Emodin Protects against Diabetic Cardiomyopathy by Regulating the AKT/GSK-3β Signaling Pathway in the Rat Model

Abstract
:1. Introduction
2. Results and Discussion
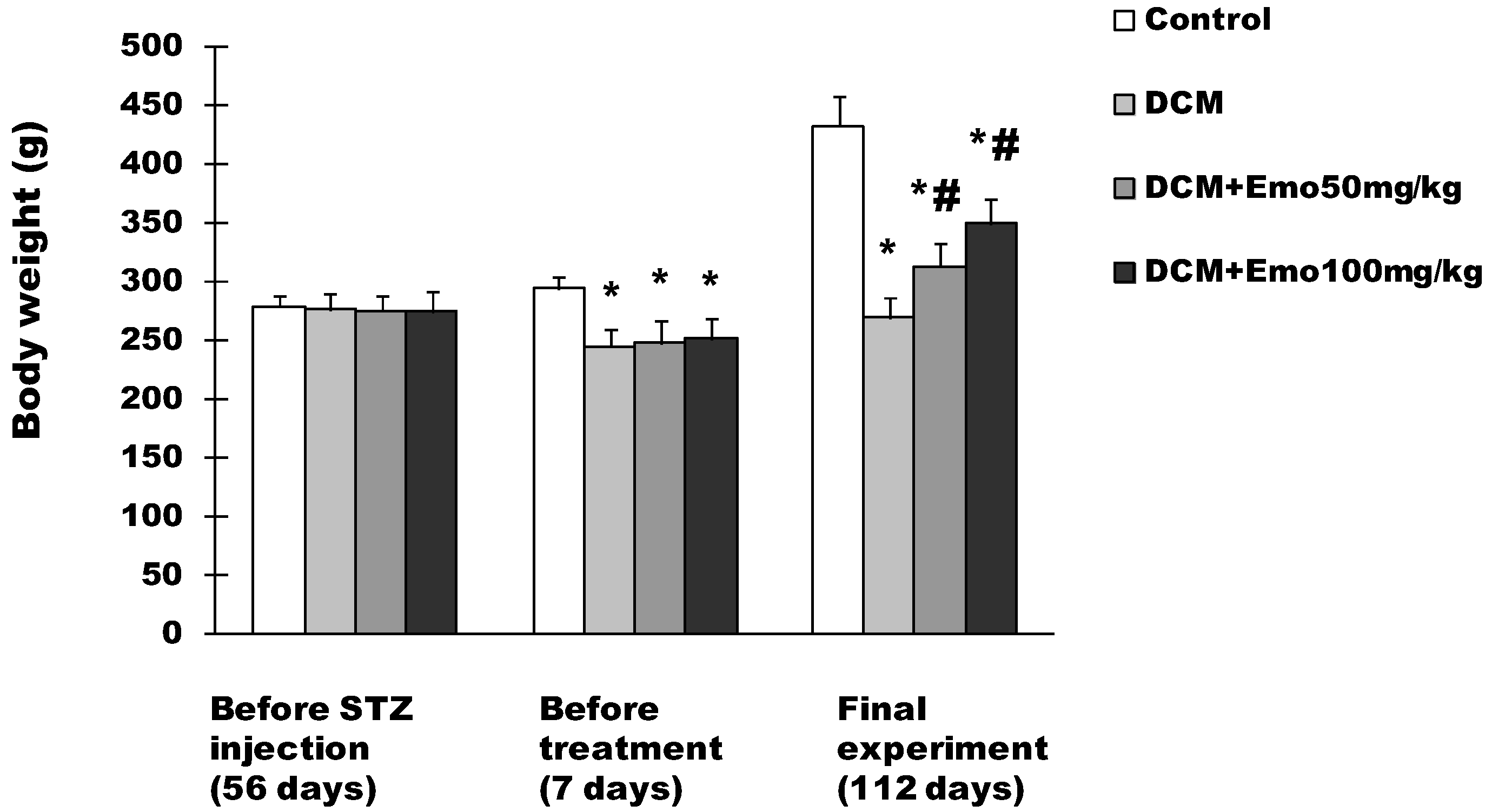
2.1. Effect of Emo on BW in STZ-Induced Diabetic Cardiomyopathy

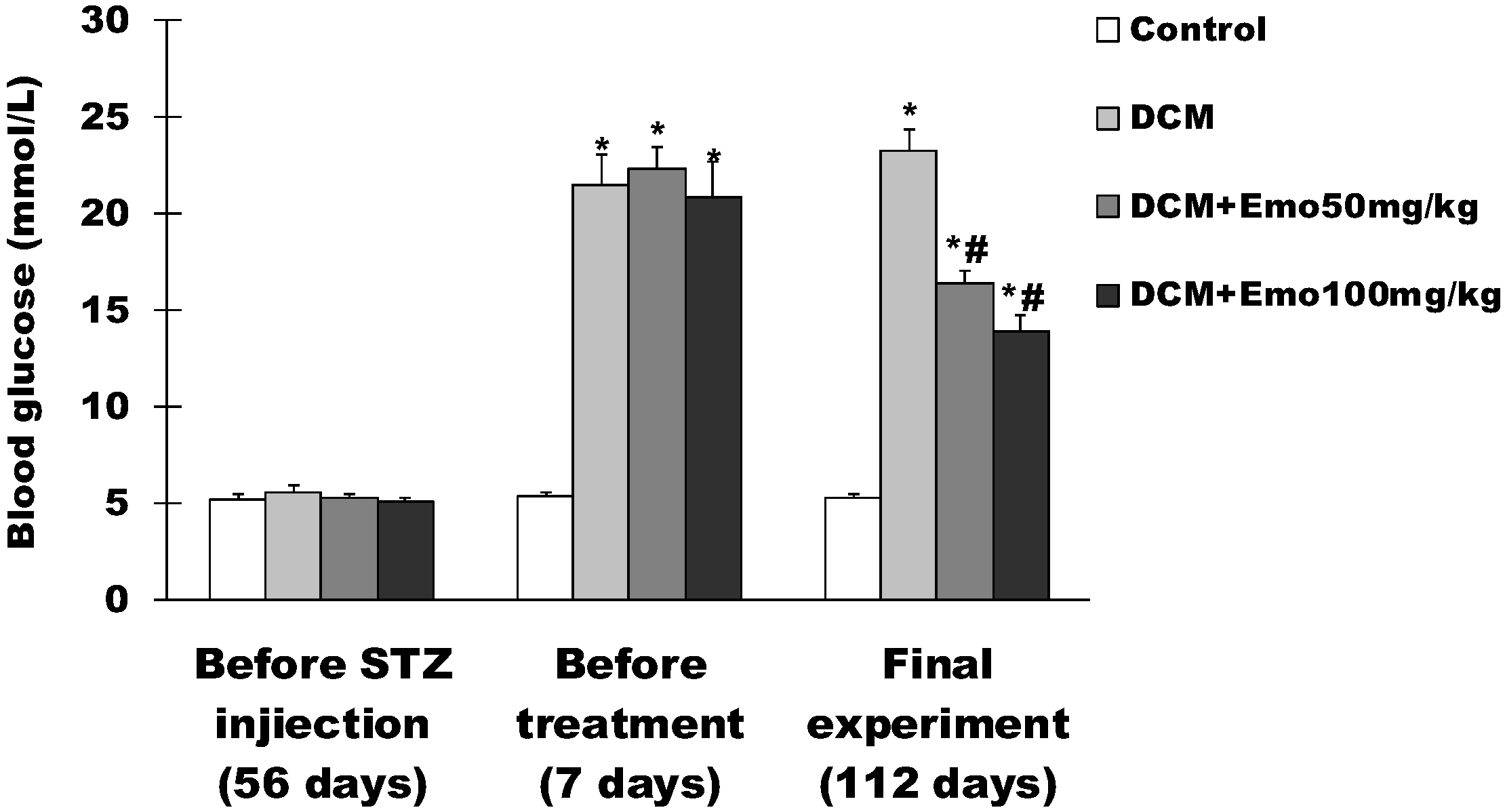
2.2. Effect of Emo on Blood Glucose in STZ-Induced Diabetic Cardiomyopathy
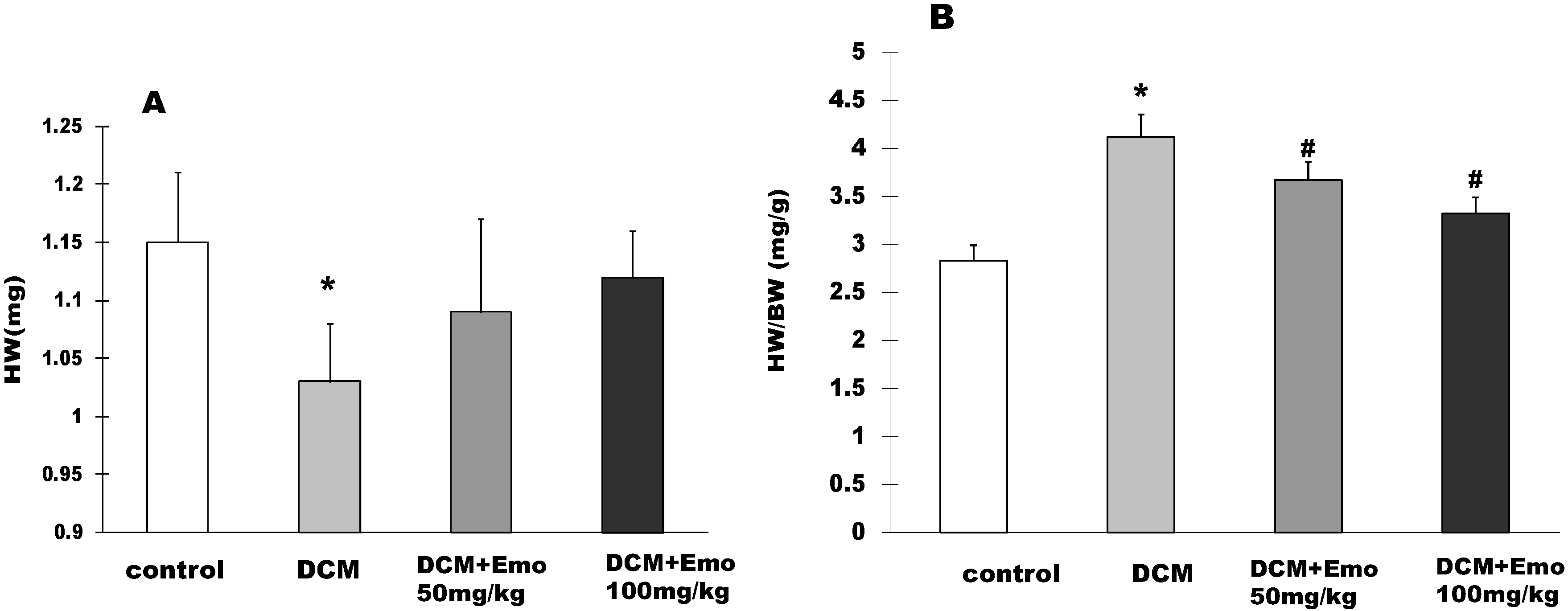
2.3. Effects of Emo on HW and HW/BW STZ-Induced Diabetic Cardiomyopathy


2.4. Emo Alleviated Left Ventricular Dysfunction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | HR (bpm) | LWPWT (mm) | IVSD (mm) | LVEDD (mm) | LVESD (mm) | FS (%) | EF (%) |
|---|---|---|---|---|---|---|---|
| Control | 384 ± 15 | 1.49 ± 0.09 | 1.34 ± 0.07 | 2.83 ± 0.21 | 1.58 ± 0.11 | 44.2 ± 2.7 | 82.6 ± 2.4 |
| DCM | 311 ± 11 * | 1.74 ± 0.11 * | 1.81 ± 0.14 * | 3.48 ± 0.31 * | 2.31 ± 0.28 * | 33.6 ± 3.2 * | 70.8 ± 3.4 * |
| DCM+Emo 50 mg/kg | 332 ± 13 # | 1.56 ± 0.13 | 1.55 ± 0.09 # | 3.11 ± 0.16 | 1.84 ± 0.19 # | 40.8 ± 2.9 | 79.3 ± 2.8 |
| DCM+Emo100 mg/kg | 358 ± 14 # | 1.63 ± 0.15 # | 1.49 ± 0.11 # | 2.89 ± 0.23 # | 1.69 ± 0.16 # | 41.5 ± 2.8 # | 80 ± 2.6 # |
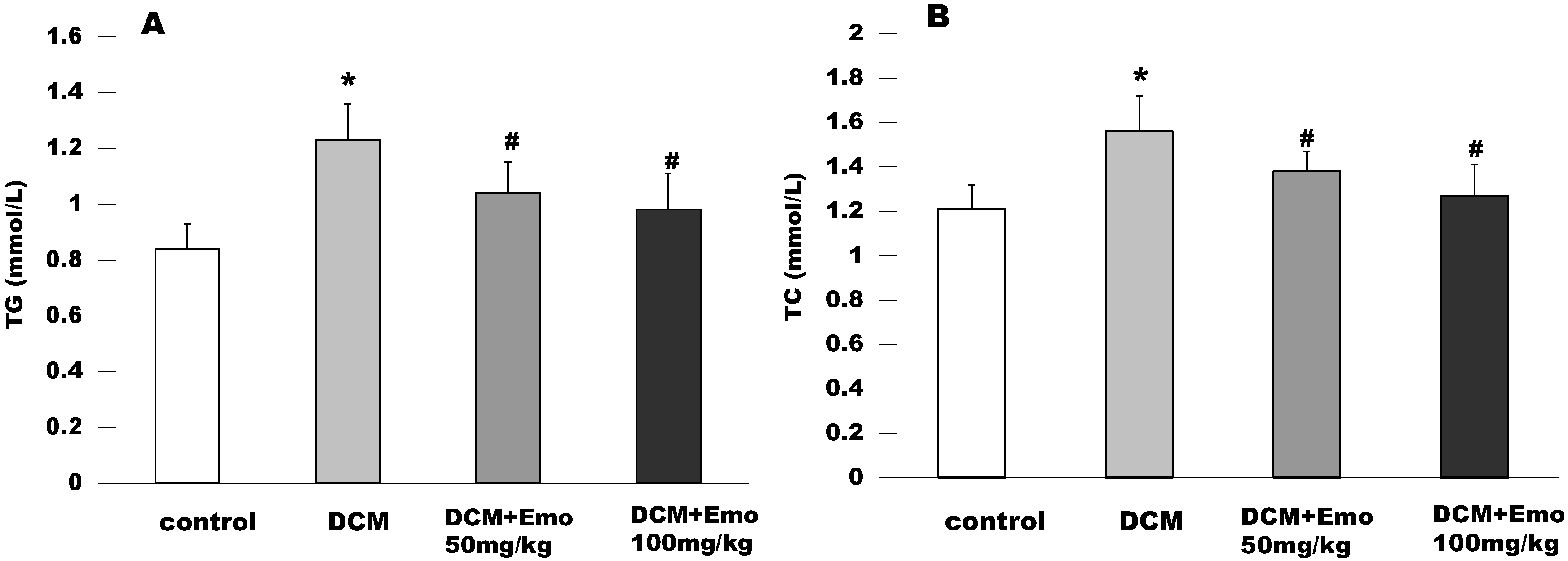
2.5. Effect of Emo on TG and TC in STZ-Induced Diabetic Cardiomyopathy

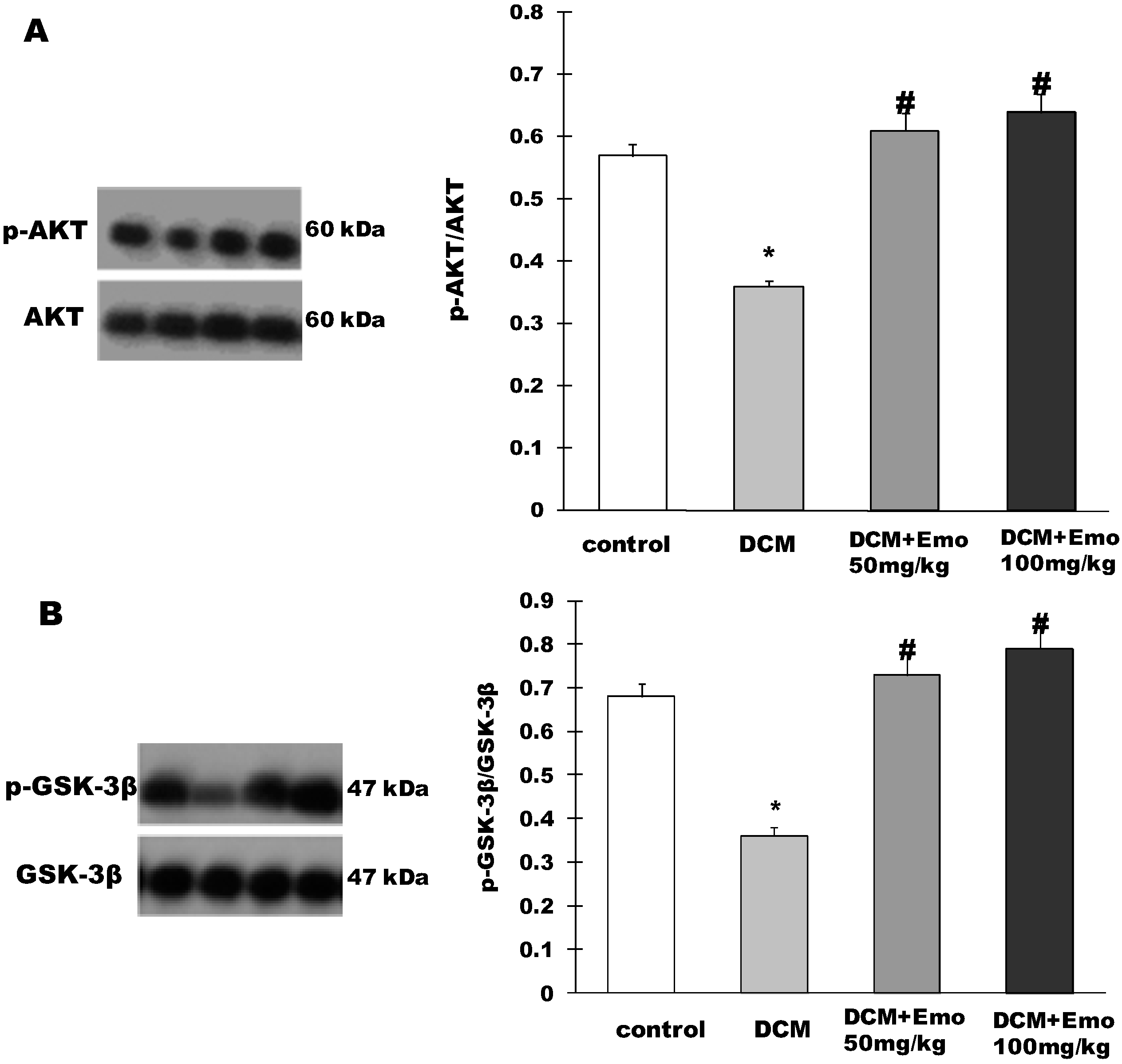
2.6. Effect of Emo on AKT/GSK-3β Signaling Pathway in STZ-Induced Diabetic Cardiomyopathy

2.7. Disscussion
3. Experimental Section
3.1. Reagents and Antibodies
3.2. Rat Model of Type 2 Diabetes
3.3. Experimental Design
3.4. Blood Analyses
3.5. Heart Weight and Body Weight
3.6. Echocardiography
3.7. Western Blotting
3.8. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Matthews, D.R.; Pramming, S. Diabetes and the global burden of non-communicable disease. Lancet 2003, 362, 1763–1764. [Google Scholar]
- Kitabchi, A.E.; Umpierrez, G.E.; Miles, J.M.; Fisher, J.N. Hyperglycemic crises in adult patients with diabetes. Diabetes Care 2009, 32, 1335–1343. [Google Scholar]
- Alberti, K.G.; Zimmet, P. Global burden of disease—Where does diabetes mellitus fit in? Nat. Rev. Endocrinol. 2013, 9, 258–260. [Google Scholar]
- King, H.; Aubert, R.E.; Herman, W.H. Global burden of diabetes, 1995–2025: Prevalence, numerical estimates, and projections. Diabetes Care 1998, 21, 1414–1431. [Google Scholar]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics—2012 update: A report from the American Heart Association. Circulation 2012, 125, e2–e220. [Google Scholar]
- Witteles, R.M.; Fowler, M.B. Insulin-resistant cardiomyopathy clinical evidence, mechanisms, and treatment options. J. Am. Coll. Cardiol. 2008, 51, 93–102. [Google Scholar]
- Battiprolu, P.K.; Gillette, T.G.; Wang, Z.V.; Lavandero, S.; Hill, J.A. Diabetic Cardiomyopathy: Mechanisms and Therapeutic Targets. Drug Discov. Today: Dis. Mech. 2010, 7, e135–e143. [Google Scholar]
- Falcao-Pires, I.; Leite-Moreira, A.F. Diabetic cardiomyopathy: Understanding the molecular and cellular basis to progress in diagnosis and treatment. Heart Fail. Rev. 2012, 17, 325–344. [Google Scholar]
- Mano, Y.; Anzai, T.; Kaneko, H.; Nagatomo, Y.; Nagai, T.; Anzai, A.; Maekawa, Y.; Takahashi, T.; Meguro, T.; Yoshikawa, T.; et al. Overexpression of human C-reactive protein exacerbates left ventricular remodeling in diabetic cardiomyopathy. Jpn. Circ. J. 2010, 75, 1717–1727. [Google Scholar]
- Wang, J.; Wang, H.; Hao, P.; Xue, L.; Wei, S.; Zhang, Y.; Chen, Y. Inhibition of aldehyde dehydrogenase 2 by oxidative stress is associated with cardiac dysfunction in diabetic rats. Mol. Med. 2011, 17, 172–179. [Google Scholar]
- Zhou, H.; Li, Y.J.; Wang, M.; Zhang, L.H.; Guo, B.Y.; Zhao, Z.S.; Meng, F.L.; Deng, Y.G.; Wang, R.Y. Involvement of RhoA/ROCK in myocardial fibrosis in a rat model of type 2 diabetes. Acta Pharmacol. Sin. 2011, 32, 999–1008. [Google Scholar]
- Thandavarayan, R.A.; Watanabe, K.; Ma, M.; Gurusamy, N.; Veeraveedu, P.T.; Konishi, T.; Zhang, S.; Muslin, A.J.; Kodama, M.; Aizawa, Y. Dominant-negative p38alpha mitogen-activated protein kinase prevents cardiac apoptosis and remodeling after streptozotocin-induced diabetes mellitus. Am. J. Physiol.-Heart C 2009, 297, H911–H919. [Google Scholar]
- Duncan, J.G. Mitochondrial dysfunction in diabetic cardiomyopathy. BBA-Mol. Cell Res. 2011, 1813, 1351–1359. [Google Scholar]
- Chun-Guang, W.; Jun-Qing, Y.; Bei-Zhong, L.; Dan-Ting, J.; Chong, W.; Liang, Z.; Dan, Z.; Yan, W. Anti-tumor activity of emodin against human chronic myelocytic leukemia K562 cell lines in vitro and in vivo. Eur. J. Pharmacol. 2010, 627, 33–41. [Google Scholar]
- Alisi, A.; Pastore, A.; Ceccarelli, S.; Panera, N.; Gnani, D.; Bruscalupi, G.; Massimi, M.; Tozzi, G.; Piemonte, F.; Nobili, V. Emodin prevents intrahepatic fat accumulation, inflammation and redox status imbalance during diet-induced hepatosteatosis in rats. Int. J. Mol. Sci. 2010, 13, 2276–2289. [Google Scholar]
- Lin, S.Z.; Wei, W.T.; Chen, H.; Chen, K.J.; Tong, H.F.; Wang, Z.H.; Ni, Z.L.; Liu, H.B.; Guo, H.C.; Liu, D.L. Antitumor activity of emodin against pancreatic cancer depends on its dual role: Promotion of apoptosis and suppression of angiogenesis. PLoS One 2012, 7, e42146. [Google Scholar]
- Zhang, X.; Zhang, R.; Lv, P.; Yang, J.; Deng, Y.; Xu, J.; Zhu, R.; Zhang, D.; Yang, Y. Emodin up-regulates glucose metabolism, decreases lipolysis, and attenuates inflammation in vitro. J. Diabetes 2014. [Google Scholar] [CrossRef]
- Yang, Z.; Zhou, E.; Wei, D.; Li, D.; Wei, Z.; Zhang, W.; Zhang, X. Emodin inhibits LPS-induced inflammatory response by activating PPAR-gamma in mouse mammary epithelial cells. Int. Immunopharmacol. 2014, 21, 354–360. [Google Scholar]
- Shuangsuo, D.; Zhengguo, Z.; Yunru, C.; Xin, Z.; Baofeng, W.; Lichao, Y.; Yan’an, C. Inhibition of the replication of hepatitis B virus in vitro by emodin. Med. Sci. Monit. 2006, 12, 302–306. [Google Scholar]
- Feng, Y.; Huang, S.L.; Dou, W.; Zhang, S.; Chen, J.H.; Shen, Y.; Shen, J.H.; Leng, Y. Emodin, a natural product, selectively inhibits 11beta-hydroxysteroid dehydrogenase type 1 and ameliorates metabolic disorder in diet-induced obese mice. Br. J. Pharmacol. 2010, 161, 113–126. [Google Scholar]
- Wang, J.; Huang, H.; Liu, P.; Tang, F.; Qin, J.; Huang, W.; Chen, F.; Guo, F.; Liu, W.; Yang, B. Inhibition of phosphorylation of p38 MAPK involved in the protection of nephropathy by emodin in diabetic rats. Eur. J. Pharmacol. 2006, 553, 297–303. [Google Scholar]
- Xue, J.; Ding, W.; Liu, Y. Anti-diabetic effects of emodin involved in the activation of PPARgamma on high-fat diet-fed and low dose of streptozotocin-induced diabetic mice. Fitoterapia 2010, 81, 173–177. [Google Scholar]
- Gao, J.; Wang, F.; Wang, W.; Su, Z.; Guo, C.; Cao, S. Emodin suppresses hyperglycemia-induced proliferation and fibronectin expression in mesangial cells via inhibiting cFLIP. PLoS One 2014, 9, e93588. [Google Scholar]
- Lee, W.; Ku, S.K.; Lee, D.; Lee, T.; Bae, J.S. Emodin-6-O-beta-D--glucoside inhibits high-glucose-induced vascular inflammation. Inflammation 2014, 37, 306–313. [Google Scholar]
- Huang, F.J.; Hsuuw, Y.D.; Chan, W.H. Characterization of apoptosis induced by emodin and related regulatory mechanisms in human neuroblastoma cells. Int. J. Mol. Sci. 2014, 14, 20139–20156. [Google Scholar]
- Rubler, S.; Dlugash, J.; Yuceoglu, Y.Z.; Kumral, T.; Branwood, A.W.; Grishman, A. New type of cardiomyopathy associated with diabetic glomerulosclerosis. Am. J. Cardiol. 1972, 30, 595–602. [Google Scholar]
- Boudina, S.; Abel, E.D. Diabetic cardiomyopathy, causes and effects. Rev. Endocr. Metab. Disord. 2010, 11, 31–39. [Google Scholar]
- Bell, D.S. Diabetic cardiomyopathy. Diabetes Care 2003, 26, 2949–51. [Google Scholar]
- Cai, L. Diabetic cardiomyopathy and its prevention by metallothionein: Experimental evidence, possible mechanisms and clinical implications. Curr. Med. Chem. 2007, 14, 2193–2203. [Google Scholar]
- Voulgari, C.; Papadogiannis, D.; Tentolouris, N. Diabetic cardiomyopathy: From the pathophysiology of the cardiac myocytes to current diagnosis and management strategies. Vasc. Health Risk Manag. 2010, 6, 883–903. [Google Scholar]
- Fredersdorf, S.; Thumann, C.; Zimmermann, W.H.; Vetter, R.; Graf, T.; Luchner, A.; Riegger, G.A.; Schunkert, H.; Eschenhagen, T.; Weil, J. Increased myocardial SERCA expression in early type 2 diabetes mellitus is insulin dependent: In vivo and in vitro data. Cardiovasc. Diabetol. 2012, 11, 57. [Google Scholar]
- Aragno, M.; Mastrocola, R.; Ghe, C.; Arnoletti, E.; Bassino, E.; Alloatti, G.; Muccioli, G. Obestatin induced recovery of myocardial dysfunction in type 1 diabetic rats: Underlying mechanisms. Cardiovasc. Diabetol. 2012, 11, 129. [Google Scholar]
- Nunes, S.; Soares, E.; Fernandes, J.; Viana, S.; Carvalho, E.; Pereira, F.C.; Reis, F. Early cardiac changes in a rat model of prediabetes: Brain natriuretic peptide overexpression seems to be the best marker. Cardiovasc. Diabetol. 2013, 12, 44. [Google Scholar]
- Bugger, H.; Abel, E.D. Rodent models of diabetic cardiomyopathy. Dis. Model. Mech. 2009, 2, 454–466. [Google Scholar]
- Wang, P.; Lloyd, S.G.; Zeng, H.; Bonen, A.; Chatham, J.C. Impact of altered substrate utilization on cardiac function in isolated hearts from Zucker diabetic fatty rats. Am. J. Physiol. Heart Circ. Physiol. 2005, 288, 2102–2110. [Google Scholar]
- Chen, W.; Xia, Y.; Zhao, X.; Wang, H.; Yu, M.; Li, Y.; Ye, H.; Zhang, Y. The critical role of astragalus polysaccharides for the improvement of PPARalpha [correction of PPRAalpha]-mediated lipotoxicity in diabetic cardiomyopathy. PLoS One 2012, 7, e45541. [Google Scholar]
- Mihm, M.J.; Seifert, J.L.; Coyle, C.M.; Bauer, J.A. Diabetes related cardiomyopathy time dependent echocardiographic evaluation in an experimental rat model. Life Sci. 2001, 69, 527–542. [Google Scholar]
- Brownlee, M. The pathobiology of diabetic complications: A unifying mechanism. Diabetes 2005, 54, 1615–1625. [Google Scholar]
- Shrimali, D.; Shanmugam, M.K.; Kumar, A.P.; Zhang, J.; Tan, B.K.; Ahn, K.S.; Sethi, G. Targeted abrogation of diverse signal transduction cascades by emodin for the treatment of inflammatory disorders and cancer. Cancer Lett. 2013, 341, 139–149. [Google Scholar]
- National Toxicology Program. NTP toxicology and carcinogenesis studies of emodin (CAS NO. 518-82-1) feed studies in F344/N rats and B6C3F1 mice. Natl. Toxicol. Program. Tech. Rep. Ser. 2001, 493, 1–278. [Google Scholar]
- Wang, Y.; Feng, W.; Xue, W.; Tan, Y.; Hein, D.W.; Li, X.K.; Cai, L. Inactivation of GSK-3beta by metallothionein prevents diabetes-related changes in cardiac energy metabolism, inflammation, nitrosative damage, and remodeling. Diabetes 2009, 58, 1391–1402. [Google Scholar] [CrossRef]
- Katare, R.G.; Caporali, A.; Oikawa, A.; Meloni, M.; Emanueli, C.; Madeddu, P. Vitamin B1 analog benfotiamine prevents diabetes-induced diastolic dysfunction and heart failure through Akt/Pim-1-mediated survival pathway. Circ. Heart Fail. 2010, 3, 294–305. [Google Scholar] [CrossRef]
- Sun, D.; Shen, M.; Li, J.; Li, W.; Zhang, Y.; Zhao, L.; Zhang, Z.; Yuan, Y.; Wang, H.; Cao, F. Cardioprotective effects of tanshinone IIA pretreatment via kinin B2 receptor-Akt-GSK-3β dependent pathway in experimental diabetic cardiomyopathy. Cardiovasc. Diabetol. 2011, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Babcock, S.A.; Hu, N.; Maris, J.R.; Wang, H.; Ren, J. Mitochondrial aldehyde dehydrogenase (ALDH2) protects against streptozotocin-induced diabetic cardiomyopathy: Role of GSK3β and mitochondrial function. BMC Med. 2012, 10, 40. [Google Scholar] [CrossRef]
- Salloum, F.N.; Chau, V.Q.; Hoke, N.N.; Abbate, A.; Varma, A.; Ockaili, R.A.; Toldo, S.; Kukreja, R.C. Phosphodiesterase-5 inhibitor, tadalafil, protects against myocardial ischemia/reperfusion through protein-kinase g-dependent generation of hydrogen sulfide. Circulation 2009, 120, 31–36. [Google Scholar] [CrossRef]
- Lin, Y.C.; Leu, S.; Sun, C.K.; Yen, C.H.; Kao, Y.H.; Chang, L.T.; Tsai, T.H.; Chua, S.; Fu, M.; Ko, S.F.; et al. Early combined treatment with sildenafil and adipose-derived mesenchymal stem cells preserves heart function in rat dilated cardiomyopathy. J. Transl. Med. 2010, 8, 88. [Google Scholar] [CrossRef]
- Sample Availability: Samples of the compounds are available from the authors.
© 2014 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Wu, Z.; Chen, Q.; Ke, D.; Li, G.; Deng, W. Emodin Protects against Diabetic Cardiomyopathy by Regulating the AKT/GSK-3β Signaling Pathway in the Rat Model. Molecules 2014, 19, 14782-14793. https://doi.org/10.3390/molecules190914782
Wu Z, Chen Q, Ke D, Li G, Deng W. Emodin Protects against Diabetic Cardiomyopathy by Regulating the AKT/GSK-3β Signaling Pathway in the Rat Model. Molecules. 2014; 19(9):14782-14793. https://doi.org/10.3390/molecules190914782
Chicago/Turabian StyleWu, Zhiqin, Qingwei Chen, Dazhi Ke, Guiqiong Li, and Wei Deng. 2014. "Emodin Protects against Diabetic Cardiomyopathy by Regulating the AKT/GSK-3β Signaling Pathway in the Rat Model" Molecules 19, no. 9: 14782-14793. https://doi.org/10.3390/molecules190914782