Asymmetric Dimethylarginine as a Surrogate Marker of Endothelial Dysfunction and Cardiovascular Risk in Patients with Systemic Rheumatic Diseases

Abstract
:1. Introduction
2. The Role of NO in Health and in Inflammation: The Beauty and the Beast?
3. ADMA as a Mediator of Cardiovascular Disease
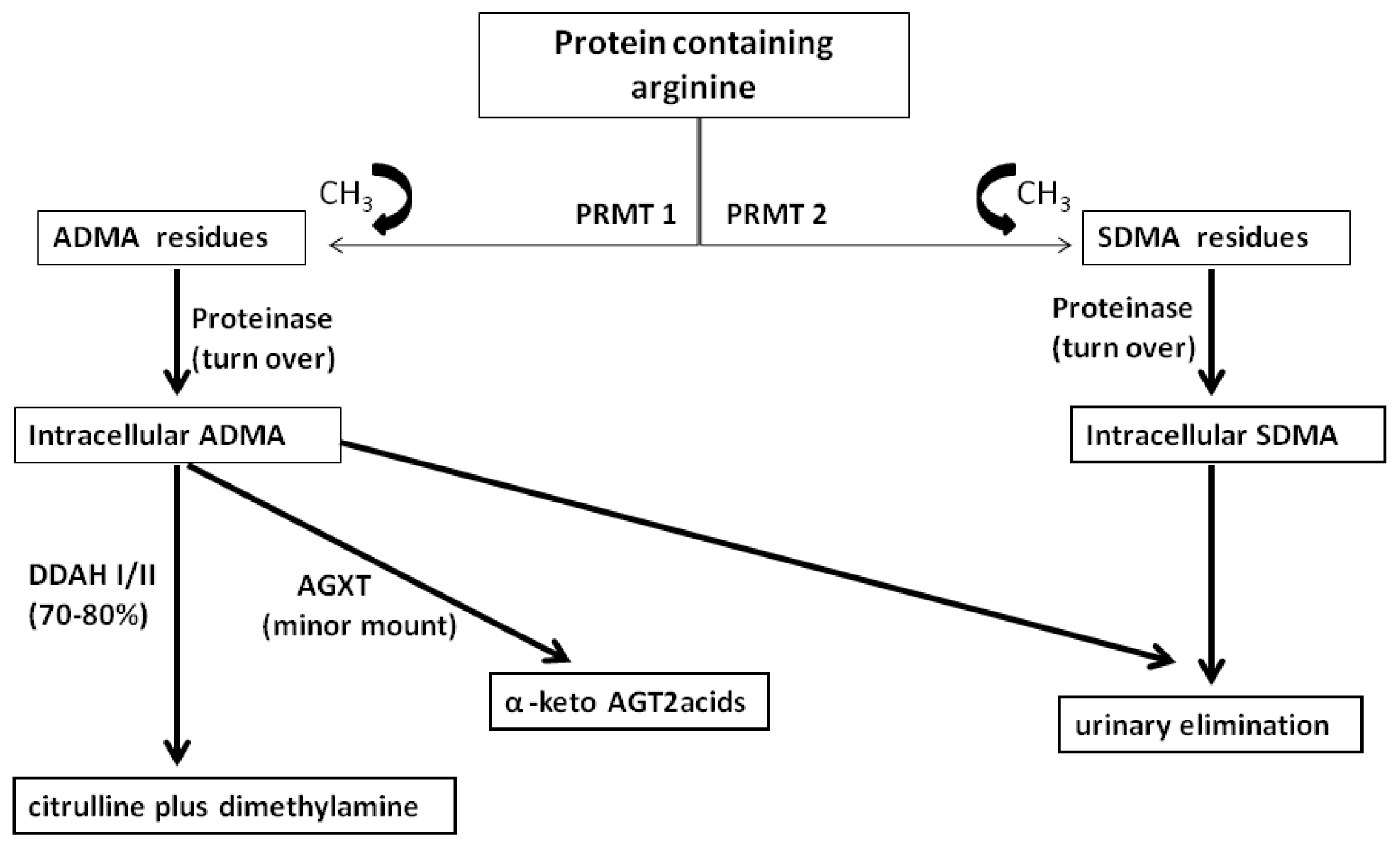
3.1. Biology
3.2. ADMA and the Regulation of Vascular Tone
3.3. ADMA and CVD
4. Cardiovascular Involvement in Rheumatic Diseases
5. ADMA as Biochemical Marker of CVD in Rheumatic Diseases
5.1. Atherosclerotic Disease
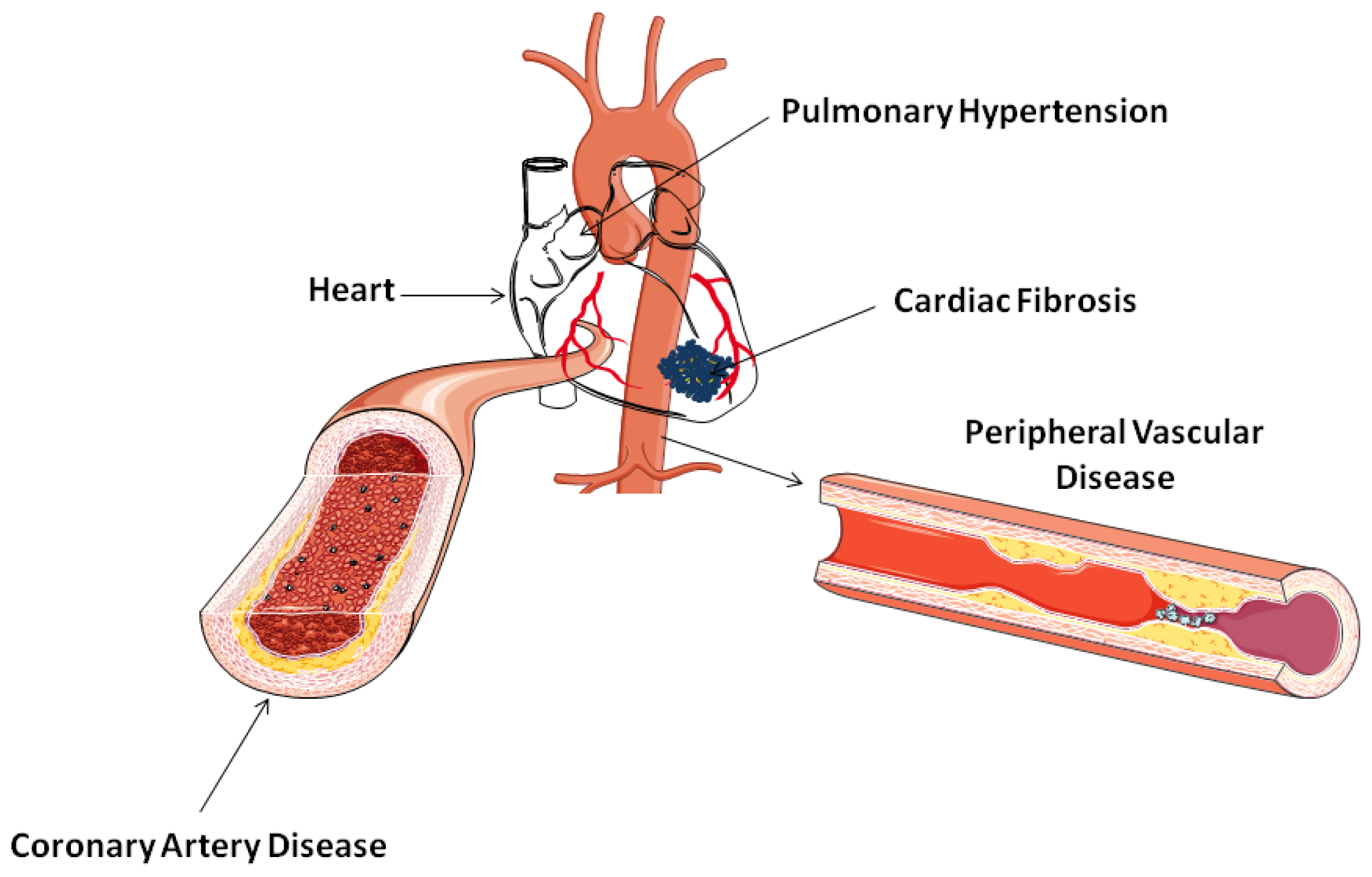
5.2. Cardiac Involvement and Pulmonary Hypertension
5.3. Peripheral Vascular Disease
6. Conclusions and Future Implications
References
- Watson, D.J.; Rhodes, T.; Guess, H.A. All-cause mortality and vascular events among patients with rheumatoid arthritis, osteoarthritis, or no arthritis in the UK General Practice Research Database. J. Rheumatol 2003, 30, 1196–1202. [Google Scholar]
- Goodson, N.J.; Wiles, N.J.; Lunt, M.; Barrett, E.M.; Silman, A.J.; Symmons, D.P. Mortality in early inflammatory polyarthritis: Cardiovascular mortality is increased in seropositive patients. Arthritis. Rheum 2002, 46, 2010–2019. [Google Scholar]
- Aviña-Zubieta, J.A.; Choi, H.K.; Sadatsafavi, M.; Etminan, E.; Esdaile, J.M.; Lacaille, D. Risk of cardiovascular mortality in patients with rheumatoid arthritis: A meta-analysis of observational studies. Arthritis. Rheum 2008, 59, 1690–1697. [Google Scholar]
- Belch, J.J.; McSwiggan, S.; Lau, C. Macrovascular disease in systemic sclerosis: The tip of an iceberg? Rheumatology (Oxford) 2008, 47, v16–v17. [Google Scholar]
- Toms, T.E.; Symmons, D.P.; Kitas, G.D. Dyslipidaemia in rheumatoid arthritis: The role of inflammation, drugs, lifestyle and genetic factors. Curr. Vasc. Pharmacol 2010, 8, 301–326. [Google Scholar]
- Summers, G.D.; Metsios, G.S.; Stavropoulos-Kalinoglou, A.; Kitas, G.D. Rheumatoid cachexia and cardiovascular disease. Nat. Rev. Rheumatol 2010, 6, 445–451. [Google Scholar]
- Panoulas, V.F.; Metsios, G.S.; Pace, A.V.; John, H.; Treharne, G.J.; Banks, M.J.; Kitas, G.D. Hypertension in rheumatoid arthritis. Rheumatology (Oxford) 2008, 47, 1286–1298. [Google Scholar]
- Stevens, R.J.; Douglas, K.M.; Saratzis, A.N.; Kitas, G.D. Inflammation and atherosclerosis in rheumatoid arthritis. Expert Rev. Mol. Med 2005, 7, 1–24. [Google Scholar]
- Onat, A.; Direskeneli, H. Excess cardiovascular risk in inflammatory rheumatic diseases: Pathophysiology and targeted therapy. Curr. Pharm. Des 2012, 18, 1465–1477. [Google Scholar]
- Gasparyan, A.Y. Cardiovascular risk and inflammation: pathophysiological mechanisms, drug design, and targets. Curr. Pharm. Des 2012, 18, 1447–1449. [Google Scholar]
- Tanasescu, C.; Jurcut, C.; Jurcut, R.; Ginghina, C. Vascular disease in rheumatoid arthritis: From subclinical lesions to cardiovascular risk. Eur. J. Intern. Med 2009, 20, 348–354. [Google Scholar]
- Van Halm, V.P.; Nielen, M.M.; Nurmohamed, M.T.; van Schaardenburg, D.; Reesink, H.W.; Voskuyl, A.E.; Twisk, J.W.; van de Stadt, R.J.; de Koning, M.H.; Habibuw, M.R.; et al. Lipids and inflammation: Serial measurements of the lipid profile of blood donors who later developed rheumatoid arthritis. AnnRheum. Dis 2007, 66, 184–188. [Google Scholar]
- Nielen, M.M.; van Schaardenburg, D.; Reesink, H.W.; Voskuyl, A.E.; Twisk, J.W.; van de Stadt, R.J.; de Koning, M.H.; Habibuw, M.R.; et al. Simultaneous development of acute phase response and autoantibodies in preclinical rheumatoid arthritis. Ann. Rheum. Dis 2006, 65, 535–537. [Google Scholar]
- Daza, L.; Aguirre, M.; Jimenez, M.; Herrera, R.; Bollain, J.J. Common carotid intima-media thickness and von Willebrand factor serum levels in rheumatoid arthritis female patients without cardiovascular risk factors. Clin. Rheumatol 2007, 26, 533–537. [Google Scholar]
- Gonzalez-Juanatey, C.; Llorca, J.; Amigo-Diaz, E.; Dierssen, T.; Martin, J.; Gonzalez-Gay, M.A. High prevalence of subclinical atherosclerosis in psoriatic arthritis patients without clinically evident cardiovascular disease or classic atherosclerosis risk factors. Arthritis. Rheum 2007, 57, 1074–1080. [Google Scholar]
- Khan, F.; Green, F.C.; Forsyth, J.S.; Greene, S.A.; Morris, A.D.; Belch, J.J.F. Impaired microvascular function in normal children: Effects of adiposity and poor glucose handling. J. Physiol 2003, 551, 705–711. [Google Scholar]
- Halcox, J.P.; Schenke, W.H.; Zalos, G.; Schenke, W.H. Prognostic value of coronary vascular endothelial dysfunction. Circulation 2002, 106, 653–658. [Google Scholar]
- Klocke, R.; Cockcroft, J.R.; Taylor, G.J.; Hall, I.R.; Blake, D.R. Arterial stiffness and central blood pressure, as determined by pulse wave analysis, in rheumatoid arthritis. Ann. Rheum. Dis 2003, 62, 414–418. [Google Scholar]
- Gonzalez-Juanatey, C.; Testa, A.; Garcia-Castelo, A.; Garcia-Porrua, C.; Llorca, J.; Vidan, J.; Hajeer, A.H.; Ollier, W.E.; Mattey, D.L.; Gonzalez-Gay, M.A. HLA-DRB1 status affects endothelial function in treated patients with rheumatoid arthritis. Am. J. Med 2003, 114, 647–652. [Google Scholar]
- Pahor, A.; Hojs, R.; Gorenjak, M.; Rozman, B. Accelerated atherosclerosis in pre-menopausal female patients with rheumatoid arthritis. Rheumatol. Int 2006, 27, 119–123. [Google Scholar]
- Bergholm, R.; Leirisalo-Repo, M.; Vehkavaara, S.; Mäkimattila, S.; Taskinen, M.-R.; Yki-Järvinen, H. Impaired responsiveness to NO in newly diagnosed patients with rheumatoid arthritis. Arterioscler. Thromb Vasc. Biol 2002, 22, 1637–1641. [Google Scholar]
- Costa, L.; Caso, F.; D’Elia, L.; Atteno, M.; Peluso, R.; Del Puente, A.; Strazzullo, P.; Scarpa, R. Psoriatic arthritis is associated with increased arterial stiffness in the absence of known cardiovascular risk factors: A case control study. Clin. Rheumatol 2012, 31, 711–715. [Google Scholar]
- Ulusoy, R.E.; Karabudak, O.; Yokusoglu, M.; Kilicaslan, F.; Kirilmaz, A.; Cebeci, B.S. Noninvasive assessment of impaired endothelial function in psoriasis. Rheumatol. Int 2010, 30, 479–483. [Google Scholar]
- Ghosh, P.; Kumar, A.; Kumar, S.; Aggarwal, A.; Sinha, N.; Misra, R. Subclinical atherosclerosis and endothelial dysfunction in young South-Asian patients with systemic lupus erythematosus. Clin. Rheumatol 2009, 28, 1259–1265. [Google Scholar]
- Colombo, B.M.; Murdaca, G.; Caiti, M.; Rodriguez, G.; Grassia, L.; Rossi, E.; Indiveri, F.; Puppo, F. Intima-media thickness: A marker of accelerated atherosclerosis in women with systemic lupus erythematosus. Ann. N.Y. Acad. Sci 2007, 1108, 121–126. [Google Scholar]
- Ahmadi, B.; Bonakdar, Z.S.; Hashemi, S.M.; Sadrkabir, S.M.; Karimifar, M. Endothelial dysfunction in Iranian lupus patients. Rheumatol. Int 2011, 31, 27–31. [Google Scholar]
- Sfikakis, P.P.; Papamichael, C.; Stamatelopoulos, K.S.; Tousoulis, D.; Fragiadaki, K.G.; Katsichti, P.; Stefanadis, C.; Mavrikakis, M. Improvement of vascular endothelial function using the oral endothelin receptor antagonist bosentan in patients with systemic sclerosis. Arthritis. Rheum 2007, 56, 1985–1993. [Google Scholar]
- Khan, F.; Galarraga, B.; Belch, J.J. The role of endothelial function and its assessment in rheumatoid arthritis. Nat. Rev. Rheumatol 2010, 6, 253–261. [Google Scholar]
- Dimitroulas, T.; Panoulas, V.; Smith, J.; Trehane, G.; Kitas, G.D.; Douglas, K. Interactions between coagulation and inflammation and metabolic factors in rheumatoid arthritis. Ann. Rheum. Dis 2010, 69, 368. [Google Scholar]
- Daoussis, D.; Kitas, G.D. Uric acid and cardiovascular risk in rheumatoid arthritis. Rheumatology (Oxford) 2011, 50, 1354–1355. [Google Scholar]
- Dimitroulas, T.; Giannakoulas, G.; Dimitroula, H.; Sfetsios, T.; Parcharidou, D.; Karvounis, H.; Settas, L. Significance of serum uric acid in pulmonary hypertension due to systemic sclerosis: A pilot study. Rheumatol. Int 2011, 31, 263–267. [Google Scholar]
- Ziolkowska, M.; Kurowska, M.; Radzikowska, A.; Luszczykiewicz, G.; Wiland, P.; Dziewczopolski, W.; Filipowicz-Sosnowska, A.; Pazdur, J.; Szechinski, J.; Kowalczewski, J.; et al. High levels of osteoprotegerin and soluble receptor activator of nuclear factor kappa B ligand in serum of rheumatoid arthritis patients and their normalization after anti-tumor necrosis factor alpha treatment. Arthritis. Rheum 2002, 46, 1744–1753. [Google Scholar]
- Szuba, A.; Podgórski, M. Asymmetric dimethylarginine (ADMA) a novel cardiovascular risk factor—Evidence from epidemiological and prospective clinical trials. Pharmacol. Rep 2006, 58, 16–20. [Google Scholar]
- Metsios, G.S.; Stavropoulos-Kalinoglou, A.; Sandoo, A.; van Zanten, J.J.C.S.V.; Toms, T.E.; John, H.; Kitas, G.D. Vascular function and inflammation in rheumatoid arthritis: The role of physical activity. Open Cardiovasc. Med. J. 2010, 4, 89–96. [Google Scholar]
- Palmer, R.M.; Ashton, D.S.; Moncada, S. Vascular endothelial cells synthesize nitric oxide from L-arginine. Nature 1988, 333, 664–666. [Google Scholar]
- Sandoo, A.; van Zanten, J.J.; Metsios, G.S.; Carroll, D.; Kitas, G.D. The endothelium and its role in regulating vascular tone. Open Cardiovasc. Med. J 2010, 4, 302–312. [Google Scholar]
- Herrick, A.L.; Matucci, C.M. The emerging problem of oxidative stress and the role of antioxidants in systemic sclerosis. Clin. Exp. Rheumatol 2001, 19, 4–8. [Google Scholar]
- Vanhoutte, P.M. Say NO to ET. J. Auton. Nerv. Syst 2000, 81, 271–277. [Google Scholar]
- Desideri, G.; Ferri, C. Endothelial activation. Sliding door to atherosclerosis. Curr. Pharm. Des 2005, 11, 2163–2175. [Google Scholar]
- Golias, C.; Tsoutsi, E.; Matziridis, A.; Makridis, P.; Batistatou, A.; Charalabopoulos, K. Leukocyte and endothelial cell adhesion molecules in inflammation focusing on inflammatory heart disease. In Vivo 2007, 21, 757–769. [Google Scholar]
- Valleggi, S.; Devaraj, S.; Dasu, M.R.; Jialal, I. C-reactive protein adversely alters the protein-protein interaction of the endothelial isoform of nitric oxide synthase. Clin. Chem 2010, 56, 1345–1348. [Google Scholar]
- Mäki-Petäjä, K.M.; Cheriyan, J.; Booth, A.D.; Hall, F.C.; Brown, J.; Wallace, S.M.; Ashby, M.J.; McEniery, C.M.; Wilkinson, I.B. Inducible nitric oxide synthase activity is increased in patients with rheumatoid arthritis and contributes to endothelial dysfunction. Int. J. Cardiol 2008, 129, 399–405. [Google Scholar]
- Shen, Y.H.; Wang, X.L.; Wilcken, D.E. Nitric oxide induces and inhibits apoptosis through different pathways. FEBS Lett 1998, 433, 125–131. [Google Scholar]
- Matucci, C.M.; Kahaleh, M.B. Beauty and the beast. The nitric oxide paradox in systemic sclerosis. Rheumatology (Oxford) 2002, 41, 843–847. [Google Scholar]
- Rawal, N.; Rajpurohit, R.; Lischwe, M.A.; Williams, K.R.; Paik, W.K.; Kim, S. Structural specifity of substrate for S-adenosylmethionine: Protein arginine N-methyltransferases. Biochim. Biophys. Acta 1995, 1248, 11–18. [Google Scholar]
- Ueda, S.; Yamagishi, S.; Okuda, S. New pathways to renal damage: Role of ADMA in retarding renal disease progression. J. Nephrol 2010, 23, 377–386. [Google Scholar]
- Achan, V.; Broadhead, M.; Malaki, M.; Whitley, G.; Leiper, J.; MacAllister, R.; Vallance, P. Asymmetric dimethylarginine causes hypertension and cardiac dysfunction in humans and is actively metabolized by dimethylarginine dimethylaminohydrolase. Arterioscler. Thromb Vasc. Biol 2003, 23, 1455–1459. [Google Scholar]
- Arrigoni, F.; Ahmetaj, B.; Leiper, J. The biology and therapeutic potential of the DDAH/ADMA pathway. Curr. Pharm. Des 2010, 16, 4089–4102. [Google Scholar]
- Ogawa, T.; Kimoto, M.; Sasaoka, K. Dimethylarginine:pyruvate aminotransferase in rats. Purification, properties, and identity with alanine:glyoxylate aminotransferase 2. J. Biol. Chem 1990, 265, 20938–20945. [Google Scholar]
- Landim, M.B.; Casella Filho, A.; Chagas, A.C. Asymmetric dimethylarginine (ADMA) and endothelial dysfunction: Implications for atherogenesis. Clinics (Sao Paulo) 2009, 64, 471–478. [Google Scholar]
- Vallance, P.; Leiper, J. Cardiovascular biology of the asymmetric dimethylarginine: dimethylarginine dimethylaminohydrolase pathway. Arterioscler. Thromb Vasc. Biol 2004, 24, 1023–1030. [Google Scholar]
- Leiper, J.; Nandi, M.; Torondel, B.; Murray-Rust, J.; Malaki, M.; O’Hara, B.; Rossiter, S.; Anthony, S.; Madhani, M.; Selwood, D.; et al. Disruption of methylarginine metabolism impairs vascular homeostasis. Nat. Med 2007, 13, 198–203. [Google Scholar]
- Pullamsetti, S.; Kiss, L.; Ghofrani, H.A.; Voswinckel, R.; Haredza, P.; Klepetko, W.; Aigner, C.; Fink, L.; Muyal, J.P.; Weissmann, N.; et al. Increased levels and reduced catabolism of asymmetric and symmetric dimethylarginines in pulmonary hypertension. FASEB J 2005, 19, 1175–1177. [Google Scholar]
- Dayoub, H.; Rodionov, R.N.; Lynch, C.; Cooke, J.P.; Arning, E.; Bottiglieri, T.; Lentz, S.R.; Faraci, F.M. Overexpression of dimethylarginine dimethylaminohydrolase inhibits asymmetric dimethylarginine-induced endothelial dysfunction in the cerebral circulation. Stroke 2008, 39, 180–184. [Google Scholar]
- Pope, A.J.; Karuppiah, K.; Cardounel, A.J. Role of the PRMT-DDAH-ADMA axis in the regulation of endothelial nitric oxide production. Pharmacol. Res 2009, 60, 461–465. [Google Scholar]
- Böger, R.H.; Maas, R.; Schulze, F.; Schwedhelm, E. Asymmetric dimethylarginine (ADMA) as a prospective marker of cardiovascular disease and mortality—An update on patient populations with a wide range of cardiovascular risk. Pharmacol. Res 2009, 60, 481–487. [Google Scholar]
- Schnabel, R.; Blankenberg, S.; Lubos, E.; Lackner, K.J.; Rupprecht, H.J.; Espinola-Klein, C.; Jachmann, N.; Post, F.; Peetz, D.; Bickel, C.; et al. Asymmetric dimethylarginine and the risk of cardiovascular events and death in patients with coronary artery disease: Results from the AtheroGene Study. Circ. Res 2005, 97, e53–e59. [Google Scholar]
- Anderssohn, M.; Schwedhelm, E.; Lüneburg, N.; Vasan, R.S.; Böger, R.H. Asymmetric dimethylarginine as a mediator of vascular dysfunction and a marker of cardiovascular disease and mortality: An intriguing interaction with diabetes mellitus. Diab. Vasc. Dis. Res 2010, 7, 105–118. [Google Scholar]
- Aucella, F.; Maas, R.; Vigilante, M.; Tripepi, G.; Schwedhelm, E.; Margaglione, M.; Gesualdo, L.; Boeger, R.; Zoccali, C. Methylarginines and mortality in patients with end stage renal disease: A prospective cohort study. Atherosclerosis 2009, 207, 541–545. [Google Scholar]
- Dückelmann, C.; Mittermayer, F.; Haider, D.G.; Altenberger, J.; Eichinger, J.; Wolzt, M. Asymmetric dimethylarginine enhances cardiovascular risk prediction in patients with chronic heart failure. Arterioscler. Thromb. Vasc. Biol 2007, 27, 2037–2042. [Google Scholar]
- Tutarel, O.; Denecke, A.; Bode-Böger, S.M.; Martens-Lobenhoffer, J.; Lovric, S.; Bauersachs, J.; Schieffer, B.; Westhoff-Bleck, M.; Kielstein, J.T. Asymmetrical dimethylarginine-more sensitive than NT-proBNP to diagnose heart failure in adults with congenital heart disease. PLoS One 2012, 7, e33795. [Google Scholar]
- Zoccali, C. Asymmetric dimethylarginine (ADMA): A cardiovascular and renal risk factor on the move. J. Hypertens 2006, 24, 611–619. [Google Scholar]
- Lu, T.M.; Chung, M.Y.; Lin, M.W.; Hsu, C.P.; Lin, S.J. Plasma asymmetric dimethylarginine predicts death and major adverse cardiovascular events in individuals referred for coronary angiography. Int. J. Cardiol 2011, 153, 135–140. [Google Scholar]
- Nijveldt, R.J.; Teerlink, T.; van Der Hoven, B.; Siroen, M.P.; Kuik, D.J.; Rauwerda, J.A.; van Leeuwen, P.A. Asymmetrical dimethylarginine (ADMA) in critically ill patients: high plasma ADMA concentration is an independent risk factor of ICU mortality. Clin. Nutr 2003, 22, 23–30. [Google Scholar]
- Böger, R.H.; Sullivan, L.M.; Schwedhelm, E.; Wang, T.J.; Maas, R.; Benjamin, E.J.; Schulze, F.; Xanthakis, V.; Benndorf, R.A.; Vasan, R.S. Plasma asymmetric dimethylarginine and incidence of cardiovascular disease and death in the community. Circulation 2009, 119, 1592–1600. [Google Scholar]
- Leong, T.; Zylberstein, D.; Graham, I.; Lissner, L.; Ward, D.; Fogarty, J.; Bengtsson, C.; Björkelund, C.; Thelle, D. For the Swedish–Irish–Norwegian collaboration. asymmetric dimethylarginine independently predicts fatal and nonfatal myocardial infarction and stroke in women: 24-year follow-up of the population study of women in Gothenburg. Arterioscler. Thromb. Vasc. Biol 2008, 28, 961–967. [Google Scholar]
- Maas, R.; Schulze, F.; Baumert, J.; Löwel, H.; Hamraz, K.; Schwedhelm, E.; Koenig, W.; Böger, R.H. Asymmetric dimethylarginine, smoking, and risk of coronary heart disease in apparently healthy men: Prospective analysis from the population-based monitoring of trends and determinants in cardiovascular disease/kooperative gesundheitsforschung in der Region Augsburg study and experimental data. Clin. Chem 2007, 53, 693–701. [Google Scholar]
- Mellana, W.M.; Aronow, W.S.; Palaniswamy, C.; Khera, S. Rheumatoid arthritis: Cardiovascular manifestations, pathogenesis, and therapy. Curr. Pharm. Des 2012, 18, 1450–1456. [Google Scholar]
- Dimitroulas, T.; Giannakoulas, G.; Karvounis, H.; Settas, L.; Kitas, G.D. Systemic sclerosis-related pulmonary hypertension: Unique characteristics and future treatment targets. Curr. Pharm. Des 2012, 18, 1457–1464. [Google Scholar]
- Symmons, D.P.; Gabriel, S.E. Epidemiology of CVD in rheumatic disease, with a focus on RA and SLE. Nat. Rev. Rheumatol 2011, 7, 399–408. [Google Scholar]
- Bacon, P.A.; Stevens, R.J.; Carruthers, D.M.; Young, S.P.; Kitas, G.D. Accelerated atherogenesis in autoimmune rheumatic diseases. Autoimmun. Rev 2002, 1, 338–347. [Google Scholar]
- Ramonda, R.; Lo Nigro, A.; Modesti, V.; Nalotto, L.; Musacchio, E.; Iaccarino, L.; Punzi, L.; Doria, A. Atherosclerosis in psoriatic arthritis. Autoimmun. Rev 2011, 10, 773–738. [Google Scholar]
- Azevedo, V.F.; Pecoits-Filho, R. Atherosclerosis and endothelial dysfunction in patients with ankylosing spondylitis. Rheumatol. Int 2010, 30, 1411–1416. [Google Scholar]
- John, H.; Toms, T.E.; Kitas, G.D. Rheumatoid arthritis: Is it a coronary heart disease equivalent? Curr. Opin. Cardiol 2011, 26, 327–333. [Google Scholar]
- Nurmohamed, M.T.; Kitas, G. Cardiovascular risk in rheumatoid arthritis and diabetes: How does it compare and when does it start? Ann. Rheum. Dis 2011, 70, 881–883. [Google Scholar]
- Sandoo, A.; Veldhuijzen van Zanten, J.J.; Metsios, G.S.; Carroll, D.; Kitas, G.D. Vascular function and morphology in rheumatoid arthritis: A systematic review. Rheumatology (Oxford) 2011, 50, 2125–2139. [Google Scholar]
- Douglas, K.M.; Pace, A.V.; Treharne, G.J.; Saratzis, A.; Nightingale, P.; Erb, N.; Banks, M.J.; Kitas, G.D. Excess recurrent cardiac events in rheumatoid arthritis patients with acute coronary syndrome. Ann. Rheum. Dis 2006, 65, 348–353. [Google Scholar]
- Panoulas, V.F.; Nikas, S.N.; Smith, J.P.; Douglas, K.M.; Nightingale, P.; Milionis, H.J.; Treharne, G.J.; Toms, T.E.; Kita, M.D.; Kitas, G.D. Lymphotoxin 252A>G polymorphism is common and associates with myocardial infarction in patients with rheumatoid arthritis. Ann. Rheum. Dis 2008, 67, 1550–1556. [Google Scholar]
- Swanberg, M.; Lidman, O.; Padyukov, L.; Eriksson, P.; Akesson, E.; Jagodic, M.; Lobell, A.; Khademi, M.; Börjesson, O.; et al. MHC2TA is associated with differential MHC molecule expression and susceptibility to rheumatoid arthritis, multiple sclerosis and myocardial infarction. Nat. Genet 2005, 37, 486–494. [Google Scholar]
- Kitas, G.D.; Gabriel, S.E. Cardiovascular disease in rheumatoid arthritis: State of the art and future perspectives. Ann. Rheum. Dis 2011, 70, 8–14. [Google Scholar]
- Boueiz, A.; Mathai, S.C.; Hummers, L.K.; Hassoun, P.M. Cardiac complications of systemic sclerosis: Recent progress in diagnosis. Curr. Opin. Rheumatol 2010, 22, 696–703. [Google Scholar]
- Chatterjee, S. Pulmonary hypertension in systemic sclerosis. Semin. Arthritis. Rheum 2011, 41, 19–37. [Google Scholar]
- Dimitroulas, T.; Giannakoulas, G.; Karvounis, H.; Gatzouli, M.A.; Settas, L. Natriuretic peptides in systemic sclerosis-related pulmonary arterial hypertension. Semin. Arthritis. Rheum 2010, 39, 278–284. [Google Scholar]
- Dimitroulas, T.; Giannakoulas, G.; Karvounis, H.; Sttas, L.; Kitas, G.D. Biomarkers in systemic sclerosis-related pulmonary arterial hypertension. Curr. Vasc. Pharmacol 2011, 9, 213–219. [Google Scholar]
- Dimitroulas, T.; Mavrogeni, S.; Kitas, G.D. Imaging modalities for the diagnosis of pulmonary hypertension in systemic sclerosis. Nat. Rev. Rheumatol 2012, 8, 203–213. [Google Scholar]
- Mavrogeni, S.; Dimitroulas, T.; Kitas, G.D. Multimodality imaging and the emerging role of cardiac magnetic resonance in autoimmune myocarditis. Autoimmun. Rev 2012. [Google Scholar] [CrossRef]
- Surdacki, A.; Martens-Lobenhoffer, J.; Wloch, A.; Marewicz, E.; Rakowski, T.; Wieczorek-Surdacka, E.; Dubiel, J.S.; Pryjma, J.; Boger, S.M. Elevated plasma asymmetric dimethyl-L-arginine levels are linked to endothelial progenitor cell depletion and carotid atherosclerosis in rheumatoid arthritis. Arthritis. Rheum 2007, 56, 809–819. [Google Scholar]
- Turiel, M.; Atzeni, F.; Tomasoni, L.; de Portu, S.; Delfino, L.; Bodini, B.D.; Longhi, M.; Sitia, S.; Bianchi, M.; Ferrario, P.; et al. Non invasive assessment of coronary flow reserve and ADMA levels: A case-control study of early rheumatoid arthritis patients. Rheumatology (Oxford) 2009, 48, 834–839. [Google Scholar]
- Sandoo, A.; Dimitroulas, T.; Veldhuijzen van Zanten, J.J.; Smith, J.P.; Metsios, G.S.; Nightingale, P.; Stavropoulos-Kalinoqlou, A.; Kitas, G.D. Lack of association between asymmetric dimethylarginine and in vivo microvascular or macrovascular endothelial function in patients with rheumatoid arthritis. Clin. Exp. Rheumatol 2012, 30, 388–396. [Google Scholar]
- Atzeni, F.; Sarzi-Puttini, P.; Sitia, S.; Tomasoni, L.; Gianturco, L.; Battellino, M.; Boccassini, L.; De Gennaro Colonna, V.; Marchesoni, A.; Turiel, M. Coronary flow reserve and asymmetric dimethylarginine levels: New measurements for identifying subclinical atherosclerosis in patients with psoriatic arthritis. J. Rheumatol 2011, 38, 1661–1664. [Google Scholar]
- Sari, I.; Kebapcilar, L.; Alacacioglu, A.; Bilgir, O.; Yildiz, Y.; Taylan, A.; Yuksel, A.; Kozaci, D.L. Increased levels of asymmetric dimethylarginine (ADMA) in patients with ankylosing spondylitis. Intern. Med 2009, 48, 1363–1368. [Google Scholar]
- Kemény-Beke, Á.; Gesztelyi, R.; Bodnár, N.; Zsuga, J.; Kerekes, G.; Zsuga, M.; Biri, B.; Kéki, S.; Szodoray, P.; Berta, A.; et al. Increased production of asymmetric dimethylarginine (ADMA) in ankylosing spondylitis: Association with other clinical and laboratory parameters. Joint Bone Spine 2011, 78, 184–187. [Google Scholar]
- Ito, A.; Tsao, P.S.; Adimoolam, S.; Kimoto, M.; Kimoto, M.; Ogawa, T.; Cooke, J.P. Novel mechanism for endothelial dysfunction: Dysregulation of dimethylarginine dimethylaminohydrolase. Circulation 1999, 99, 3092–3095. [Google Scholar]
- Ku, I.A.; Imboden, J.B.; Hsue, P.Y.; Ganz, P. Rheumatoid arthritis: Model of systemic inflammation driving atherosclerosis. Circ. J 2009, 73, 977–985. [Google Scholar]
- Sydow, K.; Münzel, T. ADMA and oxidative stress. Atheroscler. Suppl 2003, 4, 41–51. [Google Scholar]
- Kaur, H.; Halliwell, B. Evidence for nitric oxide-mediated oxidative damage in chronic inflammation. Nitrotyrosine in serum and synovial fluid from rheumatoid patients. FEBS Lett 1994, 350, 9–12. [Google Scholar]
- Kiani, A.N.; Mahoney, J.A.; Petri, M. Asymmetric dimethylarginine is a marker of poor prognosis and coronary calcium in systemic lupus erythematosus. J. Rheumatol 2007, 34, 1502–1505. [Google Scholar]
- Perna, M.; Roman, M.J.; Alpert, D.R.; Crow, M.K.; Lockshin, M.D.; Sammaritano, L.; Devereux, R.B.; Cooke, J.P.; Salmon, J.E. Relationship of asymmetric dimethylarginine and homocysteine to vascular aging in systemic lupus erythematosus patients. Arthritis. Rheum 2010, 62, 1718–1722. [Google Scholar]
- Bultink, I.E.; Teerlink, T.; Heijst, J.A.; Dijkmans, B.A.; Voskuyl, A.E. Raised plasma levels of asymmetric dimethylarginine are associated with cardiovascular events, disease activity, and organ damage in patients with systemic lupus erythematosus. Ann. Rheum. Dis 2005, 64, 1362–1365. [Google Scholar]
- Herbrig, K.; Haensel, S.; Oelschlaegel, U.; Pistrosch, F.; Foerster, S.; Passauer, J. Endothelial dysfunction in patients with rheumatoid arthritis is associated with a reduced number and impaired function of endothelial progenitor cells. Ann. Rheum. Dis 2006, 65, 157–163. [Google Scholar]
- Denny, M.F.; Thacker, S.; Mehta, H.; Somers, E.C.; Dodick, T.; Barrat, F.J.; McCune, W.J.; Kaplan, M.J. Interferon-alpha promotes abnormal vasculogenesis in lupus: A potential pathway for premature atherosclerosis. Blood 2007, 110, 2907–2915. [Google Scholar]
- Aicher, A.; Heeschen, C.; Mildner-Rihm, C.; Urbich, C.; Ihling, C.; Technau-Ihling, K.; Zeiher, A.M.; Dimmeler, S. Essential role of endothelial nitric oxide synthase for mobilization of stem and progenitor cells. Nat. Med 2003, 9, 1370–1376. [Google Scholar]
- Kwaśny-Krochin, B.; Głuszko, P.; Undas, A. Plasma asymmetric dimethyl-L-arginine (ADMA) in active rheumatoid arthritis: Links with oxidative stress and inflammation. Pol. Arch. Med. Wewn 2012, 122, 270–276. [Google Scholar]
- Turiel, M.; Tomasoni, L.; Sitia, S.; Cicala, S.; Gianturco, L.; Ricci, C.; Atzeni, F.; De Gennaro Colonna, V.; Longhi, M.; Sarzi-Puttini, P. Effects of long-term disease-modifying antirheumatic drugs on endothelial function in patients with early rheumatoid arthritis. Cardiovasc. Ther 2010, 10, 1–12. [Google Scholar]
- Sandoo, A.; Dimitroulas, T.; Toms, T.E.; Hodson, J.; Veldhuijzen van Zanten, J.J.; Smith, J.P.; Kitas, G.D. Clinical remission following treatment with tumour necrosis factor-alpha antagonists is not accompanied by changes in asymmetric dimethylarginine in patients with rheumatoid arthritis. Clin. Biochem 2012. [Google Scholar] [CrossRef]
- Dimitroulas, T.; Sandoo, A.; Veldhuijzen van Zanten, J.J.; Smith, J.P.; Metsios, G.S.; Nightingale, P.; Stavropoulos-Kalinoqlou, A.; Kitas, G.D. Predictors of assymetric dimethyl arginine in rheumatoid arthritis. Arthritis. Rheum 2011, 63, S827. [Google Scholar]
- Perticone, F.; Sciacqua, A.; Maio, R.; Perticone, M.; Galiano Leone, G.; Bruni, R.; di Cello, S.; Pascale, A.; Talarico, G.; Greco, L.; et al. Endothelial dysfunction, ADMA and insulin resistance in essential hypertension. Int. J. Cardiol 2010, 142, 236–241. [Google Scholar]
- Liang, K.P.; Kremers, H.M.; Crowson, C.S.; Snyder, M.R.; Therneau, T.M.; Roger, V.L.; Gabriel, S.E. Autoantibodies and the risk of cardiovascular events. J. Rheumatol 2009, 36, 2462–2469. [Google Scholar]
- Hjeltnes, G.; Hollan, I.; Førre, Ø.; Wiik, A.; Mikkelsen, K.; Agewall, S. Anti-CCP and RF IgM: Predictors of impaired endothelial function in rheumatoid arthritis patients. Scand. J. Rheumatol. 2011, 40, 422–427. [Google Scholar]
- Marasovic-Krstulovic, D.; Martinovic-Kaliterna, D.; Fabijanic, D.; Morovic-Vergles, J. Are the anti-cyclic citrullinated peptide antibodies independent predictors of myocardial involvement in patients with active rheumatoid arthritis? Rheumatology (Oxford) 2011, 50, 1505–1512. [Google Scholar]
- Surdacki, A.; Martens-Lobenhoffer, J.; Wloch, A.; Gluszko, P.; Rakowski, T.; Dubiel, J.S.; Boger, S.M. Plasma asymmetric dimethylarginine is related to anticitrullinated protein antibodies in rheumatoid arthritis of short duration. Metabolism 2009, 58, 316–318. [Google Scholar]
- Shao, Z.; Wang, Z.; Shrestha, K.; Thakur, A.; Borowski, A.G.; Sweet, W.; Thomas, J.D.; Moravec, C.S.; Hazen, S.L.; Tang, W.H. Pulmonary hypertension associated with advanced systolic heart failure: Dysregulated arginine metabolism and importance of compensatory dimethylarginine dimethylaminohydrolase-1. J. Am. Coll. Cardiol 2012, 59, 1150–1158. [Google Scholar]
- Cua, C.L.; Rogers, L.K.; Chicoine, L.G.; Augustine, M.; Jin, Y.; Nash, P.L.; Nelin, L.D. Down syndrome patients with pulmonary hypertension have elevated plasma levels of asymmetric dimethylarginine. Eur. J. Pediatr 2011, 170, 859–863. [Google Scholar]
- Kielstein, J.T.; Bode-Böger, S.M.; Hesse, G.; Martens-Lobenhoffer, J.; Takacs, A.; Fliser, D.; Hoeper, M.M. Asymmetrical dimethylarginine in idiopathic pulmonary arterial hypertension. Arterioscler. Thromb. Vasc. Biol 2005, 25, 1414–1418. [Google Scholar]
- Skoro-Sajer, N.; Mittermayer, F.; Panzenboeck, A.; Sadushi, R.; Hitsch, R.; Jakowitsch, J.; Klepetko, W.; Kneussl, M.P.; Wolzt, M.; Lang, I.M. Asymmetric dimethylarginine is increased in chronic thromboembolic pulmonary hypertension. Am. J. Respir. Crit. Care Med 2007, 176, 1154–1160. [Google Scholar]
- Dimitroulas, T.; Giannakoulas, G.; Papadopoulou, K.; Sfetsios, T.; Karvounis, H.; Dimitroula, H.; Parharidou, D.; Koliakos, G.; Garyfallos, A.; Styliadis Settas, L. Left atrial volume and N-terminal pro-B type natriuretic peptide are associated with elevated pulmonary artery pressure in patients with systemic sclerosis. Clin. Rheumatol 2010, 29, 957–964. [Google Scholar]
- Dimitroulas, T.; Giannakoulas, G.; Sfetsios, T.; Karvounis, H.; Dimitroula, H.; Koliakos, G.; Settas, L. Asymmetrical dimethylarginine in systemic sclerosis-related pulmonary arterial hypertension. Rheumatology (Oxford) 2008, 47, 1682–1685. [Google Scholar]
- Rolla, G.; Colagrande, P.; Scappaticci, E.; Chiavassa, G.; Dutto, L.; Cannizzo, S.; Bucca, C.; Morello, M.; Bergerone, S.; Bardini, D.; et al. Exhaled nitric oxide in systemic sclerosis: Relationships with lung involvement and pulmonary hypertension. J. Rheumatol 2000, 27, 1693–1698. [Google Scholar]
- Dimitroulas, T.; Giannakoulas, G.; Papadopoulou, K.; Karvounis, H.; Dimitroula, H.; Koliakos, G.; Karamitsos, T.; Parharidou, D.; Settas, L. Early detection of cardiac involvement in systemic sclerosis assessed by tissue-doppler echocardiography: Relationship with neurohormonal activation and endothelial dysfunction. J. Rheumatol 2010, 37, 993–999. [Google Scholar]
- Wilson Tang, W.H.; Tong, W.; Shrestha, K.; Wang, Z.; Levison, B.S.; Delfraino, B.; Hu, B.; Troughton, R.W.; Klein, A.L.; Hazen, S.L. Differential effects of arginine methylation on diastolic dysfunction and disease progression in patients with chronic systolic heart failure. Eur. Heart J 2008, 29, 2506–2513. [Google Scholar]
- Tomita, H.; Egashira, K.; Ohara, Y.; Takemoto, M.; Koyanagi, M.; Katoh, M.; Yamamoto, H.; Tamaki, K.; Shimokawa, H.; Takeshita, A. Early induction of transforming growth factor-beta via angiotensin II type 1 receptors contributes to cardiac fibrosis induced by long-term blockade of nitric oxide synthesis in rats. Hypertension 1998, 32, 273–279. [Google Scholar]
- Rajagopalan, S.; Pfenninger, D.; Kehrer, C.; Chakrabarti, A.; Somers, E.; Pavlic, R.; Mukherjee, D.; Brook, R.; D’Alecy, L.G.; Kaplan, M.J. Increased asymmetric dimethylarginine and endothelin 1 levels in secondary Raynaud’s phenomenon: implications for vascular dysfunction and progression of disease. Arthritis. Rheum 2003, 48, 1992–2000. [Google Scholar]
- Dooley, A.; Gao, B.; Bradley, N.; Abraham, D.J.; Black, C.M.; Jacobs, M.; Bruckdorfer, K.R. Abnormal nitric oxide metabolism in systemic sclerosis: Increased levels of nitrated proteins and asymmetric dimethylarginine. Rheumatology (Oxford) 2006, 45, 676–684. [Google Scholar]
- Cotton, S.A.; Herrick, A.L.; Jayson, M.I.; Freemont, A.J. Endothelial expression of nitric oxide synthases and nitrotyrosine in systemic sclerosis skin. J. Pathol 1999, 189, 273–278. [Google Scholar]
- Leiper, J.; Murray-Rust, J.; McDonald, N.; Vallance, P. S-nitrosylation of dimethylarginine dimethylaminohydrolase regulates enzyme activity: Further interactions between nitric oxide synthase and dimethylarginine dimethylaminohydrolase. Proc. Natl. Acad. Sci. USA 2002, 99, 13527–13532. [Google Scholar]
- Blaise, S.; Maas, R.; Trocme, C.; Kom, G.D.; Roustit, M.; Carpentier, P.H.; Cracowski, G.L. Correlation of biomarkers of endothelium dysfunction and matrix remodeling in patients with systemic sclerosis. J. Rheumatol 2009, 36, 984–988. [Google Scholar]
- Wipff, J.; Avouac, J.; Borderie, D.; Zerkak, D.; Lemarechal, H.; Kahan, A.; Boileau, C.; Allanore, Y. Disturbed angiogenesis in systemic sclerosis: High levels of soluble endoglin. Rheumatology (Oxford) 2008, 47, 972–975. [Google Scholar]
- Boehme, M.W.; Gao, I.K.; Norden, C.; Lemmel, E.M. Decrease in circulating endothelial cell adhesion molecule and thrombomodulin levels during oral iloprost treatment in rheumatoid arthritis patients: Preliminary results. Rheumatol. Int 2006, 26, 340–347. [Google Scholar]
- Blardi, P.; de Lalla, A.; Pieragalli, D.; De Franco, V.; Meini, S.; Ceccatelli, L.; Auteri, A. Effect of iloprost on plasma asymmetric dimethylarginine and plasma and platelet serotonin in patients with peripheral arterial occlusive disease. Prostaglandins Other Lipid Mediat 2006, 80, 175–182. [Google Scholar]
- Gonzalez, A.; Maradit Kremers, H.; Crowson, C.S.; Nicola, P.J.; Davis, J.M., III; Therneau, T.M.; Roger, V.L.; Gabriel, S.E. The widening mortality gap between rheumatoid arthritis patients and the general population. Arthritis. Rheum. 2007, 56, 3583–3587. [Google Scholar]
- Kerekes, G.; Soltész, P.; Nurmohamed, M.T.; Gonzalez-Gay, M.A.; Turiel, M.; Végh, E.; Shoenfeld, Y.; McInnes, I.; Szekanecz, Z. Validated methods for assessment of subclinical atherosclerosis in rheumatology. Nat. Rev. Rheumatol 2012, 8, 224–234. [Google Scholar]



{kind=link}
{kind=link}
| Study | Patients | Parameters assessed | Assessment tools | ADMA | Associations |
|---|---|---|---|---|---|
| Surdacki et al. [87] | 30 RA/20 controls | Atherosclerosis | Carotid U/S | ↑RA | IMT, endothelial progenitor cells count |
| Turiel et al. [88] | 25 RA/25 controls | Dipyridamole trans-thoracic stress U/S Carotid U/S | ↑RA | CFR | |
| Sandoo et al. [89] | 67 RA/29 controls | Microvascular/macrovascular function Arterial stiffness | LDI with iontophoresis of ACh and SNP FMD with high-resolution U/S of the brachial artery Augmentation index | ↑RA | No associations |
| Surdacki et al. [111] | 20 RA | Autoimmunity | APCA | APCA | |
| Kwaśny-Krochin et al. [103] | 46 RA/50 controls | Disease activity | Inflammatory markers Disease activity and disability scores | ↑RA | CRP, fibrinogen, DAS28, HAQ |
| Turiel et al. [104] | 10 RA | Response to biologics | (−) after treatment | ||
| Sandoo et al. [105] | 35 RA | ||||
| Atzeni et al. [90] | 22 PsA/35 controls | ED Atherosclerosis | Dipyridamole trans-thoracic stress U/S Carotid U/S | ↑PsA | CFR |
| Sari et al. [91] | 48 AS/38 controls | Disease activity CVD risk | Inflammatory markers | ↑AS | CRP, cholesterol |
| Kemény-Beke et al. [92] | 61 AS/26 OA | Disease activity | Inflammatory markers | ↑AS | ESR, chest expansion |
| Kiani et al. [97] | 200 SLE | Atherosclerosis Disease activity Autoimmunity | Coronary calcium score Inflammatory markers Autoantibodies | Coronary calcium, anti-dsDNA, ↓ complement, ESR | |
| Perna et al. [98] | 125 SLE | Atherosclerosis Arterial stiffness | Carotid U/S Augmentation index | Augmentation index | |
| Bultink et al. [99] | 107 SLE | CVD risk | ↑ ADMA predicts CVD events | ||
| Dooley et al. [123] | 45 SSc/19 PR/25 controls | ED | ADMA, nitration of proteins | ↑SSc ↑dSSc | |
| Blaise et al. [126] | 39 SSc/28 controls | Matrix remodelling ED | TIMP-1 ADMA | ↑SSc | TIMP-1 |
| Wipff et al. [127] | 187 SSc/48 controls | Angiogenesis ED | Soluble endoglin ADMA | no difference | |
| Dimitroulas et al. [116] | 66 SSc | SScPH | U/S | ↑SScPH | |
| Dimitroulas et al. [117] | 66 SSc/30 controls | SScPH | U/S | ↑SScPH | 6MWT |
| Dimitroulas et al. [118] | 52 SSc/25 controls | Occult cardiac involvement | TDI | ↑Cardiac disease |
© 2012 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Dimitroulas, T.; Sandoo, A.; Kitas, G.D. Asymmetric Dimethylarginine as a Surrogate Marker of Endothelial Dysfunction and Cardiovascular Risk in Patients with Systemic Rheumatic Diseases. Int. J. Mol. Sci. 2012, 13, 12315-12335. https://doi.org/10.3390/ijms131012315
Dimitroulas T, Sandoo A, Kitas GD. Asymmetric Dimethylarginine as a Surrogate Marker of Endothelial Dysfunction and Cardiovascular Risk in Patients with Systemic Rheumatic Diseases. International Journal of Molecular Sciences. 2012; 13(10):12315-12335. https://doi.org/10.3390/ijms131012315
Chicago/Turabian StyleDimitroulas, Theodoros, Aamer Sandoo, and George D. Kitas. 2012. "Asymmetric Dimethylarginine as a Surrogate Marker of Endothelial Dysfunction and Cardiovascular Risk in Patients with Systemic Rheumatic Diseases" International Journal of Molecular Sciences 13, no. 10: 12315-12335. https://doi.org/10.3390/ijms131012315