
Perimenstrual Asthma in Adolescents: A Shared Condition in Pediatric and Gynecological Endocrinology

 ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
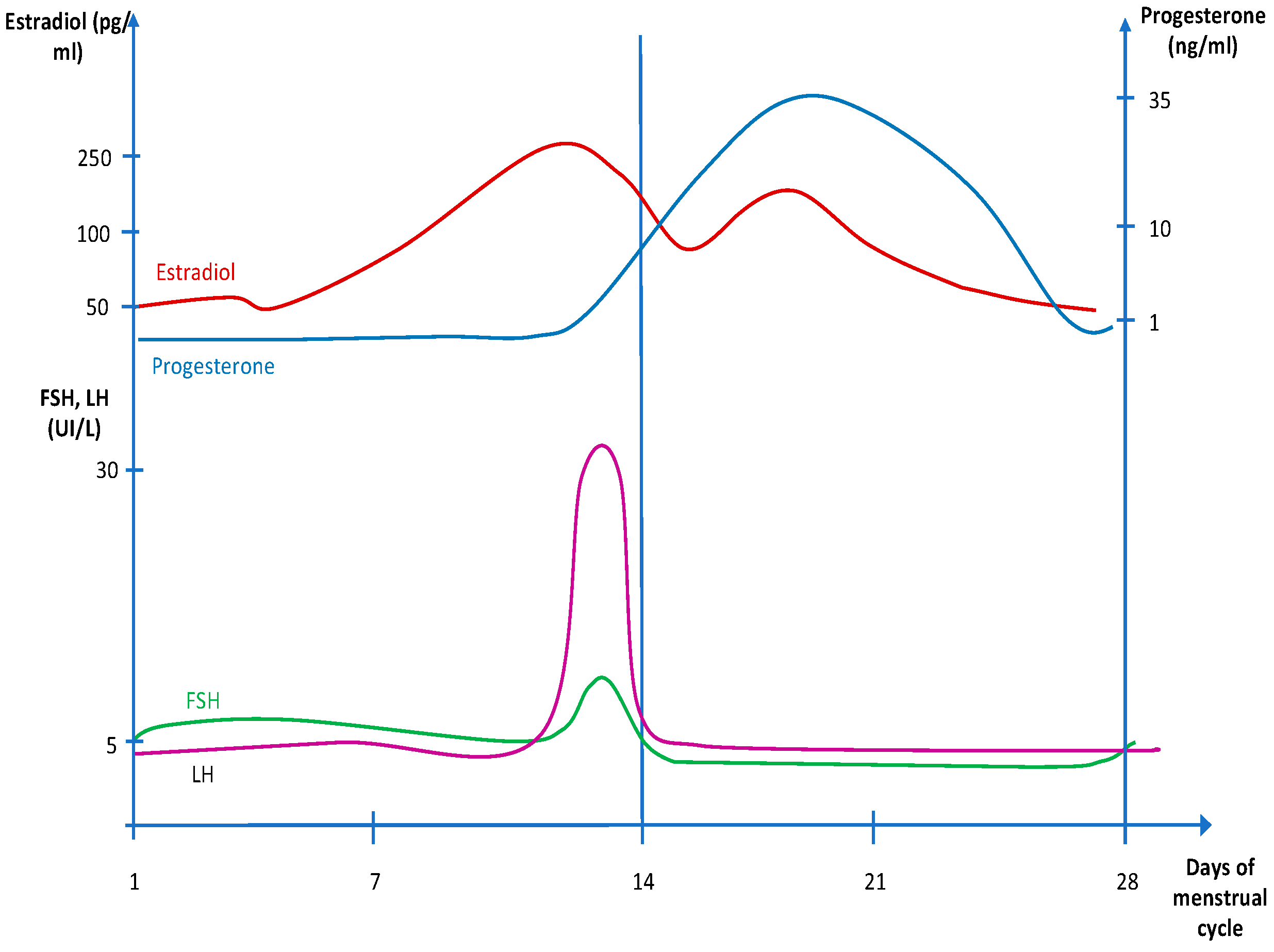
3. Hormonal Pattern of Menstrual Cycles
4. Asthma in Young Female Adolescents
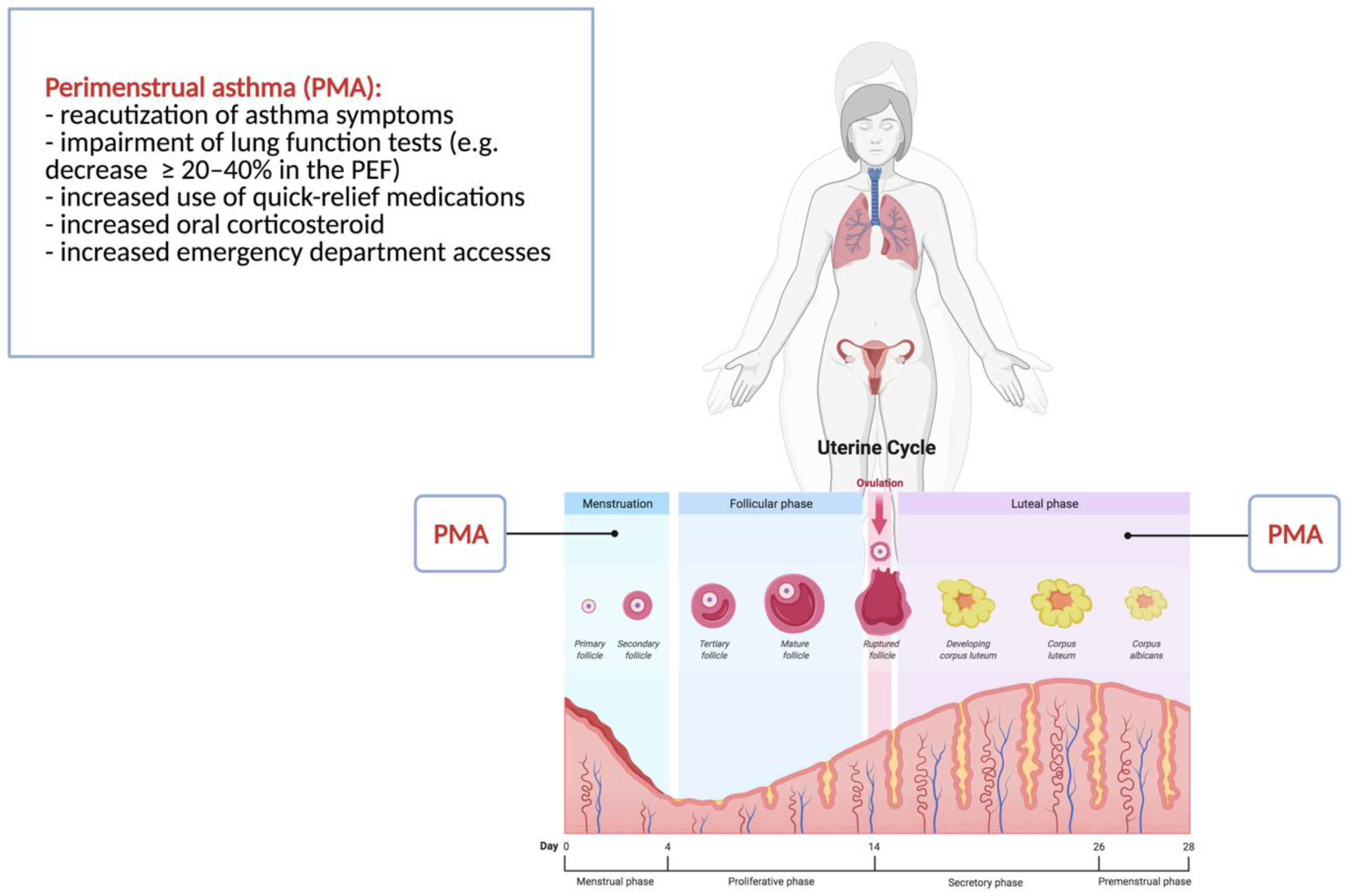
5. Perimenstrual Asthma
6. Perimenstrual Asthma and Sex Hormones
7. Perspective Strategies in Perimenstrual Asthma Treatment
7.1. Conventional Asthma Therapy
7.2. Hormonal Contraception
7.3. Estrogens, Progestogens, and Androgens
7.4. Leukotriene Receptor Antagonists
7.5. Microbiota
7.6. Vitamin D
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chipps, B.E.; Bacharier, L.B.; Farrar, J.R.; Jackson, D.J.; Murphy, K.R.; Phipatanakul, W.; Szefler, S.J.; Teague, W.G.; Zeiger, R.S. The Pediatric Asthma Yardstick: Practical Recommendations for a Sustained Step-up in Asthma Therapy for Children with Inadequately Controlled Asthma. Ann. Allergy Asthma Immunol. 2018, 120, 559–579.e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention; GINA: London, UK, 2021. [Google Scholar]
- Papi, A.; Brightling, C.; Pedersen, S.E.; Reddel, H.K. Asthma. Lancet 2018, 391, 783–800. [Google Scholar] [CrossRef]
- To, T.; Stanojevic, S.; Moores, G.; Gershon, A.S.; Bateman, E.D.; Cruz, A.A.; Boulet, L.-P. Global Asthma Prevalence in Adults: Findings from the Cross-Sectional World Health Survey. BMC Public Health 2012, 12, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Strategy for Asthma Management and Prevention (2016 Update); GINA: London, UK, 2016; Available online: https://ginasthma.org/ (accessed on 20 December 2021).
- CDC Vital Signs: Asthma Prevalence, Disease Characteristics, and Self-Management Education United States, 2001–2009; CDC: Atlanta, GA, USA, 2021.
- Frank, R.T. The Hormonal Causes of Premenstrual Tension. Arch. Neurol. Psychiatry 1931, 26, 1053–1057. [Google Scholar] [CrossRef]
- Chandler, M.H.; Schuldheisz, S.; Phillips, B.A.; Muse, K.N. Premenstrual Asthma: The Effect of Estrogen on Symptoms, Pulmonary Function, and Beta 2-Receptors. Pharmacotherapy 1997, 17, 224–234. [Google Scholar]
- Pereira-Vega, A.; Sánchez-Ramos, J.L. Questions Relating to Premenstrual Asthma. World J. Respirol. 2014, 5, 180. [Google Scholar] [CrossRef]
- Rubio Ravelo, L.; Gago Rodríguez, B.; Almirall Collazo, J.J.; Bell Heredia, L.; Fernández Fernández, L. Comparative Study of Progesterone, Estradiol and Cortisol Concentrations in Asthmatic and Non-Asthmatic Women. Allergol. Immunopathol. 1988, 16, 263–266. [Google Scholar]
- Piccinni, M.-P.; Lombardelli, L.; Logiodice, F.; Kullolli, O.; Maggi, E.; Barkley, M.S. Medroxyprogesterone Acetate Decreases Th1, Th17, and Increases Th22 Responses via AHR Signaling Which Could Affect Susceptibility to Infections and Inflammatory Disease. Front. Immunol. 2019, 10, 642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, I.S. Gender-Specific Asthma Treatment. Allergy Asthma Immunol. Res. 2011, 3, 74–80. [Google Scholar] [CrossRef] [Green Version]
- DeBoer, M.D.; Phillips, B.R.; Mauger, D.T.; Zein, J.; Erzurum, S.C.; Fitzpatrick, A.M.; Gaston, B.M.; Myers, R.; Ross, K.R.; Chmiel, J.; et al. Effects of Endogenous Sex Hormones on Lung Function and Symptom Control in Adolescents with Asthma. BMC Pulm. Med. 2018, 18, 58. [Google Scholar] [CrossRef]
- Pereira-Vega, A.; Sánchez Ramos, J.L.; Maldonado Pérez, J.A.; Vázquez Oliva, R.; Bravo Nieto, J.M.; Vázquez Rico, I.; Ignacio García, J.M.; Romero Palacios, P.; Alwakil Olbah, M.; Medina Gallardo, J.F. Premenstrual Asthma and Leukotriene Variations in the Menstrual Cycle. Allergol. Immunopathol. 2012, 40, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Nakasato, H.; Ohrui, T.; Sekizawa, K.; Matsui, T.; Yamaya, M.; Tamura, G.; Sasaki, H. Prevention of Severe Premenstrual Asthma Attacks by Leukotriene Receptor Antagonist. J. Allergy Clin. Immunol. 1999, 104, 585–588. [Google Scholar] [CrossRef]
- Alsharairi, N.A. The Role of Short-Chain Fatty Acids in the Interplay between a Very Low-Calorie Ketogenic Diet and the Infant Gut Microbiota and Its Therapeutic Implications for Reducing Asthma. Int. J. Mol. Sci. 2020, 21, 9580. [Google Scholar] [CrossRef] [PubMed]
- Ver Heul, A.; Planer, J.; Kau, A.L. The Human Microbiota and Asthma. Clin. Rev. Allergy Immunol. 2019, 57, 350–363. [Google Scholar] [CrossRef]
- Gregory, A.T.; Denniss, A.R. An Introduction to Writing Narrative and Systematic Reviews—Tasks, Tips and Traps for Aspiring Authors. Heart Lung Circ. 2018, 27, 893–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alotaibi, M.F. Physiology of Puberty in Boys and Girls and Pathological Disorders Affecting Its Onset. J. Adolesc. 2019, 71, 63–71. [Google Scholar] [CrossRef]
- Naftolin, F.; Khafaga, A.; Nachtigall, M. The Hypothalamic-Pituitary-Ovarian Axis and Regulation of the Menstrual Cycle. In Clinical Reproductive Medicine and Surgery; Springer: New York, NY, USA, 2019; pp. 1–13. [Google Scholar]
- Hall, J. Neuroendocrine Control of the Menstrual Cycle. In Yen and Jaffe’s Reproductive Endocrinology, 8th ed.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 149–166. [Google Scholar] [CrossRef]
- Skiba, M.A.; Bell, R.J.; Islam, R.M.; Handelsman, D.J.; Desai, R.; Davis, S.R. Androgens During the Reproductive Years: What Is Normal for Women? J. Clin. Endocrinol. Metab. 2019, 104, 5382–5392. [Google Scholar] [CrossRef] [PubMed]
- Walters, K.A. Role of Androgens in Normal and Pathological Ovarian Function. Reprod. Camb. Engl. 2015, 149, R193–R218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlson, L.J.; Shaw, N.D. Development of Ovulatory Menstrual Cycles in Adolescent Girls. J. Pediatr. Adolesc. Gynecol. 2019, 32, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.Z.; Kangarloo, T.; Adams, J.M.; Sluss, P.M.; Welt, C.K.; Chandler, D.W.; Zava, D.T.; McGrath, J.A.; Umbach, D.M.; Hall, J.E.; et al. Healthy Post-Menarchal Adolescent Girls Demonstrate Multi-Level Reproductive Axis Immaturity. J. Clin. Endocrinol. Metab. 2019, 104, 613–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunn, H.M.; Tsai, M.-C.; McRae, A.; Steinbeck, K.S. Menstrual Patterns in the First Gynecological Year: A Systematic Review. J. Pediatr. Adolesc. Gynecol. 2018, 31, 557–565.e6. [Google Scholar] [CrossRef] [PubMed]
- Svanes, C.; Real, F.G.; Gislason, T.; Jansson, C.; Jögi, R.; Norrman, E.; Nyström, L.; Torén, K.; Omenaas, E. Association of Asthma and Hay Fever with Irregular Menstruation. Thorax 2005, 60, 445–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Real, F.G.; Svanes, C.; Omenaas, E.R.; Antò, J.M.; Plana, E.; Janson, C.; Jarvis, D.; Zemp, E.; Wjst, M.; Leynaert, B.; et al. Menstrual Irregularity and Asthma and Lung Function. J. Allergy Clin. Immunol. 2007, 120, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Kisiel, M.A.; Berglund, C.; Janson, C.; Hasselgren, M.; Montgomery, S.; Nager, A.; Sandelowsky, H.; Ställberg, B.; Sundh, J.; Lisspers, K. Quality of Life and Asthma Control Related to Hormonal Transitions in Women’s Lives. J. Asthma 2021, 1–9, ahead of print. [Google Scholar] [CrossRef] [PubMed]
- McCleary, N.; Nwaru, B.I.; Nurmatov, U.B.; Critchley, H.; Sheikh, A. Endogenous and Exogenous Sex Steroid Hormones in Asthma and Allergy in Females: A Systematic Review and Meta-Analysis. J. Allergy Clin. Immunol. 2018, 141, 1510–1513.e8. [Google Scholar] [CrossRef] [Green Version]
- Reed, B.G.; Carr, B.R. The Normal Menstrual Cycle and the Control of Ovulation. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- de Benedictis, D.; Bush, A. Asthma in Adolescence: Is There Any News?: Asthma in Adolescence. Pediatr. Pulmonol. 2017, 52, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Gore, F.M.; Bloem, P.J.N.; Patton, G.C.; Ferguson, J.; Joseph, V.; Coffey, C.; Sawyer, S.M.; Mathers, C.D. Global Burden of Disease in Young People Aged 10–24 Years: A Systematic Analysis. Lancet 2011, 377, 2093–2102. [Google Scholar] [CrossRef]
- Leynaert, B.; Sunyer, J.; Garcia-Esteban, R.; Svanes, C.; Jarvis, D.; Cerveri, I.; Dratva, J.; Gislason, T.; Heinrich, J.; Janson, C.; et al. Gender Differences in Prevalence, Diagnosis and Incidence of Allergic and Non-Allergic Asthma: A Population-Based Cohort. Thorax 2012, 67, 625–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akar-Ghibril, N.; Casale, T.; Custovic, A.; Phipatanakul, W. Allergic Endotypes and Phenotypes of Asthma. J. Allergy Clin. Immunol. Pract. 2020, 8, 429–440. [Google Scholar] [CrossRef]
- Licari, A.; Castagnoli, R.; Brambilla, I.; Marseglia, A.; Tosca, M.A.; Marseglia, G.L.; Ciprandi, G. Asthma Endotyping and Biomarkers in Childhood Asthma. Pediatr. Allergy Immunol. Pulmonol. 2018, 31, 44–55. [Google Scholar] [CrossRef] [Green Version]
- Di Cicco, M.; D’Elios, S.; Peroni, D.G.; Comberiati, P. The Role of Atopy in Asthma Development and Persistence. Curr. Opin. Allergy Clin. Immunol. 2020, 20, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, V.; Verduci, E.; Ghezzi, M.; Cena, H.; Pascuzzi, M.C.; Regalbuto, C.; Lamberti, R.; Rossi, V.; Manuelli, M.; Bosetti, A.; et al. Pediatric Obesity-Related Asthma: The Role of Nutrition and Nutrients in Prevention and Treatment. Nutrients 2021, 13, 3708. [Google Scholar] [CrossRef] [PubMed]
- Beuther, D.A.; Sutherland, E.R. Overweight, Obesity, and Incident Asthma: A Meta-Analysis of Prospective Epidemiologic Studies. Am. J. Respir. Crit. Care Med. 2007, 175, 661–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomsen, S.F.; Ulrik, C.S.; Kyvik, K.O.; Sørensen, T.I.A.; Posthuma, D.; Skadhauge, L.R.; Steffensen, I.; Backer, V. Association between Obesity and Asthma in a Twin Cohort. Allergy 2007, 62, 1199–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cibella, F.; Cuttitta, G.; La Grutta, S.; Melis, M.R.; Bucchieri, S.; Viegi, G. A Cross-Sectional Study Assessing the Relationship between BMI, Asthma, Atopy, and ENO among Schoolchildren. Ann. Allergy Asthma Immunol. 2011, 107, 330–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinto, K.B.; Zuraw, B.L.; Poon, K.-Y.T.; Chen, W.; Schatz, M.; Christiansen, S.C. The Association of Obesity and Asthma Severity and Control in Children. J. Allergy Clin. Immunol. 2011, 128, 964–969. [Google Scholar] [CrossRef] [PubMed]
- Vijayakanthi, N.; Greally, J.M.; Rastogi, D. Pediatric Obesity-Related Asthma: The Role of Metabolic Dysregulation. Pediatrics 2016, 137, e20150812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.C.; Dong, G.H.; Lin, K.C.; Lee, Y.L. Gender Difference of Childhood Overweight and Obesity in Predicting the Risk of Incident Asthma: A Systematic Review and Meta-Analysis. Obes. Rev. 2013, 14, 222–231. [Google Scholar] [CrossRef]
- Forno, E.; Lescher, R.; Strunk, R.; Weiss, S.; Fuhlbrigge, A.; Celedón, J.C. Childhood Asthma Management Program Research Group Decreased Response to Inhaled Steroids in Overweight and Obese Asthmatic Children. J. Allergy Clin. Immunol. 2011, 127, 741–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belamarich, P.F.; Luder, E.; Kattan, M.; Mitchell, H.; Islam, S.; Lynn, H.; Crain, E.F. Do Obese Inner-City Children with Asthma Have More Symptoms than Nonobese Children with Asthma? Pediatrics 2000, 106, 1436–1441. [Google Scholar] [CrossRef] [PubMed]
- Kattan, M.; Kumar, R.; Bloomberg, G.R.; Mitchell, H.E.; Calatroni, A.; Gergen, P.J.; Kercsmar, C.M.; Visness, C.M.; Matsui, E.C.; Steinbach, S.F.; et al. Asthma Control, Adiposity, and Adipokines among Inner-City Adolescents. J. Allergy Clin. Immunol. 2010, 125, 584–592. [Google Scholar] [CrossRef] [Green Version]
- Messiah, S.E.; Arheart, K.L.; Lipshultz, S.E.; Miller, T.L. Ethnic Group Differences in Waist Circumference Percentiles among U.S. Children and Adolescents: Estimates from the 1999–2008 National Health and Nutrition Examination Surveys. Metab. Syndr. Relat. Disord. 2011, 9, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.L.; Shiao, G.; Chou, P. Association between Body Mass Index and Allergy in Teenage Girls in Taiwan. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 1999, 29, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Schachter, L.M.; Peat, J.K.; Salome, C.M. Asthma and Atopy in Overweight Children. Thorax 2003, 58, 1031–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.E.; Gibson, P.G.; Collins, C.E.; Wood, L.G. Airway and Systemic Inflammation in Obese Children with Asthma. Eur. Respir. J. 2013, 42, 1012–1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, Z.; Ulrik, C.S. Obesity and Asthma: A Coincidence or a Causal Relationship? A Systematic Review. Respir. Med. 2013, 107, 1287–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holguin, F.; Bleecker, E.R.; Busse, W.W.; Calhoun, W.J.; Castro, M.; Erzurum, S.C.; Fitzpatrick, A.M.; Gaston, B.; Israel, E.; Jarjour, N.N.; et al. Obesity and Asthma: An Association Modified by Age of Asthma Onset. J. Allergy Clin. Immunol. 2011, 127, 1486–1493.e2. [Google Scholar] [CrossRef]
- Couriel, J. Asthma in Adolescence. Paediatr. Respir. Rev. 2003, 4, 47–54. [Google Scholar] [CrossRef]
- Kaur, B.; Anderson, H.R.; Austin, J.; Burr, M.; Harkins, L.S.; Strachan, D.P.; Warner, J.O. Prevalence of Asthma Symptoms, Diagnosis, and Treatment in 12–14 Year Old Children across Great Britain (International Study of Asthma and Allergies in Childhood, ISAAC UK). BMJ 1998, 316, 118–124. [Google Scholar] [CrossRef] [Green Version]
- Siersted, H.C.; Boldsen, J.; Hansen, H.S.; Mostgaard, G.; Hyldebrandt, N. Population Based Study of Risk Factors for Underdiagnosis of Asthma in Adolescence: Odense Schoolchild Study. BMJ 1998, 316, 651–655; discussion 655–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, J.A.; Matheson, M.C.; Gurrin, L.C.; Byrnes, G.B.; Adams, K.S.; Wharton, C.L.; Giles, G.G.; Jenkins, M.A.; Hopper, J.L.; Abramson, M.J.; et al. Factors Influencing Asthma Remission: A Longitudinal Study from Childhood to Middle Age. Thorax 2011, 66, 508–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, M.; Hedman, L.; Bjerg, A.; Forsberg, B.; Lundbäck, B.; Rönmark, E. Remission and Persistence of Asthma Followed from 7 to 19 Years of Age. Pediatrics 2013, 132, e435–e442. [Google Scholar] [CrossRef]
- Roorda, R.J.; Gerritsen, J.; van Aalderen, W.M.; Schouten, J.P.; Veltman, J.C.; Weiss, S.T.; Knol, K. Follow-up of Asthma from Childhood to Adulthood: Influence of Potential Childhood Risk Factors on the Outcome of Pulmonary Function and Bronchial Responsiveness in Adulthood. J. Allergy Clin. Immunol. 1994, 93, 575–584. [Google Scholar] [CrossRef]
- Sears, M.R.; Greene, J.M.; Willan, A.R.; Wiecek, E.M.; Taylor, D.R.; Flannery, E.M.; Cowan, J.O.; Herbison, G.P.; Silva, P.A.; Poulton, R. A Longitudinal, Population-Based, Cohort Study of Childhood Asthma Followed to Adulthood. N. Engl. J. Med. 2003, 349, 1414–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phelan, P.D.; Robertson, C.F.; Olinsky, A. The Melbourne Asthma Study: 1964–1999. J. Allergy Clin. Immunol. 2002, 109, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Sekerel, B.E.; Civelek, E.; Karabulut, E.; Yildirim, S.; Tuncer, A.; Adalioglu, G. Are Risk Factors of Childhood Asthma Predicting Disease Persistence in Early Adulthood Different in the Developing World? Allergy 2006, 61, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Vink, N.M.; Postma, D.S.; Schouten, J.P.; Rosmalen, J.G.M.; Boezen, H.M. Gender Differences in Asthma Development and Remission during Transition through Puberty: The TRacking Adolescents’ Individual Lives Survey (TRAILS) Study. J. Allergy Clin. Immunol. 2010, 126, 498–504.e1–6. [Google Scholar] [CrossRef] [PubMed]
- Anderson, H.R.; Pottier, A.C.; Strachan, D.P. Asthma from Birth to Age 23: Incidence and Relation to Prior and Concurrent Atopic Disease. Thorax 1992, 47, 537–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hovland, V.; Riiser, A.; Mowinckel, P.; Carlsen, K.-H.; Lødrup Carlsen, K.C. Early Risk Factors for Pubertal Asthma. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2015, 45, 164–176. [Google Scholar] [CrossRef]
- Andersson, M.; Bjerg, A.; Forsberg, B.; Lundbäck, B.; Rönmark, E. The Clinical Expression of Asthma in Schoolchildren Has Changed between 1996 and 2006. Pediatr. Allergy Immunol. 2010, 21, 859–866. [Google Scholar] [CrossRef]
- Crump, C.; Winkleby, M.A.; Sundquist, J.; Sundquist, K. Risk of Asthma in Young Adults Who Were Born Preterm: A Swedish National Cohort Study. Pediatrics 2011, 127, e913–e920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, C.C.; Peterson, E.L.; Joseph, C.L.M.; Ownby, D.R.; Breslau, N. Birth Weight and Asthma Incidence by Asthma Phenotype Pattern in a Racially Diverse Cohort Followed through Adolescence. J. Asthma 2015, 52, 1006–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salam, M.T.; Wenten, M.; Gilliland, F.D. Endogenous and Exogenous Sex Steroid Hormones and Asthma and Wheeze in Young Women. J. Allergy Clin. Immunol. 2006, 117, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Bjerg-Bäcklund, A.; Bäcklund, A.B.; Perzanowski, M.S.; Platts-Mills, T.; Sandström, T.; Lundbäck, B.; Rönmark, E. Asthma during the Primary School Ages--Prevalence, Remission and the Impact of Allergic Sensitization. Allergy 2006, 61, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Vonk, J.M.; Boezen, H.M. Predicting Adult Asthma in Childhood. Curr. Opin. Pulm. Med. 2006, 12, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Rönmark, E.; Lindberg, A.; Watson, L.; Lundbäck, B. Outcome and Severity of Adult Onset Asthma--Report from the Obstructive Lung Disease in Northern Sweden Studies (OLIN). Respir. Med. 2007, 101, 2370–2377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arshad, S.H.; Raza, A.; Lau, L.; Bawakid, K.; Karmaus, W.; Zhang, H.; Ewart, S.; Patil, V.; Roberts, G.; Kurukulaaratchy, R. Pathophysiological Characterization of Asthma Transitions across Adolescence. Respir. Res. 2014, 15, 153. [Google Scholar] [CrossRef] [Green Version]
- Goksör, E.; Åmark, M.; Alm, B.; Ekerljung, L.; Lundbäck, B.; Wennergren, G. High Risk of Adult Asthma Following Severe Wheezing in Early Life. Pediatr. Pulmonol. 2015, 50, 789–797. [Google Scholar] [CrossRef]
- Almqvist, C.; Worm, M.; Leynaert, B.; Working group of GA2LEN WP 2.5 Gender. Impact of Gender on Asthma in Childhood and Adolescence: A GA2LEN Review. Allergy 2008, 63, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Meyer, M.R.; Haas, E.; Barton, M. Gender Differences of Cardiovascular Disease: New Perspectives for Estrogen Receptor Signaling. Hypertens. Dallas Tex 2006, 47, 1019–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Most, W.; van der Wee-Pals, L.; Ederveen, A.; Papapoulos, S.; Löwik, C. Ovariectomy and Orchidectomy Induce a Transient Increase in the Osteoclastogenic Potential of Bone Marrow Cells in the Mouse. Bone 1997, 20, 27–30. [Google Scholar] [CrossRef]
- Gillies, G.E.; Murray, H.E.; Dexter, D.; McArthur, S. Sex Dimorphisms in the Neuroprotective Effects of Estrogen in an Animal Model of Parkinson’s Disease. Pharmacol. Biochem. Behav. 2004, 78, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, S.; Swasey, C.H.; Loader, J.E.; Dakhama, A.; Joetham, A.; Ohnishi, H.; Balhorn, A.; Miyahara, N.; Takeda, K.; Gelfand, E.W. Estrogen Determines Sex Differences in Airway Responsiveness after Allergen Exposure. Am. J. Respir. Cell Mol. Biol. 2008, 38, 501–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimitropoulou, C.; White, R.E.; Ownby, D.R.; Catravas, J.D. Estrogen Reduces Carbachol-Induced Constriction of Asthmatic Airways by Stimulating Large-Conductance Voltage and Calcium-Dependent Potassium Channels. Am. J. Respir. Cell Mol. Biol. 2005, 32, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Degano, B.; Prévost, M.C.; Berger, P.; Molimard, M.; Pontier, S.; Rami, J.; Escamilla, R. Estradiol Decreases the Acetylcholine-Elicited Airway Reactivity in Ovariectomized Rats through an Increase in Epithelial Acetylcholinesterase Activity. Am. J. Respir. Crit. Care Med. 2001, 164, 1849–1854. [Google Scholar] [CrossRef] [PubMed]
- Melgert, B.N.; Ray, A.; Hylkema, M.N.; Timens, W.; Postma, D.S. Are There Reasons Why Adult Asthma Is More Common in Females? Curr. Allergy Asthma Rep. 2007, 7, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Corteling, R.; Trifilieff, A. Gender Comparison in a Murine Model of Allergen-Driven Airway Inflammation and the Response to Budesonide Treatment. BMC Pharmacol. 2004, 4, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riffo-Vasquez, Y.; Ligeiro de Oliveira, A.P.; Page, C.P.; Spina, D.; Tavares-de-Lima, W. Role of Sex Hormones in Allergic Inflammation in Mice. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2007, 37, 459–470. [Google Scholar] [CrossRef] [PubMed]
- Carey, M.A.; Card, J.W.; Bradbury, J.A.; Moorman, M.P.; Haykal-Coates, N.; Gavett, S.H.; Graves, J.P.; Walker, V.R.; Flake, G.P.; Voltz, J.W.; et al. Spontaneous Airway Hyperresponsiveness in Estrogen Receptor-Alpha-Deficient Mice. Am. J. Respir. Crit. Care Med. 2007, 175, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Taube, C.; Wei, X.; Swasey, C.H.; Joetham, A.; Zarini, S.; Lively, T.; Takeda, K.; Loader, J.; Miyahara, N.; Kodama, T.; et al. Mast Cells, Fc Epsilon RI, and IL-13 Are Required for Development of Airway Hyperresponsiveness after Aerosolized Allergen Exposure in the Absence of Adjuvant. J. Immunol. Baltim. Md 2004, 172, 6398–6406. [Google Scholar] [CrossRef] [Green Version]
- Melgert, B.N.; Postma, D.S.; Kuipers, I.; Geerlings, M.; Luinge, M.A.; van der Strate, B.W.A.; Kerstjens, H.A.M.; Timens, W.; Hylkema, M.N. Female Mice Are More Susceptible to the Development of Allergic Airway Inflammation than Male Mice. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2005, 35, 1496–1503. [Google Scholar] [CrossRef] [PubMed]
- Almeida, M.; Han, L.; Martin-Millan, M.; Plotkin, L.I.; Stewart, S.A.; Roberson, P.K.; Kousteni, S.; O’Brien, C.A.; Bellido, T.; Parfitt, A.M.; et al. Skeletal Involution by Age-Associated Oxidative Stress and Its Acceleration by Loss of Sex Steroids. J. Biol. Chem. 2007, 282, 27285–27297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, M.; Han, L.; Ambrogini, E.; Bartell, S.M.; Manolagas, S.C. Oxidative Stress Stimulates Apoptosis and Activates NF-ΚB in Osteoblastic Cells via a PKCβ/P66shc Signaling Cascade: Counter Regulation by Estrogens or Androgens. Mol. Endocrinol. 2010, 24, 2030–2037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsen, N.J.; Kovacs, W.J. Gonadal Steroids and Immunity. Endocr. Rev. 1996, 17, 369–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talal, N. Sex Steroid Hormones and Systemic Lupus Erythematosus. Arthritis Rheum. 1981, 24, 1054–1056. [Google Scholar] [CrossRef]
- Bijlsma, J.W.J.; Van Den Brink, H.R. Estrogens and Rheumatoid Arthritis. Am. J. Reprod. Immunol. 1992, 28, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M.; Wilder, R.L. Different roles for androgens and estrogens in the susceptibility to autoimmune rheumatic diseases. Rheum. Dis. Clin. N. Am. 2000, 26, 825–839. [Google Scholar] [CrossRef]
- Lang, T.J. Estrogen as an Immunomodulator. Clin. Immunol. 2004, 113, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Carruba, G.; D’Agostino, P.; Miele, M.; Calabrò, M.; Barbera, C.; Bella, G.D.; Milano, S.; Ferlazzo, V.; Caruso, R.; Rosa, M.L.; et al. Estrogen Regulates Cytokine Production and Apoptosis in PMA-Differentiated, Macrophage-like U937 Cells: Estrogen Regulates Cytokine Production in U937 Cells. J. Cell. Biochem. 2003, 90, 187–196. [Google Scholar] [CrossRef]
- Mor, G.; Sapi, E.; Abrahams, V.M.; Rutherford, T.; Song, J.; Hao, X.-Y.; Muzaffar, S.; Kohen, F. Interaction of the Estrogen Receptors with the Fas Ligand Promoter in Human Monocytes. J. Immunol. 2003, 170, 114–122. [Google Scholar] [CrossRef]
- Skobeloff, E.M.; Spivey, W.H.; St Clair, S.S.; Schoffstall, J.M. The Influence of Age and Sex on Asthma Admissions. JAMA 1992, 268, 3437–3440. [Google Scholar] [CrossRef]
- Hyndman, S.J.; Williams, D.R.; Merrill, S.L.; Lipscombe, J.M.; Palmer, C.R. Rates of Admission to Hospital for Asthma. BMJ 1994, 308, 1596–1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloomberg, G.R.; Trinkaus, K.M.; Fisher, E.B.; Musick, J.R.; Strunk, R.C. Hospital Readmissions for Childhood Asthma: A 10-Year Metropolitan Study. Am. J. Respir. Crit. Care Med. 2003, 167, 1068–1076. [Google Scholar] [CrossRef]
- Postma, D.S. Gender Differences in Asthma Development and Progression. Gend. Med. 2007, 4 (Suppl. B), S133–S146. [Google Scholar] [CrossRef]
- Dratva, J.; Schindler, C.; Curjuric, I.; Stolz, D.; Macsali, F.; Gomez, F.R.; Zemp, E. SAPALDIA Team Perimenstrual Increase in Bronchial Hyperreactivity in Premenopausal Women: Results from the Population-Based SAPALDIA 2 Cohort. J. Allergy Clin. Immunol. 2010, 125, 823–829. [Google Scholar] [CrossRef]
- Liptzin, D.R.; Landau, L.I.; Taussig, L.M. Sex and the Lung: Observations, Hypotheses, and Future Directions. Pediatr. Pulmonol. 2015, 50, 1159–1169. [Google Scholar] [CrossRef]
- Townsend, E.A.; Miller, V.M.; Prakash, Y.S. Sex Differences and Sex Steroids in Lung Health and Disease. Endocr. Rev. 2012, 33, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, C.J.; Coutts, I.I.; Lock, R.; Finnegan, O.C.; White, R.J. Premenstrual Exacerbation of Asthma. Thorax 1984, 39, 833–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauli, B.D.; Reid, R.L.; Munt, P.W.; Wigle, R.D.; Forkert, L. Influence of the Menstrual Cycle on Airway Function in Asthmatic and Normal Subjects. Am. Rev. Respir. Dis. 1989, 140, 358–362. [Google Scholar] [CrossRef]
- Ensom, M.H.H.; Chong, G.; Beaudin, B.; Bai, T.R. Estradiol in Severe Asthma with Premenstrual Worsening. Ann. Pharmacother. 2003, 37, 1610–1613. [Google Scholar] [CrossRef]
- Ensom, M.H.; Chong, E.; Carter, D. Premenstrual Symptoms in Women with Premenstrual Asthma. Pharmacotherapy 1999, 19, 374–382. [Google Scholar] [CrossRef]
- Oguzulgen, I.K.; Turktas, H.; Erbas, D. Airway Inflammation in Premenstrual Asthma. J. Asthma 2002, 39, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.J.; Lee, S.Y.; Choi, S.I.; Kim, B.-K.; Lee, E.J.; Choi, J. Population-Based Study of the Association between Asthma and Exogenous Female Sex Hormone Use. BMJ Open 2021, 11, e046400. [Google Scholar] [CrossRef]
- Bernstein, J.A. Progestogen Sensitization: A Unique Female Presentation of Anaphylaxis. Curr. Allergy Asthma Rep. 2020, 20, 4. [Google Scholar] [CrossRef]
- Pedersen, S.E.; Bateman, E.D.; Bousquet, J.; Busse, W.W.; Yoxall, S.; Clark, T.J. Gaining Optimal Asthma controL Steering Committee and Investigators Determinants of Response to Fluticasone Propionate and Salmeterol/Fluticasone Propionate Combination in the Gaining Optimal Asthma ControL Study. J. Allergy Clin. Immunol. 2007, 120, 1036–1042. [Google Scholar] [CrossRef]
- Tse, S.M.; Coull, B.A.; Sordillo, J.E.; Datta, S.; Gold, D.R. Gender- and Age-Specific Risk Factors for Wheeze from Birth through Adolescence. Pediatr. Pulmonol. 2015, 50, 955–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosewich, M.; Schulze, J.; Eickmeier, O.; Adler, S.; Rose, M.A.; Schubert, R.; Zielen, S. Early Impact of Smoking on Lung Function, Health, and Well-Being in Adolescents. Pediatr. Pulmonol. 2012, 47, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.; Kim, H.B.; Lee, S.Y.; Kim, B.S.; Kim, J.H.; Yu, J.; Kim, B.J.; Lee, D.H.; Seong, M.W.; Hong, S.J. Effect of Active Smoking on Asthma Symptoms, Pulmonary Function, and BHR in Adolescents. Pediatr. Pulmonol. 2009, 44, 954–961. [Google Scholar] [CrossRef]
- Silvestri, M.; Franchi, S.; Pistorio, A.; Petecchia, L.; Rusconi, F. Smoke Exposure, Wheezing, and Asthma Development: A Systematic Review and Meta-Analysis in Unselected Birth Cohorts. Pediatr. Pulmonol. 2015, 50, 353–362. [Google Scholar] [CrossRef]
- Hedman, L.; Bjerg, A.; Sundberg, S.; Forsberg, B.; Rönmark, E. Both Environmental Tobacco Smoke and Personal Smoking Is Related to Asthma and Wheeze in Teenagers. Thorax 2011, 66, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Thacher, J.D.; Gruzieva, O.; Pershagen, G.; Neuman, Å.; Wickman, M.; Kull, I.; Melén, E.; Bergström, A. Pre- and Postnatal Exposure to Parental Smoking and Allergic Disease through Adolescence. Pediatrics 2014, 134, 428–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, S.; Stern, D.A.; Zhou, M.; Sherrill, D.L.; Wright, A.L.; Morgan, W.J.; Martinez, F.D. Combined Effects of Parental and Active Smoking on Early Lung Function Deficits: A Prospective Study from Birth to Age 26 Years. Thorax 2013, 68, 1021–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalmers, G.W.; Macleod, K.J.; Little, S.A.; Thomson, L.J.; McSharry, C.P.; Thomson, N.C. Influence of Cigarette Smoking on Inhaled Corticosteroid Treatment in Mild Asthma. Thorax 2002, 57, 226–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooke, A.; Fergeson, J.; Bulkhi, A.; Casale, T.B. The Electronic Cigarette: The Good, the Bad, and the Ugly. J. Allergy Clin. Immunol. Pract. 2015, 3, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Polosa, R.; Morjaria, J.; Caponnetto, P.; Caruso, M.; Strano, S.; Battaglia, E.; Russo, C. Effect of Smoking Abstinence and Reduction in Asthmatic Smokers Switching to Electronic Cigarettes: Evidence for Harm Reversal. Int. J. Environ. Res. Public. Health 2014, 11, 4965–4977. [Google Scholar] [CrossRef]
- Giroud, C.; de Cesare, M.; Berthet, A.; Varlet, V.; Concha-Lozano, N.; Favrat, B. E-Cigarettes: A Review of New Trends in Cannabis Use. Int. J. Environ. Res. Public. Health 2015, 12, 9988–10008. [Google Scholar] [CrossRef] [PubMed]
- Randolph, C.C.; Fraser, B. Stressors and Concerns in Teen Asthma. Allergy Asthma Proc. 1998, 19, 193–203. [Google Scholar] [CrossRef]
- Bender, B.; Zhang, L. Negative Affect, Medication Adherence, and Asthma Control in Children. J. Allergy Clin. Immunol. 2008, 122, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Richardson, L.P.; Lozano, P.; Russo, J.; McCauley, E.; Bush, T.; Katon, W. Asthma Symptom Burden: Relationship to Asthma Severity and Anxiety and Depression Symptoms. Pediatrics 2006, 118, 1042–1051. [Google Scholar] [CrossRef] [PubMed]
- Vila, G.; Nollet-Clémençon, C.; de Blic, J.; Falissard, B.; Mouren-Simeoni, M.C.; Scheinmann, P. Assessment of Anxiety Disorders in Asthmatic Children. Psychosomatics 1999, 40, 404–413. [Google Scholar] [CrossRef]
- Burkhart, P.V.; Rayens, M.K. Self-Concept and Health Locus of Control: Factors Related to Children’s Adherence to Recommended Asthma Regimen. Pediatr. Nurs. 2005, 31, 404–409. [Google Scholar] [PubMed]
- Bruzzese, J.-M.; Fisher, P.H.; Lemp, N.; Warner, C.M. Asthma and Social Anxiety in Adolescents. J. Pediatr. 2009, 155, 398–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vila, G.; Nollet-Clemençon, C.; de Blic, J.; Mouren-Simeoni, M.C.; Scheinmann, P. Prevalence of DSM IV Anxiety and Affective Disorders in a Pediatric Population of Asthmatic Children and Adolescents. J. Affect. Disord. 2000, 58, 223–231. [Google Scholar] [CrossRef]
- Buhrmester, D.; Furman, W. The Development of Companionship and Intimacy. Child Dev. 1987, 58, 1101–1113. [Google Scholar] [CrossRef] [PubMed]
- Kyngäs, H. Support Network of Adolescents with Chronic Disease: Adolescents’ Perspective. Nurs. Health Sci. 2004, 6, 287–293. [Google Scholar] [CrossRef]
- KyngAs, H.A.; Kroll, T.; Duffy, M.E. Compliance in Adolescents with Chronic Diseases: A Review. J. Adolesc. Health 2000, 26, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Price, J.F. Issues in Adolescent Asthma: What Are the Needs? Thorax 1996, 51 (Suppl. 1), S13–S17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzgerald, D. Non-Compliance in Adolescents with Chronic Lung Disease: Causative Factors and Practical Approach. Paediatr. Respir. Rev. 2001, 2, 260–267. [Google Scholar] [CrossRef] [PubMed]
- McLean, C.P.; Anderson, E.R. Brave Men and Timid Women? A Review of the Gender Differences in Fear and Anxiety. Clin. Psychol. Rev. 2009, 29, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Breier, A.; Charney, D.S.; Heninger, G.R. Agoraphobia with Panic Attacks. Development, Diagnostic Stability, and Course of Illness. Arch. Gen. Psychiatry 1986, 43, 1029–1036. [Google Scholar] [CrossRef] [PubMed]
- Freeman, E.W. Premenstrual Syndrome and Premenstrual Dysphoric Disorder: Definitions and Diagnosis. Psychoneuroendocrinology 2003, 28 (Suppl. 3), 25–37. [Google Scholar] [CrossRef]
- Gonda, X.; Telek, T.; Juhász, G.; Lazary, J.; Vargha, A.; Bagdy, G. Patterns of Mood Changes throughout the Reproductive Cycle in Healthy Women without Premenstrual Dysphoric Disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 1782–1788. [Google Scholar] [CrossRef] [PubMed]
- Kaspi, S.P.; Otto, M.W.; Pollack, M.H.; Eppinger, S.; Rosenbaum, J.F. Premenstrual Exacerbation of Symptoms in Women with Panic Disorder. J. Anxiety Disord. 1994, 8, 131–138. [Google Scholar] [CrossRef]
- Kornstein, S.G.; Harvey, A.T.; Rush, A.J.; Wisniewski, S.R.; Trivedi, M.H.; Svikis, D.S.; McKenzie, N.D.; Bryan, C.; Harley, R. Self-Reported Premenstrual Exacerbation of Depressive Symptoms in Patients Seeking Treatment for Major Depression. Psychol. Med. 2005, 35, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Rees, L. An Aetiological Study of Premenstrual Asthma. J. Psychosom. Res. 1963, 7, 191–197. [Google Scholar] [CrossRef]
- Agarwal, A.K.; Shah, A. Menstrual-Linked Asthma. J. Asthma 1997, 34, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Vrieze, A.; Postma, D.S.; Kerstjens, H.A.M. Perimenstrual Asthma: A Syndrome without Known Cause or Cure. J. Allergy Clin. Immunol. 2003, 112, 271–282. [Google Scholar] [CrossRef] [PubMed]
- Graziottin, A.; Serafini, A. Perimenstrual Asthma: From Pathophysiology to Treatment Strategies. Multidiscip. Respir. Med. 2016, 11, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, C.K.; Moore, C.G.; Bleecker, E.; Busse, W.W.; Calhoun, W.; Castro, M.; Chung, K.F.; Erzurum, S.C.; Israel, E.; Curran-Everett, D.; et al. Characteristics of Perimenstrual Asthma and Its Relation to Asthma Severity and Control: Data from the Severe Asthma Research Program. Chest 2013, 143, 984–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, V.E.; Gibson, P.G. Premenstrual Asthma: Prevalence, Cycle-to-Cycle Variability and Relationship to Oral Contraceptive Use and Menstrual Symptoms. J. Asthma 2008, 45, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.E.; Holmes, T.M.; Mazal, B.; Camargo, C.A. Relation between Phase of the Menstrual Cycle and Asthma Presentations in the Emergency Department. Thorax 2005, 60, 806–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becklake, M.R.; Kauffmann, F. Gender Differences in Airway Behaviour over the Human Life Span. Thorax 1999, 54, 1119–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zein, J.G.; Erzurum, S.C. Asthma Is Different in Women. Curr. Allergy Asthma Rep. 2015, 15, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heitkemper, M.M.; Cain, K.C.; Jarrett, M.E.; Burr, R.L.; Hertig, V.; Bond, E.F. Symptoms across the Menstrual Cycle in Women with Irritable Bowel Syndrome. Am. J. Gastroenterol. 2003, 98, 420–430. [Google Scholar] [CrossRef] [PubMed]
- Rubtsova, K.; Marrack, P.; Rubtsov, A.V. Sexual Dimorphism in Autoimmunity. J. Clin. Investig. 2015, 125, 2187–2193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zandman-Goddard, G.; Peeva, E.; Shoenfeld, Y. Gender and Autoimmunity. Autoimmun. Rev. 2007, 6, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Wijga, A.; Tabak, C.; Postma, D.S.; Kerkhof, M.; Wieringa, M.H.; Hoekstra, M.O.; Brunekreef, B.; de Jongste, J.C.; Smit, H.A. Sex Differences in Asthma during the First 8 Years of Life: The Prevention and Incidence of Asthma and Mite Allergy (PIAMA) Birth Cohort Study. J. Allergy Clin. Immunol. 2011, 127, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Sears, M.R.; Burrows, B.; Flannery, E.M.; Herbison, G.P.; Holdaway, M.D. Atopy in Childhood. I. Gender and Allergen Related Risks for Development of Hay Fever and Asthma. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 1993, 23, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.C.; Peterson, E.L.; Ownby, D.R. Gender Differences in Total and Allergen-Specific Immunoglobulin E (IgE) Concentrations in a Population-Based Cohort from Birth to Age Four Years. Am. J. Epidemiol. 1998, 147, 1145–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulig, M.; Tacke, U.; Forster, J.; Edenharter, G.; Bergmann, R.; Lau, S.; Wahn, V.; Zepp, F.; Wahn, U. Serum IgE Levels during the First 6 Years of Life. J. Pediatr. 1999, 134, 453–458. [Google Scholar] [CrossRef]
- Mohammad, H.R.; Belgrave, D.; Kopec Harding, K.; Murray, C.S.; Simpson, A.; Custovic, A. Age, Sex and the Association between Skin Test Responses and IgE Titres with Asthma. Pediatr. Allergy Immunol. 2016, 27, 313–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uekert, S.J.; Akan, G.; Evans, M.D.; Li, Z.; Roberg, K.; Tisler, C.; Dasilva, D.; Anderson, E.; Gangnon, R.; Allen, D.B.; et al. Sex-Related Differences in Immune Development and the Expression of Atopy in Early Childhood. J. Allergy Clin. Immunol. 2006, 118, 1375–1381. [Google Scholar] [CrossRef] [PubMed]
- Douin-Echinard, V.; Calippe, B.; Billon-Galès, A.; Fontaine, C.; Lenfant, F.; Trémollières, F.; Bayard, F.; Guéry, J.-C.; Arnal, J.-F.; Gourdy, P. Estradiol Administration Controls Eosinophilia through Estrogen Receptor-Alpha Activation during Acute Peritoneal Inflammation. J. Leukoc. Biol. 2011, 90, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Huygen, K.; Palfliet, K. Strain Variation in Interferon Gamma Production of BCG-Sensitized Mice Challenged with PPD II. Importance of One Major Autosomal Locus and Additional Sexual Influences. Cell. Immunol. 1984, 85, 75–81. [Google Scholar] [CrossRef]
- Phiel, K.L.; Henderson, R.A.; Adelman, S.J.; Elloso, M.M. Differential Estrogen Receptor Gene Expression in Human Peripheral Blood Mononuclear Cell Populations. Immunol. Lett. 2005, 97, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Björnström, L.; Sjöberg, M. Mechanisms of Estrogen Receptor Signaling: Convergence of Genomic and Nongenomic Actions on Target Genes. Mol. Endocrinol. 2005, 19, 833–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filardo, E.J.; Quinn, J.A.; Frackelton, A.R.; Bland, K.I. Estrogen Action Via the G Protein-Coupled Receptor, GPR30: Stimulation of Adenylyl Cyclase and CAMP-Mediated Attenuation of the Epidermal Growth Factor Receptor-to-MAPK Signaling Axis. Mol. Endocrinol. 2002, 16, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, N.; Silveyra, P. Endocrine Regulation of Lung Disease and Inflammation. Exp. Biol. Med. 2018, 243, 1313–1322. [Google Scholar] [CrossRef] [Green Version]
- Massaro, D.; Massaro, G.D. Estrogen Regulates Pulmonary Alveolar Formation, Loss, and Regeneration in Mice. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2004, 287, L1154–L1159. [Google Scholar] [CrossRef] [PubMed]
- Straub, R.H. The Complex Role of Estrogens in Inflammation. Endocr. Rev. 2007, 28, 521–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambhore, N.S.; Kalidhindi, R.S.R.; Loganathan, J.; Sathish, V. Role of Differential Estrogen Receptor Activation in Airway Hyperreactivity and Remodeling in a Murine Model of Asthma. Am. J. Respir. Cell Mol. Biol. 2019, 61, 469–480. [Google Scholar] [CrossRef]
- Itoga, M.; Konno, Y.; Moritoki, Y.; Saito, Y.; Ito, W.; Tamaki, M.; Kobayashi, Y.; Kayaba, H.; Kikuchi, Y.; Chihara, J.; et al. Correction: G-Protein-Coupled Estrogen Receptor Agonist Suppresses Airway Inflammation in a Mouse Model of Asthma through IL-10. PLoS ONE 2015, 10, e0136326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aravamudan, B.; Goorhouse, K.J.; Unnikrishnan, G.; Thompson, M.A.; Pabelick, C.M.; Hawse, J.R.; Prakash, Y.S.; Sathish, V. Differential Expression of Estrogen Receptor Variants in Response to Inflammation Signals in Human Airway Smooth Muscle: Expression of estrogen receptor variants in the airway. J. Cell. Physiol. 2017, 232, 1754–1760. [Google Scholar] [CrossRef]
- Ambhore, N.S.; Katragadda, R.; Raju Kalidhindi, R.S.; Thompson, M.A.; Pabelick, C.M.; Prakash, Y.S.; Sathish, V. Estrogen Receptor Beta Signaling Inhibits PDGF Induced Human Airway Smooth Muscle Proliferation. Mol. Cell. Endocrinol. 2018, 476, 37–47. [Google Scholar] [CrossRef]
- Hocking, D.C. Fibronectin Matrix Deposition and Cell Contractility. Chest 2002, 122, 275S–278S. [Google Scholar] [CrossRef]
- Fahy, J.V. Type 2 Inflammation in Asthma--Present in Most, Absent in Many. Nat. Rev. Immunol. 2015, 15, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Ray, A.; Raundhal, M.; Oriss, T.B.; Ray, P.; Wenzel, S.E. Current Concepts of Severe Asthma. J. Clin. Investig. 2016, 126, 2394–2403. [Google Scholar] [CrossRef] [PubMed]
- Fahy, J.V. Eosinophilic and Neutrophilic Inflammation in Asthma: Insights from Clinical Studies. Proc. Am. Thorac. Soc. 2009, 6, 256–259. [Google Scholar] [CrossRef]
- Htet, T.D.; Teede, H.J.; de Courten, B.; Loxton, D.; Real, F.G.; Moran, L.J.; Joham, A.E. Asthma in Reproductive-Aged Women with Polycystic Ovary Syndrome and Association with Obesity. Eur. Respir. J. 2017, 49, 1601334. [Google Scholar] [CrossRef] [Green Version]
- Leon, G.; de Klerk, E.; Ho, J.; Jackman, M.; Reimer, R.A.; Connors, K.E.; Luca, P. Prevalence of Comorbid Conditions Pre-Existing and Diagnosed at a Tertiary Care Pediatric Weight Management Clinic. J. Pediatr. Endocrinol. Metab. 2018, 31, 385–390. [Google Scholar] [CrossRef]
- Maybin, J.A.; Critchley, H.O.D. Progesterone: A Pivotal Hormone at Menstruation: Progesterone and Menstruation. Ann. N. Y. Acad. Sci. 2011, 1221, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.H. Gynecology and Obstetrics. Vol. II, Chap. 3; W. F. Prior Co. Inc.: Hagerstown, MD, USA; pp. 17–50.
- Nieschlag, E.; Behre, H.M.; Nieschlag, S. Testosterone: Action, Deficiency, Substitution; Cambridge University Press: Cambridge, UK, 2012; ISBN 1-107-01290-2. [Google Scholar]
- Kouloumenta, V.; Hatziefthimiou, A.; Paraskeva, E.; Gourgoulianis, K.; Molyvdas, P.A. Non-Genomic Effect of Testosterone on Airway Smooth Muscle. Br. J. Pharmacol. 2006, 149, 1083–1091. [Google Scholar] [CrossRef] [Green Version]
- Eliasson, O.; Scherzer, H.H.; DeGraff, A.C. Morbidity in Asthma in Relation to the Menstrual Cycle. J. Allergy Clin. Immunol. 1986, 77, 87–94. [Google Scholar] [CrossRef]
- Shames, R.S.; Heilbron, D.C.; Janson, S.L.; Kishiyama, J.L.; Au, D.S.; Adelman, D.C. Clinical Differences among Women with and without Self-Reported Perimenstrual Asthma. Ann. Allergy Asthma Immunol. 1998, 81, 65–72. [Google Scholar] [CrossRef]
- Leuenberger, P.; Künzli, N.; Ackermann-Liebrich, U.; Schindler, C.; Bolognini, G.; Bongard, J.P.; Brändli, O.; Defila, C.; Domenighetti, G.; Karrer, W.; et al. Swiss Study on Air Pollution and Lung Diseases in Adults (SAPALDIA). Schweiz. Med. Wochenschr. 1998, 128, 150–161. [Google Scholar] [PubMed]
- Liou, C.-J.; Huang, W.-C. Dehydroepiandrosterone Suppresses Eosinophil Infiltration and Airway Hyperresponsiveness via Modulation of Chemokines and Th2 Cytokines in Ovalbumin-Sensitized Mice. J. Clin. Immunol. 2011, 31, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, J.; Montaño, L.M.; Perusquía, M. Nongenomic Bronchodilating Action Elicited by Dehydroepiandrosterone (DHEA) in a Guinea Pig Asthma Model. J. Steroid Biochem. Mol. Biol. 2013, 138, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, S.E.; Robinson, C.B.; Leonard, J.M.; Panettieri, R.A. Nebulized Dehydroepiandrosterone-3-Sulfate Improves Asthma Control in the Moderate-to-Severe Asthma Results of a 6-Week, Randomized, Double-Blind, Placebo-Controlled Study. Allergy Asthma Proc. 2010, 31, 461–471. [Google Scholar] [CrossRef]
- Zhang, G.-Q.; Bossios, A.; Rådinger, M.; Nwaru, B.I. Sex Steroid Hormones and Asthma in Women: State-of-the-Art and Future Research Perspectives. Expert Rev. Respir. Med. 2020, 14, 543–545. [Google Scholar] [CrossRef]
- Nwaru, B.I.; Ekström, M.; Hasvold, P.; Wiklund, F.; Telg, G.; Janson, C. Overuse of Short-Acting Β2-Agonists in Asthma Is Associated with Increased Risk of Exacerbation and Mortality: A Nationwide Cohort Study of the Global SABINA Programme. Eur. Respir. J. 2020, 55, 1901872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, J.; McSharry, J.; Hynes, L.; Matthews, S.; Van Rhoon, L.; Molloy, G.J. Prevalence and Predictors of Adherence to Inhaled Corticosteroids in Young Adults (15–30 Years) with Asthma: A Systematic Review and Meta-Analysis. J. Asthma 2021, 58, 683–705. [Google Scholar] [CrossRef] [PubMed]
- Magadle, R.; Berar-Yanay, N.; Weiner, P. Long-Acting Bronchodilators in Premenstrual Exacerbation of Asthma. Respir. Med. 2001, 95, 740–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de, C. Baldaçara, R.P.; Silva, I. Association between Asthma and Female Sex Hormones. Sao Paulo Med. J. Rev. Paul. Med. 2017, 135, 4–14. [Google Scholar] [CrossRef] [Green Version]
- Macsali, F.; Real, F.G.; Omenaas, E.R.; Bjorge, L.; Janson, C.; Franklin, K.; Svanes, C. Oral Contraception, Body Mass Index, and Asthma: A Cross-Sectional Nordic-Baltic Population Survey. J. Allergy Clin. Immunol. 2009, 123, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Erkoçoğlu, M.; Kaya, A.; Azkur, D.; Özyer, Ş.; Özcan, C.; Beşli, M.; Civelek, E.; Kocabaş, C.N. The Effect of Oral Contraceptives on Current Wheezing in Young Women. Allergol. Immunopathol. 2013, 41, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Guthikonda, K.; Zhang, H.; Nolan, V.G.; Soto-Ramírez, N.; Ziyab, A.H.; Ewart, S.; Arshad, H.S.; Patil, V.; Holloway, J.W.; Lockett, G.A.; et al. Oral Contraceptives Modify the Effect of GATA3 Polymorphisms on the Risk of Asthma at the Age of 18 Years via DNA Methylation. Clin. Epigenetics 2014, 6, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, K.S.; McFarlane, L.C.; Lipworth, B.J. Beta2-Adrenoceptor Regulation and Function in Female Asthmatic Patients Receiving the Oral Combined Contraceptive Pill. Chest 1998, 113, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Lange, P.; Parner, J.; Prescott, E.; Ulrik, C.S.; Vestbo, J. Exogenous Female Sex Steroid Hormones and Risk of Asthma and Asthma-like Symptoms: A Cross Sectional Study of the General Population. Thorax 2001, 56, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.S.; McFarlane, L.C.; Lipworth, B.J. Modulation of Airway Reactivity and Peak Flow Variability in Asthmatics Receiving the Oral Contraceptive Pill. Am. J. Respir. Crit. Care Med. 1997, 155, 1273–1277. [Google Scholar] [CrossRef] [PubMed]
- Vélez-Ortega, A.C.; Temprano, J.; Reneer, M.C.; Ellis, G.I.; McCool, A.; Gardner, T.; Khosravi, M.; Marti, F. Enhanced Generation of Suppressor T Cells in Patients with Asthma Taking Oral Contraceptives. J. Asthma 2013, 50, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Nwaru, B.I.; Sheikh, A. Hormonal Contraceptives and Asthma in Women of Reproductive Age: Analysis of Data from Serial National Scottish Health Surveys. J. R. Soc. Med. 2015, 108, 358–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, M.A.; Dharmage, S.C.; Flander, L.B.; Douglass, J.A.; Ugoni, A.M.; Carlin, J.B.; Sawyer, S.M.; Giles, G.G.; Hopper, J.L. Parity and Decreased Use of Oral Contraceptives as Predictors of Asthma in Young Women. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2006, 36, 609–613. [Google Scholar] [CrossRef]
- Nwaru, B.I.; Tibble, H.; Shah, S.A.; Pillinger, R.; McLean, S.; Ryan, D.P.; Critchley, H.; Price, D.B.; Hawrylowicz, C.M.; Simpson, C.R.; et al. Hormonal Contraception and the Risk of Severe Asthma Exacerbation: 17-Year Population-Based Cohort Study. Thorax 2021, 76, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Nwaru, B.I.; Pillinger, R.; Tibble, H.; Shah, S.A.; Ryan, D.; Critchley, H.; Price, D.; Hawrylowicz, C.M.; Simpson, C.R.; Soyiri, I.N.; et al. Hormonal Contraceptives and Onset of Asthma in Reproductive-Age Women: Population-Based Cohort Study. J. Allergy Clin. Immunol. 2020, 146, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Cruz, S.; Togno-Pierce, C.; Morales-Montor, J. Non-Reproductive Effects of Sex Steroids: Their Immunoregulatory Role. Curr. Top. Med. Chem. 2011, 11, 1714–1727. [Google Scholar] [CrossRef] [PubMed]
- Bitzer, J.; Banal-Silao, M.J.; Ahrendt, H.-J.; Restrepo, J.; Hardtke, M.; Wissinger-Graefenhahn, U.; Trummer, D. Hormone Withdrawal-Associated Symptoms with Ethinylestradiol 20 Μg/Drospirenone 3 Mg (24/4 Regimen) versus Ethinylestradiol 20 Μg/Desogestrel 150 Μg (21/7 Regimen). Int. J. Womens Health 2015, 7, 501–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nappi, R.E.; Kaunitz, A.M.; Bitzer, J. Extended Regimen Combined Oral Contraception: A Review of Evolving Concepts and Acceptance by Women and Clinicians. Eur. J. Contracept. Reprod. Health Care 2016, 21, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, K.; Borade, A. Anemia as a Risk Factor for Childhood Asthma. Lung India 2010, 27, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Borzutzky, C.; Jaffray, J. Diagnosis and Management of Heavy Menstrual Bleeding and Bleeding Disorders in Adolescents. JAMA Pediatr. 2020, 174, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.T.; Bitzer, J.; Nappi, R.E.; Ahlers, C.; Bannemerschult, R.; Parke, S. Pooled Analysis of Bleeding Profile, Efficacy and Safety of Oral Oestradiol Valerate/Dienogest in Women Aged 25 and Under. Eur. J. Contracept. Reprod. Health Care 2020, 25, 98–105. [Google Scholar] [CrossRef] [Green Version]
- Brigham, E.P.; McCormack, M.C.; Takemoto, C.M.; Matsui, E.C. Iron Status Is Associated with Asthma and Lung Function in US Women. PLoS ONE 2015, 10, e0117545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matalliotakis, M.; Goulielmos, G.N.; Matalliotaki, C.; Trivli, A.; Matalliotakis, I.; Arici, A. Endometriosis in Adolescent and Young Girls: Report on a Series of 55 Cases. J. Pediatr. Adolesc. Gynecol. 2017, 30, 568–570. [Google Scholar] [CrossRef]
- Sánchez-Ramos, J.L.; Pereira-Vega, A.R.; Alvarado-Gómez, F.; Maldonado-Pérez, J.A.; Svanes, C.; Gómez-Real, F. Risk Factors for Premenstrual Asthma: A Systematic Review and Meta-Analysis. Expert Rev. Respir. Med. 2017, 11, 57–72. [Google Scholar] [CrossRef]
- Grandi, G.; Barra, F.; Ferrero, S.; Sileo, F.G.; Bertucci, E.; Napolitano, A.; Facchinetti, F. Hormonal Contraception in Women with Endometriosis: A Systematic Review. Eur. J. Contracept. Reprod. Health Care 2019, 24, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.-Y.; Forno, E.; Celedón, J.C. Sex Steroid Hormones and Asthma in a Nationwide Study of U.S. Adults. Am. J. Respir. Crit. Care Med. 2020, 201, 158–166. [Google Scholar] [CrossRef]
- Tan, K.S.; McFarlane, L.C.; Lipworth, B.J. Loss of Normal Cyclical Beta 2 Adrenoceptor Regulation and Increased Premenstrual Responsiveness to Adenosine Monophosphate in Stable Female Asthmatic Patients. Thorax 1997, 52, 608–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlović, J.M.; Allshouse, A.A.; Santoro, N.F.; Crawford, S.L.; Thurston, R.C.; Neal-Perry, G.S.; Lipton, R.B.; Derby, C.A. Sex Hormones in Women with and without Migraine: Evidence of Migraine-Specific Hormone Profiles. Neurology 2016, 87, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Beynon, H.L.; Garbett, N.D.; Barnes, P.J. Severe Premenstrual Exacerbations of Asthma: Effect of Intramuscular Progesterone. Lancet 1988, 2, 370–372. [Google Scholar] [CrossRef]
- Tan, K.S.; McFarlane, L.C.; Lipworth, B.J. Paradoxical Down-Regulation and Desensitization of Beta2-Adrenoceptors by Exogenous Progesterone in Female Asthmatics. Chest 1997, 111, 847–851. [Google Scholar] [CrossRef] [PubMed]
- Zein, J.G.; McManus, J.M.; Sharifi, N.; Erzurum, S.C.; Marozkina, N.; Lahm, T.; Giddings, O.; Davis, M.D.; DeBoer, M.D.; Comhair, S.A.; et al. Benefits of Airway Androgen Receptor Expression in Human Asthma. Am. J. Respir. Crit. Care Med. 2021, 204, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Yung, J.A.; Fuseini, H.; Newcomb, D.C. Hormones, Sex, and Asthma. Ann. Allergy Asthma Immunol. 2018, 120, 488–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, P.J.; Mahood, C.B.; Speed, J.F.; Jury, D.R. Dehydroepiandrosterone Sulphate Concentrations in Asthmatic Patients: Pilot Study. N. Z. Med. J. 1984, 97, 805–808. [Google Scholar] [PubMed]
- Pasaoglu, G.; Mungan, D.; Abadoglu, O.; Misirligil, Z. Leukotriene Receptor Antagonists: A Good Choice in the Treatment of Premenstrual Asthma? J. Asthma 2008, 45, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Li, F.; Liang, B.; Liang, Y.; Chen, S.; Mo, X.; Ju, Y.; Zhao, H.; Jia, H.; Spector, T.D.; et al. A Metagenome-Wide Association Study of Gut Microbiota in Asthma in UK Adults. BMC Microbiol. 2018, 18, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, N.S.; Nanji, K. A Review on the Role of Vitamin D in Asthma. Cureus 2017. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Hernández, N.; Aptilon-Duque, G.; Nostroza-Hernández, M.C.; Vargas-Alarcón, G.; Rodríguez-Pérez, J.M.; Blachman-Braun, R. Vitamin D and Its Effects on Cardiovascular Diseases: A Comprehensive Review. Korean J. Intern. Med. 2016, 31, 1018–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michos, E.D.; Selvin, E.; Misialek, J.R.; McEvoy, J.W.; Ndumele, C.E.; Folsom, A.R.; Ballantyne, C.M.; Lutsey, P.L. 25-Hydroxyvitamin D Levels and Markers of Subclinical Myocardial Damage and Wall Stress: The Atherosclerosis Risk in Communities Study. J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D. Extraskeletal Actions of Vitamin D: Extraskeletal Actions of Vitamin D. Ann. N. Y. Acad. Sci. 2016, 1376, 29–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, J.H. Vitamin D Metabolism and Signaling in the Immune System. Rev. Endocr. Metab. Disord. 2012, 13, 21–29. [Google Scholar] [CrossRef]
- Franasiak, J.M. Vitamin D in Human Reproduction—an Evolving Landscape. Fertil. Steril. 2016, 106, 1650–1651. [Google Scholar] [CrossRef] [Green Version]
- Pacis, M.M.; Fortin, C.N.; Zarek, S.M.; Mumford, S.L.; Segars, J.H. Vitamin D and Assisted Reproduction: Should Vitamin D Be Routinely Screened and Repleted Prior to ART? A Systematic Review. J. Assist. Reprod. Genet. 2015, 32, 323–335. [Google Scholar] [CrossRef] [Green Version]
- Rajaei, S.; Mirahmadian, M.; Jeddi-Tehrani, M.; Tavakoli, M.; Zonoobi, M.; Dabbagh, A.; Zarnani, A.H. Effect of 1,25(OH)2 Vitamin D3 on Cytokine Production by Endometrial Cells of Women with Repeated Implantation Failure. Gynecol. Endocrinol. 2012, 28, 906–911. [Google Scholar] [CrossRef]
- Tavakoli, M.; Jeddi-Tehrani, M.; Salek-Moghaddam, A.; Rajaei, S.; Mohammadzadeh, A.; Sheikhhasani, S.; Kazemi-Sefat, G.-E.; Zarnani, A.H. Effects of 1,25(OH)2 Vitamin D3 on Cytokine Production by Endometrial Cells of Women with Recurrent Spontaneous Abortion. Fertil. Steril. 2011, 96, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Chambers, E.S.; Hawrylowicz, C.M. The Impact of Vitamin D on Regulatory T Cells. Curr. Allergy Asthma Rep. 2011, 11, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Parodi, V.; de Florentiis, D.; Martini, M.; Ansaldi, F. Inactivated Influenza Vaccines: Recent Progress and Implications for the Elderly. Drugs Aging 2011, 28, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P.; Holick, M.F. Why the IOM Recommendations for Vitamin D Are Deficient. J. Bone Miner. Res. 2011, 26, 455–457. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.; Muntner, P.; Kaskel, F.J.; Hailpern, S.M.; Melamed, M.L. Prevalence and Associations of 25-Hydroxyvitamin D Deficiency in US Children: NHANES 2001–2004. Pediatrics 2009, 124, e362–e370. [Google Scholar] [CrossRef] [Green Version]
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the Immune System. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Chinellato, I.; Piazza, M.; Sandri, M.; Peroni, D.; Piacentini, G.; Boner, A.L. Vitamin D Serum Levels and Markers of Asthma Control in Italian Children. J. Pediatr. 2011, 158, 437–441. [Google Scholar] [CrossRef]
- Devereux, G.; Wilson, A.; Avenell, A.; McNeill, G.; Fraser, W.D. A Case-Control Study of Vitamin D Status and Asthma in Adults. Allergy 2010, 65, 666–667. [Google Scholar] [CrossRef]
- Urashima, M.; Segawa, T.; Okazaki, M.; Kurihara, M.; Wada, Y.; Ida, H. Randomized Trial of Vitamin D Supplementation to Prevent Seasonal Influenza A in Schoolchildren. Am. J. Clin. Nutr. 2010, 91, 1255–1260. [Google Scholar] [CrossRef] [Green Version]
- Majak, P.; Olszowiec-Chlebna, M.; Smejda, K.; Stelmach, I. Vitamin D Supplementation in Children May Prevent Asthma Exacerbation Triggered by Acute Respiratory Infection. J. Allergy Clin. Immunol. 2011, 127, 1294–1296. [Google Scholar] [CrossRef] [PubMed]
- Yadav, M.; Mittal, K. Effect of Vitamin D Supplementation on Moderate to Severe Bronchial Asthma. Indian J. Pediatr. 2014, 81, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Gale, C.R.; Gale, R.S.; Robinson, H.N.; Harvey, N.C.; Javaid, M.K.; Jiang, B.; Martyn, C.N.; Godfrey, K.M.; Cooper, C. Maternal Vitamin D Status during Pregnancy and Child Outcomes. Eur. J. Clin. Nutr. 2008, 62, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollams, E.M.; Hart, P.H.; Holt, B.J.; Serralha, M.; Parsons, F.; de Klerk, N.H.; Zhang, G.; Sly, P.D.; Holt, P.G. Vitamin D and Atopy and Asthma Phenotypes in Children: A Longitudinal Cohort Study. Eur. Respir. J. 2011, 38, 1320–1327. [Google Scholar] [CrossRef]
- Brehm, J.M.; Celedón, J.C.; Soto-Quiros, M.E.; Avila, L.; Hunninghake, G.M.; Forno, E.; Laskey, D.; Sylvia, J.S.; Hollis, B.W.; Weiss, S.T.; et al. Serum Vitamin D Levels and Markers of Severity of Childhood Asthma in Costa Rica. Am. J. Respir. Crit. Care Med. 2009, 179, 765–771. [Google Scholar] [CrossRef] [Green Version]
- Shahin, M.Y.A.; El-lawah, A.A.; Amin, A.; El-Tawil, I.A.H. Study of Serum Vitamin D Level in Adult Patients with Bronchial Asthma. Egypt. J. Chest Dis. Tuberc. 2017, 66, 5–9. [Google Scholar] [CrossRef]
- Brehm, J.M.; Acosta-Pérez, E.; Klei, L.; Roeder, K.; Barmada, M.; Boutaoui, N.; Forno, E.; Kelly, R.; Paul, K.; Sylvia, J.; et al. Vitamin D Insufficiency and Severe Asthma Exacerbations in Puerto Rican Children. Am. J. Respir. Crit. Care Med. 2012, 186, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Tachimoto, H.; Mezawa, H.; Segawa, T.; Akiyama, N.; Ida, H.; Urashima, M. Improved Control of Childhood Asthma with Low-Dose, Short-Term Vitamin D Supplementation: A Randomized, Double-Blind, Placebo-Controlled Trial. Allergy 2016, 71, 1001–1009. [Google Scholar] [CrossRef]
- Heidari, H.; Amani, R.; Feizi, A.; Askari, G.; Kohan, S.; Tavasoli, P. Vitamin D Supplementation for Premenstrual Syndrome-Related Inflammation and Antioxidant Markers in Students with Vitamin D Deficient: A Randomized Clinical Trial. Sci. Rep. 2019, 9, 14939. [Google Scholar] [CrossRef]
- Tartagni, M.; Cicinelli, M.V.; Tartagni, M.V.; Alrasheed, H.; Matteo, M.; Baldini, D.; De Salvia, M.; Loverro, G.; Montagnani, M. Vitamin D Supplementation for Premenstrual Syndrome-Related Mood Disorders in Adolescents with Severe Hypovitaminosis D. J. Pediatr. Adolesc. Gynecol. 2016, 29, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Dadkhah, H.; Ebrahimi, E.; Fathizadeh, N. Evaluating the Effects of Vitamin D and Vitamin E Supplement on Premenstrual Syndrome: A Randomized, Double-Blind, Controlled Trial. Iran. J. Nurs. Midwifery Res. 2016, 21, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khajehei, M.; Abdali, K.; Parsanezhad, M.E.; Tabatabaee, H.R. Effect of Treatment with Dydrogesterone or Calcium plus Vitamin D on the Severity of Premenstrual Syndrome. Int. J. Gynecol. Obstet. 2009, 105, 158–161. [Google Scholar] [CrossRef] [PubMed]
- Thys-Jacobs, S.; Alvir, M.J. Calcium-Regulating Hormones across the Menstrual Cycle: Evidence of a Secondary Hyperparathyroidism in Women with PMS. J. Clin. Endocrinol. Metab. 1995, 80, 2227–2232. [Google Scholar] [CrossRef] [PubMed]
- Thys-Jacobs, S. Vitamin D and Calcium in Menstrual Migraine. Headache J. Head Face Pain 1994, 34, 544–546. [Google Scholar] [CrossRef] [PubMed]
- Azizieh, F.; Alyahya, K.; Dingle, K. Association of Self-Reported Symptoms with Serum Levels of Vitamin D and Multivariate Cytokine Profile in Healthy Women. J. Inflamm. Res. 2017, 10, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertone-Johnson, E.R.; Ronnenberg, A.G.; Houghton, S.C.; Nobles, C.; Zagarins, S.E.; Takashima-Uebelhoer, B.B.; Faraj, J.L.; Whitcomb, B.W. Association of Inflammation Markers with Menstrual Symptom Severity and Premenstrual Syndrome in Young Women. Hum. Reprod. 2014, 29, 1987–1994. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Early Follicular Phase | Preovulatory Phase | Midluteal Phase | |
|---|---|---|---|
| Estradiol (pg/mL) | 40–50 | 250–380 | 100–250 |
| Progesterone (ng/mL) | <1 | 10–35 | |
| Androstenedione (ng/mL) | 2.2 | 2.7 | 2.6 |
| Testosterone (nmol/L) | 0.96 | 1.27 | 0.91 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calcaterra, V.; Nappi, R.E.; Farolfi, A.; Tiranini, L.; Rossi, V.; Regalbuto, C.; Zuccotti, G. Perimenstrual Asthma in Adolescents: A Shared Condition in Pediatric and Gynecological Endocrinology. Children 2022, 9, 233. https://doi.org/10.3390/children9020233
Calcaterra V, Nappi RE, Farolfi A, Tiranini L, Rossi V, Regalbuto C, Zuccotti G. Perimenstrual Asthma in Adolescents: A Shared Condition in Pediatric and Gynecological Endocrinology. Children. 2022; 9(2):233. https://doi.org/10.3390/children9020233
Chicago/Turabian StyleCalcaterra, Valeria, Rossella Elena Nappi, Andrea Farolfi, Lara Tiranini, Virginia Rossi, Corrado Regalbuto, and Gianvincenzo Zuccotti. 2022. "Perimenstrual Asthma in Adolescents: A Shared Condition in Pediatric and Gynecological Endocrinology" Children 9, no. 2: 233. https://doi.org/10.3390/children9020233
APA StyleCalcaterra, V., Nappi, R. E., Farolfi, A., Tiranini, L., Rossi, V., Regalbuto, C., & Zuccotti, G. (2022). Perimenstrual Asthma in Adolescents: A Shared Condition in Pediatric and Gynecological Endocrinology. Children, 9(2), 233. https://doi.org/10.3390/children9020233