
The Traditional Chinese Medicine DangguiBuxue Tang Sensitizes Colorectal Cancer Cells to Chemoradiotherapy

 ,
, 
Abstract
:1. Introduction
2. Results
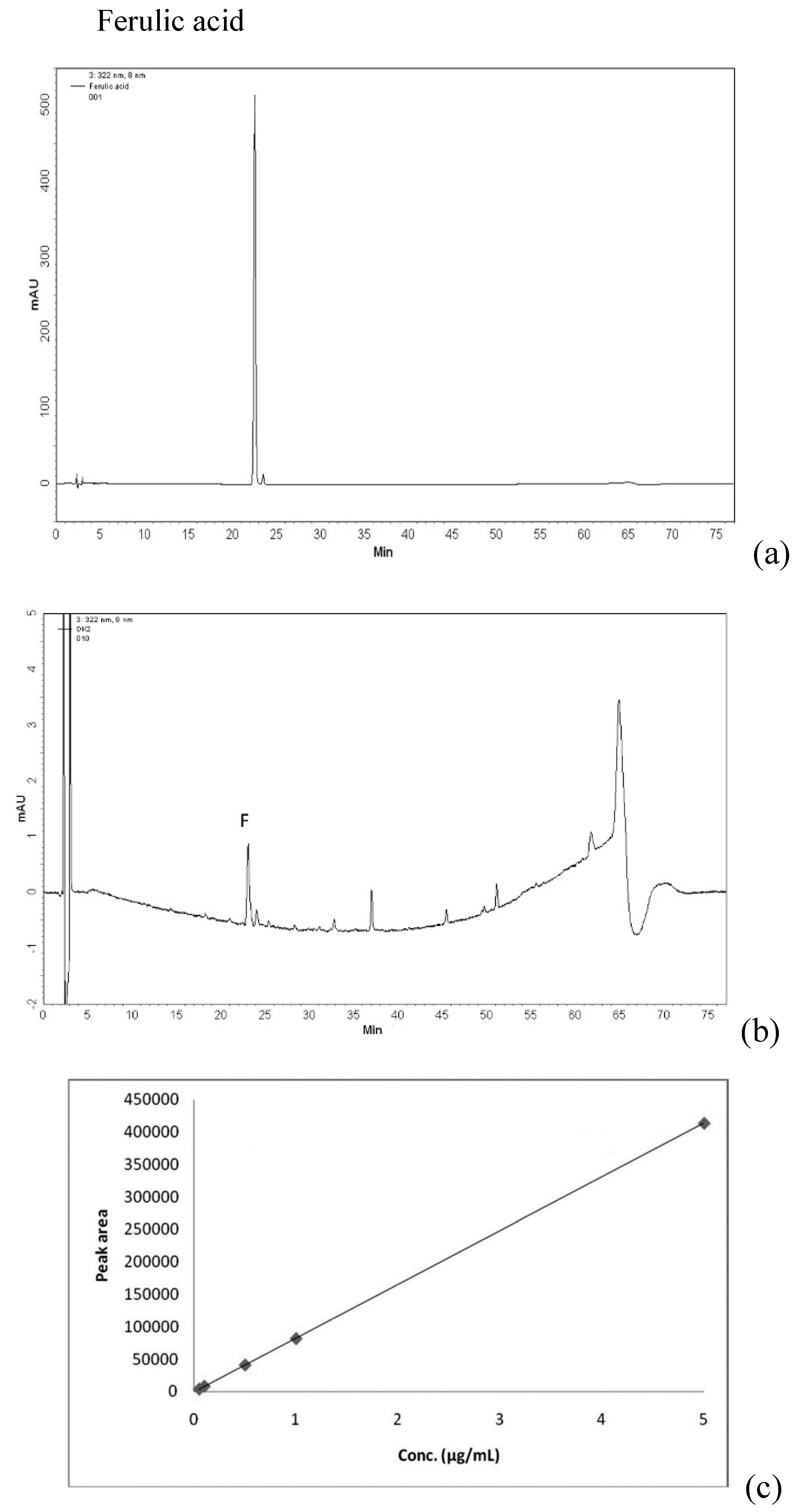
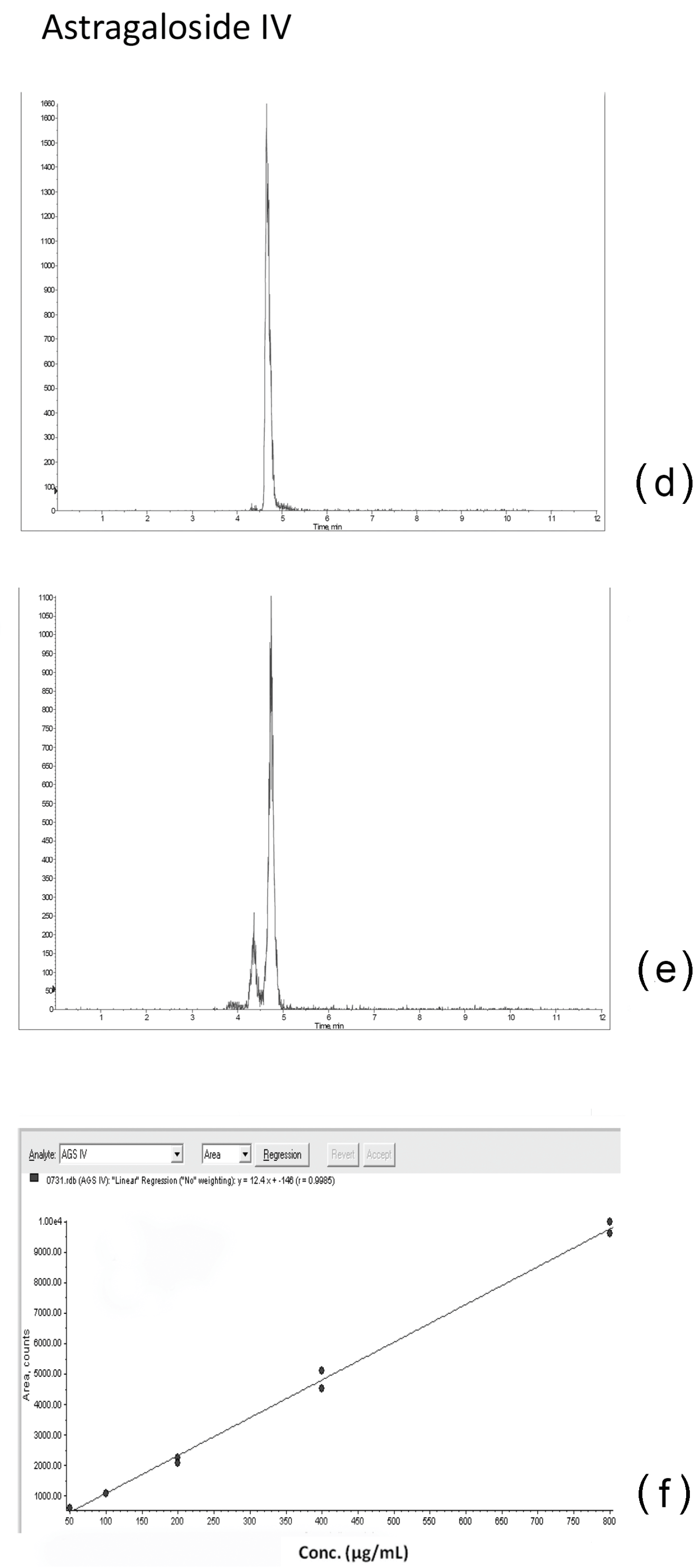
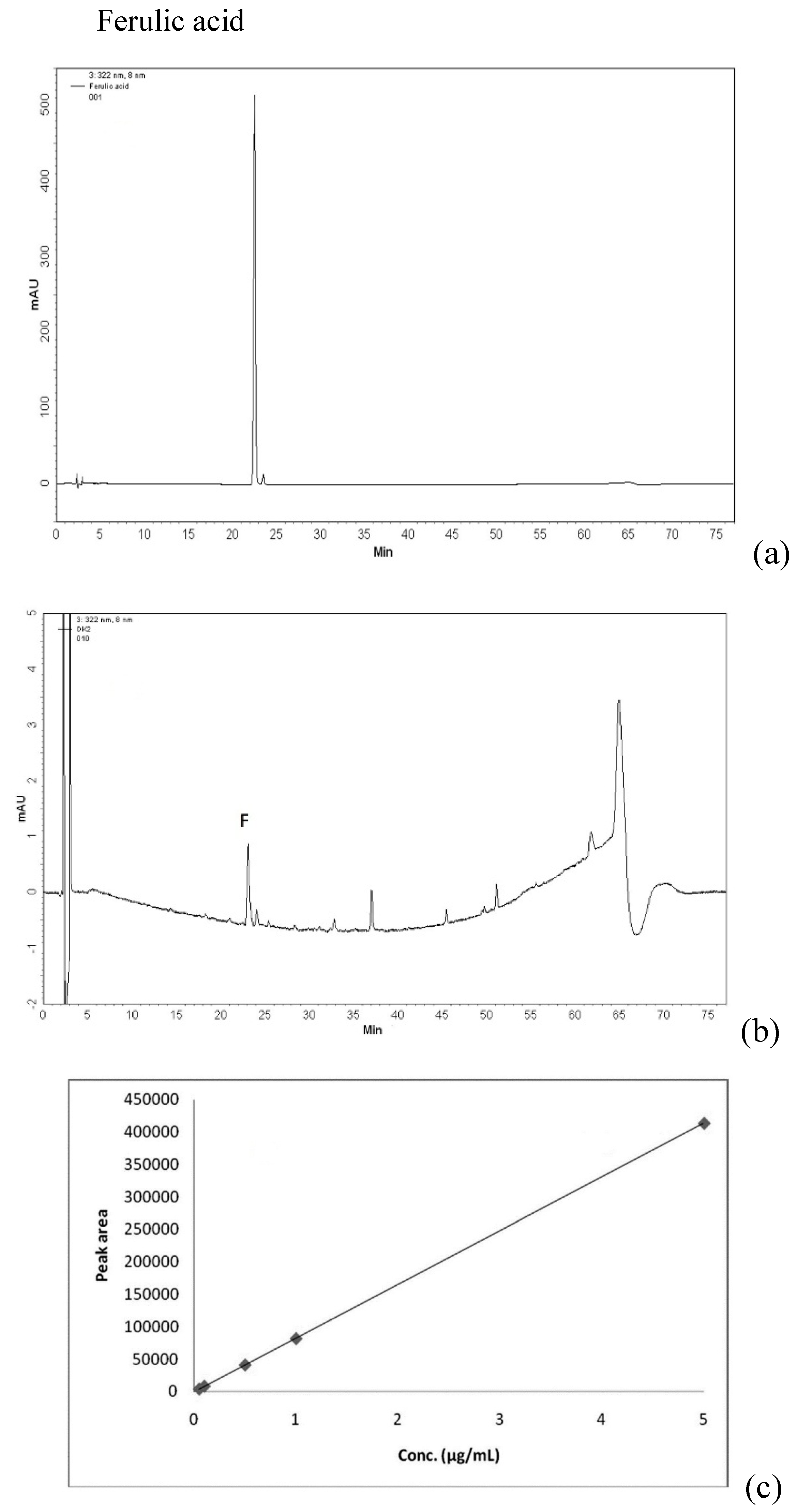
2.1. Qualitative and Quantitative Analysis of Ferulic Acid and Astragaloside IV in DBT
2.2. Osmolality of Culture Medium Containing DBT-PD
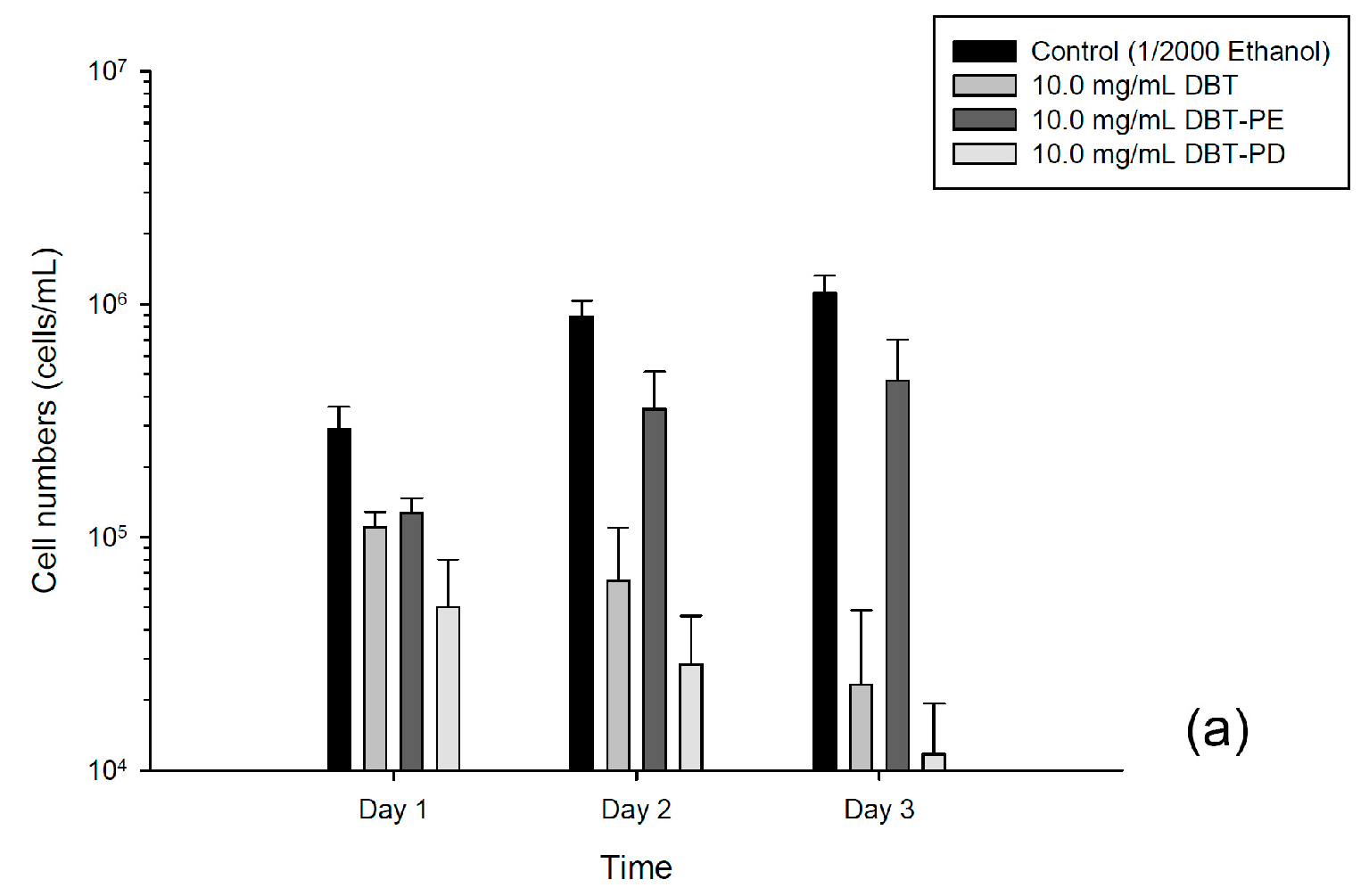
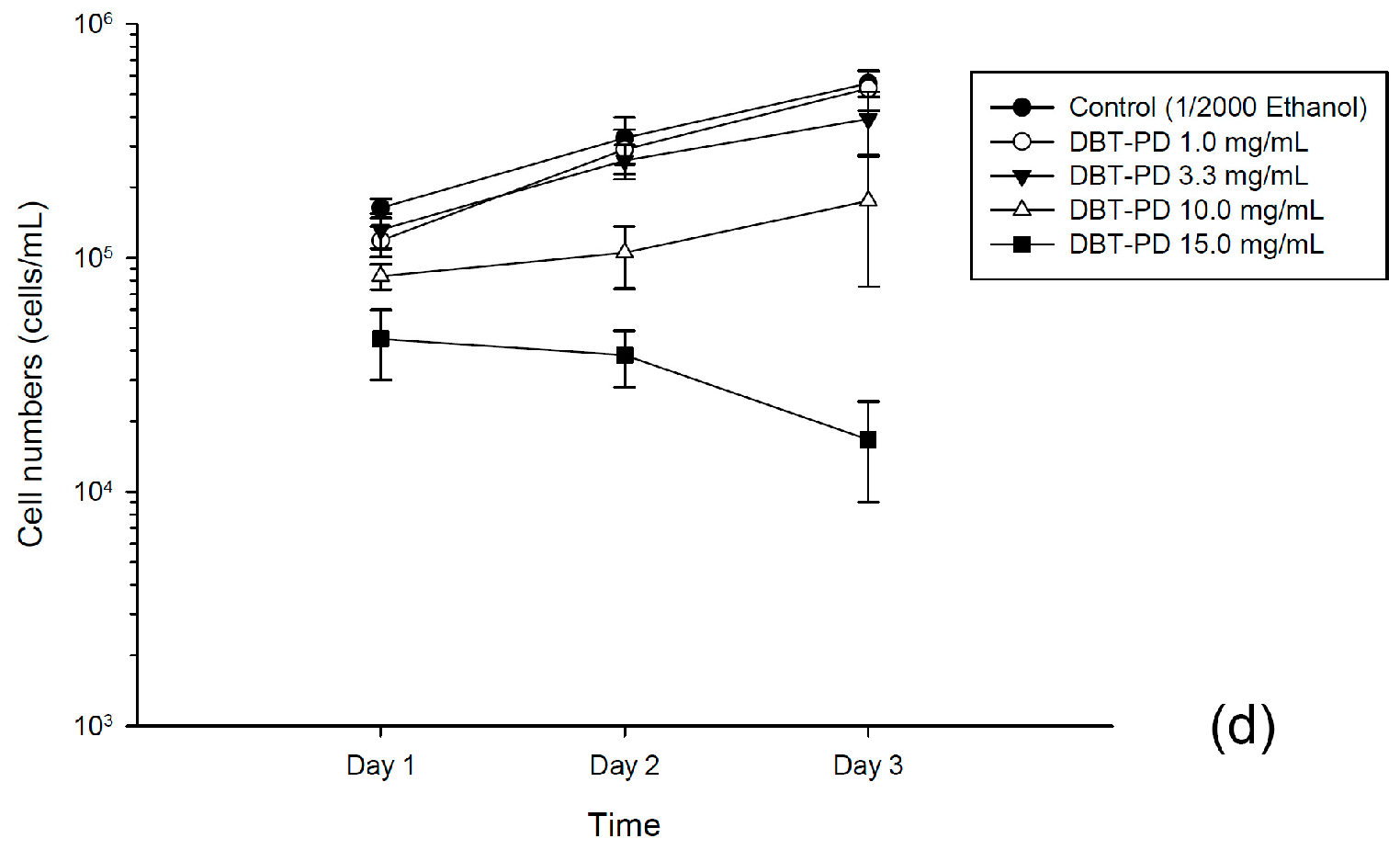
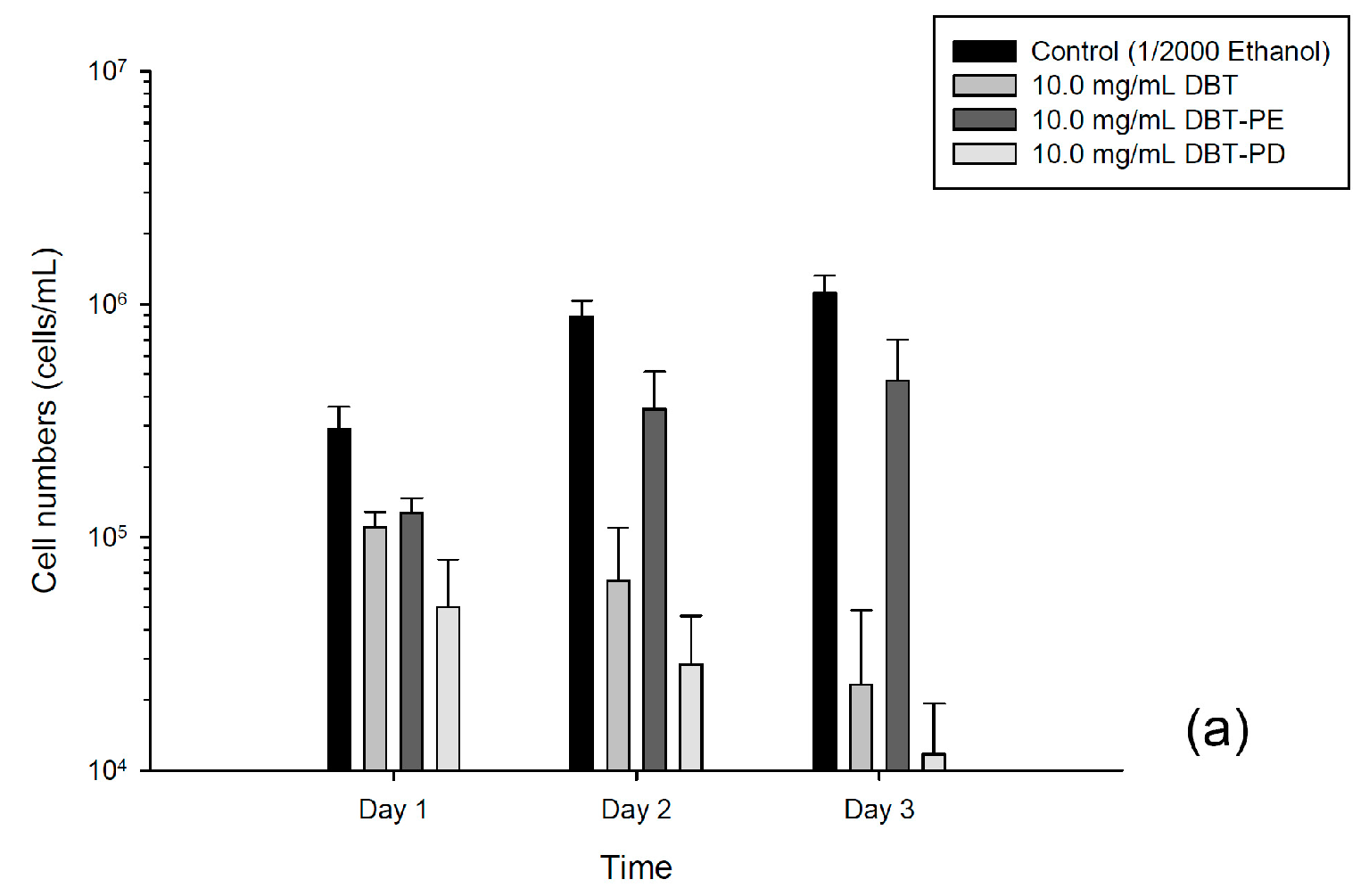
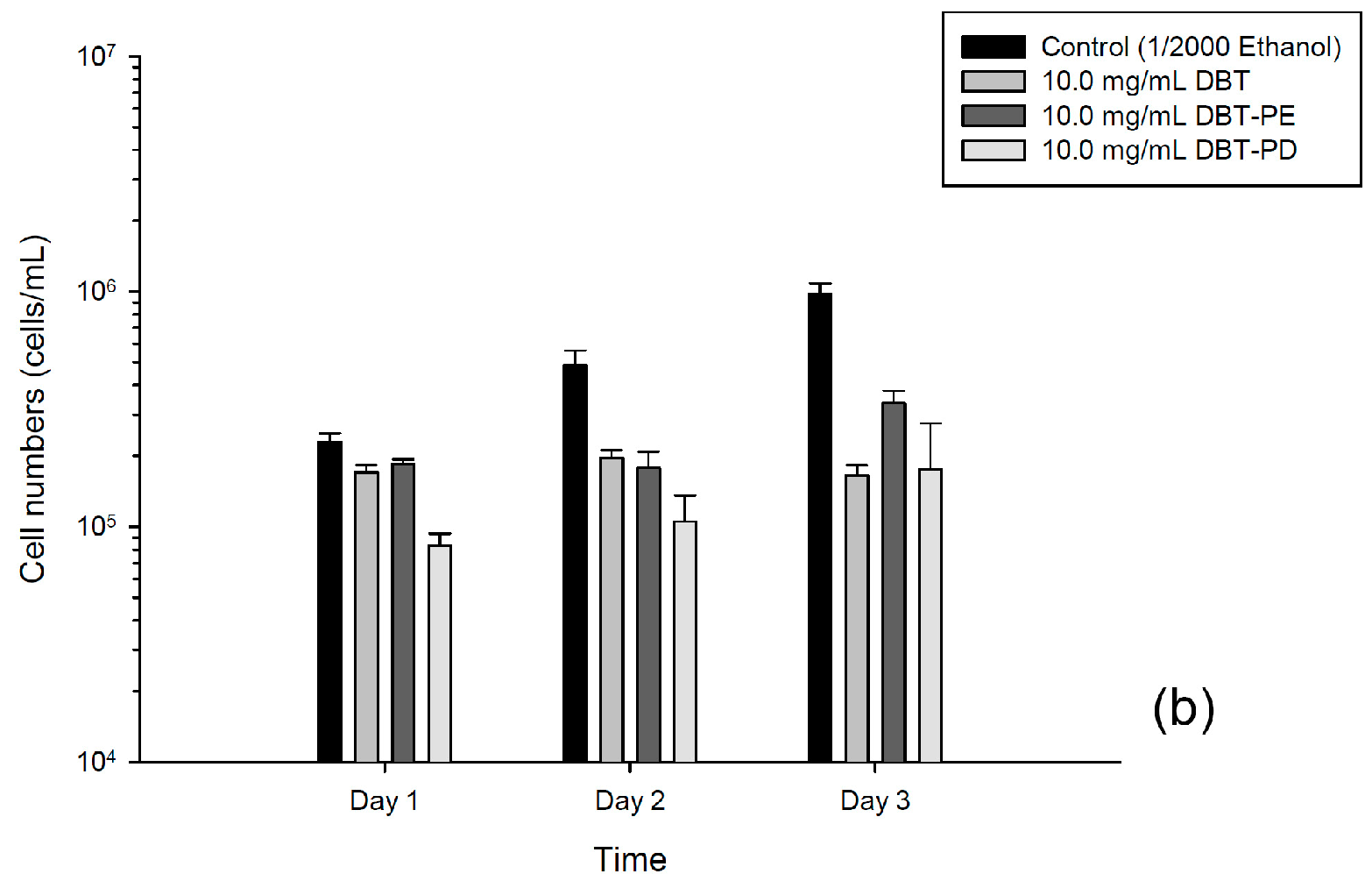
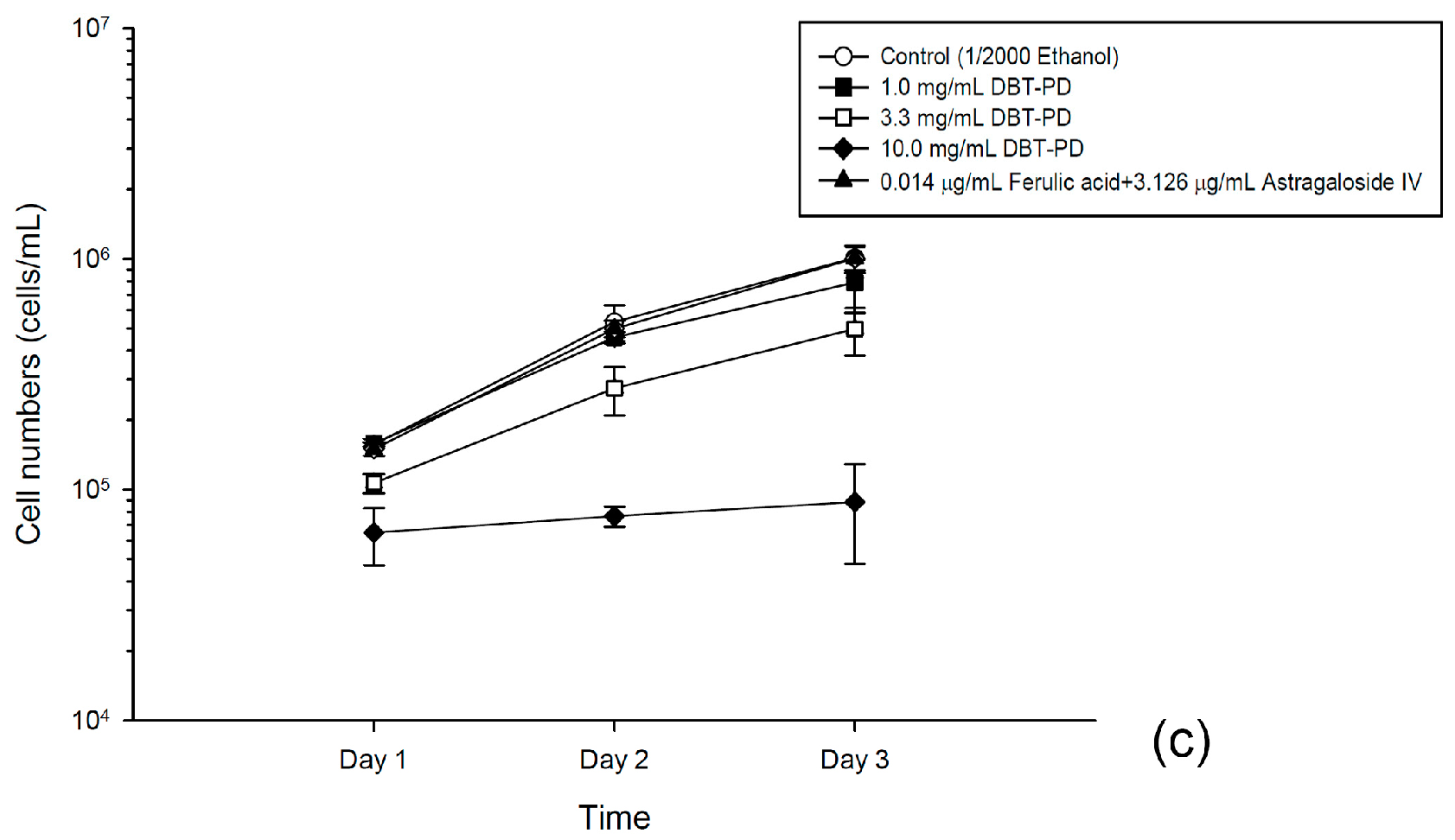
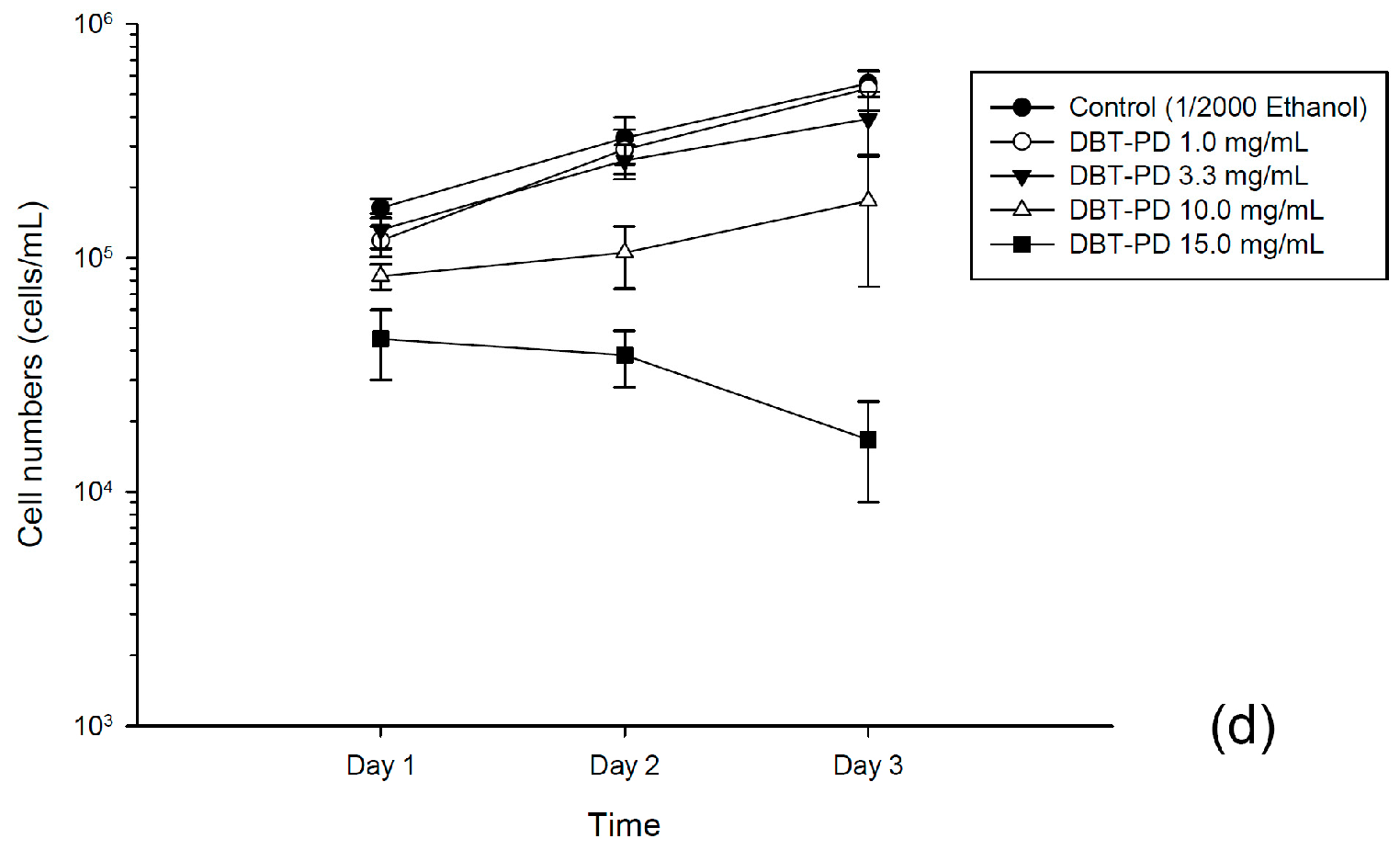
2.3. Inhibition of Viability of CT26 and HT-29 Cells by DBT-PD
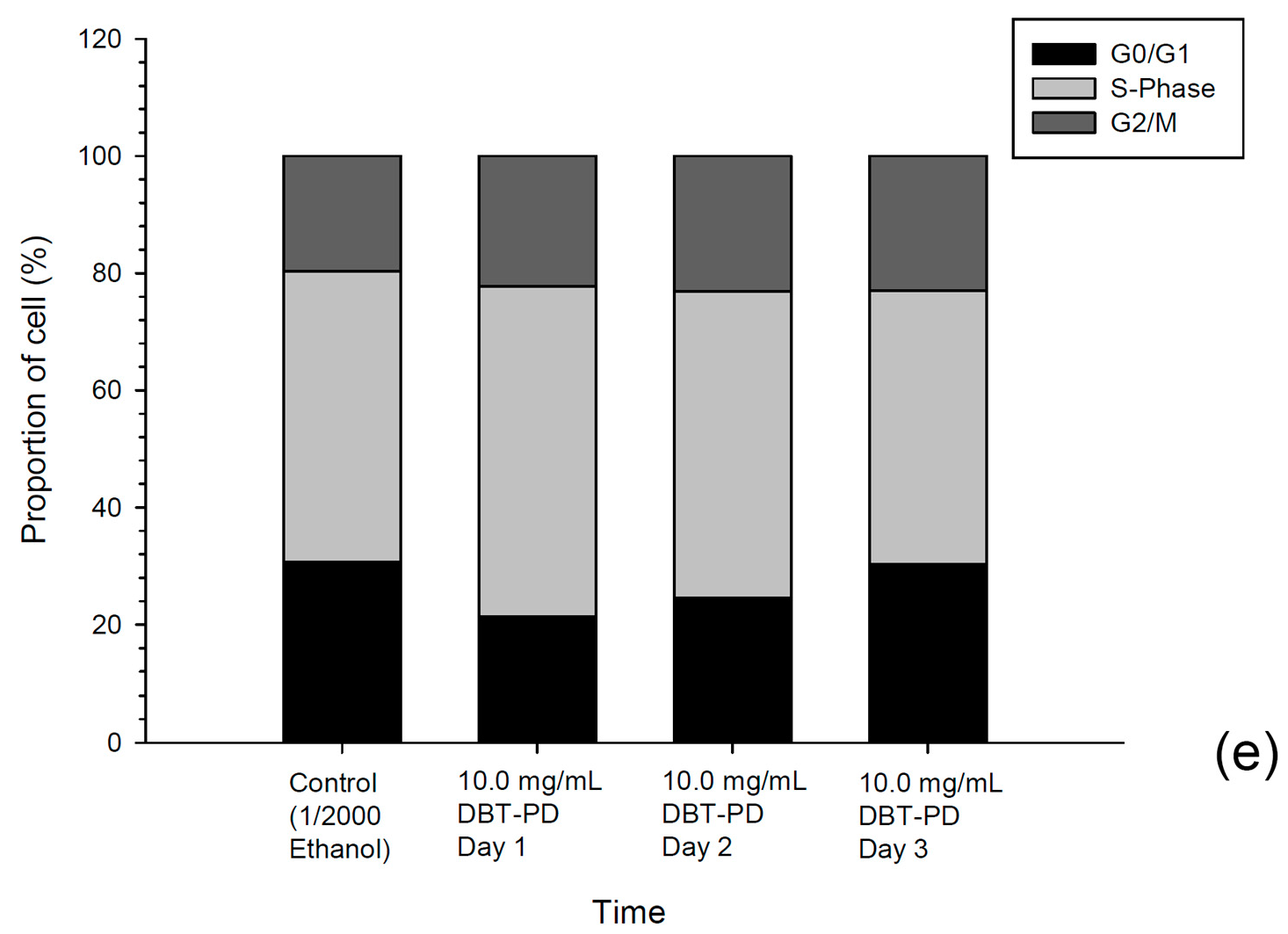
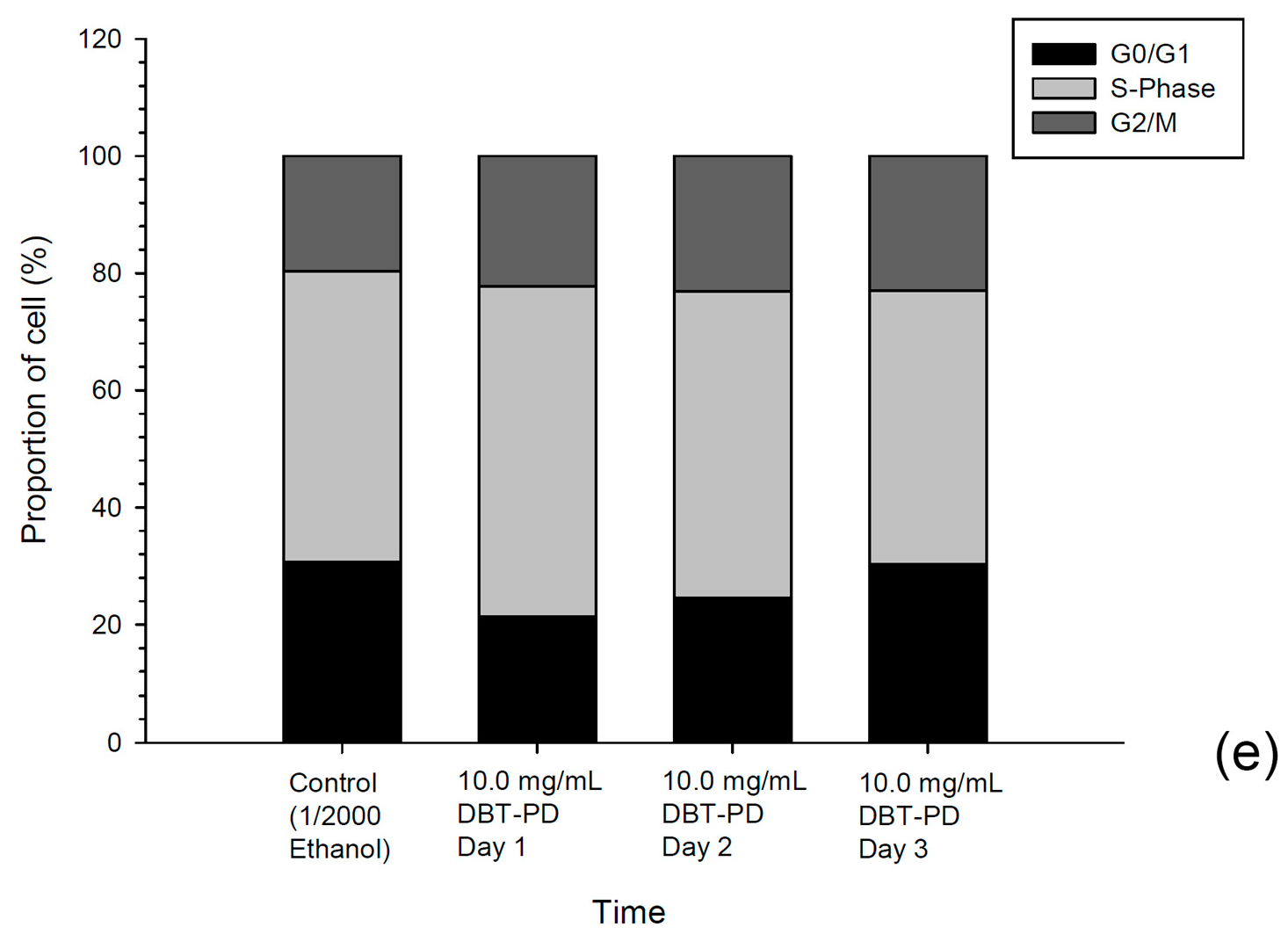
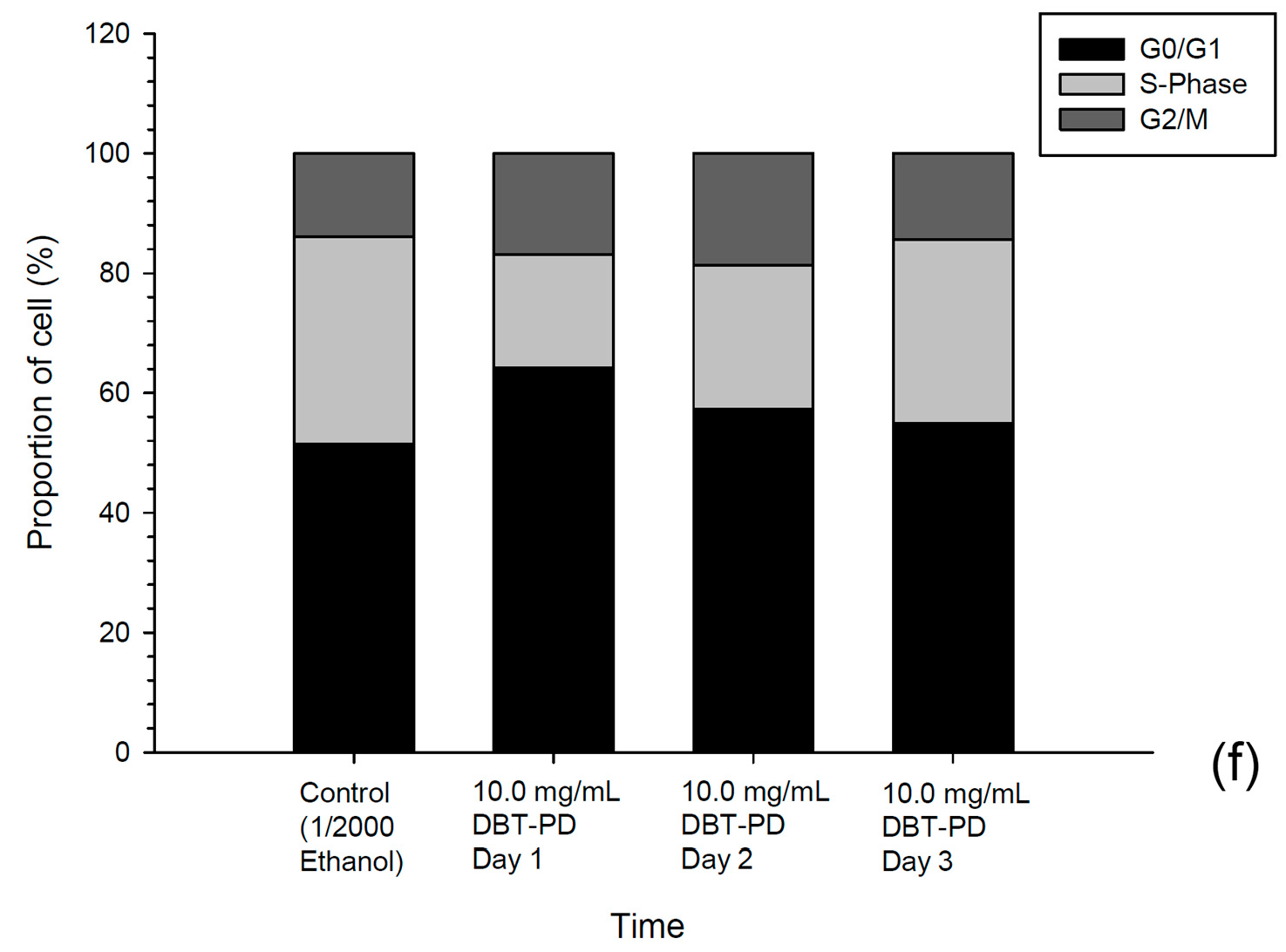
2.4. Cell Cycle Assay
2.5. Caspase Activities
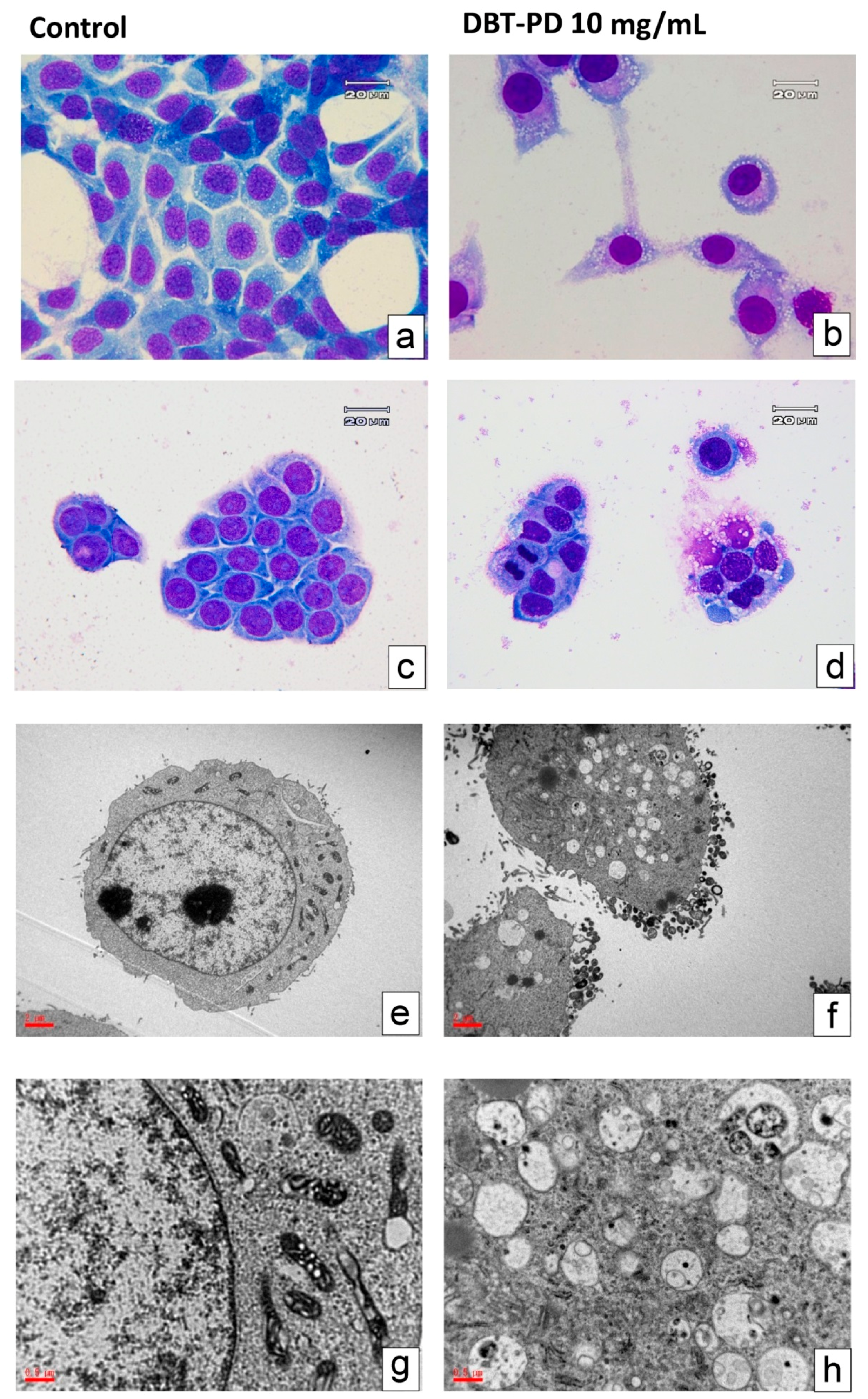
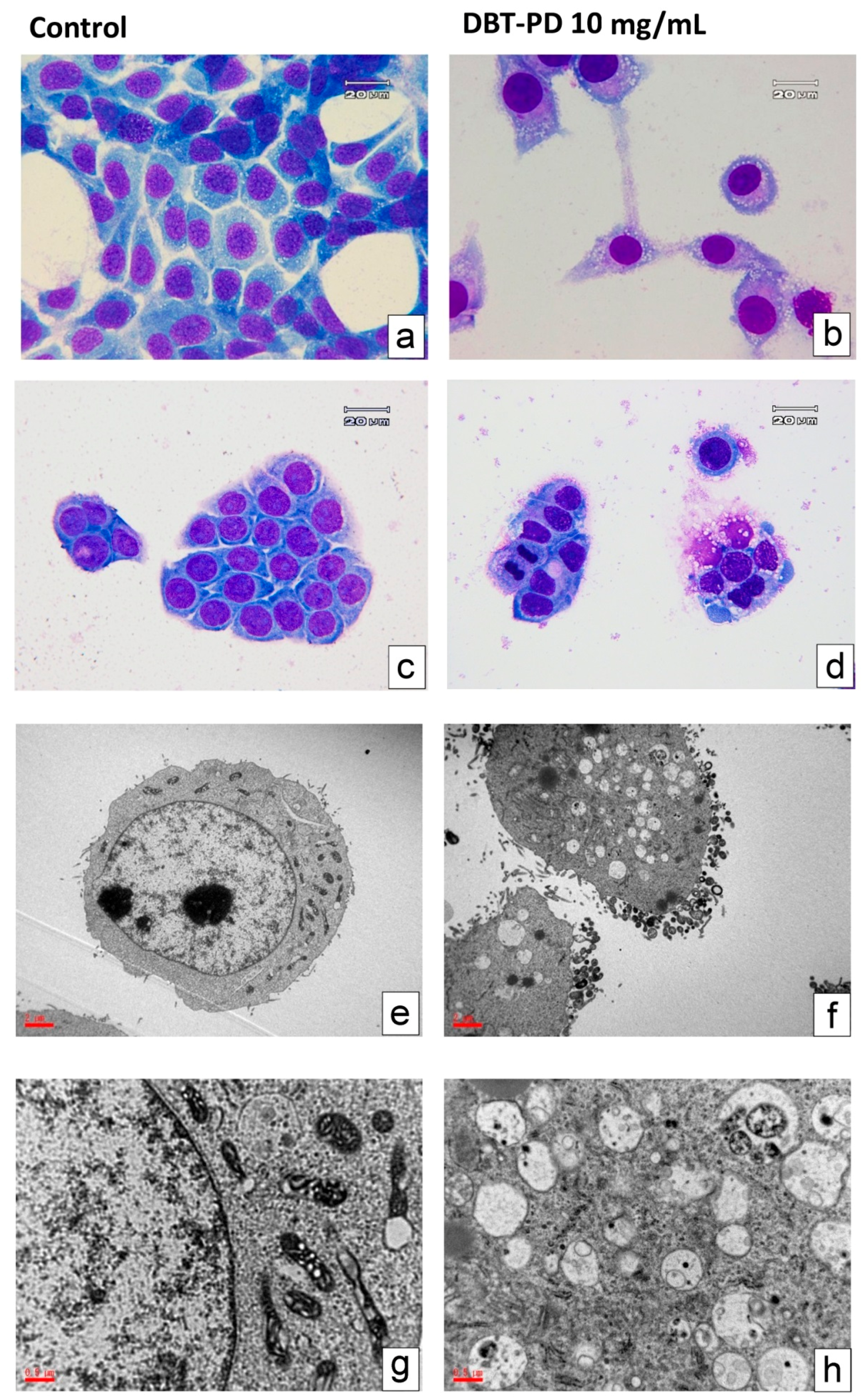
2.6. Cell Morphology
2.7. Enhancement of 5-Fluorouracil (5-FU) Effect by DBT-PD
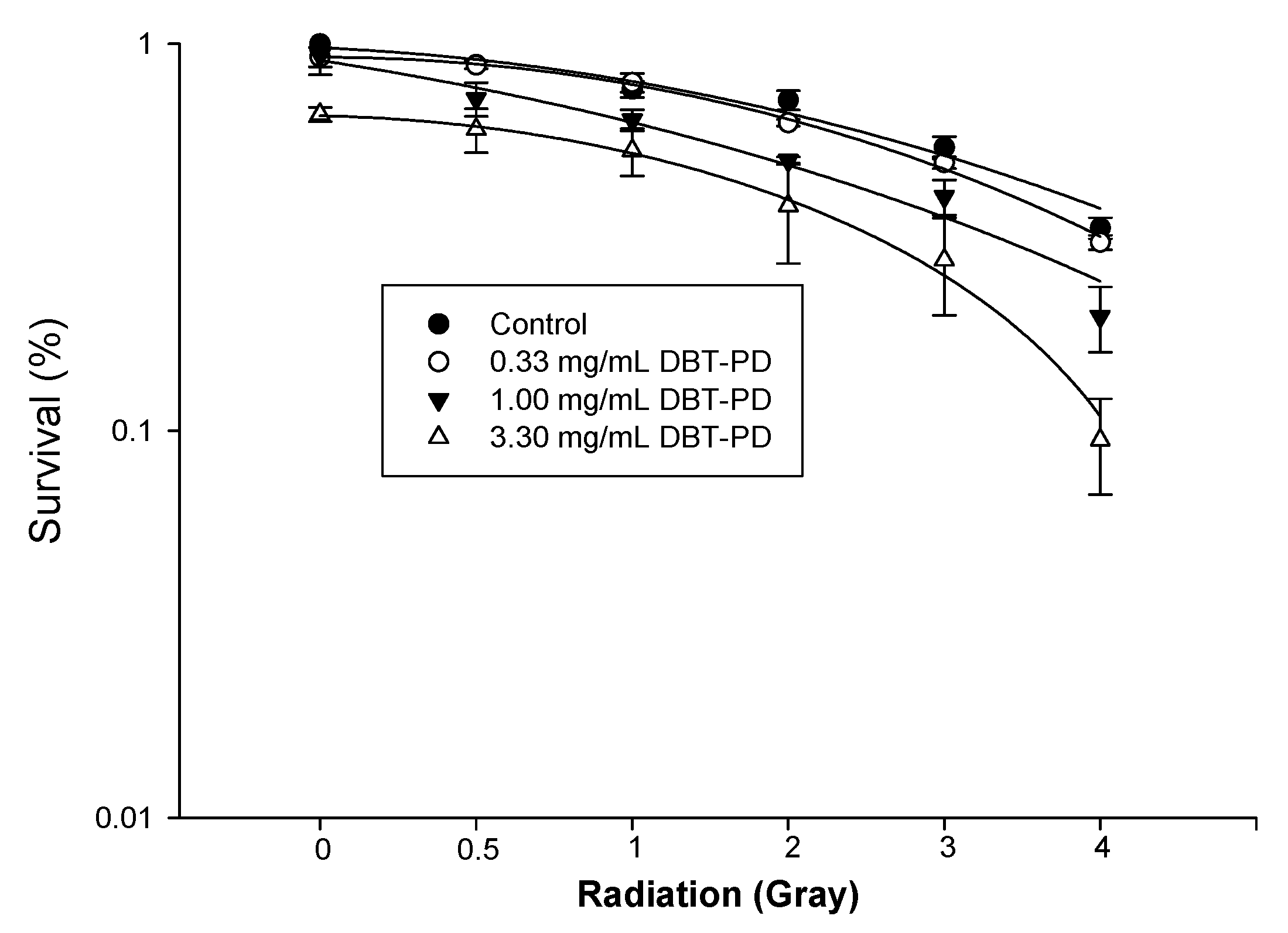
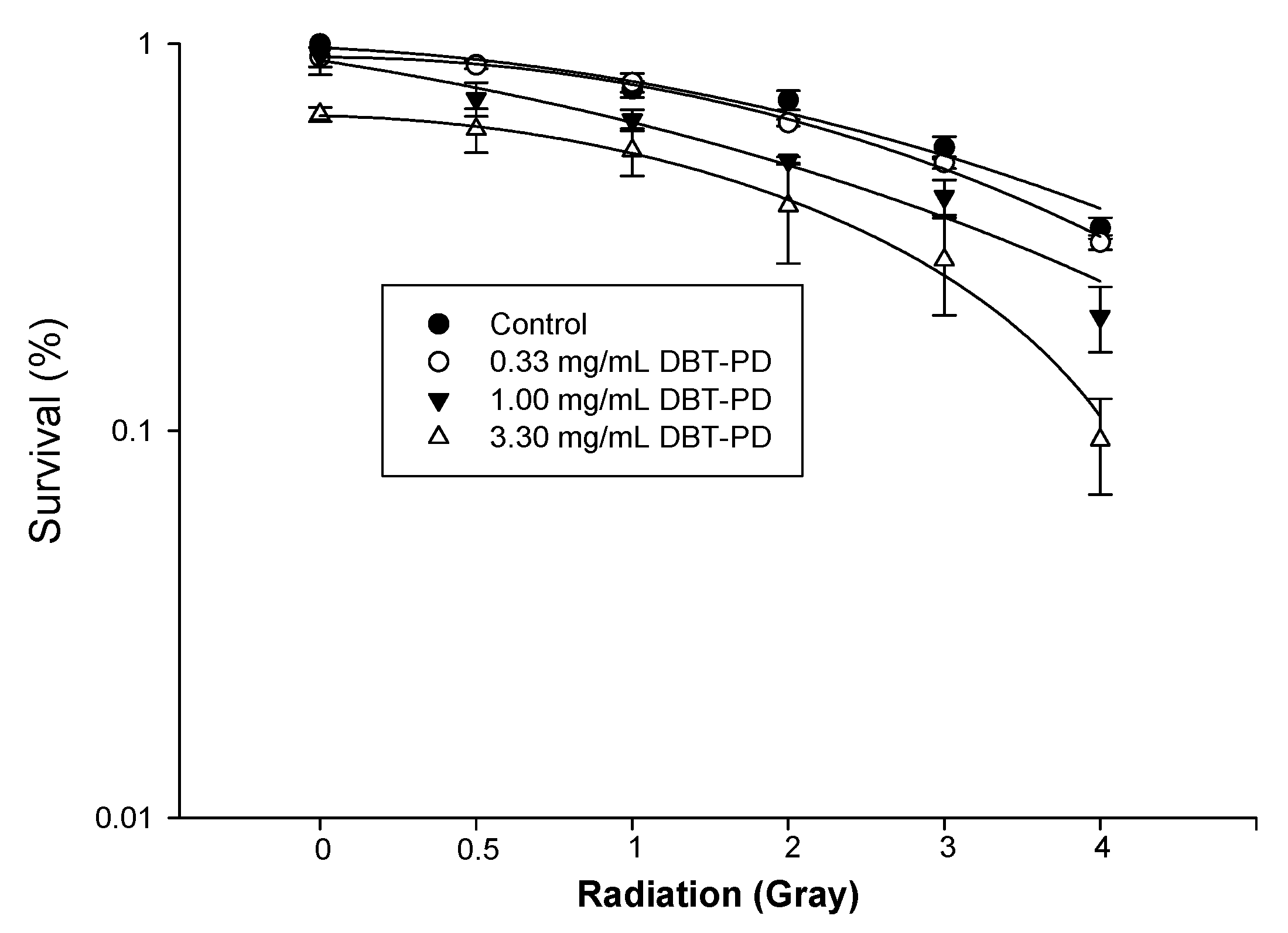
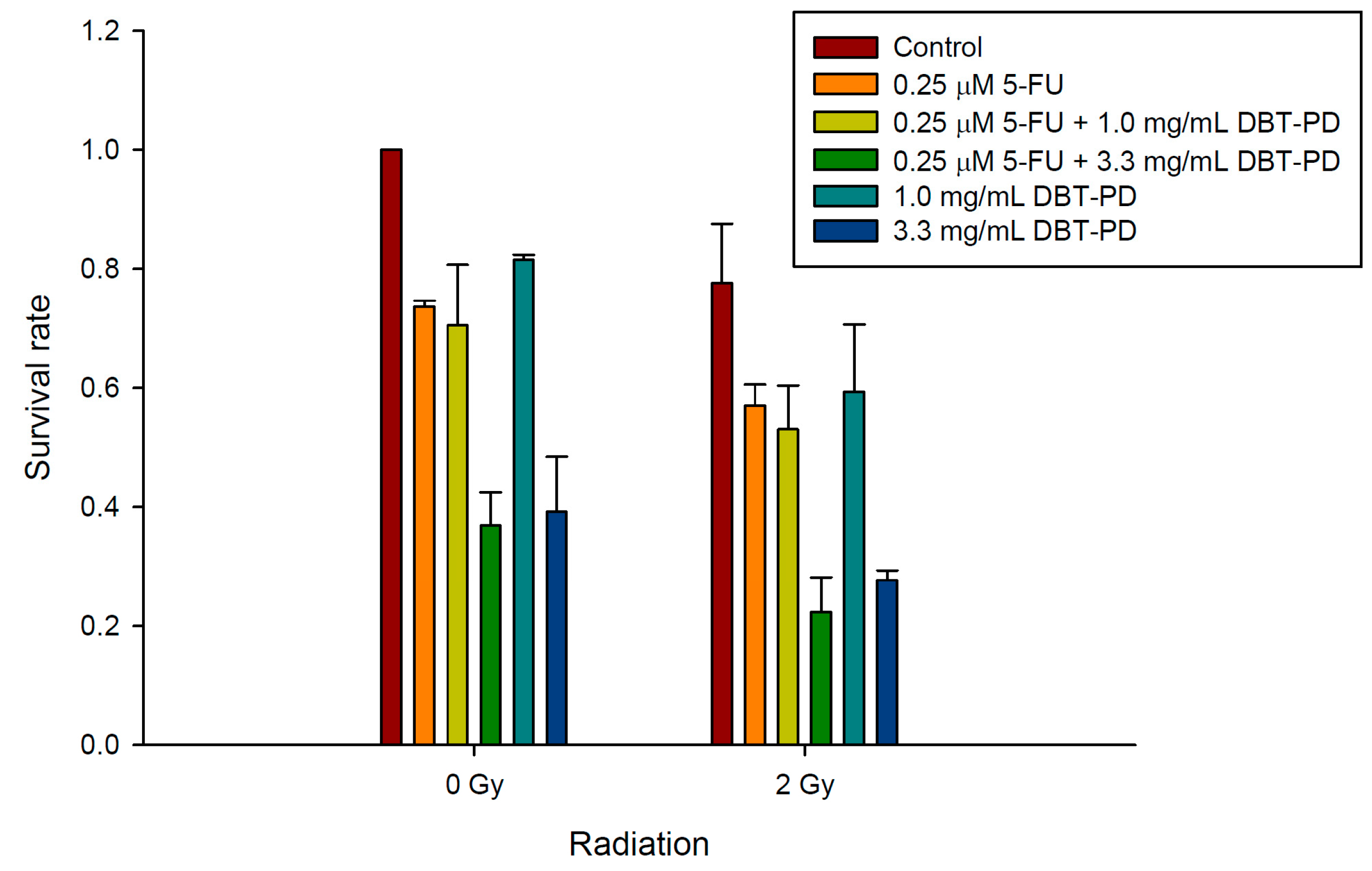
2.8. The Sensitizing Effect of DBT-PD on RT and CCRT
3. Discussion
4. Materials and Methods
4.1. Plant Materials and Preparation of DBT
4.2. Chemical Standardization of DBT
4.3. CT26 and HT-29 Cell Culture
4.4. Determination of Osmolality in Culture Medium
4.5. Cell Viability Assays
4.6. Cell Cycle Analysis by Flow Cytometry
4.7. Measurement of Caspase Activities
4.8. Morphological Observation by Light and Transmission Electron Microscopy
4.9. Irradiation of Cells and Colony Formation Analysis
4.10. Statistical Analysis
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA: Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA: Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.B.; Maggard, M.A.; Ko, C.Y. Colon cancer survival rates with the new american joint committee on cancer sixth edition staging. J. Natl. Cancer Inst. 2004, 96, 1420–1425. [Google Scholar] [CrossRef] [PubMed]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rodel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef] [PubMed]
- Roh, M.S.; Colangelo, L.H.; O’Connell, M.J.; Yothers, G.; Deutsch, M.; Allegra, C.J.; Kahlenberg, M.S.; Baez-Diaz, L.; Ursiny, C.S.; Petrelli, N.J.; et al. Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: Nsabp r-03. J. Clin. Oncol. 2009, 27, 5124–5130. [Google Scholar] [CrossRef] [PubMed]
- Lam, W.; Jiang, Z.; Guan, F.; Hu, R.; Liu, S.H.; Chu, E.; Cheng, Y.C. The number of intestinal bacteria is not critical for the enhancement of antitumor activity and reduction of intestinal toxicity of irinotecan by the chinese herbal medicine phy906 (kd018). BMC Complement. Altern. Med. 2014, 14, 490. [Google Scholar] [CrossRef] [PubMed]
- Saif, M.W.; Li, J.; Lamb, L.; Kaley, K.; Elligers, K.; Jiang, Z.; Bussom, S.; Liu, S.H.; Cheng, Y.C. First-in-human phase ii trial of the botanical formulation phy906 with capecitabine as second-line therapy in patients with advanced pancreatic cancer. Cancer Chemother. Pharmacol. 2014, 73, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Li, D.Y. Differentiation on Endogenous and Exogenous Diseases, 1st ed.; People’s Medical Publishing House: Beijing, China, 2011; pp. 24–25. [Google Scholar]
- Gao, Q.T.; Cheung, J.K.; Choi, R.C.; Cheung, A.W.; Li, J.; Jiang, Z.Y.; Duan, R.; Zhao, K.J.; Ding, A.W.; Dong, T.T.; et al. A chinese herbal decoction prepared from radix astragali and radix angelicae sinensis induces the expression of erythropoietin in cultured hep3b cells. Planta Med. 2008, 74, 392–395. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.T.; Cheung, J.K.; Li, J.; Chu, G.K.; Duan, R.; Cheung, A.W.; Zhao, K.J.; Dong, T.T.; Tsim, K.W. A chinese herbal decoction, danggui buxue tang, prepared from radix astragali and radix angelicae sinensis stimulates the immune responses. Planta Med. 2006, 72, 1227–1231. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Chan, G.C.; Deng, R.; Ng, M.H.; Cheng, S.W.; Lau, C.P.; Ye, J.Y.; Wang, L.; Liu, C. An herbal decoction of radix astragali and radix angelicae sinensis promotes hematopoiesis and thrombopoiesis. J. Ethnopharmacol. 2009, 124, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.T.; Choi, R.C.; Cheung, A.W.; Zhu, J.T.; Li, J.; Chu, G.K.; Duan, R.; Cheung, J.K.; Jiang, Z.Y.; Dong, X.B.; et al. Danggui buxue tang—A chinese herbal decoction activates the phosphorylations of extracellular signal-regulated kinase and estrogen receptor alpha in cultured mcf-7 cells. FEBS Lett. 2007, 581, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Cheng, K.F.; Lo, W.M.; Law, C.; Li, L.; Leung, P.C.; Chung, T.K.; Haines, C.J. A randomized, double-blind, multiple-dose escalation study of a chinese herbal medicine preparation (dang gui buxue tang) for moderate to severe menopausal symptoms and quality of life in postmenopausal women. Menopause 2013, 20, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Choi, R.C.; Gao, Q.T.; Cheung, A.W.; Zhu, J.T.; Lau, F.T.; Li, J.; Li, W.Z.; Chu, G.K.; Duan, R.; Cheung, J.K.; et al. A chinese herbal decoction, danggui buxue tang, stimulates proliferation, differentiation and gene expression of cultured osteosarcoma cells: Genomic approach to reveal specific gene activation. Evid. Based Complement. Altern. Med. 2011, 2011, 307548. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.L.; Sheu, S.Y.; Chen, Y.S.; Kao, S.T.; Fu, Y.T.; Kuo, T.F.; Chen, K.Y.; Yao, C.H. Evaluating the bone tissue regeneration capability of the chinese herbal decoction danggui buxue tang from a molecular biology perspective. BioMed Res. Int. 2014, 2014, 853234. [Google Scholar] [PubMed]
- Dong, T.T.; Zhao, K.J.; Gao, Q.T.; Ji, Z.N.; Zhu, T.T.; Li, J.; Duan, R.; Cheung, A.W.; Tsim, K.W. Chemical and biological assessment of a chinese herbal decoction containing radix astragali and radix angelicae sinensis: Determination of drug ratio in having optimized properties. J. Agric. Food Chem. 2006, 54, 2767–2774. [Google Scholar] [CrossRef] [PubMed]
- Chiu, P.Y.; Leung, H.Y.; Siu, A.H.; Poon, M.K.; Dong, T.T.; Tsim, K.W.; Ko, K.M. Dang-gui buxue tang protects against oxidant injury by enhancing cellular glutathione in h9c2 cells: Role of glutathione synthesis and regeneration. Planta Med. 2007, 73, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.T.; Cheung, J.K.; Li, J.; Jiang, Z.Y.; Chu, G.K.; Duan, R.; Cheung, A.W.; Zhao, K.J.; Choi, R.C.; Dong, T.T.; et al. A chinese herbal decoction, danggui buxue tang, activates extracellular signal-regulated kinase in cultured t-lymphocytes. FEBS Lett. 2007, 581, 5087–5093. [Google Scholar] [CrossRef] [PubMed]
- Shintani, T.; Klionsky, D.J. Autophagy in health and disease: A double-edged sword. Science 2004, 306, 990–995. [Google Scholar] [CrossRef] [PubMed]
- Rubinsztein, D.C.; Gestwicki, J.E.; Murphy, L.O.; Klionsky, D.J. Potential therapeutic applications of autophagy. Nat. Rev. Drug Discov. 2007, 6, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Lum, J.J.; DeBerardinis, R.J.; Thompson, C.B. Autophagy in metazoans: Cell survival in the land of plenty. Nat. Rev. Mol. Cell. Biol. 2005, 6, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Panganiban, R.A.; Snow, A.L.; Day, R.M. Mechanisms of radiation toxicity in transformed and non-transformed cells. Int. J. Mol. Sci. 2013, 14, 15931–15958. [Google Scholar] [CrossRef] [PubMed]
- Ondrej, M.; Cechakova, L.; Durisova, K.; Pejchal, J.; Tichy, A. To live or let die: Unclear task of autophagy in the radiosensitization battle. Radiother. Oncol. 2016, 119, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Klionsky, D.J.; Abdalla, F.C.; Abeliovich, H.; Abraham, R.T.; Acevedo-Arozena, A.; Adeli, K.; Agholme, L.; Agnello, M.; Agostinis, P.; Aguirre-Ghiso, J.A.; et al. Guidelines for the use and interpretation of assays for monitoring autophagy. Autophagy 2012, 8, 445–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, T.C.; Talalay, P. Quantitative analysis of dose-effect relationships: The combined effects of multiple drugs or enzyme inhibitors. Adv. Enzym. Regul. 1984, 22, 27–55. [Google Scholar] [CrossRef]
- Zhang, N.; Fu, J.N.; Chou, T.C. Synergistic combination of microtubule targeting anticancer fludelone with cytoprotective panaxytriol derived from panax ginseng against mx-1 cells in vitro: Experimental design and data analysis using the combination index method. Am. J. Cancer Res. 2016, 6, 97–104. [Google Scholar] [PubMed]
- Sample Availability: Not available.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index Component | DBT | DBT-PE | DBT-PD |
|---|---|---|---|
| Ferulic acid (µg/g) | 0.294 | 0.433 | 1.404 |
| Astragaloside IV (µg/g) | 48.462 | 11.367 | 312.626 |
| Control | 1/2000 Ethanol | DBT-PD 3.3 mg/mL | DBT-PD 10 mg/mL | DBT-PD 15 mg/mL | DBT-PD 30 mg/mL |
|---|---|---|---|---|---|
| 291.0 ± 5.2 | 375.3 ± 34.1 | 370.7 ± 11.0 | 360.0 ± 21.7 | 387.3 ± 14.4 | 507.7 ± 18.8 |
| Caspase | Control | DBT-PD 10 mg/mL |
|---|---|---|
| 1 | 28.00 ± 2.76 | 23.07 ± 2.66 |
| 2 | 32.05 ± 6.72 | 31.20 ± 4.17 |
| 3/7 | 30.49 ± 6.91 | 29.87 ± 7.85 |
| 4 | 33.18 ± 1.63 | 33.26 ± 3.57 |
| 5 | 21.39 ± 4.02 | 20.56 ± 2.92 |
| 6 | 27.81 ± 1.92 | 27.81 ± 2.14 |
| 8 | 23.72 ± 0.75 | 20.60 ± 0.50 |
| 9 | 22.09 ± 1.84 | 22.94 ± 5.54 |
| 10 | 25.38 ± 8.83 | 24.53 ± 4.71 |
| Treatment Time | DBT-PD (mg/mL) | 5-FU (μM) | |||
|---|---|---|---|---|---|
| 0.0 | 0.1 | 0.5 | 1.0 | ||
| 24 h | 0.0 | - | 6.7% ± 1.6% | 58.6% ± 11.2% | 76.3% ± 9.2% |
| 1.0 | 30.5% ± 1.0% | 29.7% ± 3.0% (1.45) | 67.2% ± 1.6% (0.82) | 77.7% ± 8.3% (1.11) | |
| 3.3 | 48.8% ± 14.8% | 62.4% ± 7.2% (0.61) | 84.0% ± 6.0% (0.49) | 80.8% ± 6.5% (1.06) | |
| 48 h | 0.0 | 10.9% ± 9.6% | 76.0% ± 8.4% | 91.7% ± 2.9% | |
| 1.0 | 34.1% ± 6.1% | 51.5% ± 5.7% (0.87) | 83.1% ± 5.1% (0.93) | 94.4% ± 2.5% (0.94) | |
| 3.3 | 68.9% ± 3.4% | 74.2% ± 4.3% (1.01) | 95.9% ± 0.9% (0.53) | 96.2% ± 2.9% (0.84) | |
| 72 h | 0.0 | 16.4% ± 4.9% | 83.5% ± 4.4% | 95.6% ± 1.9% | |
| 1.0 | 34.1% ± 8.7% | 37.7% ± 6.9% (1.46) | 88.4% ± 3.9% (0.93) | 96.8% ± 2.5% (0.86) | |
| 3.3 | 65.8% ± 12.4% | 72.0% ±7.0% (1.10) | 97.7% ± 1.5% (0.42) | 98.4% ± 0.3% (0.66) | |
| Treatment Time | DBT-PD (mg/mL) | 5-FU (μM) | |||
|---|---|---|---|---|---|
| 0.0 | 0.1 | 0.5 | 1.0 | ||
| 72 h | 0.0 | 27.4% ± 10.0% | 38.1% ± 14.8% | 66.4% ± 4.3% | |
| 1.0 | 22.2% ± 11.3% | 42.4% ± 5.0% (0.65) | 59.7% ± 9.6% (0.72) | 66.5% ± 3.5% (0.77) | |
| 3.3 | 46.4% ± 7.6% | 59.1% ± 10.2% (0.75) | 34.5% ± 4.6% (4.07) | 73.1% ± 5.1% (0.73) | |
© 2016 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.-T.; Lee, T.-Y.; Tsai, T.-H.; Lin, Y.-C.; Lin, C.-P.; Shieh, H.-R.; Hsu, M.-L.; Chi, C.-W.; Lee, M.-C.; Chang, H.-H.; et al. The Traditional Chinese Medicine DangguiBuxue Tang Sensitizes Colorectal Cancer Cells to Chemoradiotherapy. Molecules 2016, 21, 1677. https://doi.org/10.3390/molecules21121677
Chen S-T, Lee T-Y, Tsai T-H, Lin Y-C, Lin C-P, Shieh H-R, Hsu M-L, Chi C-W, Lee M-C, Chang H-H, et al. The Traditional Chinese Medicine DangguiBuxue Tang Sensitizes Colorectal Cancer Cells to Chemoradiotherapy. Molecules. 2016; 21(12):1677. https://doi.org/10.3390/molecules21121677
Chicago/Turabian StyleChen, Shun-Ting, Tzung-Yan Lee, Tung-Hu Tsai, Yin-Cheng Lin, Chin-Ping Lin, Hui-Ru Shieh, Ming-Ling Hsu, Chih-Wen Chi, Ming-Cheng Lee, Hen-Hong Chang, and et al. 2016. "The Traditional Chinese Medicine DangguiBuxue Tang Sensitizes Colorectal Cancer Cells to Chemoradiotherapy" Molecules 21, no. 12: 1677. https://doi.org/10.3390/molecules21121677