Antimicrobial Activity of Geranium Oil against Clinical Strains of Staphylococcus aureus


Abstract
:1. Introduction
2. Results
2.1. Chemical Composition of Geranium Oil

{kind=link}
| Number | Compound | % (relative) | RI |
|---|---|---|---|
| 1 | α-Pinene | 0.7 | 929 |
| 2 | β-Pinene | tr | 979 |
| 3 | Myrcene | 0.1 | 983 |
| 4 | Car-2-ene | tr | 986 |
| 5 | α-Phellandrene | 0.1 | 996 |
| 6 | p-Cymene | 0.1 | 1,012 |
| 7 | β-Phellandrene | tr | 1,020 |
| 8 | Limonene | 0.2 | 1,021 |
| 9 | (Z)-β-Ocimene | tr | 1,028 |
| 10 | (E)-β-Ocimene | 0.1 | 1,039 |
| 11 | cis-Linlool oxide (f) | 0.3 | 1,058 |
| 12 | trans-Linlool oxide (f) | 0.1 | 1,072 |
| 13 | Terpinolene | tr | 1,079 |
| 14 | Linalool | 5.2 | 1,086 |
| 15 | cis-Rose oxide | 1.4 | 1,097 |
| 16 | trans-Rose oxide | 0.6 | 1,113 |
| 17 | α-Cyclogeraniol | tr | 1,127 |
| 18 | Isopulegol | 0.1 | 1,130 |
| 19 | Menthone | 1.6 | 1,133 |
| 20 | Isomenthone | 6.3 | 1,144 |
| 21 | Isomenthol | 0.1 | 1,168 |
| 22 | α-Terpineol | 0.3 | 1,173 |
| 23 | Estragole | 0.1 | 1,177 |
| 24 | Citronellol | 26.7 | 1,217 |
| 25 | Nerol | 8.7 | 1,220 |
| 26 | Geraniol | 13.4 | 1,243 |
| 27 | Geranial | 1.1 | 1,246 |
| 28 | Citronellyl formate | 7.1 | 1,261 |
| 29 | Neryl formate | 0.1 | 1,264 |
| 30 | Geranyl formate | 2.5 | 1,283 |
| 31 | Bicycloelemene Citronellyl acetate | 0.4 | 1,334 |
| 32 | α-Cubebene | 0.2 | 1,349 |
| 33 | Geranyl acetate | 0.4 | 1,361 |
| 34 | α-Copaene | 0.5 | 1,377 |
| 35 | β-Bourbonene | 1.1 | 1,385 |
| 36 | 1,5-di-epi-Bourbonene | 0.2 | 1,388 |
| 37 | α-Gurjunene | 0.1 | 1,411 |
| 38 | β-Caryophyllene | 1.5 | 1,419 |
| 39 | Citronellyl propionate | 0.3 | 1,425 |
| 40 | β-Copaene | 0.2 | 1,428 |
| 41 | Guaia-6,9-diene | 0.3 | 1,439 |
| 42 | 4aH,10aH-Guaia-1(5),6-diene | 0.1 | 1,442 |
| 43 | 4bH,10aH-Guaia-1(5),6-diene | 0.5 | 1,445 |
| 44 | Geranyl propionate | 1.0 | 1,452 |
| 45 | Alloaromadendrene | 0.2 | 1,459 |
| 46 | 7aH,10bH-Cadina-1(6),4-diene | 0.2 | 1,469 |
| 47 | γ-Muurolene | 0.1 | 1,471 |
| 48 | Germacrene D | 1.0 | 1,477 |
| 49 | γ-Selinene | 0.1 | 1,479 |
| 50 | β-Selinene | 0.2 | 1,482 |
| 51 | Bicyclogermacrene | 0.7 | 1,491 |
| 52 | α-Muurolene | 0.2 | 1,496 |
| 53 | Dihydroagarofuran | 0.1 | 1,500 |
| 54 | γ-Cadinene | 0.6 | 1,509 |
| 55 | trans-Calamenene | 0.3 | 1,510 |
| 56 | δ-Cadinene | 0.9 | 1,515 |
| 57 | Zonarene | 0.2 | 1,518 |
| 58 | Cadina-1,4-diene | 0.1 | 1,525 |
| 59 | Selina-4(15),7(11)-diene | 0.2 | 1,530 |
| 60 | Geranyl butyrate | 1.4 | 1,537 |
| 61 | Phenylethyl tiglate | 0.7 | 1,554 |
| 62 | Geranyl isovalerate | 0.1 | 1,582 |
| 63 | 10-epi-γ-Eudesmol | 4.4 | 1,613 |
| 64 | γ-Eudesmol | 0.1 | 1,620 |
| 65 | Geranyl tiglate | 1.0 | 1,675 |
| 66 | Geranyl ester I | 0.2 | 1,694 |
| 67 | Geranyl ester II | 0.1 | 1,730 |
2.2. Susceptibility to Antibiotics among the Clinical S. aureus Strains
| No. | MIC of geranium essential oil [µL/mL] | Susceptibility to antibiotics | Total | ||||||||||||||||||
| FOX MIC [µg/mL] | P | CIP | CN | E | DA | QD | TE | TGC | C | FD | LZD | RA | VA | DPC | SXT | R | I | S | |||
| 1. | 0.75 | R | 24 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 4 | 0 | 12 |
| 2. | 1.75 | R | 24 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 4 | 0 | 12 |
| 3. | 0.25 | S | 2 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 3 | 0 | 13 |
| 4. | 1.00 | R | 16 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 4 | 0 | 12 |
| 5. | 1.50 | R | 8 | R | S | S | S | S | S | R | S | R | S | S | S | S | S | S | 4 | 0 | 12 |
| 6. | 1.00 | R | 8 | R | S | R | R | R | S | I | S | S | S | S | S | S | S | S | 5 | 1 | 10 |
| 7. | 1.00 | S | 3 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 3 | 0 | 13 |
| 8. | 1.00 | R | 32 | R | R | R | R | R | S | S | S | S | S | S | S | S | S | S | 6 | 0 | 10 |
| No. | MIC of geranium essential oil [µL/mL] | Susceptibility to antibiotics | Total | ||||||||||||||||||
| FOX MIC [µg/mL] | P | CIP | CN | E | DA | QD | TE | TGC | C | FD | LZD | RA | VA | DPC | SXT | R | I | S | |||
| 1. | 0.25 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 2. | 1.00 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 3. | 1.00 | S | 2 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 4. | 1.00 | S | 1.5 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 5. | 0.25 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 6. | 1.25 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 7. | 1.50 | R | 32 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 4 | 0 | 12 |
| 8. | 1.00 | R | 12 | R | S | R | R | R | S | S | S | S | S | S | S | S | S | S | 5 | 0 | 11 |
| 9. | 1.00 | R | 12 | R | S | S | R | R | S | S | S | R | S | S | S | S | S | S | 5 | 0 | 11 |
| No. | MIC of geranium essential oil [µL/mL] | Susceptibility to antibiotics | Total | ||||||||||||||||||
| FOX MIC [µg/mL] | P | CIP | CN | E | DA | QD | TE | TGC | C | FD | LZD | RA | VA | DPC | SXT | R | I | S | |||
| 1. | 1.00 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 2. | 1.25 | S | 3 | S | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 0 | 0 | 16 |
| 3. | 2.25 | R | 8 | R | S | S | S | S | S | R | S | S | S | S | S | S | S | S | 3 | 0 | 13 |
| 4. | 2.25 | S | 3 | S | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 0 | 0 | 16 |
| 5. | 1.00 | S | 3 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 3 | 0 | 13 |
| 6. | 0.75 | S | 3 | S | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
| 7. | 1.50 | R | 8 | R | S | S | R | R | S | R | S | R | S | S | S | S | S | S | 6 | 0 | 10 |
| 8. | 0.50 | R | 48 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
| No. | MIC of geranium essential oil [µL/mL] | Susceptibility to antibiotics | Total | ||||||||||||||||||
| FOX MIC [µg/mL] | P | CIP | CN | E | DA | QD | TE | TGC | C | FD | LZD | RA | VA | DPC | SXT | R | I | S | |||
| 1. | 0.25 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 2. | 0.25 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 3. | 1.00 | R | 96 | R | R | S | R | R | S | S | S | S | S | S | S | S | S | S | 5 | 0 | 11 |
| 4. | 0.25 | S | 2 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 5. | 1.50 | R | 24 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
| 6. | 1.50 | S | 2 | S | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 0 | 0 | 16 |
| 7. | 0.25 | R | 16 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 4 | 0 | 12 |
| 8. | 0.25 | R | 24 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
| 9. | 0.75 | R | 24 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 4 | 0 | 12 |
| 10. | 0.75 | R | 48 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
| 11. | 2.50 | R | 8 | R | S | S | R | R | S | R | S | R | S | S | S | S | S | S | 6 | 0 | 10 |
| 12. | 0.50 | R | 256 | R | R | R | R | R | S | R | S | S | S | S | S | S | S | S | 7 | 0 | 9 |
| 13. | 1.50 | R | 128 | R | R | S | R | R | S | S | S | S | S | S | S | S | S | S | 5 | 0 | 11 |
| 14. | 1.50 | R | 8 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
| No. | MIC of geranium essential oil [µL/mL] | Susceptibility to antibiotics | Total | ||||||||||||||||||
| FOX MIC [µg/mL] | P | CIP | CN | E | DA | QD | TE | TGC | C | FD | LZD | RA | VA | DPC | SXT | R | I | S | |||
| 1. | 0.25 | R | 32 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
| 2. | 0.75 | S | 3 | S | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 0 | 0 | 16 |
| 3. | 0.75 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 4. | 1.50 | S | 1.5 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 5. | 1.00 | S | 2 | S | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
| 6. | 1.00 | R | 12 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 4 | 0 | 12 |
| No. | MIC of geranium essential oil [µL/mL] | Susceptibility to antibiotics | Total | ||||||||||||||||||
| FOX MIC [µg/mL] | P | CIP | CN | E | DA | QD | TE | TGC | C | FD | LZD | RA | VA | DPC | SXT | R | I | S | |||
| 1. | 1.00 | S | 3 | R | S | S | S | S | S | R | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
| 2. | 0.25 | S | 1.5 | S | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 0 | 0 | 16 |
| 3. | 2.25 | S | 3 | S | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 0 | 0 | 16 |
| 4. | 1.00 | S | 3 | S | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 0 | 0 | 16 |
| 5. | 1.50 | S | 2 | R | S | S | S | S | S | R | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
| 6. | 0.75 | S | 3 | S | S | R | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 7. | 1.00 | R | 12 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 4 | 0 | 12 |
| 8. | 0.75 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 9. | 2.50 | R | 12 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 4 | 0 | 12 |
| 10. | 2.50 | R | 32 | R | S | R | S | S | S | R | S | S | S | S | S | S | S | S | 4 | 0 | 12 |
| 11 | 1.00 | R | 48 | R | S | S | S | S | S | R | S | S | S | S | S | S | S | S | 3 | 0 | 13 |
| No. | MIC of geranium essential oil [µL/mL] | Susceptibility to antibiotics | Total | ||||||||||||||||||
| FOX MIC [µg/mL] | P | CIP | CN | E | DA | QD | TE | TGC | C | FD | LZD | RA | VA | DPC | SXT | R | I | S | |||
| 1. | 0.25 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 2. | 0.25 | S | 3 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 3 | 0 | 13 |
| 3. | 0.25 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 4. | 0.25 | R | 64 | R | R | S | R | R | S | S | S | S | S | S | S | S | S | S | 5 | 0 | 11 |
| 5. | 1.00 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 6. | 0.75 | S | 2 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 7. | 2.25 | S | 3 | S | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 0 | 0 | 16 |
| 8. | 2.00 | S | 3 | S | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 0 | 0 | 16 |
| 9. | 0.75 | S | 3 | S | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 0 | 0 | 16 |
| 10. | 1.00 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 11. | 1.25 | S | 3 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 1 | 0 | 15 |
| 12. | 1.50 | S | 2 | R | S | S | R | R | S | S | S | S | S | S | S | S | S | S | 3 | 0 | 13 |
| 13. | 2.50 | R | 16 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
| 14. | 1.00 | R | 32 | R | S | S | S | S | S | S | S | S | S | S | S | S | S | S | 2 | 0 | 14 |
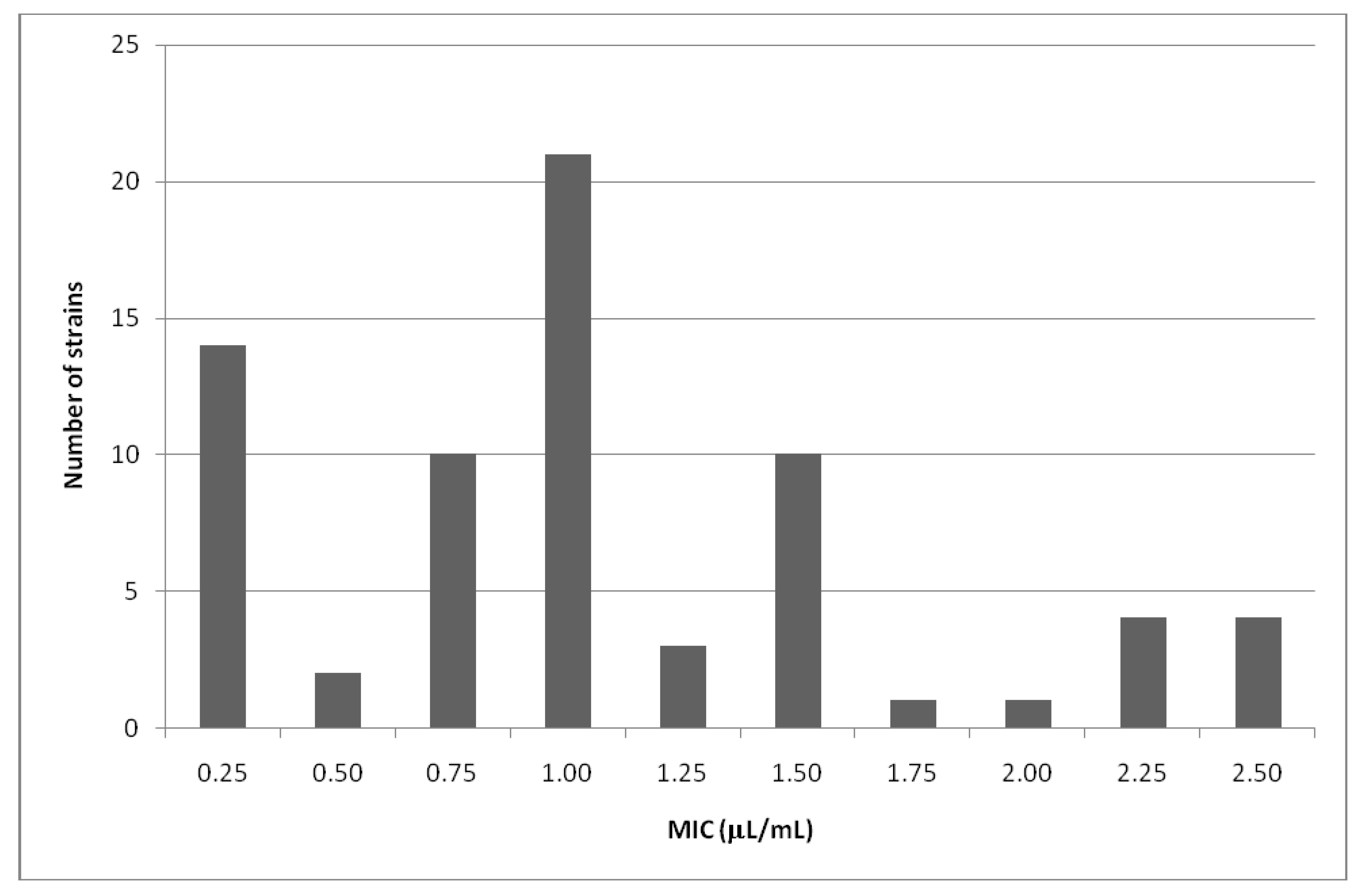
2.3. Susceptibility of the Clinical S. aureus Strains to the Geranium Oil

| Number of strains | MIC of geranium oil [µL/mL] | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0.25 | 0.50 | 0.75 | 1.00 | 1.25 | 1.50 | 1.75 | 2.00 | 2.25 | 2.50 | |
| MRSA | 4 | 2 | 3 | 10 | 0 | 6 | 1 | 0 | 1 | 4 |
| MSSA | 10 | 0 | 7 | 11 | 3 | 4 | 0 | 1 | 3 | 0 |
| Total | 14 | 2 | 10 | 21 | 3 | 10 | 1 | 1 | 4 | 4 |
| Number of strains with different MLSB mechanisms | MIC of geranium oil [µL/mL] | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0.25 | 0.50 | 0.75 | 1.00 | 1.25 | 1.50 | 1.75 | 2.00 | 2.25 | 2.50 | |
| Inducible MLSB | 3 | 1 | 3 | 5 | 0 | 1 | 1 | 0 | 0 | 0 |
| Constitutive MLSB | 1 | 0 | 0 | 6 | 0 | 2 | 0 | 0 | 0 | 2 |
| Constitutive and inducible MLSB | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Total | 4 | 1 | 3 | 11 | 0 | 4 | 1 | 0 | 0 | 2 |
3. Discussion
4. Experimental
4.1. Essential Oil Analysis
4.2. Antibacterial Activity of Essential Oil
4.3. Antibiotic Susceptibility of the Clinical S. aureus Strains
5. Conclusions
- 1. Geranium oil obtained from Pelargonium graveolens Ait. was active at concentrations of 0.25–2.50 μL/mL against multidrug resistant staphylococci of different origin.
- 2. No correlation was found between MICs values for geranium oil inhibiting the growth of S. aureus strains and MICs values for cefoxitin.
- 3. The growth of most MLSB-positive S. aureus strains was inhibited in lower MICs values of the tested oil.
Acknowledgements
References
- DeLeo, F.R.; Otto, M.; Kreiswirth, B.N.; Chambers, H.N. Community-associated methicillin-resistant Staphylococcus aureus. Lancet 2010, 375, 1557–1568. [Google Scholar] [CrossRef]
- Rafee, Y.; Abdel-Haq, N.; Asmar, B.; Salimnia, T.; Pharm, C.V.; Rybak, P.M.J.; Amjad, M. Increased prevalence of methicillin-resistant Staphylococcus aureus nasal colonization in household contacts of children with community acquired disease. BMC Infect. Dis. 2012. [Google Scholar]
- Wang, J.T.; Liao, C.H.; Fang, C.T.; Chie, W.C.; Lai, M.S.; Lauderdale, T.L.; Chang, S.C. Incidence of and risk factors for community-associated methicillin-resistant Staphylococcus aureus acquired infection or colonization in intensive-care-unit patients. J. Clin. Microbiol. 2010, 48, 4439–4444. [Google Scholar]
- Bigos, M.; Denys, A. The MRSA hospital infections. Int. Rev. Allergol. Clin. Immunol. 2008, 14, 101–109. [Google Scholar]
- Boers, S.A.; van Ess, I.; Euser, S.M.; Jansen, R.; Tempelman, F.R.; Diederen, B.M. An outbreak of a multiresistant methicillin-susceptible Staphylococcus aureus (MR-MSSA) strain in a burn centre: The importance of routine molecular typing. Burns 2011, 37, 808–813. [Google Scholar] [CrossRef]
- Loomba, P.S.; Taneja, J.; Mishra, B. Methicillin and vancomycin resistant S. aureus in hospitalized patients. J. Glob. Infect. Dis. 2010, 2, 275–283. [Google Scholar] [CrossRef]
- Warren, R. Staphylococcus aureus—A cross sectional study of prevalence and risk factors in one general practice. Aust. Fam. Physician 2012, 41, 325–328. [Google Scholar]
- Cheng, V.C.; Chan, J.F.; Lau, E.H.; Yam, W.C.; Ho, S.K.; Yau, M.C.; Tse, E.Y.; Wong, A.C.; Tai, J.W.; Fan, S.T.; et al. Studying the transmission dynamics of meticillin-resistant Staphylococcus aureus in Hong Kong using spa typing. J. Hosp. Infect. 2011, 79, 206–210. [Google Scholar] [CrossRef]
- Kim, S.P.; Shah, N.D.; Karnes, R.J.; Weight, C.J.; Frank, I.; Moriarty, J.P.; Han, L.C.; Borah, B.; Tollefson, M.K.; Boorjian, S.A. The implications of hospitalacquired adverse events on mortality, length of stay and costs for patients undergoing radical cystectomy for bladder cancer. J. Urol. 2012, 187, 2011–2017. [Google Scholar]
- Edris, A.E. Pharmaceutical and therapeutic potentials of essential oils and their individual volatile constituents: A review. Phytother. Res. 2007, 21, 308–323. [Google Scholar] [CrossRef]
- Bakkali, F.; Averbeck, S.; Averbeck, D.; Idaomar, M. Biological effect of essential oils—A review. Food Chem. Toxicol. 2008, 46, 446–475. [Google Scholar] [CrossRef]
- Silva, N.C.C.; Fernandes Júnior, A. Biological properties of medicinal plants: A review of their antimicrobial activity. J. Venom. Anim. Toxins Incl. Trop. Dis. 2010, 16, 402–413. [Google Scholar] [CrossRef]
- Reichling, J.; Schnitzler, P.; Suschke, U.; Saller, R. Essential oils of aromatic plants with antibacterial, antifungal, antiviral and cytotoxic properties—An oview. Forsch. Komplementment. 2009, 16, 79–90. [Google Scholar]
- Lis-Balchin, M. Geranium. In Hand Book of Herbs and Species; Peter, K.V., Ed.; Woodhead Publishing Limited: London, UK, 2004. [Google Scholar]
- Verma, R.K.; Laiq-ur-Rahman; Verma, R.S.; Kalra, A.; Kukreja, A.K.; Bisht, A.S.; Chauhan, A.; Khanuja, S.P.S. Assessing N-use efficiency, planting time and economics of fertilizer N in rose-scented geranium (Pelargonium graveolens L’ Herit) in Western Himalayan Region of India. Afr. J. Agric. Res. 2011, 6, 553–559. [Google Scholar]
- Shawl, A.S.; Kumar, T.; Chishi, N.; Shabir, S. Cultivation of rose scented Geranium (Pelargonium sp.) as a cash crop in Kasmir Valley. Asian J. Plant Sci. 2006, 5, 673–675. [Google Scholar] [CrossRef]
- Rosato, A.; Vitali, C.; De Laurentiis, N.; Armenise, D.; Antonietta Milillo, M. Antibacterial effect of some essential oils administered alone or in combination with Norfloxacin. Phytomedicine 2007, 14, 727–732. [Google Scholar]
- Ramirez, P.; Fernández-Barat, L.; Torres, A. New therapy options for MRSA with respiratory infection/pneumonia. Curr. Opin. Infect. Dis. 2012, 25, 159–165. [Google Scholar] [CrossRef]
- Fernandez, J.; Abbanat, D.; Shang, W.; He, W.; Amsler, K.; Hastings, J.; Queenan, A.M.; Melton, J.L.; Barron, A.M.; Flamm, R.K.; et al. Synergistic activity of ceftobiprole and vancomycin in a rat model of infective endocarditis caused by methicillin-resistant and glycopeptide-intermediate Staphylococcus aureus. Antimicrob. Agents Chemother. 2012, 56, 1476–1484. [Google Scholar]
- Vilhena, C.; Bettencourt, A. Daptomycin: A review of properties, clinical use, drug delivery and resistance. Mini-Rev. Med. Chem. 2012, 12, 202–209. [Google Scholar]
- Lis-Balchin, M.; Deans, S.G.; Hart, S. Bioactive Geranium oils from different commercial sources. J. Essent. Oil Res. 2007, 8, 281–290. [Google Scholar] [CrossRef]
- Fabio, A.; Cermelli, C.; Fabio, G.; Nicoletti, P.; Quaglio, P. Screening of the antibacterial effects of a variety of essential oils on microorganisms responsible for respiratory infections. Phytother. Res. 2007, 21, 374–377. [Google Scholar] [CrossRef]
- Chao, S.; Young, G.; Oberg, C.; Nakaoka, K. Inhibition of methicillin-resistant Staphylococcus aureus (MRSA) by essential oils. Flavour Fragr. J. 2008, 23, 444–449. [Google Scholar]
- Prabuseenivasan, S.; Jayakumar, M.; Ignacimuthu, S. In vitro antibacterial activity of some plant essential oils. BMC Complement. Altern. Med. 2006, 6. [Google Scholar]
- Edwards-Jones, V.; Buck, R.; Shawcross, S.G.; Dawson, M.M.; Dunn, K. The effect of essential oils on methicillin-resistant Staphylococcus aureus using a dressing model. Burns 2004, 30, 772–777. [Google Scholar] [CrossRef]
- Malik, T.; Singh, P. Antibacterial effects of essentials oils against uropathogens with varying sensitivity to antibiotics. Asian J. Biol. Sci. 2010, 3, 92–98. [Google Scholar] [CrossRef]
- Dorian, A.L.; Morden, W.E.; Dunn, K.; Edwards-Jones, V. Vapour-phase activities of essential oils against antibiotic sensitive and resistant bacteria including MRSA. Lett. Appl. Mcrobiol. 2009, 48, 387–392. [Google Scholar]
- Bearden, D.T.; Allen, G.P.; Christensen, J.M. Comparative in vitro activities of topical wound care products against community-associated methicillin-resistant Staphylococcus aureus. J. Antimicrob. Chemother. 2008, 62, 769–772. [Google Scholar] [CrossRef]
- Karpanen, T.J.; Worthington, T.; Hendry, E.R.; Conway, B.R.; Lambert, P.A. Antimicrobial efficacy of chlorhexidine digluconate alone and in combination with eucalyptus oil, tea tree oil and thymol against planktonic and biofilm cultures of Staphylococcus epidermidis. J. Antimicrob. Chemother. 2008, 62, 1031–1036. [Google Scholar] [CrossRef]
- Vercesi, A.E.; Kowaltowski, A.J.; Grijalba, M.T.; Meinicke, A.R.; Castilho, R.F. The role of the reactive oxygen species in mitochondrial permeability transition. Biosci. Rep. 1997, 17, 43–52. [Google Scholar] [CrossRef]
- Schmitt, S.; Schaefer, U.F.; Doebler, L.; Reichling, J. Cooperative interaction of monoterpenes and phenylpropanoids on the in vitro human skin permeation of complex composed essential oils. Planta Med. 2009, 75, 1381–1385. [Google Scholar] [CrossRef]
- Ohkawara, S.; Tanaka-Kagawa, T.; Furukawa, Y.; Nishimura, T.; Jinno, H. Activation of the human transient receptor potential vanilloid subtype 1 by essential oils. Biol. Pharm. Bull. 2010, 33, 1434–1437. [Google Scholar] [CrossRef]
- Sienkiewicz, M.; Kowalczyk, E.; Wasiela, M. Recent patents regarding essential oils and the significance of their constituents in human health and treatment. Recent Pat. Anti-Infect. Drug Discov. 2012, 7, 133–140. [Google Scholar] [CrossRef]
- Adams, R.P. Identification of Essential Oil Components by Gas Chromatography/Mass Spectroscopy, 4th ed; Allured Publishing Corporation: Carol Stream, IL, USA, 2007. [Google Scholar]
- Joulain, D.; König, W.A. The Atlas of Spectral Data of Sesquiterpene Hydrocarbons; E.B.-Verlag: Hamburg, Germany, 1998. [Google Scholar]
- Kalemba, D.; Kunicka, A. Antibacterial and antifungal properties of essential oils. Curr. Med. Chem. 2003, 10, 813–829. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). Breakpoint Tables for Interpretation of MICs and Zone Diameters, version 2.0. Available online: http://www.eucast.org (accessed on 16 August 2012). valid from 1 January 2012.
- Sample Availability: Samples of the geranium oil (POLLENA-AROMA Poland) are available from the authors.
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Bigos, M.; Wasiela, M.; Kalemba, D.; Sienkiewicz, M. Antimicrobial Activity of Geranium Oil against Clinical Strains of Staphylococcus aureus. Molecules 2012, 17, 10276-10291. https://doi.org/10.3390/molecules170910276
Bigos M, Wasiela M, Kalemba D, Sienkiewicz M. Antimicrobial Activity of Geranium Oil against Clinical Strains of Staphylococcus aureus. Molecules. 2012; 17(9):10276-10291. https://doi.org/10.3390/molecules170910276
Chicago/Turabian StyleBigos, Monika, Małgorzata Wasiela, Danuta Kalemba, and Monika Sienkiewicz. 2012. "Antimicrobial Activity of Geranium Oil against Clinical Strains of Staphylococcus aureus" Molecules 17, no. 9: 10276-10291. https://doi.org/10.3390/molecules170910276