

Application of the Single Source—Detector Separation Algorithm in Wearable Neuroimaging Devices: A Step toward Miniaturized Biosensor for Hypoxia Detection


Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedures
2.3. Measurement Device
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
3.1. HbO Change Due to the Breath-Holding Task
3.2. Cerebral StO2-SRS Change Due to the Breath-Holding Task
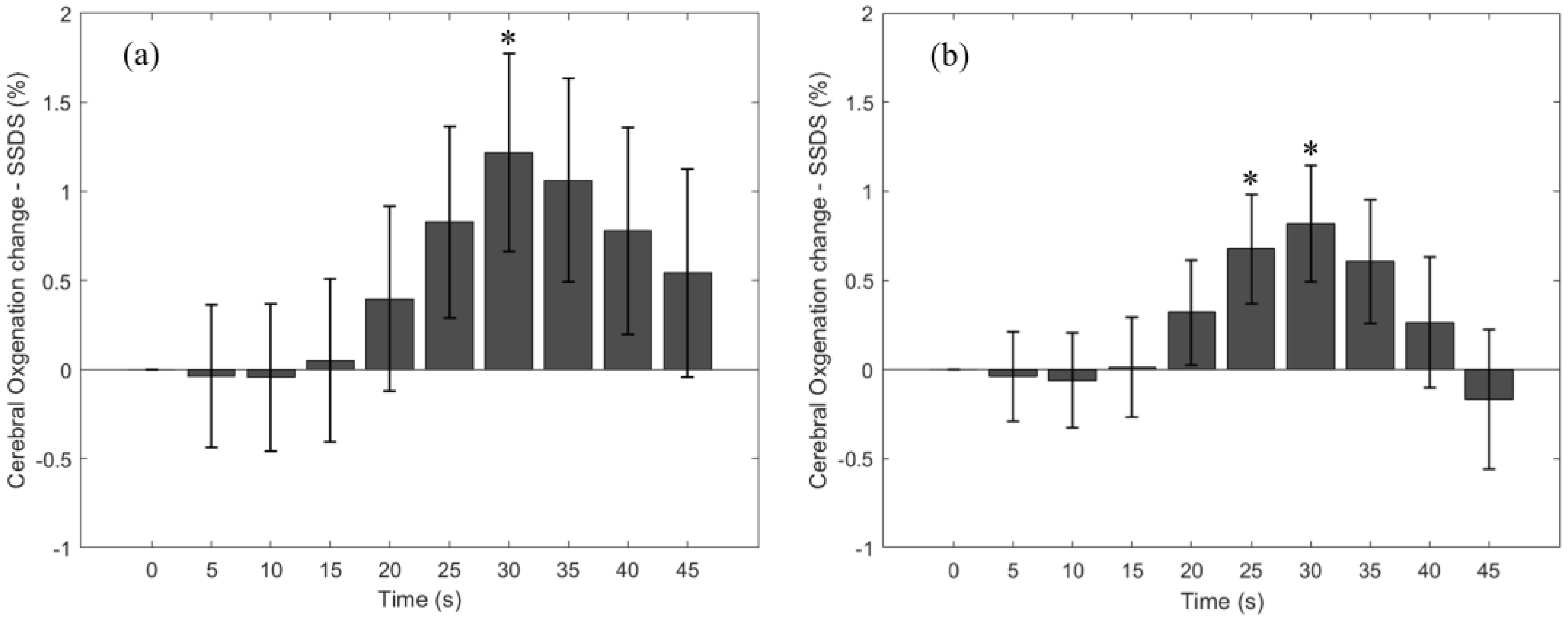
3.3. Cerebral StO2-SSDS Change Due to the Breath-Holding Task
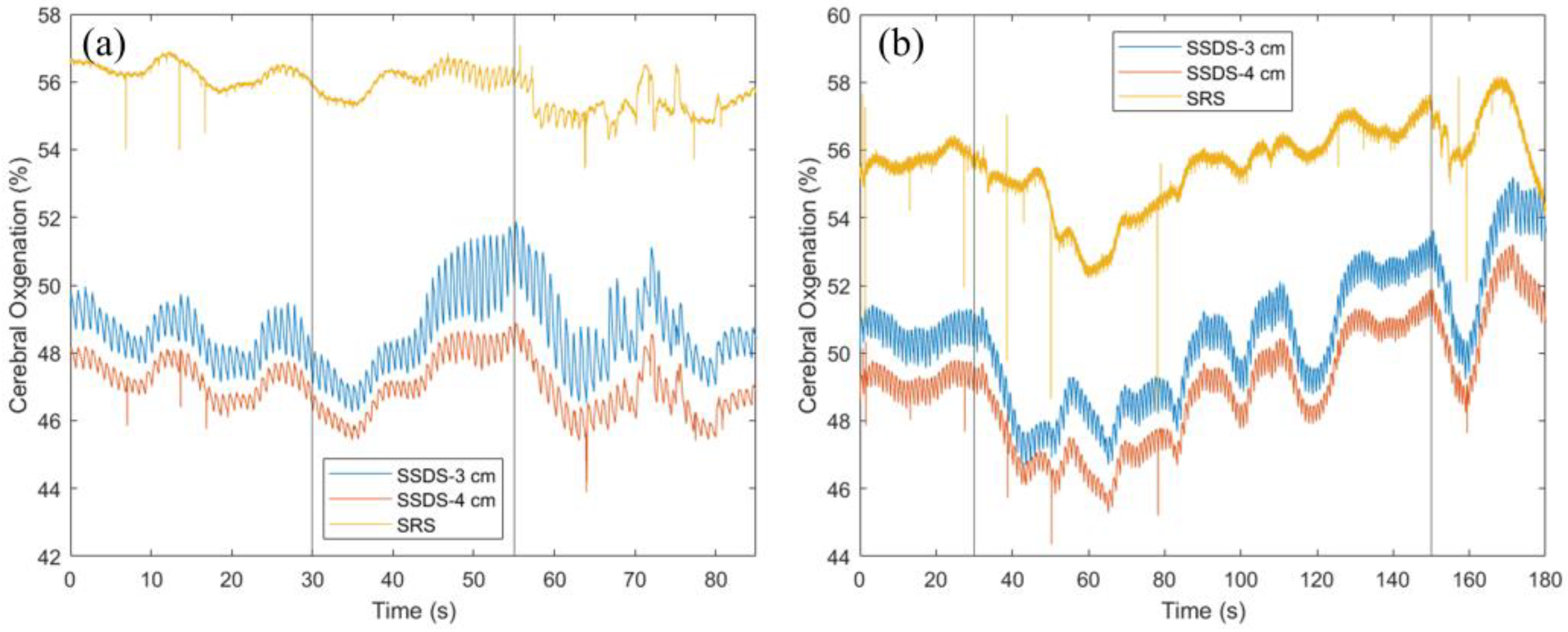
3.4. Cerebral StO2 during a Long versus Short Breath-Holding Task
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhutta, B.S.; Alghoula, F.; Berim, I. Hypoxia. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2024. [Google Scholar]
- Lacerte, M.; Hays Shapshak, A.; Mesfin, F.B. Hypoxic Brain Injury. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2024. [Google Scholar]
- Barud, M.; Dabrowski, W.; Siwicka-Gieroba, D.; Robba, C.; Bielacz, M.; Badenes, R. Usefulness of Cerebral Oximetry in TBI by NIRS. J. Clin. Med. 2021, 10, 2938. [Google Scholar] [CrossRef] [PubMed]
- Zhong, W.; Ji, Z.; Sun, C. A Review of Monitoring Methods for Cerebral Blood Oxygen Saturation. Healthcare 2021, 9, 1104. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.M.K.; Hsiang, J.N.K.; Poon, W.S. Monitoring of autoregulation using laser Doppler flowmetry in patients with head injury. J. Neurosurg. 1997, 86, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Lara, L.; Zorrilla-Vaca, A.; Geocadin, R.G.; Healy, R.J.; Ziai, W.; Mirski, M.A. Cerebral Autoregulation-oriented Therapy at the Bedside: A Comprehensive Review. Anesthesiology 2017, 126, 1187–1199. [Google Scholar] [CrossRef] [PubMed]
- Brady, K.M.; Lee, J.K.; Kibler, K.K.; Smielewski, P.; Czosnyka, M.; Easley, R.B.; Koehler, R.C.; Shaffner, D.H. Continuous time-domain analysis of cerebrovascular autoregulation using near-infrared spectroscopy. Stroke 2007, 38, 2818–2825. [Google Scholar] [CrossRef] [PubMed]
- Kane, A.D.; Kothmann, E.; Giussani, D.A. Detection and response to acute systemic hypoxia. BJA Educ. 2020, 20, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Pesenti, A.; Matthay, M. Understanding blood gas analysis. Intensive Care Med. 2018, 44, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Castro, D.; Patil, S.M.; Zubair, M.; Keenaghan, M. Arterial Blood Gas. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2024. [Google Scholar]
- Lima-Oliveira, G.; Lippi, G.; Salvagno, G.L.; Montagnana, M.; Picheth, G.; Guidi, G.C. Different manufacturers of syringes: A new source of variability in blood gas, acid-base balance and related laboratory test? Clin. Biochem. 2012, 45, 683–687. [Google Scholar] [CrossRef] [PubMed]
- Albert, T.J.; Swenson, E.R. Circumstances When Arterial Blood Gas Analysis Can Lead Us Astray. Respir Care 2016, 61, 119–121. [Google Scholar] [CrossRef]
- Haider, M.Z.; Anwer, F. Secondary Polycythemia. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Billett, H.H. Hemoglobin and Hematocrit. In Clinical Methods: The History, Physical, and Laboratory Examinations; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworth Publishers, a division of Reed Publishing: Boston, MA, USA, 1990. [Google Scholar]
- Mithoowani, S.; Laureano, M.; Crowther, M.A.; Hillis, C.M. Investigation and management of erythrocytosis. Cmaj 2020, 192, E913–E918. [Google Scholar] [CrossRef]
- Sakisaka, S.; Watanabe, M.; Tateishi, H.; Harada, M.; Shakado, S.; Mimura, Y.; Gondo, K.; Yoshitake, M.; Noguchi, K.; Hino, T.; et al. Erythropoietin production in hepatocellular carcinoma cells associated with polycythemia: Immunohistochemical evidence. Hepatology 1993, 18, 1357–1362. [Google Scholar] [CrossRef]
- Bouzat, P.; Sala, N.; Payen, J.F.; Oddo, M. Beyond intracranial pressure: Optimization of cerebral blood flow, oxygen, and substrate delivery after traumatic brain injury. Ann. Intensive Care 2013, 3, 23. [Google Scholar] [CrossRef]
- Mirza, H.; Hashmi, M.F. Lung Ventilation Perfusion Scan (VQ Scan). In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2024. [Google Scholar]
- Sarkar, M.; Niranjan, N.; Banyal, P.K. Mechanisms of hypoxemia. Lung India 2017, 34, 47–60. [Google Scholar] [CrossRef]
- Soye, J.A.; Loughrey, C.B.; Hanley, P.D. Computed tomography pulmonary angiography: A sample of experience at a District General Hospital. Ulster Med. J. 2008, 77, 175–180. [Google Scholar]
- Bickler, P.E.; Feiner, J.R.; Severinghaus, J.W. Effects of skin pigmentation on pulse oximeter accuracy at low saturation. J. Am. Soc. Anesthesiol. 2005, 102, 715–719. [Google Scholar] [CrossRef]
- Feiner, J.R.; Severinghaus, J.W.; Bickler, P.E. Dark skin decreases the accuracy of pulse oximeters at low oxygen saturation: The effects of oximeter probe type and gender. Anesth. Analg. 2007, 105, S18–S23. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.-K.I.; Charpignon, M.; Kim, H.; Josef, C.; De Hond, A.A.; Fojas, J.J.; Tabaie, A.; Liu, X.; Mireles-Cabodevila, E.; Carvalho, L. Analysis of discrepancies between pulse oximetry and arterial oxygen saturation measurements by race and ethnicity and association with organ dysfunction and mortality. JAMA Netw. Open 2021, 4, e2131674. [Google Scholar] [CrossRef] [PubMed]
- Crooks, C.J.; West, J.; Morling, J.R.; Simmonds, M.; Juurlink, I.; Briggs, S.; Cruickshank, S.; Hammond-Pears, S.; Shaw, D.; Card, T.R. Pulse oximeter measurement error of oxygen saturation in patients with SARS-CoV-2 infection stratified by smoking status. Eur. Respir. J. 2022, 60, 2201190. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat-Yazdi, F.; Torres, A., Jr.; Fortuna, R.; Geiss, D.M. Pulse oximeter accuracy and precision affected by sensor location in cyanotic children. Pediatr. Crit. Care Med. 2008, 9, 393–397. [Google Scholar] [CrossRef]
- Foglia, E.E.; Whyte, R.K.; Chaudhary, A.; Mott, A.; Chen, J.; Propert, K.J.; Schmidt, B. The effect of skin pigmentation on the accuracy of pulse oximetry in infants with hypoxemia. J. Pediatr. 2017, 182, 375–377.e372. [Google Scholar] [CrossRef]
- Harris, B.U.; Char, D.S.; Feinstein, J.A.; Verma, A.; Shiboski, S.C.; Ramamoorthy, C. Accuracy of pulse oximeters intended for hypoxemic pediatric patients. Pediatr. Crit. Care Med. 2016, 17, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; Palmer, G.M.; Dewhirst, M.W. Chapter 46—Imaging Hypoxia. In Molecular Imaging, 2nd; Ross, B.D., Gambhir, S.S., Eds.; Academic Press: Cambridge, MA, USA, 2021; pp. 869–895. [Google Scholar] [CrossRef]
- Nguyen, L.S.; Helias, M.; Raia, L.; Nicolas, E.; Jaubert, P.; Benghanem, S.; Ait Hamou, Z.; Dupland, P.; Charpentier, J.; Pène, F. Impact of COVID-19 on the association between pulse oximetry and arterial oxygenation in patients with acute respiratory distress syndrome. Sci. Rep. 2022, 12, 1462. [Google Scholar] [CrossRef] [PubMed]
- Pu, L.J.; Shen, Y.; Lu, L.; Zhang, R.Y.; Zhang, Q.; Shen, W.F. Increased blood glycohemoglobin A1c levels lead to overestimation of arterial oxygen saturation by pulse oximetry in patients with type 2 diabetes. Cardiovasc. Diabetol. 2012, 11, 110. [Google Scholar] [CrossRef]
- Wilson, B.J.; Cowan, H.J.; Lord, J.A.; Zuege, D.J.; Zygun, D.A. The accuracy of pulse oximetry in emergency department patients with severe sepsis and septic shock: A retrospective cohort study. BMC Emerg. Med. 2010, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Ross, P.A.; Newth, C.J.; Khemani, R.G. Accuracy of pulse oximetry in children. Pediatrics 2014, 133, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Ascha, M.; Bhattacharyya, A.; Ramos, J.A.; Tonelli, A.R. Pulse oximetry and arterial oxygen saturation during cardiopulmonary exercise testing. Med. Sci. Sports Exerc. 2018, 50, 1992. [Google Scholar] [CrossRef] [PubMed]
- Petterson, M.T.; Begnoche, V.L.; Graybeal, J.M. The effect of motion on pulse oximetry and its clinical significance. Anesth. Analg. 2007, 105, S78–S84. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.I.; Chung, P.C.; Lee, C.W.; Yu, H.P. Cerebral perfusion monitoring in acute care surgery: Current and perspective use. Expert. Rev. Med. Devices 2016, 13, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Zhang, K.; Zhang, L.; Zong, H.; Meng, L.; Han, R. Cerebral near-infrared spectroscopy (NIRS) for perioperative monitoring of brain oxygenation in children and adults. Cochrane Database Syst. Rev. 2018, 1, CD010947. [Google Scholar] [CrossRef]
- Nguyen, T.; Park, S.; Hill, B.; Gandjbakhche, A.H. Single Source-Detector Separation Approach to Calculate Tissue Oxygen Saturation Using Continuous Wave Near-infrared Spectroscopy. IEEE Open J. Eng. Med. Biol. 2023, 4, 79–84. [Google Scholar] [CrossRef]
- Zijlstra, W.G.; Buursma, A.; der Roest, W.P.M.-V. Absorption spectra of human fetal and adult oxyhemoglobin, de-oxyhemoglobin, carboxyhemoglobin, and methemoglobin. Clin. Chem. 1991, 37, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Bouten, J.; Bourgois, J.G.; Boone, J. Hold your breath: Peripheral and cerebral oxygenation during dry static apnea. Eur. J. Appl. Physiol. 2020, 120, 2213–2222. [Google Scholar] [CrossRef] [PubMed]
- Parkes, M.J. Breath-holding and its breakpoint. Exp. Physiol. 2006, 91, 1–15. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, T.; Park, S.; Park, J.; Sodager, A.; George, T.; Gandjbakhche, A. Application of the Single Source—Detector Separation Algorithm in Wearable Neuroimaging Devices: A Step toward Miniaturized Biosensor for Hypoxia Detection. Bioengineering 2024, 11, 385. https://doi.org/10.3390/bioengineering11040385
Nguyen T, Park S, Park J, Sodager A, George T, Gandjbakhche A. Application of the Single Source—Detector Separation Algorithm in Wearable Neuroimaging Devices: A Step toward Miniaturized Biosensor for Hypoxia Detection. Bioengineering. 2024; 11(4):385. https://doi.org/10.3390/bioengineering11040385
Chicago/Turabian StyleNguyen, Thien, Soongho Park, Jinho Park, Asma Sodager, Tony George, and Amir Gandjbakhche. 2024. "Application of the Single Source—Detector Separation Algorithm in Wearable Neuroimaging Devices: A Step toward Miniaturized Biosensor for Hypoxia Detection" Bioengineering 11, no. 4: 385. https://doi.org/10.3390/bioengineering11040385