Hepatic Mitochondrial Redox Potential in Patients with Liver Metastatic Cancers and Circulatory Insufficiency

Abstract
:Introduction

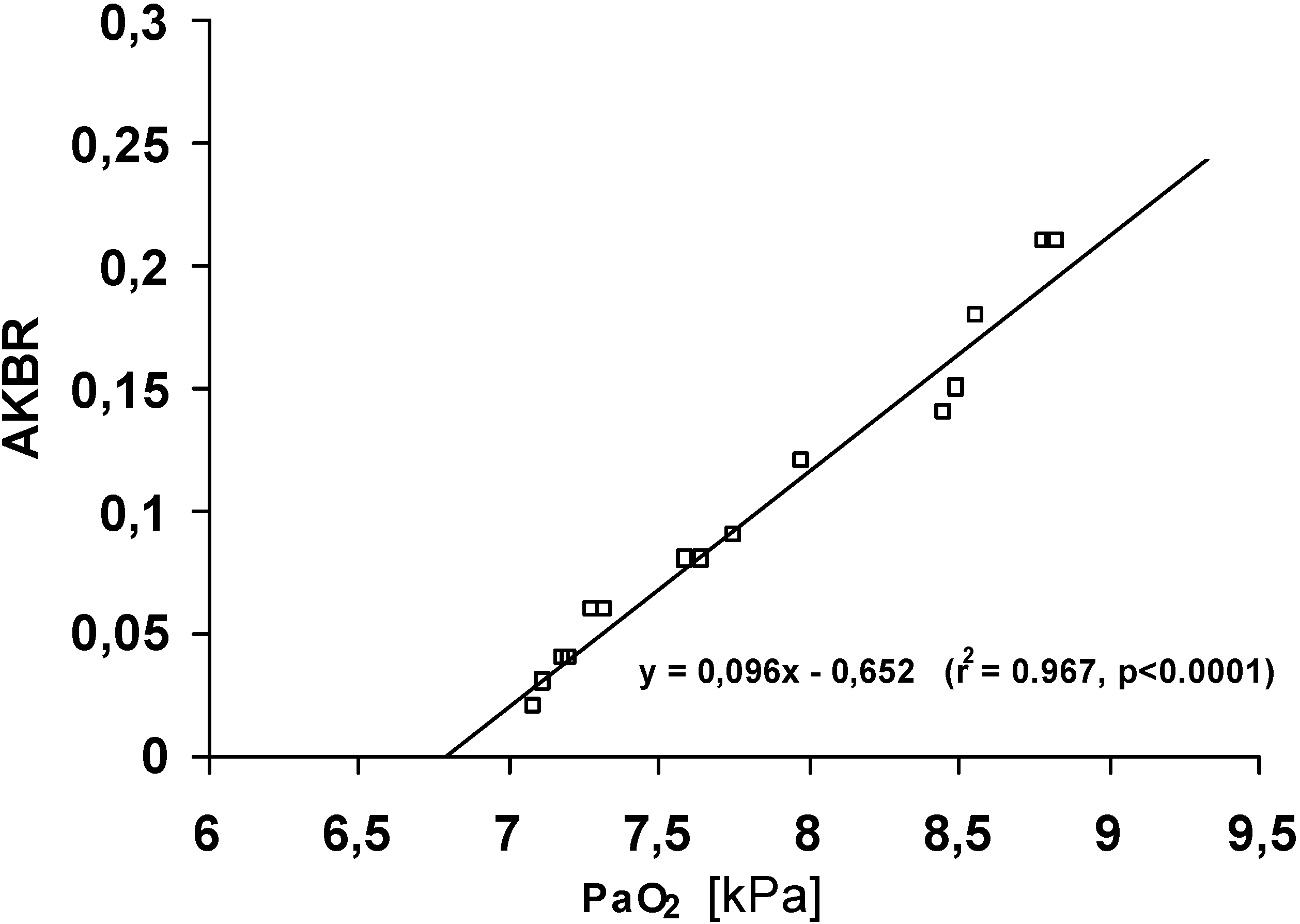
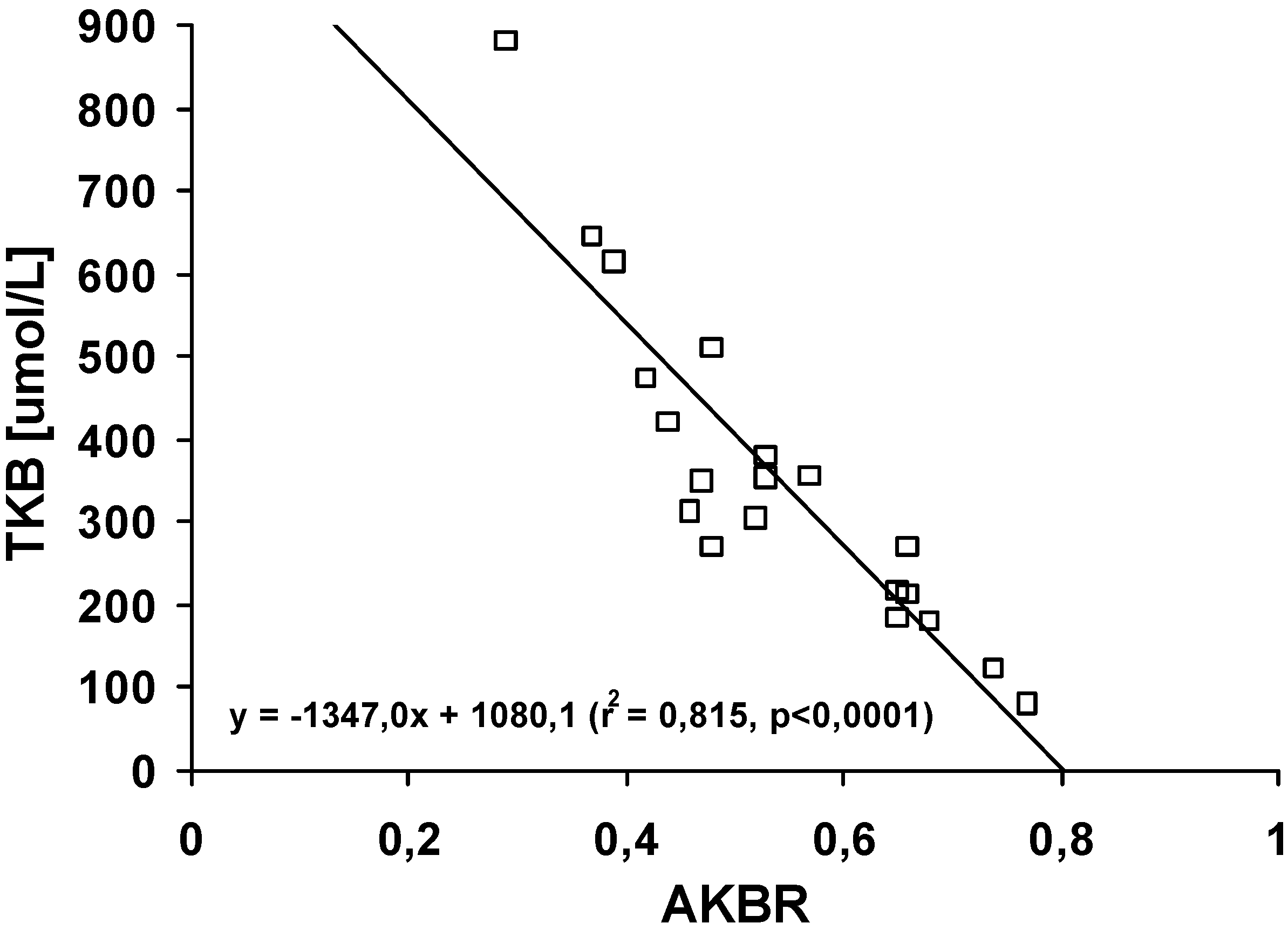
Results and Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A | Group B | |
| Diagnosis | Carcinoma hepatis metastaticum and good circulatory condition | Carcinoma hepatis metastaticum and chronic cardiogenic circulatory insufficiency |
| Number of patients | N = 20 | n = 16 |
| Age interval | 31-71 years | 39-72 years |
| Sex (female/male) | 11/9 | 7/9 |
| AKBR | 0.54 ± 0.03 | 0.10 ± 0.02 |
| TKB [μmol/L] | 355.40 ± 43.55 | 430.00 ± 61.25 |
| PaO2 [kPa] | 11.0 ± 0.3 | 7.9 ± 0.2 |



Conclusions
Experimental
References
- Chapman, M.J.; Miller, L.R.; Ontro, T.A. Localization of the Enzymes of Ketogenesis in Rat Liver Mitochondria. J. Cell. Biol. 1973, 58, 284–306. [Google Scholar]
- Couinaud, C. Distribution de l’artére hépapique dans le foie. Acta Anat. 1954, 22, 49–81. [Google Scholar]
- Gubernatis, G.; Bornscheuer, A.; Taki, Y.; Farle, M.; Lübbe, N.; Yamaoka, Y.; Beneking, M.; Burdelski, M.; Oellerich, M. Total Oxygen Consumption Ketone Body Ratio and a Special Score as Early Indications of Irreversible Liver Allograft Dysfunction. Transplant. Proc. 1989, 21, 2279–2281. [Google Scholar]
- Gutiérrez-Salinas, J.; Miranda-Garduño, L.; Trejo-Izquierdo, E.; Díaz-Muñoz, M.; Vidrio, S.; Morales-Gonzáles, J. A.; Hernández-Muñoz, R. Redox State and Energy Metabolism during Liver Regeneration. Alterations Produced by Acute Ethanol Administration. Biochem. Pharmacol. 1999, 58, 1831–1839. [Google Scholar]
- Iwata, S.; Ozawa, K.; Shimahara, Y.; Mori, K.; Kobayashi, N.; Kumada, K.; Yamaoka, Y. Diurnal Fluctuations of Arterial Ketone Body Ratio in Normal Subjects and Patients with Liver Dysfunction. Gastroenterology 1991, 100, 1371–1378. [Google Scholar]
- Katsuyama, K.; Ozawa, K. M.; Morikawa, S.; Iwata, S.; Mori, A. Myocardial High-energy Phosphates and Hepatic Redox State in Jaundiced Rats. J. Surg. Res. 1999, 82, 88–94. [Google Scholar]
- Kiyama, H. Significance of Arterial Ketone Body Ratio as a Parameter of Oxygen Metabolism in Cardiac Surgery. Nippon Kyobu Geka Gekkai Zasshi 1997, 45, 1525–1531. [Google Scholar]
- Ozawa, K.; Aoyama, H.; Yasuda, K.; Shimahara, Y.; Nakatani, T.; Tanaka, J.; Yamamoto, M.; Kamiyama, Y.; Tobe, T. Metabolic Abnormalities Associated with Postoperative Organ Failure. A Redox Theory. Arch. Surg. 1983, 118, 1245–1251. [Google Scholar]
- Pardela, M. S.; Lemiszewski, A. Prognostic Value of Arterial Ketone Body Ratio (AKBR) in Evaluation of The Early Liver Survival After Transplantation or Extend Hepatectomy in Adults. Med. Sci. Monit. 1999, 5, 585–590. [Google Scholar]
- Pszenny, C.; Krawczyk, M.; Paluszkiewicz, R.; Hevelke, P.; Zieniewicz, K.; Grzelak, I.; Tomaszewski, P.; Kuczyńska, J.; Pachecka, J. Biochemical Function of the Donor Liver in Living Related Liver Transplantation. Transplant. Proc. 2002, 34, 621–622. [Google Scholar]
- Shimahara, Y.; Yamamoto, N.; Kobayashi, N.; Ozawa, K. Surgical Nutrition: Strategies in Critically Ill Patients; Latifi, R., Dudrick, S.J., Eds.; Springer-Verlag: New York, 1995; p. 171. [Google Scholar]
- Takahashi, M.; Ueda, K.; Tabata, R.; Iwata, S.; Ozawa, K.; Uno, S.; Kinoshita, M. Arterial Ketone Body Ratio as a Prognostic Indicator in Acute Heart Failure. J. Lab. Clin. Med. 1997, 129, 72–80. [Google Scholar]
- Tomaszewski, P.; Kubiak, G.; Pachecka, J. Hepatic Mitochondrial Redox Potential in Patients with Liver Cancers. Fol. Histochem. Cytobiol. 1999, 37 suppl.1, 17. [Google Scholar]
- Uno, S.; Ito, S.; Kurono, M.; Yamaoka, Y.; Kamiyama, Y.; Ozawa, K. A Simple and Sensitive Assay for Blood Ketone Bodies Using Highly Purified 3-Hydroxybutyrate Dehydrogenase. Clin. Chim. Acta 1987, 168, 253–255. [Google Scholar]
- Williamson, D. H.; Lund, P.; Krebs, H. A. The Redox State of Free Nicotinamide Adenine Dinucleotide in The Cytoplasm and Mitochondria of Rat Liver. Biochem. J. 1967, 103, 514–527. [Google Scholar]
- Williamson, D.H.; Mellanby, J.; Krebs, H. Enzymatic Determination of D-(-)-β-hydroxybutyric Acid and Acetoacetic Acid in Blood. Biochem. J. 1962, 82, 90–96. [Google Scholar]
© 2003 by MDPI ( http://www.mdpi.org). Reproduction is permitted for noncommercial purposes.
Share and Cite
Tomaszewski, P.; Kubiak-Tomaszewska, G.; Pachecka, J.; Balcerzak, M.; Haznar, B.; Pszenny, C.; Krawczyk, M.; Paczkowski, P.; Jarecki, M. Hepatic Mitochondrial Redox Potential in Patients with Liver Metastatic Cancers and Circulatory Insufficiency. Molecules 2003, 8, 146-152. https://doi.org/10.3390/80100146
Tomaszewski P, Kubiak-Tomaszewska G, Pachecka J, Balcerzak M, Haznar B, Pszenny C, Krawczyk M, Paczkowski P, Jarecki M. Hepatic Mitochondrial Redox Potential in Patients with Liver Metastatic Cancers and Circulatory Insufficiency. Molecules. 2003; 8(1):146-152. https://doi.org/10.3390/80100146
Chicago/Turabian StyleTomaszewski, Piotr, Grazyna Kubiak-Tomaszewska, Jan Pachecka, Marcin Balcerzak, Bozena Haznar, Cezary Pszenny, Marek Krawczyk, Pawel Paczkowski, and Marek Jarecki. 2003. "Hepatic Mitochondrial Redox Potential in Patients with Liver Metastatic Cancers and Circulatory Insufficiency" Molecules 8, no. 1: 146-152. https://doi.org/10.3390/80100146