Candida Colonization Index in Patients Admitted to an ICU

Abstract
:1. Introduction
2. Materials and Methods
2.1. Microbiological Methods
2.2. Definitions
2.3. Statistical Investigation
3. Results
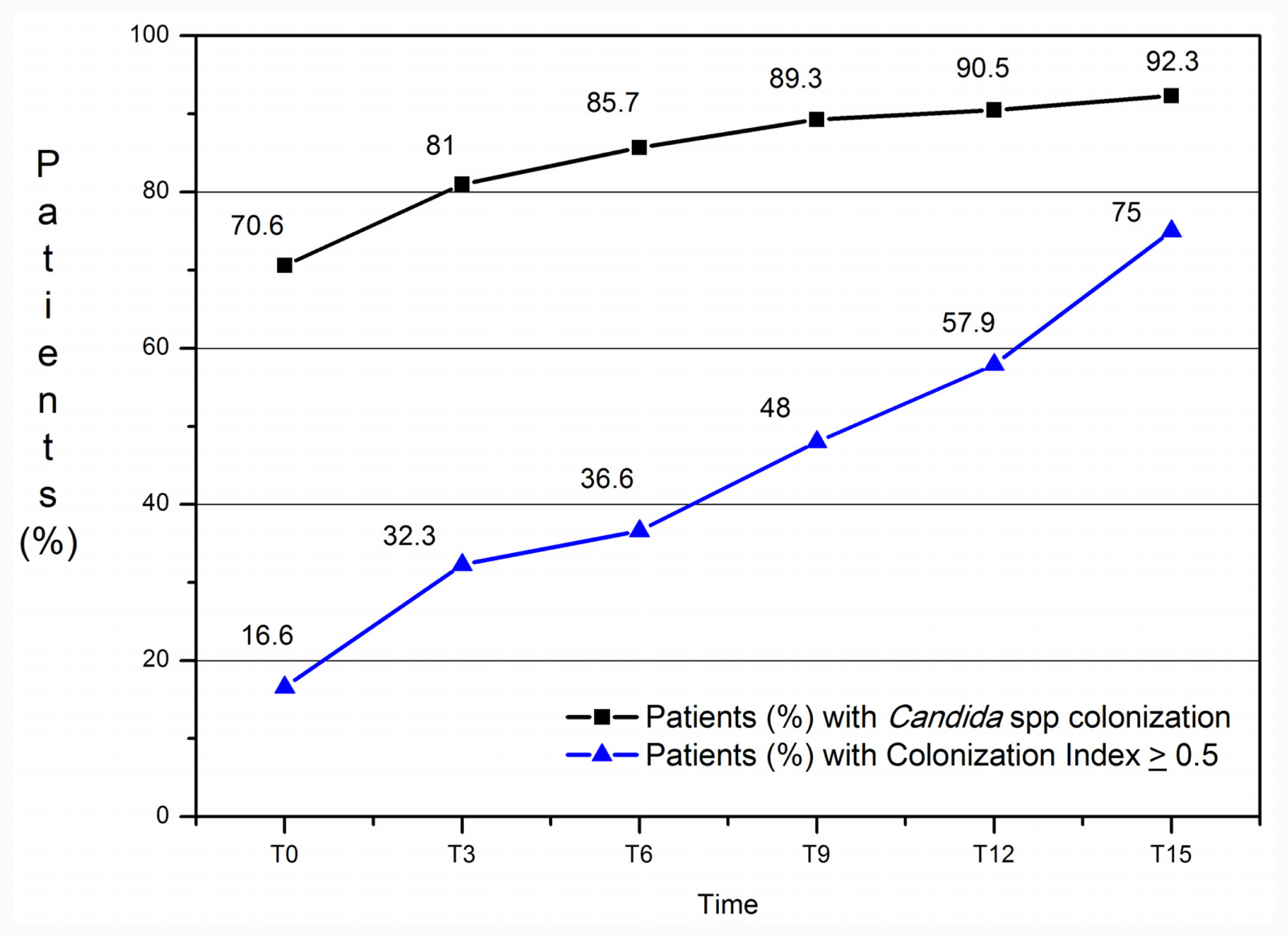
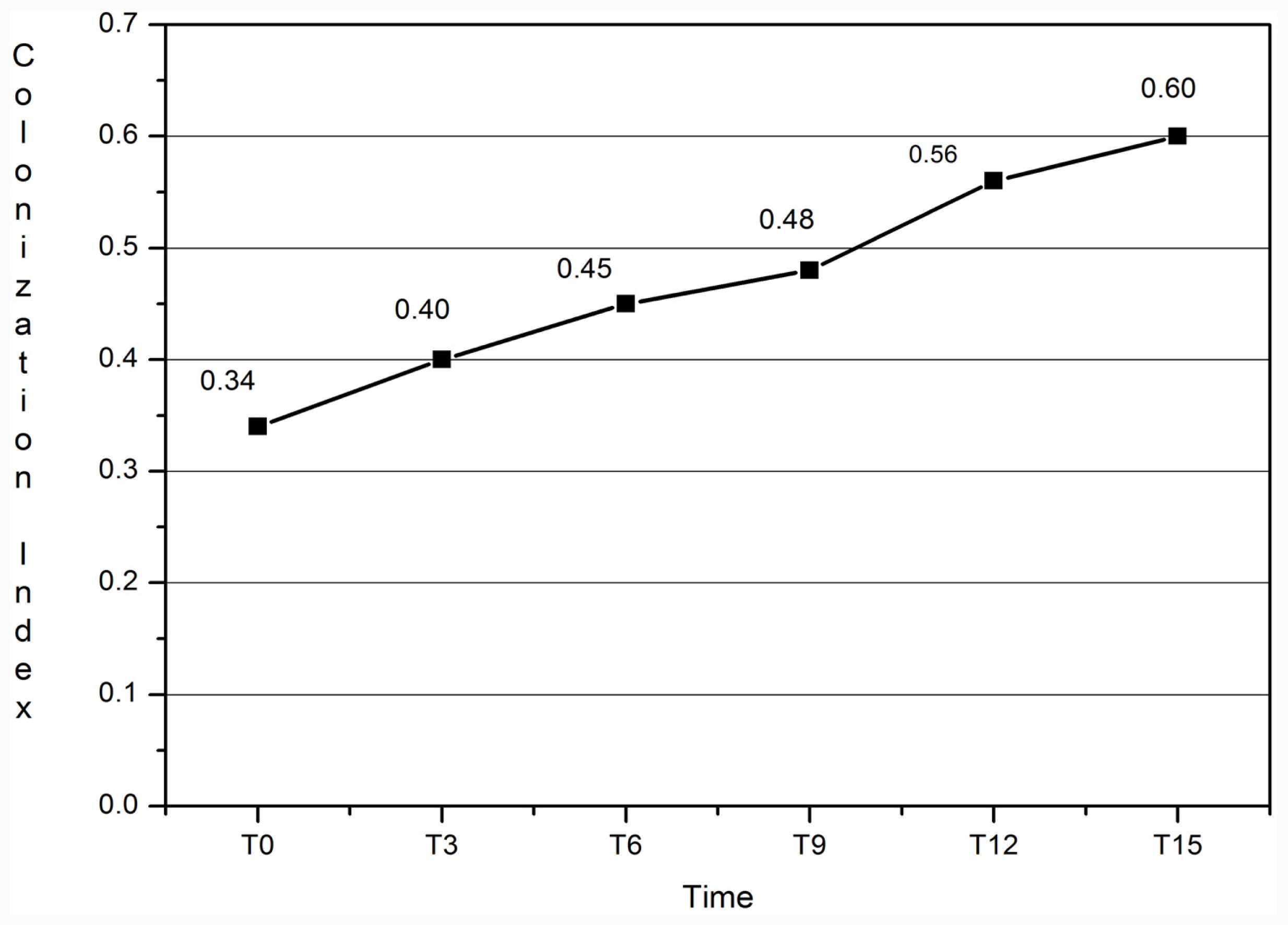
3.1. Colonization Index
3.2. Candida Mannan Antigen and Anti-Mannan Antibodies
4. Discussion
5. Conclusions
- Conflict of InterestThe authors declare no conflict of interest.
References
- Caggiano, G; Iatta, R; Laneve, A; Manca, F; Montagna, MT. Observational study on candidaemia at a university hospital in southern Italy from 1998 to 2004. Mycoses 2008, 51, 123–128. [Google Scholar]
- Zaoutis, TE; Prasad, PA; Localio, AR; Coffin, SE; Bell, LM; Walsh, TJ; Gross, R. Risk factors and predictors for candidemia in pediatric intensive care unit patients: implications for prevention. Clin. Infect. Dis 2010, 51, 38–45. [Google Scholar]
- Pfaller, MA; Diekema, DJ. Epidemiology of invasive candidiasis: A persistent public health problem. Clin. Microbiol. Rev 2007, 20, 133–163. [Google Scholar]
- Bouza, E; Munoz, P. Epidemiology of candidemia in intensive care units. Int J Antimicrob Agents 2008, 3(2), 87–91. [Google Scholar]
- Eggimann, P; Garbino, J; Pittet, D. Epidemiology of Candida species infections in critically ill non immunosuppressed patients. Lancet Infect. Dis 2003, 3, 685–702. [Google Scholar]
- Klempp-Selb, B; Rimek, D; Kappe, R. Karyotiping of Candida albicans and Candida glabrata from patients with Candida sepsis. Mycoses 2000, 43, 159–163. [Google Scholar]
- Singhi, S; Rao, DS; Chakrabarti, A. Candida colonization and candidemia in a pediatric intensive care unit. Pediatr. Crit. Care Med 2008, 9, 91–95. [Google Scholar]
- Ruping, MJ; Vehreschild, JJ; Cornely, OA. Patients at high risk of invasive fungal infection: when and how to treat. Drugs 2008, 68, 1941–1962. [Google Scholar]
- Wey, SB; Mori, M; Pfaller, MA; Woolson, RF; Wenzel, RP. Risk factors for hospital-acquired candidemia. A matched case-control study. Arch. Int. Med 1989, 149, 2349–2353. [Google Scholar]
- Agvald-Ohman, C; Klingspor, L; Hjelmqvist, H; Edlund, C. Invasive candidiasis in long-term patients at a multidisciplinary intensive care unit: Candida colonization index, risk factors, treatment and outcome. Scand. J. Infect. Dis 2008, 40, 145–153. [Google Scholar]
- Almirante, B; Rodríguez, D; Park, BJ; Cuenca-Estrella, M; Planes, AM; Almela, M; Mensa, J; Sanchez, F; Ayats, J; Gimenez, M; et al. Epidemiology and predictors of mortality in cases of Candida bloodstream infection: Results from population-based surveillance, Barcelona, Spain, from 2002 to 2003. J. Clin. Microbial 2005, 43, 1829–1835. [Google Scholar]
- Charles, PE; Dalle, F; Aube, H; Doise, JM; Quenot, JP; Aho, LS; Chavanet, P; Blettery, B. Candida spp. colonization significance in critically ill medical patients: A prospective study. Intensive Care Med 2005, 31, 393–400. [Google Scholar]
- Paphitou, NI; Ostrosky-Zeichner, L; Rex, JH. Rules for identifying patients at increased risk for candidal infections in the surgical intensive care unit: Approach to developing practical criteria for systematic use in antifungal prophylaxis trials. Med. Mycol 2005, 43, 235–243. [Google Scholar]
- Petri, MG; Konig, J; Moecke, HP. Epidemiology of invasive mycosis in ICU patients: A prospective multicenter study in 435 non-neutropenic patients. Intensive Care Med 1997, 23, 317–325. [Google Scholar]
- Slotman, G; Shapiro, E; Moffa, S. Fungal sepsis: multisite colonization versus fungemia. Am. Surg 1994, 60, 107–113. [Google Scholar]
- Pittet, D; Monod, M; Suter, PM; Frenk, E; Auckenthaler, R. Candida colonization and subsequent infections in critically ill surgical patients. Ann. Surg 1994, 220, 751–758. [Google Scholar]
- Clinical and Laboratory Standard Institute, Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi, 2nd ed; Clinical and Laboratory Standard Institute: Wayne, PA, USA, 2008; CLSI Document M38-A2.
- Pfaller, MA; Diekema, DJ; Jones, RN; Sader, HS; Fluit, AC; Hollis, RJ; Messer, SA. SENTRY Participant Group. International surveillance of bloodstream infections due to Candida species: frequency of occurrence and in vitro susceptibilities to fluconazole, ravuconazole, voriconazole of isolates collected from 1997 through 1999 in the SENTRY antimicrobial surveillance program. J. Clin. Microbiol 2001, 39, 3254–3259. [Google Scholar]
- Diekema, DJ; Messer, SA; Boyken, LB; Hollis, RJ; Kroeger, J; Tendolkar, S; Pfaller, MA. In vitro activity of seven systemically active antifungal agents against a large global rare Candida species as determined by CLSI broth microdilution methods. J. Clin. Microbiol 2009, 47, 3170–3177. [Google Scholar]
- Garbino, J; Lew, DP; Romand, JA; Hugonnet, S; Auckenthaler, R; Pittet, D. Prevention of severe Candida infections in non-neutropenic, high-risk, critically ill patients. A randomized, double-blind, placebo-controlled trial in SDD-treated patients. Intensive Care Med 2002, 28, 1708–1717. [Google Scholar]
- Dubau, B; Triboulet, C; Winnock, S. Utilisation pratique de l’index de colonisation. Ann. Fr. Anesth. Reanim 2001, 20, 418–420. [Google Scholar]
- Ellis, M; Al-Rmandi, B; Bernsen, R; Kristensen, J; Alizadeh, H; Hedstrom, U. Prospective evaluation of mannan and anti-manna antibodies for diagnosis of invasive Candida infections in patients with neutropenic fever. J. Med. Microbiol 2009, 58, 606–615. [Google Scholar]
- Laín, A; Elguezabal, N; Moragues, MD; García-Ruiz, JC; Del Palacio, A; Pontón, J. Contribution of serum biomarkers to the diagnosis of invasive candidiasis. Expert Rev. Mol. Diagn 2008, 8, 315–325. [Google Scholar]
- Pontón, J. Usefulness of biological markers in the diagnosis of invasive candidiasis. Rev. Iberoam. Micol 2009, 26, 8–14. [Google Scholar]
- Prella, M; Bille, J; Pugnale, M; Duvoisin, B; Cavassini, M; Calandra, T; Marchetti, O. Early diagnosis of invasive candidiasis with mannan antigenemia and antimannan antibodies. Diagn. Microbiol. Infect. Dis 2005, 51, 95–101. [Google Scholar]
- Shea, YR. Algorithms for Detection and Identification of Fungi. In Manual of Clinical Microbiology, 9th ed; Murray, P, Baron, EJ, Jorgensen, J, Landry, ML, Pfaller, M, Eds.; ASM Press: Washington, DC, USA, 2007; pp. 1745–1761. [Google Scholar]
- Sendid, B; Poirot, JL; Tabouret, M; Bonnin, A; Caillot, D; Camus, D; Poulain, D. Combined detection of mannanaemia and antimannan antibodies as a strategy for the diagnosis of systemic infection caused by pathogenic Candida species. J. Med. Microbiol 2002, 51, 433–442. [Google Scholar]
- Sendid, B; Caillot, DE; Baccouch-Humbert, B; Klingspor, L; Grandjean, M; Bonnin, A; Poulain, D. Contribution of the Platelia Candida Specific Antibody and Antigen tests to early diagnosis of systemic Candida tropicalis infection in neutropenic adults. J. Clin. Microbiol 2003, 41, 4551–4558. [Google Scholar]



{kind=link}
{kind=link}
| Pt 1 | Pt 2 | Pt 3 | |
|---|---|---|---|
| Sex | M | F | F |
| Age | 26 | 79 | 52 |
| Sofa | 8 | 8 | 8 |
| WBC | 20 × 103/mm3 | 7.5 × 103/mm3 | 15 × 103/mm3 |
| MV (days) | 27 | 50 | 15 |
| Admission days in ICU (no.) | 36 | 57 | 15 |
| CI (the day of candidemia) | 0.5 | 0.7 | 0.5 |
| Mannan Ag | + | /// | + |
| Ag Circulation | 4 d P | /// | 1 d P |
| Ab-anti Candida | 14.5 UA/mL | 12.8 UA/mL | 11.20 UA/mL |
| Ab Circulation | 7 d B | 4 d B | 5 d B |
| Outcome | living | died | living |
© 2011 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Caggiano, G.; Puntillo, F.; Coretti, C.; Giglio, M.; Alicino, I.; Manca, F.; Bruno, F.; Montagna, M.T. Candida Colonization Index in Patients Admitted to an ICU. Int. J. Mol. Sci. 2011, 12, 7038-7047. https://doi.org/10.3390/ijms12107038
Caggiano G, Puntillo F, Coretti C, Giglio M, Alicino I, Manca F, Bruno F, Montagna MT. Candida Colonization Index in Patients Admitted to an ICU. International Journal of Molecular Sciences. 2011; 12(10):7038-7047. https://doi.org/10.3390/ijms12107038
Chicago/Turabian StyleCaggiano, Giuseppina, Filomena Puntillo, Caterina Coretti, Mariateresa Giglio, Ilaria Alicino, Fabio Manca, Francesco Bruno, and Maria Teresa Montagna. 2011. "Candida Colonization Index in Patients Admitted to an ICU" International Journal of Molecular Sciences 12, no. 10: 7038-7047. https://doi.org/10.3390/ijms12107038