

Management of Upper-Limb Spasticity Using Modern Rehabilitation Techniques versus Botulinum Toxin Injections Following Stroke

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Evaluation Scales
2.3. Statistical Analysis
3. Results
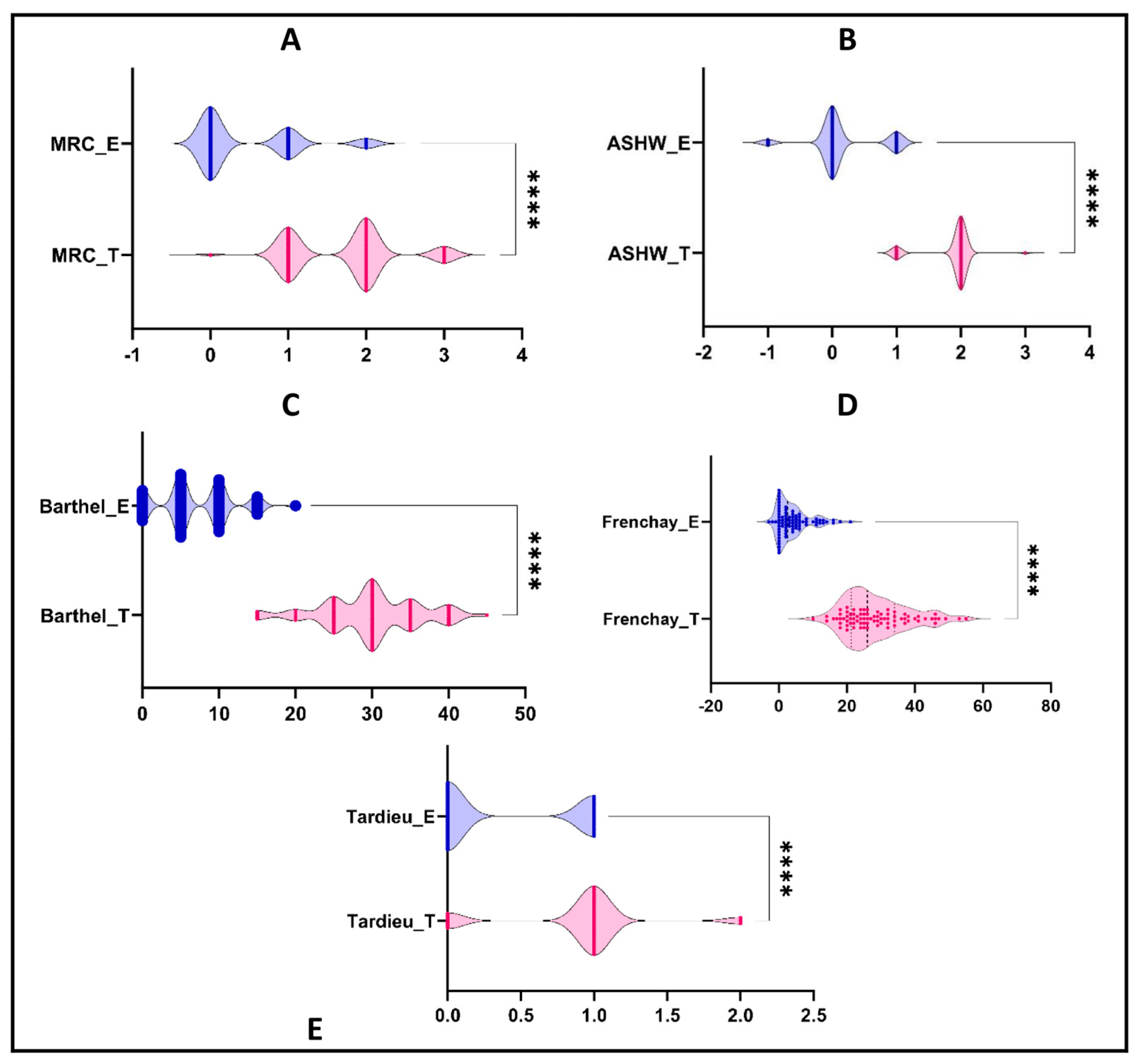
3.1. The Effect of BTx Injection and Electrostimulation on Upper Limb Spasticity
3.2. Differences between the Improvements of the Analyzed Scales between the Two Treatments
3.3. Correlations between the Measured Scales
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wajngarten, M.; Silva, G.S. Hypertension and Stroke: Update on Treatment. Eur. Cardiol. Rev. 2019, 14, 111–115. [Google Scholar] [CrossRef]
- Feigin, V.L.; Brainin, M.; Norrving, B.; Martins, S.; Sacco, R.L.; Hacke, W.; Fisher, M.; Pandian, J.; Lindsay, P. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int. J. Stroke 2022, 17, 18–29, Erratum in Int. J. Stroke 2022, 17, 478. [Google Scholar] [CrossRef] [PubMed]
- Guard Report. Available online: https://raportuldegarda.ro/infografic-accidentul-vascular-cerebral-romania/ (accessed on 24 August 2023).
- Wafa, H.A.; Wolfe, C.D.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of Stroke in Europe: Thirty-Year Projections of Incidence, Prevalence, Deaths, and Disability-Adjusted Life Years. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef] [PubMed]
- Coculescu, B.-I.; Stocheci, C.M.; Totan, A.R.; Coculescu, E.C. A statistical analysis of acute ischemic stroke before and during the COVID-19 pandemic. Rom. J. Med. Pract. 2022, 17, 41–46. [Google Scholar] [CrossRef]
- Safe Stroke. Available online: https://www.safestroke.eu/wp-content/uploads/2017/12/SAFE_STROKE_ROMANIA.pdf (accessed on 12 October 2023).
- WHO. Available online: https://data.who.int/countries/642 (accessed on 24 August 2023).
- Markus, H.; Pereira, A. Oxford Specialist Handbooks in Neurology Stroke Medicine, 2nd ed.; Oxford University Press: Oxford, UK, 2017; pp. 462–466. [Google Scholar]
- Ropper, A.H.; Samuels, M.A.; Klein, J.P.; Prasad, S. Adams and Victor’s Principles of Neurology, 11th ed.; McGraw-Hill Education: New York, NY, USA, 2019; Volume 65–66, pp. 798–801. [Google Scholar]
- Trompetto, C.; Marinelli, L.; Mori, L.; Pelosin, E.; Currà, A.; Molfetta, L.; Abbruzzese, G. Pathophysiology of Spasticity: Implications for Neurorehabilitation. BioMed Res. Int. 2014, 2014, 354906. [Google Scholar] [CrossRef]
- Lan, Y.; Yao, J.; Dewald, J.P.A. The impact of shoulder abduction loading on volitional hand opening and grasping in chronic hemiparetic stroke. Neurorehabilit. Neural Repair 2017, 31, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Moeini-Naghani, I.; Hashemi-Zonouz, T.; Jabbari, B. Botulinum Toxin Treatment of Spasticity in Adults and Children. Semin. Neurol. 2016, 36, 064–072. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Francisco, G.E. New insights into the pathophysiology of post-stroke spasticity. Front. Hum. Neurosci. 2015, 9, 192. [Google Scholar] [CrossRef]
- Simpson, D.M.; Patel, A.T.; Alfaro, A.; Ayyoub, Z.; Charles, D.; Dashtipour, K.; Esquenazi, A.; Graham, G.D.; McGuire, J.R.; Odderson, I. OnabotulinumtoxinA Injection for Poststroke Upper-Limb Spasticity: Guidance for Early Injectors from a Delphi Panel Process. PM&R 2016, 9, 136–148. [Google Scholar] [CrossRef]
- Opheim, A.; Danielsson, A.; Murphy, M.A.; Persson, H.C.; Sunnerhagen, K.S. Upper-limb spasticity during the first year after stroke: Stroke arm longitudinal study at the University of Gothenburg. Am. J. Phys. Med. Rehabil. 2014, 93, 884–896. [Google Scholar] [CrossRef]
- Rosales, R.L.; Balcaitiene, J.; Berard, H.; Maisonobe, P.; Goh, K.J.; Kumthornthip, W.; Mazlan, M.; Latif, L.A.; Santos, M.M.D.D.; Chotiyarnwong, C.; et al. Early AbobotulinumtoxinA (Dysport®) in Post-Stroke Adult Upper Limb Spasticity. Toxins 2018, 10, 253. [Google Scholar] [CrossRef] [PubMed]
- Beer, R.F.; Dewald, J.P.; Rymer, W.Z. Deficits in the coordination of multijoint arm movements in patients with hemiparesis: Evidence for disturbed control of limb dynamics. Exp. Brain Res. 2000, 131, 305–319. [Google Scholar] [CrossRef]
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum Neurotoxins: Biology, Pharmacology, and Toxicology. Pharmacol. Rev. 2017, 69, 200–235. [Google Scholar] [CrossRef] [PubMed]
- Muscle Power Assessment Scale. Available online: https://geekymedics.com/muscle-power-assessment-mrc-scale/ (accessed on 27 September 2023).
- Manual of Stroke. Available online: https://www.stroke-manual.com/barthel-index/ (accessed on 24 August 2023).
- Modified Ashworth Scale. Available online: https://strokengine.ca/en/assessments/modified-ashworth-scale/ (accessed on 24 August 2023).
- Marvin, K.; Korner-Bitensky, N.; McDermott, A.O.T. Tardieu Scale and Modified Tardieu Scale (MTS), Stroke Engine. 2011. Available online: https://strokengine.ca/en/assessments/tardieu-scale-and-modified-tardieu-scale-mts/ (accessed on 12 October 2023).
- Gracies, J.-M.; Marosszeky, J.E.; Renton, R.; Sandanam, J.; Gandevia, S.C.; Burke, D. Short-term effects of dynamic Lycra splints on upper limb in hemiplegic patients. Arch. Phys. Med. Rehabil. 2000, 81, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- Tardieu Scale. Available online: https://www.physio-pedia.com/Tardieu_Scale (accessed on 12 October 2023).
- Laclergue, Z.; Ghédira, M.; Gault-Colas, C.; Billy, L.; Gracies, J.-M.; Baude, M. Reliability of the Modified Frenchay Scale for the Assessment of Upper Limb Function in Adults with Hemiparesis. Arch. Phys. Med. Rehabil. 2023, 104, 1596–1605. [Google Scholar] [CrossRef] [PubMed]
- Modified Frenchay Scale. Available online: https://neuroloco.wixsite.com/mfs-scale (accessed on 12 October 2023).
- Martínez, I.M.; Sempere-Rubio, N.; Navarro, O.; Faubel, R. Effectiveness of Shock Wave Therapy as a Treatment for Spasticity: A Systematic Review. Brain Sci. 2020, 11, 15. [Google Scholar] [CrossRef]
- Dymarek, R.; Ptaszkowski, K.; Ptaszkowska, L.; Kowal, M.; Sopel, M.; Taradaj, J.; Rosińczuk, J. Shock Waves as a Treatment Modality for Spasticity Reduction and Recovery Improvement in Post-Stroke Adults—Current Evidence and Qualitative Systematic Review. Clin. Interv. Aging 2020, 15, 9–28. [Google Scholar] [CrossRef]
- Kamo, T.; Wada, Y.; Okamura, M.; Sakai, K.; Momosaki, R.; Taito, S. Repetitive peripheral magnetic stimulation for impairment and disability in people after stroke. Cochrane Database Syst. Rev. 2022, 2022, CD011968. [Google Scholar] [CrossRef]
- Fheodoroff, K.; Ashford, S.; Jacinto, J.; Maisonobe, P.; Balcaitiene, J.; Turner-Stokes, L. Factors Influencing Goal Attainment in Patients with Post-Stroke Upper Limb Spasticity Following Treatment with Botulinum Toxin A in Real-Life Clinical Practice: Sub-Analyses from the Upper Limb International Spasticity (ULIS)-II Study. Toxins 2015, 7, 1192–1205. [Google Scholar] [CrossRef]
- Mas, M.; Li, S.; Francisco, G. Centrally mediated late motor recovery after botulinum toxin injection: Case reports and a review of current evidence. J. Rehabilitation Med. 2017, 49, 609–619. [Google Scholar] [CrossRef]
- Lee, J.-M.; Gracies, J.-M.; Park, S.-B.; Lee, K.H.; Lee, J.Y.; Shin, J.-H. Botulinum Toxin Injections and Electrical Stimulation for Spastic Paresis Improve Active Hand Function Following Stroke. Toxins 2018, 10, 426. [Google Scholar] [CrossRef] [PubMed]
- Picelli, A.; Roncari, L.; Baldessarelli, S.; Berto, G.; Lobba, D.; Santamato, A.; Fiore, P.; Smania, N. Accuracy of botulinum toxin type A injection into the forearm muscles of chronic stroke patients with spastic flexed wrist and clenched fist: Manual needle placement evaluated using ultrasonography. J. Rehabil. Med. 2014, 46, 1042–1045. [Google Scholar] [CrossRef]
- Azzollini, V.; Dalise, S.; Chisari, C. How, Does Stroke Affect Skeletal Muscle? State of the Art and Rehabilitation Perspective, Review article. Front. Neurol. 2021, 12, 797559. [Google Scholar] [CrossRef] [PubMed]
- Teasell, R.; Foley, N.; Pereira, S.; Sequeira, K.; Miller, T. Evidence to Practice: Botulinum Toxin in the Treatment of Spasticity Post Stroke. Top. Stroke Rehabil. 2012, 19, 115–121. [Google Scholar] [CrossRef]
- Rekand, T.; Biering-Sörensen, B.; He, J.; Vilholm, O.J.; Christensen, P.B.; Ulfarsson, T.; Belusa, R.; Ström, T.; Myrenfors, P.; Maisonobe, P.; et al. Botulinum toxin treatment of spasticity targeted to muscle endplates: An international, randomised, evaluator-blinded study comparing two different botulinum toxin injection strategies for the treatment of upper limb spasticity. BMJ Open 2019, 9, e024340. [Google Scholar] [CrossRef]
- Wissel, J.; Fheodoroff, K.; Hoonhorst, M.; Müngersdorf, M.; Gallien, P.; Meier, N.; Hamacher, J.; Hefter, H.; Maisonobe, P.; Koch, M. Effectiveness of AbobotulinumtoxinA in Post-stroke Upper Limb Spasticity in Relation to Timing of Treatment. Front. Neurol. 2020, 11, 104. [Google Scholar] [CrossRef]
- Owen, M.; Ingo, C.; Dewald, J.P.A. Upper Extremity Motor Impairments and Microstructural Changes in Bulbospinal Pathways in Chronic Hemiparetic Stroke. Front. Neurol. 2017, 8, 257. [Google Scholar] [CrossRef]
- Hesse, S.; Mach, H.; Fröhlich, S.; Behrend, S.; Werner, C.; Melzer, I. An early botulinum toxin A treatment in subacute stroke patients may prevent a disabling finger flexor stiffness six months later: A randomized controlled trial. Clin. Rehabil. 2012, 26, 237–245. [Google Scholar] [CrossRef]
- Meythaler, J.M.; Vogtle, L.; Brunner, R.C. A preliminary assessment of the benefits of the addition of botulinum toxin a to a conventional therapy program on the function of people with longstanding stroke. Arch. Phys. Med. Rehabil. 2009, 90, 1453–1461. [Google Scholar] [CrossRef]
- Francisco, G.; Balbert, A.; Bavikatte, G.; Bensmail, D.; Carda, S.; Deltombe, T.; Draulans, N.; Escaldi, S.; Gross, R.; Jacinto, J.; et al. A practical guide to optimizing the benefits of post-stroke spasticity interventions with botulinum toxin A: An international group consensus. J. Rehabil. Med. 2021, 53, jrm00134. [Google Scholar] [CrossRef]
- Rousseaux, M.; Kozlowski, O.; Froger, J. Efficacy of botulinum toxin A in upper limb function of hemiplegic patients. J. Neurol. 2002, 249, 76–84. [Google Scholar] [CrossRef]
- Brashear, A.; Gordon, M.F.; Elovic, E.; Kassicieh, V.D.; Marciniak, C.; Do, M.; Lee, C.-H.; Jenkins, S.; Turkel, C. Intramuscular Injection of Botulinum Toxin for the Treatment of Wrist and Finger Spasticity after a Stroke. N. Engl. J. Med. 2002, 347, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Turner-Stokes, L.; Fheodoroff, K.; Jacinto, J. Results from the Upper Limb International Spasticity Study-II (ULIS-II): A large, international, prospective cohort study investigating practice and goal attainment following treatment with botulinum toxin A in real-life clinical management. BMJ Open 2013, 3, e002771. [Google Scholar] [CrossRef]
- Turcu-Stiolica, A.; Subtirelu, M.-S.; Bumbea, A.-M. Can Incobotulinumtoxin-A Treatment Improve Quality of Life Better Than Conventional Therapy in Spastic Muscle Post-Stroke Patients? Results from a Pilot Study from a Single Center. Brain Sci. 2021, 11, 934. [Google Scholar] [CrossRef]
- El Husseini, N.; Katzan, I.L.; Rost, N.S.; Blake, M.L.; Byun, E.; Pendlebury, S.T.; Aparicio, H.J.; Marquine, M.J.; Gottesman, R.F.; Smith, E.E.; et al. Cognitive Impairment After Ischemic and Hemorrhagic Stroke: A Scientific Statement from the American Heart Association/American Stroke Association. Stroke 2023, 54, E272–E291. [Google Scholar] [CrossRef]
- Constantin, A.-M.; Mihu, C.M.; Boşca, A.B.; Melincovici, C.S.; Mărginean, M.V.; Jianu, E.M.; Onofrei, M.M.; Micu, C.M.; Alexandru, B.C.; Sufleţel, R.T.; et al. Short histological kaleidoscope—Recent findings in histology. Part III. Rom. J. Morphol. Embryol. 2023, 64, 115–133. [Google Scholar] [CrossRef]
- Onose, G.; Anghelescu, A.; Blendea, D.; Ciobanu, V.; Daia, C.; Firan, F.C.; Oprea, M.; Spinu, A.; Popescu, C.; Ionescu, A.; et al. Cellular and Molecular Targets for Non-Invasive, Non-Pharmacological Therapeutic/Rehabilitative Interventions in Acute Ischemic Stroke. Int. J. Mol. Sci. 2022, 23, 907. [Google Scholar] [CrossRef]
- Turcu-Stiolica, A.; Subtirelu, M.-S.; Bumbea, A.-M. Cost-utility analysis of incobotulinumtoxin-A compared with conventional therapy in the management of post-stroke spasticity in Romania. Front. Pharmacol. 2019, 10, 1516. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.-T.; Yong, V.; Chen, H.-W.; Saito, Y. Disabled life expectancy with and without stroke: A 10-year Japanese prospective cohort study. Qual. Life Res. 2019, 28, 3055–3064. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.W.; Hong, B.Y.; Jo, L.; Kim, J.-S.; Park, J.G.; Shin, B.K.; Lim, S.H. Effects of Age on Long-Term Functional Recovery in Patients with Stroke. Medicina 2020, 56, 451. [Google Scholar] [CrossRef] [PubMed]
- Belagaje, S.R. Stroke Rehabilitation. Contin. Lifelong Learn. Neurol. 2017, 23, 238–253. [Google Scholar] [CrossRef] [PubMed]
- Doan, T.-N.; Kuo, M.-Y.; Chou, L.-W. Efficacy and Optimal Dose of Botulinum Toxin A in Post-Stroke Lower Extremity Spasticity: A Systematic Review and Meta-Analysis. Toxins 2021, 13, 428. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.-C.; Chang, K.-V.; Chiu, Y.-H.; Wu, W.-T.; Özçakar, L. Comparative Effectiveness of Botulinum Toxin Injections and Extracorporeal Shockwave Therapy for Post-Stroke Spasticity: A Systematic Review and Network Meta-Analysis. eClinical Med. 2021, 43, 101222. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Mao, G.; Xie, Y.; Cao, S.; Zhou, S.; Jiang, J.; Yao, T.; Fan, J.; Liu, D.; Kang, F.; et al. Efficacy of baishao luoshi decoction on synaptic plasticity in rats with post stroke spasticity. J. Tradit. Chin. Med. 2023, 43, 295–302. [Google Scholar] [CrossRef]
- Trompetto, C.; Marinelli, L.; Mori, L.; Puce, L.; Avanti, C.; Saretti, E.; Biasotti, G.; Amella, R.; Cotellessa, F.; Restivo, D.A.; et al. Effectiveness of Botulinum Toxin on Pain in Stroke Patients Suffering from Upper Limb Spastic Dystonia. Toxins 2022, 14, 39. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Botulinum Toxin Group (BT Group) (n = 80) | Electrostimulation and Shockwave Group (ES Group) (n = 80) | p-Value |
|---|---|---|---|
| Age, years | 58.74 ± 10.56 61.5 (54.25–66) | 67.76 ± 10.51 67 (62.3–74.5) | <0.0001 |
| Gender, male | 47 (58.8%) | 44 (55.0%) | 0.750 |
| Time since stroke | 3.52 ± 2.09 3 (2–5) | 3.39 ± 2.92 2 (1–5) | 0.124 |
| Stroke type Ischemic Hemorrhagic | 51 (63.8%) 29 (36.2%) | 55 (68.8%) 25 (31.2%) | 0.616 |
| Hypertension, yes | 74 (92.5%) | 78 (97.5%) | 0.276 |
| Coronary heart disease, yes | 65 (81.3%) | 78 (97.5%) | 0.001 *** |
| Atrial fibrillation, yes | 34 (42.5%) | 42 (52.5%) | 0.268 |
| Diabetes, yes | 28 (35.0%) | 24 (30.0%) | 0.613 |
| Dyslipidemia, yes | 66 (82.5%) | 73 (91.3%) | 0.159 |
| Characteristics Mean ± SD Median (IQR) | Botulinum Toxin Group (BT Group) (n = 80) | Electrostimulation and Shockwave Group (ES Group) (n = 80) | ||||
|---|---|---|---|---|---|---|
| Baseline | Post-Treatment | p-Value | Baseline | Post-Treatment | p-Value | |
| Medical Research Council scale | 1.6 ± 0.5 2 (1–2) | 3.3 ± 0.7 3 (3–4) | <0.0001 **** | 1.8 ± 0.6 2 (1–2) | 2.2 ± 0.7 2 (2–3) | <0.0001 **** |
| Ashworth | 3.1 ± 0.2 3 (3–3) | 1.2 ± 0.4 1 (1–1) | <0.0001 **** | 2.5 ± 0.8 3 (2–3) | 2.4 ± 0.6 2 (2–3) | 0.1745 |
| Frenchay | 19.4 ± 9.3 20 (11–28.8) | 47.9 ± 7.7 48 (42.3–53) | <0.0001 **** | 24.6 ± 10.8 25 (13.5–32) | 28.8 ± 11.3 30 (22–34) | 0.0180 * |
| Tardieu | 3.4 ± 0.6 3 (3–4) | 2.5 ± 0.5 2 (2–3) | <0.0001 **** | 3.1 ± 0.7 3 (3–3) | 2.8 ± 0.6 3 (2–3) | 0.0006 *** |
| Barthel | 25 ± 6.9 25 (20–30) | 54.8 ± 7.3 55 (50–60) | <0.0001 **** | 26.9 ± 10.6 25 (20–35) | 33.9 ± 11.2 35 (25–40) | 0.0001 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bumbea, A.M.; Rogoveanu, O.C.; Turcu-Stiolica, A.; Pirici, I.; Cioroianu, G.; Stanca, D.I.; Criciotoiu, O.; Biciusca, V.; Traistaru, R.M.; Caimac, D.V. Management of Upper-Limb Spasticity Using Modern Rehabilitation Techniques versus Botulinum Toxin Injections Following Stroke. Life 2023, 13, 2218. https://doi.org/10.3390/life13112218
Bumbea AM, Rogoveanu OC, Turcu-Stiolica A, Pirici I, Cioroianu G, Stanca DI, Criciotoiu O, Biciusca V, Traistaru RM, Caimac DV. Management of Upper-Limb Spasticity Using Modern Rehabilitation Techniques versus Botulinum Toxin Injections Following Stroke. Life. 2023; 13(11):2218. https://doi.org/10.3390/life13112218
Chicago/Turabian StyleBumbea, Ana Maria, Otilia Constantina Rogoveanu, Adina Turcu-Stiolica, Ionica Pirici, George Cioroianu, Diana Iulia Stanca, Oana Criciotoiu, Viorel Biciusca, Rodica Magdalena Traistaru, and Danut Visarion Caimac. 2023. "Management of Upper-Limb Spasticity Using Modern Rehabilitation Techniques versus Botulinum Toxin Injections Following Stroke" Life 13, no. 11: 2218. https://doi.org/10.3390/life13112218