
From Eye Care to Hair Growth: Bimatoprost
by
 , , , , and
, , , , and
Marco Zeppieri
1,* ,
,
Caterina Gagliano
2,3,
Leopoldo Spadea
4,
Carlo Salati
1,
Ekele Caleb Chukwuyem
5, 
Ehimare Samuel Enaholo
5,
Fabiana D’Esposito
6 and
Mutali Musa
7 1
Department of Ophthalmology, University Hospital of Udine, p.le S. Maria della Misericordia 15, 33100 Udine, Italy
2
Department of Medicine and Surgery, University of Enna “Kore”, Piazza dell’Università, 94100 Enna, Italy
3
Eye Clinic, Catania University, San Marco Hospital, Viale Carlo Azeglio Ciampi, 95121 Catania, Italy
4
Eye Clinic, Policlinico Umberto I, “ Sapienza” University of Rome, 00142 Rome, Italy
5
Centre for Sight Africa, Nkpor, Onitsha 434112, Nigeria
6
Imperial College Ophthalmic Research Group (ICORG) Unit, Imperial College, London NW1 5QH, UK
7
Department of Optometry, University of Benin, Benin City 300238, Nigeria
*
Author to whom correspondence should be addressed.
Pharmaceuticals 2024, 17(5), 561; https://doi.org/10.3390/ph17050561
Submission received: 25 March 2024
/
Revised: 17 April 2024
/
Accepted: 25 April 2024
/
Published: 27 April 2024
(This article belongs to the Special Issue Ophthalmic Pharmacology)
Abstract
:Background: Bimatoprost has emerged as a significant medication in the field of medicine over the past several decades, with diverse applications in ophthalmology, dermatology, and beyond. Originally developed as an ocular hypotensive agent, it has proven highly effective in treating glaucoma and ocular hypertension. Its ability to reduce intraocular pressure has established it as a first-line treatment option, improving management and preventing vision loss. In dermatology, bimatoprost has shown promising results in the promotion of hair growth, particularly in the treatment of alopecia and hypotrichosis. Its mechanism of action, stimulating the hair cycle and prolonging the growth phase, has led to the development of bimatoprost-containing solutions for enhancing eyelash growth. Aim: The aim of our review is to provide a brief description, overview, and studies in the current literature regarding the versatile clinical use of bimatoprost in recent years. This can help clinicians determine the most suitable individualized therapy to meet the needs of each patient. Methods: Our methods involve a comprehensive review of the latest advancements reported in the literature in bimatoprost formulations, which range from traditional eye drops to sustained-release implants. These innovations offer extended drug delivery, enhance patient compliance, and minimize side effects. Results: The vast literature published on PubMed has confirmed the clinical usefulness of bimatoprost in lowering intraocular pressure and in managing patients with glaucoma. Numerous studies have shown promising results in dermatology and esthetics in promoting hair growth, particularly in treating alopecia and hypotrichosis. Its mechanism of action involves stimulating the hair cycle and prolonging the growth phase, leading to the development of solutions that enhance eyelash growth. The global use of bimatoprost has expanded significantly, with applications growing beyond its initial indications. Ongoing research is exploring its potential in glaucoma surgery, neuroprotection, and cosmetic procedures. Conclusions: Bimatoprost has shown immense potential for addressing a wide range of therapeutic needs through various formulations and advancements. Promising future perspectives include the exploration of novel delivery systems such as contact lenses and microneedles to further enhance drug efficacy and patient comfort. Ongoing research and future perspectives continue to shape its role in medicine, promising further advancements and improved patient outcomes.
1. Introduction
Bimatoprost has emerged as an essential medication in the field of medicine over the past two decades, with diverse applications in ophthalmology, dermatology, and beyond [1]. It was first approved for use in 2001 [2] and is still extensively researched to understand its long-term prospects and interactions [3]. Bimatoprost amide is classified as a prostaglandin analogue (PGF2α) [4,5] and can be derived from dichloro-containing bicyclic ketone-6a [6]. Initially developed as an ocular hypotensive agent, bimatoprost has proven to be highly effective in the treatment of glaucoma [7,8] and for its neuroprotective properties [9,10,11]. It is a small synthetic molecule and its patent is currently owned by Allergan which is headquartered in Ireland [10]. Its molecular structure is shown in Figure 1 below [10].
Bimatoprost is rapidly hydrolyzed to bimatoprost free acid in the eye which in turn activates its intraocular pressure (IOP) reduction mechanism [12]. With respect to its mechanism of action, bimatoprost closely mimics the prostamides in up-stimulating the rate of aqueous humor flow. Its ocular hypotensive action is due primarily to a 26% reduction in the tonographic resistance to outflow via the trabecular meshwork [13]. Its pharmacokinetics reveal rapid absorption following ocular administration, with peak plasma concentrations typically attained within one to two hours post-application. This rapid absorption is facilitated by the highly vascularized conjunctiva, allowing bimatoprost to enter the systemic circulation swiftly [14]. Once absorbed, bimatoprost undergoes metabolism primarily in the liver via oxidation, hydrolysis, and conjugation processes, ultimately forming inactive metabolites that are excreted primarily through renal elimination. The elimination half-life ranges from approximately 45 min to 4 h, indicative of its relatively short duration of action. Pharmacodynamically, bimatoprost acts by increasing the outflow of aqueous humor from the eye, thereby reducing intraocular pressure (IOP). It achieves this by binding to and activating prostaglandin receptors (specifically, the prostamide receptor) in the ciliary muscle of the eye [13]. Activation of these receptors leads to relaxation of the ciliary muscle and enlargement of the trabecular meshwork spaces, facilitating increased drainage of aqueous humor from the eye. Additionally, bimatoprost may also enhance uveoscleral outflow, further contributing to its IOP-lowering effects [14]. By modulating these physiological pathways, bimatoprost effectively mitigates the risk of optic nerve damage and visual field loss associated with elevated IOP, making it a cornerstone in the management of glaucoma and ocular hypertension.
Thus, bimatoprost enhances the pressure-sensitive outflow pathway [13,14]. Bimatoprost use is reportedly a viable temporary protective measure in cases of non-inflammatory angle closure glaucoma [15]. Glaucoma, often referred to as the “silent thief of sight”, is a group of eye conditions that damage the optic nerve, leading to gradual vision loss and potentially blindness if left untreated. This disease typically develops when fluid pressure within the eye, known as intraocular pressure, increases, causing damage to the optic nerve fibers responsible for transmitting visual information to the brain. The onset of glaucoma is insidious, often progressing without noticeable symptoms until significant vision loss occurs [16]. While there is no cure for glaucoma, early detection through regular eye exams and timely treatment, such as medication, laser therapy, or surgery, can help slow its progression and preserve remaining vision. Glaucoma underscores the importance of proactive eye care and underscores the necessity of regular eye check-ups to maintain healthy vision.
Shen et al. measured bimatoprost presence in quantitative amounts up to one hour post-application, and bimatoprost acid up to seven hours after application in the aqueous and ciliary processes [17]. Heo et al., among other authors, suggested that bimatoprost achieves its ocular hypotensive effects by increasing the activity of matrix metalloproteinases, specifically MMPs-1,3,9 and TIMP-2,4 [18,19]. Stamer et al. suggested that the cellular basis for the antiglaucoma effects of bimatoprost can also be viewed from its ability to decrease cellular contractility of the trabecular meshwork, canal of Schlemm, and ciliary smooth muscle [20]. Its ability to reduce intraocular pressure has made it a first-line treatment option for these conditions [21], offering patients improved management and prevention of vision loss. Bimatoprost is also a viable option for individuals with reduced response to latanoprost due to the activity of Allele C in the rs3753380 receptor [22]. Multiple clinical trials have been concluded and have unanimously found bimatoprost to be a viable drug for intraocular pressure reduction [23].
We aim to provide a brief description and overview of studies in the current literature regarding the versatile clinical use of bimatoprost in the past two decades. Descriptive headings have been used to summarize the specific issues regarding bimatoprost in this paper. The purpose of this review is not to present a prospective clinical study, however, but to provide a quick overlook of the versatile uses of this substance in different fields of medicine, and the evolution of how things have changed regarding its posology and usage since 2000.
2. Methods
The authors developed inclusion criteria comprising published articles from 2010 and newer ones available in PubMed and Cochrane libraries. Full-length publications, review papers, and case reports were considered for this research using the search string “(“bimatoprost”[MeSH Terms] OR “bimatoprost”[All Fields]) AND (2010:2023[pdat])”. Papers that were not in the English language, outside the scope of this review, and duplicates were excluded. A total of 583 records were returned for PubMed while only one record was returned for Cochrane Library. A minimum of two of the authors reviewed each study for relevance and assigned ratings to them. Figure 2 shows the flow chart according to the PRISMA [24] and the details regarding the selection.
3. Results
In our review, a total of 583 papers were identified, which became 579 after duplicate removal. Articles were excluded for the following reasons: (1) not relevant to the research topic (73 articles), (2) a lack of clear method/results details (11 articles), (3) language (3 articles), (4) retraction (2 articles), and (5) unavailable full text/abstract (65 articles). This study consisted of 27 case reports, 3 editorials, 1 drug guideline, 321 original research papers, and 81 reviews. All studies included in the analysis had at least one or more outcome measures available for one or more of the patient groups analyzed. A total of 425 studies were considered. A bibliography of the articles reviewed is shown in Figure 3.
The vast literature has shown the clinically effective IOP-lowering effects of bimatoprost. This drug has been extensively used in clinics and in research studies, thus it is vastly reported on in the literature on glaucoma and ocular hypertension. A large-scale UK-based study revealed that the bimatoprost–timolol fixed combination was only second to latanoprost–timolol prescriptions among 2015 patients [25]. Rahman et al. also reported that bimatoprost was the second most common drug that a sample of 1006 patients persisted with [26]. Heo et al. carried out a retrospective study into patients’ persistence with prostaglandin analogues and reported that bimatoprost was the least option that persisted compared to latanoprost and travoprost [27]. Bimatoprost is a drug of choice for non-respondent patients previously on other antiglaucoma medications [28,29]. Another study suggested that this may not be the case, as 83 non-responders in a clinical trial did not show an added statistical reduction in IOP with bimatoprost [30]. Crichton et al. reported an average, additional reduction of 10–15% after switching from other antiglaucoma medications to bimatoprost [31]. Furthermore, a large-scale pharmaceutical-based review suggested that there was better compliance to bimatoprost, 0.01% as compared to its 0.03% variant [32]. The bimatoprost–dorzolamide regimen has also been determined to improve retrobulbar blood flow, thereby inhibiting glaucomatous ocular morbidity [33]. Bimatoprost also retains its efficacy even after up to three years of use with minimal tolerance reports [34].
The local drops of bimatoprost are available in different concentrations and formulations. Bimatoprost is usually dispensed as an aqueous mixture with or without preservatives [35] and is also available as an ocular insert device. Its effectiveness may however be affected by its instability in aqueous solutions and isomerism [36]. The average washout period for prostaglandin analogues has been researched to be 4.56 weeks (±1.25) after the last application [37]. Lim et al. suggested that washout may take up to 6 weeks [38]. Bimatoprost has been found to be safe in breastfeeding mothers as it hardly gets into the bloodstream [39].
4. Selected Comparison Studies on Bimatoprost
4.1. Bimatoprost vs. Bimatoprost
Bimatoprost has been shown to be potent as a monotherapy and as a combination therapy [40,41]. As far as population-based efficacy reports, Bimatoprost has shown good efficacy among both primary open-angle glaucoma (POAG) and normal-tension glaucoma (NTG) patients in several Chinese and Japanese studies, respectively [42,43].
Konstas et al. examined IOP in 60 eyes being managed by bimatoprost and reported a drop from 29 mmHg to 20.8 mm Hg (p < 0.001) and combining bimatoprost with timolol resulted in a statistically significant average IOP reduction of 10.2 mmHg in the morning (p = 0.006) [44]. The presence or absence of preservatives such as benzalkonium chloride does not affect its efficacy [45,46]. Bimatoprost concentration affects its bioavailability in the aqueous humor with the 0.03% preparation, showing a statistically higher concentration in the aqueous after 30 min (11.5 ± 2.1 ng/mL versus 37.8 ± 28.8 ng/mL) [47,48]. This has been reported to enhance long-term outcomes [49]. Preservative-free bimatoprost 0.01% is reported to be less irritating [50], and non-cytotoxic as compared to the 0.03% variant that was reported to be cytotoxic and shown to reduce corneal endothelial cell viability after long-term use [51]. Bimatoprost 0.01% was found to reduce adverse ocular surface effects [52] while also maintaining efficacious IOP control than 0.03% and 0.0125% formulations of bimatoprost, respectively [53,54], with a drop of −4.9 ± 3.5 (p < 0.001). Patients who switched from 0.01% to 0.03% bimatoprost experienced a significant further reduction in IOP but with increased numbers of adverse effects, especially hyperemia [55]. Bimatoprost 0.01% monotherapy increased ocular perfusion pressure (OPP) in twenty hours of observing POAG patients [56] and extended treatment persistence in the chronic management of glaucoma [57].
4.2. Bimatoprost vs. Beta Blockers and α2 Agonists
Prostaglandins became a first-line therapy for glaucoma management [58], partly due to their relatively easier once-daily dosing [59]. Natt et al. also reported similar superior IOP-lowering effects of bimatoprost when compared to brimonidine as shown in bimatoprost IOP reduction values of 8.9 ± 1.598 mmHg compared to 6.55 ± 1.26 mmHg among subjects that received Brimonidine [60]. Artunay et al. reported that brimonidine 0.2% was inferior to bimatoprost 0.003% for the prevention of post-YAG laser capsulotomy spikes in intraocular pressure [61].
4.3. Bimatoprost vs. Prostaglandin Analogues
Bimatoprost yields more IOP reduction than latanoprost in the preservative-free formulation [62]. Both aforementioned prostaglandin analogues (PGAs) have been reported to show greater first-line ocular hypotensive effects than timolol fixed combination agent adepts of PGAs; latanoprost had been suggested to pose good tolerability amongst study participants [63]. Novel preservative-free tafluprost 0.0015% has shown efficient IOP control with, of course, more improved tolerability than bimatoprost monotherapy [64,65,66].
As with other prostaglandin analogues, bimatoprost shows a stable reduction in IOP when compared with baseline values at 6-month and 5-year follow-ups [67]. The lower tonicity of 0.01% bimatoprost formulations has led to better treatment continuation outcomes among patients, superior to those of other PGA-based/first-line anti-OHT agents [68,69]. Tang et al. reported that bimatoprost 0.03% appeared more effective when used in long-term care as compared to other prostaglandin analogues [70], while Turan-Vural et al. suggested that Ketrolac enhanced the anti-glaucoma abilities of bimatoprost [71]. Nepafenac has also been shown to potentiate the effects of three major prostaglandin analogues: latanoprost, travoprost, and bimatoprost [72]. A clinical trial suggested that bimatoprost possessed the best efficacy of prostaglandin analogues during the initial phases of use [73] and among patients switched to bimatoprost from other antiglaucoma therapies [74]. The presence of nucleotide polymorphisms of the prostaglandin F-receptor (rs11578155 and rs6672484) has been described to be negatively correlated with prostaglandin analogues, including bimatoprost [75].
Bimatoprost is reported to be the most expensive antiglaucoma eye drop preparation available to most patients [76,77]. It has the second widest coverage under Medicare both in branded and generic forms [78]. Studies comparing the tolerability and suitability of bimatoprost and travoprost in patients revealed a statistically significant reduction in diurnal IOP as compared to standard latanoprost, i.e., 2.1 mmHg additional reduction in IOP with bimatoprost compared to 1.4 mmHg with travoprost; another study reported a 9.9 mmHg from baseline values for latanoprost as against 15.88 nnHg for bimatoprost [79,80,81]. The drug showed better quality of life indices as compared to latanoprost, travoprost, and tafluprost [82]. Among prostaglandin analogues (PGAs), bimatoprost has been reported to exert better diurnal IOP control in glaucoma monotherapy than latanoprost single therapy and is poised to exert greater intraocular pressure control, with Mishra et al. reporting the highest reduction with a 35.9 ± 3.5% reduction in IOP compared to 29.9 ± 3.5%, 30.8 ± 2.6% and 26.6 ± 2.3 for latanoprost, travoprost, and timolol respectively [83,84]. Kook et al. also reported as part of the APPEAL study that switching participants from other therapies to bimatoprost 0.01% single therapy resulted in a statistical decrease in IOP [85]. More so, BTFC was preferred to travoprost by patients [86,87].
Bimatoprost could be linked with a lower comparative number of non-respondents in NTG [88]. Findings by Sato et al.; Sawada et al.; and Germano et al. suggested that transitioning from latanoprost to bimatoprost yielded better therapeutic effects; furthermore, latanoprost was noted to be the least tolerated among all prostaglandin analogues [89,90,91,92]. Bimatoprost, travoprost, and latanoprost have been reported to portend equivalent ocular surface tolerability with medium-term use [93]; latanoprost and travoprost yielded more visible ocular hyperemia than bimatoprost in human and murine studies, respectively [94,95]. The type of prostaglandin analogue preservative had no significant effect on ocular side effects [96]. Toxic effects of topical prostaglandin analogues bimatoprost, travoprost, and latanoprost on rabbit eyes were more dependent on the concentration of BAK preservative than agent selection [97]. Bimatoprost had a stronger association with the deepening of the upper eyelid sulcus (DUES) among Japanese patients, following a switch from latanoprost [98,99]. Other authors have, however, suggested that switching from fixed prostaglandin therapy to combination therapies which include beta blockers can help reduce hyperemia [100]. Bimatoprost has been subjectively linked to increased hyperemia and more side effects in human patient studies [101,102,103]. A keratograph may suggest better objective automated grading of ocular hyperemia [104].
Topical PGAs tend to have high-cost implications when initiated with adjunctive therapy [105,106]. For many years, latanoprost has been the most common prostaglandin analogue used as a topical therapy for glaucoma, accounting for about 65% of prostaglandin prescriptions [107]. Latanoprost had been associated with more persistent periods of use, probably due to lower cost implications than bimatoprost and travoprost [108,109]. Bimatoprost has, however, been linked with higher first-year expenditure than both travoprost and latanoprost [110]. Slower rates of glaucoma progression for patients on bimatoprost have, however, been theorized to increase long-term cost savings in their favor [111]. Islam and Spyry also opined that bimatoprost was the most cost-effective prostaglandin analogue in the Canadian community [112]. Eyes with thinner cornea centers may be more responsive to the antihypertensive effects of topical bimatoprost [113]. This may have to do with its comparatively reduced corneal tissue permeability [114]. Bimatoprost 0.01% demonstrates good treatment outcomes in clinical studies [41,115].
Tafluprost remained inferior to bimatoprost as an IOP-regulating agent [116,117] except when optimized with benzalkonium chloride [118]. Bimatoprost formulation has been reported to maintain optimal stability under various thermal conditions, unlike travoprost and latanoprost [119]. Bimatoprost 0.01% also compares to travoprost 0.04% in controlling late-day IOP levels [120]; Bimatoprost 0.03% has on the other hand, been suggested to control IOP better than travoprost at 12 weeks following onset of use [121].
Adverse periocular manifestations are common with topical use of PGAs [122]. Kucukevcilioglu et al. compared periorbitopathy with latanoprost, bimatoprost, and travoprost, concluding that these were most severe and frequent in the bimatoprost-treated group [123,124]. Long-term use of bimatoprost may affect periorbital cosmesis largely by significant inhibition of adipogenesis by bimatoprost acid in vitro [125,126]; this was suggested in a case report as well [127]. Similarly, switching away from bimatoprost therapy may lead to an improvement in DUES [128].
4.4. Bimatoprost vs. Multi-Class IOP Lowering Medications
While timolol has often been touted as the most cost-effective anti-glaucoma drug, bimatoprost was reported as the most effective alternate option in situations where beta blockers are contraindicated [129]. Other studies recommend prostaglandin analogues as first-line treatment for glaucoma [130,131].
A review of practice patterns by eyecare practitioners in the United States outlined bimatoprost among commonly used first-line agents [132]. A survey of 150 Mexican Ophthalmologists revealed bimatoprost was the most preferred prostaglandin analogue prescribed, with 62% of respondents preferring the drug [133]. Another study reported that bimatoprost comparatively increased OPP when compared to Timolol [134]. Prostaglandin therapies are associated with lesser diurnal fluctuations in intraocular pressure control than other mono-therapeutics [135,136]. It is therefore not unexpected that a bimatoprost-timolol fixed combination is one of the most tolerated and satisfactory pressure-lowering regimens in POAG [137]. The same holds true in patients with chronic angle closure glaucoma [138]. In fact, the IOP-lowering effects of bimatoprost have been clocked to persist longest amongst the PGAs at 48 h after a single dose [139]. Fixed combination bimatoprost/timolol was reported to reduce IOP more optimally than dorzolamide/brimonidine/timolol combination drops [140]. Brief et al. also reported that BTFC is associated with good tolerability and adherence among the majority of participants in glaucoma/ocular hypertension treatment studies [141]. It has been suggested that morning use of bimatoprost with dorzolamide hydrochloride as an adjunctive agent also reduced diurnal IOP variation [142]. Reports from the APPEAL Taiwan Study reaffirmed the clinical usability of bimatoprost 0.01% [143], however, prostaglandin analogs generally have been associated with thickening of the macula, but Selen et al. have suggested that there are no significant inter-drug differences [144].
4.5. Bimatoprost vs. Fixed Combination Therapies
Common anti-glaucoma combination drugs usually consist of a prostaglandin analogue and a beta-blocker [145,146]. They are especially important in patients who do not have a satisfactory IOP reduction in IOP with monotherapy [147,148]. Prostaglandin-timolol fixed combinations (PTFCs) have generally demonstrated improved treatment efficacy over non-fixed formulations [149,150,151,152,153], reduced individual PGA-induced hyperemia [154,155], cost implications [156], potentially regularized dosing regimen [157,158], and improved long-term adherence to treatment [159,160]. In Belfort et al.’s study BTFC patients reported lower levels of hyperemia with prostaglandin fixed combination drops [161]. Bourne et al. have differed on this, stating that switching patients from a BTFC to a tafluprost-timolol combination mitigated hyperemia signs [162].
Prostaglandin/timolol unfixed combinations were tagged as more effective than PTFCs in a pilot study [163,164]. Notably, the therapeutic effects of PTFCs varied with the choice of PGA component in formulations [165]. Bimatoprost single therapy, however, was equally comparable to latanoprost–timolol fixed combination in reducing IOP strength according to Maruyama et al.’s study [166]. The diurnal IOP-control effects of bimatoprost monotherapy were reportedly equal to the latanoprost/timolol fixed combination [167,168,169,170]. Bimatoprost–timolol fixed combination drops were reported by Lee et al. to further reduce IOP in patients who had been switched from separate latanoprost and timolol drops [171].
Ganfort, a preparation of bimatoprost/timolol was reported to better decrease IOP in a cohort of patients with neovascular glaucoma [172,173], as well as treatment-naive and NTG patients [174,175]. Bimatoprost/timolol fixed combination reportedly exerted greater IOP reduction than travoprost/timolol and latanoprost/timolol in open-angle glaucoma patients [176,177]. Hartleben et al., however, reported slightly different findings, stating that triple agent combinations containing bimatoprost performed better than bimatoprost–timolol fixed combinations [178]. A triple-fixed combination of anti-glaucoma also performed better than a double-fixed combination in the study by Menon and Goodkin, albeit in poorly controlled patients [179]. Interestingly, Sussana et al. reported that a once-daily administration of the triple-fixed therapy bimatoprost–timolol-brimonidine performed better than a bi-daily administration of the same drug [180].
Travoprost/timolol and latanoprost/timolol were previously assumed to achieve better IOP control effects than several other common agents in fixed combinations with Timolol [181]. Nevertheless, bimatoprost/timolol formulations have demonstrated good efficacy, even without benzalkonium chloride (BAK) preservatives [182,183]. A study reports improved treatment outcomes upon transition from bimatoprost 0.03%/timolol 0.5% to travoprost 0.004%/timolol 0.5% in resistant OHT cases [184]. Bimatoprost monotherapy demonstrated equivalence to latanoprost/brinzolamide as valuable transition options following prior latanoprost monotherapy [185]. A significant reduction in hyperemia was found after switching from monotherapy with prostaglandins or prostamide to a fixed combination of prostamide and a β-blocker [186]. Conversely, a proportion of patients who transitioned from a bimatoprost/timolol to a travoprost/timolol fixed combination reportedly gained improvements in IOP and tolerability with their new therapy [187]. Once-daily BTFC has been found to be more effective in mean IOP control than the dorzolamide/timolol combination used twice daily [188] or latanoprost/timolol [189], with no differences found in the safety profiles of both agents [190].
Pfennigsdorf et al. reported that BTFC lowered mean IOP from baseline by 5.4 mmHg over the 12-week duration of the studies (p < 0.0001) [191]. BTFC, latanoprost/timolol, and travoprost/timolol fixed combinations reportedly yield equivalent degrees of tolerability for patients requiring adjunctive topical agents [192]. When side effects were measured objectively using factors such as hyperemia, no significant difference was found between PGAs [193]. A prospective study of the effects of bimatoprost as compared to dorzolamide–timolol showed comparable IOP-lowering effects for both drugs [194]. Inference from the United Kingdom general practitioner research database suggested that lower-cost travoprost-centric therapies were linked with longer treatment resistance than other PGA-centric therapies [195]. Xu et al. also suggested in a study out of China that Bimatoprost was the most cost-effective among other anti-glaucoma drugs [196]. Moreover, across the continent in Russia, Kosakyan et al. also recommended bimatoprost for its comparatively minimal adverse effects and hypotensive properties [197].
The evaluation of hyperemia caused by ocular medications can be very subjective; to this end, Sumi et al. developed an automated hyperemia analysis computer-based software [198]. Clinical decisions on which therapy to recommend are achieved by collating results across multiple studies. Kymes et al. were able to demonstrate an artificial intelligence tool that correctly analyzed multiple publications, analyzing their results and IOP endpoints, before they eventually concluded that bimatoprost comparatively achieved a better IOP drop when tested with other prostaglandin analogues [199], notwhitstanding possible side effects of prostaglandins generally [200]. A comparative analysis of the IOP-lowering effect of bimatoprost is depicted in Table 1 below.
5. Complications of Bimatoprost
As with any chemotherapeutic agent, there are bound to be complications with the use of bimatoprost. Systemically, prostaglandins have been reported to cause contraction of the uterine muscles and eventual spontaneous abortion. However, there are not enough data to confirm if this same complication is present in topical prostaglandin analogs [207]. Tanito et al. recommended a grading system for prostaglandin-associated orbitopathy [PAP] [208]. They found that bimatoprost was associated with higher PAP grades as compared to tafluprost and omidenepag. This was echoed by Hikage et al., who reported that omidenepag may not cause sunken eyeballs [209]. PAP has been reported to be positively associated with bimatoprost and age, while a high BMI gave a negative correlation [210]. Sarnoff and Gotkin suggested adjusting the mnemonic from PAP to PAPS, to accommodate the words ‘periorbital syndrome’ to capture the beneficial properties of bimatoprost [211]. Ida et al. have recently demonstrated in vitro that bimatoprost acid inhibited adipogenesis, and its action is also potentiated by the addition of an EP2 agonist such as omidenepag [212]. Ocular hyperemia after topical instillation of bimatoprost is also a recurring theme in studies sampled [213,214]. Some of these complications are listed in Table 2.
Liang et al. suggested that human corneal endothelium (HCE) cytotoxicity as reported amongst prostaglandin analogues was at least partly caused by preservatives [261]. Their research demonstrated that preservative-free tafluprost showed the least HCE cytotoxicity as compared to other prostaglandin analogues containing different concentrations of benzalkonium chloride. Benzalkonium chloride itself has been implicated to exacerbate dry eye symptoms in study mice [262,263] and also delay wound healing [264]. Nakakura et al. [265], however suggested that sunken eyelids secondary to bimatoprost use can be reversed by switching patients to latanoprost. Altieri and Ferrari also disputed that bimatoprost use resulted in eyelid position changes [266]. Radcliffe has also suggested that the addition of timolol to bimatoprost to be dispensed as a single fixed combination drop greatly reduces the risk of hyperemia as a side effect [267]. Other studies suggested that Rho-kinase inhibitors may inhibit the effect of bimatoprost on orbital tissue [268,269]. Specifically, preservative-free bimatoprost–timolol may be the most tolerated anti-glaucoma fixed combination drug [270,271,272].
Ocular adverse events included pruritus, periocular hyperpigmentation, hypertrichosis, and irritation [273,274]; these were deemed easily reversible upon discontinuation of bimatoprost ophthalmic solution among those who switched medications [275]. On average, PTFCs induce more conjunctival infiltration [276]. Ocular adnexal, specifically conjunctival and palpebral infiltration of macrophages were associated with long-term use of preservative-free bimatoprost. These effects were hypothesized to be owing to residual excipients within the solution [277]. When added to bimatoprost, benzalkonium chloride, polyoxyethylene hardening castor oil 40 (HCO-40), and polysorbate 80 (P-80) have demonstrated toxicity to corneal and conjunctival cells in vitro [278]. Alternate analysis of conjunctiva-associated lymphoid tissue changes in rabbit models found common inflammatory infiltration changes for all PGAs preserved with BAK [279,280]. In contrast, latanoprost and tafluprost were linked with a reduction in the cytotoxicity of BAK on human conjunctival cell cultures [281]. BAK concentrations in bimatoprost also had cytotoxic effects on in vivo models of mature human adipocytes and preadipocytes [282]. Bimatoprost-induced DUES was ameliorated following its discontinuation [283].
Upregulation of matrix metalloproteinase expression via human non-pigmented ciliary epithelial cells bodes potential aggravation of prior low-grade inflammatory processes within the eye following consistent and prolonged topical instillation of bimatoprost, as with several other PGAs [284]. There were sparse case reports of bimatoprost use associated with choroidal detachment in the eyes of elderly persons; previous intraocular surgery seemed to be a prevailing risk factor in affected eyes [285].
Much like most antiglaucoma drop formulations containing a non-selective beta-blocker, BTFC was linked with an alteration of normal pulmonary physiology in a case report [286]. Situations in which topical drops alone cannot reduce IOP to acceptable levels may necessitate glaucoma surgery. Bimatoprost use pre-surgery may result in recurrent IOP elevation up to two years after trabeculotomy [287].
Psychometric analyses via quality-of-life questionnaires were used to assess patients’ outlook toward the side effects of bimatoprost among other anti-glaucoma drugs. Results of this study concluded that respondents were more concerned by the side effects of bimatoprost over other anti-glaucoma drugs tested [288]. Some complications of bimatoprost are shown in Figure 4 below.
6. Bimatoprost in Other Fields
Bimatoprost indications have grown beyond ophthalmology and dermatology, with ongoing research exploring its applications in glaucoma surgery, neuroprotection, and even cosmetic procedures [289,290,291]. Care, however, must be taken to be wary of the effects of eye cosmetics on the eye in general [292]. Gregorio et al. reported on an interesting case of unpredicted resolution of floppy iris syndrome and ectropion in a geriatric patient after unrelated management for glaucoma using bimatoprost [293].
In dermatology, bimatoprost has shown promising results in the promotion of hair growth, particularly in the treatment of alopecia/hypotrichosis [294,295,296,297,298], leukoderma [299,300], and for general eyelash enhancement [301,302]. Its use in this respect was fully approved by the Food and Drug Authority in 2008 [303]. Alopecia areata is a condition presenting with variable hair loss [304,305] and can be a side effect of anti-cancer chemotherapy [306,307]. A common treatment for alopecia areata is the steroid Clobetasol propionate cream [308] and Pentoxifylline [309]. Bimatoprost induced eyelash growth over one year in a portion of patients who had alopecia areata [310,311,312]. It was also shown to be effective in steroid-resistant cases [313]. Anbar et al. reported that three different prostaglandin analogues (including bimatoprost) were capable of producing skin pigmentation in murine models [314]. Its mechanism of action, stimulating the hair cycle and prolonging the growth phase, has led to the development of bimatoprost-containing solutions for enhancing eyelash growth [315]. This has been well-received by patients seeking longer, fuller eyelashes [316]. Improvement of lash properties may be dependent on the location of the hairs on the face [317]. There are, however, ethical issues to be resolved in this percept. Banazek [318] warned that the complications of bimatoprost use far outweigh the potential cosmetic applications.
Subedi et al. formulated an enhanced bimatoprost preparation named BIM-TF#5 and it was found to be five times more potent than bimatoprost-in-ethanol in dermal drug penetration [289]. Lasers are indicated for enhancing the uptake of drugs into skin tissue [319]. Waibel et al. compared three treatment modalities for managing skin hypopigmentation, namely fractional lasers, laser-mediated bimatoprost delivery, and a dermal melanocyte harvesting technique [320]. There was a statistically significant improvement in hypopigmentation in laser-mediated bimatoprost delivery as compared to the other two techniques. Thus, bimatoprost has been reported for its ability to induce melanogenesis and hyperpigmentation. Nguyen et al. [321] suggested that micro-needling hypopigmented burn scars with bimatoprost is a viable way to induce darker tones on skin tissue. Other authors reported that a combination of fractional ablation and bimatoprost therapy resulted in the repigmentation of hypopigmented skin tissue [322,323]. Regis et al. also reported a case series of two patients presenting with hypopigmented scars on their lower legs following treatment laser hair removal procedure. Both patients showed complete repigmentation after treatment with fractional resurfacing and topical bimatoprost therapy [324]. Following the pandemic, various novel medical complaints and conditions were presented and new therapies had to be formulated. Acute respiratory distress is a common symptom seen in COVID-19 patients and its management involves prolonged prone positioning resulting in facial lesions. Laser-mediated bimatoprost delivery with microneedling was shown to reverse pigmentation [325].
Another dermatological concern managed with bimatoprost is vitiligo [326,327,328]. Vitiligo may occur non-segmented or segmented. Using the Vitiligo Area Scoring Index (VASI), Silpa-Archer et al. were able to demonstrate that bimatoprost combined with NB-UVB therapy improved the scores in patients with non-segmented vitiligo, while Jha et al. demonstrated same using photographs [329,330]. This NB-UVB technique was also used in addition to fractional carbon dioxide laser to achieve repigmentation in non-facial vitiligo [331].
Idiopathic guttate hypomelanosis is a condition associated with pale patches on the extremities. Kreeshnan and Madan published a case report detailing how they used bimatoprost in combination with a 308 nm excimer light, reversing pigmentation loss [332].
7. Bimatoprost and Hair Growth
Research shows success with the off-label aesthetic use of bimatoprost with varying disorders [333,334], although study groups sampled have lacked adequate racial diversity [335]. PGAs are constituents in certain over-the-counter cosmetics for lash enhancement [336]. Bimatoprost is emerging as an important player in cosmetics, albeit sometimes illegally [337]. Faigen used a patient-reported outcomes (PROs) questionnaire to assess the experience of 278 adults treated with bimatoprost for eyelash extensions and reported that cutaneous application of bimatoprost 0.03% produced favorable safety and tolerability [338]. Dilute levels of bimatoprost applied cutaneously for hair growth were found in the blood of test mice [339]. Bimatoprost gel and 0.03% solution both ameliorated madarosis post-chemotherapy in study groups [340,341,342]. Rossi et al. further advised that bimatoprost only be used after chemotherapy and not before or during chemotherapy [343]. Bimatoprost is reported to produce quantifiable enhanced hair and lash growth within one to two months of the commencement of the regimen [344,345], although female pattern androgenetic alopecia failed to respond to an injection of bimatoprost 0.03% [346]. The hair-growth potentials of bimatoprost were considered for possible treatments of androgenic alopecia [347,348]. Theoretically, bimatoprost was suggested to stimulate scalp follicles, potentially remedying scalp alopecia [349]. Bimatoprost achieves this by stimulating hair in the telogen stage to the anagen stage [350]. Chronic forms of alopecia, specifically alopecia totalis and universalis, may not show eruption of new hairs, but existing hairs may be lengthened after bimatoprost treatment [351]. Lu et al. examined common cosmetic products for the presence of prostaglandin analogues using nuclear magnetic resonance and other techniques, discovering a trend of illegal addition of bimatoprost and latanoprost as ingredients in these items [352]. Johansson et al. and Lee et al. also confirmed the presence of illegal supplementation with bimatoprost inside eyelash extension preparations [353,354]. Bimatoprost has also been reported as a management option for androgenetic alopecia [355] and for eyebrow rejuvenation [356,357].
Bimatoprost is safe in children [358] as in adults and has been prominently implicated in the literature to cause elongation of facial hair and has been reported to be as potent as Minoxidil [359,360,361]. Using a baseline of three factors, namely length, fullness, and satisfaction with hair, Fagien et al. demonstrated that bimatoprost 0.03% applied topically outperformed control groups in a multicenter study [362]. Another scale used is the Global Eyelash Assessment scale, and with this scale, Kwon et al. reported that bimatoprost use resulted in the safe elongation of the eyelashes of participating Asian females [363]. Use of bimatoprost 0.03% gel over a six-month period resulting in desired cosmesis with the enhancement of the eyelashes [361,362]. When compared to a placebo, bimatoprost produced statistically significant elongation of eyelashes, establishing that the extension obtained with this drug did not occur due to chance [364,365,366]. On the bright side, bimatoprost does not cause iris pigmentation when used periocularly and not as an eyedrop [367]. Bimatoprost has also been reported to be safe and well-tolerated as a therapy for the loss of eyebrow hair [368]. To this end, Suchonwanit et al. showed that 0.03% bimatoprost improved eyebrow trichosis as compared to bimatoprost 0.01% [369].
Hereditary linked progressive loss of scalp hair can also benefit from bimatoprost therapy [370]. Hypotrichosis can also be secondary as in the case of its chemically induced variant. Bimatoprost 0.03% has again been reported to induce hair growth in chemically induced hypotrichosis [371,372]. Electron microscopy revealed that bimatoprost-treated hairs possessed thicker dermis [373]. Chanasumon et al. suggested that bimatoprost’s restorative mechanism involves stimulation of the PGF2α and PGE2 receptors that potentiate hair growth [374,375,376]. Wirta similarly confirmed the ability of bimatoprost to simulate hair growth in a pooled study [377]. However, care should be taken in this regard, as Wirta et al. pooled a study of six multicentered studies lasting at least three months and reported that significant adverse effects were associated with the management of hypotrichosis using bimatoprost. However, the microneedling technique administered with vitamin D3 combined with bimatoprost is reported to improve hair production as compared to treatment with bimatoprost or vitamin D3 alone [378]. Patients may potentially avoid/reduce unwanted eyelash-lengthening effects of bimatoprost by using an absorbent material to wipe off excess eye drops after installation [379]. Palmer et al. examined the effect of bimatoprost 0.01% on nail growth and found that changes were not significant after one month of treatment [380].
8. Evolution of Bimatoprost Therapies
Drug compliance and persistence is a major problem in patients on long-term medication for chronic conditions like glaucoma [381]. The evolution from traditional eye drops to sustained-release implants and timolol gel-forming solutions has enhanced patient compliance and convenience [382]. These formulations offer extended drug delivery, reducing the frequency of administration and minimizing side effects [383]. With these, bimatoprost’s global use has expanded significantly, with healthcare professionals recognizing its potential benefits.
Implantable drugs and sensors can come to the rescue for such patients [384]. In such patients, a single intracameral insert may solve this problem and remove the need for a daily regimen of drugs [385]. Intracameral delivery of drug formulations achieves the double aim of bypassing the selective layers of the cornea and also ensuring instant bioavailability of the administered agent [386]. Mathematical models predict that intracameral slow-release devices are capable of achieving between 26–30% IOP reductions over a 6-month period [387]. Bimatoprost is also available as a sustained-release injection and this has been reported to lower pressure and thereby reduce multi-drug therapies even in post-selective laser trabeculectomy patients [388]. Some researchers have suggested using these sustained-release devices as an additive therapy against using them as an alternative to topical instillation [389]. However, the dose response for bimatoprost sustained-release devices in lowering IOP was more consistent than that obtained with topical instillation. Lewis et al. have shown the good tolerance and IOP-lowering abilities of bimatoprost implants after 6 months [390]. A single implant is potentially capable of delivering consistent IOP-lowering medication and results for years [391] and even up to two years [392]. These implants are available in different doses and have been found to have dose-dependent IOP-lowering effects [393]. Examples of other devices include nVISTA [394], iDose, OTX-TP, Latanoprost free acid SR, and ENV515, which are in different stages of trials [395]. Xu et al., however, reported that 15 of 48 eyes fitted with a bimatoprost sustained-release device suffered a device failure [396]. An intracameral implant was recently studied by Sirinek and Lin [397] and they noted that corneal endothelial cell loss is a possible complication of these devices.
Satyanarayana et al. reported on a novel bimatoprost delivery formulation using solid nanoparticles [398]. Studies on canine eyes revealed that bimatoprost SR significantly maintained lower IOP than topical administration [399]. Mean venous pressure has also been shown to reduce after bimatoprost use significantly [400]. It, however, remains to see how this novel delivery will be tolerated in the human eye in vivo, and what will be the best delivery method if well tolerated. Yadav et al. reported on a novel nano vesicular sustained release device designed to carry bimatoprost [401]. In vivo and in vitro insertion of the device was reported to be non-problematic without any resulting inflammatory signs [402]. Conjunctival fornix sustained-delivery inserts containing bimatoprost were tested in vivo using murine models and had good IOP reduction indices [403]. Topical bimatoprost inserts translated well to patient groups: they were associated with good long-term IOP control and insert retention in a phase II clinical trial [404].
Furthermore, these sustained-release devices can still be used safely in the eye that has undergone selective laser trabeculoplasty [405]. The ARTEMIS study evaluated the biodegradation rates of bimatoprost implants in 372 eyes, concluding that while there was statistical variability between sampled eyes, the majority of eyes showed significant biodegradation of implants after one year [406].
9. Novel Delivery Technologies for Bimatoprost
Promising future perspectives for bimatoprost include the exploration of novel delivery systems, such as contact lenses [407] to enhance drug efficacy and patient comfort. Through various formulations, advancements, and global use, bimatoprost has shown immense potential for addressing a wide range of therapeutic needs.
Sustained release delivery of drugs via contact lens is an emerging field due to the popularity of contact lens wear and its non-invasive status [408]. This, however, has implications for the dose delivery levels in patients wearing contact lenses. For example, Lotrafilcon-A-based contact lenses have been reported to show an uptake of up to 86% for bimatoprost contained in a 60 μL drop within one hour, leading researchers to suggest that wearers remove such contact lenses before the use of bimatoprost [409]. Graphene oxide fortification of contact lens polymers has been shown to enhance bimatoprost affinity to contact lenses and amplify drug delivery, albeit in murine models [410]. Vitamin E impregnation at a rate of 0.2 g per gram of hydrogel is reported to prolong the bimatoprost adherence and delivery dynamics over 10-fold [411]. Contact lenses loaded with gold nanoparticles have also been shown to increase drug retention and give better distribution of bimatoprost over time [412]. A novel biodegradable intracameral delivery technology passed phase 1 FDA approval [413]. Allergan’s single-use implant, “Durysta”, could potentially elongate treatment effects in glaucoma patients [413].
Nanosponge technology is another new medical innovation in eye care. Lambert et al. reported that bimatoprost-loaded nanosponges were able to lower IOP by up to 30% in mice that had artificially induced ocular hypertension [414].
10. Future Perspective for Bimatoprost
Ongoing research and future perspectives continue to shape its role in medicine, promising further advancements and improved patient outcomes. The aim of our review is to provide a brief description, overview, and studies in the current literature regarding the versatile clinical use of bimatoprost over the past 25 years. This can help clinicians determine the most suitable individualized therapy to meet the needs of each patient.
Bimatoprost has been described in the literature as the best agent for ocular hypertension and glaucoma management [415]. Efforts made in developing even more stable novel formulations are bound to be worthwhile. Because of its popularity and acceptability, bimatoprost may be easily abused seeing as it is a long-term, occasionally over-the-counter medication [416].
Despite the well-documented adverse PAP effects of bimatoprost, this very phenomenon suggests possible therapeutic use in resolving orbital proptosis in patients with Grave’s orbitopathy (GO) [417]. Draman et al. reported a reduction, though insignificant, in exophthalmometry results in patients suffering GO after a three-month regimen of bimatoprost [418]. Melovatskiy et al. have also theorized a similar application of bimatoprost to mitigate thyroid orbitopathy [419]. Eiger-Moscovich et al. conducted a blind study to assess the effects of bimatoprost on ocular tissue in patients with inactive thyroid orbitopathy’ they opined that bimatoprost reduced periorbital fat tissue expansion on visual observation [420]. Practically, Higashiyama and Ohji reported that a year-long bimatoprost therapy did not significantly reduce the extraocular fat volume or extraocular muscle volume [421].
The very effects of prostaglandins as documented In decreasing the corneal endothelial cell count suggest that caution be taken in the measurement and prescription of these classes of drugs to chronic glaucoma patients [422]. Proper diligence must be taken by periodically standardizing intraocular pressure measurements using pachymetry. Evolving technologies such as the automated visual field [423], scanning laser polarimetry [424], and dynamic contour tonometry [425,426] show promise in helping better manage glaucoma.
Adapting automated means of analysis into clinical trials centered on varying formulations of bimatoprost may more reliably facilitate the determination of adverse drug events with better objectivity [427].
Bastia et al. [428] examined retinal cell physiology restorative properties of different preparations of bimatoprost. They induced retinal cell disruption by administration of endothelin-1 and observed significant changes in electroretinogram patterns. Studies based on special formulations of bimatoprost treatment (NCX 470) subsequently returned values to baseline after six weeks. NCX 470 is a nitric oxide-donating prostaglandin analog. This lends credence to the ability of bimatoprost to offer neuroprotection [429]. NCX 470 is also more effective than latanoprost [430] and equimolar bimatoprost for IOP reduction in canine models [431,432]. Studies based on a special 0.01% preparation of bimatoprost, named JV-GL1, with a prostaglandin E2 receptor, have also shown tremendous promise by producing better IOP-lowering results than bimatoprost 0.03% [433].
11. Conclusions
Prostaglandin analogues will continue to be the mainstay of glaucoma management going into the next few decades. Bimatoprost ranks as arguably the most potent antiglaucoma and anti-OHT agent available on the open market. However, the data available do not give a definitive picture of its relative standing in comparison to other antiglaucoma drugs. However, more work still needs to be done as regards its adverse effects, especially hyperemia. Hirsutism, lash elongation, and skin pigmentation are amongst some of its side effects, but interestingly, these can also be clinically desired in other patients. Further research will be required in how to standardize bimatoprost preparations for use in extraocular conditions.
Author Contributions
Conceptualization, M.Z.; methodology, M.Z., C.G., C.S., L.S., E.C.C., E.S.E., F.D. and M.M.; validation, M.Z. and M.M.; formal analysis, M.Z. and M.M.; investigation, M.M. and M.M.; resources, C.S., C.G. and L.S.; writing—original draft preparation, M.Z., C.S., C.G., L.S., E.C.C., E.S.E., F.D. and M.M.; validation, M.Z. and M.M.; writing—review and editing, M.Z., C.G., C.S., L.S., F.D. and M.M.; validation, M.Z. and M.M.; visualization, M.Z., C.G., C.S., L.S., F.D. and M.M.; supervision, C.S. and L.S.; project administration, M.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Subbulakshmi, S.; Kavitha, S.; Venkatesh, R. Prostaglandin analogs in ophthalmology. Indian. J. Ophthalmol. 2023, 71, 1768–1776. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Mantravadi, A.V.; Myers, J.S. Patient considerations in ocular hypertension: Role of Bimatoprost ophthalmic solution. Clin. Ophthalmol. 2017, 11, 1273–1280. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, A.; Riva, I.; Bozkurt, B.; Hollo, G.; Quaranta, L.; Oddone, F.; Irkec, M.; Dutton, G.N.; Konstas, A.G. A new look at the safety and tolerability of prostaglandin analogue eyedrops in glaucoma and ocular hypertension. Expert. Opin. Drug Saf. 2022, 21, 525–539. [Google Scholar] [CrossRef]
- Meymandi, S.S.; Safari, A.; Meymandi, M.S.; Aflatoonian, M. The role of fractional laser-assisted drug delivery in enhancing the efficacy of topical bimatoprost solution in the treatment of alopecia areata: An intra-patient comparative randomized clinical trial. J. Cosmet. Dermatol. 2024, 23, 1663–1668. [Google Scholar] [CrossRef] [PubMed]
- Klimko, P.G.; Sharif, N.A. Discovery, characterization and clinical utility of prostaglandin agonists for the treatment of glaucoma. Br. J. Pharmacol. 2019, 176, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.; Jiang, M.; Ye, B.; Zhang, G.T.; Li, W.; Tang, P.; Huang, Z.; Chen, F. A unified strategy to prostaglandins: Chemoenzymatic total synthesis of cloprostenol, Bimatoprost, PGF(2alpha), fluprostenol, and travoprost guided by biocatalytic retrosynthesis. Chem. Sci. 2021, 12, 10362–10370. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.S.; Meyer, J.J. Bimatoprost Ophthalmic Solution; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Doucette, L.P.; Walter, M.A. Prostaglandins in the eye: Function, expression, and roles in glaucoma. Ophthalmic Genet. 2017, 38, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Kobelt, G.; Texier-Richard, B.; Buchholz, P.; Bron, A.; Renard, J.P.; Rouland, J.F.; Nordmann, J.P. Treatment of glaucoma in clinical practice: Four-year results from a patient registry in France. J. Glaucoma 2010, 19, 199–206. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 5311027, Bimatoprost. PubChem. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Bimatoprost (accessed on 13 April 2024).
- Yamagishi, R.; Aihara, M.; Araie, M. Neuroprotective effects of prostaglandin analogues on retinal ganglion cell death independent of intraocular pressure reduction. Exp. Eye Res. 2011, 93, 265–270. [Google Scholar] [CrossRef]
- Faulkner, R.; Sharif, N.A.; Orr, S.; Sall, K.; Dubiner, H.; Whitson, J.T.; Moster, M.; Craven, E.R.; Curtis, M.; Pailliotet, C.; et al. Aqueous humor concentrations of Bimatoprost free acid, Bimatoprost and travoprost free acid in cataract surgical patients administered multiple topical ocular doses of LUMIGAN or TRAVATAN. J. Ocul. Pharmacol. Ther. 2010, 26, 147–156. [Google Scholar] [CrossRef]
- Brubaker, R.F. Mechanism of action of bimatoprost (Lumigan). Surv. Ophthalmol. 2001, 45, S347–S351. [Google Scholar] [CrossRef]
- Woodward, D.F.; Krauss, A.H.; Nilsson, S.F. Bimatoprost effects on aqueous humor dynamics in monkeys. J. Ophthalmol. 2010, 2010, 926192. [Google Scholar] [CrossRef]
- Vyas, P.; Naik, U.; Gangaiah, J.B. Efficacy of Bimatoprost 0.03% in reducing intraocular pressure in patients with 360 degrees synechial angle-closure glaucoma: A preliminary study. Indian. J. Ophthalmol. 2011, 59, 13–16. [Google Scholar]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef]
- Shen, J.; Goodkin, M.L.; Tong, W.; Attar, M. Ocular pharmacokinetics and tolerability of Bimatoprost ophthalmic solutions administered once or twice daily in rabbits, and clinical dosing implications. Clin. Ophthalmol. 2017, 11, 1761–1767. [Google Scholar] [CrossRef]
- Heo, J.Y.; Ooi, Y.H.; Rhee, D.J. Effect of prostaglandin analogs: Latanoprost, Bimatoprost, and unoprostone on matrix metalloproteinases and their inhibitors in human trabecular meshwork endothelial cells. Exp. Eye Res. 2020, 194, 108019. [Google Scholar] [CrossRef]
- Hwang, H.B.; Kim, S.Y. The Effect of Prostaglandin Analogues on the Ciliary Zonular Fibers of the Rabbit Crystalline Lens. Curr. Eye Res. 2018, 43, 1357–1361. [Google Scholar] [CrossRef]
- Stamer, W.D.; Piwnica, D.; Jolas, T.; Carling, R.W.; Cornell, C.L.; Fliri, H.; Martos, J.; Pettit, S.N.; Wang, J.W.; Woodward, D.F. Cellular basis for Bimatoprost effects on human conventional outflow. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5176–5181. [Google Scholar] [CrossRef]
- Angeli, A.; Supuran, C.T. Prostaglandin receptor agonists as antiglaucoma agents (a patent review 2013–2018). Expert. Opin. Ther. Pat. 2019, 29, 793–803. [Google Scholar] [CrossRef]
- Li, X.; Liu, G.; Wang, Y.; Yu, W.; Xiang, H.; Liu, X. A case hypersensitive to Bimatoprost and dexamethasone. J. Ocul. Pharmacol. Ther. 2011, 27, 519–523. [Google Scholar] [CrossRef]
- Comparison of Bimatoprost SR to Selective Laser Trabeculoplasty in Patients with Open-Angle Glaucoma or Ocular Hypertension; Identifier NCT02507687; U.S. National Library of Medicine: Bethesda, MD, USA, 2023. Available online: https://clinicaltrials.gov/ct2/show/study/NCT02507687 (accessed on 14 April 2024).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Loftus, J.; Christopoulou, D.; Blak, B.T.; Hards, M. Topical prostaglandin fixed combinations in UK primary care: Observational study using data from the health improvement network. Eur. J. Ophthalmol. 2012, 22, 376–387. [Google Scholar] [CrossRef]
- Rahman, M.Q.; Abeysinghe, S.S.; Kelly, S.; Roskell, N.S.; Shannon, P.R.; Abdlseaed, A.A.; Montgomery, D.M. Persistence of glaucoma medical therapy in the Glasgow Glaucoma Database. Br. J. Ophthalmol. 2011, 95, 966–970. [Google Scholar] [CrossRef]
- Heo, J.H.; Rascati, K.L.; Wilson, J.P.; Lawson, K.A.; Richards, K.M.; Nair, R. Comparison of Prostaglandin Analog Treatment Patterns in Glaucoma and Ocular Hypertension. J. Manag. Care Spec. Pharm. 2019, 25, 1001–1010. [Google Scholar] [CrossRef]
- Dams, I.; Wasyluk, J.; Prost, M.; Kutner, A. Therapeutic uses of prostaglandin F(2alpha) analogues in ocular disease and novel synthetic strategies. Prostaglandins Other Lipid Mediat. 2013, 104, 109–121. [Google Scholar] [CrossRef]
- Woodward, D.F.; Phelps, R.L.; Krauss, A.H.; Weber, A.; Short, B.; Chen, J.; Liang, Y.; Wheeler, L.A. Bimatoprost: A novel antiglaucoma agent. Cardiovasc. Drug Rev. 2004, 22, 103–120. [Google Scholar] [CrossRef]
- Blondeau, P.; Hamid, M.; Ghalie, Z. Prospective randomized clinical trial on the effects of Latanoprost, travoprost and Bimatoprost on Latanoprost non-responders. J. Fr. Ophtalmol. 2019, 42, 894–899. [Google Scholar] [CrossRef]
- Crichton, A.C.; Nixon, D.R.; Simonyi, S.; Bhogal, M.; Sigouin, C.S.; Discepola, M.J.; Hutnik, C.M.; Baptiste, D.C.; Yan, D.B. An observational study of Bimatoprost 0.01% in patients on prior intraocular pressure-lowering therapy: The Canadian Lumigan((R)) RC Early Analysis Review (CLEAR) trial. Clin. Ophthalmol. 2014, 8, 1031–1038. [Google Scholar]
- Campbell, J.H.; Schwartz, G.; Labounty, B.; Kowalski, J.; Patel, V.D. Comparison of adherence and persistence with Bimatoprost 0.01% versus Bimatoprost 0.03% topical ophthalmic solutions. Curr. Med. Res. Opin. 2013, 29, 1201–1209. [Google Scholar] [CrossRef]
- Stankiewicz, A.; Wierzbowska, J.; Siemiatkowska, A.; Fuksinska, B.; Robaszkiewicz, J.; Zegadlo, A.; Ehrlich, R.; Siesky, B.; Harris, A. The additive effect of dorzolamide hydrochloride (Trusopt) and a morning dose of Bimatoprost (Lumigan) on intraocular pressure and retrobulbar blood flow in patients with primary open-angle glaucoma. Br. J. Ophthalmol. 2010, 94, 1307–1311. [Google Scholar] [CrossRef]
- Inoue, K.; Shiokawa, M.; Fujimoto, T.; Tomita, G. Effects of treatment with Bimatoprost 0.03% for 3 years in patients with normal-tension glaucoma. Clin. Ophthalmol. 2014, 8, 1179–1183. [Google Scholar] [CrossRef]
- Deshpande, S.S.; Sonty, S.; Ahmad, A. Evaluating intraocular pressure-lowering solutions for the treatment of open-angle glaucoma: Comparison between Bimatoprost 0.03% and Bimatoprost 0.01%—An observational switch study. Clin. Ophthalmol. 2017, 11, 1371–1376. [Google Scholar] [CrossRef]
- Asendrych-Wicik, K.; Zarczuk, J.; Walaszek, K.; Ciach, T.; Markowicz-Piasecka, M. Trends in development and quality assessment of pharmaceutical formulations—F2alpha analogues in the glaucoma treatment. Eur. J. Pharm. Sci. 2023, 180, 106315. [Google Scholar] [CrossRef] [PubMed]
- Diaconita, V.; Quinn, M.; Jamal, D.; Dishan, B.; Malvankar-Mehta, M.S.; Hutnik, C. Washout Duration of Prostaglandin Analogues: A Systematic Review and Meta-analysis. J. Ophthalmol. 2018, 2018, 3190684. [Google Scholar] [CrossRef]
- Lim, C.W.; Diaconita, V.; Liu, E.; Ault, N.; Lizotte, D.; Nguyen, M.; Hutnik, C.M.L. Effect of 6-week washout period on intraocular pressure following chronic prostaglandin analogue treatment: A randomized controlled trial. Can. J. Ophthalmol. 2020, 55, 143–151. [Google Scholar] [CrossRef]
- Bimatoprost. Drugs and Lactation Database (LactMed(R)); Bimatoprost: Bethesda, MD, USA, 2006. [Google Scholar]
- Shazly, T.A.; Latina, M.A. Comparison of intraocular pressure-lowering effect of every night versus every other night dosing of Bimatoprost 0.03%. J. Ocul. Pharmacol. Ther. 2011, 27, 369–371. [Google Scholar] [CrossRef]
- Nixon, D.R.; Simonyi, S.; Bhogal, M.; Sigouin, C.S.; Crichton, A.C.; Discepola, M.; Hutnik, C.M.; Yan, D.B. An observational study of Bimatoprost 0.01% in treatment-naive patients with primary open angle glaucoma or ocular hypertension: The CLEAR trial. Clin. Ophthalmol. 2012, 6, 2097–2103. [Google Scholar]
- Wang, K.; Xu, L.; Yuan, Z.; Yao, K.; Zhao, J.; Xu, L.; Fang, A.; Zhang, M.; Wu, L.; Ji, J.; et al. Intraocular pressure-lowering efficacy and safety of Bimatoprost 0.03% therapy for primary open-angle glaucoma and ocular hypertension patients in China. BMC Ophthalmol. 2014, 14, 21. [Google Scholar] [CrossRef]
- Tsumura, T.; Yoshikawa, K.; Suzumura, H.; Kimura, T.; Sasaki, S.; Kimura, I.; Takeda, R. Bimatoprost ophthalmic solution 0.03% lowered intraocular pressure of normal-tension glaucoma with minimal adverse events. Clin. Ophthalmol. 2012, 6, 1547–1552. [Google Scholar] [CrossRef]
- Konstas, A.G.; Hollo, G.; Mikropoulos, D.; Tsironi, S.; Haidich, A.B.; Embeslidis, T.; Georgiadou, I.; Irkec, M.; Melamed, S. Twenty-four-hour intraocular pressure control with Bimatoprost and the Bimatoprost/timolol fixed combination administered in the morning, or evening in exfoliative glaucoma. Br. J. Ophthalmol. 2010, 94, 209–213. [Google Scholar] [CrossRef]
- Day, D.G.; Walters, T.R.; Schwartz, G.F.; Mundorf, T.K.; Liu, C.; Schiffman, R.M.; Bejanian, M. Bimatoprost 0.03% preservative-free ophthalmic solution versus Bimatoprost 0.03% ophthalmic solution (Lumigan) for glaucoma or ocular hypertension: A 12-week, randomized, double-masked trial. Br. J. Ophthalmol. 2013, 97, 989–993. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, I.; Gil Pina, R.; Lanzagorta-Aresti, A.; Schiffman, R.M.; Liu, C.; Bejanian, M. Bimatoprost 0.03%/timolol 0.5% preservative-free ophthalmic solution versus Bimatoprost 0.03%/timolol 0.5% ophthalmic solution (Ganfort) for glaucoma or ocular hypertension: A 12-week randomized controlled trial. Br. J. Ophthalmol. 2014, 98, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Ogundele, A.B.; Jasek, M.C. Aqueous humor penetration of topical Bimatoprost 0.01% and Bimatoprost 0.03% in rabbits. Clin. Ophthalmol. 2010, 4, 1447–1450. [Google Scholar] [CrossRef] [PubMed]
- Chang-Lin, J.E.; Batoosingh, A.L.; Hollander, D.A.; Schiffman, R.M.; Tang-Liu, D.D. Aqueous humor penetration of topical Bimatoprost 0.01% and Bimatoprost 0.03% in rabbits: Response to authors. Clin. Ophthalmol. 2011, 5, 1119–1120. [Google Scholar] [CrossRef] [PubMed]
- Pfennigsdorf, S.; Ramez, O.; von Kistowski, G.; Mader, B.; Eschstruth, P.; Frobose, M.; Thelen, U.; Spraul, C.; Schnober, D.; Cooper, H.; et al. Multicenter, prospective, open-label, observational study of Bimatoprost 0.01% in patients with primary open-angle glaucoma or ocular hypertension. Clin. Ophthalmol. 2012, 6, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Filippelli, M.; Campagna, G.; Ciampa, N.; Fioretto, G.; Giannini, R.; Marino, P.F.; dell’Omo, R.; Costagliola, C. Ocular Tolerability of Bimatoprost 0.1 mg/mL Preservative-Free versus Bimatoprost 0.1 mg/mL with Benzalkonium Chloride or Bimatoprost 0.3 mg/mL Preservative-Free in Patients with Primary Open-Angle Glaucoma. J. Clin. Med. 2022, 11, 3518. [Google Scholar] [CrossRef]
- Petricca, S.; Celenza, G.; Costagliola, C.; Tranfa, F.; Iorio, R. Cytotoxicity, Mitochondrial Functionality, and Redox Status of Human Conjunctival Cells after Short and Chronic Exposure to Preservative-Free Bimatoprost 0.03% and 0.01%: An In Vitro Comparative Study. Int. J. Mol. Sci. 2022, 23, 14113. [Google Scholar] [CrossRef] [PubMed]
- Nixon, D.R. A randomized, prospective study of Bimatoprost 0.01% or travoprost/timolol in patients previously treated with Latanoprost and timolol to reduce intraocular pressure. J. Ocul. Pharmacol. Ther. 2013, 29, 876–881. [Google Scholar] [CrossRef] [PubMed]
- Katz, L.J.; Cohen, J.S.; Batoosingh, A.L.; Felix, C.; Shu, V.; Schiffman, R.M. Twelve-month, randomized, con-trolled trial of Bimatoprost 0.01%, 0.0125%, and 0.03% in patients with glaucoma or ocular hypertension. Am. J. Ophthalmol. 2010, 149, 661–671 e1. [Google Scholar] [CrossRef]
- Figus, M.; Nardi, M.; Piaggi, P.; Sartini, M.; Guidi, G.; Martini, L.; Lazzeri, S. Bimatoprost 0.01% vs. Bimatoprost 0.03%: A 12-month prospective trial of clinical and in vivo confocal microscopy in glaucoma patients. Eye 2014, 28, 422–429. [Google Scholar] [CrossRef]
- Xu, K.M.; Cho, R.; Chan, T.Y.B. Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Pa-tients with Various Types of Glaucoma and Ocular Hypertension. Clin. Ophthalmol. 2022, 16, 2385–2390. [Google Scholar] [CrossRef] [PubMed]
- Tung, J.D.; Tafreshi, A.; Weinreb, R.N.; Slight, J.R.; Medeiros, F.A.; Liu, J.H. Twenty-four-hour effects of Bima-toprost 0.01% monotherapy on intraocular pressure and ocular perfusion pressure. BMJ Open 2012, 2, e001106. [Google Scholar] [CrossRef] [PubMed]
- Alany, R.G. Adherence, persistence and cost-consequence comparison of Bimatoprost topical ocular formulations. Curr. Med. Res. Opin. 2013, 29, 1187–1189. [Google Scholar] [CrossRef] [PubMed]
- Hollo, G.; Thelen, U.; Teus, M.A.; Quaranta, L.; Ferkova, S.; Babic, N.; Misiuk-Hojlo, M.; Mikropoulos, D.G.; Kaluzny, B.J.; Kozobolis, V.; et al. Long-term outcomes of prostaglandin analog versus timolol maleate in ocular hypertensive or primary open-angle glaucoma patients in Europe. J. Ocul. Pharmacol. Ther. 2011, 27, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Giannico, A.T.; Lima, L.; Shaw, G.C.; Russ, H.H.; Froes, T.R.; Montiani-Ferreira, F. Effects of prostaglandin analogs on blood flow velocity and resistance in the ophthalmic artery of rabbits. Arq. Bras. Oftalmol. 2016, 79, 33–36. [Google Scholar] [CrossRef]
- Natt, N.K.; Gupta, A.; Singh, G.; Singh, T. A pharmacoeconomic analysis to determine the relative cost-effectiveness of Bimatoprost 0.03% eye drops and brimonidine 0.2% eye drops in patients of primary open-angle glaucoma/ocular hypertension. Indian J. Ophthalmol. 2014, 62, 1136–1140. [Google Scholar] [CrossRef] [PubMed]
- Artunay, O.; Yuzbasioglu, E.; Unal, M.; Rasier, R.; Sengul, A.; Bahcecioglu, H. Bimatoprost 0.03% versus brimonidine 0.2% in the prevention of intraocular pressure spike following neodymium:yttrium-aluminum-garnet la-ser posterior capsulotomy. J. Ocul. Pharmacol. Ther. 2010, 26, 513–517. [Google Scholar] [CrossRef]
- Stalmans, I.; Oddone, F.; Cordeiro, M.F.; Hommer, A.; Montesano, G.; Ribeiro, L.; Sunaric-Megevand, G.; Rossetti, L. Comparison of preservative-free Latanoprost and preservative-free Bimatoprost in a multicenter, random-ized, investigator-masked cross-over clinical trial, the SPORT trial. Graefes Arch. Clin. Exp. Ophthalmol. 2016, 254, 1151–1158. [Google Scholar] [CrossRef] [PubMed]
- Orme, M.; Collins, S.; Dakin, H.; Kelly, S.; Loftus, J. Mixed treatment comparison and meta-regression of the effi-cacy and safety of prostaglandin analogues and comparators for primary open-angle glaucoma and ocular hypertension. Curr. Med. Res. Opin. 2010, 26, 511–528. [Google Scholar] [CrossRef]
- Gimenez-Gomez, R.; Garcia-Catalan, M.R.; Gallardo-Galera, J.M. Tear clearance and ocular symptoms in patients treated with preservative-free prostaglandins. Arch. Soc. Esp. Oftalmol. 2013, 88, 88–91. [Google Scholar] [CrossRef]
- Hommer, A.; Kimmich, F. Switching patients from preserved prostaglandin-analog monotherapy to preservative-free tafluprost. Clin. Ophthalmol. 2011, 5, 623–631. [Google Scholar] [PubMed]
- Ranno, S.; Sacchi, M.; Brancato, C.; Gilardi, D.; Lembo, A.; Nucci, P. A prospective study evaluating IOP changes after switching from a therapy with prostaglandin eye drops containing preservatives to non-preserved tafluprost in glaucoma patients. Sci. World J. 2012, 2012, 804730. [Google Scholar] [CrossRef] [PubMed]
- Kara, C.; Sen, E.M.; Elgin, K.U.; Serdar, K.; Yilmazbas, P. Does the intraocular pressure-lowering effect of prostaglandin analogues continue over the long term? Int. Ophthalmol. 2017, 37, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.H.; Schwartz, G.F.; LaBounty, B.; Kowalski, J.W.; Patel, V.D. Patient adherence and persistence with topical ocular hypotensive therapy in real-world practice: A comparison of Bimatoprost 0.01% and travoprost Z 0.004% ophthalmic solutions. Clin. Ophthalmol. 2014, 8, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.S.; Vold, S.; Zaman, F.; Williams, J.M.; Hollander, D.A. Bimatoprost 0.01% or 0.03% in patients with glaucoma or ocular hypertension previously treated with Latanoprost: Two randomized 12-week trials. Clin. Ophthalmol. 2014, 8, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Zhang, F.; Liu, K.; Duan, X. Efficacy and safety of prostaglandin analogues in primary open-angle glaucoma or ocular hypertension patients: A meta-analysis. Medicine 2019, 98, e16597. [Google Scholar] [CrossRef]
- Turan-Vural, E.; Torun-Acar, B.; Acar, S. Effect of ketorolac add-on treatment on intraocular pressure in glaucoma patients receiving prostaglandin analogues. Ophthalmologica 2012, 227, 205–209. [Google Scholar] [CrossRef]
- Ozyol, P.; Ozyol, E.; Erdogan, B.D. The Interaction of Nepafenac and Prostaglandin Analogs in Primary Open-angle Glaucoma Patients. J. Glaucoma 2016, 25, e145-9. [Google Scholar] [CrossRef] [PubMed]
- Faridi, U.A.; Saleh, T.A.; Ewings, P.; Venkateswaran, M.; Cadman, D.H.; Samarasinghe, R.A.; Vodden, J.; Claridge, K.G. Comparative study of three prostaglandin analogues in the treatment of newly diagnosed cases of ocular hypertension, open-angle and normal tension glaucoma. Clin. Exp. Ophthalmol. 2010, 38, 678–682. [Google Scholar] [CrossRef]
- Brennan, N.; Dehabadi, M.H.; Nair, S.; Quartilho, A.; Bunce, C.; Reekie, I.; Obikpo, R. Efficacy and safety of Bimatoprost in glaucoma and ocular hypertension in non-responder patients. Int. J. Ophthalmol. 2017, 10, 1251–1254. [Google Scholar]
- Zhou, L.; Zhan, W.; Wei, X. Clinical pharmacology and pharmacogenetics of prostaglandin analogues in glaucoma. Front. Pharmacol. 2022, 13, 1015338. [Google Scholar] [CrossRef] [PubMed]
- Priluck, A.Z.; Havens, S.J. Variation in Prostaglandin Analog Prices Paid for Through Medicare Part D. J. Glaucoma 2019, 28, e17–e20. [Google Scholar] [CrossRef] [PubMed]
- Lazcano-Gomez, G.; Hernandez-Oteyza, A.; Iriarte-Barbosa, M.J.; Hernandez-Garciadiego, C. Topical glaucoma therapy cost in Mexico. Int. Ophthalmol. 2014, 34, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, V.L.; Liu, P.; Dhruva, S.S.; Shah, N.D.; Bollinger, K.E.; Ross, J.S. Prostaglandin Coverage and Costs to Medicare and Medicare Beneficiaries, 2009–2017. J. Manag. Care Spec. Pharm. 2020, 26, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Kammer, J.A.; Katzman, B.; Ackerman, S.L.; Hollander, D.A. Efficacy and tolerability of Bimatoprost versus travoprost in patients previously on Latanoprost: A 3-month, randomised, masked-evaluator, multicentre study. Br. J. Ophthalmol. 2010, 94, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Kausar, N.; Thapa, K. Comparative study of Latanoprost (0.005%) and Bimatoprost (0.03%) in primary open angle glaucoma. Nepal. J. Ophthalmol. 2022, 14, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Zhao, Y.J.; Chew, P.T.; Sng, C.C.; Wong, H.T.; Yip, L.W.; Wu, T.S.; Bautista, D.; Teng, M.; Khoo, A.L.; et al. Comparative efficacy and tolerability of topical prostaglandin analogues for primary open-angle glaucoma and ocular hypertension. Ann. Pharmacother. 2014, 48, 1585–1593. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.C.; Brown, M.M. Patient Preference-Based Comparative Effectiveness and Cost-Utility Analysis of the Prostamides for Open-Angle Glaucoma. J. Ocul. Pharmacol. Ther. 2019, 35, 145–160. [Google Scholar] [CrossRef] [PubMed]
- Calugaru, D.; Calugaru, M. Monotherapy with lipid structural derivatives in glaucoma. Oftalmologia 2010, 54, 30–43. [Google Scholar]
- Mishra, D.; Sinha, B.P.; Kumar, M.S. Comparing the efficacy of Latanoprost (0.005%), Bimatoprost (0.03%), travoprost (0.004%), and timolol (0.5%) in the treatment of primary open angle glaucoma. Korean J. Ophthalmol. 2014, 28, 399–407. [Google Scholar] [CrossRef]
- Kook, M.S.; Simonyi, S.; Sohn, Y.H.; Kim, C.Y.; Park, K.H. Bimatoprost 0.01% for previously treated patients with open-angle glaucoma or ocular hypertension in the Korean clinical setting. Jpn. J. Ophthalmol. 2015, 59, 325–334. [Google Scholar] [CrossRef]
- Solish, A.M.; James, F.; Walt, J.G.; Chiang, T.H. Paired-eye comparison of medical therapies for glaucoma. Clin. Ophthalmol. 2010, 4, 1131–1135. [Google Scholar] [CrossRef]
- Macky, T.A. Bimatoprost versus travoprost in an Egyptian population: A hospital-based prospective, randomized study. J. Ocul. Pharmacol. Ther. 2010, 26, 605–610. [Google Scholar] [CrossRef]
- Inoue, K.; Setogawa, A.; Tomita, G. Nonresponders to Prostaglandin Analogs Among Normal-Tension Glaucoma Patients. J. Ocul. Pharmacol. Ther. 2016, 32, 90–96. [Google Scholar] [CrossRef]
- Sato, S.; Hirooka, K.; Baba, T.; Mizote, M.; Fujimura, T.; Tenkumo, K.; Ueda, H.; Shiraga, F. Efficacy and safety of switching from topical Latanoprost to Bimatoprost in patients with normal-tension glaucoma. J. Ocul. Pharmacol. Ther. 2011, 27, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Sawada, A.; Yamamoto, T. Switching efficacy on intraocular pressure from Latanoprost to Bimatoprost in eyes with open angle glaucoma: Implication to the changes of central corneal thickness. Jpn. J. Ophthalmol. 2014, 58, 423–428. [Google Scholar] [CrossRef]
- Germano, R.A.; Susanna, R., Jr.; De Moraes, C.G.; Susanna, B.N.; Susanna, C.N.; Chibana, M.N. Effect of Switching from Latanoprost to Bimatoprost in Primary Open-Angle Glaucoma Patients Who Experienced Intraocular Pressure Elevation During Treatment. J. Glaucoma 2016, 25, e359–e366. [Google Scholar] [CrossRef] [PubMed]
- El Hajj Moussa, W.G.; Farhat, R.G.; Nehme, J.C.; Sahyoun, M.A.; Schakal, A.R.; Jalkh, A.E.; Abi Karam, M.P.; Azar, G.G. Comparison of Efficacy and Ocular Surface Disease Index Score between Bimatoprost, Latanoprost, Travoprost, and Tafluprost in Glaucoma Patients. J. Ophthalmol. 2018, 2018, 1319628. [Google Scholar] [CrossRef] [PubMed]
- Whitson, J.T.; Trattler, W.B.; Matossian, C.; Williams, J.; Hollander, D.A. Ocular surface tolerability of prosta-glandin analogs in patients with glaucoma or ocular hypertension. J. Ocul. Pharmacol. Ther. 2010, 26, 287–292. [Google Scholar] [CrossRef]
- Craven, E.R.; Liu, C.C.; Batoosingh, A.; Schiffman, R.M.; Whitcup, S.M. A randomized, controlled comparison of macroscopic conjunctival hyperemia in patients treated with Bimatoprost 0.01% or vehicle who were previously con-trolled on Latanoprost. Clin. Ophthalmol. 2010, 4, 1433–1440. [Google Scholar] [CrossRef]
- Demirel, S.; Doganay, S.; Gurses, I.; Iraz, M. Toxic-inflammatory effects of prostaglandin analogs on the ocular surface. Ocul. Immunol. Inflamm. 2013, 21, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Crichton, A.C.; Vold, S.; Williams, J.M.; Hollander, D.A. Ocular surface tolerability of prostaglandin analogs and prostamides in patients with glaucoma or ocular hypertension. Adv. Ther. 2013, 30, 260–270. [Google Scholar] [CrossRef]
- Pellinen, P.; Huhtala, A.; Tolonen, A.; Lokkila, J.; Maenpaa, J.; Uusitalo, H. The cytotoxic effects of preserved and preservative-free prostaglandin analogs on human corneal and conjunctival epithelium in vitro and the distribution of benzalkonium chloride homologs in ocular surface tissues in vivo. Curr. Eye Res. 2012, 37, 145–154. [Google Scholar] [CrossRef]
- Aihara, M.; Shirato, S.; Sakata, R. Incidence of deepening of the upper eyelid sulcus after switching from Latanoprost to Bimatoprost. Jpn. J. Ophthalmol. 2011, 55, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Shiokawa, M.; Wakakura, M.; Tomita, G. Deepening of the upper eyelid sulcus caused by 5 types of prostaglandin analogs. J. Glaucoma 2013, 22, 626–631. [Google Scholar] [CrossRef]
- Sakata, R.; Shirato, S.; Miyata, K.; Aihara, M. Recovery from deepening of the upper eyelid sulcus after switching from Bimatoprost to Latanoprost. Jpn. J. Ophthalmol. 2013, 57, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; McCluskey, P. Clinical utility and differential effects of prostaglandin analogs in the management of raised intraocular pressure and ocular hypertension. Clin. Ophthalmol. 2010, 4, 741–764. [Google Scholar]
- Yanagi, M.; Kiuchi, Y.; Yuasa, Y.; Yoneda, T.; Sumi, T.; Hoshikawa, Y.; Kobayashi, M.; Fukushima, A. Association between glaucoma eye drops and hyperemia. Jpn. J. Ophthalmol. 2016, 60, 72–77. [Google Scholar] [CrossRef]
- Guedes, R.A.; Guedes, V.M.; Freitas, S.M.; Chaoubah, A. Quality of life of glaucoma patients under medical therapy with different prostaglandins. Clin. Ophthalmol. 2012, 6, 1749–1753. [Google Scholar] [CrossRef]
- Giannaccare, G.; Pellegrini, M.; Bernabei, F.; Senni, C.; Aloi, M.; Scalzo, G.C.; Ceravolo, D.; Iovino, C.; Scorcia, V. Comparative analysis of ocular redness score evaluated automatically in glaucoma patients under different topical medications. Eur. J. Ophthalmol. 2021, 31, 2405–2411. [Google Scholar] [CrossRef]
- Schmier, J.K.; Lau, E.C.; Covert, D.W. Two-year treatment patterns and costs in glaucoma patients initiating treat-ment with prostaglandin analogs. Clin. Ophthalmol. 2010, 4, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Schmier, J.K.; Covert, D.W.; Robin, A.L. First-year treatment costs among new initiators of topical prostaglandin analog identified from November 2007 through April 2008. Curr. Med. Res. Opin. 2010, 26, 2769–2777. [Google Scholar] [CrossRef] [PubMed]
- Alm, A. Latanoprost in the treatment of glaucoma. Clin. Ophthalmol. 2014, 8, 1967–1985. [Google Scholar]
- Arias, A.; Schargel, K.; Ussa, F.; Canut, M.I.; Robles, A.Y.; Sanchez, B.M. Patient persistence with first-line an-tiglaucomatous monotherapy. Clin. Ophthalmol. 2010, 4, 261–267. [Google Scholar]
- Hahn, S.R.; Kotak, S.; Tan, J.; Kim, E. Physicians’ treatment decisions, patient persistence, and interruptions in the continuous use of prostaglandin therapy in glaucoma. Curr. Med. Res. Opin. 2010, 26, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Schmier, J.K.; Covert, D.W. First-year treatment costs among new initiators of topical prostaglandin analogs: Pooled results. Clin. Ophthalmol. 2010, 4, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Berenson, K.L.; Kymes, S.; Hollander, D.A.; Fiscella, R.; Burk, C.; Patel, V.D. Cost-offset analysis: Bimatoprost versus other prostaglandin analogues in open-angle glaucoma. Am. J. Manag. Care 2011, 17, e365-74. [Google Scholar] [PubMed]
- Islam, S.; Spry, C. Prostaglandin Analogues for Ophthalmic Use: A Review of Comparative Clinical Effectiveness, Cost-Effectiveness, and Guidelines; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2020. [Google Scholar]
- Birt, C.M.; Buys, Y.M.; Kiss, A.; Trope, G.E.; Toronto Area Glaucoma, S. The influence of central corneal thickness on response to topical prostaglandin analogue therapy. Can. J. Ophthalmol. 2012, 47, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Ichhpujani, P.; Katz, L.J.; Hollo, G.; Shields, C.L.; Shields, J.A.; Marr, B.; Eagle, R.; Alvim, H.; Wizov, S.S.; Acheampong, A.; et al. Comparison of human ocular distribution of Bimatoprost and Latanoprost. J. Ocul. Pharmacol. Ther. 2012, 28, 134–145. [Google Scholar] [CrossRef]
- Stevens, A.; Iliev, M.E.; de Jong, L.; Grobeiu, I.; Hommer, A. A combined analysis of four observational studies evaluating the intraocular pressure-lowering ability and tolerability of Bimatoprost 0.01% in patients with primary open-angle glaucoma or ocular hypertension. Clin. Ophthalmol. 2016, 10, 635–641. [Google Scholar] [CrossRef]
- Kawaguchi, I.; Higashide, T.; Ohkubo, S.; Kawaguchi, C.; Sugiyama, K. Comparison of efficacy of four prosta-glandin analogues by bilateral treatment in healthy subjects. Jpn. J. Ophthalmol. 2012, 56, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Lemmens, S.; Rossetti, L.; Oddone, F.; Sunaric-Megevand, G.; Hommer, A.; Vandewalle, E.; Francesca Cor-deiro, M.; McNaught, A.; Montesano, G.; Stalmans, I. Comparison of preserved Bimatoprost 0.01% with preserva-tive-free tafluprost: A randomised, investigator-masked, 3-month crossover, multicentre trial, SPORT II. Eur. J. Ophthalmol. 2021, 32, 11206721211006573. [Google Scholar]
- Suzuki, K.; Teranishi, S.; Sagara, T.; Yoshino, H.; Nakayama, M.; Enoki, M.; Nuno, Y.; Hirano, S.; Wakuta, M.; Takahashi, N.; et al. Safety and Efficacy of Benzalkonium Chloride-optimized Tafluprost in Japanese Glaucoma Patients with Existing Superficial Punctate Keratitis. J. Glaucoma 2015, 24, e145-50. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.V.; Gupta, P.K.; Vudathala, D.K.; Blair, I.A.; Tanna, A.P. Thermal stability of Bimatoprost, Latanoprost, and travoprost under simulated daily use. J. Ocul. Pharmacol. Ther. 2011, 27, 51–59. [Google Scholar] [CrossRef] [PubMed]
- DuBiner, H.B.; Hubatsch, D.A. Late-day intraocular pressure-lowering efficacy and tolerability of travoprost 0.004% versus Bimatoprost 0.01% in patients with open-angle glaucoma or ocular hypertension: A randomized trial. BMC Ophthalmol. 2014, 14, 151. [Google Scholar] [CrossRef] [PubMed]
- Birt, C.M.; Buys, Y.M.; Ahmed, I.I.; Trope, G.E.; The Toronto Area Glaucoma Society. Prostaglandin efficacy and safety study undertaken by race (the PRESSURE study). J. Glaucoma 2010, 19, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Shiokawa, M.; Higa, R.; Sugahara, M.; Soga, T.; Wakakura, M.; Tomita, G. Adverse periocular reac-tions to five types of prostaglandin analogs. Eye 2012, 26, 1465–1472. [Google Scholar] [CrossRef]
- Kucukevcilioglu, M.; Bayer, A.; Uysal, Y.; Altinsoy, H.I. Prostaglandin associated periorbitopathy in patients using Bimatoprost, Latanoprost and travoprost. Clin. Exp. Ophthalmol. 2014, 42, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Itoh, K.; Hikage, F.; Ida, Y.; Ohguro, H. Prostaglandin F2alpha Agonists Negatively Modulate the Size of 3D Organ-oids from Primary Human Orbital Fibroblasts. Investig. Ophthalmol. Vis. Sci. 2020, 61, 13. [Google Scholar] [CrossRef]
- Patil, A.J.; Vajaranant, T.S.; Edward, D.P. Bimatoprost—A review. Expert Opin. Pharmacother. 2009, 10, 2759–2768. [Google Scholar] [CrossRef]
- Choi, H.Y.; Lee, J.E.; Lee, J.W.; Park, H.J.; Lee, J.E.; Jung, J.H. In vitro study of antiadipogenic profile of Lat-anoprost, travoprost, Bimatoprost, and tafluprost in human orbital preadiopocytes. J. Ocul. Pharmacol. Ther. 2012, 28, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Jamison, A.; Okafor, L.; Ullrich, K.; Schiedler, V.; Malhotra, R. Do Prostaglandin Analogue Lash Lengtheners Cause Eyelid Fat and Volume Loss? Aesthet. Surg. J. 2022, 42, 1241–1249. [Google Scholar] [CrossRef]
- Nakakura, S.; Terao, E.; Fujisawa, Y.; Tabuchi, H.; Kiuchi, Y. Changes in Prostaglandin-associated Periorbital Syndrome After Switch from Conventional Prostaglandin F2alpha Treatment to Omidenepag Isopropyl in 11 Consecutive Patients. J. Glaucoma 2020, 29, 326–328. [Google Scholar] [CrossRef] [PubMed]
- El-Khamery, A.A.; Mohamed, A.I.; Swify, H.E.; Mohamed, A.I. Cost-effectiveness of glaucoma management with monotherapy medications in Egypt. J. Adv. Pharm. Technol. Res. 2017, 8, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Lindsley, K.; Rouse, B.; Hong, H.; Shi, Q.; Friedman, D.S.; Wormald, R.; Dickersin, K. Comparative Effectiveness of First-Line Medications for Primary Open-Angle Glaucoma: A Systematic Review and Network Meta-analysis. Ophthalmology 2016, 123, 129–140. [Google Scholar] [CrossRef]
- Inoue, K.; Ishida, K.; Tomita, G.; Noma, H. A scoping review and network meta-analysis for efficacy and safety of glaucoma medication in Japanese patients. Jpn. J. Ophthalmol. 2020, 64, 103–113. [Google Scholar] [CrossRef]
- Priluck, A.Z.; Dietze, J. Ophthalmologist and Optometrist Glaucoma Prescribing Patterns Based on 2015 Medicare Part D Data. Ophthalmol. Glaucoma 2019, 2, 63–66. [Google Scholar] [CrossRef]
- Lazcano-Gomez, G.; Alvarez-Ascencio, D.; Haro-Zuno, C.; Turati-Acosta, M.; Garcia-Huerta, M.; Jimenez-Arroyo, J.; Castaneda-Diez, R.; Castillejos-Chevez, A.; Gonzalez-Salinas, R.; Dominguez-Duenas, F.; et al. Glaucoma Medication Preferences among Glaucoma Specialists in Mexico. J. Curr. Glaucoma Pract. 2017, 11, 97–100. [Google Scholar]
- Rennie, G.; Wilkinson, A.; White, A.; Ruospo, M.; Teixeira-Pinto, A.; Strippoli, G. Topical medical therapy and ocular perfusion pressure in open angle glaucoma: A systematic review and meta-analysis. Curr. Med. Res. Opin. 2019, 35, 1421–1431. [Google Scholar] [CrossRef]
- Stewart, W.C.; Konstas, A.G.; Kruft, B.; Mathis, H.M.; Stewart, J.A. Meta-analysis of 24-h intraocular pressure fluctuation studies and the efficacy of glaucoma medicines. J. Ocul. Pharmacol. Ther. 2010, 26, 175–180. [Google Scholar] [CrossRef]
- Huang, H.L.; Sun, X.H.; Xiao, M. Comparison of intraocular pressure reducing effects of three prostaglandin eye drops in open-angle glaucoma. Zhonghua Yan Ke Za Zhi 2011, 47, 109–113. [Google Scholar] [PubMed]
- Tamcelik, N.; Izgi, B.; Temel, A.; Yildirim, N.; Okka, M.; Ozcan, A.; Yuksel, N.; Elgin, U.; Altan, C.; Ozer, B. Prospective, non-interventional, multicenter study of the intraocular pressure-lowering effects of prostaglandin ana-log/prostamide-containing therapies in previously treated patients with open-angle glaucoma or ocular hypertension. Clin. Ophthalmol. 2017, 11, 723–731. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Lin, X.; Yu, M. Meta-analysis of randomized controlled trials comparing Latanoprost with other glaucoma medications in chronic angle-closure glaucoma. Eur. J. Ophthalmol. 2015, 25, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Curran, M.P. Bimatoprost: A review of its use in open-angle glaucoma and ocular hypertension. Drugs Aging 2009, 26, 1049–1071. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Lopez, A.; Paczka, J.A.; Jimenez-Roman, J.; Hartleben, C. Efficacy and tolerability of fixed-combination Bimatoprost/timolol versus fixed-combination dorzolamide/brimonidine/timolol in patients with primary open-angle glaucoma or ocular hypertension: A multicenter, prospective, crossover study. BMC Ophthalmol. 2014, 14, 161. [Google Scholar] [CrossRef] [PubMed]
- Brief, G.; Lammich, T.; Nagel, E.; Pfennigsdorf, S.; Spraul, C.W.; Ho, S. Fixed combination of Bimatoprost and timolol in patients with primary open-angle glaucoma or ocular hypertension with inadequate IOP adjustment. Clin. Ophthalmol. 2010, 4, 1125–1129. [Google Scholar] [CrossRef] [PubMed]
- Stankiewicz, A.; Misiuk-Hojlo, M.; Grabska-Liberek, I.; Romanowska-Dixon, B.; Wierzbowska, J.; Wasyluk, J.; Mulak, M.; Szuscik, I.; Sierdzinski, J.; Ehrlich, R.; et al. Intraocular pressure and ocular hemody-namics in patients with primary open-angle glaucoma treated with the combination of morning dosing of Bimatoprost and dorzolamide hydrochloride. Acta Ophthalmol. 2011, 89, e57–e63. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Wang, T.H.; Liu, C.; Wu, K.Y.; Chiu, S.L.; Simonyi, S.; Lu, D.W. Tolerability and efficacy of Bima-toprost 0.01% in patients with open-angle glaucoma or ocular hypertension evaluated in the Taiwanese clinical setting: The Asia Pacific Patterns from Early Access of Lumigan 0.01% (APPEAL Taiwan) study. BMC Ophthalmol. 2016, 16, 162. [Google Scholar] [CrossRef] [PubMed]
- Selen, F.; Tekeli, O.; Yanik, O. Assessment of the Anterior Chamber Flare and Macular Thickness in Patients Treated with Topical Antiglaucomatous Drugs. J. Ocul. Pharmacol. Ther. 2017, 33, 170–175. [Google Scholar] [CrossRef]
- Xing, Y.; Zhu, L.; Zhang, K.; Huang, S. The efficacy of the fixed combination of Latanoprost and timolol versus other fixed combinations for primary open-angle glaucoma and ocular hypertension: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0229682. [Google Scholar] [CrossRef]
- Guven Yilmaz, S.; Degirmenci, C.; Karakoyun, Y.E.; Yusifov, E.; Ates, H. The efficacy and safety of Bimato-prost/timolol maleate, Latanoprost/timolol maleate, and travoprost/timolol maleate fixed combinations on 24-h IOP. Int. Ophthalmol. 2018, 38, 1425–1431. [Google Scholar] [CrossRef] [PubMed]
- Rossetti, L.; Sacchi, M.; Karabatsas, C.H.; Topouzis, F.; Vetrugno, M.; Centofanti, M.; Boehm, A.; Vorwerk, C.; Goldblum, D.; Fogagnolo, P. Comparison of the effects of Bimatoprost and a fixed combination of Latanoprost and timolol on 24-hour blood and ocular perfusion pressures: The results of a randomized trial. BMC Ophthalmol. 2015, 15, 7. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.W.; Gan, L.Y.; Yao, X.; Zhou, J. Long-term assessment of prostaglandin analogs and timolol fixed combinations vs. prostaglandin analogs monotherapy. Int. J. Ophthalmol. 2016, 9, 750–756. [Google Scholar] [PubMed]
- Rotsos, T.G.; Kliafa, V.G.; Asher, K.J.; Papaconstantinou, D. Bimatoprost/timolol fixed combination (BTFC) in pa-tients with primary open angle glaucoma or ocular hypertension in Greece. Int. J. Ophthalmol. 2016, 9, 69–75. [Google Scholar] [PubMed]
- Choi, E.Y.; Johnson, N.A.; Stinnett, S.; Rosdahl, J.; Moya, F.; Herndon, L.W. The Effect of Bimatoprost Implant on Glaucoma Patients: An Observational Study. J. Glaucoma 2024. [Google Scholar] [CrossRef] [PubMed]
- Aptel, F.; Cucherat, M.; Denis, P. Efficacy and tolerability of prostaglandin-timolol fixed combinations: A meta-analysis of randomized clinical trials. Eur. J. Ophthalmol. 2012, 22, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, A.; Dastiridou, A.I.; Fanariotis, M.; Kotoula, M.; Tsironi, E.E. Bimatoprost and Bimatoprost/timolol fixed combination in patients with open-angle glaucoma and ocular hypertension. J. Ocul. Pharmacol. Ther. 2011, 27, 67–71. [Google Scholar] [CrossRef]
- Shim, S.H.; Kim, J.M.; Choi, C.Y.; Kim, C.Y. Diurnal intraocular pressure with Bimatoprost/timolol fixed combi-nation versus Latanoprost/timolol fixed combination in healthy subjects. Korean J. Ophthalmol. 2014, 28, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Ling, Z.; Sun, X. Fixed-combination treatments for intraocular hypertension in Chinese patients—Focus on Bimatoprost-timolol. Drug Des. Devel. Ther. 2015, 9, 2617–2625. [Google Scholar]
- Shin, D.H.; Feldman, R.M.; Sheu, W.P.; Fixed Combination Latanoprost/Timolol Study Group. Efficacy and safety of the fixed combinations Latanoprost/timolol versus dorzolamide/timolol in patients with elevated intraocular pressure. Ophthalmology 2004, 111, 276–282. [Google Scholar] [CrossRef]
- Calugaru, M.; Calugaru, D. The latest developments in glaucoma therapy using fixed combination products. Oftalmologia 2011, 55, 53–69. [Google Scholar] [PubMed]
- Ling, Z.; Zhang, M.; Hu, Y.; Yin, Z.; Xing, Y.; Fang, A.; Ye, J.; Chen, X.; Liu, D.; Wang, Y.; et al. Safety and efficacy of Bimatoprost/timolol fixed combination in Chinese patients with open-angle glaucoma or ocular hypertension. Chin. Med. J. 2014, 127, 905–910. [Google Scholar] [CrossRef]
- Mrukwa-Kominek, E.; Misiuk-Hojlo, M.; Csutak, A.; Stalmans, I.; Garhofer, G. A randomized clinical trial comparing three fixed combinations of Bimatoprost with timolol in patients with open-angle glaucoma or ocular hypertension. Curr. Med. Res. Opin. 2023, 39, 775–783. [Google Scholar] [CrossRef]
- Lequeu, I.; Theuwis, K.; Abegao Pinto, L.; Vandewalle, E.; Stalmans, I. Long term IOP lowering efficacy of Bimatoprost/timolol fixed combination: A 12 month prospective study. Bull. Soc. Belge. Ophtalmol. 2013, 322, 105–110. [Google Scholar]
- Konstas, A.G.; Haidich, A.B.; Rossetti, L.; Webers, C. Prostaglandin-timolol fixed combinations efficacy: Myth or reality? Eur. J. Ophthalmol. 2012, 22, 1–4. [Google Scholar] [CrossRef]
- Belfort, R., Jr.; Paula, J.S.; Lopes Silva, M.J.; Della Paolera, M.; Kim, T.; Chen, M.Y.; Goodkin, M.L. Fixed-combination Bimatoprost/Brimonidine/Timolol in Glaucoma: A Randomized, Masked, Controlled, Phase III Study Conducted in Brazil(☆). Clin. Ther. 2020, 42, 263–275. [Google Scholar] [CrossRef]
- Bourne, R.R.A.; Kaarniranta, K.; Lorenz, K.; Traverso, C.E.; Vuorinen, J.; Ropo, A. Changes in ocular signs and symptoms in patients switching from Bimatoprost-timolol to tafluprost-timolol eye drops: An open-label phase IV study. BMJ Open 2019, 9, e024129. [Google Scholar] [CrossRef]
- Nucci, C.; Varesi, C.; Martucci, A.; Cesareo, M.; Cedrone, C.; Mancino, R.; Cerulli, L. Efficacy of Timolol 0.1% Gel and a Prostaglandin Analog in an Unfixed Combination Compared to the Corresponding Fixed Combinations. Eur. J. Ophthalmol. 2013, 23, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Quaranta, L.; Biagioli, E.; Riva, I.; Rulli, E.; Poli, D.; Katsanos, A.; Floriani, I. Prostaglandin analogs and timolol-fixed versus unfixed combinations or monotherapy for open-angle glaucoma: A systematic review and meta-analysis. J. Ocul. Pharmacol. Ther. 2013, 29, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Lou, H.; Wang, H.; Zong, Y.; Cheng, J.W.; Wei, R.L. Efficacy and tolerability of prostaglandin-timolol fixed combinations: An updated systematic review and meta-analysis. Curr. Med. Res. Opin. 2015, 31, 1139–1147. [Google Scholar] [CrossRef]
- Maruyama, Y.; Ikeda, Y.; Mori, K.; Ueno, M.; Yoshikawa, H.; Kinoshita, S. Comparison between Bimatoprost and Latanoprost-timolol fixed combination for efficacy and safety after switching patients from Latanoprost. Clin. Ophthalmol. 2015, 9, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Lin, M.; Duan, X.; Zhang, C.; Ming, J. Patient satisfaction with fixed-combination Bimatoprost/timolol ophthalmic solution: A survey study in patients with glaucoma in China. Patient Prefer. Adherence 2017, 11, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Mesci, C.; Aydin, N.; Erbil, H.H. Twenty-four-hour intraocular pressure control with Latanoprost-timolol-fixed combination versus Bimatoprost in patients who switched from timolol. J. Glaucoma 2011, 20, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Konstas, A.G.; Hollo, G.; Mikropoulos, D.G.; Haidich, A.B.; Dimopoulos, A.T.; Empeslidis, T.; Teus, M.A.; Ritch, R. 24-hour efficacy of the Bimatoprost-timolol fixed combination versus Latanoprost as first choice therapy in subjects with high-pressure exfoliation syndrome and glaucoma. Br. J. Ophthalmol. 2013, 97, 857–861. [Google Scholar] [CrossRef]
- Gutierrez-Diaz, E.; Silva Cotta, J.; Munoz-Negrete, F.J.; Gutierrez-Ortiz, C.; Morgan-Warren, R.J.; Maltman, J. Bimatoprost/timolol fixed combination versus Latanoprost in treatment-naive glaucoma patients at high risk of progression: A pilot study. Clin. Ophthalmol. 2014, 8, 725–732. [Google Scholar] [CrossRef]
- Lee, M.Y.; Teh, N.C.; Nur Zulekha, M.; Thayanithi, S.; Jelinar, M.N.; Rizal, A.M.; Arfah, W. The Effects of Fixed Combination of Bimatoprost-Timolol and Travoprost-Timolol on Intraocular Pressure in Patients with Primary Open-Angle Glaucoma or Ocular Hypertension, Previously on Non-fixed Combination of Latanoprost and Timolol. Asia Pac. J. Ophthalmol. 2012, 1, 208–212. [Google Scholar] [CrossRef]
- Hommer, A. Combination therapy in the medical treatment of glaucoma. Klin. Monbl. Augenheilkd. 2013, 230, 133–140. [Google Scholar] [PubMed]
- Lipatov, D.V.; Chistiakov, T.A.; Kuz’min, A.G.; Tolkacheva, A.A. Evaluation of the effectiveness of Ganfort treatment in patients with secondary neovascular glaucoma associated with diabetes mellitus. Vestn. Oftalmol. 2014, 130, 45–48. [Google Scholar]
- Cordeiro, M.F.; Goldberg, I.; Schiffman, R.; Bernstein, P.; Bejanian, M. Efficacy of a preservative-free formulation of fixed-combination Bimatoprost and timolol (Ganfort PF) in treatment-naive patients vs. previously treated patients. Clin. Ophthalmol. 2015, 9, 1605–1611. [Google Scholar] [CrossRef]
- Takagi, Y.; Santo, K.; Hashimoto, M.; Fukuchi, T. Ocular hypotensive effects of prostaglandin analogs in Japanese patients with normal-tension glaucoma: A literature review. Clin. Ophthalmol. 2018, 12, 1837–1844. [Google Scholar] [CrossRef]
- Centofanti, M.; Oddone, F.; Gandolfi, S.; Hommer, A.; Boehm, A.; Tanga, L.; Sangermani, C.; Sportelli, V.; Haustein, M.; Manni, G.; et al. Comparison of Travoprost and Bimatoprost plus timolol fixed combinations in open-angle glaucoma patients previously treated with Latanoprost plus timolol fixed combination. Am. J. Ophthalmol. 2010, 150, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Macky, T.A. Bimatoprost/timolol versus travoprost/timolol fixed combinations in an Egyptian population: A hospi-tal-based prospective randomized study. J. Glaucoma 2014, 23, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Hartleben, C.; Parra, J.C.; Batoosingh, A.; Bernstein, P.; Goodkin, M. A Masked, Randomized, Phase 3 Comparison of Triple Fixed-Combination Bimatoprost/Brimonidine/Timolol versus Fixed-Combination Brimonidine/Timolol for Lowering Intraocular Pressure. J. Ophthalmol. 2017, 2017, 4586763. [Google Scholar] [CrossRef] [PubMed]
- Menon, M.G.; Goodkin, M.L. Triple Fixed-Combination Bimatoprost/Brimonidine/Timolol in Glaucoma and Ocular Hypertension in India: A Multicenter, Open-Label, Phase 3 Study. Clin. Ophthalmol. 2022, 16, 3559–3569. [Google Scholar] [CrossRef] [PubMed]
- Susanna, B.N.; Susanna, C.N.; Susanna, F.N.; Mota, R.T.; Barbosa, G.C.S.; Lima, V.L.; Susanna, R., Jr. Intraocular Peak Pressure in Patients Under Treatment with Fixed Combination of Bimatoprost/Timolol/Brimonidine Once Daily Versus Twice Daily. J. Glaucoma 2022, 31, e96–e100. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.W.; Cheng, S.W.; Gao, L.D.; Lu, G.C.; Wei, R.L. Intraocular pressure-lowering effects of commonly used fixed-combination drugs with timolol: A systematic review and meta-analysis. PLoS ONE 2012, 7, e45079. [Google Scholar] [CrossRef]
- Shen, J.; Bejanian, M. Effect of preservative removal from fixed-combination Bimatoprost/timolol on intraocular pres-sure lowering: A potential timolol dose-response phenomenon. Clin. Ophthalmol. 2016, 10, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Kim, Y.H.; Kang, S.H.; Lee, K.W.; Park, Y.J. In vitro effects of preservative-free and preserved prosta-glandin analogs on primary cultured human conjunctival fibroblast cells. Korean J. Ophthalmol. 2013, 27, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Schnober, D.; Hubatsch, D.A.; Scherzer, M.L. Efficacy and safety of fixed-combination travoprost 0.004%/timolol 0.5% in patients transitioning from Bimatoprost 0.03%/timolol 0.5% combination therapy. Clin. Ophthalmol. 2015, 9, 825–832. [Google Scholar] [CrossRef]
- Imasawa, M.; Tanabe, J.; Kashiwagi, F.; Kashiwagi, K. Efficacy and Safety of Switching Latanoprost Monotherapy to Bimatoprost Monotherapy or Combination of Brinzolamide and Latanoprost. Open Ophthalmol. J. 2016, 10, 94–102. [Google Scholar] [CrossRef]
- Paranhos, A.; Mendonca, M.; Silva, M.J.; Giampani, J.; Torres, R.J.; Della Paolera, M.; Russ, H.; Lottenberg, C.L. Hyperemia reduction after administration of a fixed combination of Bimatoprost and timolol maleate to patients on prostaglandin or prostamide monotherapy. J. Ocul. Pharmacol. Ther. 2010, 26, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Scherzer, M.L.; Liehneova, I.; Negrete, F.J.; Schnober, D. Travoprost 0.004%/timolol 0.5% fixed combination in patients transitioning from fixed or unfixed Bimatoprost 0.03%/timolol 0.5%. Adv. Ther. 2011, 28, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Jothi, R.; Ismail, A.M.; Senthamarai, R.; Pal, S. A comparative study on the efficacy, safety, and cost-effectiveness of Bimatoprost/timolol and dorzolamide/timolol combinations in glaucoma patients. Indian J. Pharmacol. 2010, 42, 362–365. [Google Scholar] [PubMed]
- Soto, J.; Diaz, S. Does the fixed combination of Bimatoprost/timolol really produce a better benefit/risk balance than the fixed combination of Latanoprost/timolol? Eur. J. Ophthalmol. 2010, 20, 246–247, author reply 247-8. [Google Scholar] [CrossRef] [PubMed]
- Sacchi, M.; Specchia, C.; Williams, S.E.; Villani, E.; Nucci, P. Efficacy of Bimatoprost Plus Timolol Fixed Combina tion in Open Angle Glaucoma Patients Previously Treated with Dorzolamide Plus Timolol Fixed Combination. Curr. Eye Res. 2016, 41, 1433–1437. [Google Scholar] [CrossRef]
- Pfennigsdorf, S.; de Jong, L.; Makk, S.; Fournichot, Y.; Bron, A.; Morgan-Warren, R.J.; Maltman, J. A combined analysis of five observational studies evaluating the efficacy and tolerability of Bimatoprost/timolol fixed combination in patients with primary open-angle glaucoma or ocular hypertension. Clin. Ophthalmol. 2013, 7, 1219–1225. [Google Scholar] [CrossRef] [PubMed]
- Aptel, F.; Denis, P. Balancing efficacy and tolerability of prostaglandin analogues and prostaglandin-timolol fixed combinations in primary open-angle glaucoma. Curr. Med. Res. Opin. 2011, 27, 1949–1958. [Google Scholar] [CrossRef]
- Russ, H.H.; Nogueira-Filho, P.A.; Barros, J.N.; Faria, N.V.; Montiani-Ferreira, F.; Gomes, J.A.; Mello, P.A. Ocular surface evaluation in patients treated with a fixed combination of prostaglandin analogues with 0.5% timolol maleate topical monotherapy: A randomized clinical trial. Clinics 2013, 68, 1318–1324. [Google Scholar] [CrossRef]
- Day, D.G.; Sharpe, E.D.; Beischel, C.J.; Jenkins, J.N.; Stewart, J.A.; Stewart, W.C. Safety and efficacy of Bimato-prost 0.03% versus timolol maleate 0.5%/dorzolamide 2% fixed combination. Eur. J. Ophthalmol. 2005, 15, 336–342. [Google Scholar] [CrossRef]
- Lafuma, A.; Salmon, J.F.; Robert, J.; Berdeaux, G. Treatment persistence and cost-effectiveness of Latano-prost/Latanoprost-timolol, Bimatoprost/Bimatoprost-timolol, and travoprost/travoprost-timolol in glaucoma: An analysis based on the United Kingdom general practitioner research database. Clin. Ophthalmol. 2011, 5, 361–367. [Google Scholar]
- Xu, C.; Guo, R.; Huang, D.; Ji, J.; Liu, W. Daily Costs and Cost Effectiveness of Glaucoma Fixed Combinations in China. J. Ophthalmol. 2020, 2020, 2406783. [Google Scholar] [CrossRef] [PubMed]
- Kosakyan, S.M.; Robustova, O.V.; Bessmertny, A.M.; Kalinina, O.M.; Vasilenkova, L.V. Effectiveness and safety of drug combination therapy in patients with advanced primary open-angle glaucoma. Vestn. Oftalmol. 2020, 136, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Sumi, T.; Yoneda, T.; Fukuda, K.; Hoshikawa, Y.; Kobayashi, M.; Yanagi, M.; Kiuchi, Y.; Yasumitsu-Lovell, K.; Fukushima, A. Development of automated conjunctival hyperemia analysis software. Cornea 2013, 32 (Suppl. S1), S52-9. [Google Scholar] [CrossRef] [PubMed]
- Kymes, S.M.; Burk, C.; Feinman, T.; Williams, J.M.; Hollander, D.A. Demonstration of an online tool to assist managed care formulary evidence-based decision making: Meta-analysis of topical prostaglandin analog efficacy. Ther. Clin. Risk Manag. 2011, 7, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Vu, J.T.; Hong, B.; Gottlieb, C. Uveitis and cystoid macular oedema secondary to topical prostaglandin analogue use in ocular hypertension and open angle glaucoma. Br. J. Ophthalmol. 2020, 104, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Holmstrom, S.; Buchholz, P.; Walt, J.; Wickstrom, J.; Aagren, M. Analytic review of bimatoprost, latanoprost and travoprost in primary open angle glaucoma. Curr. Med. Res. Opin. 2005, 21, 1875–1883. [Google Scholar] [CrossRef]
- Denis, P.; Lafuma, A.; Khoshnood, B.; Mimaud, V.; Berdeaux, G. A meta-analysis of topical prostaglandin analogues intra-ocular pressure lowering in glaucoma therapy. Curr. Med. Res. Opin. 2007, 23, 601–608. [Google Scholar] [CrossRef]
- Noecker, R.J.; Earl, M.L.; Mundorf, T.; Peace, J.; Williams, R.D. Bimatoprost 0.03% versus travoprost 0.004% in black Americans with glaucoma or ocular hypertension. Adv. Ther. 2003, 20, 121–128. [Google Scholar] [CrossRef]
- Noecker, R.S.; Dirks, M.S.; Choplin, N.T.; Bernstein, P.; Batoosingh, A.L.; Whitcup, S.M.; Bimatoprost/Latanoprost Study, G. A six-month randomized clinical trial comparing the intraocular pressure-lowering efficacy of bimatoprost and latanoprost in patients with ocular hypertension or glaucoma. Am. J. Ophthalmol. 2003, 135, 55–63. [Google Scholar] [CrossRef]
- Parrish, R.K.; Palmberg, P.; Sheu, W.P.; Group, X.L.T.S. A comparison of latanoprost, bimatoprost, and travoprost in patients with elevated intraocular pressure: A 12-week, randomized, masked-evaluator multicenter study. Am. J. Ophthalmol. 2003, 135, 688–703. [Google Scholar] [CrossRef]
- Cantor, L.B.; WuDunn, D.; Cortes, A.; Hoop, J.; Knotts, S. Ocular hypotensive efficacy of bimatoprost 0.03% and travoprost 0.004% in patients with glaucoma or ocular hypertension. Surv. Ophthalmol. 2004, 49 (Suppl. S1), S12–S18. [Google Scholar] [CrossRef] [PubMed]
- Sakai, T.; Mori, C.; Koshiba, H.; Yuminaga, R.; Tanabe, K.; Ohtsu, F. Pregnancy Loss Signal from Prostaglandin Eye Drop Use in Pregnancy: A Disproportionality Analysis Using Japanese and US Spontaneous Reporting Databases. Drugs-Real World Outcomes 2022, 9, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Tanito, M.; Ishida, A.; Ichioka, S.; Takayanagi, Y.; Tsutsui, A.; Manabe, K.; Shirakami, T.; Sugihara, K.; Matsuo, M. Proposal of a simple grading system integrating cosmetic and tonometric aspects of prostaglandin-associated periorbitopathy. Medicine 2021, 100, e26874. [Google Scholar] [CrossRef]
- Hikage, F.; Ida, Y.; Ouchi, Y.; Watanabe, M.; Ohguro, H. Omidenepag, a Selective, Prostanoid EP2 Agonist, Does Not Suppress Adipogenesis in 3D Organoids of Human Orbital Fibroblasts. Transl. Vis. Sci. Technol. 2021, 10, 6. [Google Scholar] [CrossRef] [PubMed]
- Patradul, C.; Tantisevi, V.; Manassakorn, A. Factors Related to Prostaglandin-Associated Periorbitopathy in Glaucoma Patients. Asia Pac. J. Ophthalmol. 2017, 6, 238–242. [Google Scholar]
- Sarnoff, D.S.; Gotkin, R.H. Bimatoprost-induced chemical blepharoplasty. J. Drugs Dermatol. 2015, 14, 472–477. [Google Scholar]
- Ida, Y.; Watanabe, M.; Umetsu, A.; Ohguro, H.; Hikage, F. Addition of EP2 agonists to an FP agonist additively and synergistically modulates adipogenesis and the physical properties of 3D 3T3-L1 sphenoids. Prostaglandins Leukot. Essent. Fatty Acids 2021, 171, 102315. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Cao, M.; Liu, K.; Duan, X. Analysis of the Responsiveness of Latanoprost, Travoprost, Bimatoprost, and Tafluprost in the Treatment of OAG/OHT Patients. J. Ophthalmol. 2021, 2021, 5586719. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Robinson, M.R.; Weinreb, R.N. Episcleral Venous Pressure and the Ocular Hypotensive Effects of Topical and Intracameral Prostaglandin Analogs. J. Glaucoma 2019, 28, 846–857. [Google Scholar] [CrossRef]
- Kaliaperumal, S.; Govindaraj, I.; Kopparapu, P.K.; Ahuja, S. Hirsutism following the use of Bimatoprost eyedrops for glaucoma. J. Pharmacol. Pharmacother. 2014, 5, 208–210. [Google Scholar] [CrossRef]
- Sano, I.; Takahashi, H.; Inoda, S.; Sakamoto, S.; Arai, Y.; Takahashi, Y.; Ohkubo, A.; Kawashima, H.; Mayama, C. Shortening of Interpupillary Distance after Instillation of Topical Prostaglandin Analog Eye Drops. Am. J. Ophthalmol. 2019, 206, 11–16. [Google Scholar] [CrossRef]
- Hutchison, D.M.; Duffens, A.; Yale, K.; Park, A.; Cardenas, K.; Mesinkovska, N.A. Eyelash trichomegaly: A systematic review of acquired and congenital aetiologies of lengthened lashes. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 536–546. [Google Scholar] [CrossRef]
- Skorin, L., Jr.; Dailey, K.H. Clicking Eyelids: A New Finding of Prostaglandin-Associated Periorbitopathy. Optom. Vis. Sci. 2016, 93, 779–781. [Google Scholar] [CrossRef]
- Karslioglu, M.Z.; Hosal, M.B.; Tekeli, O. Periocular changes in topical Bimatoprost and Latanoprost use. Turk. J. Med. Sci. 2015, 45, 925–930. [Google Scholar] [CrossRef]
- Deveau, A.P.; da Silva, F.N.; Ly, T.Y.; Hussain, A. Periocular invasive melanoma manifestation in a patient using Bimatoprost: Case report and literature review. Orbit 2023, 42, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Kent, T.L.; Custer, P.L. Structural and Histologic Eyelid Changes Associated with 6 Months of Topical Bimatoprost in the Rabbit. J. Glaucoma 2017, 26, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Noma, K.; Kakizaki, H. Bilateral upper eyelid retraction caused by topical Bimatoprost therapy. Ophthalmic Plast. Reconstr. Surg. 2012, 28, e33-5. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W.; Choi, Y.J.; Lee, K.W.; Lee, M.J. Periorbital changes associated with prostaglandin analogs in Korean patients. BMC Ophthalmol. 2017, 17, 126. [Google Scholar] [CrossRef]
- Jbara, D.; Eiger-Moscovich, M.; Didkovsky, E.; Keshet, Y.; Avisar, I. In Vivo Effects of Prostaglandin Analogues Application by Topical Drops or Retrobulbar Injections on the Orbital Fat of a Rat Model. Ocul. Immunol. Inflamm. 2023, 31, 298–303. [Google Scholar] [CrossRef]
- Rabinowitz, M.P.; Katz, L.J.; Moster, M.R.; Myers, J.S.; Pro, M.J.; Spaeth, G.L.; Sharma, P.; Stefanyszyn, M.A. Unilateral Prostaglandin-Associated Periorbitopathy: A Syndrome Involving Upper Eyelid Retraction Distinguishable from the Aging Sunken Eyelid. Ophthalmic Plast. Reconstr. Surg. 2015, 31, 373–378. [Google Scholar] [CrossRef]
- Higashiyama, T.; Minamikawa, T.; Kakinoki, M.; Sawada, O.; Ohji, M. Decreased orbital fat and enophthalmos due to Bimatoprost: Quantitative analysis using magnetic resonance imaging. PLoS ONE 2019, 14, e0214065. [Google Scholar] [CrossRef] [PubMed]
- Eftekhari, K.; Vagefi, M.R.; Lee, V.; Hui, J.Z.; Zhu, M.; Dine, K.; Anderson, R.L.; Koeberlein, B.; Sulaimankutty, R.; Shindler, K.S. In Vivo Effects of Retrobulbar Bimatoprost Injection on Orbital Fat. Ophthalmic Plast. Reconstr. Surg. 2018, 34, 201–204. [Google Scholar] [CrossRef]
- Taketani, Y.; Yamagishi, R.; Fujishiro, T.; Igarashi, M.; Sakata, R.; Aihara, M. Activation of the prostanoid FP receptor inhibits adipogenesis leading to deepening of the upper eyelid sulcus in prostaglandin-associated periorbitopathy. Investig. Ophthalmol. Vis. Sci. 2014, 55, 1269–1276. [Google Scholar] [CrossRef]
- Ida, Y.; Hikage, F.; Itoh, K.; Ida, H.; Ohguro, H. Prostaglandin F2alpha agonist-induced suppression of 3T3-L1 cell adipogenesis affects spatial formation of extra-cellular matrix. Sci. Rep. 2020, 10, 7958. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Berke, S. Latanoprost-induced prostaglandin-associated periorbitopathy. Optom. Vis. Sci. 2013, 90, e245–e247. [Google Scholar] [CrossRef]
- Wang, P.X.; Koh, V.T.; Cheng, J.F. Periorbital muscle atrophy associated with topical Bimatoprost therapy. Clin. Ophthalmol. 2014, 8, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Priluck, J.C.; Fu, S. Latisse-induced periocular skin hyperpigmentation. Arch. Ophthalmol. 2010, 128, 792–793. [Google Scholar] [CrossRef]
- Lewis, R.A.; Gross, R.L.; Sall, K.N.; Schiffman, R.M.; Liu, C.C.; Batoosingh, A.L.; Ganfort Investigators, G., II. The safety and efficacy of Bimatoprost/timolol fixed combination: A 1-year double-masked, randomized parallel comparison to its individual components in patients with glaucoma or ocular hypertension. J. Glaucoma 2010, 19, 424–426. [Google Scholar] [CrossRef]
- Park, K.H.; Simonyi, S.; Kim, C.Y.; Sohn, Y.H.; Kook, M.S. Bimatoprost 0.01% in treatment-naive patients with open-angle glaucoma or ocular hypertension: An observational study in the Korean clinical setting. BMC Ophthalmol. 2014, 14, 160. [Google Scholar] [CrossRef]
- Sun, X.; Yao, K.; Liu, Q.; Zhang, H.; Xing, X.; Fang, A.; Duan, X.; Yu, M.; Chen, M.Y.; Yang, J.; et al. Safety of Fixed-Combination Bimatoprost 0.03%/Timolol 0.5% Ophthalmic Solution at 6 Months in Chinese Patients with Open-Angle Glaucoma or Ocular Hypertension. Ophthalmol. Ther. 2023, 12, 341–353. [Google Scholar] [CrossRef]
- Aydin, S.; Isikligil, I.; Teksen, Y.A.; Kir, E. Recovery of orbital fat pad prolapsus and deepening of the lid sulcus from topical Bimatoprost therapy: 2 case reports and review of the literature. Cutan. Ocul. Toxicol. 2010, 29, 212–216. [Google Scholar] [CrossRef]
- Jayaprakasam, A.; Ghazi-Nouri, S. Periorbital fat atrophy—An unfamiliar side effect of prostaglandin analogues. Orbit 2010, 29, 357–359. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Cho, H.K.; Moon, J.I. Changes to upper eyelid orbital fat from use of topical Bimatoprost, travoprost, and Latanoprost. Jpn. J. Ophthalmol. 2011, 55, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.; Sahay, P.; Padhy, D.; Sarangi, S.; Suar, M.; Modak, R.; Rao, A. Tear biomarkers in Latanoprost and Bimatoprost treated eyes. PLoS ONE 2018, 13, e0201740. [Google Scholar] [CrossRef] [PubMed]
- Ulas, F.; Balbaba, M.; Celebi, S. Effect of prophylactic intraocular pressure-lowering medication on pain during cataract surgery. J. Ocul. Pharmacol. Ther. 2013, 29, 658–662. [Google Scholar] [CrossRef]
- Bafa, M.; Georgopoulos, G.; Mihas, C.; Stavrakas, P.; Papaconstantinou, D.; Vergados, I. The effect of prostaglandin analogues on central corneal thickness of patients with chronic open-angle glaucoma: A 2-year study on 129 eyes. Acta Ophthalmol. 2011, 89, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Shen, X.; Yu, J.; Tan, H.; Cheng, Y. The comparison of the effects of Latanoprost, travoprost, and Bimatoprost on central corneal thickness. Cornea 2011, 30, 861–864. [Google Scholar] [CrossRef] [PubMed]
- Eraslan, N.; Celikay, O. Effects of topical prostaglandin therapy on corneal layers thickness in primary open-angle glaucoma patients using anterior segment optical coherence tomography. Int. Ophthalmol. 2023, 43, 3175–3184. [Google Scholar] [CrossRef]
- Kim, J.Y.; Yim, H.W. Effect of Topical Prostaglandin Analogue Therapy on Central Corneal Thickness: A Systematic Review. J. Clin. Med. 2022, 12, 44. [Google Scholar] [CrossRef]
- Wu, J.H.; Wang, T.H.; Huang, J.Y.; Su, C.C. Ocular Surface Disease in Glaucoma Patients Randomized to Benzalkonium Chloride-Containing Latanoprost and Preservative-Free Bimatoprost. J. Ocul. Pharmacol. Ther. 2021, 37, 556–564. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, Y.; Yu, A.; Wu, J.; Zhu, M.; Jiang, M.; Li, X.; Zhu, D.; Zhang, P.; Zheng, X.; et al. Effect of travoprost, Latanoprost and Bimatoprost PGF2alpha treatments on the biomechanical properties of in-vivo rabbit cornea. Exp. Eye Res. 2022, 215, 108920. [Google Scholar] [CrossRef] [PubMed]
- Eraslan, N.; Ekici, E.; Celikay, O. The effect of topical Bimatoprost on corneal clarity in primary open-angle glaucoma: A longitudinal prospective assessment. Int. Ophthalmol. 2022, 42, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Tong, L.; Matsuura, E.; Takahashi, M.; Nagano, T.; Kawazu, K. Effects of Anti-Glaucoma Prostaglandin Ophthalmic Solutions on Cultured Human Corneal Epithelial Cells. Curr. Eye Res. 2019, 44, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Pozarowska, D.; Pozarowski, P.; Darzynkiewicz, Z. Cytometric assessment of cytostatic and cytotoxic effects of topical glaucoma medications on human epithelial corneal line cells. Cytometry B Clin. Cytom. 2010, 78, 130–137. [Google Scholar] [CrossRef]
- Padhy, D.; Rao, A. Bimatoprost (0.03%)-induced accommodative spasm and pseudomyopia. BMJ Case Rep. 2015, 2015, bcr2015211820. [Google Scholar]
- Agange, N.; Mosaed, S. Prostaglandin-induced cystoid macular edema following routine cataract extraction. J. Ophthalmol. 2010, 2010, 690707. [Google Scholar] [CrossRef] [PubMed]
- Wendel, C.; Zakrzewski, H.; Carleton, B.; Etminan, M.; Mikelberg, F.S. Association of Postoperative Topical Prostaglandin Analog or Beta-Blocker Use and Incidence of Pseudophakic Cystoid Macular Edema. J. Glaucoma 2018, 27, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.H.; Badar, A.; Bakhsh, S.; Jusufbegovic, D. Bilateral Cystoid Macular Edema Following Bimatoprost Implants. Retin. Cases Brief. Rep. 2022, 18, 218–220. [Google Scholar] [CrossRef] [PubMed]
- Moschos, M.M.; Nitoda, E.; Chatziralli, I.P.; Panos, G.D.; Demopoulos, C.A. Impact of prostaglandin glaucoma drops on platelet-activating factor action: An in vitro study. Drug Des. Devel Ther. 2016, 10, 3977–3981. [Google Scholar] [CrossRef] [PubMed]
- Addison, P.K.; Papadopoulos, M.; Nischal, K.K.; Hykin, P.G. Serous retinal detachment induced by topical Bimatoprost in a patient with Sturge-Weber syndrome. Eye 2011, 25, 124–125. [Google Scholar] [CrossRef]
- Ogundele, A.B.; Li, G.; Ellis, J.J. Impact of topical Bimatoprost 0.01% and Bimatoprost 0.03% on conjunctival irritation in rabbits. Clin. Ophthalmol. 2010, 4, 77–80. [Google Scholar] [CrossRef]
- Nakakura, S.; Noguchi, A.; Tabuchi, H.; Kiuchi, Y. Bimatoprost-induced late-onset choroidal detachment after trabeculectomy: A case report and review of the literature. Medicine 2017, 96, e5927. [Google Scholar] [CrossRef]
- Akyol, N.; Kalkisim, A.; Turk, A.; Kola, M.; Imamoglu, H.I. Evaluation of the effects on choroidal thickness of Bimatoprost 0.03% versus a brinzolamide 1.0%/timolol maleate 0.5% fixed combination. Cutan. Ocul. Toxicol. 2017, 36, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.A.; Kim, N.W.; Kang, S.S.; Kim, M.L.; Sung, K.R. In vitro Effects of Prostaglandin Analogs on Cultured Astrocytes Obtained from the Lamina Cribrosa. Curr. Eye Res. 2016, 41, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Ogundele, A.B.; Earnest, D.; McLaughlin, M.A. In vivo comparative study of ocular vasodilation, a relative indicator of hyperemia, in guinea pigs following treatment with Bimatoprost ophthalmic solutions 0.01% and 0.03%. Clin. Ophthalmol. 2010, 4, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Pauly, A.; Riancho, L.; Baudouin, C.; Brignole-Baudouin, F. Toxicological evaluation of preservative-containing and preservative-free topical prostaglandin analogues on a three-dimensional-reconstituted corneal epithelium system. Br. J. Ophthalmol. 2011, 95, 869–875. [Google Scholar] [CrossRef]
- Barabino, S.; Antonelli, S.; Cimbolini, N.; Mauro, V.; Bouzin, M. The effect of preservatives and antiglaucoma treatments on the ocular surface of mice with dry eye. Investig. Ophthalmol. Vis. Sci. 2014, 55, 6499–6504. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, E.J.; Kim, Y.H.; Kim, Y.I.; Lee, S.H.; Jung, J.C.; Lee, K.W.; Park, Y.J. In Vivo Effects of Preservative-free and Preserved Prostaglandin Analogs: Mouse Ocular Surface Study. Korean J. Ophthalmol. 2015, 29, 270–279. [Google Scholar] [CrossRef]
- Liang, H.; Baudouin, C.; Daull, P.; Garrigue, J.S.; Brignole-Baudouin, F. In Vitro Corneal and Conjunctival Wound-Healing Assays as a Tool for Antiglaucoma Prostaglandin Formulation Characterization. Front. Biosci. (Landmark Ed) 2022, 27, 147. [Google Scholar] [CrossRef] [PubMed]
- Nakakura, S.; Tabuchi, H.; Kiuchi, Y. Latanoprost therapy after sunken eyes caused by travoprost or Bimatoprost. Optom. Vis. Sci. 2011, 88, 1140–1144. [Google Scholar] [CrossRef]
- Altieri, M.; Ferrari, E. Do prostaglandin analogs affect eyelid position and motility? J. Ocul. Pharmacol. Ther. 2011, 27, 511–517. [Google Scholar] [CrossRef]
- Radcliffe, N.M. The impact of timolol maleate on the ocular tolerability of fixed-combination glaucoma therapies. Clin. Ophthalmol. 2014, 8, 2541–2549. [Google Scholar] [CrossRef] [PubMed]
- Hikage, F.; Ichioka, H.; Watanabe, M.; Umetsu, A.; Ohguro, H.; Ida, Y. Addition of ROCK inhibitors to prostaglandin derivative (PG) synergistically affects adipogenesis of the 3D spheroids of human orbital fibroblasts (HOFs). Hum. Cell 2022, 35, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Ida, Y.; Sato, T.; Umetsu, A.; Watanabe, M.; Furuhashi, M.; Hikage, F.; Ohguro, H. Addition of ROCK Inhibitors Alleviates Prostaglandin-Induced Inhibition of Adipogenesis in 3T3L-1 Spheroids. Bioengineering 2022, 9, 702. [Google Scholar] [CrossRef] [PubMed]
- Agnifili, L.; Mastropasqua, R.; Fasanella, V.; Brescia, L.; Scatena, B.; Oddone, F.; Mastropasqua, L. Meibomian Gland Features and Conjunctival Goblet Cell Density in Glaucomatous Patients Controlled with Prostaglandin/Timolol Fixed Combinations: A Case Control, Cross-sectional Study. J. Glaucoma 2018, 27, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Pfennigsdorf, S.; Eschstruth, P.; Hasemeyer, S.; Feuerhake, C.; Brief, G.; Grobeiu, I.; Shirlaw, A. Preservative-free Bimatoprost 0.03%/timolol 0.5% fixed combination in patients with glaucoma in clinical practice. Clin. Ophthalmol. 2016, 10, 1837–1846. [Google Scholar] [CrossRef] [PubMed]
- Pillunat, L.E.; Eschstruth, P.; Hasemeyer, S.; Thelen, U.; Foja, C.; Leaback, R.; Pfennigsdorf, S. Preservative-free Bimatoprost 0.03% in patients with primary open-angle glaucoma or ocular hypertension in clinical practice. Clin. Ophthalmol. 2016, 10, 1759–1765. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Shiokawa, M.; Sugahara, M.; Higa, R.; Wakakura, M.; Tomita, G. Iris and periocular adverse reactions to Bimatoprost in Japanese patients with glaucoma or ocular hypertension. Clin. Ophthalmol. 2012, 6, 111–116. [Google Scholar] [CrossRef]
- Wirta, D.; Vandenburgh, A.M.; Weng, E.; Whitcup, S.M.; Kurstjens, S.; Beddingfield, F.C., 3rd. Long-term safety evaluation of Bimatoprost ophthalmic solution 0.03%: A pooled analysis of six double-masked, randomized, active-controlled clinical trials. Clin. Ophthalmol. 2011, 5, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Higginbotham, E.J.; Schuman, J.S.; Goldberg, I.; Gross, R.L.; VanDenburgh, A.M.; Chen, K.; Whitcup, S.M. One-year, randomized study comparing Bimatoprost and timolol in glaucoma and ocular hypertension. Arch. Ophthalmol. 2002, 120, 1286–1293. [Google Scholar] [CrossRef]
- de Faria, N.V.; Russ, H.H.; Rose, P.; Noronha, L.; Mello, P.A.; Montiani-Ferreira, F.; Sobrinho, S.C. Conjunctival changes and inflammatory aspects in rabbits’ conjunctivas induced by fixed combinations of prostaglandin analogues and timolol maleate. J. Ophthalmic Inflamm. Infect. 2013, 3, 22. [Google Scholar] [CrossRef]
- Trzeciecka, A.; Paterno, J.J.; Toropainen, E.; Koskela, A.; Podracka, L.; Korhonen, E.; Kauppinen, A.; Kaarniranta, K.; Smedowski, A. Long-term topical application of preservative-free prostaglandin analogues evokes macrophage infiltration in the ocular adnexa. Eur. J. Pharmacol. 2016, 788, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, M.; Shibata, S.; Shibata, N.; Hagihara, K.; Yaguchi, H.; Osada, H.; Takahashi, N.; Kubo, E.; Sasaki, H. Safety comparison of additives in antiglaucoma prostaglandin (PG) analog ophthalmic formulations. Clin. Ophthalmol. 2013, 7, 515–520. [Google Scholar] [CrossRef]
- Whitson, J.T.; Petroll, W.M. Corneal epithelial cell viability following exposure to ophthalmic solutions containing preservatives and/or antihypertensive agents. Adv. Ther. 2012, 29, 874–888. [Google Scholar]
- Liang, H.; Baudouin, C.; Labbe, A.; Riancho, L.; Brignole-Baudouin, F. Conjunctiva-associated lymphoid tissue (CALT) reactions to antiglaucoma prostaglandins with or without BAK-preservative in rabbit acute toxicity study. PLoS ONE 2012, 7, e33913. [Google Scholar] [CrossRef] [PubMed]
- Ayaki, M.; Iwasawa, A.; Niwano, Y. Cell viability score as an integrated indicator for cytotoxicity of benzalkonium chloride-containing antiglaucoma eyedrops. Biocontrol Sci. 2012, 17, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Seibold, L.K.; Ammar, D.A.; Kahook, M.Y. Acute effects of glaucoma medications and benzalkonium chloride on pre-adipocyte proliferation and adipocyte cytotoxicity in vitro. Curr. Eye Res. 2013, 38, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, H.; Yunoki, T.; Tojo, N.; Hayashi, A. Effectiveness of Blepharoptosis Surgery in Patients with Deepening of the Upper Eyelid Sulcus. J. Craniofac Surg. 2020, 31, 1284–1286. [Google Scholar] [CrossRef] [PubMed]
- Yamada, H.; Yoneda, M.; Gosho, M.; Kato, T.; Zako, M. Bimatoprost, Latanoprost, and tafluprost induce differential expression of matrix metalloproteinases and tissue inhibitor of metalloproteinases. BMC Ophthalmol. 2016, 16, 26. [Google Scholar] [CrossRef] [PubMed]
- Cheggour, M.; Gambrelle, J. Massive choroidal detachment secondary to topical use of Bimatoprost: Report of two cases. J. Fr. Ophtalmol. 2012, 35, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; Turnbull, C.; Akhtar, M.M.; Fleet, J. Ganfort, a blinding drug to the physician. BMJ Case Rep. 2012, 2012, bcr0120125648. [Google Scholar] [CrossRef]
- Miki, T.; Naito, T.; Fujiwara, M.; Araki, R.; Kiyoi, R.; Shiode, Y.; Fujiwara, A.; Morizane, Y.; Shiraga, F. Effects of pre-surgical administration of prostaglandin analogs on the outcome of trabeculectomy. PLoS ONE 2017, 12, e0181550. [Google Scholar] [CrossRef]
- Rodriguez-Agramonte, F.; Jimenez, J.C.; Montes, J.R. Periorbital Changes associated with Topical Prostaglandins Analogues in a Hispanic Population. P. R. Health Sci. J. 2017, 36, 218–222. [Google Scholar] [PubMed]
- Subedi, L.; Pandey, P.; Shim, J.H.; Kim, K.T.; Cho, S.S.; Koo, K.T.; Kim, B.J.; Park, J.W. Preparation of topical Bimatoprost with enhanced skin infiltration and in vivo hair regrowth efficacy in androgenic alopecia. Drug Deliv. 2022, 29, 328–341. [Google Scholar] [CrossRef]
- Manabe, M.; Tsuboi, R.; Itami, S.; Osada, S.I.; Amoh, Y.; Ito, T.; Inui, S.; Ueki, R.; Ohyama, M.; Kurata, S.; et al. Guidelines for the diagnosis and treatment of male-pattern and female-pattern hair loss, 2017 version. J. Dermatol. 2018, 45, 1031–1043. [Google Scholar] [CrossRef] [PubMed]
- Boubertakh, B.; Courtemanche, O.; Marsolais, D.; Di Marzo, V.; Silvestri, C. New role for the anandamide metabolite prostaglandin F(2alpha) ethanolamide: Rolling preadipocyte proliferation. J. Lipid Res. 2023, 64, 100444. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.; Evans, K.; North, R.V.; Jones, L.; Purslow, C. Impact of Eye Cosmetics on the Eye, Adnexa, and Ocular Surface. Eye Contact Lens 2016, 42, 211–220. [Google Scholar] [CrossRef] [PubMed]
- De Gregorio, A.; Pedrotti, E.; Stevan, G.; Scala, A.; Lambiase, A.; Morselli, S. Floppy eyelid syndrome and ectropion improvement after 1 month of 0.03% Bimatoprost topical therapy. Am. J. Ophthalmol. Case Rep. 2020, 20, 100938. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Hao, Z.; Qi, W.; Wang, Z.; Zhou, M.; Guo, N. The efficacy of topical prostaglandin analogs for hair loss: A systematic review and meta-analysis. Front. Med. 2023, 10, 1130623. [Google Scholar] [CrossRef] [PubMed]
- Ocampo-Garza, J.; Griggs, J.; Tosti, A. New drugs under investigation for the treatment of alopecias. Expert. Opin. Investig. Drugs 2019, 28, 275–284. [Google Scholar] [CrossRef]
- Barron-Hernandez, Y.L.; Tosti, A. Bimatoprost for the treatment of eyelash, eyebrow and scalp alopecia. Expert. Opin. Investig. Drugs 2017, 26, 515–522. [Google Scholar] [CrossRef]
- Alshahrani, Y.F.; Alghamdi, S.; Alkhathami, A.; Alshahrani, A.; Alshahrani, S.M.; Korkoman, A. Attitudes and Practices of Female University Students in Saudi Arabia Regarding the Cosmetic Use of Careprost (Bimatoprost) Eye Drops. Cureus 2024, 16, e56233. [Google Scholar] [CrossRef]
- Vergilis-Kalner, I.J. Application of Bimatoprost ophthalmic solution 0.03% for the treatment of eyebrow hypotrichosis: Series of ten cases. Dermatol. Online J. 2014, 20, 8. [Google Scholar] [CrossRef]
- Sarsik, S.M.; El-Amawy, H.S. Uses of eye drops in dermatology, literature review. J. Dermatolog. Treat. 2022, 33, 2758–2770. [Google Scholar] [CrossRef] [PubMed]
- Fukaya, S.; Kamata, M.; Kasanuki, T.; Yokobori, M.; Takeoka, S.; Hayashi, K.; Tanaka, T.; Fukuyasu, A.; Ishikawa, T.; Ohnishi, T.; et al. Open-label pilot study to evaluate the effectiveness of topical Bimatoprost on rhododendrol-induced refractory leukoderma. J. Dermatol. 2018, 45, 1283–1288. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.L.; Rivkin, A.; Dayan, S.; Shamban, A.; Werschler, W.P.; Teller, C.F.; Kaminer, M.S.; Sykes, J.M.; Weinkle, S.H.; Garcia, J.K. Multimodal Facial Aesthetic Treatment on the Appearance of Aging, Social Confidence, and Psychological Well-being: HARMONY Study. Aesthet. Surg. J. 2022, 42, NP115–NP124. [Google Scholar] [CrossRef]
- Suchonwanit, P.; Chanasumon, N.; Sriphojanart, T. Efficacy and Safety of Bimatoprost 0.01% for the Treatment of Eyebrow Hypotrichosis: A Randomized, Double-Blind, Vehicle-Controlled Study. Dermatol. Surg. 2019, 45, 1549–1556. [Google Scholar] [CrossRef] [PubMed]
- Steinsapir, K.D.; Steinsapir, S.M.G. Revisiting the Safety of Prostaglandin Analog Eyelash Growth Products. Dermatol. Surg. 2021, 47, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Zaher, H.; Gawdat, H.I.; Hegazy, R.A.; Hassan, M. Bimatoprost versus Mometasone Furoate in the Treatment of Scalp Alopecia Areata: A Pilot Study. Dermatology 2015, 230, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Levy, L.L.; Emer, J.J. Female pattern alopecia: Current perspectives. Int. J. Womens Health 2013, 5, 541–556. [Google Scholar]
- Wikramanayake, T.C.; Haberland, N.I.; Akhundlu, A.; Laboy Nieves, A.; Miteva, M. Prevention and Treatment of Chemotherapy-Induced Alopecia: What Is Available and What Is Coming? Curr. Oncol. 2023, 30, 3609–3626. [Google Scholar] [CrossRef]
- Rubio-Gonzalez, B.; Juhasz, M.; Fortman, J.; Mesinkovska, N.A. Pathogenesis and treatment options for chemotherapy-induced alopecia: A systematic review. Int. J. Dermatol. 2018, 57, 1417–1424. [Google Scholar] [CrossRef]
- Bhusal, M.; Bhattarai, S.; Thapa, B.; Shrestha, P.R.; Sagar, G.C. Bimatoprost versus Clobetasol Propionate in Scalp Alopecia Areata: A Prospective Non-Randomized Open-Label Clinical Trial. Indian. Dermatol. Online J. 2023, 14, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Fukumoto, T.; Fukumoto, R.; Magno, E.; Oka, M.; Nishigori, C.; Horita, N. Treatments for alopecia areata: A systematic review and network meta-analysis. Dermatol. Ther. 2021, 34, e14916. [Google Scholar] [CrossRef] [PubMed]
- Jha, A.K.; Sarkar, R.; Udayan, U.K.; Roy, P.K.; Jha, A.K.; Chaudhary, R.K.P. Bimatoprost in Dermatology. Indian Dermatol. Online J. 2018, 9, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Dubey, A.K. An effect of Bimatoprost: Adverse for some, therapeutic for others. Int. J. Trichol. 2011, 3, 129–130. [Google Scholar] [CrossRef] [PubMed]
- Vila, T.O.; Camacho Martinez, F.M. Bimatoprost in the treatment of eyelash universalis alopecia areata. Int. J. Trichol. 2010, 2, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Li, A.W.; Antaya, R.J. Successful Treatment of Pediatric Alopecia Areata of the Scalp Using Topical Bimatoprost. Pediatr. Dermatol. 2016, 33, e282–e283. [Google Scholar] [CrossRef] [PubMed]
- Anbar, T.S.; El-Ammawi, T.S.; Barakat, M.; Fawzy, A. Skin pigmentation after NB-UVB and three analogues of prostaglandin F(2alpha) in guinea pigs: A comparative study. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Yoelin, S.; Walt, J.G.; Earl, M. Safety, effectiveness, and subjective experience with topical Bimatoprost 0.03% for eyelash growth. Dermatol. Surg. 2010, 36, 638–649. [Google Scholar] [CrossRef] [PubMed]
- Harii, K.; Arase, S.; Tsuboi, R.; Weng, E.; Daniels, S.; VanDenburgh, A. Bimatoprost for eyelash growth in Japanese subjects: Two multicenter controlled studies. Aesthetic Plast. Surg. 2014, 38, 451–460. [Google Scholar] [CrossRef]
- Suchonwanit, P.; Thammarucha, S. Eyebrow growth pattern analysis in patients with eyebrow hypotrichosis after receiving topical treatment: A retrospective study. J. Cosmet. Dermatol. 2020, 19, 1404–1408. [Google Scholar] [CrossRef]
- Banaszek, A. Company profits from side effects of glaucoma treatment. Can. Med. Assoc. J. 2011, 183, E1058. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.V.; Friedman, P.M.; Agron, S.; Konda, A.; Parker, C.; Geronemus, R.G. Enhanced Uptake and Retention of 0.03% Bimatoprost, 0.5% 5-Fluorouracil, and 5% Minoxidil After 1,550-nm or 1,927-nm Nonablative Laser Pretreatment. Dermatol. Surg. 2022, 48, 932–936. [Google Scholar] [CrossRef] [PubMed]
- Waibel, J.S.; Rudnick, A.; Arheart, K.L.; Nagrani, N.; Gonzalez, A.; Gianatasio, C. Re-pigmentation of Hypopigmentation: Fractional Lasers vs. Laser-Assisted Delivery of Bimatoprost vs. Epidermal Melanocyte Harvesting System. J. Drugs Dermatol. 2019, 18, 1090–1096. [Google Scholar] [PubMed]
- Nguyen, N.; Helms, J.; Conza, A.; Petty, A.; Akanji, J.; Imahiyerobo-Ip, J. Microneedling with Bimatoprost to Treat Hypopigmented Skin Caused by Burn Scars. Cutis 2023, 111, E31–E33. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.R. Laser-assisted drug delivery for the treatment of androgenetic alopecia: Ablative laser fractional photothermolysis to enhance cutaneous topical delivery of platelet-rich plasma—With or without concurrent Bimatoprost and/or minoxidil. Dermatol. Online J. 2019, 25, 3. [Google Scholar] [CrossRef]
- Massaki, A.B.; Fabi, S.G.; Fitzpatrick, R. Repigmentation of hypopigmented scars using an erbium-doped 1,550-nm fractionated laser and topical Bimatoprost. Dermatol. Surg. 2012, 38 Pt 1, 995–1001. [Google Scholar] [CrossRef]
- Regis, A.; MacGregor, J.; Chapas, A. Fractional Resurfacing and Topical Bimatoprost for the Treatment of Laser Induced Postinflammatory Hypopigmentation on the Lower Extremities. Dermatol. Surg. 2018, 44, 883–886. [Google Scholar] [CrossRef]
- Wilson, B.N.; Aleisa, A.; Menzer, C.; Rossi, A.M. Bimatoprost drug delivery with fractional laser and microneedling for the management of COVID-19 prone positioning-induced facial atrophy and hypopigmentation. JAAD Case Rep. 2021, 15, 26–29. [Google Scholar] [CrossRef]
- Zubair, R.; Lyons, A.B.; Vellaichamy, G.; Peacock, A.; Hamzavi, I. What’s New in Pigmentary Disorders. Dermatol. Clin. 2019, 37, 175–181. [Google Scholar] [CrossRef]
- Kanokrungsee, S.; Pruettivorawongse, D.; Rajatanavin, N. Clinical outcomes of topical Bimatoprost for nonsegmental facial vitiligo: A preliminary study. J. Cosmet. Dermatol. 2021, 20, 812–818. [Google Scholar] [CrossRef]
- Barbulescu, C.C.; Goldstein, N.B.; Roop, D.R.; Norris, D.A.; Birlea, S.A. Harnessing the Power of Regenerative Therapy for Vitiligo and Alopecia Areata. J. Investig. Dermatol. 2020, 140, 29–37. [Google Scholar] [CrossRef]
- Silpa-Archa, N.; Likittanasombat, S.; Apinuntham, C.; Pruksaeakanan, C.; Charoenpipatsin, N.; Chaiyabutr, C.; Wongpraparut, C. The efficacy of Bimatoprost ophthalmic solution combined with NB-UVB phototherapy in non-segmental and segmental vitiligo: A single-blind randomized controlled study. Sci. Rep. 2023, 13, 6438. [Google Scholar] [CrossRef] [PubMed]
- Jha, A.K.; Prasad, S.; Sinha, R. Bimatoprost ophthalmic solution in facial vitiligo. J. Cosmet. Dermatol. 2018, 17, 437–440. [Google Scholar] [CrossRef]
- Kanokrungsee, S.; Khunkhet, S.; Rojhirunsakool, S.; Thadvibun, K.; Sahaspot, T. Triple combination therapy of narrowband ultraviolet B, fractional carbon dioxide laser and topical Bimatoprost 0.01% for non-segmental vitiligo on non-facial areas: A randomized half-body, double-blind, placebo-controlled, comparative study. Dermatol. Ther. 2022, 35, e15198. [Google Scholar] [CrossRef] [PubMed]
- Kreeshan, F.C.; Madan, V. Idiopathic Guttate Hypomelanosis Treated with 308-nm Excimer Light and Topical Bimatoprost. J. Cutan. Aesthet. Surg. 2021, 14, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Peabody, T.; Reitz, S.; Smith, J.; Teti, B. Clinical management of trichotillomania with Bimatoprost. Optom. Vis. Sci. 2013, 90, e167-71. [Google Scholar] [CrossRef] [PubMed]
- Schweiger, E.S.; Pinchover, L.; Bernstein, R.M. Topical Bimatoprost for the treatment of eyebrow hypotrichosis. J. Drugs Dermatol. 2012, 11, 106–108. [Google Scholar]
- Smith, S.; Fagien, S.; Whitcup, S.M.; Ledon, F.; Somogyi, C.; Weng, E.; Beddingfield, F.C., 3rd. Eyelash growth in subjects treated with Bimatoprost: A multicenter, randomized, double-masked, vehicle-controlled, parallel-group study. J. Am. Acad. Dermatol. 2012, 66, 801–806. [Google Scholar] [CrossRef]
- Jones, D. Enhanced eyelashes: Prescription and over-the-counter options. Aesthetic Plast. Surg. 2011, 35, 116–121. [Google Scholar] [CrossRef]
- Rahman, M.S.; Yoshida, N.; Hanafusa, M.; Matsuo, A.; Zhu, S.; Stub, Y.; Takahashi, C.; Tsuboi, H.; Matsushita, R.; Maekawa, K.; et al. Screening and quantification of undeclared PGF(2alpha) analogs in eyelash-enhancing cosmetic serums using LC-MS/MS. J. Pharm. Biomed. Anal. 2022, 219, 114940. [Google Scholar] [CrossRef]
- Fagien, S. Management of hypotrichosis of the eyelashes: Focus on Bimatoprost. Clin. Cosmet. Investig. Dermatol. 2010, 3, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Woodward, D.F.; Tang, E.S.; Attar, M.; Wang, J.W. The biodisposition and hypertrichotic effects of Bimatoprost in mouse skin. Exp. Dermatol. 2013, 22, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Wirta, D.; Baumann, L.; Bruce, S.; Ahluwalia, G.; Weng, E.; Daniels, S. Safety and Efficacy of Bimatoprost for Eyelash Growth in Postchemotherapy Subjects. J. Clin. Aesthet. Dermatol. 2015, 8, 11–20. [Google Scholar] [PubMed]
- Ahluwalia, G.S. Safety and efficacy of Bimatoprost solution 0.03% topical application in patients with chemotherapy-induced eyelash loss. J. Investig. Dermatol. Symp. Proc. 2013, 16, S73–S76. [Google Scholar] [CrossRef] [PubMed]
- Morris, C.L.; Stinnett, S.; Woodward, J. The role of Bimatoprost eyelash gel in chemotherapy-induced madarosis: An analysis of efficacy and safety. Int. J. Trichol. 2011, 3, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Caro, G.; Fortuna, M.C.; Pigliacelli, F.; D’Arino, A.; Carlesimo, M. Prevention and Treatment of Chemotherapy-Induced Alopecia. Dermatol. Pract. Concept. 2020, 10, e2020074. [Google Scholar] [CrossRef] [PubMed]
- Bitton, E.; Courey, C.; Giancola, P.; Diaconu, V.; Wise, J.; Wittich, W. Effects of LATISSE (Bimatoprost 0.03 per cent topical solution) on the ocular surface. Clin. Exp. Optom. 2017, 100, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Giannico, A.T.; Lima, L.; Russ, H.H.; Montiani-Ferreira, F. Eyelash growth induced by topical prostaglandin analogues, Bimatoprost, tafluprost, travoprost, and Latanoprost in rabbits. J. Ocul. Pharmacol. Ther. 2013, 29, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Emer, J.J.; Stevenson, M.L.; Markowitz, O. Novel treatment of female-pattern androgenetic alopecia with injected Bimatoprost 0.03% solution. J. Drugs Dermatol. 2011, 10, 795–798. [Google Scholar]
- Gupta, A.K.; Bamimore, M.A.; Foley, K.A. Efficacy of non-surgical treatments for androgenetic alopecia in men and women: A systematic review with network meta-analyses, and an assessment of evidence quality. J. Dermatol. Treat. 2022, 33, 62–72. [Google Scholar] [CrossRef]
- McElwee, K.J.; Shapiro, J.S. Promising therapies for treating and/or preventing androgenic alopecia. Skin. Therapy Lett. 2012, 17, 1–4. [Google Scholar] [PubMed]
- Khidhir, K.G.; Woodward, D.F.; Farjo, N.P.; Farjo, B.K.; Tang, E.S.; Wang, J.W.; Picksley, S.M.; Randall, V.A. The prostamide-related glaucoma therapy, Bimatoprost, offers a novel approach for treating scalp alopecias. FASEB J. 2013, 27, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Law, S.K. Bimatoprost in the treatment of eyelash hypotrichosis. Clin. Ophthalmol. 2010, 4, 349–358. [Google Scholar] [CrossRef]
- Ricar, J.; Cetkovska, P.; Hordinsky, M.; Ricarova, R. Topical Bimatoprost in the treatment of eyelash loss in alopecia totalis and universalis: A prospective, open-label study. Dermatol. Ther. 2022, 35, e15438. [Google Scholar] [CrossRef]
- Lu, Y.; He, Y.; Wang, X.; Wang, H.; Qiu, Q.; Wu, B.; Wu, X. Screening, characterization, and determination of suspected additives Bimatoprost and Latanoprost in cosmetics using NMR and LC-MS methods. Anal. Bioanal. Chem. 2023, 415, 3549–3558. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kang, G.; Park, H.N.; Kim, J.; Kim, N.S.; Park, S.; Park, S.K.; Baek, S.Y.; Kang, H. Determination of illegal adulteration of dietary supplements with synthetic hair-growth compounds by UPLC and LC-Q-TOF/MS. Food Addit. Contam. Part. A Chem. Anal. Control Expo. Risk Assess. 2018, 35, 191–199. [Google Scholar] [CrossRef]
- Johansson, M.; Fransson, D.; Rundlof, T.; Huynh, N.H.; Arvidsson, T. A general analytical platform and strategy in search for illegal drugs. J. Pharm. Biomed. Anal. 2014, 100, 215–229. [Google Scholar] [CrossRef]
- Yazdanian, N.; Mozafarpoor, S.; Goodarzi, A. Phosphodiesterase inhibitors and prostaglandin analogues in dermatology: A comprehensive review. Dermatol. Ther. 2021, 34, e14669. [Google Scholar] [CrossRef]
- Nasir, W.; Aguilera, S.B.; Weiss, E. Non-Surgical Eyebrow Rejuvenation Techniques: A Review. J. Drugs Dermatol. 2021, 20, 970–978. [Google Scholar] [CrossRef]
- Riahi, R.R.; Cohen, P.R. Topical Treatment of Eyebrow Hypotrichosis with Bimatoprost 0.03% Solution: Case Report and Literature Review. Cureus 2018, 10, e2666. [Google Scholar] [CrossRef]
- Borchert, M.; Bruce, S.; Wirta, D.; Yoelin, S.G.; Lee, S.; Mao, C.; VanDenburgh, A. An evaluation of the safety and efficacy of Bimatoprost for eyelash growth in pediatric subjects. Clin. Ophthalmol. 2016, 10, 419–429. [Google Scholar] [PubMed]
- Zaky, M.S.; Hashem, O.A.; Mahfouz, S.M.; Elsaie, M.L. Comparative study of the efficacy and safety of topical minoxidil 2% versus topical Bimatoprost 0.01% versus topical Bimatoprost 0.03% in treatment of eyebrow hypotrichosis: A randomized controlled trial. Arch. Dermatol. Res. 2023, 315, 2635–2641. [Google Scholar] [CrossRef] [PubMed]
- Li, L.C.; Lei, T.C.; Xing, F. Bimatoprost promotes hair growth of reconstructed hair follicles in mice through activation of the Wnt/beta-catenin signaling pathway. Zhonghua Yi Xue Za Zhi 2021, 101, 1529–1534. [Google Scholar] [PubMed]
- Gupta, A.K.; Carviel, J.; Abramovits, W. Treating Alopecia Areata: Current Practices Versus New Directions. Am. J. Clin. Dermatol. 2017, 18, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Fagien, S.; Walt, J.G.; Carruthers, J.; Cox, S.E.; Wirta, D.; Weng, E.; Beddingfield, F.C., 3rd. Patient-reported outcomes of Bimatoprost for eyelash growth: Results from a randomized, double-masked, vehicle-controlled, parallel-group study. Aesthet. Surg. J. 2013, 33, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Kwon, O.; Kim, J.Y.; Paik, S.H.; Jeon, H.C.; Jung, Y.J.; Lee, Y.; Baek, J.H.; Chun, J.H.; Lee, W.S.; Lee, J.Y.; et al. Long-term utility and durability of the therapeutic effects of Bimatoprost 0.03% for eyelash augmentation in healthy Asian subjects. Dermatology 2014, 229, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Beer, K.R.; Julius, H.; Dunn, M.; Wilson, F. Treatment of eyebrow hypotrichosis using Bimatoprost: A randomized, double-blind, vehicle-controlled pilot study. Dermatol. Surg. 2013, 39, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Woodward, J.A.; Haggerty, C.J.; Stinnett, S.S.; Williams, Z.Y. Bimatoprost 0.03% gel for cosmetic eyelash growth and enhancement. J. Cosmet. Dermatol. 2010, 9, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Wester, S.T.; Lee, W.W.; Shi, W. Eyelash growth from application of Bimatoprost in gel suspension to the base of the eyelashes. Ophthalmology 2010, 117, 1024–1031. [Google Scholar] [CrossRef]
- Zaleski-Larsen, L.A.; Ruth, N.H.; Fabi, S.G. Retrospective Evaluation of Topical Bimatoprost and Iris Pigmentation Change. Dermatol. Surg. 2017, 43, 1431–1433. [Google Scholar] [CrossRef]
- Carruthers, J.; Beer, K.; Carruthers, A.; Coleman, W.P., 3rd; Draelos, Z.D.; Jones, D.; Goldman, M.P.; Pucci, M.L.; VanDenburgh, A.; Weng, E.; et al. Bimatoprost 0.03% for the Treatment of Eyebrow Hypotrichosis. Dermatol. Surg. 2016, 42, 608–617. [Google Scholar] [CrossRef] [PubMed]
- Suchonwanit, P.; Harnchoowong, S.; Chanasumon, N.; Sriphojanart, T. Comparison of the efficacy and safety of using 0.01% versus 0.03% Bimatoprost for the treatment of eyebrow hypotrichosis: A randomized, double-blind, split-face, comparative study. J. Cosmet. Dermatol. 2020, 19, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Yoelin, S.G.; Fagien, S.; Cox, S.E.; Davis, P.G.; Campo, A.; Caulkins, C.A.; Gallagher, C.J. A retrospective review and observational study of outcomes and safety of Bimatoprost ophthalmic solution 0.03% for treating eyelash hypotrichosis. Dermatol. Surg. 2014, 40, 1118–1124. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.M.; Diehl, J.; Levins, P.C. Promising alternative clinical uses of prostaglandin F2alpha analogs: Beyond the eyelashes. J. Am. Acad. Dermatol. 2015, 72, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Glaser, D.A.; Hossain, P.; Perkins, W.; Griffiths, T.; Ahluwalia, G.; Weng, E.; Beddingfield, F.C. Long-term safety and efficacy of Bimatoprost solution 0.03% application to the eyelid margin for the treatment of idiopathic and chemotherapy-induced eyelash hypotrichosis: A randomized controlled trial. Br. J. Dermatol. 2015, 172, 1384–1394. [Google Scholar] [CrossRef] [PubMed]
- Sayed, K.M.; Mostafa, E.M.; Mounir, A.; Abd Elhaliem, N.G.; Alsmman, A.H. Analysis of Bimatoprost-Induced changes on Rabbits eyelash Follicle: Clinical and Electron microscopic study. Clin. Ophthalmol. 2019, 13, 2421–2426. [Google Scholar] [CrossRef]
- Shin, D.W. The physiological and pharmacological roles of prostaglandins in hair growth. Korean J. Physiol. Pharmacol. 2022, 26, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.H.; Chu, H.; Ahn, Y.; Kim, J.; Kim, D.Y. HMGB1 promotes hair growth via the modulation of prostaglandin metabolism. Sci. Rep. 2019, 9, 6660. [Google Scholar] [CrossRef] [PubMed]
- Chanasumon, N.; Sriphojanart, T.; Suchonwanit, P. Therapeutic potential of Bimatoprost for the treatment of eyebrow hypotrichosis. Drug Des. Devel Ther. 2018, 12, 365–372. [Google Scholar] [CrossRef]
- Wirta, D.; Pariser, D.M.; Yoelin, S.G.; Arase, S.; McMichael, A.; Weng, E.; Mao, C.; Demos, G.; Vandenburgh, A. Bimatoprost 0.03% for the Treatment of Eyelash Hypotrichosis: A Pooled Safety Analysis of Six Randomized, Double-masked Clinical Trials. J. Clin. Aesthet. Dermatol. 2015, 8, 17–29. [Google Scholar]
- Ali, M.S.; Hafiz, H.S.A.; Ahmed, N.A.; Galal, S.A. Combined microneedling with topical vitamin D3 or Bimatoprost versus microneedling alone in the treatment of alopecia areata: A comparative randomized trial. J. Cosmet. Dermatol. 2023, 22, 1286–1296. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Wang, X.; Wu, M. Topical medication instillation techniques for glaucoma. Cochrane Database Syst. Rev. 2017, 2, CD010520. [Google Scholar] [CrossRef] [PubMed]
- Palmer, D.J.; Scheman, A.; Tanna, A.P.; Bueno, A. The effect of cutaneous prostaglandin application on nail growth, nail brittleness, and intraocular pressure. J. Cosmet. Dermatol. 2018, 17, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Reardon, G.; Schwartz, G.F.; Kotak, S. Persistence on prostaglandin ocular hypotensive therapy: An assessment using medication possession and days covered on therapy. BMC Ophthalmol. 2010, 10, 5. [Google Scholar] [CrossRef] [PubMed]
- Aref, A.A. Sustained drug delivery for glaucoma: Current data and future trends. Curr. Opin. Ophthalmol. 2017, 28, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Kesav, N.P.; Young, C.E.C.; Ertel, M.K.; Seibold, L.K.; Kahook, M.Y. Sustained-release drug delivery systems for the treatment of glaucoma. Int. J. Ophthalmol. 2021, 14, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Gillmann, K.; Mansouri, K. Minimally Invasive Surgery, Implantable Sensors, and Personalized Therapies. J. Ophthalmic Vis. Res. 2020, 15, 531–546. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, F.A.; Sheybani, A.; Shah, M.M.; Rivas, M.; Bai, Z.; Werts, E.; Ahmed, I.I.K.; Craven, E.R. Single Administration of Intracameral Bimatoprost Implant 10 microg in Patients with Open-Angle Glaucoma or Ocular Hypertension. Ophthalmol. Ther. 2022, 11, 1517–1537. [Google Scholar] [CrossRef]
- Gautam, M.; Gupta, R.; Singh, P.; Verma, V.; Verma, S.; Mittal, P.; Karkhur, S.; Sampath, A.; Mohan, R.R.; Sharma, B. Intracameral Drug Delivery: A Review of Agents, Indications, and Outcomes. J. Ocul. Pharmacol. Ther. 2023, 39, 102–116. [Google Scholar] [CrossRef]
- Kompella, R.; Patil, M. Pharmacokinetic-pharmacodynamic model to predict drug concentrations and intraocular pressure lowering effect for a Bimatoprost six-month slow-release system. Eur. J. Ophthalmol. 2022, 33, 11206721221135910. [Google Scholar] [CrossRef]
- Wong, M.K.; Bowers, M.E.; Ventimiglia, J.; Niknam, R.M.; Moster, M.R.; Pro, M.J.; Dale, E.; Kolomeyer, N.N.; Lee, D.; Zheng, C.X. Short-Term Outcomes of Bimatoprost Sustained-Release Intracameral Implant in Glaucoma. J. Glaucoma 2023, 32, 738–743. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Almazan, A.; Decker, S.; Zhong, Y.; Ghebremeskel, A.N.; Hughes, P.; Robinson, M.R.; Burke, J.A.; Weinreb, R.N. Intraocular Pressure Effects and Mechanism of Action of Topical Versus Sustained-Release Bimatoprost. Transl. Vis. Sci. Technol. 2019, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.A.; Christie, W.C.; Day, D.G.; Craven, E.R.; Walters, T.; Bejanian, M.; Lee, S.S.; Goodkin, M.L.; Zhang, J.; Whitcup, S.M.; et al. Bimatoprost Sustained-Release Implants for Glaucoma Therapy: 6-Month Results from a Phase I/II Clinical Trial. Am. J. Ophthalmol. 2017, 175, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, R.N.; Christie, W.C.; Medeiros, F.A.; Craven, E.R.; Kim, K.; Nguyen, A.; Bejanian, M.; Wirta, D.L. Single Administration of Bimatoprost Implant: Effects on 24-Hour Intraocular Pressure and 1-Year Outcomes. Ophthalmol. Glaucoma 2023, 6, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Craven, E.R.; Walters, T.; Christie, W.C.; Day, D.G.; Lewis, R.A.; Goodkin, M.L.; Chen, M.; Wangsadipura, V.; Robinson, M.R.; Bejanian, M.; et al. 24-Month Phase I/II Clinical Trial of Bimatoprost Sustained-Release Implant (Bimatoprost SR) in Glaucoma Patients. Drugs 2020, 80, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Robinson, M.R.; Struble, C.; Attar, M. Nonclinical Pharmacokinetic and Pharmacodynamic Assessment of Bimatoprost Following a Single Intracameral Injection of Sustained-Release Implants. Transl. Vis. Sci. Technol. 2020, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Di Trani, N.; Jain, P.; Chua, C.Y.X.; Ho, J.S.; Bruno, G.; Susnjar, A.; Pons-Faudoa, F.P.; Sizovs, A.; Hood, R.L.; Smith, Z.W.; et al. Nanofluidic microsystem for sustained intraocular delivery of therapeutics. Nanomedicine 2019, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Belamkar, A.; Harris, A.; Zukerman, R.; Siesky, B.; Oddone, F.; Verticchio Vercellin, A.; Ciulla, T.A. Sustained release glaucoma therapies: Novel modalities for overcoming key treatment barriers associated with topical medications. Ann. Med. 2022, 54, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Zhou, P.; Kansara, N.D.; Frankfort, B.J.; Blieden, L.S.; Chang, P.T. Intraocular Pressure and Eyedrop Usage Reduction with Intracameral Bimatoprost Implant. J. Ocul. Pharmacol. Ther. 2023, 39, 398–403. [Google Scholar] [CrossRef]
- Sirinek, P.E.; Lin, M.M. Intracameral sustained release bimatoprost implants (Durysta). Semin. Ophthalmol. 2022, 37, 385–390. [Google Scholar] [CrossRef]
- Satyanarayana, S.D.; Abu Lila, A.S.; Moin, A.; Moglad, E.H.; Khafagy, E.S.; Alotaibi, H.F.; Obaidullah, A.J.; Charyulu, R.N. Ocular Delivery of Bimatoprost-Loaded Solid Lipid Nanoparticles for Effective Management of Glaucoma. Pharmaceuticals 2023, 16, 1001. [Google Scholar] [CrossRef] [PubMed]
- Seal, J.R.; Robinson, M.R.; Burke, J.; Bejanian, M.; Coote, M.; Attar, M. Intracameral Sustained-Release Bimatoprost Implant Delivers Bimatoprost to Target Tissues with Reduced Drug Exposure to Off-Target Tissues. J. Ocul. Pharmacol. Ther. 2019, 35, 50–57. [Google Scholar] [CrossRef]
- Lee, S.S.; Burke, J.; Shen, J.; Almazan, A.; Orilla, W.; Hughes, P.; Zhang, J.; Li, H.; Struble, C.; Miller, P.E.; et al. Bimatoprost sustained-release intracameral implant reduces episcleral venous pressure in dogs. Vet. Ophthalmol. 2018, 21, 376–381. [Google Scholar] [CrossRef]
- Yadav, M.; Guzman-Aranguez, A.; Perez de Lara, M.J.; Singh, M.; Singh, J.; Kaur, I.P. Bimatoprost loaded nanovesicular long-acting sub-conjunctival in-situ gelling implant: In vitro and in vivo evaluation. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 103, 109730. [Google Scholar] [CrossRef]
- Yadav, M.; Guzman-Aranguez, A.; Perez de Lara, M.J.; Singh, M.; Singh, J.; Kaur, I.P. Safety data on in situ gelling Bimatoprost loaded nanovesicular formulations. Data Brief. 2019, 25, 104361. [Google Scholar] [CrossRef] [PubMed]
- Franca, J.R.; Foureaux, G.; Fuscaldi, L.L.; Ribeiro, T.G.; Rodrigues, L.B.; Bravo, R.; Castilho, R.O.; Yoshida, M.I.; Cardoso, V.N.; Fernandes, S.O.; et al. Bimatoprost-loaded ocular inserts as sustained release drug delivery systems for glaucoma treatment: In vitro and in vivo evaluation. PLoS ONE 2014, 9, e95461. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, F.A.; Walters, T.R.; Kolko, M.; Coote, M.; Bejanian, M.; Goodkin, M.L.; Guo, Q.; Zhang, J.; Robinson, M.R.; Weinreb, R.N.; et al. Phase 3, Randomized, 20-Month Study of Bimatoprost Implant in Open-Angle Glaucoma and Ocular Hypertension (ARTEMIS 1). Ophthalmology 2020, 127, 1627–1641. [Google Scholar] [CrossRef] [PubMed]
- Ghosn, C.; Rajagopalan, L.; Ugarte, S.; Mistry, S.; Orilla, W.; Goodkin, M.L.; Robinson, M.R.; Engles, M.; Dibas, M. Intraocular Pressure-Lowering Efficacy of a Sustained-Release Bimatoprost Implant in Dog Eyes Pretreated with Selective Laser Trabeculoplasty. J. Ocul. Pharmacol. Ther. 2022, 38, 311–318. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Bacharach, J.; Brubaker, J.W.; Medeiros, F.A.; Bejanian, M.; Bernstein, P.; Robinson, M.R. Bimatoprost Implant Biodegradation in the Phase 3, Randomized, 20-Month ARTEMIS Studies. J. Ocul. Pharmacol. Ther. 2023, 39, 55–62. [Google Scholar] [CrossRef]
- Desai, A.R.; Maulvi, F.A.; Desai, D.M.; Shukla, M.R.; Ranch, K.M.; Vyas, B.A.; Shah, S.A.; Sandeman, S.; Shah, D.O. Multiple drug delivery from the drug-implants-laden silicone contact lens: Addressing the issue of burst drug release. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 112, 110885. [Google Scholar] [CrossRef]
- Miller, P.E.; Eaton, J.S. Medical anti-glaucoma therapy: Beyond the drop. Vet. Ophthalmol. 2021, 24 (Suppl. S1), 2–15. [Google Scholar] [CrossRef]
- Kenley, R.A.; Filippone, H.; Giske, M.; Beidler, D.; Vehige, J.; Fleitman, J. Equilibrium binding interactions between lotrafilcon a soft contact lenses and the two prostaglandin antiglaucoma drugs Bimatoprost and tafluprost. Eye Contact Lens 2013, 39, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Maulvi, F.A.; Soni, P.D.; Patel, P.J.; Desai, A.R.; Desai, D.T.; Shukla, M.R.; Shah, S.A.; Shah, D.O.; Willcox, M.D.P. Controlled Bimatoprost release from graphene oxide laden contact lenses: In vitro and in vivo studies. Colloids Surf. B Biointerfaces 2021, 208, 112096. [Google Scholar] [CrossRef]
- Sekar, P.; Chauhan, A. Effect of vitamin-E integration on delivery of prostaglandin analogs from therapeutic lenses. J. Colloid Interface Sci. 2019, 539, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Ma, C.; Ma, Y.; Ma, Y.; Mao, Y.; Meng, Z. Sustained Bimatoprost release using gold nanoparticles laden contact lenses. J. Biomater. Sci. Polym. Ed. 2021, 32, 1618–1634. [Google Scholar] [CrossRef]
- Shirley, M. Bimatoprost Implant: First Approval. Drugs Aging 2020, 37, 549, Erratum in Drugs Aging 2020, 37, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Lambert, W.S.; Carlson, B.J.; van der Ende, A.E.; Shih, G.; Dobish, J.N.; Calkins, D.J.; Harth, E. Nanosponge-Mediated Drug Delivery Lowers Intraocular Pressure. Transl. Vis. Sci. Technol. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Dams, I.; Chodynski, M.; Krupa, M.; Pietraszek, A.; Zezula, M.; Cmoch, P.; Kosinska, M.; Kutner, A. A novel convergent synthesis of the antiglaucoma PGF2alpha analogue Bimatoprost. Chirality 2013, 25, 170–179. [Google Scholar] [CrossRef]
- Yasmeen, A.; Syed, M.H.; Alqahtani, S.S.; Kashan Syed, N.; Meraya, A.M.; Wazaify, M.; Van Hout, M.C. Suspected inappropriate use of prescription and non-prescription drugs among requesting customers: A Saudi community pharmacists’ perspective. Saudi Pharm. J. 2023, 31, 1254–1264. [Google Scholar] [CrossRef]
- Ichioka, H.; Ida, Y.; Watanabe, M.; Ohguro, H.; Hikage, F. Prostaglandin F2alpha and EP2 agonists, and a ROCK inhibitor modulate the formation of 3D organoids of Grave’s orbitopathy related human orbital fibroblasts. Exp. Eye Res. 2021, 205, 108489. [Google Scholar] [CrossRef]
- Draman, M.S.; Morris, D.S.; Evans, S.; Haridas, A.; Pell, J.; Greenwood, R.; Foy, C.; Taylor, P.; Pooprasert, P.; Muller, I.; et al. Prostaglandin F2-Alpha Eye Drops (Bimatoprost) in Graves’ Orbitopathy: A Randomized Controlled Double-Masked Crossover Trial (BIMA Trial). Thyroid 2019, 29, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Melovatskiy, P.D.; Krylova, E.I.; Grusha, Y.O. Prospects of the use of prostaglandin analogues in the treatment of patients with thyroid eye disease. Vestn. Oftalmol. 2022, 138, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Eiger-Moscovich, M.; Stiebel-Kalish, H.; Yassur, I.; Barash, D.; Gaton, D.; Avisar, I. Prostaglandin analogue drops for the treatment of soft tissue expansion and exophthalmos in patients with inactive thyroid eye disease. Can. J. Ophthalmol. 2019, 54, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Higashiyama, T.; Ohji, M. Treatment with Bimatoprost for exophthalmos in patients with inactive thyroid-associated ophthalmopathy. Clin. Ophthalmol. 2018, 12, 2415–2421. [Google Scholar] [CrossRef] [PubMed]
- Weber, U. Central corneal thickness and corneal endothelial morphology with and without therapy using commercially available antiglaucomatous drugs. Klin. Monbl Augenheilkd. 2012, 229, 716–723. [Google Scholar] [PubMed]
- Salvetat, M.L.; Zeppieri, M.; Tosoni, C.; Parisi, L.; Brusini, P. Non-conventional perimetric methods in the detection of early glaucomatous functional damage. Eye 2010, 24, 835–842. [Google Scholar] [CrossRef]
- Brusini, P.; Salvetat, M.L.; Parisi, L.; Zeppieri, M.; Tosoni, C. Discrimination between normal and early glaucomatous eyes with scanning laser polarimeter with fixed and variable corneal compensator settings. Eur. J. Ophthalmol. 2005, 15, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Fogagnolo, P.; Figus, M.; Frezzotti, P.; Iester, M.; Oddone, F.; Zeppieri, M.; Ferreras, A.; Brusini, P.; Rossetti, L.; Orzalesi, N. Test-retest variability of intraocular pressure and ocular pulse amplitude for dynamic contour tonometry: A multicentre study. Br. J. Ophthalmol. 2010, 94, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Salvetat, M.L.; Zeppieri, M.; Tosoni, C.; Brusini, P. Baseline factors predicting the risk of conversion from ocular hypertension to primary open-angle glaucoma during a 10-year follow-up. Eye 2016, 30, 784–795. [Google Scholar] [CrossRef]
- Yoneda, T.; Sumi, T.; Takahashi, A.; Hoshikawa, Y.; Kobayashi, M.; Fukushima, A. Automated hyperemia analysis software: Reliability and reproducibility in healthy subjects. Jpn. J. Ophthalmol. 2012, 56, 1–7. [Google Scholar] [CrossRef]
- Bastia, E.; Sgambellone, S.; Lucarini, L.; Provensi, G.; Brambilla, S.; Galli, C.; Almirante, N.; Impagnatiello, F. NCX 470 Restores Ocular Hemodynamics and Retinal Cell Physiology After ET-1-Induced Ischemia/Reperfusion Injury of Optic Nerve and Retina in Rabbits. J. Ocul. Pharmacol. Ther. 2022, 38, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Mohan, N.; Chakrabarti, A.; Nazm, N.; Mehta, R.; Edward, D.P. Newer advances in medical management of glaucoma. Indian J. Ophthalmol. 2022, 70, 1920–1930. [Google Scholar] [PubMed]
- Walters, T.R.; Kothe, A.C.; Boyer, J.L.; Usner, D.W.; Lopez, K.; Duquesroix, B.; Fechtner, R.D.; Navratil, T. A Randomized, Controlled Comparison of NCX 470 (0.021%, 0.042%, and 0.065%) and Latanoprost 0.005% in Patients with Open-angle Glaucoma or Ocular Hypertension: The Dolomites Study. J. Glaucoma 2022, 31, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Impagnatiello, F.; Bastia, E.; Almirante, N.; Brambilla, S.; Duquesroix, B.; Kothe, A.C.; Bergamini, M.V.W. Prostaglandin analogues and nitric oxide contribution in the treatment of ocular hypertension and glaucoma. Br. J. Pharmacol. 2019, 176, 1079–1089. [Google Scholar] [CrossRef] [PubMed]
- Impagnatiello, F.; Toris, C.B.; Batugo, M.; Prasanna, G.; Borghi, V.; Bastia, E.; Ongini, E.; Krauss, A.H. Intraocular Pressure-Lowering Activity of NCX 470, a Novel Nitric Oxide-Donating Bimatoprost in Preclinical Models. Investig. Ophthalmol. Vis. Sci. 2015, 56, 6558–6564. [Google Scholar] [CrossRef]
- Woodward, D.F.; Coleman, R.A.; Woodrooffe, A.J.; Spada, C.S.; Wang, J.W. Effect of the Antiglaucoma Agent JV-GL1 and Related Compounds in the Canine Eye. J. Ocul. Pharmacol. Ther. 2020, 36, 636–648. [Google Scholar] [CrossRef]
Figure 1.
Chemical structure of the bimatoprost molecule.

Figure 2.
PRISMA flowchart showing selection of articles used in this study.

Figure 3.
Graphical depiction of studies used for the literature review: (a) spread of articles used by date of publication; (b) spread of articles used in this review by location of research.
Figure 3.
Graphical depiction of studies used for the literature review: (a) spread of articles used by date of publication; (b) spread of articles used in this review by location of research.

Figure 4.
External ocular complications of bimatoprost use: (A) eyelash darkening, DUES, and growth in a 70-year-old male patient using bimatoprost for POAG; (B) 63-year-old glaucomatous female patient with DUES, mild conjunctival hyperemia, ocular dryness, iris darkening, eyelash growth, and periorbital pigmentation.
Figure 4.
External ocular complications of bimatoprost use: (A) eyelash darkening, DUES, and growth in a 70-year-old male patient using bimatoprost for POAG; (B) 63-year-old glaucomatous female patient with DUES, mild conjunctival hyperemia, ocular dryness, iris darkening, eyelash growth, and periorbital pigmentation.


{kind=link}
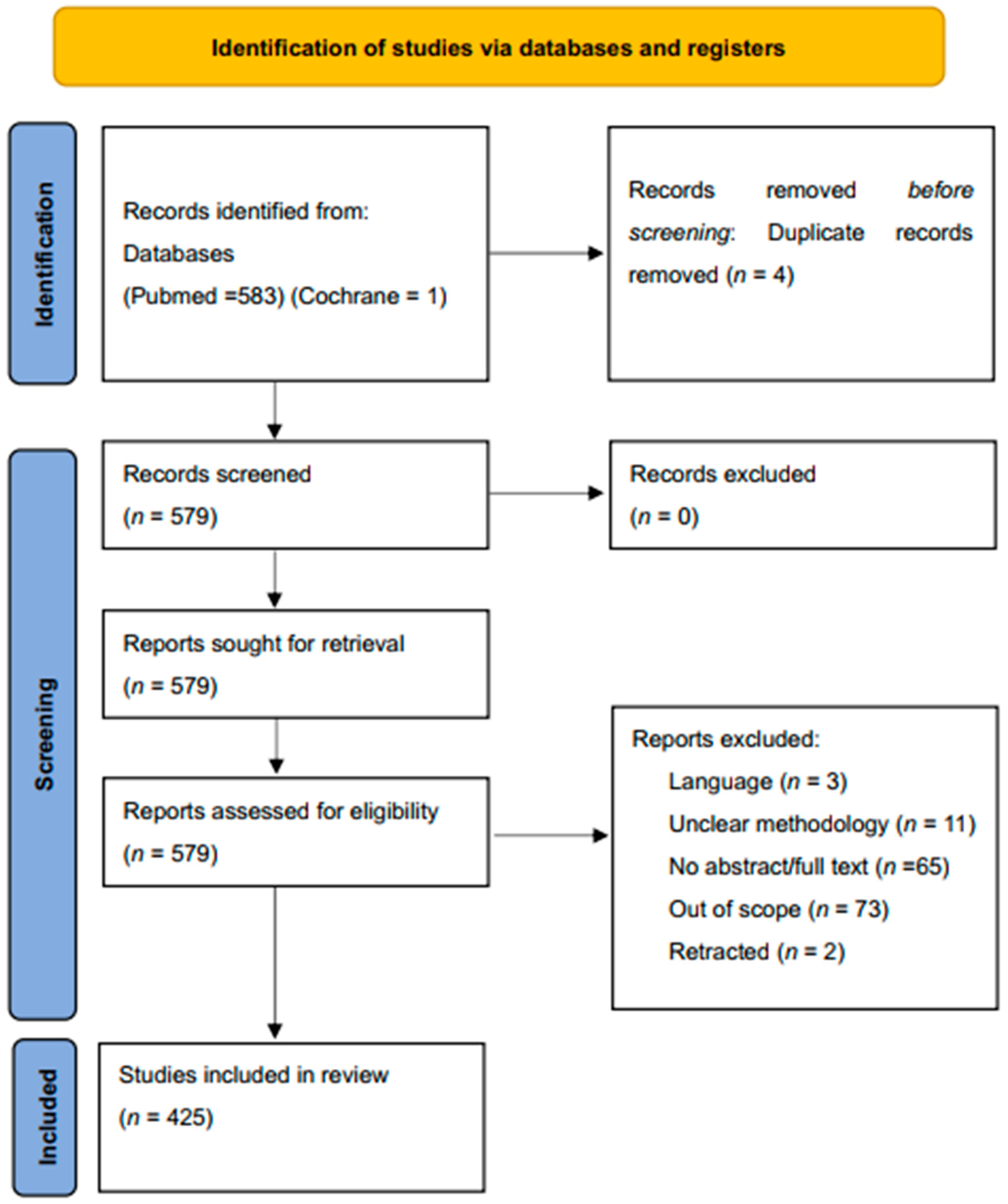{kind=link}
{kind=link}
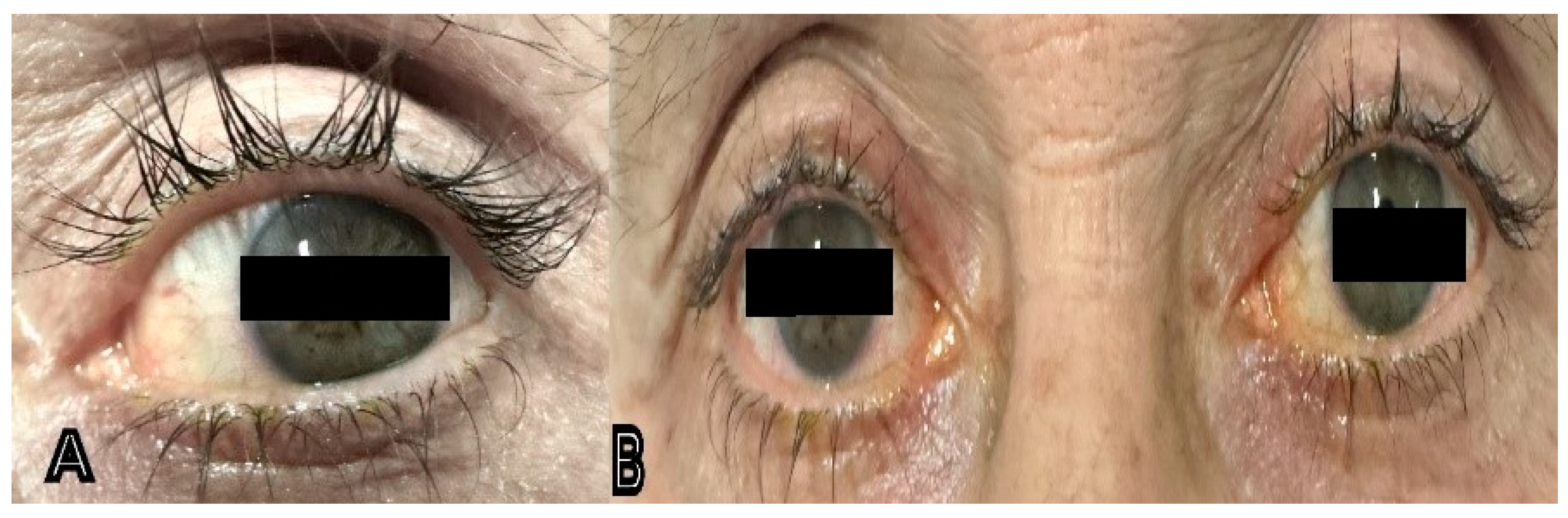{kind=link}
Table 1.
Studies regarding the comparative IOP-lowering effects of bimatoprost.
| Study and Year | Design | Study Population | Main Outcomes with p Values |
|---|---|---|---|
| Holstrom et al., 2005 [201] | Meta-analysis | 9295 (42 studies) | 30.3% reduction in IOP from baseline with bimatoprost compared to 28.7% with travoprost and 26.7% with latanoprost (p = 0.001) |
| Denis et al., 2007 [202] | Meta-analysis | 1318 (6 studies) | bimatoprost produced the largest reduction in IOP (−1.04 mmHg, 95% CI: −2.11; 0.04; p = 0.06) compared to bimatoprost (−0.98 mmHg, 95% CI: −2.08; 0.13; p = 0.08) and a reference latanoprost treated population |
| Noecker et al., 2003 [203] | Clinical Trial | 31 | bimatoprost produced a mean IOP reduction of 8.4 mmHg (33.7%) compared to 7.9 mmHg (30%) with travoprost (p = 0.671) |
| Noecker et al., 2003 [204] | Clinical Trial | 269 | From baselines before treatments of 24.0 ± 0.27 mm Hg (bimatoprost) and 23.3 ± 0.27 mm Hg (latanoprost), IOP reduced statistically more in the bimatoprost group as compared to the latanoprost group (16.5–17.4 mm Hg; 17.6–18.9 mm Hg, p ≤ 0.008) |
| Parrish et al., 2003 [205] | Clinical Trial | 393 | Three separate groups of participants achieved IOP lowering of 8.6 ± 0.3 mmHg, 8.7 ± 0.3 mmHg, and 8.0 ± 0.3 mmHg when treated with latanoprost, bimatoprost or travporost respectively (p = 0.128 for difference among groups). |
| Cantor et al., 2004 [206] | Clinical Trial | 26 | IOP reduced by 7.4–8.8 mmHg with bimatoprost as compared to 4.6–7.2 mmHg with travoprost (p = 0.057) |
Table 2.
Summary of complications related to bimatoprost.
| Summary of Findings | Formulation | Location of Complication | Authors |
|---|---|---|---|
| Bimatoprost use was implicated in the sudden expression of non-vellus hairs in a female patient | Lumigan 0.03%, (Allergan, Dublin, ON, Canada) | Face | Kaliaperumal et al. [215] |
| The bimatoprost regimen was associated with a reduction in IPD | Lumigan 0.03%, (Senju Pharmaceutical Co., Osaka, Japan) | Interpupillary distance | Sano et al. [216] |
| Bimatoprost is implicated in eyelash trichomegaly | Bimatoprost * | Eyelash | Hutchinson et al. [217] |
| The doctor noticed audible clicking of eyelashes secondary to eyelash elongation | Bimatoprost * | Eyelash | Skorin and Dailey [218] |
| Bimatoprost produced more upper eyelid changes as compared to latanoprost | Bimatoprost 0.03% * | Eyelid | Karslioglu et al. [219] |
| Hypopigmentation progressing to Lentigo Maligna Melanoma | Bimatoprost 0.03% * | Eyelid tissue | Deveau et al. [220] |
| Bimatoprost use resulted in eyelid tightening and shortening in the mouse model | Bimatoprost 0.03% * | Eyelid tissue | Kent and Custer [221] |
| Bilateral upper lid retraction was observed with bimatoprost use | Bimatoprost 0.03% * | Eyelids (upper) | Noma and Kakizaki [222] |
| DUES was the most common complication seen in an Asian study | Bimatoprost * | Orbit | Kim et al. [223] |
| Topical and retrobulbar injection of bimatoprost resulted in a drop in adipocyte cell count | Lumigan 0.03%, Allergan | Orbital fat | Jbara et al. [224] |
| Orbital fat reduced as evidenced by adnexal photographs | Bimatoprost * | Orbital fat | Rabinowitz et al. [225] |
| MRI and computer image algorithms respectively showed reduced orbital fat after bimatoprost use | bimatoprost (Allergan, Inc.), | Orbital fat | Higoshima et al. [226], and Eftekhari et al. [227] |
| Prostaglandins inhibit adipogenesis resulting in DUES | Bimaopost and Bimatoprost acid (Cayman Chemical Co., Ann Arbor, MI, USA) | Orbital tissue | Taketani et al. [228] and Ida et al. [229] |
| Bimatoprost implicated in peri-orbitopathy | Bimatoprost * | Periorbital | Tan and Berke [230] |
| Atrophy of the eyelid levator muscle was observed after the use of bimatoprost monocularly | Lumigan 0.03%, Allergan | Periorbital muscle | Wang et al. [231] |
| Bimatoprost (Latisse) induced skin discoloration | Bimatoprost solution, 0.3% (Latisse; Allergan Inc., Dublin, ON, Canada) | Periocular discoloration | Priluck and Fu [232] |
| Adverse effects include conjunctival hyperemia, burning sensation, and growth of eyelashes | Bimatoprost 0.03% *, Bimatoprost 0.01% * | External eye | Lewis et al. [233] and Park et al. [234] |
| Hyperemia and eyelash elongation were the most common side effects reported in a large Asian study | Lumigan 0.03%, Allergan | external eye | Sun et al. [235] |
| Bimatoprost use resulted in orbital fat prolapse and iris pigmentation | Lumigan 0.03%, Allergan | Eyeball tissue and iris | Aydin et al. [236], Jayaprakasam and Ghazi-Nouri [237], and Park et al. [238] |
| The tear profile of patients on bimatoprost revealed elevated cytokines mediating allergenic pathway | Bimaotoprost 0.01% * | Tears | Reddy et al. [239] |
| Bimatoprost scored highest on the pain scale in cataract surgery patients | Bimaotoprost * | Anterior eye | Ulas et al. [240] |
| A slight but significant increase in thickness observed | Bimatoprost 0.03% * | Central corneal thickness | Bafa et al. [241] |
| A slight but significant reduction in thickness observed | Bimatoprost 0.03% * | Central corneal thickness | Zhong et al. [242] and Eraslan and Celikay [243] |
| A systematic review showed that prostaglandin analogs result in thinning of the CCT | Bimatoprost * | Central corneal thickness (CCT) | Kim and Yim [244] |
| Bimatoprost was associated with conjunctival hyperemia | Lumigan PF 0.03% | Conjunctiva/cornea | Wu et al. [245] |
| PGF2α including bimatoprost-induced reduction in tissue stiffness and cornea microstructure changes | Bimatoprost * | Cornea | Wang et al. [246] |
| Scheimflug-aided analysis showed a longitudinal reduction in CCD after bimatoprost use | Bimatoprost * | Cornea cell density (CCD) | Eraslan et al. [247] |
| Bimatoprost demonstrated cytotoxicity to tested cells | Lumigan 0.01%, and Lumigan 0.03% | Corneal endothelial cells | Tong et al. [248] |
| Bimatoprost was found to cause cell necrosis and stifle proliferation | Bimatoprost * | Corneal epithelium | Pozarowska et al. [249] |
| Bimatoprost 0.03% triggered accommodative spasm and the patient manifested pseudomyopia | bimatoprost 0.03% * | Accommodative system | Padhy and Rao [250] |
| Cystoid macula edema resulted after bimatoprost therapy | Lumigan 0.03% | Macula | Agange and Mosaed [251] |
| Prostaglandin use postoperatively associated with cystoid macular edema | Bimatoprost * | Macula | Wendel et al. [252] |
| A geriatric patient was found to have developed bilateral macula edema after receiving bimatoprost implants | Bimatoprost implant (Durysta) | Macula | Patel et al. [253] |
| Bimatoprost-induced inhibition of platelet activation action. | Lumigan UD® (bimatoprost 0.3 mg/mL | Platelets | Moschos et al. [254] |
| Serous retinal detachment occurred after starting the bimatoprost regimen | Bimatoprost * | Retina | Addison et al. [255] |
| Bimatoprost 0.03 and 0.01 both resulted in conjunctival congestion after topical administration | Bimatoprost 0.01% | Scleral blood vessels | Ogundele et al. [256] |
| A case report of bimatoprost inducing late onset choroidal detachment in a patient after trabeculectomy | Bimatoprost 0.03% | Choroid | Nakakura et al. [257] |
| Bimatoprost 0.03% was associated with the thickening of the choroid. | Bimatoprost 0.03% * | Choroidal layer | Akyol et al. [258] |
| In-vitro analysis of the effect of bimatoprost on lamina cribosa astrocytes revealed apoptosis | Bimatoprost Acid * | Optic nerve head astrocytes | Shin et al. [259] |
| Bimatoprost resulted in prolonged vasodilation of ocular vessels, an indication of hyperemia | Bimatoprost 0.01% or Bimatoprost 0.03% * | Pig eyes in-vivo | Ogundele et al. [260] |
* Formulation not completely stated.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zeppieri, M.; Gagliano, C.; Spadea, L.; Salati, C.; Chukwuyem, E.C.; Enaholo, E.S.; D’Esposito, F.; Musa, M. From Eye Care to Hair Growth: Bimatoprost. Pharmaceuticals 2024, 17, 561. https://doi.org/10.3390/ph17050561
AMA Style
Zeppieri M, Gagliano C, Spadea L, Salati C, Chukwuyem EC, Enaholo ES, D’Esposito F, Musa M. From Eye Care to Hair Growth: Bimatoprost. Pharmaceuticals. 2024; 17(5):561. https://doi.org/10.3390/ph17050561
Chicago/Turabian StyleZeppieri, Marco, Caterina Gagliano, Leopoldo Spadea, Carlo Salati, Ekele Caleb Chukwuyem, Ehimare Samuel Enaholo, Fabiana D’Esposito, and Mutali Musa. 2024. "From Eye Care to Hair Growth: Bimatoprost" Pharmaceuticals 17, no. 5: 561. https://doi.org/10.3390/ph17050561
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.