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016–2040 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [Green Version]
- Group KDIGOKCW. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 2, 1–163. [Google Scholar] [CrossRef] [Green Version]
- Liew, A. Perspectives in renal replacement therapy: Haemodialysis. Nephrology 2018, 23, 95–99. [Google Scholar] [CrossRef] [Green Version]
- Golshayan, D.; Pascual, M. Burden of end-stage renal disease and evolving challenges in kidney transplantation. Transpl. Int. 2019, 32, 889–891. [Google Scholar] [CrossRef]
- Thurlow, J.S.; Joshi, M.; Yan, G.; Norris, K.C.; Agodoa, L.Y.; Yuan, C.M.; Nee, R. Global Epidemiology of End-Stage Kidney Disease and Disparities in Kidney Replacement Therapy. Am. J. Nephrol. 2021, 52, 98–107. [Google Scholar] [CrossRef]
- Johansen, K.L.; Shubert, T.; Doyle, J.; Soher, B.; Sakkas, G.K.; Kent-Braun, J.A. Muscle atrophy in patients receiving hemodialysis: Effects on muscle strength, muscle quality, and physical function. Kidney Int. 2003, 63, 291–297. [Google Scholar] [CrossRef] [Green Version]
- Morishita, S.; Tsubaki, A.; Shirai, N. Physical function was related to mortality in patients with chronic kidney disease and dialysis. Hemodial. Int. 2017, 21, 483–489. [Google Scholar] [CrossRef]
- Chu, S.W.F.; Ng, W.J.; Yeam, C.T.; Khan, R.Q.; Low, L.L.; Quah, J.H.M.; Foo, W.Y.M.; Seng, J.J.B. Manipulative and body-based methods in chronic kidney disease patients: A systematic review of randomized controlled trials. Complement. Ther. Clin. Pract. 2022, 48, 101593. [Google Scholar] [CrossRef]
- Yeam, C.T.; Yo, T.E.; Tan, Y.L.C.; Liew, A.; Seng, J.J.B. Complementary and alternative medicine therapies for uremic pruritus—A systematic review of randomized controlled trials. Complement. Ther. Med. 2021, 56, 102609. [Google Scholar] [CrossRef] [PubMed]
- Xiong, W.; He, F.F.; You, R.Y.; Xiong, J.; Wang, Y.M.; Zhang, C.; Meng, X.F.; Su, H. Acupuncture Application in Chronic Kidney Disease and its Potential Mechanisms. Am. J. Chin. Med. 2018, 46, 1169–1185. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Kim, T.H.; Kang, J.W.; Sul, J.U.; Lee, M.S.; Kim, J.I.; Shin, M.S.; Jung, S.Y.; Kim, A.R.; Kang, K.W.; et al. Acupuncture for symptom management in hemodialysis patients: A prospective, observational pilot study. J. Altern. Complement. Med. 2011, 17, 741–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bullen, A.; Awdishu, L.; Lester, W.; Moore, T.; Trzebinska, D. Effect of Acupuncture or Massage on Health-Related Quality of Life of Hemodialysis Patients. J. Altern. Complement. Med. 2018, 24, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.S.; Ho, C.H.; Wang, H.Y.; Chen, Y.H.; Hsieh, C.L. Acupuncture on Renal Function in Patients with Chronic Kidney Disease: A Single-Blinded, Randomized, Preliminary Controlled Study. J. Altern. Complement. Med. 2017, 23, 624–631. [Google Scholar] [CrossRef]
- Kim, K.H.; Lee, M.S.; Kim, T.H.; Kang, J.W.; Choi, T.Y.; Lee, J.D. Acupuncture and related interventions for symptoms of chronic kidney disease. Cochrane Database Syst. Rev. 2016, 6, Cd009440. [Google Scholar] [CrossRef]
- Soares Mendes Damasceno, G.; Teixeira, T.H.M.M.; Souza, V.C.D.; Neiva, T.S.; Prudente Pereira, K.; Teles Landim, M.D.F.; Melo, G.F.D.; Tolêdo Nóbrega, O.; de Azevedo, C. Acupuncture Treatment in Elderly People with Sarcopenia: Effects on the Strength and Inflammatory Mediators. J. Aging Res. 2019, 2019, 8483576. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.; Huang, L.P.; Liu, J.; Yu, J.H.; Tian, Q.; Cao, L.J. Bilateral effects of 6 weeks’ unilateral acupuncture and electroacupuncture on ankle dorsiflexors muscle strength: A pilot study. Arch. Phys. Med. Rehabil. 2012, 93, 50–55. [Google Scholar] [CrossRef]
- Wang, Y.; Hou, Y.Q.; Yang, J.W.; Wang, L.Q.; Shao, J.K.; Zou, X.; Yang, N.N.; Huang, J.; Liu, C.Z. Acupuncture of different treatment frequency in postprandial distress syndrome: A pilot randomized clinical trial. Neurogastroenterol. Motil. 2020, 32, e13812. [Google Scholar] [CrossRef]
- Lin, L.L.; Tu, J.F.; Wang, L.Q.; Yang, J.W.; Shi, G.X.; Li, J.L.; Zhang, N.; Shao, J.K.; Zou, X.; Liu, C.Z. Acupuncture of different treatment frequencies in knee osteoarthritis: A pilot randomised controlled trial. Pain 2020, 161, 2532–2538. [Google Scholar] [CrossRef]
- Ma, S.X. Establishing an adequate dose of acupuncture is essential for clinical trial studies. Clin. Res. Trials 2020, 6, 295. [Google Scholar] [CrossRef]
- Maciocia, G. (Ed.) The Foundations of Chinese Medicine. A Comprehensive Text, 3rd ed.; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Li, W.F.D. Clinical nephrology. In Chinese Medicine; Blue Poppy Press: Portland, OR, USA, 2003. [Google Scholar]
- Matos, L.C.; Machado, J.P.; Monteiro, F.J.; Greten, H.J. Understanding Traditional Chinese Medicine Therapeutics: An Overview of the Basics and Clinical Applications. Healthcare 2021, 9, 257. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Yuan, C.S. Clinical Handbook of Chinese Medicine; World Scientific: Singapore, 2013. [Google Scholar]
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT statement. PLoS Med. 2010, 7, e1000261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS Statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, P.H.S.; de Souza Veloso, L.R.; Lima, M.M.O.; Vieira, C.F.D.; Alves, F.L.; Lacerda, A.C.R.; Lima, V.P.; Rodrigues, V.G.B.; Maciel, E.H.B.; Costa, H.S. The reliability and validity of the 30-seconds sit-to-stand test and its capacity for assessment of the functional status of hemodialysis patients. J. Bodyw. Mov. Ther. 2021, 27, 157–164. [Google Scholar] [CrossRef]
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef]
- Bobos, P.; Nazari, G.; Lu, Z.; MacDermid, J.C. Measurement Properties of the Hand Grip Strength Assessment: A Systematic Review With Meta-analysis. Arch. Phys. Med. Rehabil. 2020, 101, 553–565. [Google Scholar] [CrossRef]
- Bohannon, R.W. Test-Retest Reliability of Measurements of Hand-Grip Strength Obtained by Dynamometry from Older Adults: A Systematic Review of Research in the PubMed Database. J. Frailty Aging 2017, 6, 83–87. [Google Scholar] [CrossRef]
- Leal, V.O.; Mafra, D.; Fouque, D.; Anjos, L.A. Use of handgrip strength in the assessment of the muscle function of chronic kidney disease patients on dialysis: A systematic review. Nephrol. Dial. Transplant. 2011, 26, 1354–1360. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM SPSS Statistics for Windows; Version 27.0; IBM Corp.: Armonk, NY, USA, 2020. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- James, K.E.; Bloch, D.A.; Lee, K.K.; Kraemer, H.C.; Fuller, R.K. An index for assessing blindness in a multi-centre clinical trial: Disulfiram for alcohol cessation—A VA cooperative study. Stat. Med. 1996, 15, 1421–1434. [Google Scholar] [CrossRef]
- Kolahi, J.; Bang, H.; Park, J. Towards a proposal for assessment of blinding success in clinical trials: Up-to-date review. Community Dent. Oral Epidemiol. 2009, 37, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.M.N. Blinding Assessment Indexes for Randomized, Controlled, Clinical Trials. 2021. Available online: https://cran.r-project.org/web/packages/BI/index.html (accessed on 24 September 2022).
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Kittiskulnam, P.; Sheshadri, A.; Johansen, K.L. Consequences of CKD on Functioning. Semin. Nephrol. 2016, 36, 305–318. [Google Scholar] [CrossRef] [Green Version]
- Yuan, J.; Purepong, N.; Hunter, R.F.; Kerr, D.P.; Park, J.; Bradbury, I.; McDonough, S. Different frequencies of acupuncture treatment for chronic low back pain: An assessor-blinded pilot randomised controlled trial. Complement. Ther. Med. 2009, 17, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Klein, J.D.; Hassounah, F.; Cai, H.; Zhang, C.; Xu, P.; Wang, X.H. Low-frequency electrical stimulation attenuates muscle atrophy in CKD--a potential treatment strategy. J. Am. Soc. Nephrol. 2015, 26, 626–635. [Google Scholar] [CrossRef] [Green Version]
- Langevin, H.M.; Churchill, D.L.; Cipolla, M.J. Mechanical signaling through connective tissue: A mechanism for the therapeutic effect of acupuncture. FASEB J. 2001, 15, 2275–2282. [Google Scholar] [CrossRef] [Green Version]
- De Moraes Kohl, L.; Signori, L.U.; Ribeiro, R.A.; Silva, A.M.V.; Moreira, P.R.; Dipp, T.; Sbruzzi, G.; Lukrafka, J.L.; Plentz, R.D.M. Prognostic value of the six-minute walk test in end-stage renal disease life expectancy: A prospective cohort study. Clinics 2012, 67, 581–586. [Google Scholar] [CrossRef]
- Hwang, S.H.; Lee, D.H.; Min, J.; Jeon, J.Y. Handgrip Strength as a Predictor of All-Cause Mortality in Patients With Chronic Kidney Disease Undergoing Dialysis: A Meta-Analysis of Prospective Cohort Studies. J. Ren. Nutr. 2019, 29, 471–479. [Google Scholar] [CrossRef]
- Vogt, B.P.; Borges, M.C.C.; Goés, C.R.; Caramori, J.C.T. Handgrip strength is an independent predictor of all-cause mortality in maintenance dialysis patients. Clin. Nutr. 2016, 35, 1429–1433. [Google Scholar] [CrossRef]
- Matos, C.M.; Silva, L.F.; Santana, L.D.; Santos, L.S.; Protásio, B.M.; Rocha, M.T.; Ferreira, V.L.; Azevedo, M.F.; Martins, M.T.S.; Lopes, G.B.; et al. Handgrip strength at baseline and mortality risk in a cohort of women and men on hemodialysis: A 4-year study. J. Ren. Nutr. 2014, 24, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Goh, Z.S.; Griva, K. Anxiety and depression in patients with end-stage renal disease: Impact and management challenges—A narrative review. Int. J. Nephrol. Renovasc. Dis. 2018, 11, 93–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Regional Office for the Western Pacific. WHO Standard Acupuncture Point Locations in the Western Pacific Region; World Health Organization: Manila, Philippines, 2008.
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]


| Experimental Group | Placebo Group | Control Group | ||||
|---|---|---|---|---|---|---|
| Verum Acupuncture (VA) | Sham Acupuncture (SA) | Waiting-List (WL) | ||||
| DETAILS OF NEEDLING | Number of needles | 5 fixed acupoints and a total of 8 needle insertions per subject and session. | 5 fixed acupoints and a total of 8 needle insertions per subject and session. | No acupuncture treatment will be performed from the time of randomization until the end of the follow-up period. | ||
| Names of points used | Taixi (KI3), bilateral. Sanyinjiao (SP6), bilateral. Zusanli (ST36), bilateral. Shenmen (HT7) unilateral, in the arm without arteriovenous fistula. Guanyuan (CV4), unilateral. | Non-acupuncture points near the acupuncture points selected as described in Appendix A, Table A2. | ||||
| Depth of insertion | CV4, ST36, KI3 and SP6 were inserted perpendicularly (15 to 20 mm depth) and HT7 was inserted slightly oblique (10 mm depth). | Superficial needling (5 mm depth) at non-acupuncture points abovementioned. | ||||
| Response sought | De qi sensation (described as a compositional sensation including numbness, soreness, distention, heaviness) was achieved through lifting, thrusting and twirling manipulations. | No De qi sensation. | ||||
| Needle stimulation | Manual stimulation. After generating needling sensation, needles were manipulated for one minute every ten minutes during needle retention. | No stimulation. | ||||
| Needle retention time | 25 min. | 25 min. | ||||
| Needle type | Sterilized stainless-steel needle (0.25 × 25 mm) Tewa, asia-med GmbH, Kirchplatz 182,049 Pullach, Germany. | Sterilized stainless-steel needle (0.25 × 25 mm) Tewa, asia-med GmbH, Kirchplatz 182,049 Pullach, Germany. | ||||
| TREATMENT REGIMEN | Number of treatment sessions | 9 treatment sessions. | 9 treatment sessions. | Not applicable. | ||
| Frequency of treatment sessions | VA subgroup A (VA.A) Three times a week for 3 weeks. (3 × 3) | VA subgroup B (VA.B) Once a week for 9 weeks. (1 × 9) | SA subgroup A (SA.A) Three times a week for 3 weeks. (3 × 3) | SA subgroup B (SA.B) Once a week for 9 weeks. (1 × 9) | ||
| Variables | Total (n = 67) | Verum Acupuncture Group (n = 23) | Sham Acupuncture Group (n = 22) | Non-Acupuncture Group (n = 22) | p |
|---|---|---|---|---|---|
| Sociodemographic | |||||
| Sex | |||||
| Female | 26 (38.8%) | 9 (39.1%) | 8 (36.4%) | 9 (40.9%) | 1.000 (1) |
| Male | 41 (61.2%) | 14 (60.9%) | 14 (63.6%) | 13 (59.1%) | |
| Age | |||||
| Minimum–Maximum | 56–91 | 60–84 | 57–91 | 56–87 | |
| Mean (SD) | 71.6 (7.7) | 71.2 (5.1) | 72.6 (8.3) | 71.0 (9.4) | 0.764 (2) |
| Residence | |||||
| Urban | 24 (35.8%) | 9 (39.1%) | 8 (36.4%) | 7 (31.8%) | 0.948 (1) |
| Rural | 43 (64.2%) | 14 (60.9%) | 14 (63.6%) | 15 (68.2%) | |
| Education level | |||||
| No literacy | 5 (7.5%) | 0 (0.0%) | 2 (9.1%) | 3 (13.6%) | 0.279 (1) |
| 1° Cycle (4 years) | 49 (73.1%) | 20 (87.0%) | 17 (77.3%) | 12 (54.5%) | |
| 2° Cycle (6 years) | 7 (10.4%) | 2 (8.7%) | 1 (4.5%) | 4 (18.2%) | |
| 3° Cycle (9 years) | 1 (1.5%) | 0 (0.0%) | 0 (0.0%) | 1 (4.5%) | |
| High school (12 years) | 5 (7.5%) | 1 (4.3%) | 2 (9.1%) | 2 (9.1%) | |
| Professional status | |||||
| Employed | 4 (6.0%) | 0 (0.0%) | 2 (9.1%) | 2 (9.1%) | 0.481 (1) |
| Self-employed | 4 (6.0%) | 2 (8.7%) | 0 (0.0%) | 2 (9.1%) | |
| Unemployed | 2 (3.0%) | 1 (4.3%) | 1 (4.5%) | 0 (0.0%) | |
| Retired | 57 (85.1%) | 20 (87.0%) | 19 (86.4%) | 18 (81.8%) | |
| Clinical | |||||
| CKD causes | |||||
| Diabetes mellitus | 29 (43.3%) | 10 (43.5%) | 10 (45.5%) | 9 (40.9%) | 0.537 (1) |
| Chronic rejection | 7 (10.4%) | 1 (4.3%) | 4 (18.2%) | 2 (9.1%) | |
| Hypertensive nephropathy | 4 (6.0%) | 3 (13.0%) | 0 (0.0%) | 1 (4.5%) | |
| High blood pressure | 2 (3.0%) | 0 (0.0%) | 1 (4.5%) | 1 (4.5%) | |
| Glomerulonephritis | 2 (3.0%) | 1 (4.3%) | 0 (0.0%) | 1 (4.5%) | |
| Polycystic disease | 2 (3.0%) | 0 (0.0%) | 0 (0.0%) | 2 (9.1%) | |
| Interstitial tubular necrosis | 2 (3.0%) | 0 (0.0%) | 2 (9.1%) | 0 (0.0%) | |
| Other | 5 (7.5%) | 3 (13.0%) | 1 (4.5%) | 1 (4.5%) | |
| Unknown | 14 (20.9%) | 5 (21.7%) | 4 (18.2%) | 5 (22.7%) | |
| Hemodialysis time | |||||
| <12 months | 2 (3.0%) | 2 (8.7%) | 0 (0.0%) | 0 (0.0%) | 0.240 (1) |
| 12 to 120 months | 56 (83.6%) | 19 (82.6%) | 20 (90.9%) | 17 (77.3%) | |
| >120 months | 9 (13.4%) | 2 (8.7%) | 2 (9.1%) | 5 (22.7%) | |
| Vascular access | |||||
| Arteriovenous fistula | 61 (91.0%) | 22 (95.7%) | 18 (81.8%) | 21 (95.5%) | 0.306 (1) |
| Central venous catheter | 6 (9.0%) | 1 (4.3%) | 4 (18.2%) | 1 (4.5%) | |
| Laboratorial | Mean (SD) | ||||
| Hemoglobin | 10.93 (1.03) | 10.88 (0.94) | 10.86 (1.05) | 11.05 (1.12) | 0.797 (2) |
| Potassium | 5.44 (0.81) | 5.52 (0.89) | 5.35 (0.81) | 5.45 (0.74) | 0.799 (2) |
| Calcium | 9.11 (0.51) | 9.13 (0.55) | 9.10 (0.49) | 9.10 (0.51) | 0.970 (2) |
| Phosphorus | 4.74 (1.13) | 4.71 (1.17) | 4.70 (1.25) | 4.80 (1.00) | 0.944 (2) |
| Sodium | 138.1 (3.0) | 138.5 (2.9) | 138.6 (3.8) | 137.3 (2.0) | 0.296 (2) |
| Albumin | 3.91 (0.28) | 3.98 (0.27) | 3.81 (0.27) | 3.95 (0.29) | 0.101 (2) |
| Urea (before) | 152.6 (37.5) | 161.0 (37.9) | 145.3 (36.2) | 151.0 (38.3) | 0.369 (2) |
| Creatinine | 9.94 (2.12) | 10.15 (2.26) | 9.51 (1.94) | 10.16 (2.16) | 0.514 (2) |
| Parathyroid hormone | 418.0 (243.2) | 454.2 (256.9) | 358.2 (193.3) | 439.9 (271.5) | 0.370 (2) |
| Cholesterol | 162.8 (37.1) | 166.0 (47.2) | 155.5 (35.8) | 166.6 (25.0) | 0.536 (2) |
| Effects | 6MWT | STS-30 Test | HGS Test |
|---|---|---|---|
| Time | p = 0.001, η2p = 0.114 | p < 0.001, η2p = 0.240 | p = 0.004, η2p = 0.168 |
| Interaction time*group | p < 0.001, η2p = 0.521 | p < 0.001, η2p = 0.600 | p = 0.032, η2p = 0.083 |
| Interaction time*treatment frequency | p = 0.172, η2p = 0.028 | p = 0.438, η2p = 0.027 | p = 0.843, η2p = 0.002 |
| Verum Acupuncture (VA) Group (n = 23) | Sham Acupuncture (SA) Group (n = 22) | Waiting-List (WL) Group (n = 22) | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |
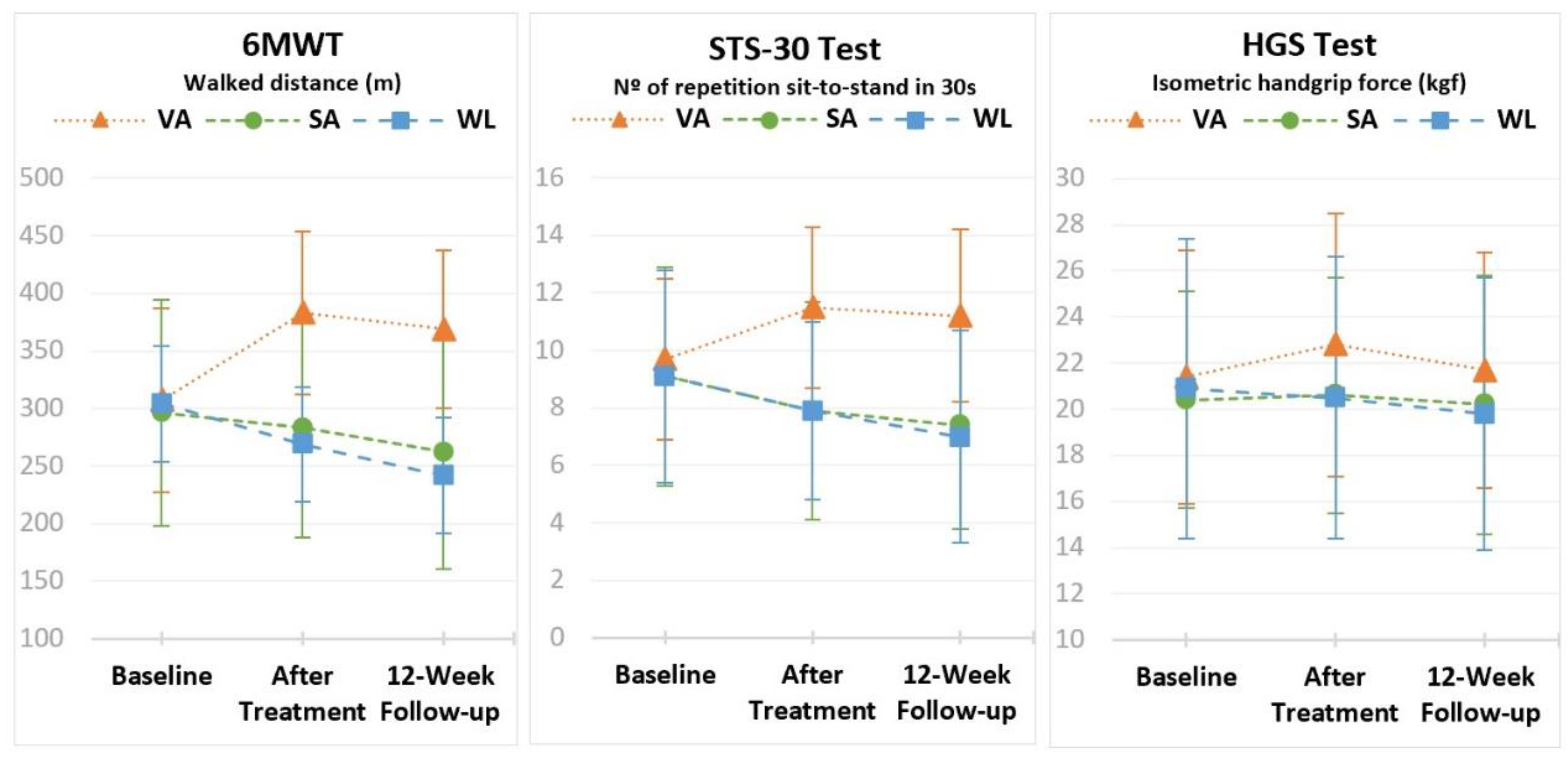
| 6MWT, Walked distance (m) | |||
| Baseline | 307.2 ± 80.1 a | 296.2 ± 97.8 a | 304.1 ± 119.3 a |
| After treatment | 383.2 ± 70.7 b | 283.4 ± 95.2 a | 268.8 ± 113.8 b |
| Follow-up | 368.9 ± 68.2 b | 262.5 ± 101.8 b | 241.7 ± 118.1 c |
| ANOVA (1) | p < 0.001 | p < 0.001 | p < 0.001 |
| Interaction time*group | p < 0.001, η2p = 0.509 | ||
| STS-30 Test, Repetition number of sit-to-stand in 30 s | |||
| Baseline | 9.7 ± 2.8 a | 9.1 ± 3.8 a | 9.1 ± 3.7 a |
| After treatment | 11.5 ± 2.8 b | 7.9 ± 3.8 b | 7.9 ± 3.1 b |
| Follow-up | 11.2 ± 3.0 b | 7.4 ± 3.6 b | 7.0 ± 3.7 c |
| ANOVA (1) | p < 0.001 | p < 0.001 | p < 0.001 |
| Interaction time*group | p < 0.001, η2p = 0.565 | ||
| HGS Test, Isometric handgrip force (kgf) | |||
| Baseline | 21.4 ± 5.5 a | 20.4 ± 4.7 a | 20.9 ± 6.5 a |
| After treatment | 22.8 ± 5.7 b | 20.6 ± 5.1 a | 20.5 ± 6.1 a |
| Follow-up | 21.7 ± 5.1 ab | 20.2 ± 5.6 a | 19.8 ± 5.9 a |
| ANOVA (1) | p = 0.012 | p = 0.601 | p = 0.112 |
| Interaction time*group | p = 0.043, η2p = 0.083 | ||
| Participants’ Guess, n (%) | |||
|---|---|---|---|
| Groups | Verum Acupuncture | Sham Acupuncture | Do Not Know |
| Verum Acupuncture (n = 23) | 7 (30.4%) | 0 (0.0%) | 16 (69.6%) |
| Sham Acupuncture (n = 22) | 7 (31.8%) | 0 (0.0%) | 15 (68.2%) |
| Total (n = 45) | 14 (31.1%) | 0 (0.0%) | 31 (68.9%) |
| Blinding Index: 0.84 (95% Confidence Interval: 0.78–0.91) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Correia de Carvalho, M.; Nunes de Azevedo, J.; Azevedo, P.; Pires, C.; Laranjeira, M.; Machado, J.P. Effect of Acupuncture on Functional Capacity in Patients Undergoing Hemodialysis: A Patient-Assessor Blinded Randomized Controlled Trial. Healthcare 2022, 10, 1947. https://doi.org/10.3390/healthcare10101947
Correia de Carvalho M, Nunes de Azevedo J, Azevedo P, Pires C, Laranjeira M, Machado JP. Effect of Acupuncture on Functional Capacity in Patients Undergoing Hemodialysis: A Patient-Assessor Blinded Randomized Controlled Trial. Healthcare. 2022; 10(10):1947. https://doi.org/10.3390/healthcare10101947
Chicago/Turabian StyleCorreia de Carvalho, Marta, José Nunes de Azevedo, Pedro Azevedo, Carlos Pires, Manuel Laranjeira, and Jorge Pereira Machado. 2022. "Effect of Acupuncture on Functional Capacity in Patients Undergoing Hemodialysis: A Patient-Assessor Blinded Randomized Controlled Trial" Healthcare 10, no. 10: 1947. https://doi.org/10.3390/healthcare10101947