
Urinary Volatile Organic Compound Metabolites Are Associated with Reduced Lung Function in U.S. Children and Adolescents
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Urinary VOC Metabolites
2.3. Spirometry
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Distribution of Urinary VOC Metabolites
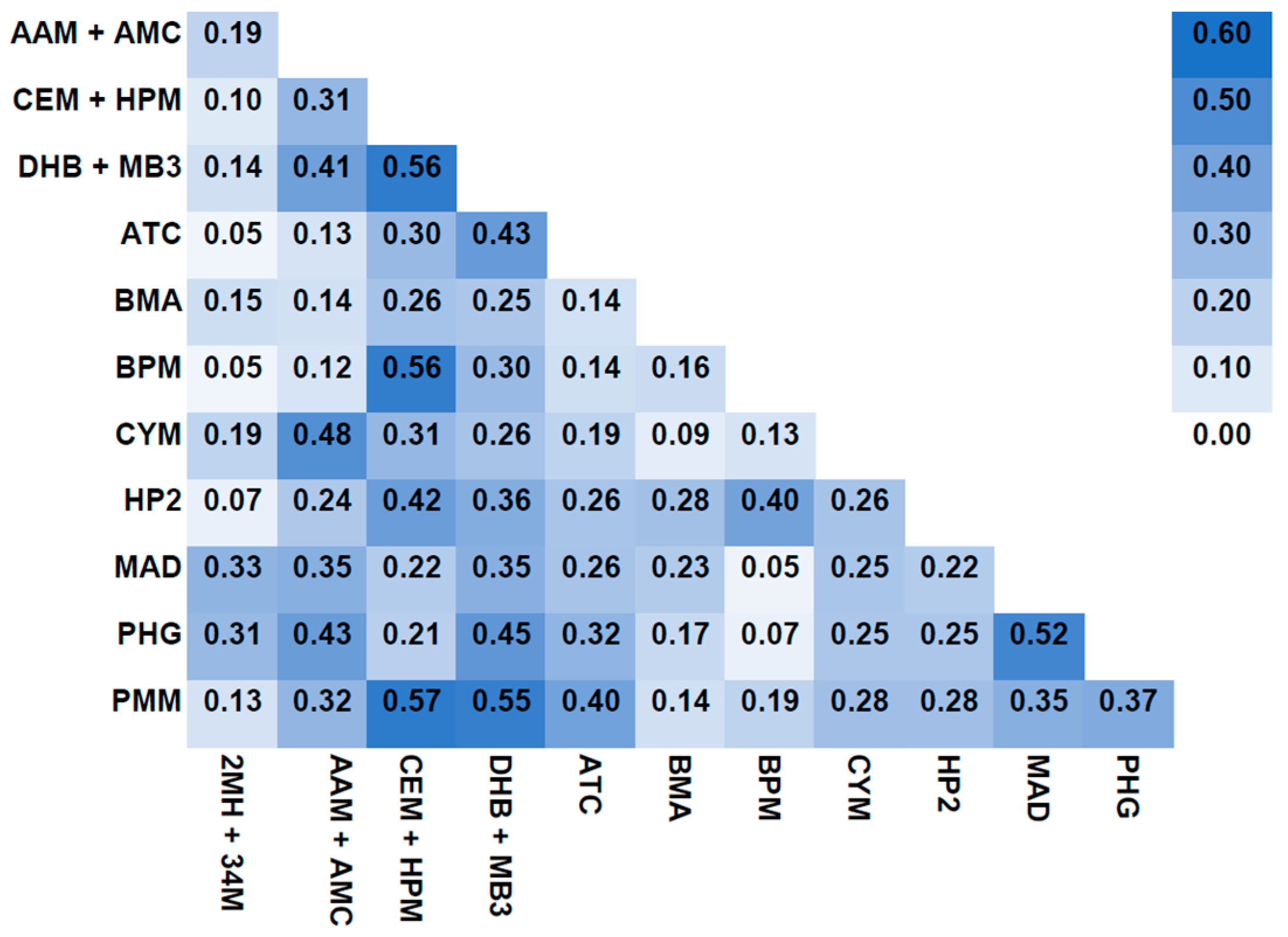
3.2. Urinary VOC Metabolites Intercorrelation
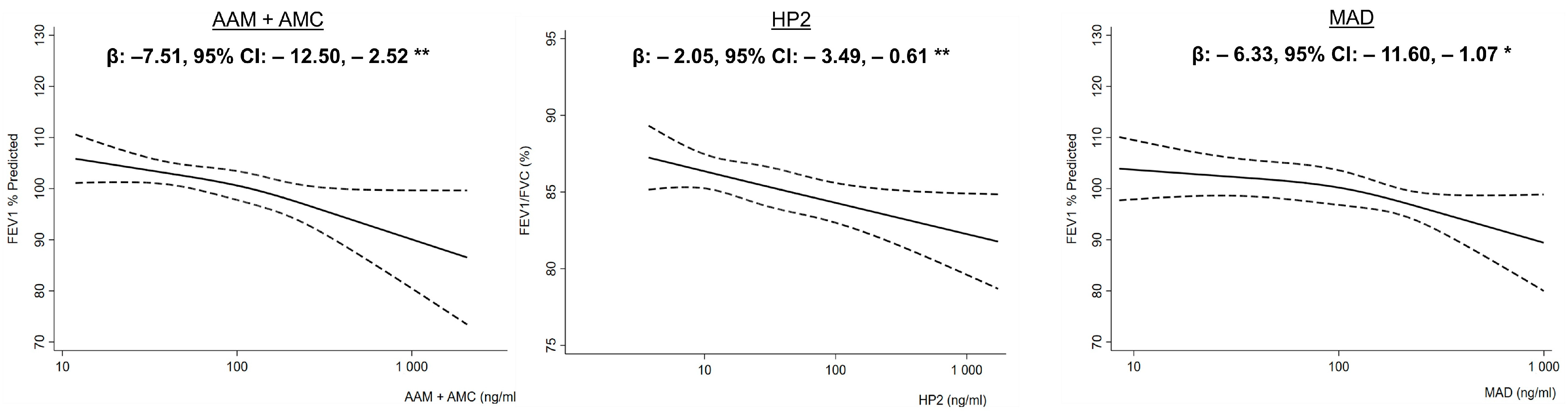
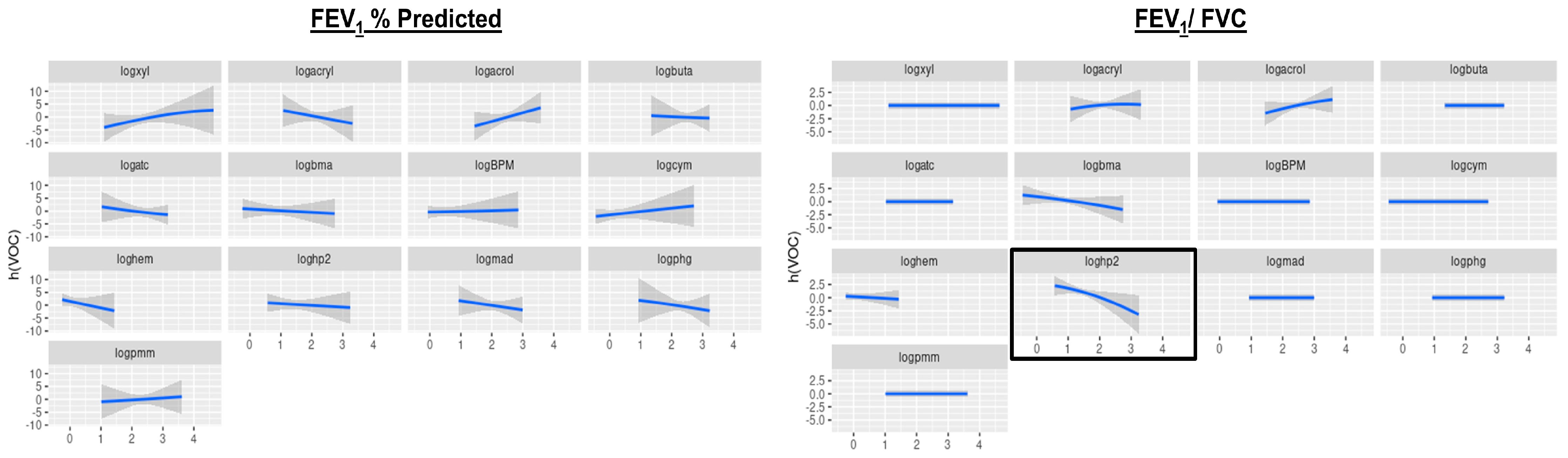
3.3. VOC Urinary Metabolites and Lung Function
4. Discussion
4.1. Acrylamide and Lower FEV1 % Predicted
4.2. Propylene Oxide and Lower FEV1/FVC
4.3. Styrene and Lower FEV1 % Predicted
4.4. 1-Bromopropane, Crotonaldehyde and Effect Modification by Serum Cotinine and Obesity
4.5. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuang, H.; Li, Z.; Lv, X.; Wu, P.; Tan, J.; Wu, Q.; Li, Y.; Jiang, W.; Pang, Q.; Wang, Y.; et al. Exposure to volatile organic compounds may be associated with oxidative DNA damage-mediated childhood asthma. Ecotoxicol. Environ. Saf. 2021, 210, 111864. [Google Scholar] [CrossRef] [PubMed]
- Bari, M.A.; Kindzierski, W.B.; Wheeler, A.J.; Héroux, M.-È.; Wallace, L.A. Source apportionment of indoor and outdoor volatile organic compounds at homes in Edmonton, Canada. Build. Environ. 2015, 90, 114–124. [Google Scholar] [CrossRef]
- Vaidyanathan, A.; Foy, J.W.; Schatz, R. Inhibition of rat respiratory-tract cytochrome P-450 isozymes following inhalation of m-Xylene: Possible role of metabolites. J. Toxicol. Environ. Health A 2003, 66, 1133–1143. [Google Scholar] [CrossRef] [PubMed]
- Nurmatov, U.; Tagieva, N.; Semple, S.; Devereux, G.; Sheikh, A. Volatile organic compounds and risk of asthma and allergy: A systematic review and meta-analysis of observational and interventional studies. Prim. Care Respir. J. 2013, 22, Ps9-15. [Google Scholar] [CrossRef] [PubMed]
- Alford, K.L.; Kumar, N. Pulmonary Health Effects of Indoor Volatile Organic Compounds-A Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 1578. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, I.; Rehwagen, M.; Diez, U.; Seiffart, A.; Rolle-Kampczyk, U.; Richter, M.; Wetzig, H.; Borte, M.; Herbarth, O. Enhanced in vivo IgE production and T cell polarization toward the type 2 phenotype in association with indoor exposure to VOC: Results of the LARS study. Int. J. Hyg. Environ. Health 2001, 204, 211–221. [Google Scholar] [CrossRef]
- Mendy, A.; Merianos, A.L.; Mersha, T.B.; Mahabee-Gittens, E.M. Blood volatile organic compounds associated with non-reversible and reversible airflow obstruction in US adults. Eur. Respir. J. 2022, 60, 2201185. [Google Scholar] [CrossRef]
- Mendy, A.; Burcham, S.; Merianos, A.L.; Mersha, T.B.; Mahabee-Gittens, E.M.; Chen, A.; Yolton, K. Urinary volatile organic compound metabolites and reduced lung function in U.S. adults. Respir. Med. 2022, 205, 107053. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services (DHHS); Centers for Disease Control and Prevention (CDC); National Center for Health Statistics (NCHS). The National Health and Nutrition Examination Survey (NHANES). Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 24 November 2023).
- Alwis, K.U.; Blount, B.C.; Britt, A.S.; Patel, D.; Ashley, D.L. Simultaneous analysis of 28 urinary VOC metabolites using ultra high performance liquid chromatography coupled with electrospray ionization tandem mass spectrometry (UPLC-ESI/MSMS). Anal. Chim. Acta 2012, 750, 152–160. [Google Scholar] [CrossRef]
- Hankinson, J.L.; Bang, K.M. Acceptability and reproducibility criteria of the American Thoracic Society as observed in a sample of the general population. Am. Rev. Respir. Dis. 1991, 143, 516–521. [Google Scholar] [CrossRef]
- Hankinson, J.L.; Odencrantz, J.R.; Fedan, K.B. Spirometric reference values from a sample of the general U.S. population. Am. J. Respir. Crit. Care Med. 1999, 159, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Fuhlbrigge, A.L.; Kitch, B.T.; Paltiel, A.D.; Kuntz, K.M.; Neumann, P.J.; Dockery, D.W.; Weiss, S.T. FEV(1) is associated with risk of asthma attacks in a pediatric population. J. Allergy Clin. Immunol. 2001, 107, 61–67. [Google Scholar] [CrossRef]
- Mendy, A.; Mersha, T.B. Comorbidities in childhood-onset and adult-onset asthma. Ann. Allergy Asthma Immunol. 2022, 129, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Mendy, A.; Salo, P.M.; Wilkerson, J.; Feinstein, L.; Ferguson, K.K.; Fessler, M.B.; Thorne, P.S.; Zeldin, D.C. Association of urinary levels of bisphenols F and S used as bisphenol A substitutes with asthma and hay fever outcomes. Environ. Res. 2020, 183, 108944. [Google Scholar] [CrossRef] [PubMed]
- Merianos, A.L.; Jandarov, R.A.; Mahabee-Gittens, E.M. Tobacco Smoke Exposure, Respiratory Health, and Health-care Utilization Among US Adolescents. Chest 2020, 158, 1104–1114. [Google Scholar] [CrossRef] [PubMed]
- Barr, D.B.; Wilder, L.C.; Caudill, S.P.; Gonzalez, A.J.; Needham, L.L.; Pirkle, J.L. Urinary creatinine concentrations in the U.S. population: Implications for urinary biologic monitoring measurements. Environ. Health Perspect. 2005, 113, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.N.; Hou, C.Y.; Lu, P.C.; Chang-Chien, G.P.; Lin, S.; Tain, Y.L. Association between Acrylamide Metabolites and Cardiovascular Risk in Children With Early Stages of Chronic Kidney Disease. Int. J. Mol. Sci. 2020, 21, 5855. [Google Scholar] [CrossRef]
- Stølevik, S.B.; Nygaard, U.C.; Namork, E.; Haugen, M.; Kvalem, H.E.; Meltzer, H.M.; Alexander, J.; van Delft, J.H.; Loveren, H.; Løvik, M.; et al. Prenatal exposure to polychlorinated biphenyls and dioxins is associated with increased risk of wheeze and infections in infants. Food Chem. Toxicol. 2011, 49, 1843–1848. [Google Scholar] [CrossRef]
- Wang, B.; Wang, X.; Yang, S.; Cheng, M.; Zhou, Y.; Zhou, M.; Ye, Z.; Qiu, W.; He, H.; Cen, X.; et al. Acrylamide exposure and pulmonary function reduction in general population: The mediating effect of systemic inflammation. Sci. Total Environ. 2021, 778, 146304. [Google Scholar] [CrossRef]
- National Research Council (US) Committee on Acute Exposure Guideline Levels. Acute Exposure Guideline Levels for Selected Airborne Chemicals: Volume 9; The National Academies Press: Washington, DC, USA, 2010. [Google Scholar] [CrossRef]
- Liu, W.; Wang, B.; Yang, S.; Xu, T.; Yu, L.; Wang, X.; Cheng, M.; Zhou, M.; Chen, W. Associations of propylene oxide exposure with fasting plasma glucose and diabetes: Roles of oxidative DNA damage and lipid peroxidation. Environ. Pollut. 2022, 292, 118453. [Google Scholar] [CrossRef]
- Committee to Review the Styrene Assessment in the National Toxicology Program 12th Report on Carcinogens; Board on Environmental Studies and Toxicology; Division on Earth and Life Studies; National Research Council. Review of the Styrene Assessment in the National Toxicology Program 12th Report on Carcinogens: Workshop Summary; National Academies Press (US): Washington, DC, USA, 2014. [Google Scholar]
- Su, F.C.; Mukherjee, B.; Batterman, S. Trends of VOC exposures among a nationally representative sample: Analysis of the NHANES 1988 through 2004 data sets. Atmos. Environ. 2011, 45, 4858–4867. [Google Scholar] [CrossRef] [PubMed]
- Zulu, Z.; Naidoo, R.N. Styrene associated respiratory outcomes among reinforced plastic industry workers. Arch. Environ. Occup. Health 2022, 77, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Diez, U.; Kroessner, T.; Rehwagen, M.; Richter, M.; Wetzig, H.; Schulz, R.; Borte, M.; Metzner, G.; Krumbiegel, P.; Herbarth, O. Effects of indoor painting and smoking on airway symptoms in atopy risk children in the first year of life results of the LARS-study. Leipzig Allergy High-Risk Children Study. Int. J. Hyg. Environ. Health 2000, 203, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Zhou, M.; Wang, B.; Mu, G.; Wang, X.; Yuan, J.; Chen, W. Lipid peroxidation mediated the association of urinary 1-bromopropane metabolites with plasma glucose and the risk of diabetes: A cross-sectional study of urban adults in China. J. Hazard. Mater. 2020, 389, 121889. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xiao, J.; Lv, J.; Chen, X.; Li, Y.; Yang, H.; Miao, Q.; Wuhan, B.; Gao, W.; Li, B. Biomarkers of exposure and effect in the serum and urine of rats or workers exposed to 1-bromopropane. Toxicol. Ind. Health 2022, 38, 351–364. [Google Scholar] [CrossRef] [PubMed]
- Miao, R.; Ding, B.; Zhang, Y.; Zhao, R.; Li, Y.; Zhu, B. Large-scale label-free proteomics analysis of occupational poisoned patients of 1-bromopropane, workers exposed to 1-bromopropane and healthy individuals. Hum. Exp. Toxicol. 2018, 37, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Fan, L.; Yang, S.; Zhou, M.; Mu, G.; Liu, W.; Yu, L.; Yang, M.; Cheng, M.; Wang, X.; et al. Cross-sectional and longitudinal relationships between urinary 1-bromopropane metabolite and pulmonary function and underlying role of oxidative damage among urban adults in the Wuhan-Zhuhai cohort in China. Environ. Pollut. 2022, 313, 120147. [Google Scholar] [CrossRef] [PubMed]
- Hajizadeh, Y.; Amin, M.-M.; Parseh, I. Crotonaldehyde removal from polluted air using a biofilter packed with a mixed bed. J. Ind. Eng. Chem. 2018, 62, 418–426. [Google Scholar] [CrossRef]
- Huang, J.F.; Zhu, D.M.; Ma, J.F.; Zhong, M. Acute respiratory distress syndrome due to exposure to high-concentration mixture of ethenone and crotonaldehyde. Toxicol. Ind. Health 2015, 31, 585–587. [Google Scholar] [CrossRef]
- Li, Y.; Chang, J.; Cui, Y.; Zhao, R.; Ding, Y.; Hou, Y.; Zhou, Z.; Ji, H.L.; Nie, H. Novel mechanisms for crotonaldehyde-induced lung edema. Oncotarget 2017, 8, 83509–83522. [Google Scholar] [CrossRef]
- Wang, L.; Yang, Z.; Xu, L.; Pan, X.; Liu, X.; Zhao, J.; Li, X.; Zhu, M.; Xie, J. Acute exposure to crotonaldehyde induces dysfunction of immune system in male Wistar rats. J. Toxicol. Sci. 2018, 43, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.C.; Yang, Z.H.; Pan, X.J.; Liu, X.Y.; Zhu, M.X.; Xie, J.P. Crotonaldehyde induces apoptosis and immunosuppression in alveolar macrophages. Toxicol. Vitr. 2013, 27, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Permaul, P.; Gaffin, J.M.; Petty, C.R.; Baxi, S.N.; Lai, P.S.; Sheehan, W.J.; Camargo, C.A., Jr.; Gold, D.R.; Phipatanakul, W. Obesity may enhance the adverse effects of NO2 exposure in urban schools on asthma symptoms in children. J. Allergy Clin. Immunol. 2020, 146, 813–820.e812. [Google Scholar] [CrossRef] [PubMed]
- Shore, S.A.; Rivera-Sanchez, Y.M.; Schwartzman, I.N.; Johnston, R.A. Responses to ozone are increased in obese mice. J. Appl. Physiol. 2003, 95, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Salo, P.M.; Mendy, A.; Wilkerson, J.; Molsberry, S.A.; Feinstein, L.; London, S.J.; Fessler, M.B.; Thorne, P.S.; Zeldin, D.C. Serum antioxidant vitamins and respiratory morbidity and mortality: A pooled analysis. Respir. Res. 2022, 23, 150. [Google Scholar] [CrossRef] [PubMed]
- Mendy, A.; Percy, Z.; Braun, J.M.; Lanphear, B.; La Guardia, M.J.; Hale, R.C.; Yolton, K.; Chen, A. Prenatal exposure to replacement flame retardants and organophosphate esters and childhood adverse respiratory outcomes. Environ. Res. 2024, 240, 117523. [Google Scholar] [CrossRef] [PubMed]
- Mendy, A.; Percy, Z.; Braun, J.M.; Lanphear, B.; La Guardia, M.J.; Hale, R.C.; Yolton, K.; Chen, A. Exposure to dust organophosphate and replacement brominated flame retardants during infancy and risk of subsequent adverse respiratory outcomes. Environ. Res. 2023, 235, 116560. [Google Scholar] [CrossRef] [PubMed]
- Maesano, C.N.; Caillaud, D.; Youssouf, H.; Banerjee, S.; Prud’Homme, J.; Audi, C.; Horo, K.; Toloba, Y.; Ramousse, O.; Annesi-Maesano, I. Indoor exposure to particulate matter and volatile organic compounds in dwellings and workplaces and respiratory health in French farmers. Multidiscip. Respir. Med. 2019, 14, 33. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.S.; Blount, B.C.; Valentin-Blasini, L.; Applewhite, H.S.; Xia, Y.; Watson, C.H.; Ashley, D.L. Simultaneous determination of six mercapturic acid metabolites of volatile organic compounds in human urine. Chem. Res. Toxicol. 2009, 22, 1018–1025. [Google Scholar] [CrossRef]
- Vardoulakis, S.; Giagloglou, E.; Steinle, S.; Davis, A.; Sleeuwenhoek, A.; Galea, K.S.; Dixon, K.; Crawford, J.O. Indoor Exposure to Selected Air Pollutants in the Home Environment: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 8972. [Google Scholar] [CrossRef]
- Pappas, G.P.; Herbert, R.J.; Henderson, W.; Koenig, J.; Stover, B.; Barnhart, S. The respiratory effects of volatile organic compounds. Int. J. Occup. Environ. Health 2000, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Urinary Metabolites | Abbreviations | Parent Compounds | LOD (ng/mL) | Detection % |
|---|---|---|---|---|
| 2-Methylhippuric acid | 2 MH | Xylene | 5.00 | 95.0 |
| 3-Methylhippuric acid and 4-Methylhippuric acid | 34 M | Xylene | 8.00 | 100.0 |
| N-Acetyl-S-(2-carbamoylethyl)-L-Cysteine | AAM | Acrylamide | 2.20 | 100.0 |
| N-Acetyl-S-(N-methylcarbamoyl)-L-Cysteine | AMC | Acrylamide | 6.26 | 99.8 |
| N-Acetyl-S-(2-Carboxyethyl)-L-Cysteine | CEM | Acrolein | 6.96 | 98.0 |
| N-Acetyl-S-(3-Hydroxypropyl)-L-Cysteine | HPM | Acrolein | 13.00 | 100.0 |
| N-Acetyl-S- (3,4-Dihydroxybutyl)-L-Cysteine | DHB | 1,3-Butadiene | 5.25 | 100.0 |
| N-Acetyl-S-(4-hydroxy-2-butenyl)-L-Cysteine | MB3 | 1,3-Butadiene | 0.60 | 95.4 |
| 2-Aminothiazoline-4-carboxylic acid | ATC | Cyanide | 15.00 | 96.5 |
| N-Acetyl-S-(benzyl)-L-Cysteine | BMA | Toluene | 0.50 | 99.7 |
| N-Acetyl-S-(n-propyl)-L-Cysteine | BPM | 1-Bromopropane | 1.20 | 64.5 |
| N-Acetyl-S-(2-cyanoethyl)-L-Cysteine | CYM | Acrylonitrile | 0.50 | 91.7 |
| N-Acetyl-S-(2-hydroxypropyl)-L-Cysteine | HP2 | Propylene oxide | 5.30 | 93.0 |
| Mandelic acid | MAD | Styrene | 12.00 | 99.0 |
| Phenylglyoxylic acid | PHG | Ethylbenzene, styrene | 12.00 | 99.5 |
| N-Acetyl-S-(3-hydroxypropyl-1-methyl)-L-Cysteine | PMM | Crotonaldehyde | 1.13 | 100.0 |
| Characteristics | % | VOC Urinary Metabolites (ng/g Creatinine) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 MH + 34 M | AAM + AMC | CEM + HPM | DHB + MB3 | ATC | BMA | BPM | CYM | HP2 | MAD | PHG | PMM | ||
| All | 100 | 251.06 (15.62) | 142.44 (4.91) | 302.93 (14.05) | 316.24 (9.88) | 204.29 (10.49) | 7.52 (0.33) | 3.29 (0.37) | 2.10 (0.14) | 29.68 (1.54) | 116.66 (4.13) | 196.57 (5.25) | 208.32 (7.73) |
| Age groups | |||||||||||||
| 6 to 11 years old | 47.0 | 248.22 (16.25) | 149.40 (2.48) | 344.57 (11.04) | 381.32 (14.66) | 344.03 (16.62) | 8.86 (0.41) | 3.56 (0.23) | 2.15 (0.11) | 25.56 (1.97) | 130.51 (5.48) | 230.28 (5.67) | 249.06 (10.76) |
| 12 to 17 years old | 53.0 | 253.60 (19.74) | 136.54 (8.84) | 270.21 (20.68) | 267.84 (8.90) | 128.62 (9.08) | 6.51 (0.51) | 3.04 (0.56) | 2.06 (0.21) | 25.59 (1.69) | 105.60 (6.60) | 170.81 (7.78) | 177.78 (11.05) |
| Sex | |||||||||||||
| Males | 50.1 | 248.98 (23.69) | 138.56 (4.59) | 296.21 (9.32) | 321.67 (9.05) | 176.51 (15.09) | 7.11 (0.49) | 3.04 (0.29) | 1.90 (0.14) | 29.08 (1.86) | 113.81 (3.96) | 188.73 (4.84) | 198.40 (8.43) |
| Females | 49.9 | 253.16 (17.10) | 146.45 (7.47) | 309.84 (26.36) | 310.89 (15.16) | 236.58 (14.76) | 7.96 (0.39) | 3.55 (0.66) | 2.33 (0.27) | 30.30 (2.09) | 119.59 (5.52) | 204.77 (7.52) | 218.79 (13.35) |
| Race/ethnicity | |||||||||||||
| Non-Hispanic White | 54.1 | 276.90 (25.78) | 160.52 (7.26) | 294.33 (23.38) | 337.73 (18.89) | 207.98 (15.22) | 7.06 (0.49) | 3.04 (0.57) | 2.27 (0.24) | 29.56 (2.61) | 118.20 (5.34) | 224.78 (5.67) | 216.79 (11.92) |
| Non-Hispanic Black | 16.0 | 255.52 (12.18) | 115.69 (5.87) | 305.79 (17.95) | 267.06 (9.68) | 165.80 (17.95) | 9.33 (0.88) | 3.57 (0.38) | 2.25 (0.22) | 28.65 (2.14) | 106.92 (6.33) | 160.02 (5.29) | 177.40 (10.71) |
| Mexican American | 16.0 | 225.52 (12.84) | 134.52 (3.11) | 309.46 (19.06) | 308.42 (13.70) | 226.05 (30.95) | 7.64 (0.56) | 3.52 (0.63) | 1.64 (0.05) | 32.79 (1.93) | 124.82 (5.37) | 177.33 (4.97) | 212.26 (16.87) |
| Other | 13.9 | 190.06 (13.73) | 121.40 (3.40) | 327.16 (20.67) | 306.12 (8.94) | 215.64 (26.23) | 7.37 (0.56) | 3.75 (0.45) | 1.92 (0.17) | 28.03 (1.50) | 113.34 (5.69) | 166.37 (5.64) | 210.06 (14.74) |
| PIR | |||||||||||||
| ≤1 | 24.0 | 230.12 (18.45) | 136.42 (6.25) | 305.64 (17.76) | 308.81 (14.43) | 202.84 (19.26) | 8.06 (0.59) | 3.75 (0.41) | 2.34 (0.26) | 29.11 (2.11) | 111.25 (5.47) | 178.49 (8.81) | 205.00 (12.71) |
| >1 | 76.0 | 258.06 (18.09) | 144.40 (5.69) | 302.08 (17.21) | 318.63 (10.69) | 204.75 (12.81) | 7.36 (0.35) | 3.16 (0.39) | 2.03 (0.13) | 29.86 (1.66) | 118.42 (4.60) | 202.65 (4.78) | 209.38 (10.48) |
| Cotinine | |||||||||||||
| <1.0 ng/mL | 88.6 | 241.54 (18.03) | 138.06 (4.86) | 297.44 (13.65) | 312.44 (8.66) | 203.33 (12.47) | 7.65 (0.37) | 3.31 (0.40) | 1.75 (0.09) | 28.73 (1.46) | 115.30 (4.77) | 193.89 (5.24) | 204.00 (7.73) |
| ≥1.0 ng/mL | 11.4 | 338.52 (42.90) | 181.37 (16.79) | 349.00 (31.79) | 347.30 (32.20) | 211.90 (34.49) | 6.63 (0.77) | 3.10 (0.54) | 8.72 (1.62) | 38.21 (5.32) | 127.72 (8.05) | 218.58 (15.14) | 245.03 (24.32) |
| BMI | |||||||||||||
| Normal | 78.9 | 265.95 (17.56) | 147.20 (5.57) | 315.01 (15.11) | 330.45 (10.60) | 231.39 (13.89) | 7.78 (0.28) | 3.48 (0.42) | 2.05 (0.14) | 31.15 (1.85) | 119.05 (4.91) | 208.70 (5.32) | 221.69 (9.96) |
| Overweight | 12.5 | 217.87 (41.61) | 134.60 (12.14) | 264.28 (21.65) | 280.23 (17.66) | 117.48 (20.39) | 5.96 (0.72) | 2.62 (0.51) | 2.31 (0.35) | 22.86 (1.90) | 111.03 (10.76) | 161.31 (12.20) | 168.63 (11.36) |
| Obese | 8.6 | 181.82 (18.03) | 114.36 (10.07) | 258.18 (18.71) | 251.96 (10.85) | 145.92 (15.86) | 7.78 (1.04) | 2.69 (0.62) | 2.35 (0.46) | 27.93 (3.89) | 104.06 (10.21) | 151.35 (14.05) | 160.16 (9.23) |
| Urinary Metabolites | Parent VOC | FEV1 % Predicted | FEV1/FVC |
|---|---|---|---|
| 2 MH + 34 M | Xylene | 0.44 (−2.33, 3.21) | 0.11 (−1.60, 1.83) |
| AAM + AMC | Acrylamide | −7.95 (−13.69, −2.21) ** | −2.25 (−6.08, 1.57) |
| CEM + HPM | Acrolein | 2.06 (−3.73, 7.85) | −1.70 (−4.06, 0.67) |
| DHB + MB3 | 1, 3-Butadiene | −3.94 (−11.37, 3.50) | 0.82 (−4.65, 3.01) |
| ATC | Cyanide | 1.38 (−3.09, 5.86) | −0.74 (−3.06, 1.58) |
| BMA | Toluene | −2.93 (−9.82, 3.96) | −1.22 (−3.53, 1.09) |
| BPM | 1-Bromopropane | 2.20 (−2.58, 6.97) | −0.70 (−1.95, 0.54) |
| CYM | Acrylonitrile | 0.53 (−6.14, 7.21) | −1.21 (−3.13, 0.71) |
| HP2 | Propylene oxide | −1.74 (−6.92, 3.43) | −2.05 (−3.49, −0.61) ** |
| MAD | Styrene | −6.33 (−11.60, −1.07) * | 0.56 (−1.74, 2.87) |
| PHG | Ethylbenzene, styrene | −3.33 (−10.09, 3.43) | −1.83 (−4.35, 0.69) |
| PMM | Crotonaldehyde | 1.36 (−3.32, 6.05) | −1.17 (−4.34, 2.01) |
| Urinary Metabolites | Parent VOC | Obesity | Serum Cotinine | ||||
|---|---|---|---|---|---|---|---|
| No | Yes | Pinteraction | ≤1 ng/mL | >1 ng/mL | Pinteraction | ||
| 2 MH + 34 M | Xylene | 1.25 (−2.42, 4.93) | −2.40 (−8.78, 3.99) | 0.48 | −0.27 (−2.8, 2.04) | 6.99 (−0.43, 14.41) | 0.21 |
| AAM + AMC | Acrylamide | −4.92 (−11.78, 1.94) | −15.40 (−23.56, −7.24) *** | 0.90 | −7.28 (−11.78, −2.79) ** | −7.55 (−33.77, 18.68) | 0.57 |
| CEM + HPM | Acrolein | 4.92 (−2.04, 11.87) | −1.54 (−14.15, 9.07) | 0.78 | 3.10 (−3.10, 9.30) | 5.21 (−8.63, 19.05) | 0.69 |
| DHB + MB3 | 1,3 Butadiene | 0.75 (−8.58, 10.92) | −16.61 (−28.80, −4.41) * | 0.70 | −4.26 (−12.86, 4.33) | 8.37 (−9.97, 26.72) | 0.31 |
| ATC | Cyanide | 1.97 (−2.24, 6.19) | 2.03 (−5.40, 9.45) | 0.99 | 1.20 (−2.87, 5.28) | 4.98 (−12.20, 22.17) | 0.88 |
| BMA | Toluene | −1.75 (−10.19, 6.70) | −4.58 (−13.44, 4.28) | 0.66 | −2.38 (−8.20, 3.45) | −0.81 (−16.92, 15.29) | 0.66 |
| BPM | 1-Bromopropane | 4.54 (−1.14, 10.23) | −1.49 (−5.38, 2.29) | 0.15 | 4.29 (−0.15, 8.73) | −6.26 (−9.69, −2.82) ** | 0.04 |
| CYM | Acrylonitrile | 0.88 (−6.70, 8.45) | 1.54 (−8.88, 11.95) | 0.82 | 0.81 (−5.93, 7.56) | −2.62 (−21.65, 16.40) | 0.56 |
| HP2 | Propylene oxide | 0.25 (−5.35, 5.86) | −7.36 (−17.73, 3.01) | 0.76 | −0.38 (−6.26, 5.49) | −11.70 (−31.40, 8.00) | 0.72 |
| MAD | Styrene | −4.97 (−11.66, 3.72) | −14.93 (−25.66, −4.20) ** | 0.93 | −5.38 (−11.02, 0.25) | −16.17 (−34.09, 1.75) | 0.72 |
| PHG | Ethylbenzene, styrene | −0.61 (−10.22, 9.01) | −10.42 (−20.77, −0.06) * | 0.92 | −2.61 (−9.29, 4.06) | −8.66 (−42.78, 25.45) | 0.80 |
| PMM | Crotonaldehyde | 4.96 (−0.80, 10.72) | −15.42 (−26.76, −4.08) * | <0.001 | 2.07 (−4.20, 8.33) | 3.84 (−12.90, 20.57) | 0.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendy, A.; Burcham, S.; Merianos, A.L.; Mersha, T.B.; Yolton, K.; Chen, A.; Mahabee-Gittens, E.M. Urinary Volatile Organic Compound Metabolites Are Associated with Reduced Lung Function in U.S. Children and Adolescents. Toxics 2024, 12, 289. https://doi.org/10.3390/toxics12040289
Mendy A, Burcham S, Merianos AL, Mersha TB, Yolton K, Chen A, Mahabee-Gittens EM. Urinary Volatile Organic Compound Metabolites Are Associated with Reduced Lung Function in U.S. Children and Adolescents. Toxics. 2024; 12(4):289. https://doi.org/10.3390/toxics12040289
Chicago/Turabian StyleMendy, Angelico, Sara Burcham, Ashley L. Merianos, Tesfaye B. Mersha, Kimberly Yolton, Aimin Chen, and E. Melinda Mahabee-Gittens. 2024. "Urinary Volatile Organic Compound Metabolites Are Associated with Reduced Lung Function in U.S. Children and Adolescents" Toxics 12, no. 4: 289. https://doi.org/10.3390/toxics12040289