
Consumption of Tree Nuts as Snacks Reduces Metabolic Syndrome Risk in Young Adults: A Randomized Trial


Abstract
:1. Introduction
2. Materials and Methods
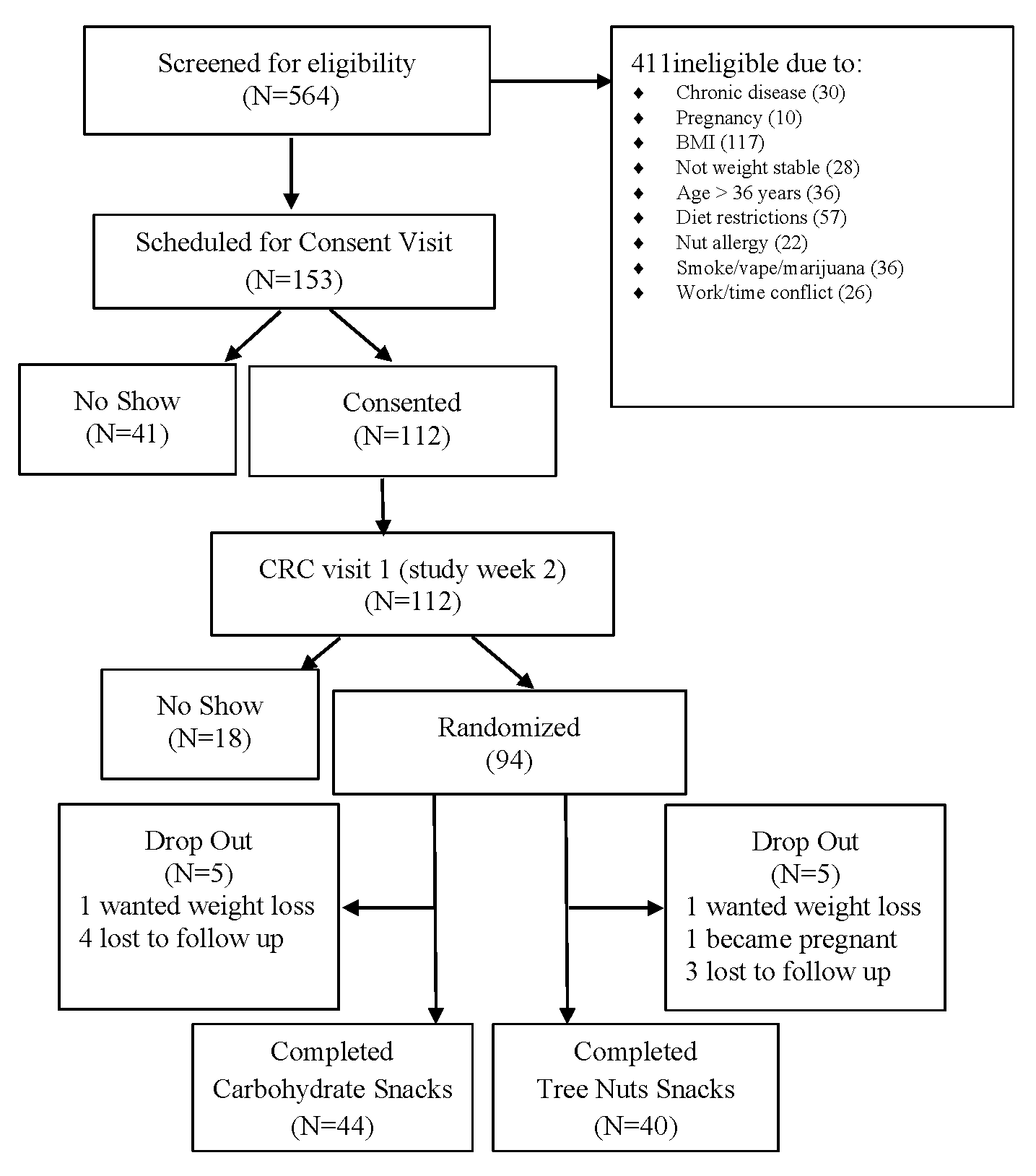
2.1. Recruitment and Participants
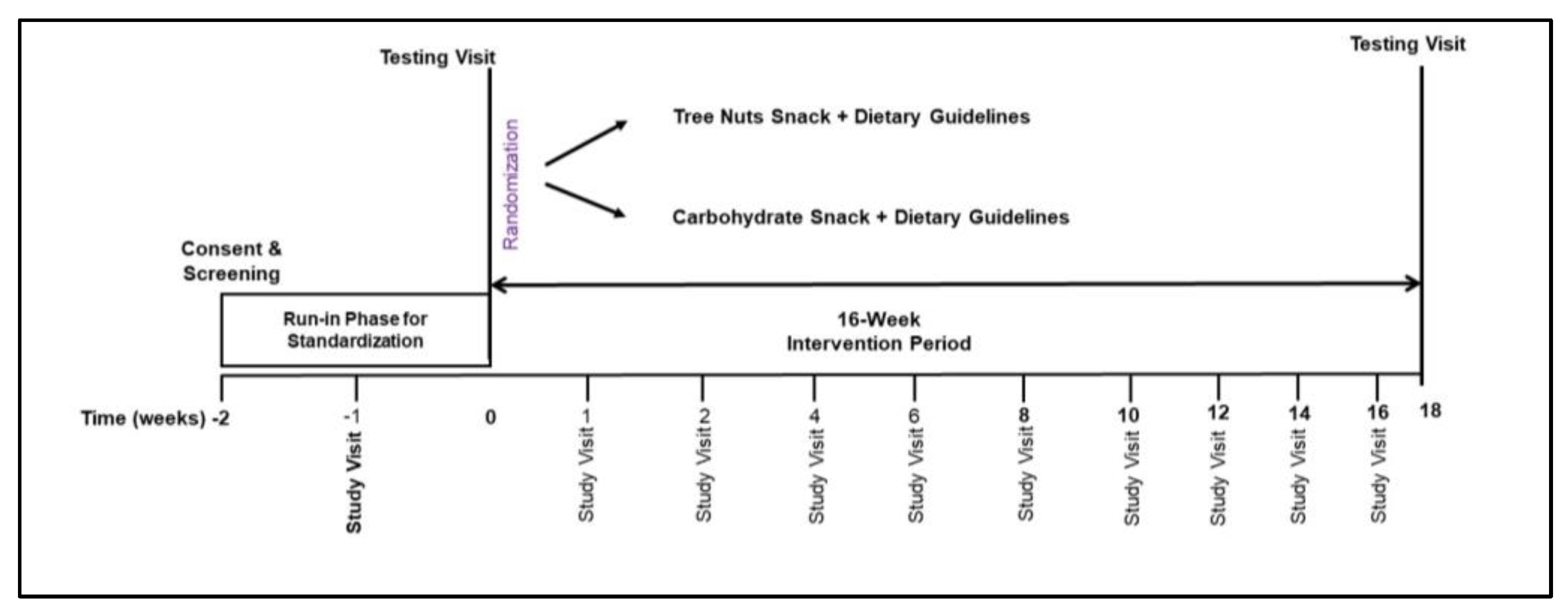
2.2. Study Design
2.3. Diet and Snack Intervention
2.4. Anthropometrics and Computed Tomography Morphometrics
2.5. Resting Energy Expenditure
2.6. Physical Activity Monitoring
2.7. Clinical Biomarkers
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Sample
3.2. Effects of Snack Treatment on Dietary Intakes and Physical Activity
3.3. Effects of Snack Treatment on Weight, Waist Circumference, Body Composition, and Energy Expenditure
3.4. Effects of Snack Treatment on Clinical Biomarkers and Metabolic Syndrome Risk Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hirode, G.; Wong, R.J. Trends in the Prevalence of Metabolic Syndrome in the United States, 2011–2016. JAMA 2020, 323, 2526–2528. [Google Scholar] [CrossRef]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist Circumference as a Vital Sign in Clinical Practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Kuczmarski, M.T.F.; Wang, Y.; Mason, M.A.; Evans, M.K.; Zonderman, A.B. Receiver-Operating Characteristics of Adiposity for Metabolic Syndrome: The Healthy Aging in Neighborhoods of Diversity across the Life Span (HANDLS) Study. Public Health Nutr. 2011, 14, 77–92. [Google Scholar] [CrossRef]
- Shen, W.; Punyanitya, M.; Chen, J.; Gallagher, D.; Albu, J.; Pi-Sunyer, X.; Lewis, C.E.; Grunfeld, C.; Heshka, S.; Heymsfield, S.B. Waist Circumference Correlates with Metabolic Syndrome Indicators Better than Percentage Fat. Obesity 2006, 14, 727–736. [Google Scholar] [CrossRef]
- Albrecht, S.S.; Gordon-Larsen, P.; Stern, D.; Popkin, B.M. Is Waist Circumference per Body Mass Index Rising Differentially across the United States, England, China and Mexico? Eur. J. Clin. Nutr. 2015, 69, 1306–1312. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Maynard, L.M.; Li, C. Trends in Mean Waist Circumference and Abdominal Obesity among US Adults, 1999–2012. JAMA 2014, 312, 1151–1153. [Google Scholar] [CrossRef] [PubMed]
- Nolan, P.B.; Carrick-Ranson, G.; Stinear, J.W.; Reading, S.A.; Dalleck, L.C. Prevalence of Metabolic Syndrome and Metabolic Syndrome Components in Young Adults: A Pooled Analysis. Prev. Med. Rep. 2017, 7, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; Micha, R.; Wu, J.H.Y.; de Otto, M.C.O.; Otite, F.O.; Abioye, A.I.; Mozaffarian, D. Effects of Saturated Fat, Polyunsaturated Fat, Monounsaturated Fat, and Carbohydrate on Glucose-Insulin Homeostasis: A Systematic Review and Meta-Analysis of Randomised Controlled Feeding Trials. PLoS Med. 2016, 13, e1002087. [Google Scholar] [CrossRef]
- Vafeiadou, K.; Weech, M.; Altowaijri, H.; Todd, S.; Yaqoob, P.; Jackson, K.G.; Lovegrove, J.A. Replacement of Saturated with Unsaturated Fats Had No Impact on Vascular Function but Beneficial Effects on Lipid Biomarkers, E-Selectin, and Blood Pressure: Results from the Randomized, Controlled Dietary Intervention and VAScular Function (DIVAS) Study. Am. J. Clin. Nutr. 2015, 102, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Bao, Y.; Han, J.; Hu, F.B.; Giovannucci, E.L.; Stampfer, M.J.; Willett, W.C.; Fuchs, C.S. Association of Nut Consumption with Total and Cause-Specific Mortality. N. Engl. J. Med. 2013, 369, 2001–2011. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Montero, A.; Bes-Rastrollo, M.; Beunza, J.J.; Barrio-Lopez, M.T.; de la Fuente-Arrillaga, C.; Moreno-Galarraga, L.; Martínez-González, M.A. Nut Consumption and Incidence of Metabolic Syndrome after 6-Year Follow-up: The SUN (Seguimiento Universidad de Navarra, University of Navarra Follow-up) Cohort. Public Health Nutr. 2013, 16, 2064–2072. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferré, M.; Bulló, M.; Martínez-González, M.Á.; Ros, E.; Corella, D.; Estruch, R.; Fitó, M.; Arós, F.; Wärnberg, J.; Fiol, M.; et al. Frequency of Nut Consumption and Mortality Risk in the PREDIMED Nutrition Intervention Trial. BMC Med. 2013, 11, 164. [Google Scholar] [CrossRef] [PubMed]
- Jaceldo-Siegl, K.; Haddad, E.; Oda, K.; Fraser, G.E.; Sabaté, J. Tree Nuts Are Inversely Associated with Metabolic Syndrome and Obesity: The Adventist Health Study-2. PLoS ONE 2014, 9, e85133. [Google Scholar] [CrossRef]
- Li, H.; Li, X.; Yuan, S.; Jin, Y.; Lu, J. Nut Consumption and Risk of Metabolic Syndrome and Overweight/Obesity: A Meta-Analysis of Prospective Cohort Studies and Randomized Trials. Nutr. Metab. 2018, 15, 46. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, R.; Mesas, A.E.; Garrido-Miguel, M.; Martínez-Ortega, I.A.; Jiménez-López, E.; Martínez-Vizcaíno, V. The Relationship of Tree Nuts and Peanuts with Adiposity Parameters: A Systematic Review and Network Meta-Analysis. Nutrients 2021, 13, 2251. [Google Scholar] [CrossRef] [PubMed]
- Dietary Guidelines for Americans, 2020–2025; US Department of Agriculture, US Department of Health and Human Services: Washington, DC, USA, 2020.
- The Fourth Annual State of Snacking 2022 Global Consumer Trends Study. Available online: https://www.mondelezinternational.com/ (accessed on 30 December 2022).
- Piernas, C.; Popkin, B.M. Snacking Increased among U.S. Adults between 1977 and 2006. J. Nutr. 2010, 140, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, R.S.; Enns, C.W.; Goldman, J.D. Snacking Patterns of U.S. Adults: What We Eat in America, NHANES 2007–2008. In FSRG Dietary Data Briefs; United States Department of Agriculture (USDA): Beltsville, MD, USA, 2010. [Google Scholar]
- Nuts and Dried Fruit Statistical Yearbook 2022/2023. Available online: https://inc.nutfruit.org/wp-content/uploads/2023/05/Statistical-Yearbook-2022-2023.pdf (accessed on 30 December 2022).
- Nielsen, S.J.; Kit, B.K.; Ogden, C.L. Nut Consumption among U.S. Adults, 2009–2010. NCHS Data Brief 2014, 176, 1–8. [Google Scholar]
- Hess, J.; Rao, G.; Slavin, J. The Nutrient Density of Snacks: A Comparison of Nutrient Profiles of Popular Snack Foods Using the Nutrient-Rich Foods Index. Glob. Pediatr. Health 2017, 4, 2333794X17698525. [Google Scholar] [CrossRef]
- Rehm, C.D.; Drewnowski, A. Replacing American Snacks with Tree Nuts Increases Consumption of Key Nutrients among US Children and Adults: Results of an NHANES Modeling Study. Nutr. J. 2017, 16, 17. [Google Scholar] [CrossRef]
- Martinson, M.L.; Lapham, J.; Ercin-Swearinger, H.; Teitler, J.O.; Reichman, N.E. Generational Shifts in Young Adult Cardiovascular Health? Millennials and Generation X in the United States and England. J. Gerontol. B Psychol. Sci. Soc. Sci. 2022, 77, S177–S188. [Google Scholar] [CrossRef]
- Pereira, M.A.; Jacobs, D.R.; Van Horn, L.; Slattery, M.L.; Kartashov, A.I.; Ludwig, D.S. Dairy Consumption, Obesity, and the Insulin Resistance Syndrome in Young Adults: The CARDIA Study. JAMA 2002, 287, 2081–2089. [Google Scholar] [CrossRef]
- Arnold, M.J.; Harding, M.C.; Conley, A.T. Dietary Guidelines for Americans 2020–2025: Recommendations from the U.S. Departments of Agriculture and Health and Human Services. Am. Fam. Physician 2021, 104, 533–536. [Google Scholar]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids. (Commentary). J. Am. Diet. Assoc. 2002, 102, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, D.G.; Murayi, T.; Clemens, J.C.; Baer, D.J.; Sebastian, R.S.; Moshfegh, A.J. The USDA Automated Multiple-Pass Method Accurately Assesses Population Sodium Intakes. Am. J. Clin. Nutr. 2013, 97, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Kaess, B.M.; Pedley, A.; Massaro, J.M.; Murabito, J.; Hoffmann, U.; Fox, C.S. The Ratio of Visceral to Subcutaneous Fat, a Metric of Body Fat Distribution, Is a Unique Correlate of Cardiometabolic Risk. Diabetologia 2012, 55, 2622–2630. [Google Scholar] [CrossRef]
- Weir, J.B.D.B. New Methods for Calculating Metabolic Rate with Special Reference to Protein Metabolism. J. Physiol. 1949, 109, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Frayn, K.N. Calculation of Substrate Oxidation Rates in Vivo from Gaseous Exchange. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1983, 55, 628–634. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Keast, D.R.; Nicklas, T.A.; Fulgoni, V.L. Nut Consumption Is Associated with Decreased Health Risk Factors for Cardiovascular Disease and Metabolic Syndrome in U.S. Adults: NHANES 1999–2004. J. Am. Coll. Nutr. 2011, 30, 502–510. [Google Scholar] [CrossRef]
- Ibarrola-Jurado, N.; Bulló, M.; Guasch-Ferré, M.; Ros, E.; Martínez-González, M.A.; Corella, D.; Fiol, M.; Wärnberg, J.; Estruch, R.; Román, P.; et al. Cross-Sectional Assessment of Nut Consumption and Obesity, Metabolic Syndrome and Other Cardiometabolic Risk Factors: The PREDIMED Study. PLoS ONE 2013, 8, e57367. [Google Scholar] [CrossRef]
- Hosseinpour-Niazi, S.; Hosseini, S.; Mirmiran, P.; Azizi, F. Prospective Study of Nut Consumption and Incidence of Metabolic Syndrome: Tehran Lipid and Glucose Study. Nutrients 2017, 9, 1056. [Google Scholar] [CrossRef]
- Alasalvar, C.; Salvadó, J.-S.; Ros, E. Bioactives and Health Benefits of Nuts and Dried Fruits. Food Chem. 2020, 314, 126192. [Google Scholar] [CrossRef] [PubMed]
- Katsoulis, M.; Lai, A.G.; Diaz-Ordaz, K.; Gomes, M.; Pasea, L.; Banerjee, A.; Denaxas, S.; Tsilidis, K.; Lagiou, P.; Misirli, G.; et al. Identifying Adults at High-Risk for Change in Weight and BMI in England: A Longitudinal, Large-Scale, Population-Based Cohort Study Using Electronic Health Records. Lancet Diabetes Endocrinol. 2021, 9, 681–694. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.Y.; Mattes, R.D. Appetitive, Dietary and Health Effects of Almonds Consumed with Meals or as Snacks: A Randomized, Controlled Trial. Eur. J. Clin. Nutr. 2013, 67, 1205–1214. [Google Scholar] [CrossRef] [PubMed]
- Zaveri, S.; Drummond, S. The Effect of Including a Conventional Snack (Cereal Bar) and a Nonconventional Snack (Almonds) on Hunger, Eating Frequency, Dietary Intake and Body Weight. J. Hum. Nutr. Diet. 2009, 22, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Swiatkiewicz, I.; Wozniak, A.; Taub, P.R. Time-Restricted Eating and Metabolic Syndrome: Current Status and Future Perspectives. Nutrients 2021, 13, 221. [Google Scholar] [CrossRef]
- Liu, B.; Du, Y.; Wu, Y.; Snetselaar, L.G.; Wallace, R.B.; Bao, W. Trends in Obesity and Adiposity Measures by Race or Ethnicity among Adults in the United States 2011–2018: Population Based Study. BMJ 2021, 372, n365. [Google Scholar] [CrossRef]
- Kuk, J.L.; Lee, S.; Heymsfield, S.B.; Ross, R. Waist Circumference and Abdominal Adipose Tissue Distribution: Influence of Age and Sex. Am. J. Clin. Nutr. 2005, 81, 1330–1334. [Google Scholar] [CrossRef]
- Ebbert, J.O.; Jensen, M.D. Fat Depots, Free Fatty Acids, and Dyslipidemia. Nutrients 2013, 5, 498–508. [Google Scholar] [CrossRef]
- Jones, P.J.; Pencharz, P.B.; Clandinin, M.T. Whole Body Oxidation of Dietary Fatty Acids: Implications for Energy Utilization. Am. J. Clin. Nutr. 1985, 42, 769–777. [Google Scholar] [CrossRef]
- Sanz, M.; Lopez-Bote, C.J.; Menoyo, D.; Bautista, J.M. Abdominal Fat Deposition and Fatty Acid Synthesis Are Lower and Beta-Oxidation Is Higher in Broiler Chickens Fed Diets Containing Unsaturated Rather than Saturated Fat. J. Nutr. 2000, 130, 3034–3037. [Google Scholar] [CrossRef]
- Okuno, M.; Kajiwara, K.; Imai, S.; Kobayashi, T.; Honma, N.; Maki, T.; Suruga, K.; Goda, T.; Takase, S.; Muto, Y.; et al. Perilla Oil Prevents the Excessive Growth of Visceral Adipose Tissue in Rats by Down-Regulating Adipocyte Differentiation. J. Nutr. 1997, 127, 1752–1757. [Google Scholar] [CrossRef]
- Garrido-Miguel, M.; Martinez-Vizcaino, V.; Fernandez-Rodriquez, R.; Martinez-Ortega, I.A.; Hernandez-Castillo, L.E.; Bizzozero-Peroni, B.; Ruiz-Grao, M.C.; Mesas, A.E. The Role of Physical Fitness in the Relationship between Nut Consumption and Body Composition in Young Adults. Nutrients 2021, 13, 2126. [Google Scholar] [CrossRef] [PubMed]
- Eslami, O.; Khorramrouz, F.; Sohouli, M.; Bagheri, N.; Shidfar, F.; Fernandez, M.L. Effect of Nuts on Components of Metabolic Syndrome in Healthy Adults with Overweight/Obesity: A Systematic Review and Meta-Analysis. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2459–2469. [Google Scholar] [CrossRef]
- Rezapour, M.; Shahesmaeili, A.; Hossinzadeh, A.; Zahedi, R.; Najafipour, H.; Gozashti, M.H. Comparison of Lipid Ratios to Identify Metabolic Syndrome. Arch. Iran. Med. 2018, 21, 572–577. [Google Scholar] [PubMed]
- Chauhan, A.; Singhal, A.; Goyal, P. TG/HDL Ratio: A Marker for Insulin Resistance and Atherosclerosis in Prediabetics or Not? J. Family Med. Prim. Care 2021, 10, 3700–3705. [Google Scholar] [CrossRef] [PubMed]
- Cenedella, R.J.; Allen, A. Differences between the Metabolism of Linoleic and Palmitic Acid: Utilization for Cholesterol Synthesis and Oxidation to Respiratory CO2. Lipids 1969, 4, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.J.; Schoeller, D.A. Polyunsaturated:Saturated Ratio of Diet Fat Influences Energy Substrate Utilization in the Human. Metabolism 1988, 37, 145–151. [Google Scholar] [CrossRef] [PubMed]
- DeLany, J.P.; Windhauser, M.M.; Champagne, C.M.; Bray, G.A. Differential Oxidation of Individual Dietary Fatty Acids in Humans. Am. J. Clin. Nutr. 2000, 72, 905–911. [Google Scholar] [CrossRef]
- Tapsell, L.; Batterham, M.; Tan, S.-Y.; Warensjö, E. The Effect of a Calorie Controlled Diet Containing Walnuts on Substrate Oxidation during 8-Hours in a Room Calorimeter. J. Am. Coll. Nutr. 2009, 28, 611–617. [Google Scholar] [CrossRef]
- Tindall, A.M.; Johnston, E.A.; Kris-Etherton, P.M.; Petersen, K.S. The Effect of Nuts on Markers of Glycemic Control: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Clin. Nutr. 2019, 109, 297–314. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| a. Males | ||||||||
|---|---|---|---|---|---|---|---|---|
| Tree Nuts Group | CHO Group | Treatment Effect | ||||||
| Baseline | Change | p-Value | Baseline | Change | p-Value | Mean Difference | p-Value | |
| Height (cm) | 179.52 ± 8.55 | n/a | n/a | 177.88 ± 6.46 | n/a | n/a | 1.64 ± 2.50 | 0.52 |
| Weight (kg) | 93.66 ± 12.63 | 0.29 ± 4.32 | 0.80 | 92.87 ± 14.53 | 0.57 ± 2.39 | 0.30 | 0.28 ± 1.20 | 0.80 |
| Body Mass Index (kg/m2) | 29.03 ± 3.26 | 0.13 ± 1.23 | 0.67 | 29.28 ± 3.75 | 0.18 ± 0.78 | 0.32 | 0.05 ± 0.34 | 0.89 |
| Waist Circumference (cm) | 101.95 ± 9.37 | −0.78 ± 1.11 | 0.15 | 102.33 ± 12.00 | −0.14 ± 2.17 | 0.77 | 0.64 ± 0.91 | 0.47 |
| Hip Circumference (cm) | 109.06 ± 6.33 | −0.37 ± 4.03 | 0.72 | 110.41 ± 6.56 | −0.26 ± 3.42 | 0.74 | 0.11 ± 1.24 | 0.93 |
| Waist:Hip (ratio) | 0.94 ± 0.08 | −0.01 ± 0.06 | 0.44 | 0.92 ± 0.06 | −0.01 ± 0.02 | 0.16 | 0.00 ± 0.02 | 0.77 |
| Waist:Height (ratio) | 0.57 ± 0.05 | −0.01 ± 0.03 | 0.31 | 0.58 ± 0.06 | −0.00 ± 0.02 | 0.79 | 0.00 ± 0.01 | 0.75 |
| Systolic Blood Pressure (mm Hg) | 124.83 ± 9.69 | −1.78 ± 9.46 | 0.47 | 119.90 ± 11.02 | 3.15 ± 7.67 | 0.05 | 4.92 ± 2.85 | 0.04 |
| Diastolic Blood Pressure (mm Hg) | 75.14 ± 8.07 | −0.29 ± 7.55 | 0.88 | 75.15 ± 7.41 | 0.25 ± 7.95 | 0.89 | 0.44 ± 2.58 | 0.68 |
| Physical Activity Level | 11.59 ± 7.67 | −0.73 ± 3.85 | 0.46 | 8.20 ± 3.64 | −1.11 ± 6.31 | 0.44 | 0.44 ± 1.80 | 0.61 |
| Glucose (mg/dL) | 88.88 ± 12.03 | −1.38 ± 1.19 | 0.22 | 83.20 ± 8.83 | 3.00 ± 3.53 | 0.10 | 5.23 ± 4.66 | 0.03 |
| Insulin (mIU/L) | 8.06 ± 7.63 | −1.14 ± 1.41 | 0.05 | 6.45 ± 4.04 | 1.08 ± 4.09 | 0.25 | 2.22 ± 1.60 | 0.09 |
| HOMA-IR (score) | 1.86 ± 1.97 | −0.25 ± 1.57 | 0.54 | 1.34 ± 0.89 | 0.28 ± 0.99 | 0.22 | 0.54 ± 0.43 | 0.11 |
| C Reactive Protein (mg/dL) | 2.01 ± 3.99 | −0.49 ± 4.34 | 0.66 | 2.39 ± 3.12 | 0.71 ± 2.24 | 0.17 | 1.20 ± 1.12 | 0.29 |
| Total Cholesterol (mg/dL) | 165.44 ± 31.92 | −1.89 ± 22.64 | 0.75 | 174.05 ± 33.82 | −2.00 ± 30.51 | 0.77 | 0.13 ± 9.16 | 0.98 |
| HDL-Cholesterol (mg/dL) | 48.44 ± 16.64 | −2.50 ± 9.17 | 0.20 | 46.65 ± 10.53 | −1.30 ± 6.78 | 0.40 | 1.10 ± 2.66 | 0.69 |
| LDL-Cholesterol (mg/dL) | 98.38 ± 25.17 | −2.31 ± 19.01 | 0.36 | 107.75 ± 32.16 | 4.05 ± 25.68 | 0.49 | 6.36 ± 7.45 | 0.20 |
| Triglycerides (mg/dL) | 92.94 ± 58.15 | −8.81 ± 22.78 | 0.14 | 98.45 ± 46.20 | 6.25 ± 50.13 | 0.58 | 15.06 ± 13.56 | 0.15 |
| TG:HDL (ratio) | 2.29 ± 1.96 | −0.25 ± 1.17 | 0.19 | 2.32 ± 1.38 | 4.09 ± 6.68 | 0.58 | 4.06 ± 4.92 | 0.02 |
| Metabolic Syndrome (score) | 1.94 ± 1.23 | −0.81 ± 0.54 | 0.003 | 1.70 ± 0.89 | 0.05 ± 0.60 | 0.27 | 0.86 ± 0.19 | < 0.001 |
| b. Females | ||||||||
| Tree Nuts Group | CHO Group | Treatment Effect | ||||||
| Baseline | Change | p-value | Baseline | Change | p-value | Mean Difference | p-value | |
| Height (cm) | 165.83 ± 7.75 | n/a | n/a | 165.53 ± 8.02 | n/a | n/a | 0.29 ± 2.28 | 0.90 |
| Weight (kg) | 77.91 ± 12.07 | −0.84 ± 1.55 | 0.08 | 74.67 ± 12.78 | 0.95 ± 1.52 | 0.006 | 1.72 ± 0.61 | 0.08 |
| Body Mass Index (kg/m2) | 28.31 ± 3.82 | −0.39 ± 0.94 | 0.10 | 27.17 ± 3.59 | 0.44 ± 0.54 | 0.005 | 0.05 ± 0.22 | 0.33 |
| Waist Circumference (cm) | 94.36 ± 9.94 | −1.59 ± 2.31 | 0.003 | 90.44 ± 10.77 | 0.60 ± 2.74 | 0.29 | 2.20 ± 0.73 | 0.004 |
| Hip Circumference (cm) | 110.08 ± 8.25 | −0.61 ± 3.23 | 0.37 | 107.30 ± 8.29 | 0.95 ± 3.25 | 0.17 | 1.04 ± 0.93 | 0.05 |
| Waist:Hip (ratio) | 0.86 ± 0.06 | −0.01 ± 0.03 | 0.32 | 0.84 ± 0.06 | −0.00 ± 0.04 | 0.95 | 0.01 ± 0.00 | 0.57 |
| Waist:Height (ratio) | 0.57 ± 0.06 | −0.01 ± 0.02 | 0.30 | 0.55 ± 0.06 | −0.00 ± 0.02 | 0.98 | 0.01 ± 0.01 | 0.44 |
| Systolic Blood Pressure (mm Hg) | 112.70 ± 9.87 | −0.23 ± 10.06 | 0.92 | 111.92 ± 8.23 | −0.22 ± 8.51 | 0.86 | 0.09 ± 2.81 | 0.97 |
| Diastolic Blood Pressure (mm Hg) | 73.52 ± 9.89 | −1.73 ± 8.26 | 0.34 | 72.58 ± 7.37 | −0.59 ± 6.41 | 0.67 | 1.14 ± 2.23 | 0.61 |
| Physical Activity Level | 9.28 ± 3.94 | −0.84 ± 1.05 | 0.43 | 8.56 ± 5.50 | −0.62 ± 1.56 | 0.82 | 0.22 ± 1.40 | 0.66 |
| Glucose (mg/dL) | 84.58 ± 9.04 | −1.08 ± 1.65 | 0.49 | 82.71 ± 7.88 | 0.82 ± 1.92 | 0.33 | 1.29 ± 2.68 | 0.63 |
| Insulin (mIU/L) | 10.15 ± 11.18 | −1.52 ± 1.78 | 0.13 | 7.13 ± 2.95 | 0.65 ± 1.92 | 0.13 | 1.87 ± 1.67 | 0.07 |
| HOMA-IR (score) | 2.27 ± 3.04 | −0.60 ± 0.42 | 0.15 | 1.49 ± 0.70 | 0.13 ± 0.56 | 0.27 | 0.77 ± 0.44 | 0.19 |
| C Reactive Protein (mg/dL) | 3.08 ± 2.78 | −0.52 ± 1.89 | 0.19 | 1.39 ± 1.65 | 0.57 ± 1.17 | 0.03 | 1.00 ± 0.45 | 0.04 |
| Total Cholesterol (mg/dL) | 187.63 ± 39.09 | −7.04 ± 28.31 | 0.24 | 175.83 ± 35.84 | −6.17 ± 31.39 | 0.33 | 0.95 ± 8.45 | 0.92 |
| HDL-Cholesterol (mg/dL) | 54.33 ± 14.31 | −2.46 ± 9.64 | 0.22 | 57.58 ± 13.71 | −1.04 ± 7.63 | 0.52 | 1.41 ± 2.53 | 0.58 |
| LDL-Cholesterol (mg/dL) | 115.29 ± 34.22 | −6.96 ± 31.38 | 0.29 | 102.25 ± 31.40 | −2.43 ± 23.91 | 0.63 | 4.52 ± 8.16 | 0.18 |
| Triglycerides (mg/dL) | 103.67 ± 59.56 | −6.54 ± 38.83 | 0.42 | 80.17 ± 32.38 | −13.54 ± 25.93 | 0.02 | 7.16 ± 9.67 | 0.01 |
| TG:HDL (ratio) | 2.11 ± 1.51 | −0.24 ± 0.49 | 0.02 | 1.50 ± 0.72 | 0.07 ± 0.93 | 0.03 | 0.36 ± 0.25 | 0.05 |
| Metabolic Syndrome (score) | 1.58 ± 0.83 | −1.06 ± 0.19 | 0.005 | 1.33 ± 0.38 | 0.00 ± 0.10 | <0.001 | 1.05 ± 0.13 | 0.001 |
| a. Males | ||||||||
|---|---|---|---|---|---|---|---|---|
| Tree Nuts Group | CHO Group | Treatment Effect | ||||||
| Baseline | Change | p-Value | Baseline | Change | p-Value | Mean Difference | p-Value | |
| Sedentary time (min) | 793.79 ± 124.05 | 17.44 ± 54.17 | 0.71 | 748.86 ± 134.89 | 3.92 ± 13.83 | 0.91 | 14.44 ± 18.64 | 0.68 |
| Light activity time (min) | 320.26 ± 83.16 | −41.75 ± 81.68 | 0.14 | 304.65 ± 71.62 | −20.82 ± 77.23 | 0.31 | 20.94 ± 29.63 | 0.31 |
| Moderate activity time (min) | 163.36 ± 78.73 | 19.17 ± 25.21 | 0.04 | 152.20 ± 43.04 | 16.59 ± 32.16 | 0.37 | 2.58 ± 19.56 | 0.86 |
| Vigorous activity time (min) | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.99 | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.99 | 0.00 ± 0.00 | 0.99 |
| Total Active Time (min) | 483.62 ± 135.07 | −29.92 ± 41.79 | 0.11 | 455.95 ± 101.51 | −4.42 ± 11.65 | 0.46 | 24.49 ± 37.35 | 0.25 |
| Percent of Day Active (%) | 33.59 ± 9.38 | −0.07 ± 0.12 | 0.57 | 31.66 ± 7.05 | −0.02 ± 0.09 | 0.75 | 0.05 ± 0.04 | 0.09 |
| Steps per Day (count) | 10,827.61 ± 3391.96 | −1262.46 ± 1640.40 | 0.04 | 9643.29 ± 2543.50 | −729.61 ± 3371.44 | 0.42 | −532.85 ± 1013.34 | 0.60 |
| Physical Activity METs | 1.503 ± 0.253 | −0.06 ± 0.09 | 0.08 | 1.447 ± 0.128 | −0.03 ± 0.18 | 0.21 | 0.02 ± 0.06 | 0.72 |
| Physical Activity Energy Expenditure (kcal) | 1570.55 ± 918.31 | −100.50 ± 151.65 | 0.07 | 1273.14 ± 433.67 | −38.86 ± 49.74 | 0.77 | 61.63 ± 75.40 | 0.36 |
| Resting Energy Expenditure (kcal) | 1921.0 ± 272.02 | −0.13 ± 262.00 | 0.85 | 1899.79 ± 248.80 | 50.94 ± 196.14 | 0.27 | 64.01 ± 77.51 | 0.42 |
| Respiratory Quotient | 0.83 ± 0.06 | 0.01 ± 0.09 | 0.71 | 0.81 ± 0.04 | 0.02 ± 0.06 | 0.29 | 0.02 ± 0.03 | 0.35 |
| Carbohydrate Oxidation (% REE kcal) | 40.13 ± 17.30 | −6.19 ± 6.96 | <0.001 | 30.26 ± 14.13 | 4.77 ± 2.63 | <0.001 | 0.07 ± 4.72 | 0.98 |
| Fat Oxidation (% REE kcal) | 43.67 ± 17.09 | 4.35 ± 4.63 | <0.001 | 52.82 ± 14.68 | −8.48 ± 8.71 | <0.001 | 26.13 ± 15.70 | 0.34 |
| Protein Oxidation (% REE kcal) | 16.51 ± 7.46 | 2.30 ± 2.64 | <0.001 | 17.34 ± 7.91 | 4.11 ± 6.25 | <0.001 | 4.19 ± 2.70 | 0.13 |
| Visceral Adipose Tissue Area (cm) | 109.98 ± 65.63 | −4.12 ± 4.96 | 0.12 | 111.19 ± 60.65 | −2.58 ± 28.26 | 0.69 | 1.58 ± 10.04 | 0.67 |
| Subcutaneous Adipose Tissue Area (cm) | 242.51 ± 101.09 | −12.15 ± 14.98 | 0.29 | 274.40 ± 141.74 | −10.08 ± 82.66 | 0.59 | 2.23 ± 2.44 | 0.53 |
| VAT:SAT (ratio) | 0.45 ± 0.22 | −0.02 ± 0.11 | 0.43 | 0.46 ± 0.22 | 0.01 ± 0.12 | 0.51 | 0.03 ± 0.09 | 0.43 |
| b. Females | ||||||||
| Tree Nuts Group | CHO Group | Treatment Effect | ||||||
| Baseline | Change | p-value | Baseline | Change | p-value | Mean Difference | p-value | |
| Sedentary time (min) | 703.36 ± 113.03 | 53.13 ± 54.77 | 0.002 | 802.22 ± 163.23 | −10.14 ± 99.66 | 0.69 | 49.29 ± 36.74 | 0.19 |
| Light activity time (min) | 367.76 ± 112.46 | −83.74 ± 110.20 | 0.01 | 336.20 ± 97.40 | −35.96 ± 103.85 | 0.19 | 47.78 ± 38.44 | 0.23 |
| Moderate activity time (min) | 169.99 ± 61.44 | 31.95 ± 43.85 | 0.04 | 152.53 ± 59.55 | −12.19 ± 41.41 | 0.26 | 43.24 ± 85.47 | 0.42 |
| Vigorous activity time (min) | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.99 | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.99 | 0.00 ± 0.00 | 0.99 |
| Total Active Time (min) | 538.44 ± 113.71 | −56.68 ± 77.69 | 0.04 | 488.74 ± 138.19 | −46.55 ± 117.32 | 0.13 | 10.13 ± 19.42 | 0.75 |
| Percent of Day Active (%) | 37.39 ± 7.90 | −0.06 ± 0.08 | 0.62 | 33.94 ± 9.60 | -0.04 ± 0.09 | 0.44 | 0.02 ± 0.02 | 0.35 |
| Steps per Day (count) | 10,468.64 ± 2599.30 | −825.21 ± 2107.47 | 0.15 | 10,126.04 ± 2727.41 | −780.32 ± 2222.45 | 0.18 | 44.88 ± 779.07 | 0.95 |
| Physical Activity METs | 1.468 ± 0.151 | −0.06 ± 0.08 | 0.03 | 1.396 ± 0.145 | −0.01 ± 0.09 | 0.90 | 0.05 ± 0.03 | 0.11 |
| Physical Activity Energy Expenditure (kcal) | 1236.56 ± 366.22 | −192.12 ± 248.54 | 0.11 | 1055.16 ± 342.82 | −8.92 ± 284.69 | 0.92 | 181.85 ± 96.26 | 0.05 |
| Resting Energy Expenditure (kcal) | 1508.92 ± 175.88 | −28.63 ± 228.18 | 0.55 | 1497.58 ± 191.29 | −3.83 ± 189.57 | 0.82 | 24.79 ± 61.33 | 0.69 |
| Respiratory Quotient | 0.82 ± 0.06 | 0.00 ± 0.07 | 0.76 | 0.82 ± 0.06 | −0.01 ± 0.07 | 0.58 | 0.01 ± 0.02 | 0.54 |
| Carbohydrate Oxidation (% REE kcal) | 29.21 ± 10.37 | −6.46 ± 6.67 | <0.001 | 33.31 ± 14.86 | 3.83 ± 3.39 | <0.001 | 6.63 ± 5.92 | 0.22 |
| Fat Oxidation (% REE kcal) | 56.68 ± 12.04 | 2.85 ± 3.66 | <0.001 | 49.34 ± 16.03 | −3.63 ± 3.57 | <0.001 | 34.13 ± 13.73 | 0.27 |
| Protein Oxidation (% REE kcal) | 14.37 ± 4.64 | 5.97 ± 5.69 | <0.001 | 17.81 ± 6.82 | −1.41 ± 1.50 | 0.05 | 0.55 ± 1.94 | 0.77 |
| Visceral Adipose Tissue Area (cm) | 67.23 ± 41.92 | −5.27 ± 13.05 | 0.06 | 57.56 ± 48.18 | 4.49 ± 13.08 | 0.10 | 7.78 ± 10.77 | 0.44 |
| Subcutaneous Adipose Tissue Area (cm) | 287.65 ± 110.56 | −2.14 ± 42.11 | 0.81 | 244.27 ± 71.78 | 5.00 ± 30.89 | 0.44 | 7.14 ± 10.66 | 0.51 |
| VAT:SAT (ratio) | 0.23 ± 0.13 | −0.02 ± 0.05 | 0.16 | 0.22 ± 0.16 | −0.01 ± 0.08 | 0.30 | 0.02 ± 0.05 | 0.64 |
| Dependent Variable = Metabolic Syndrome Score | Dependent Variable = Triglycerides | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Source | Type III Sum of Squares | df | Mean Square | F | p-Value | Source | Type III Sum of Squares | df | Mean Square | F | p-Value |
| Corrected Model | 67.139 | 4 | 16.785 | 60.955 | <0.001 | Corrected Model | 210,000.721 | 4 | 52,500.180 | 21.072 | <0.001 |
| Intercept | 0.017 | 1 | 0.017 | 0.063 | 0.80 | Intercept | 643.928 | 1 | 643.928 | 0.258 | 0.61 |
| Met Sx (baseline) | 52.613 | 1 | 52.613 | 191.066 | <0.001 | Triglycerides (baseline) | 180,492.047 | 1 | 180,492.047 | 72.443 | <0.001 |
| Sex | 2.345 | 1 | 2.345 | 8.517 | 0.005 | Sex | 8609.145 | 1 | 8609.145 | 3.455 | 0.07 |
| Treatment = Tree Nuts | 1.127 | 1 | 1.127 | 4.091 | 0.04 | Treatment = Tree Nuts | 9924.296 | 1 | 9924.296 | 3.983 | 0.04 |
| Treatment * Sex | 3.252 | 1 | 3.252 | 11.810 | <0.001 | Treatment * Sex | 1978.462 | 1 | 1978.462 | 0.794 | 0.37 |
| Error | 21.754 | 79 | 0.275 | Error | 194,338.339 | 79 | 2491.517 | ||||
| Total | 167.000 | 84 | Total | 1,142,246.000 | 84 | ||||||
| Corrected Total | 88.893 | 83 | Corrected Total | 404,339.06 | 83 | ||||||
| Dependent Variable = Fasting Insulin Level | Dependent Variable = TG/HDL Ratio | ||||||||||
| Source | Type III Sum of Squares | df | Mean Square | F | p-value | Source | Type III Sum of Squares | df | Mean Square | F | p-value |
| Corrected Model | 209.299 | 4 | 52.325 | 12.001 | <0.001 | Corrected Model | 177.386 | 4 | 44.347 | 20.691 | <0.001 |
| Intercept | 67.554 | 1 | 67.554 | 15.494 | <0.001 | Intercept | 1.470 | 1 | 1.470 | 0.686 | 0.41 |
| Insulin (baseline) | 181.423 | 1 | 181.423 | 41.610 | <0.001 | TG/HDL ratio (baseline) | 142.676 | 1 | 142.676 | 66.568 | <0.001 |
| Sex | 0.006 | 1 | 0.006 | 0.001 | 0.97 | Sex | 5.193 | 1 | 5.193 | 2.423 | 0.12 |
| Treatment = Tree Nuts | 12.256 | 1 | 12.256 | 3.811 | 0.05 | Treatment = Tree Nuts | 9.138 | 1 | 9.138 | 4.264 | 0.04 |
| Treatment * Sex | 7.017 | 1 | 7.017 | 1.609 | 0.21 | Treatment * Sex | 2.989 | 1 | 2.989 | 1.395 | 0.24 |
| Error | 344.451 | 79 | 4.36 | Error | 167.178 | 79 | 2.143 | ||||
| Total | 1016.700 | 84 | Total | 714.978 | 84 | ||||||
| Corrected Total | 553.750 | 83 | Corrected Total | 344.564 | 83 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sumislawski, K.; Widmer, A.; Suro, R.R.; Robles, M.E.; Lillegard, K.; Olson, D.; Koethe, J.R.; Silver, H.J. Consumption of Tree Nuts as Snacks Reduces Metabolic Syndrome Risk in Young Adults: A Randomized Trial. Nutrients 2023, 15, 5051. https://doi.org/10.3390/nu15245051
Sumislawski K, Widmer A, Suro RR, Robles ME, Lillegard K, Olson D, Koethe JR, Silver HJ. Consumption of Tree Nuts as Snacks Reduces Metabolic Syndrome Risk in Young Adults: A Randomized Trial. Nutrients. 2023; 15(24):5051. https://doi.org/10.3390/nu15245051
Chicago/Turabian StyleSumislawski, Kate, Annaliese Widmer, Robert R. Suro, Michelle E. Robles, Kate Lillegard, Dianna Olson, John R. Koethe, and Heidi J. Silver. 2023. "Consumption of Tree Nuts as Snacks Reduces Metabolic Syndrome Risk in Young Adults: A Randomized Trial" Nutrients 15, no. 24: 5051. https://doi.org/10.3390/nu15245051
APA StyleSumislawski, K., Widmer, A., Suro, R. R., Robles, M. E., Lillegard, K., Olson, D., Koethe, J. R., & Silver, H. J. (2023). Consumption of Tree Nuts as Snacks Reduces Metabolic Syndrome Risk in Young Adults: A Randomized Trial. Nutrients, 15(24), 5051. https://doi.org/10.3390/nu15245051