Expression and Role of GPR87 in Urothelial Carcinoma of the Bladder

Abstract
:1. Introduction
2. Results and Discussion
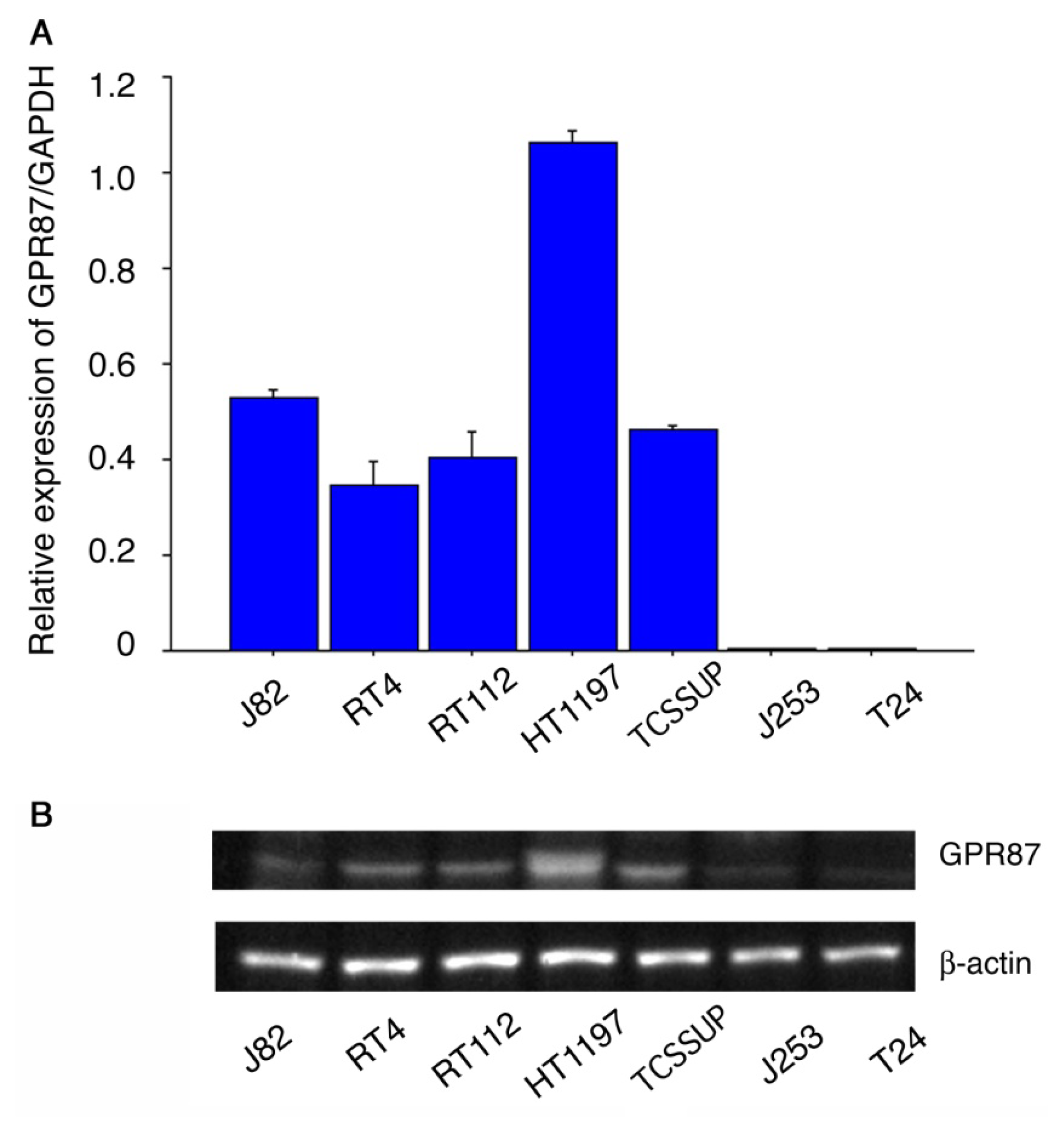
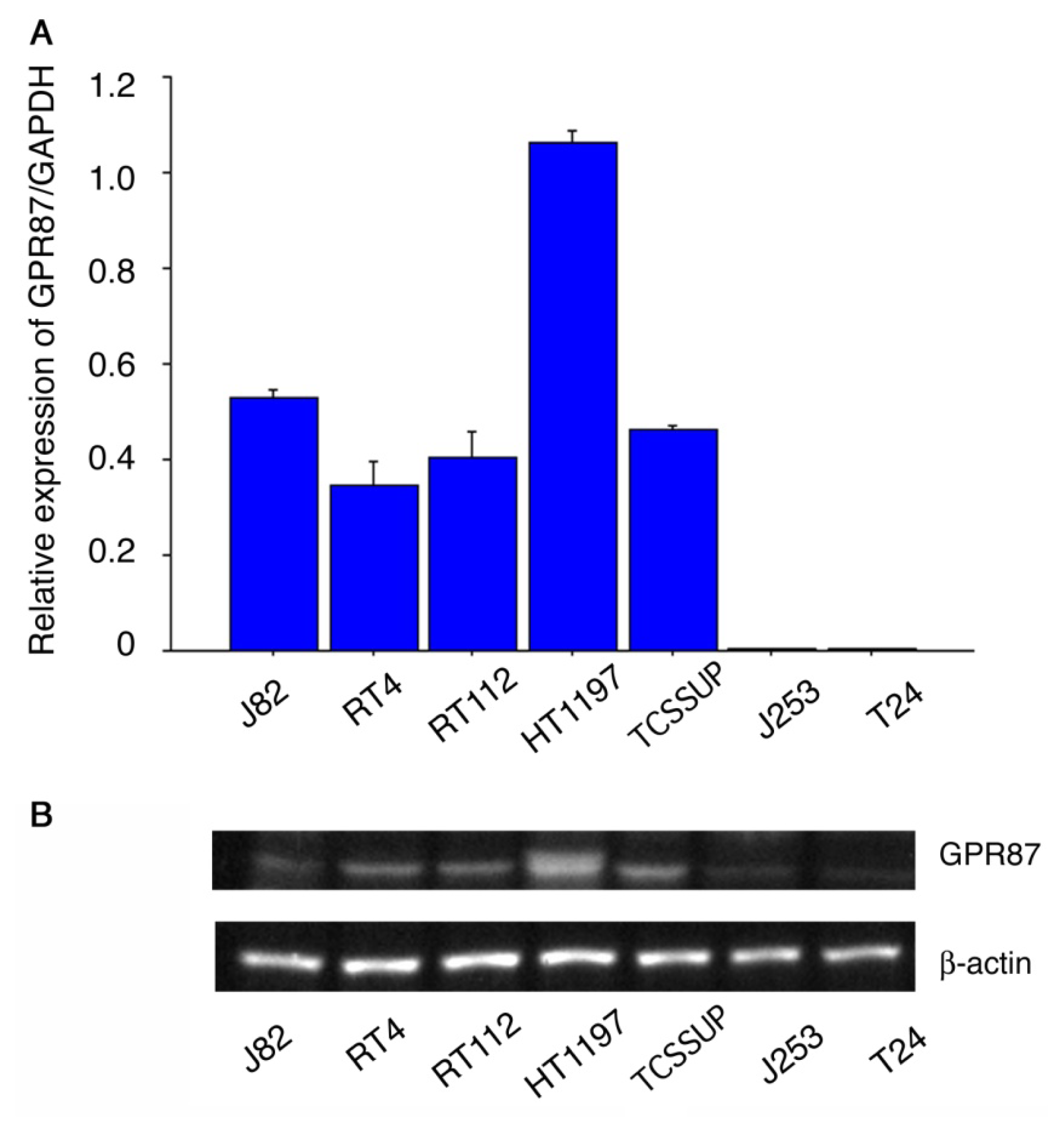
2.1. GPR87 Expression in Bladder Cancer Cell Lines
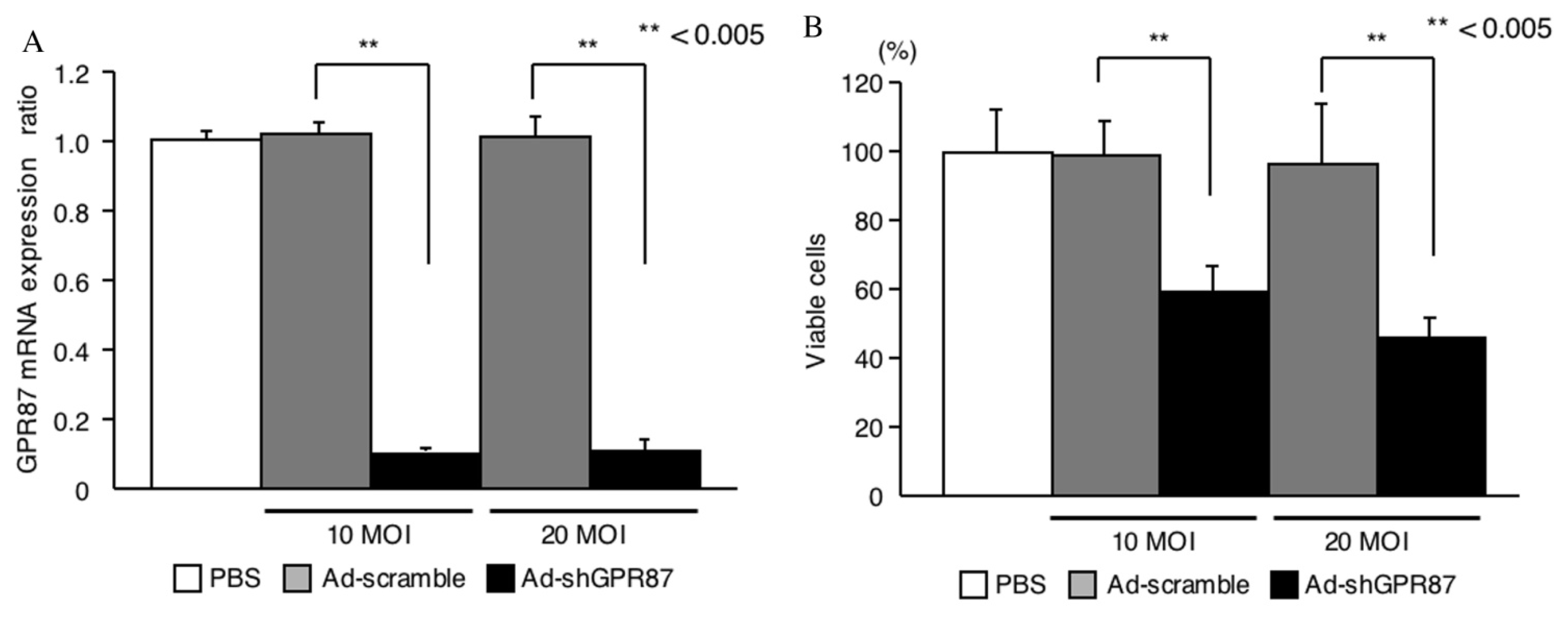
2.2. GPR87 Knockdown
2.3. GPR87 Expression in Tumors
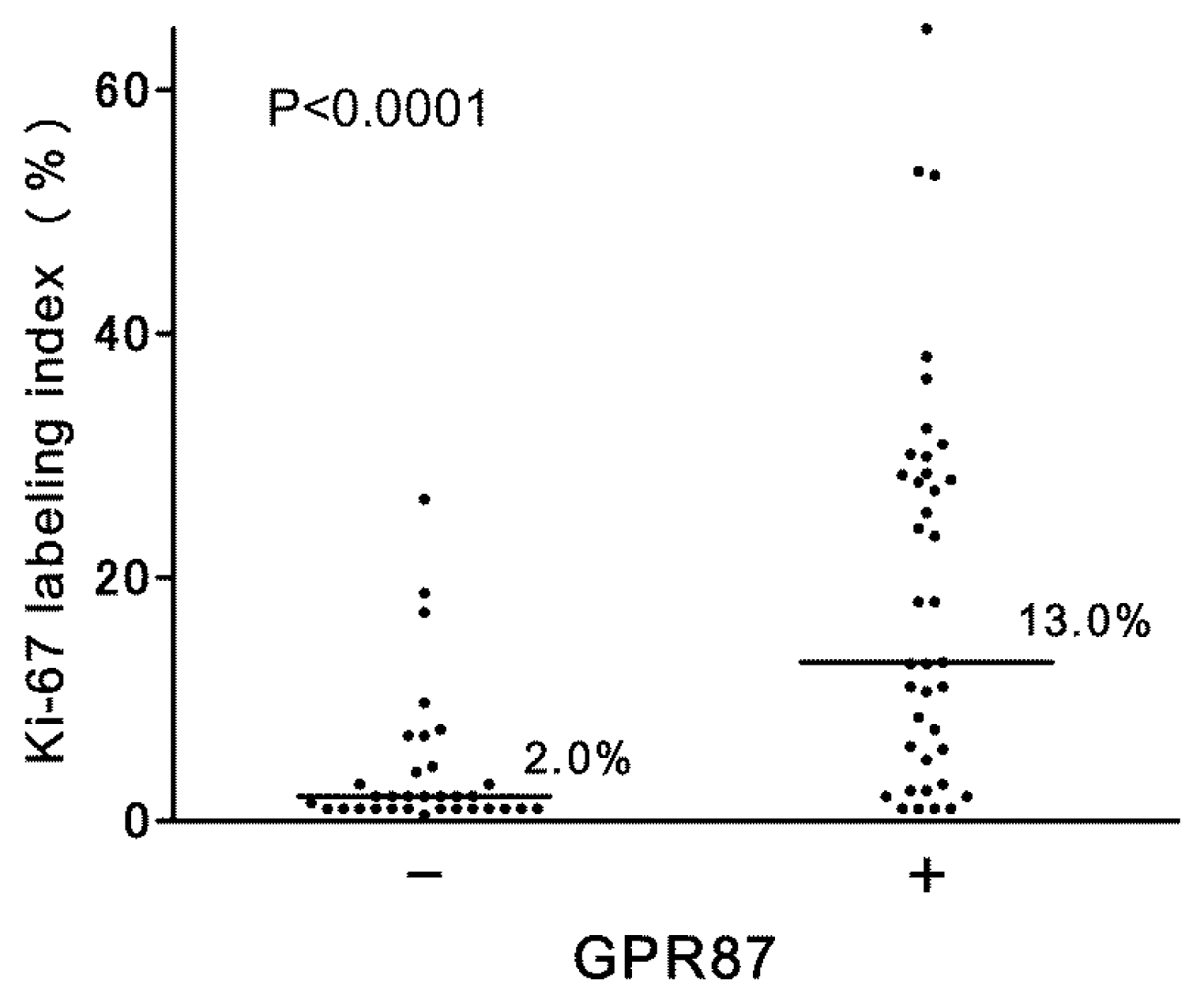
2.3.1. Association with Proliferation
2.3.2. Association with Intravesical Recurrence and Progression
3. Experimental Section
3.1. Cell Lines
3.2. RNA Preparation and Real-Time RT-PCR
3.3. Protein Preparation and Western Blots
3.4. Ad-shGPR87 Mediated Knockdown
3.5. Cell Proliferation
3.6. Patients and Tissue Specimens
3.7. Immunohistochemistry
3.8. Statistical Analysis
4. Conclusions
Acknowledgments
Abbreviations
| GPR87 | G protein-coupled receptor 87 |
| GPCR | G protein-coupled receptor |
| LPA | lysophosphatidic acid |
| RT-PCR | reverse-transcription polymerase chain reaction |
| lysoPLD | lysophospholipase D |
| MTT | 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide |
| shRNA | short hairpin RNA |
| cDNA | complementary DNA |
| GAPDH | glyceraldehyde 3-phosphate dehydrogenase |
| MOI | multiplicity of infection |
Conflict of Interest
References
- Fredriksson, R.; Lagerstrom, M.C.; Lundin, L.G.; Schioth, H.B. The G-protein-coupled receptors in the human genome form five main families. Phylogenetic analysis, paralogon groups, and fingerprints. Mol. Pharmacol 2003, 63, 1256–1272. [Google Scholar]
- Dorsam, R.T.; Gutkind, J.S. G-protein-coupled receptors and cancer. Nat. Rev. Cancer 2007, 7, 79–94. [Google Scholar]
- Hakak, Y.; Shrestha, D.; Goegel, M.C.; Behan, D.P.; Chalmers, D.T. Global analysis of G-protein-coupled receptor signaling in human tissues. FEBS Lett 2003, 550, 11–17. [Google Scholar]
- Howard, A.D.; McAllister, G.; Feighner, S.D.; Liu, Q.; Nargund, R.P.; van der Ploeg, L.H.; Patchett, A.A. Orphan G-protein-coupled receptors and natural ligand discovery. Trends Pharmacol. Sci 2001, 22, 132–140. [Google Scholar]
- Lee, D.K.; Nguyen, T.; Lynch, K.R.; Cheng, R.; Vanti, W.B.; Arkhitko, O.; Lewis, T.; Evans, J.F.; George, S.R.; O’Dowd, B.F. Discovery and mapping of ten novel G protein-coupled receptor genes. Gene 2001, 275, 83–91. [Google Scholar]
- Tabata, K.; Baba, K.; Shiraishi, A.; Ito, M.; Fujita, N. The orphan GPCR GPR87 was deorphanized and shown to be a lysophosphatidic acid receptor. Biochem. Biophys. Res. Commun 2007, 363, 861–866. [Google Scholar]
- Takuwa, Y.; Takuwa, N.; Sugimoto, N. The Edg family G protein-coupled receptors for lysophospholipids: Their signaling properties and biological activities. J. Biochem 2002, 131, 767–771. [Google Scholar]
- Zeng, Y.; Kakehi, Y.; Nouh, M.A.; Tsunemori, H.; Sugimoto, M.; Wu, X.X. Gene expression profiles of lysophosphatidic acid-related molecules in the prostate: Relevance to prostate cancer and benign hyperplasia. Prostate 2009, 69, 283–292. [Google Scholar]
- Gugger, M.; White, R.; Song, S.; Waser, B.; Cescato, R.; Riviere, P.; Reubi, J.C. GPR87 is an overexpressed G-protein coupled receptor in squamous cell carcinoma of the lung. Dis. Markers 2008, 24, 41–50. [Google Scholar]
- Glatt, S.; Halbauer, D.; Heindl, S.; Wernitznig, A.; Kozina, D.; Su, K.C.; Puri, C.; Garin-Chesa, P.; Sommergruber, W. hGPR87 contributes to viability of human tumor cells. Int. J. Cancer J. Int. Cancer 2008, 122, 2008–2016. [Google Scholar]
- Lummen, G.; Virchow, S.; Rumenapp, U.; Schmidt, M.; Wieland, T.; Otto, T.; Rubben, H.; Jakobs, K.H. Identification of G protein-coupled receptors potently stimulating migration of human transitional-cell carcinoma cells. Naunyn-Schmiedeberg’s Archives Pharmacol 1997, 356, 769–776. [Google Scholar]
- Blazer-Yost, B.L.; Blacklock, B.J.; Flaig, S.; Bacallao, R.L.; Gattone, V.H. Lysophosphatidic acid is a modulator of cyst growth in autosomal dominant polycystic kidney disease. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol 2011, 28, 1255–1264. [Google Scholar]
- Rubben, H.; Lutzeyer, W.; Fischer, N.; Deutz, F.; Lagrange, W.; Giani, G. Natural history and treatment of low and high risk superficial bladder tumors. J. Urol 1988, 139, 283–285. [Google Scholar]
- Ozono, S.; Hinotsu, S.; Tabata, S.; Takashima, K.; Fujimoto, K.; Okajima, E.; Hirao, Y.; Ohashi, Y.; Akaza, H.; Fukushima, S. Treated natural history of superficial bladder cancer. Jpn. J. Clin. Oncol 2001, 31, 536–540. [Google Scholar]
- Babjuk, M.; Oosterlinck, W.; Sylvester, R.; Kaasinen, E.; Bohle, A.; Palou-Redorta, J.; Roupret, M. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder, the 2011 update. Eur. Urol 2011, 59, 997–1008. [Google Scholar]
- Sylvester, R.J.; van der Meijden, A.P.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.W.; Kurth, K. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: A combined analysis of 2596 patients from seven EORTC trials. Eur. Urol 2006, 49, 466–465, ; discussion 475–477.. [Google Scholar]
- Millan-Rodriguez, F.; Chechile-Toniolo, G.; Salvador-Bayarri, J.; Palou, J.; Vicente-Rodriguez, J. Multivariate analysis of the prognostic factors of primary superficial bladder cancer. J. Urol 2000, 163, 73–78. [Google Scholar]
- Sakai, I.; Miyake, H.; Harada, K.; Hara, I.; Inoue, T.A.; Fujisawa, M. Analysis of factors predicting intravesical recurrence of superficial transitional cell carcinoma of the bladder without concomitant carcinoma in situ. Int. J. Urol. Off. J. Jpn. Urol. Assoc 2006, 13, 1389–1392. [Google Scholar]
- Lou, L.; Chen, Y.X.; Jin, L.; Li, X.; Tao, X.; Zhu, J.; Chen, X.; Wu, S.; Ye, W.; He, J.; et al. Enhancement of invasion of hepatocellular carcinoma cells through lysophosphatidic acid receptor. J. Int. Med. Res 2013, 41, 55–63. [Google Scholar]
- Ward, Y.; Lake, R.; Yin, J.J.; Heger, C.D.; Raffeld, M.; Goldsmith, P.K.; Merino, M.; Kelly, K. LPA receptor heterodimerizes with CD97 to amplify LPA-initiated RHO-dependent signaling and invasion in prostate cancer cells. Cancer Res 2011, 71, 7301–7311. [Google Scholar]
- Nouh, M.A.; Wu, X.X.; Okazoe, H.; Tsunemori, H.; Haba, R.; Abou-Zeid, A.M.; Saleem, M.D.; Inui, M.; Sugimoto, M.; Aoki, J.; et al. Expression of autotaxin and acylglycerol kinase in prostate cancer: Association with cancer development and progression. Cancer Sci 2009, 100, 1631–1638. [Google Scholar]
- Takahashi, A.; Tsukamoto, T.; Tobisu, K.; Shinohara, N.; Sato, K.; Tomita, Y.; Komatsubara, S.; Nishizawa, O.; Igarashi, T.; Fujimoto, H.; et al. Radical cystectomy for invasive bladder cancer: Results of multi-institutional pooled analysis. Jpn. J. Clin. Oncol 2004, 34, 14–19. [Google Scholar]
- Santos, L.; Amaro, T.; Costa, C.; Pereira, S.; Bento, M.J.; Lopes, P.; Oliveira, J.; Criado, B.; Lopes, C. Ki-67 index enhances the prognostic accuracy of the urothelial superficial bladder carcinoma risk group classification. Int. J. Cancer J. Int. Cancer 2003, 105, 267–272. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| Hazard ratio | 95% CI | p | Hazard ratio | 95% CI | p | |
| Gender (M vs. F) | 1.55 | 0.690–3.486 | 0.289 | |||
| Onset (primary vs. recurrence) | 1.17 | 0.587–2.345 | 0.652 | |||
| Multiplicity (single vs. multiple) | 2.41 | 1.211–4.811 | 0.012 | 1.87 | 0.873–4.911 | 0.107 |
| Maximal tumor size (<3 cm vs. ≥3 cm) | 3.16 | 1.096–9.090 | 0.033 | 1.53 | 0.638–3.689 | 0.339 |
| Tumor type (papillary vs. non-papillary) | 1.45 | 0.574–3.663 | 0.432 | |||
| T stage (Ta vs. T1) | 1.54 | 0.661–3.585 | 0.318 | |||
| Grade (low grade vs. high grade) | 1.21 | 0.585–2.489 | 0.610 | |||
| Adjuvant intravesical chemotherapy | 1.21 | 0.614–2.381 | 0.582 | |||
| Ki-67 (<18% vs. ≥18%) | 1.61 | 0.555–2.426 | 0.691 | |||
| GPR87 (negative vs. positive) | 2.40 | 1.230–4.666 | 0.010 | 2.25 | 1.035–4.911 | 0.041 |
| Parameters | ||
|---|---|---|
| Age | range, median | 41–95, 72 |
| Gender | M | 59 |
| F | 12 | |
| Stage | Tis | 2 |
| Ta | 53 | |
| T1 | 16 | |
| Tumor grade (2004WHO/ISUP) | Low grade | 46 |
| High grade | 25 | |
| Multiplicity of tumor | Single | 34 |
| Multiple | 37 | |
| Tumor type | papillary | 58 |
| non-papillary | 13 | |
| Maxmal tumor size | <3 cm | 54 |
| ≥3 cm | 12 | |
| unknown | 5 | |
| On-set | Primary | 44 |
| Recurrence | 27 | |
| Adjuvant intravesical chemotherapy | Yes | 31 |
| No | 40 | |
| Ki-67 index | <18% | 50 |
| ≥18% | 21 | |
| GPR87 | positive | 38 |
| negative | 33 | |
© 2013 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Okazoe, H.; Zhang, X.; Liu, D.; Shibuya, S.; Ueda, N.; Sugimoto, M.; Kakehi, Y. Expression and Role of GPR87 in Urothelial Carcinoma of the Bladder. Int. J. Mol. Sci. 2013, 14, 12367-12379. https://doi.org/10.3390/ijms140612367
Okazoe H, Zhang X, Liu D, Shibuya S, Ueda N, Sugimoto M, Kakehi Y. Expression and Role of GPR87 in Urothelial Carcinoma of the Bladder. International Journal of Molecular Sciences. 2013; 14(6):12367-12379. https://doi.org/10.3390/ijms140612367
Chicago/Turabian StyleOkazoe, Homare, Xia Zhang, Dage Liu, Shinsuke Shibuya, Nobufumi Ueda, Mikio Sugimoto, and Yoshiyuki Kakehi. 2013. "Expression and Role of GPR87 in Urothelial Carcinoma of the Bladder" International Journal of Molecular Sciences 14, no. 6: 12367-12379. https://doi.org/10.3390/ijms140612367