1. Introduction
Metabolic complications are complex medical disorders which exert multidirectional effects on human life and health. Metabolic syndrome (MS) is a complex medical condition defined as a constellation of co-occurring metabolic derangements: obesity, hypertension, diabetes mellitus (DM), and dyslipidaemia. MS has been linked with numerous comorbidities and adverse survival outcomes in the general population [
1]. It is a well-established risk factor for increased cardiovascular morbidity [
1] and accelerated deterioration of kidney function [
2]. MS was also associated with an increased risk of liver steatosis and fibrosis [
3] as well as the development of several types of cancer [
4]. According to the global projections, MS affects between 12.5% and 31.4% of the adult individuals worldwide, depending on the MS definition applied [
5] and its prevalence continues to rise. Numbers posited for the European region are slightly higher ranging from 22.3% to 31.5% [
5]. Accordingly, non-alcoholic fatty liver disease, which is considered a liver manifestation of MS, has been reported as an increasing cause of end-stage liver disease which is qualified for liver transplantation, and it is expected to become the leading cause by 2030 [
6].
Obesity and DM epidemics, along with an increasing incidence of MS in the general population, translate into an evolving metabolic profile of liver transplant (Ltx) candidates, increasing the demand for Ltx procedures and compromising long-term post-transplantation (post-Ltx) morbidity and mortality statistics [
7,
8]. A large cross-sectional study reported that approximately 5.4% of Ltx candidates suffered from MS [
9]. However, this area remains largely unexplored with values likely to be underestimated. The pre-transplantation (pre-Ltx) period abounds in multiple confounding factors which preclude the successful identification of metabolic disturbances at the time. On the other hand, MS appears to be a common phenomenon after Ltx, affecting 44–58% of recipients [
9,
10,
11]. MS has been recognised as a risk factor for increased morbidity and mortality in the post-Ltx setting, with pre-Ltx metabolic derangements tending to persist, worsen, or rapidly recur after a transplantation procedure [
8]. The underlying cause of these findings appears to be multifactorial. However, the resolution of cirrhosis-related hypermetabolic and malabsorptive state, along with chronic disease resolution and the use of immunosuppressants, appear to have key importance [
8].
Obesity is not a homogeneous condition, as historically thought. Adipose tissue is a complex and metabolically active organ. Significant inter-individual variability has been noted in patients with obesity in terms of body fat distribution and metabolic profile [
12]. A growing body of evidence has confirmed the prominent role of regional fat distribution in predicting clinical outcomes, as compared to overall fat content [
13,
14]. Abdominal adipose tissue can be divided into two compartments, (subcutaneous and visceral), both of which exert significant structural and functional differences [
15,
16]. Available evidence indicates that there is an important link between the excessive accumulation of visceral fat and the many facets of MS, including glucose intolerance, hypertension, and dyslipidaemia [
17,
18]. Both subcutaneous and visceral fat depots have been shown to play a role in the development of insulin resistance [
18,
19]. Visceral adipose tissue (VAT) was found to be more metabolically active, promoting pro-inflammatory state and lipolysis. It has also been linked with increased cardiovascular risk, while no such correlation has been found for its subcutaneous counterpart [
14,
20]. Factors determining abdominal fat distribution and its association with the overall metabolic profile of Ltx recipients have not been thoroughly investigated.
Numerous biochemical biomarkers have been explored over the years in the context of metabolic complications. Evidence suggests that ferritin, uric acid, and vitamin D are associated with MS, many individual metabolic disturbances, and the amount of VAT [
21,
22,
23,
24,
25]. Nevertheless, their role and potential diagnostic or therapeutic utilization remain inconclusively substantiated.
Although liver is the second most commonly transplanted organ worldwide, it also continues to be the second most awaited transplant procedure [
26,
27]. With the demand for Ltx increasing worldwide, the shortage of available liver organs from deceased donors is also well known. Over the years, it has become apparent that not only the quantity but also the quality of organs should be taken into consideration. In 2006, a drop in Ltx volume was reported, owing to the worsened quality of donated organs [
28]. Since then, many attempts have been made to structure the liver utilisation process to balance the donor pool and the potential consequences for the recipients [
28]. Despite a 2.41% increase in the number of deceased liver donors in 2022, the organ utilisation rate continues to decline [
26]. As evidenced by numerous studies, organ donor characteristics may both predispose and protect the recipients from metabolic complications [
29,
30]. Older age [
31,
32], male sex [
33], and diseased-liver transplants [
32,
33] were linked to an increased risk of post-Ltx DM. Given this evidence, it deems crucial to augment the current knowledge of donor-related metabolic risk factors.
Taking the above-mentioned facts into consideration, this study aimed to investigate the metabolic profile of Ltx recipients and its association with body fat distribution. We also examined the impact of pre- and post-Ltx factors on the risk of nutritional and metabolic abnormalities following the Ltx procedure.
2. Materials and Methods
2.1. Study Population
This monocentric study was conducted at the Nephrology and Transplant Medicine Outpatient Clinic, Medical University of Warsaw between April 2021 and April 2022. Adult participants who provided written informed consent were enrolled. Adults who underwent a de novo elective cadaveric-donor Ltx procedure at the Department of General and Transplant Surgery, Medical University of Warsaw, within at least 5 months prior to study enrolment and presented a stable medical condition were eligible for the study. Patients < 18 years of age at the time of transplantation and those who underwent re-transplantation or combined kidney-liver transplantation were excluded from the study. To mitigate the effect of confounding factors, patients who were pregnant or lactating; presented clinical or laboratory signs of an active infection or acute inflammatory disease; received vitamin D/iron, any multi-ingredient supplementation, or red blood cell transfusion within the last 6 months; or had ferritin levels > 300 ng/mL and haemoglobin levels < 12 g/dL were not included in the study. Considering the potential influence of thyroid hormone imbalance on metabolic parameters and adipose tissue accumulation and distribution, the participants' fasting thyroid stimulating hormone (TSH) levels during the last 6 months were reviewed. Individuals were considered eligible only when these were within reference ranges, irrespective of the diagnosis of a thyroid function disorder.
All patients received the same intra- and postoperative care. The first-line immunosuppressive regimen consisted of glucocorticosteroids (GSKs), calcineurin inhibitors (CNIs)—tacrolimus (TAC), and antimetabolic drugs. Glucocorticoid administration was generally discontinued within 3 to 6 months following the transplant. Mycophenolate mofetil (MMF) was continued in cases where a second immunosuppressive agent was required to facilitate dose reduction in CNIs. Patients with underlying immune-mediated liver diseases were maintained on low-dose steroids (2.5–5 mg of prednisone, where four patients were receiving prednisone at the dose of 10 mg).
2.2. Data Collection
The data regarding patients’ pre-Ltx comorbidities; vital signs (blood pressure); anthropometric measurements (weight, height, and body mass index (BMI)); laboratory results (fasting glucose, high-density lipoprotein (HDL), and triglycerides); liver disease aetiology; date of transplant; length of follow-up; presence of hepatocellular carcinoma (HCC); immunosuppressive regimen (at discharge and maintenance); and acute organ rejection episodes requiring intravenous steroid administration were retrospectively retrieved from the medical records. The body weight of the transplant candidates was adjusted for fluid overload. Donor characteristics (sex, age, weight, BMI, and waist circumference (WC)) were obtained from the National Transplant Registry.
The data on participants’ post-Ltx metabolic status were extracted from medical records and supplemented with medical evaluation during follow-up visits. During the medical consultation, information about the current clinical status along with vital signs (blood pressure and body temperature), anthropometric measurements (BMI, WC, hip–waist (HW), and waist-to-hip ratio (WHR)), and information on alcohol consumption and tobacco use were also obtained. Peripheral blood samples were collected to evaluate the following biochemical and morphological parameters: haemoglobin, CRP, vitamin D, ferritin, glucose, insulin, haemoglobin A1C, HDL and triglycerides, creatinine, AST, ALT, and uric acid. Study participants fasted for 6–8 h before blood sample collection. Serum TAC concentrations during the last 6 months were reviewed and used to calculate the mean 6-month TAC concentration level. Analysis of the overall body composition (fat mass (FM), fat-free mass (FFM), muscle mass (MM), and abdominal tissue composition broken down via visceral and subcutaneous compartments) was performed using the multi-frequency bioelectrical impedance (BIA) method measured using the Maltron BioScan-920-II device in fasting participants. The biological material would be stored and disposed of in accordance with the procedures enforced at the Medical University of Warsaw.
2.3. Metabolic Syndrome Diagnosis
MS was diagnosed based on the adapted recommendations of the International Diabetes Federation, the American Heart Association, and the National Heart, Lung, and Blood Institute [
34]. Considering that the WC values may be significantly affected by fluid overload in the Ltx candidates with cirrhosis, a modification was applied to the central obesity criterion. BMI ≥ 30 kg/m
2 was used as a surrogate indicator in Ltx candidates and as a joint indicator for assessing central obesity in the post-Ltx setting. Simultaneous coexistence of at least three out of five of the following factors was tantamount to MS diagnosis:
central obesity (WC ≥ 94 cm in males; ≥80 cm in females, BMI ≥ 30 kg/m2 in both sexes)
triglycerides ≥ 150 mg/dL (1.7 mmol/L) or drug treatment for elevated triglycerides
HDL cholesterol ≤ 40 mg/dL (1.0 mmol/L) in males; ≤50 mg/dL (1.3 mmol/L) in females, or specific treatment for this lipid abnormality
systolic blood pressure ≥ 130 mmHg; diastolic blood pressure ≥ 85 mmHg, or hypotensive pharmacological treatment in a patient with a medical history of hypertension
fasting glucose ≥ 100 mg/dL (5.5 mmol/L), or pharmacological management of previously diagnosed DM
Cases of de novo MS were defined as metabolic derangements first diagnosed in the post-Ltx setting.
Insulin resistance was calculated according to the homeostasis model assessment for insulin resistance (HOMA-IR) using the following equation: ((fasting serum insulin in µU/mL) × (fasting plasma glucose in mg/dL)/405).
The study was conducted in accordance with provisions of the Declaration of Helsinki and received a favourable local Ethics Committee opinion.
2.4. Statistical Analysis
Descriptive statistics were computed for the study group. Continuous variables are presented as mean and standard deviation (SD) or a median with first and third quartile values (IQR) as indicated, while frequency tables were produced for categorical variables.
Initially, the Shapiro–Wilk test was used to check if the continuous variables followed a normal distribution. Based on the test results and small sample sizes of the considered subgroups, non-parametric tests were used for subgroup comparisons. The Mann–Whitney U test was used to compare continuous variables between the two groups. Only the mean 6-month TAC concentration variable followed a normal distribution based on the Shapiro–Wilk test and was tested using parametric tests (t-student test, ANOVA).
The relationship between two nominal variables was examined using Fisher’s exact test or the Chi-square test.
Correlations between variables were examined using the Spearman’s rank correlation or the point-biserial correlation coefficient. The following classification of correlation strength was used:
0.0 ≤ |r| ≤ 0.2—no correlation,
0.2 ≤ |r| ≤ 0.4—low correlation,
0.4 ≤ |r| ≤ 0.7—moderate correlation,
0.7 ≤ |r| ≤ 0.9—high correlation,
0.9 ≤ |r| ≤ 1.0—very high correlation.
The analysis was carried out in two stages to examine the relationship between the continuous variables of liver donor profiles. First, the correlation matrix of point-two-tailed coefficients was calculated, and then the non-parametric Mann–Whitney U tests were performed for double verification.
The risk of new-onset MS was assessed on the basis of 38 potential explanatory variables. Simple logistic regression was performed for each variable, and the odds ratio (OR) was determined along with a 95% confidence interval (CI) in each case. Each of these variables was then considered in the multivariate model. Based on the Akaike information criterion (AIC), a stepwise forward selection was used to select the best fitting model. With the given predictor being a dichotomous variable, we assumed a value of one for the event and zero otherwise. To make the results more meaningful, the analysis was performed only for the complete sets of observations.
To verify the relationship between VAT and subcutaneous adipose tissue (SAT), two separate linear regression models were created. The best fitted multivariate linear model was chosen based on stepwise forward selection using AIC. However, before starting this procedure, collinear variables were eliminated from the set of potential explanatory variables. Owing to the lack of coincidence of models created on the basis of forward stepwise selection, variables for which the sign of the corresponding coefficient did not agree with the direction of the previously observed relationship were removed. For each model, R2 and the adjusted R2 were calculated.
The level of significance was set to p = 0.05; however, statistically significant results for p = 0.01 and p = 0.001 levels were also indicated.
All calculations were performed using the R statistical package version 4.0.2.
4. Discussion
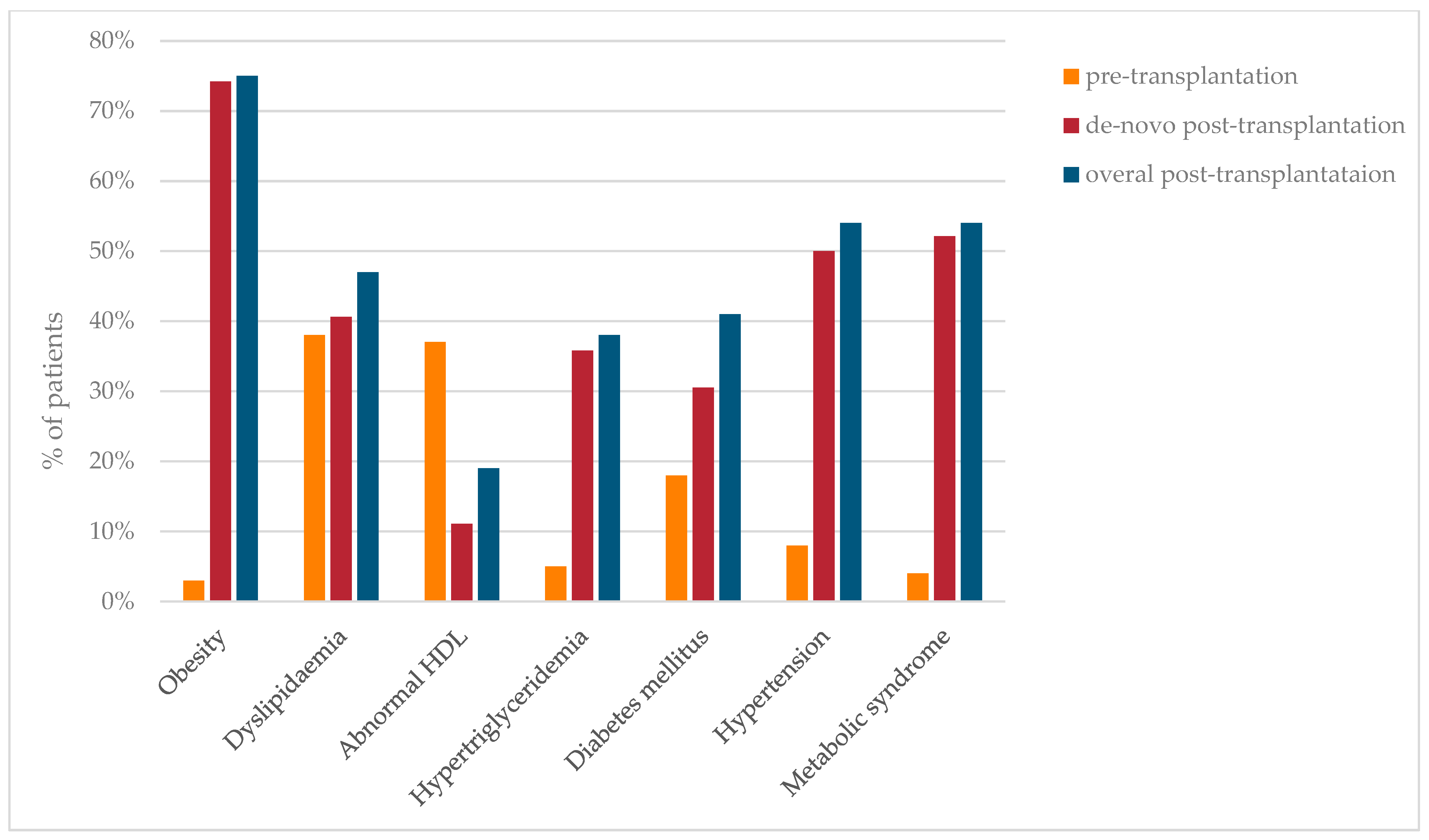
Our study showed that metabolic complications were rare in Ltx candidates, with a significant rising trend observed following the transplant procedure. In contrast to previous reports, despite negligible pre-Ltx occurrence, post-Ltx obesity notably outperformed the remaining new-onset metabolic complications with an unprecedented prevalence of 74.2% [
9,
10,
35]. This may be partially explained by the timing of the study, which was conducted during the COVID-19 pandemic. During this difficult time, imposed restrictions and social isolation resulted in reduced physical activity, adverse nutritional habits, and comfort eating. Bolesławska et al. demonstrated that SARS-CoV-2-related confinement led to weight gain in 40% of Polish men and 50% of Polish women [
36]. We should draw conclusions from this dire lesson and follow the example of countries that handled obesity management during pandemics exceptionally well to be prepared to provide uninterrupted medical assistance regardless of external circumstances.
The estimated prevalence of MS in Ltx individuals ranges from 44 to 58%, depending on the study [
9,
10,
35]. The most recent meta-analysis by Thoefner et al. found de novo MS only in 35% of Ltx recipients [
37]. However, our study showed a significantly higher rate of MS, which affected approximately 50% of the study population. These discrepancies could be explained by several factors. First, in our study, we utilised an adapted IDF Task Force on the Epidemiology and Prevention criteria to identify individuals with MS before and after transplantation, while most studies included in the meta-analysis applied the original or adapted NCEP ATP III definition with higher cut-off values for WC and fasting glucose, or used BMI as an abdominal adiposity indicator. Notably, the variability of definitions applied and the varying inclusion/exclusion criteria also limited data extraction and pooling for meta-analysis. Although, our outcomes are not consistent with those of the most recent meta-analysis, they are supported by the findings of many individual analyses conducted in this specific population. Nevertheless, the ongoing pandemic might have influenced our results.
MS, as a state of subclinical chronic low-grade inflammation frequently associated with the excessive accumulation of adipose tissue, results in an increased concentration of proinflammatory cytokines as well as serum levels of acute-phase reactants. SFC has reportedly been positively correlated with many metabolic disorders and abdominal adiposity [
21,
22,
38]. Our study outcomes support this notion. Furthermore, we demonstrated that SFC was independently and positively associated with MS, which is consistent with the results of the two independent meta-analyses [
22,
38]. However, in contrast to a study by Iwasaki et al. [
21], our analysis did not show an independent association between this acute-phase protein and abdominal adiposity. This may be explained by the fact that different populations were investigated (general Japanese population vs. post-Ltx European population), and the divergent techniques of abdominal adiposity quantifying (BIA vs. computed tomography) were used. Ethnicity-related differences in visceral fat accumulation have been well-established and prompted an issuance of a new consensus to define MS by incorporating considerable ethnic and national differences impinging on actual cardio-metabolic risk [
34].
Abril-Ulloa et al. suggested that ferritin might be utilised as a putative screening biomarker for the identification of patients who are at a high risk of MS development [
22]. Regretfully, there are many confounding factors that have to be considered or ruled out before referring to SFC in the metabolic context, thus limiting its application in broad clinical practice. We applied an adequate mitigation strategy to limit the effect of confounding factors during the analysis. However, this also impacted our sample size and study group characteristics.
As expected, poor glycaemic and blood pressure control and adverse lipid profiles were observed in the MS group. Of these, haemoglobin A1C, de novo hypertriglyceridemia, and SFC were independently associated with new-onset MS. Considering that the occurrence of post-Ltx diabetes and hypertriglyceridemia are key diagnostic criteria for MS and that ferritin was identified as an independent predictor of MS in the meta-analyses, such results might be anticipated [
22,
38]. Additionally, Suárez-Ortegón et al. reported that of the MS constituents, high triglycerides and a high fasting glucose were strongly interconnected with SFC [
38]. All of these factors may account for our study results.
Over the years, many controversies have surrounded the relationship between MS and SUA [
24,
39]. A growing body of longitudinal studies have consentaneously identified SUA as a significant contributing factor for MS [
40,
41]. A similar association was determined by Rospleszcz et al. for visceral fat accumulation but not for subcutaneous depots [
25]. Our results have replicated previously reported findings. However, the strength of the evidence was weak.
Vitamin D deficiency has been linked to the development of obesity and DM. Convincing evidence exists connecting vitamin D deficiency to the development of MS [
23]. Even so, insufficient data were gathered to recommend vitamin D supplementation as a precautionary measure. We found that vitamin D concentrations were inversely associated with MS and VAT accumulation in the post-Ltx setting. None of these associations were confirmed in the multivariate models.
Numerous studies have demonstrated that abdominal fat distribution is affected by various pre- and post-Ltx factors. Of these, HCV infection, male gender, and older age are the best documented factors [
15,
37,
42]. Our results support these findings. We also determined an association amongst pre-Ltx DM, both pre- and post-Ltx MS, and abdominal fat distribution.
The link between VAT and the risk for developing MS is well-established [
43,
44]. However, the same association for SAT has not been consistently documented in the literature. Some reports have revealed a positive correlation between SAT and MS but failed to adjust their results for age or sex, whereas others did not consider the effect of VAT [
43,
45]. Lastly, some studies have proven that no such association exists or have proposed an actual protective effect of SAT in the context of MS development [
13,
17,
18,
46]. Our results showed a positive correlation only between new-onset MS and VAT. Accordingly, most of post-Ltx metabolic abnormalities were linked to visceral abdominal adiposity. However, this association was not confirmed in the multivariate analysis.
Based on our study, the WC and BMI post-Ltx were found to be independent risk factors for visceral adiposity, while only WC proved to be of importance for its subcutaneous counterpart. The same was confirmed by previous publications, which reported the superiority of WC in estimating abdominal fat accumulation, and, by extension, in the assessment of cardiovascular risk [
47]. It is important to note that the independent risk factors identified for new-onset MS and the pattern of abdominal fat distribution did not correspond. One may find this surprising considering that a documented association exists between MS and VAT accumulation, in particular. On the other hand, recognising that the high intra-individual variability of body fat distribution and metabolic profiles were documented among patients with and without concurrent obesity, it is not surprising that individuals with normal abdominal fat accumulation are diagnosed with MS and, inversely, that cases of excessive visceral fat accumulation are noted in patients who did not meet the MS criteria [
12,
13]. Within this context, the phenomenon of metabolic obesity in people with normal body weight (MONW) has attracted significant attention over the past decade. It appears to be as important as it is challenging to define. To date, no harmonised or universally accepted definition of the disorder has been proposed. Nevertheless, the concept of MONW is based on impaired insulin sensitivity and body fat distribution, with visceral obesity playing a major role [
12]. Several studies demonstrated that obesity indices used to define metabolic syndrome may remain within the pre-defined reference ranges despite excessive VAT accumulation [
48,
49].
This underpins the complex and multi-causal nature of both metabolic complications and abdominal fat distribution resulting from the multifaceted interplay between genetic, environmental, behavioural, social, and iatrogenic factors, which are highly unlikely to be reflected by one standardised constellation of biochemical, anthropometric, or clinical factors. All of these depict the imperative role of holistic and patient-tailored approaches in preventing metabolic complications from going unnoticed.
Life-long exposure to immunosuppressants is unavoidable after Ltx. At the same time, immunosuppressive treatment has been identified as one of the incriminating factors promoting metabolic disorders, particularly the use of GSKs and CNIs. Therefore, these immunosuppressants have been broadly discussed in the literature and reflected in the guidelines for maintenance therapy. In accordance with these guidelines, it is recommended that GSKs be discontinued up to 3 months following Ltx along with a simultaneous reduction in CNI dosage, which is expected to be challenging, if even feasible, in patients with an autoimmune aetiology of liver disease [
50,
51]. Therefore, we investigated immunosuppressive-related variables from different perspectives. In keeping with what has been previously reported, neither any particular maintenance immunosuppressive scheme nor immunosuppressive agent were found to be associated with the increased metabolic risk [
9,
10,
35]. However, we were not able to capture all the immunosuppression-related factors which occurred in the studied population (changes in dosage regimen and the modifications of the immunosuppressive regimen). The literature evidence has failed to link immunosuppression-related variables with visceral adiposity, which is especially interesting in the context of GSKs administration [
52,
53]. GSK receptors have a higher density within VAT and are known to mediate both adipose tissue metabolism and body fat distribution [
15]. Nevertheless, our results are congruent with those previously reported. This may stem from the fact that the latest guidelines on maintenance immunosuppressive therapy were followed in all patients. All individuals, except for those with autoimmune liver diseases, were discontinued from the administration of steroids early. A sizeable proportion of the patients received metabolically neutral MMF to facilitate CNI dose reduction. Those who continued on long-term steroids were generally maintained on low steroid doses not exceeding 5 mg of prednisone. Interestingly, based on our results, one may conclude that GSKs may play a protective role with regards to metabolic complications, which appears to be biologically implausible. Similar results were also obtained by Lattanzi et al. [
54]. Therefore, we further investigated this surprising path and found that patients who were chronically continued on steroids were subjected to more heightened medical scrutiny than those on recommended CNI-tapered regimens. This, in our opinion, led to the successful identification of metabolic complications at the early stages, which was followed by appropriate non-pharmacological and pharmacological guidance, resulting in a lower rate of metabolic abnormalities. These unexpected findings exemplify the need for a personalised approach during post-Ltx medical care regardless of the initially calculated risk of metabolic complications. Concentrating our efforts predominantly on high-risk patients may result in an underdiagnosis of those in other risk groups. This, however, does not change the fact that the implementation of appropriate immunosuppressive guidelines turned out to be insufficient to successfully protect our patients from developing MS.
In view of the aging global population and metabolic epidemics being on the rise, significant impacts may be expected on the profile of potential and actual liver donors, and by extension, on post-organ transplantation outcomes [
28]. The metabolic status of deceased-liver donors appears to be an interesting and largely unexplored area, with possible impacts on liver recipients.
Taking the above-mentioned facts into consideration, we analysed basic liver donor parameters in the context of metabolic complications in organ recipients. Our two-step analysis confirmed the pronounced role of excessive adiposity of the donor on the recipients' metabolic risk. Many previous publications have suggested that DM is an important donor factor. We were unable to analyse this additional parameter owing to incomplete information for some individuals.
More in-depth and comprehensive analyses of liver donor profiles. combined with a more inclusive study designs, are needed to draw firm conclusions on the actual impact of donor metabolic status on the risk of de novo metabolic complications. Nevertheless, our results displayed that global metabolic pandemic considerably impacted the metabolic profiles of liver donors, and, thus, resulted in post-Ltx implications.
This study had a few limitations., with one being the partially retrospective and monocentric nature of the study, which, by extension, resulted in limited subgroup representation. The comprehensive analysis of metabolic profiles of Ltx recipients and the implementation of mitigation strategies to reduce the effect of confounding factors during the analysis can be considered as strengths of the study. However, this may also be perceived as a significant drawback, as rigorous inclusion criteria resulted in the disqualification of many liver transplant recipients from participating in the study. Furthermore, despite the global rising trend for Ltx due to NASH, our study population was represented by only one such case and five cases of cryptogenic cirrhosis. Having said that, our results should be analysed with caution, as the sample may not adequately reflect a real-life representation of the Ltx population managed at our medical facility.

 ,
, 

{kind=link}