
Clinical Signs, Staphylococcus and Atopic Eczema-Related Seromarkers

 ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
3.1. Anti-Staphylococcus Enterotoxins Immunoglobulin E (anti-SE IgE)
3.2. Th Cytokines
3.3. Treg Cytokines
3.4. APC Cytokines
3.5. Quality of Life
4. Patients and Methods
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Leung, A.K.; Hon, K.L.; Robson, W.L. Atopic dermatitis. Adv. Pediatr. 2007, 54, 241–273. [Google Scholar] [CrossRef] [PubMed]
- Leung, T.N.; Hon, K.L. Eczema therapeutics in children: what do the clinical trials say? Hong Kong Med. J. 2015, 21, 251–260. [Google Scholar] [PubMed]
- Williams, H.C.; Burney, P.G.; Pembroke, A.C.; Hay, R.J. The U.K. Working Party’s Diagnostic Criteria for Atopic Dermatitis. III. Independent hospital validation. Br. J. Dermatol. 1994, 131, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.C.; Burney, P.G.; Hay, R.J.; Archer, C.B.; Shipley, M.J.; Hunter, J.J.; Bingham, E.A.; Finlay, A.Y.; Pembroke, A.C.; Graham-Brown, R.A.; et al. The U.K. Working Party’s Diagnostic Criteria for Atopic Dermatitis. I. Derivation of a minimum set of discriminators for atopic dermatitis. Br. J. Dermatol. 1994, 131, 383–396. [Google Scholar] [PubMed]
- Eyerich, K.; Novak, N. Immunology of atopic eczema: Overcoming the Th1/Th2 paradigm. Allergy 2013, 68, 974–982. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.; Leung, T.F. Seromarkers in childhood atopic dermatitis. Expert Rev. Dermatol. 2010, 5, 299–314. [Google Scholar] [CrossRef]
- Hon, K.L.; Ching, G.K.; Wong, K.Y.; Leung, T.F.; Leung, A.K. A pilot study to explore the usefulness of antibody array in childhood atopic dermatitis. J. Natl. Med. Assoc. 2008, 100, 500–504. [Google Scholar] [PubMed]
- Homey, B.; Steinhoff, M.; Ruzicka, T.; Leung, D.Y. Cytokines and chemokines orchestrate atopic skin inflammation. J. Allergy Clin. Immunol. 2006, 118, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, S.; Uchi, H.; Moroi, Y.; Furue, M. Decrease in circulating Th17 cells correlates with increased levels of CCL17, IgE and eosinophils in atopic dermatitis. J. Dermatol. Sci. 2011, 61, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Kung, J.S.; Wang, M.; Pong, N.H.; Li, A.M.; Leung, T.F. Clinical scores of sleep loss/itch and antihistamine/topical corticosteroid usage for childhood eczema. Br. J. Dermatol. 2016, 175, 1076–1078. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Luk, C.K.; Tsang, Y.C.; Pong, N.H.; Leung, T.F. Objective measurement of two clinical signs in childhood atopic eczema in research and therapeutics. J. Dermatolog. Treat. 2016, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Ching, G.K.; Ng, P.C.; Leung, T.F. Exploring CCL18, eczema severity and atopy. Pediatr. Allergy Immunol. 2011, 22, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Lam, M.C.; Wong, K.Y.; Leung, T.F.; Ng, P.C. Pathophysiology of nocturnal scratching in childhood atopic dermatitis: The role of brain-derived neurotrophic factor and substance P. Br. J. Dermatol. 2007, 157, 922–925. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Tsang, Y.C.; Pong, N.H.; Ng, C.; Ip, M.; Leung, T.F. Clinical features and Staphylococcus aureus colonization/infection in childhood atopic dermatitis. J. Dermatol. Treat. 2016, 27, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Tsang, Y.C.; Pong, N.H.; Leung, T.F.; Ip, M. Exploring Staphylococcus epidermidis in atopic eczema: Friend or foe? Clin. Exp. Dermatol. 2016, 41, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Tsang, Y.C.; Lee, V.W.; Pong, N.H.; Ha, G.; Lee, S.T.; Chow, C.M.; Leung, T.F. Efficacy of sodium hypochlorite (bleach) baths to reduce Staphylococcus aureus colonization in childhood onset moderate-to-severe eczema: A randomized, placebo-controlled cross-over trial. J. Dermatol. Treat. 2016, 27, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, K.; Barath, S.; Nagy, G.; Mocsai, G.; Gyimesi, E.; Szodoray, P.; Irinyi, B.; Zeher, M.; Remenyik, É.; Szegedi, A. Regulatory T-cell subsets with acquired functional impairment: Important indicators of disease severity in atopic dermatitis. Acta Derm. Venereol. 2015, 95, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Kunz, B.; Oranje, A.P.; Labreze, L.; Stalder, J.F.; Ring, J.; Taieb, A. Clinical validation and guidelines for the SCORAD index: Consensus report of the European Task Force on Atopic Dermatitis. Dermatology 1997, 195, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Wang, S.S.; Pong, N.H.; Leung, T.F. Circulating Immunoglobulins, Leucocytes and Complements in Childhood-onset Atopic Eczema. Indian J. Pediatr. 2013, 80, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Hanifin, J.; Rajka, G. Diagnostic features of atopic dermatitis. Acta Derm. Venereol. (Stockh.) 1980, 2, 44–47. [Google Scholar]
- Severity scoring of atopic dermatitis: The SCORAD Index. Consensus Report of the European Task Force on Atopic Dermatitis. Dermatology 1993, 186, 23–31.
- Charman, C.; Williams, H. Outcome measures of disease severity in atopic eczema. Arch. Dermatol. 2000, 136, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Charman, C.; Chambers, C.; Williams, H. Measuring atopic dermatitis severity in randomized controlled clinical trials: What exactly are we measuring? J. Investig. Dermatol. 2003, 120, 932–941. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.; Kam, W.Y.; Lam, M.; Leung, T.; Ng, P.C. CDLQI, SCORAD and NESS: Are they Correlated? Qual. Life Res. 2006, 15, 1551–1558. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Lam, M.C.; Leung, T.F.; Kam, W.Y.; Li, M.C.; Ip, M.; Fok, T.F. Clinical features associated with nasal Staphylococcus aureus colonisation in Chinese children with moderate-to-severe atopic dermatitis. Ann. Acad. Med. Singap. 2005, 34, 602–605. [Google Scholar] [PubMed]
- Sonkoly, E.; Muller, A.; Lauerma, A.I.; Pivarcsi, A.; Soto, H.; Kemeny, L.; Alenius, H.; Dieu-Nosjean, M.C.; Meller, S.; Rieker, J.; et al. IL-31: A new link between T cells and pruritus in atopic skin inflammation. J. Allergy Clin. Immunol. 2006, 117, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.C.; Barber, K.A. Managing childhood atopic dermatitis. Adv. Ther. 2003, 20, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.; Jain, N.; Leo, H.L. New concepts in the pathogenesis of atopic dermatitis. Curr. Opin. Immunol. 2003, 15, 634–638. [Google Scholar] [CrossRef] [PubMed]
- Abramovits, W. Atopic dermatitis. J. Am. Acad. Dermatol. 2005, 53 (Suppl. 1), S86–S93. [Google Scholar] [CrossRef] [PubMed]
- Mosmann, T.R.; Coffman, R.L. TH1 and TH2 cells: Different patterns of lymphokine secretion lead to different functional properties. Ann. Rev. Immunol. 1989, 7, 145–173. [Google Scholar] [CrossRef] [PubMed]
- Luster, A.D. Chemokines—Chemotactic cytokines that mediate inflammation. N. Eng. J. Med. 1998, 338, 436–445. [Google Scholar]
- Sakaguchi, S. Regulatory T cells: Key controllers of immunologic self-tolerance. Cell 2000, 101, 455–458. [Google Scholar] [CrossRef]
- Lee, N.; Shin, J.U.; Jin, S.; Yun, K.N.; Kim, J.Y.; Park, C.O.; Kim, S.H.; Noh, J.Y.; Lee, K.H. Upregulation of CD47 in Regulatory T Cells in Atopic Dermatitis. Yonsei Med. J. 2016, 57, 1435–1445. [Google Scholar] [CrossRef] [PubMed]
- Roesner, L.M.; Floess, S.; Witte, T.; Olek, S.; Huehn, J.; Werfel, T. Foxp3(+) regulatory T cells are expanded in severe atopic dermatitis patients. Allergy 2015, 70, 1656–1660. [Google Scholar] [CrossRef] [PubMed]
- Laborel-Preneron, E.; Bianchi, P.; Boralevi, F.; Lehours, P.; Fraysse, F.; Morice-Picard, F.; Sugai, M.; Sato’o, Y.; Badiou, C.; Lina, G.; et al. Effects of the Staphylococcus aureus and Staphylococcus epidermidis Secretomes Isolated from the Skin Microbiota of Atopic Children on CD4+ T Cell Activation. PLoS ONE 2015, 10, e0141067. [Google Scholar] [CrossRef] [PubMed]
- Kodelja, V.; Muller, C.; Politz, O.; Hakij, N.; Orfanos, C.E.; Goerdt, S. Alternative macrophage activation-associated CC-chemokine-1, a novel structural homologue of macrophage inflammatory protein-1 alpha with a Th2-associated expression pattern. J. Immunol. 1998, 160, 1411–1418. [Google Scholar] [PubMed]
- Vulcano, M.; Struyf, S.; Scapini, P.; Cassatella, M.; Bernasconi, S.; Bonecchi, R.; Calleri, A.; Penna, G.; Adorini, L.; Luini, W.; et al. Unique regulation of CCL18 production by maturing dendritic cells. J. Immunol. 2003, 170, 3843–3849. [Google Scholar] [CrossRef] [PubMed]
- De Nadai, P. Involvement of CCL18 in Inflammatory Allergic Diseases. J. Allergy Clin. Immunol. 2004, 113, S262. [Google Scholar] [CrossRef]
- Hon, K.L.E.; Leung, T.F.; Ma, K.C.; Wong, C.K.P.; Wan, H.M.R.C.; Lam, C.W. Serum Concentration of IL-18 Correlates with Disease Extent in Young Children with Atopic Dermatitis. Pediatr. Dermatol. 2004, 21, 619–622. [Google Scholar] [CrossRef] [PubMed]
- Okamura, H.; Tsutsui, H.; Komatsu, T.; Yutsudo, M.; Hakura, A.; Tanimoto, T.; Torigoe, K.; Okura, T.; Nukada, Y.; Hattori, K.; et al. Cloning of a new cytokine that induces IFN-gamma production by T cells. Nature 1995, 378, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Yoshizawa, Y.; Nomaguchi, H.; Izaki, S.; Kitamura, K. Serum cytokine levels in atopic dermatitis. Clin. Exp. Dermatol. 2002, 27, 225–229. [Google Scholar] [CrossRef] [PubMed]
- El Mezzein, R.E.H.; Matsumoto, T.; Nomiyama, H.; Miike, T. Increased secretion of IL-18 in vitro by peripheral blood mononuclear cells of patients with bronchial asthma and atopic dermatitis. Clin. Exp. Immunol. 2001, 126, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Higashi, N.M.; Gesser, B.P.; Kawana, S.M.; Thestrup-Pedersen, K.M.P. Expression of IL-18 mRNA and secretion of IL-18 are reduced in monocytes from patients with atopic dermatitis. J. Allergy Clin. Immunol. 2001, 108, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, T.; Wiltrout, R.H.; Young, H.A. IL-18 is a potent coinducer of IL-13 in NK and T cells: A new potential role for IL-18 in modulating the immune response. J. Immunol. 1999, 162, 5070–5077. [Google Scholar] [PubMed]
- Wild, J.S.; Sigounas, A.; Sur, N.; Siddiqui, M.S.; Alam, R.; Kurimoto, M.; Sur, S. IFN-gamma-inducing factor (IL-18) increases allergic sensitization, serum IgE, Th2 cytokines, and airway eosinophilia in a mouse model of allergic asthma. J. Immunol. 2000, 164, 2701–2710. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.; Chu, I.M.; Hon, K.L.; Tsang, M.S.; Lam, C.W. Aberrant Expression of Bacterial Pattern Recognition Receptor NOD2 of Basophils and Microbicidal Peptides in Atopic Dermatitis. Molecules 2016, 21, E471. [Google Scholar] [CrossRef] [PubMed]
- Chuh, A.A. Validation of a Cantonese version of the Children’s Dermatology Life Quality Index. Pediatr. Dermatol. 2003, 20, 479–481. [Google Scholar] [CrossRef] [PubMed]
- Lewis-Jones, M.S.; Finlay, A.Y. The Children’s Dermatology Life Quality Index (CDLQI): Initial validation and practical use. Br. J. Dermatol. 1995, 132, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Wong, K.Y.; Leung, T.F.; Chow, C.M.; Ng, P.C. Comparison of Skin Hydration Evaluation Sites and Correlations among Skin Hydration, Transepidermal Water Loss, SCORAD Index, Nottingham Eczema Severity Score, and Quality of Life in Patients with Atopic Dermatitis. Am. J. Clin. Dermatol. 2008, 9, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Sample Availability: Samples of the compounds are not available from the authors.


{kind=link}
| Total (n = 40) | Moderate AD (n = 16) | Severe AD (n = 24) | p | ||
|---|---|---|---|---|---|
| Demographics | |||||
| Age, years | 13.1 (7.9) | 12.8 (7.2) | 13.7 (6.5) | 0.345 * | |
| Sex–Male, n (%) | 23 (57.5) | 10 (62.5) | 13 (54.2) | 0.601 | |
| Personal allergic rhinitis, n (%) | 28 (70.0) | 10 (62.5) | 18 (75.0) | 0.490 ** | |
| Personal asthma, n (%) | 19 (47.5) | 6 (37.5) | 13 (54.2) | 0.301 | |
| Clinical parameters | |||||
| Objective SCORAD | 45.0 (11.7) | 38.2 (8.7) | 48.6 (6.5) | <0.0005 * | |
| Extent, % | 54.7 ± 14.8 | 43.9 ± 13.0 | 61.8 ± 11.2 | <0.0005 | |
| Intensity | 9.5 (3.0) | 8.0 (2.0) | 10.5 (2.0) | <0.0005 * | |
| Pruritus | 6.7 ± 1.9 | 6.6 ± 1.9 | 6.8 ± 1.9 | 0.786 | |
| Sleep loss | 5.9 ± 2.8 | 5.9 ± 2.6 | 5.9 ± 3.0 | 0.946 | |
| CDLQI | 10.0 (8.0) | 10.0 (8.0) | 10.5 (9.0) | 0.594 * | |
| SH | 32.8 ± 13.5 | 37.4 ± 13.2 | 29.7 ± 13.0 | 0.078 | |
| TEWL, g/m2/h | 12.1 ± 1.7 | 11.7 ± 1.3 | 12.4 ± 1.8 | 0.181 | |
| S. aureus, n (%) # | No | 4 (10.0) | 2 (12.5) | 2 (8.3) | 0.184 ** |
| Scanty | 18 (45.0) | 10 (62.5) | 8 (33.3) | ||
| Moderate | 15 (37.5) | 3 (18.8) | 12 (50.0) | ||
| Heavy | 3 (7.5) | 1 (6.2) | 2 (8.3) | ||
| S. epidermidis, n (%) # | No | 23 (57.5) | 8 (50.0) | 15 (62.5) | 0.150 ** |
| Scanty | 11 (27.5) | 7 (43.8) | 4 (16.7) | ||
| Moderate | 6 (15.0) | 1 (6.2) | 5 (20.8) | ||
| Blood/Serum Markers | Total (n = 40) | Moderate AD (n = 16) | Severe AD (n = 24) | p |
|---|---|---|---|---|
| Eosinophil % in WBC | 10.0 (7.0) | 9.0 (6.0) | 10.5 (6.0) | 0.039 * |
| log (Total IgE count in kU/L) | 3.79 ± 0.51 | 3.53 ± 0.57 | 3.96 ± 0.39 | 0.008 |
| Anti-SEA IgE, kU/L | 0.81 (2.68) | 0.37 (2.64) | 1.17 (2.66) | 0.279 * |
| Anti-SEB IgE, kU/L | 0.90 (3.15) | 0.83 (1.96) | 1.10 (2.87) | 0.202 * |
| IFN-γ, pg/mL | 5.83 (6.24) | 4.76 (2.86) | 9.04 (6.79) | 0.005 * |
| TGF-β, pg/mL | 607 (530) | 804 (526) | 558 (489) | 0.192 * |
| TNF-α, pg/mL | 1.90 (1.07) | 1.74 (1.21) | 2.06 (0.91) | 0.165 * |
| IL-9, pg/mL | 0.71 (1.16) (n = 34) | 0.41 (0.89) (n = 12) | 0.71 (1.11) (n = 22) | 0.276 * |
| IL-10, pg/mL | 0.51 (0.58) (n = 29) | 0.41 (0.53) (n = 9) | 0.63 (0.45) (n = 20) | 0.077 * |
| IL-12, pg/mL | 0.44 (0.20) | 0.37 (0.10) | 0.44 (0.2) | 0.079 * |
| IL-18, pg/mL | 18.15 (15.95) | 13.68 (9.50) | 22.96 (20.81) | 0.007 * |
| IL-23, pg/mL | 1.08 (0.46) | 1.08 (0.46) | 1.08 (0.46) | 0.946 * |
| S. aureus Density * | S. epidermidis Density * | Objective SCORAD | Extent, % | Intensity | Pruritus | Sleep Loss | CDLQI | SH | TEWL, g/m2/h | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| S. aureus isolation * | rho | 0.093 | 0.436 | 0.237 | 0.459 | 0.503 | 0.208 | 0.007 | −0.198 | 0.280 | |
| p | 0.583 | 0.007 | 0.158 | 0.004 | 0.002 | 0.217 | 0.969 | 0.240 | 0.094 | ||
| S. epidermidis isolation * | rho | 0.045 | 0.103 | 0.013 | 0.342 | 0.209 | 0.134 | 0.044 | −0.012 | ||
| p | 0.791 | 0.545 | 0.938 | 0.038 | 0.215 | 0.428 | 0.797 | 0.942 | |||
| Eosinophil % in WBC | rho | 0.478 | 0.015 | 0.476 | 0.362 | 0.448 | 0.295 | 0.275 | 0.425 | −0.370 | −0.024 |
| p | 0.003 | 0.928 | 0.003 | 0.028 | 0.005 | 0.077 | 0.100 | 0.009 | 0.024 | 0.889 | |
| log(Total IgE count in kU/L) | rho | 0.436 | 0.053 | 0.552 | 0.423 | 0.518 | 0.415 | 0.179 | 0.405 | −0.350 | 0.122 |
| p | 0.007 | 0.756 | 0.000 | 0.009 | 0.001 | 0.011 | 0.288 | 0.013 | 0.034 | 0.473 | |
| Anti-SEA IgE, kU/L | rho | 0.051 | −0.083 | 0.214 | −0.009 | 0.209 | 0.173 | −0.097 | 0.399 | −0.032 | −0.107 |
| p | 0.764 | 0.626 | 0.204 | 0.957 | 0.214 | 0.306 | 0.566 | 0.014 | 0.850 | 0.528 | |
| Anti-SEB IgE, kU/L | rho | 0.167 | 0.031 | 0.361 | 0.290 | 0.342 | 0.206 | 0.031 | 0.360 | −0.416 | 0.105 |
| p | 0.324 | 0.854 | 0.028 | 0.081 | 0.038 | 0.221 | 0.856 | 0.029 | 0.010 | 0.538 | |
| IFN-γ, pg/mL | rho | 0.339 | −0.120 | 0.531 | 0.530 | 0.516 | 0.324 | 0.204 | −0.047 | −0.227 | 0.193 |
| p | 0.040 | 0.478 | 0.001 | 0.001 | 0.001 | 0.050 | 0.225 | 0.780 | 0.177 | 0.252 | |
| TGF-β, pg/mL | rho | −0.110 | 0.108 | −0.191 | −0.259 | −0.122 | −0.007 | 0.098 | 0.157 | 0.084 | −0.091 |
| p | 0.517 | 0.523 | 0.258 | 0.121 | 0.473 | 0.968 | 0.564 | 0.353 | 0.619 | 0.592 | |
| TNF-α, pg/mL | rho | 0.231 | −0.038 | 0.422 | 0.593 | 0.371 | 0.258 | 0.264 | 0.070 | −0.132 | 0.066 |
| p | 0.168 | 0.825 | 0.009 | 0.000 | 0.024 | 0.123 | 0.114 | 0.680 | 0.437 | 0.697 | |
| IL-9, pg/mL (n = 34) | rho | −0.065 | −0.201 | 0.202 | 0.562 | 0.115 | 0.123 | 0.282 | −0.138 | −0.184 | 0.072 |
| p | 0.730 | 0.279 | 0.275 | 0.001 | 0.536 | 0.509 | 0.124 | 0.460 | 0.322 | 0.702 | |
| IL-10, pg/mL (n = 29) | rho | 0.228 | −0.084 | 0.554 | 0.571 | 0.468 | −0.043 | 0.218 | 0.007 | −0.002 | −0.100 |
| p | 0.264 | 0.684 | 0.003 | 0.002 | 0.016 | 0.836 | 0.284 | 0.974 | 0.994 | 0.627 | |
| IL-12, pg/mL | rho | 0.254 | −0.071 | 0.390 | 0.570 | 0.331 | 0.234 | 0.060 | −0.204 | −0.196 | 0.215 |
| p | 0.129 | 0.676 | 0.017 | 0.000 | 0.045 | 0.164 | 0.723 | 0.226 | 0.244 | 0.201 | |
| IL-18, pg/mL | rho | 0.426 | 0.042 | 0.587 | 0.547 | 0.562 | 0.380 | 0.261 | 0.022 | −0.121 | 0.268 |
| p | 0.009 | 0.804 | 0.000 | 0.000 | 0.000 | 0.020 | 0.119 | 0.899 | 0.474 | 0.109 | |
| IL-23, pg/mL | rho | 0.309 | 0.016 | 0.202 | 0.301 | 0.166 | 0.389 | 0.338 | −0.080 | −0.083 | 0.042 |
| p | 0.063 | 0.925 | 0.231 | 0.070 | 0.327 | 0.017 | 0.041 | 0.637 | 0.623 | 0.807 | |
| SH | rho | −0.198 | 0.044 | −0.352 | −0.356 | −0.337 | −0.200 | −0.267 | −0.320 | 0.163 | |
| p | 0.240 | 0.797 | 0.033 | 0.031 | 0.041 | 0.234 | 0.111 | 0.054 | 0.335 | ||
| TEWL, g/m2/h | rho | 0.280 | −0.012 | 0.214 | 0.158 | 0.215 | 0.277 | 0.205 | −0.225 | ||
| p | 0.094 | 0.942 | 0.203 | 0.349 | 0.200 | 0.097 | 0.223 | 0.181 | |||
| S. aureus Isolation | % of eosinophils in blood white cell counts (B = 0.083, p = 0.001), serum concentration of anti-SEB IgE (B = 0.027, p = 0.046) and TEWL (B = 0.224, p = 0.004) were positively and independently associated with S. aureus isolation. |
| S. epidermidis Isolation | Serum concentration of anti-SEB IgE (B = 0.033, p = 0.043) was positively associated with S. epidermidis isolation. |
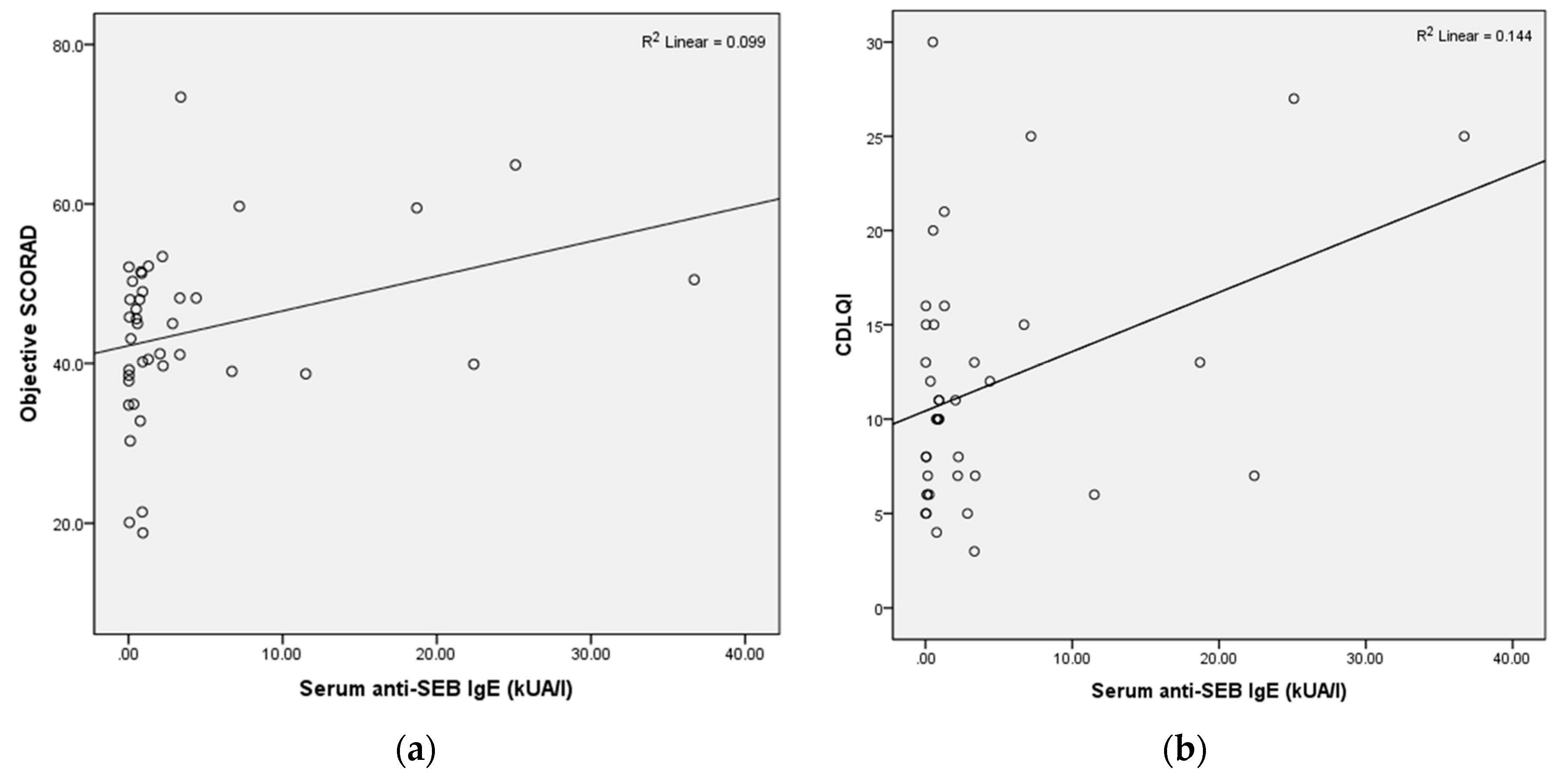
| Objective SCORAD | % of eosinophils in blood white cell counts (B = 0.843, p = 0.003), serum concentrations of anti-SEB IgE (B = 0.445, p = 0.007) and TNF-α (B = 4.935, p = 0.010) were positively and independently associated with objective SCORAD. |
| Extent | Serum concentrations of anti-SEB IgE (B = 0.554, p = 0.006) and IL-18 (B = 0.438, p = 0.001) were positively and independently associated with extent, while serum concentrations of TGF-β (B = −0.015, p = 0.001) and IL-23 (B = −2.812, p = 0.006), and SH (B = −0.605, p = 0.001) were negatively and independently associated with extent. |
| Intensity | Presence of personal asthma (B = 1.265, p = 0.044), % of eosinophils in blood white cell counts (B = 0.197, p = 0.004), serum concentration of anti-SEB IgE (B = 0.099, p = 0.012) and TEWL (B = 0.421, p = 0.040) were positively and independently associated with intensity. |
| Pruritus | S. aureus density (B = 0.815, p = 0.004) and S. epidermidis density (B = 0.709, p = 0.010), and serum concentration of IL-23 (B = 0.387, p = 0.007) were positively and independently associated with pruritus, while age of admission (B = −0.216, p < 0.0005) was negatively associated with pruritus. |
| Sleep Loss | S. epidermidis density (B = 1.478, p = 0.038) was positively associated with sleep loss, while age of admission (B = −0.392, p = 0.002) and presence of personal asthma (B = −2.386, p = 0.027) were negatively and independently associated with sleep loss.None of the studied blood markers were independently associated with sleep loss. |
| CDLQI | Presence of personal asthma (B = 3.441, p = 0.041), % of eosinophils in blood white cell counts (B = 0.482, p = 0.004) and serum concentration of anti-SEB IgE (B = 0.421, p < 0.0005) were positively and independently associated with CDLQI; while age of admission (B = −0.361, p = 0.050) and presence of personal allergic rhinitis (B = −9.269, p < 0.0005) were negatively and independently associated with CDLQI. |
| SH | None of the studied blood markers were independently associated with SH. |
| TEWL | Serum concentration of IL-18 (B = 0.040, p = 0.010) was positively associated with TEWL. |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hon, K.L.; Tsang, K.Y.C.; Kung, J.S.C.; Leung, T.F.; Lam, C.W.K.; Wong, C.K. Clinical Signs, Staphylococcus and Atopic Eczema-Related Seromarkers. Molecules 2017, 22, 291. https://doi.org/10.3390/molecules22020291
Hon KL, Tsang KYC, Kung JSC, Leung TF, Lam CWK, Wong CK. Clinical Signs, Staphylococcus and Atopic Eczema-Related Seromarkers. Molecules. 2017; 22(2):291. https://doi.org/10.3390/molecules22020291
Chicago/Turabian StyleHon, Kam Lun, Kathy Yin Ching Tsang, Jeng Sum C. Kung, Ting Fan Leung, Christopher W. K. Lam, and Chun Kwok Wong. 2017. "Clinical Signs, Staphylococcus and Atopic Eczema-Related Seromarkers" Molecules 22, no. 2: 291. https://doi.org/10.3390/molecules22020291