Dietary Phytoestrogen Intake is Inversely Associated with Hypertension in a Cohort of Adults Living in the Mediterranean Area

 ,
,
Abstract
:1. Introduction
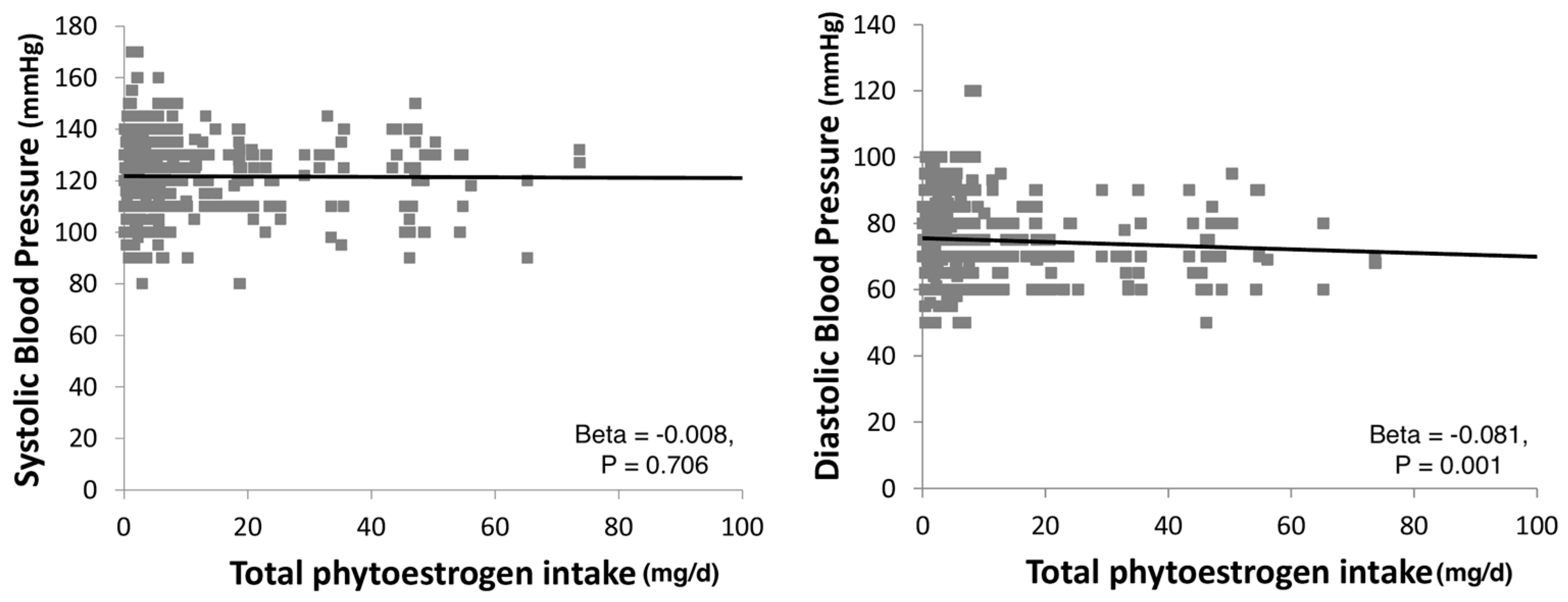
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Design and Population
4.2. Data Collection
4.3. Dietary Assessment
4.4. Estimation of Polyphenol Intake
4.5. Anthropometric Measurements and Outcome Ascertainment
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Grosso, G.; Godos, J.; Lamuela-Raventos, R.; Ray, S.; Micek, A.; Pajak, A.; Sciacca, S.; D’Orazio, N.; Rio, D.D.; Galvano, F. A comprehensive meta-analysis on dietary flavonoid and lignan intake and cancer risk: Level of evidence and limitations. Mol. Nutr. Food Res. 2016. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Micek, A.; Godos, J.; Pajak, A.; Sciacca, S.; Galvano, F.; Giovannucci, E.L. Dietary flavonoid and lignan intake and mortality in prospective cohort studies: Systematic review and dose-response meta-analysis. Am. J. Epidemiol. 2017, 185, 1304–1316. [Google Scholar] [CrossRef] [PubMed]
- Rietjens, I.; Louisse, J.; Beekmann, K. The potential health effects of dietary phytoestrogens. Br. J. Pharmacol. 2017, 174, 1263–1280. [Google Scholar] [CrossRef] [PubMed]
- Rietjens, I.M.; Sotoca, A.M.; Vervoort, J.; Louisse, J. Mechanisms underlying the dualistic mode of action of major soy isoflavones in relation to cell proliferation and cancer risks. Mol. Nutr. Food Res. 2013, 57, 100–113. [Google Scholar] [CrossRef] [PubMed]
- Gencel, V.B.; Benjamin, M.M.; Bahou, S.N.; Khalil, R.A. Vascular effects of phytoestrogens and alternative menopausal hormone therapy in cardiovascular disease. Mini Rev. Med. Chem. 2012, 12, 149–174. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Kuhnle, G.G.; Dell’Aquila, C.; Aspinall, S.M.; Runswick, S.A.; Mulligan, A.A.; Bingham, S.A. Phytoestrogen content of beverages, nuts, seeds, and oils. J. Agric. Food Chem. 2008, 56, 7311–7315. [Google Scholar] [CrossRef] [PubMed]
- Bai, W.; Wang, C.; Ren, C. Intakes of total and individual flavonoids by US adults. Int. J. Food Sci. Nutr. 2014, 65, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Ros, R.; Knaze, V.; Lujan-Barroso, L.; Kuhnle, G.G.; Mulligan, A.A.; Touillaud, M.; Slimani, N.; Romieu, I.; Powell, N.; Tumino, R.; et al. Dietary intakes and food sources of phytoestrogens in the European prospective investigation into cancer and nutrition (epic) 24-hour dietary recall cohort. Eur. J. Clin. Nutr. 2012, 66, 932–941. [Google Scholar] [CrossRef] [PubMed]
- Zappalà, G.; Buscemi, S.; Mulè, S.; La Verde, M.; D’Urso, M.; Corleo, D.; Marranzano, M. High adherence to Mediterranean diet, but not individual foods or nutrients, is associated with lower likelihood of being obese in a Mediterranean cohort. Eat. Weight Disord. 2017. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Sinatra, D.; Blanco, I.; Mule, S.; La Verde, M.; Marranzano, M. Association between dietary phenolic acids and hypertension in a mediterranean cohort. Nutrients 2017, 9, 1069. [Google Scholar] [CrossRef] [PubMed]
- Tse, G.; Eslick, G.D. Soy and isoflavone consumption and risk of gastrointestinal cancer: A systematic review and meta-analysis. Eur. J. Nutr. 2016, 55, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Jing, X.; Li, H.; Zhao, X.; Wang, D. Soy isoflavone consumption and colorectal cancer risk: A systematic review and meta-analysis. Sci. Rep. UK 2016, 6, 25939. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.; Chen, M.L.; Qin, Y.; Zhang, Q.Y.; Xu, H.X.; Zhou, Y.; Mi, M.T.; Zhu, J.D. Isoflavone consumption and risk of breast cancer: A dose-response meta-analysis of observational studies. Asia Pac. J. Clin. Nutr. 2013, 22, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.X.; Li, S.H.; Chen, J.Z.; Sun, K.; Wang, X.J.; Wang, X.G.; Hui, R.T. Effect of soy isoflavones on blood pressure: A meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Taku, K.; Lin, N.; Cai, D.; Hu, J.; Zhao, X.; Zhang, Y.; Wang, P.; Melby, M.K.; Hooper, L.; Kurzer, M.S.; et al. Effects of soy isoflavone extract supplements on blood pressure in adult humans: Systematic review and meta-analysis of randomized placebo-controlled trials. J. Hypertens. 2010, 28, 1971–1982. [Google Scholar] [CrossRef] [PubMed]
- Khosravi-Boroujeni, H.; Nikbakht, E.; Natanelov, E.; Khalesi, S. Can sesame consumption improve blood pressure? A systematic review and meta-analysis of controlled trials. J. Sci. Food Agric. 2017. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A.; Soranna, D.; Liu, X.; Thomopoulos, C.; Simental-Mendia, L.E.; Derosa, G.; Maffioli, P.; Parati, G. A systematic review and meta-analysis of randomized controlled trials investigating the effects of supplementation with nigella sativa (black seed) on blood pressure. J. Hypertens. 2016, 34, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Khalesi, S.; Irwin, C.; Schubert, M. Flaxseed consumption may reduce blood pressure: A systematic review and meta-analysis of controlled trials. J. Nutr. 2015, 145, 758–765. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.; Dwyer, J.; Adlercreutz, H.; Scalbert, A.; Jacques, P.; McCullough, M.L. Dietary lignans: Physiology and potential for cardiovascular disease risk reduction. Nutr. Rev. 2010, 68, 571–603. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Estruch, R. Nut consumption and age-related disease. Maturitas 2016, 84, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Pluchinotta, F.R.; Marventano, S.; Buscemi, S.; Li Volti, G.; Galvano, F.; Grosso, G. Coffee components and cardiovascular risk: Beneficial and detrimental effects. Int. J. Food Sci. Nutr. 2014, 65, 925–936. [Google Scholar] [CrossRef] [PubMed]
- Ramdath, D.D.; Padhi, E.M.; Sarfaraz, S.; Renwick, S.; Duncan, A.M. Beyond the cholesterol-lowering effect of soy protein: A review of the effects of dietary soy and its constituents on risk factors for cardiovascular disease. Nutrients 2017, 9, 324. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.; Zhang, X.; Li, C.; Jiao, S.; Dong, W. Association between consumption of soy and risk of cardiovascular disease: A meta-analysis of observational studies. Eur. J. Prev. Cardiol. 2017, 24, 735–747. [Google Scholar] [CrossRef] [PubMed]
- Guo, K.; Zhou, Z.; Jiang, Y.; Li, W.; Li, Y. Meta-analysis of prospective studies on the effects of nut consumption on hypertension and type 2 diabetes mellitus. J. Diabetes 2015, 7, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Yang, J.; Marventano, S.; Micek, A.; Galvano, F.; Kales, S.N. Nut consumption on all-cause, cardiovascular, and cancer mortality risk: A systematic review and meta-analysis of epidemiologic studies. Am. J. Clin. Nutr. 2015, 101, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Afshin, A.; Micha, R.; Khatibzadeh, S.; Mozaffarian, D. Consumption of nuts and legumes and risk of incident ischemic heart disease, stroke, and diabetes: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Marventano, S.; Izquierdo Pulido, M.; Sanchez-Gonzalez, C.; Godos, J.; Speciani, A.; Galvano, F.; Grosso, G. Legume consumption and cvd risk: A systematic review and meta-analysis. Public Health Nutr. 2017, 20, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Micek, A.; Godos, J.; Sciacca, S.; Pajak, A.; Martinez-Gonzalez, M.A.; Giovannucci, E.L.; Galvano, F. Coffee consumption and risk of all-cause, cardiovascular, and cancer mortality in smokers and non-smokers: A dose-response meta-analysis. Eur. J. Epidemiol. 2016, 31, 1191–1205. [Google Scholar] [CrossRef] [PubMed]
- Steffen, M.; Kuhle, C.; Hensrud, D.; Erwin, P.J.; Murad, M.H. The effect of coffee consumption on blood pressure and the development of hypertension: A systematic review and meta-analysis. J. Hypertens. 2012, 30, 2245–2254. [Google Scholar] [CrossRef] [PubMed]
- Kreijkamp-Kaspers, S.; Kok, L.; Bots, M.L.; Grobbee, D.E.; van der Schouw, Y.T. Dietary phytoestrogens and vascular function in postmenopausal women: A cross-sectional study. J. Hypertens. 2004, 22, 1381–1388. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Stepaniak, U.; Micek, A.; Stefler, D.; Bobak, M.; Pajak, A. Dietary polyphenols are inversely associated with metabolic syndrome in polish adults of the hapiee study. Eur. J. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Marventano, S.; Mistretta, A.; Galvano, F.; Grosso, G. Dietary sources of polyphenols in the mediterranean healthy eating, aging and lifestyle (meal) study cohort. Int. J. Food Sci. Nutr. 2017, 68, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Marventano, S.; Godos, J.; Platania, A.; Galvano, F.; Mistretta, A.; Grosso, G. Mediterranean diet adherence in the mediterranean healthy eating, aging and lifestyle (meal) study cohort. Int. J. Food Sci. Nutr. 2017, 69, 100–107. [Google Scholar] [CrossRef] [PubMed]
- La Verde, M.; Mule, S.; Zappala, G.; Privitera, G.; Maugeri, G.; Pecora, F.; Marranzano, M. Higher adherence to the mediterranean diet is inversely associated with having hypertension: Is low salt intake a mediating factor? Int. J. Food Sci. Nutr. 2017, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Rapisarda, G.; Marventano, S.; Galvano, F.; Mistretta, A.; Grosso, G. Association between polyphenol intake and adherence to the mediterranean diet in sicily, southern italy. NFS J. 2017, 8, 1–7. [Google Scholar] [CrossRef]
- Hall, W.L.; Rimbach, G.; Williams, C.M. Isoflavones and endothelial function. Nutr. Res. Rev. 2005, 18, 130–144. [Google Scholar] [CrossRef] [PubMed]
- Santhakumar, A.B.; Bulmer, A.C.; Singh, I. A review of the mechanisms and effectiveness of dietary polyphenols in reducing oxidative stress and thrombotic risk. J. Hum. Nutr. Diet. 2014, 27, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Prasad, K. Flaxseed and cardiovascular health. J. Cardiovasc. Pharmacol. 2009, 54, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Adlercreutz, H. Lignans and human health. Crit. Rev. Clin. Lab. Sci. 2007, 44, 483–525. [Google Scholar] [CrossRef] [PubMed]
- Hallmans, G.; Zhang, J.X.; Lundin, E.; Stattin, P.; Johansson, A.; Johansson, I.; Hulten, K.; Winkvist, A.; Aman, P.; Lenner, P.; et al. Rye, lignans and human health. Proc. Nutr. Soc. 2003, 62, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Fuller, S.; Beck, E.; Salman, H.; Tapsell, L. New horizons for the study of dietary fiber and health: A review. Plant Foods Hum. Nutr. 2016, 71, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Marventano, S.; Kolacz, P.; Castellano, S.; Galvano, F.; Buscemi, S.; Mistretta, A.; Grosso, G. A review of recent evidence in human studies of n-3 and n-6 pufa intake on cardiovascular disease, cancer, and depressive disorders: Does the ratio really matter? Int. J. Food Sci. Nutr. 2015, 66, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Marventano, S.; D’Urso, M.; Mistretta, A.; Galvano, F. The mediterranean healthy eating, ageing, and lifestyle (meal) study: Rationale and study design. Int. J. Food Sci. Nutr. 2017, 68, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Buscemi, S.; Rosafio, G.; Vasto, S.; Massenti, F.M.; Grosso, G.; Galvano, F.; Rini, N.; Barile, A.M.; Maniaci, V.; Cosentino, L.; et al. Validation of a food frequency questionnaire for use in italian adults living in sicily. Int. J. Food Sci. Nutr. 2015, 66, 426–438. [Google Scholar] [CrossRef] [PubMed]
- Marventano, S.; Mistretta, A.; Platania, A.; Galvano, F.; Grosso, G. Reliability and relative validity of a food frequency questionnaire for Italian adults living in Sicily, southern Italy. Int. J. Food Sci. Nutr. 2016, 67, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Istituto Nazionale di Ricerca per gli Alimenti e la Nutrizione. Tabelle di Composizione Degli Alimenti; INRAN: Rome, Italy, 2009. [Google Scholar]
- Platania, A.; Zappala, G.; Mirabella, M.U.; Gullo, C.; Mellini, G.; Beneventano, G.; Maugeri, G.; Marranzano, M. Association between Mediterranean diet adherence and dyslipidaemia in a cohort of adults living in the Mediterranean area. Int. J. Food Sci. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Neveu, V.; Perez-Jiménez, J.; Vos, F.; Crespy, V.; Du Chaffaut, L.; Mennen, L.; Knox, C.; Eisner, R.; Cruz, J.; Wishart, D.; et al. Phenol-Explorer: An Online Comprehensive Database on Polyphenol Contents in Foods. Database 2010. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, J.A.; Perez-Jimenez, J.; Neveu, V.; Medina-Remon, A.; M’Hiri, N.; Garcia-Lobato, P.; Manach, C.; Knox, C.; Eisner, R.; Wishart, D.S.; et al. Phenol-explorer 3.0: A major update of the phenol-explorer database to incorporate data on the effects of food processing on polyphenol content. Database J. Biol. Databases Curation 2013, 2013, bat070. [Google Scholar] [CrossRef] [PubMed]
- Bognar, A. Tables on Weight Yield of Food and Retention Factors of Food Constituents for the Calculation of Nutrient Composition of Cooked Foods (Dishes); BFE: Karlsruhe, Germany, 2002. [Google Scholar]
- Willett, W.; Lenart, E. Reproducibility and validity of food frequency questionnaire. In Nutritional Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Mistretta, A.; Marventano, S.; Platania, A.; Godos, J.; Galvano, F.; Grosso, G. Metabolic profile of the mediterranean healthy eating, lifestyle and aging (meal) study cohort. Mediterr. J. Nutr. Metab. 2017, 10, 131–140. [Google Scholar] [CrossRef]
Sample Availability: Samples of the compounds are not available from the authors. |


{kind=link}
| Total Phytoestrogens Intake | p | ||||
|---|---|---|---|---|---|
| Q1 (Median = 258.56) | Q2 (Median = 432.43) | Q3 (Median = 604.97) | Q4 (Median = 1054.63) | ||
| Age (years), mean (SD) | 47.9 (18.7) | 49.4 (17.2) | 49.5 (17.6) | 46.7 (16.7) | 0.040 |
| Sex, n (%) | 0.011 | ||||
| Male | 190 (23.6) | 224 (27.9) | 217 (27.0) | 173 (21.5) | |
| Female | 272 (24) | 271 (23.9) | 276 (24.4) | 313 (27.7) | |
| Educational level, n (%) | 0.434 | ||||
| Low | 161 (23.1) | 168 (24.1) | 188 (27.0) | 180 (25.8) | |
| Medium | 168 (23.3) | 195 (27.1) | 188 (26.1) | 169 (23.5) | |
| High | 133 (25.6) | 132 (25.4) | 117 (22.5) | 137 (26.4) | |
| Occupational level, n (%) | 0.001 | ||||
| Unemployed | 109 (23.6) | 85 (18.4) | 121 (26.2) | 146 (31.7) | |
| Low | 51 (19.2) | 57 (21.4) | 88 (33.1) | 70 (26.3) | |
| Medium | 109 (24.8) | 119 (27.0) | 113 (25.7) | 99 (22.5) | |
| High | 131 (26.7) | 125 (25.5) | 131 (27.3) | 104 (25.3) | |
| Smoking status, n (%) | 0.014 | ||||
| Non smoker | 270 (22.6) | 296 (24.8) | 301 (25.2) | 328 (27.4) | |
| Ex-smoker | 121 (26.0) | 121 (26.0) | 111 (23.9) | 112 (24.1) | |
| Current smoker | 71 (25.7) | 78 (28.3) | 81 (29.3) | 46 (16.7) | |
| Physical activity, n (%) | <0.001 | ||||
| Low | 89 (27.1) | 55 (16.7) | 83 (25.2) | 102 (31.0) | |
| Medium | 221 (25.8) | 238 (27.8) | 175 (20.4) | 222 (25.9) | |
| High | 97 (17.9) | 159 (29.3) | 165 (30.4) | 122 (22.5) | |
| Alcohol consumption, n (%) | <0.001 | ||||
| No | 97 (25.9) | 95 (25.3) | 84 (22.4) | 99 (26.4) | |
| Moderate (<12 g/d) | 311 (25.8) | 303 (25.1) | 334 (27.7) | 258 (21.4) | |
| Regular (≥12 g/d) | 54 (15.2) | 97 (27.2) | 75 (21.1) | 130 (36.5) | |
| Na (microg/d), mean ± SD | 2724.6 ± 1155.7 | 2869.9 ± 1045.8 | 2870.8 ± 1060.4 | 2947.8 ± 1147.3 | 0.021 |
| K (microg/d), mean ± SD | 2920.4 ± 897.0 | 3269.6 ± 941.2 | 3915.5 ± 1068.3 | 4589.9 ± 1806.8 | <0.001 |
| Systolic blood pressure (mmHg), mean ± SD | 122.1 ± 12.9 | 121.3 ± 12.4 | 121.4 ± 12.2 | 121.5 ± 13.8 | 0.723 |
| Diastolic blood pressure (mmHg), mean ± SD | 76.1 ± 9.9 | 75.7 ± 9.9 | 75.1 ± 10.3 | 73.4 ± 11.2 | <0.001 |
| OR (95% CI) | ||||
|---|---|---|---|---|
| Polyphenols (mg/d) | Q1 | Q2 | Q3 | Q4 |
| Total phytoestrogens, median (range) | 0.89 (0.20, 1.23) | 1.77 (1.24, 2.33) | 3.61 (2.33, 5.41) | 10.21 (5.42, 101.72) |
| No. of cases | 247 | 260 | 257 | 212 |
| Model a | 1 | 0.85 (0.63, 1.14) | 0.79 (0.58, 1.07) | 0.68 (0.49, 0.96) |
| Model b | 1 | 0.87 (0.61, 1.26) | 0.69 (0.47, 1.00) | 0.66 (0.44, 0.98) |
| Isoflavones, median (range) | 0.01 (0.00, 0.01) | 0.03 (0.01, 0.04) | 0.07 (0.05, 0.08) | 5.53 (0.09, 92.98) |
| No. of cases | 240 | 267 | 265 | 204 |
| Model a | 1 | 0.97 (0.72, 1.31) | 0.87 (0.64, 1.17) | 0.96 (0.69, 1.34) |
| Model b | 1 | 0.81 (0.56, 1.15) | 0.94 (0.65, 1.35) | 0.93 (0.64, 1.36) |
| Daidzein, median (range) | 0.01 (0.00, 0.01) | 0.02 (0.01, 0.02) | 0.04 (0.03, 0.05) | 0.14 (0.05, 6.49) |
| Model a | 1 | 1.14 (0.84, 1.55) | 1.03 (0.76, 1.40) | 0.94 (0.68, 1.29) |
| Model b | 1 | 0.95 (0.66, 1.36) | 1.05 (0.73, 1.52) | 1.03 (0.70, 1.51) |
| Genistein, median (range) | 0.00 (0.00, 0.00) | 0.01 (0.00, 0.01) | 0.02 (0.01, 0.02) | 0.14 (0.02, 7.77) |
| Model a | 1 | 1.23 (0.91, 1.65) | 1.04 (0.76, 1.42) | 0.99 (0.72, 1.36) |
| Model b | 1 | 1.05 (0.73, 1.49) | 1.08 (0.73, 1.58) | 1.07 (0.73, 1.57) |
| Biochanin A, median (range) | 0.00 (0.00, 0.00) | 0.36 (0.10, 0.50) | 0.95 (0.70, 1.70) | 2.50 (1.80, 34.3) |
| Model a | 1 | 0.99 (0.72, 1.35) | 1.24 (0.91, 1.69) | 0.63 (0.46, 0.87) |
| Model b | 1 | 0.99 (0.65, 1.48) | 0.99 (0.66, 1.50) | 0.63 (0.41, 0.96) |
| Lignans, median (range) | 0.71 (0.00, 1.07) | 1.41 (1.07, 1.99) | 2.46 (2.00, 3.62) | 5.41 (3.63, 23.56) |
| No. of cases | 225 | 232 | 275 | 244 |
| Model a | 1 | 0.66 (0.49, 0.89) | 1.14 (0.83, 1.56) | 0.77 (0.55, 1.09) |
| Model b | 1 | 0.59 (0.41, 0.86) | 0.88 (0.61, 1.27) | 0.71 (0.47, 1.08) |
| Lariciresinol, median (range) | 0.25 (0.00, 0.48) | 0.69 (0.48, 1.06) | 1.23 (1.06, 2.00) | 3.11 (2.01, 13.98) |
| Model a | 1 | 0.65 (0.48, 0.88) | 1.03 (0.76, 1.40) | 0.79 (0.56, 1.10) |
| Model b | 1 | 0.60 (0.41, 0.86) | 0.84 (0.58, 1.21) | 0.69 (0.46, 1.03) |
| Matairesinol, median (range) | 0.00 (0.00, 0.01) | 0.01 (0.01, 0.02) | 0.02 (0.02, 0.04) | 0.06 (0.04, 0.30) |
| Model a | 1 | 1.00 (0.74, 1.35) | 1.47 (1.07, 2.01) | 1.03 (0.73, 1.44) |
| Model b | 1 | 0.95 (0.65, 1.37) | 1.08 (0.74, 1.58) | 0.91 (0.60, 1.38) |
| Pinoresinol, median (range) | 0.31 (0.00, 0.41) | 0.52 (0.41, 0.70) | 0.87 (0.70, 1.24) | 1.75 (1.25, 7.30) |
| Model a | 1 | 0.62 (0.46, 0.85) | 0.94 (0.68, 1.29) | 0.65 (0.46, 0.92) |
| Model b | 1 | 0.58 (0.40, 0.84) | 0.79 (0.54, 1.16) | 0.59 (0.39, 0.89) |
| Secoisolariciresinol, median (range) | 0.03 (0.00, 0.05) | 0.06 (0.05, 0.08) | 0.11 (0.08, 0.14) | 0.21 (0.14, 0.90) |
| Model a | 1 | 0.78 (0.58, 1.06) | 1.11 (0.80, 1.53) | 0.80 (0.56, 1.14) |
| Model b | 1 | 0.73 (0.51, 1.06) | 0.88 (0.60, 1.30) | 0.69 (0.44, 1.06) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Godos, J.; Bergante, S.; Satriano, A.; Pluchinotta, F.R.; Marranzano, M. Dietary Phytoestrogen Intake is Inversely Associated with Hypertension in a Cohort of Adults Living in the Mediterranean Area. Molecules 2018, 23, 368. https://doi.org/10.3390/molecules23020368
Godos J, Bergante S, Satriano A, Pluchinotta FR, Marranzano M. Dietary Phytoestrogen Intake is Inversely Associated with Hypertension in a Cohort of Adults Living in the Mediterranean Area. Molecules. 2018; 23(2):368. https://doi.org/10.3390/molecules23020368
Chicago/Turabian StyleGodos, Justyna, Sonia Bergante, Angela Satriano, Francesca Romana Pluchinotta, and Marina Marranzano. 2018. "Dietary Phytoestrogen Intake is Inversely Associated with Hypertension in a Cohort of Adults Living in the Mediterranean Area" Molecules 23, no. 2: 368. https://doi.org/10.3390/molecules23020368