The hOGG1 Ser326Cys Gene Polymorphism and the Risk of Coronary Ectasia in the Chinese Population

Abstract
:1. Introduction
2. Results and Discussion
2.1. Clinical Characteristics
2.2. hOGG1 Ser326Cys Genotype
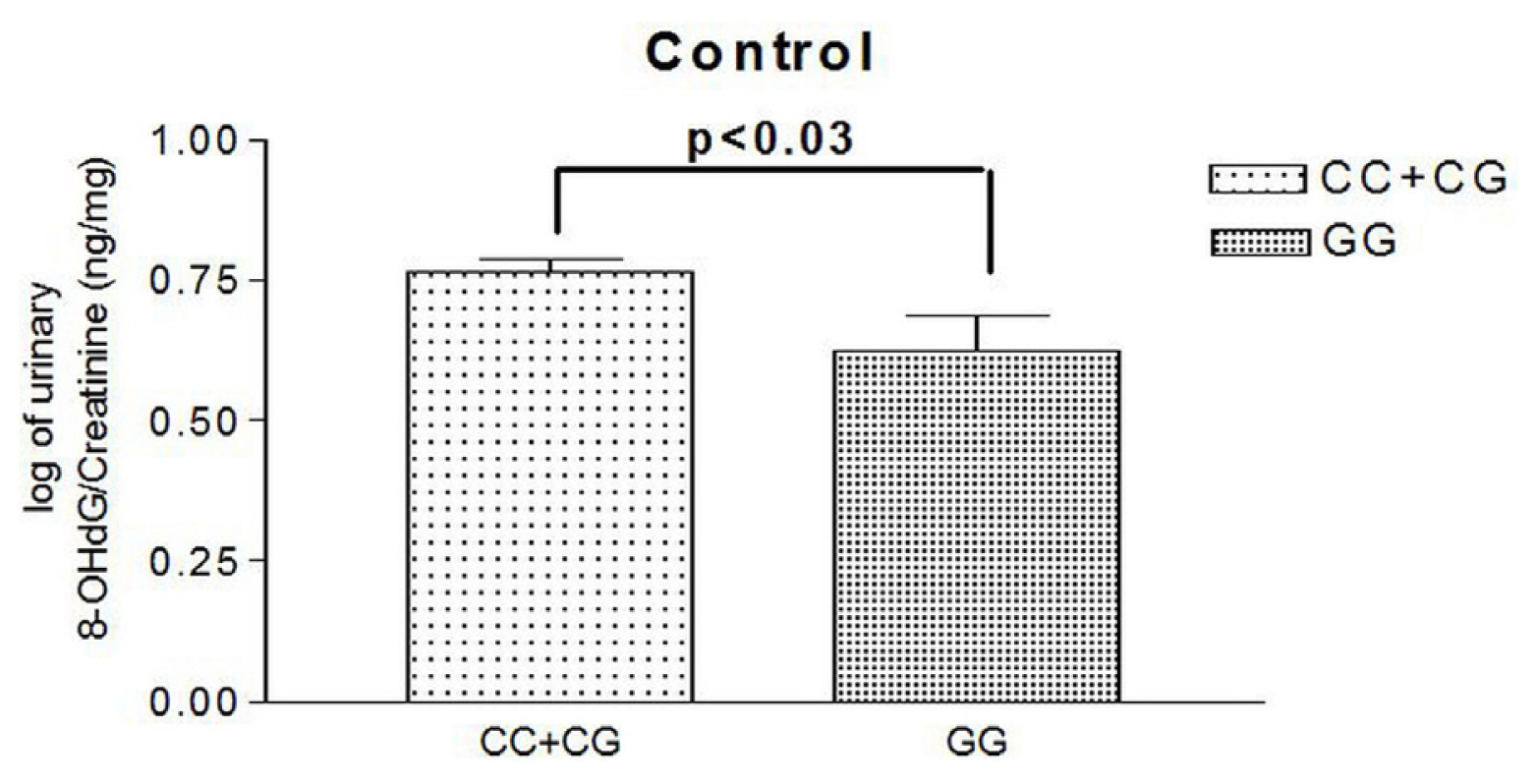
2.3. Urinary Levels of 8OHdG
2.4. Multivariate Regression Analysis
2.5. Discussion
3. Experimental Section
3.1. Study Subjects
3.2. Coronary Angiography
3.3. DNA Isolation and Genotyping
3.4. Urine 8OHdG Measurement by Enzyme-Linked Immunosorbent Assay (ELISA)
3.5. Statistical Analysis
4. Conclusions
Acknowledgments
Conflicts of Interest
References
- Oliveros, R.A.; Falsetti, H.L.; Carroll, R.J.; Heinle, R.A.; Ryan, G.F. Atherosclerotic coronary artery aneurysm: Report of five cases and a review of the literature. Arch. Intern. Med 1974, 134, 1072–1076. [Google Scholar]
- Swaye, P.S.; Fisher, L.D.; Litwin, P.; Vignola, P.A.; Judkins, M.P.; Kemp, H.G.; Mudd, J.G.; Gosselin, A.J. Aneurysmal coronary artery disease. Circulation 1983, 67, 134–138. [Google Scholar]
- Hartnell, G.G.; Parnell, B.M.; Pridie, R.B. Coronary artery ectasia. Its prevalence and clinical significance in 4993 patients. Br. Heart. J 1985, 54, 392–395. [Google Scholar]
- Yilmaz, H.; Sayar, N.; Yilmaz, M.; Tangürek, B.; Cakmak, N.; Gürkan, U.; Gül, M.; Simşek, D.; Bolca, O. Coronary artery ectasia: clinical and angiographical evaluation. Turk. Kardiyol. Dern. Ars 2008, 36, 530–535. [Google Scholar]
- Sharma, S.N.; Kaul, U.; Sharma, S.; Wasir, H.S.; Manchanda, S.C.; Bahl, V.K.; Talwar, K.K.; Rajani, M.; Bhatia, M.L. Coronary arteriographic profile in young and old Indian patients with ischaemic heart disease: A comparative study. Indian Heart J 1990, 42, 365–369. [Google Scholar]
- Swanton, R.H.; Thomas, M.L.; Coltart, D.J.; Jenkins, B.S.; Webb-Peploe, M.M.; Williams, B.T. Coronary artery ectasia—A variant of occlusive coronary arteriosclerosis. Br. Heart. J 1978, 40, 393–400. [Google Scholar]
- Rodbars, S.; Ikeda, K.; Montes, M. An analysis of mechanisms of poststenotic dilatation. Angiology 1967, 18, 349–353. [Google Scholar]
- Ozbay, Y.; Akbulut, M.; Balin, M.; Kayancicek, H.; Baydas, A.; Korkmaz, H. The level of hs-CRP in coronary artery ectasia and its response to statin and angiotensin-converting enzyme inhibitor treatment. Mediators Inflamm 2007, 2007, 89649. [Google Scholar]
- Li, J.J.; Nie, S.P.; Qian, X.W.; Zeng, H.S.; Zhang, C.Y. Chronic inflammatory status in patients with coronary artery ectasia. Cytokine 2009, 46, 61–64. [Google Scholar]
- Sezen, Y.; Bas, M.; Polat, M.; Yildiz, A.; Buyukhatipoglu, H.; Kucukdurmaz, Z.; Kaya, Z.; Demirbag, R. The relationship between oxidative stress and coronary artery ectasia. Cardiol. J 2010, 17, 488–494. [Google Scholar]
- Singh, U.; Jialal, I. Oxidative stress and atherosclerosis. Pathophysiology 2006, 13, 129–142. [Google Scholar]
- Vogiatzi, G.; Tousoulis, D.; Stefanadis, C. The role of oxidative stress in atherosclerosis. Hellenic. J. Cardiol 2009, 50, 402–409. [Google Scholar]
- Suzuki, S.; Kaneko, M.; Chapman, D.C.; Dhalla, N.S. Alterations in cardiac contractile proteins due to oxygen free radicals. Biochim. Biophys. Acta 1991, 24, 95–100. [Google Scholar]
- Biglioli, P.; Cannata, A.; Alamanni, F.; Naliato, M.; Porqueddu, M.; Zanobini, M.; Tremoli, E.; Parolari, A. Biological effects of off-pump vs. on-pump coronary artery surgery: Focus on inflammation, hemostasis and oxidative stress. Eur. J. Cardiothorac. Surg 2003, 24, 260–269. [Google Scholar]
- Madamanchi, N.R.; Hakim, Z.S.; Runge, M.S. Oxidative stress in atherogenesis and arterial thrombosis: The disconnect between cellular studies and clinical outcomes. J. Thromb. Haemost 2005, 3, 254–267. [Google Scholar]
- Wiseman, H.; Halliwell, B. Damage to DNA by reactive oxygen and nitrogen species: Role in inflammatory disease and progression to cancer. Biochem. J 1996, 313, 17–29. [Google Scholar]
- Shibutani, S.; Takeshita, M.; Grollman, A.P. Insertion of specific bases during DNA synthesis past the oxidation-damaged base 8-oxodG. Nature 1991, 349, 431–434. [Google Scholar]
- Wu, L.L.; Chiou, C.C.; Chang, P.Y.; Wu, J.T. Urinary 8-OHdG: A marker of oxidative stress to DNA and a risk factor for cancer, atherosclerosis and diabetics. Clin. Chim. Acta 2004, 339, 1–9. [Google Scholar]
- Croteau, D.L.; Bohr, V.A. Repair of oxidative damage to nuclear and mitochondrial DNA in mammalian cells. J. Biol. Chem 1997, 272, 25409–25412. [Google Scholar]
- Bruner, S.D.; Norman, D.P.; Verdine, G.L. Structural basis for rec ognition and repair of the endogenous mutagen 8-oxoguanine in DNA. Nature 2000, 403, 859–866. [Google Scholar]
- Li, H.; Hao, X.; Zhang, W.; Wei, Q.; Chen, K. The hOGG1 Ser326Cys polymorphism and lung cancer risk: a meta-analysis. Cancer. Epidemiol. Biomarkers Prev 2008, 17, 1739–1745. [Google Scholar]
- Xing, D.Y.; Tan, W.; Song, N.; Lin, D.X. Ser326Cys polymorphism in hOGG1 gene and risk of esophageal cancer in a Chinese population. Int. J. Cancer 2001, 95, 140–143. [Google Scholar]
- Xu, J.; Zheng, S.L.; Turner, A.; Isaacs, S.D.; Wiley, K.E.; Hawkins, G.A.; Chang, B.L.; Bleecker, E.R.; Walsh, P.C.; Meyers, D.A.; et al. Associations between hOGG1 sequence variants and prostate cancer susceptibility. Cancer Res 2002, 62, 2253–2257. [Google Scholar]
- Tsukino, H.; Hanaoka, T.; Otani, T.; Iwasaki, M.; Kobayashi, M.; Hara, M.; Natsukawa, S.; Shaura, K.; Koizumi, Y.; Kasuga, Y.; et al. hOGG1 Ser326Cys polymorphism, interaction with environmental exposures, and gastric cancer risk in Japanese populations. Cancer. Sci 2004, 95, 977–983. [Google Scholar]
- Jiao, X.; Huang, J.; Wu, S.; Lv, M.; Hu, Y.; Jianfu; Su, X.; Luo, C.; Ce, B. hOGG1 Ser326Cys polymorphism and susceptibility to gallbladder cancer in a Chinese population. Int. J. Cancer 2007, 121, 501–505. [Google Scholar]
- Zhao, H.; Qin, C.; Yan, F.; Wu, B.; Cao, Q.; Wang, M.; Zhang, Z.; Yin, C. hOGG1 Ser326Cys polymorphism and renal cell carcinoma risk in a Chinese population. DNA. Cell. Biol 2011, 30, 317–321. [Google Scholar]
- Wang, C.L.; Hsieh, M.C.; Hsin, S.C.; Lin, H.Y.; Lin, K.D.; Lo, C.S.; Chen, Z.H.; Shin, S.J. The hOGG1 Ser326Cys gene polymorphism is associated with decreased insulin sensitivity in subjects with normal glucose tolerance. J. Hum. Genet 2006, 51, 124–128. [Google Scholar]
- Sun, C.; Liu, X.; Zhang, H.; Guo, W.; Cai, Z.; Chen, H.; Zhang, K.; Zhu, D.; Wang, Y. Functional polymorphism of hOGG1 gene is associated with type 2 diabetes mellitus in Chinese population. Mol. Cell. Endocrinol 2010, 325, 128–134. [Google Scholar]
- Wang, C.L.; Lin, T.H.; Lin, H.Y.; Sheu, S.H.; Yu, M.L.; Hsiao, P.J.; Lin, K.D.; Hsu, C.; Yang, Y.H.; Shin, S.J. The 8-oxoguanine glycosylase I (hOGG1) Ser326Cys variant affects the susceptibility to multi-vessel disease in Taiwan coronary artery disease patients. Thromb. Res 2010, 126, 319–323. [Google Scholar]
- Chiou, C.C.; Chang, P.Y.; Chan, E.C.; Wu, T.L.; Tsao, K.C.; Wu, J.T. Urinary 8-hydroxydeoxyguanosine and its analogs as DNA marker of oxidative stress: Development of an ELISA and measurement in both bladder and prostate cancers. Clin. Chim. Acta 2003, 334, 87–94. [Google Scholar]
- Negishi, H.; Ikeda, K.; Kuga, S.; Noguchi, T.; Kanda, T.; Njelekela, M.; Liu, L.; Miki, T.; Nara, Y.; Sato, T.; et al. The relation of oxidative DNA damage to hypertension and other cardiovascular risk factors in Tanzania. J. Hypertens 2001, 19, 529–533. [Google Scholar]
- Serdar, M.; Sertoglu, E.; Uyanik, M.; Tapan, S.; Akin, K.; Bilgi, C.; Kurt, I. Comparison of 8-hydroxy-2′-deoxyguanosine (8-OHdG) levels using mass spectrometer and urine albumin creatinine ratio as a predictor of development of diabetic nephropathy. Free. Radic. Res 2012, 46, 1291–1295. [Google Scholar]
- Xu, G.W.; Yao, Q.H.; Weng, Q.F.; Su, B.L.; Zhang, X.; Xiong, J.H. Study of urinary 8-hydroxydeoxyguanosine as a biomarker of oxidative DNA damage in diabetic nephropathy patients. J. Pharm. Biomed. Anal 2004, 36, 101–104. [Google Scholar]
- Aka, P.; Mateuca, R.; Buchet, J.P.; Thierens, H.; Kirsch-Volders, M. Are genetic polymorphisms in OGG1, XRCC1 and XRCC3 genes predictive for the DNA strand break repair phenotype and genotoxicity in workers exposed to low dose ionising radiations? Mutat. Res 2004, 556, 169–181. [Google Scholar]
- Thomas, D.; Scot, A.D.; Barbey, R.; Padula, M.; Boiteux, S. Inactivation of OGG1 increases the incidence of G. C-->T. A transversions in Saccharomyces cerevisiae: Evidence for endogenous oxidative damage to DNA in eukaryotic cells. Mol. Gen. Genet 1997, 254, 171–178. [Google Scholar]
- Ross, R. Atherosclerosis--an inflammatory disease. N. Engl. J. Med 1999, 340, 115–126. [Google Scholar]
- Befeler, B.; Aranda, M.J.; Embi, A.; Mullin, F.L.; El-Sherif, N.; Lazzara, R. Coronary artery aneurysms: study of their etiology, clinical course and effect on left ventricular function and prognosis. Am. J. Cardiol 1977, 62, 597–607. [Google Scholar]
- Waly, H.M.; Elayda, M.A.; Lee, V.V.; El-Said, G.; Reul, G.J.; Hall, R.J. Coronary artery ectasia in Egyptian patients with coronary artery disease. Tex. Heart. Inst. J 1997, 24, 349–352. [Google Scholar]


{kind=link}
| Parameters | Non-CE N = 494 | CE N = 53 | p-value |
|---|---|---|---|
| N (%) or Mean ± SD | |||
| Sex (male) | 348 (70.4) | 42 (79.2) | 0.178 |
| Age (years) | 61.6 ± 12.4 | 62.8 ± 12.7 | 0.502 |
| DM | 180 (36.4) | 15 (28.3) | 0.240 |
| Hypertension | 315 (63.8) | 40 (75.5) | 0.090 |
| Smoking | 257 (52.0) | 32 (60.4) | 0.247 |
| Family history of premature CAD | 11 (2.2) | 1 (1.9) | 1.000 |
| Hypercholesterolemia (%) | 255 (51.6) | 21 (39.6) | 0.097 |
| CAD number | 0.431 | ||
| Non-significant lesion | 156 (31.7) | 15 (28.3) | |
| 1-vessel disease | 107 (21.7) | 13 (24.5) | |
| 2-vessel disease | 83 (16.9) | 13 (24.5) | |
| 3-vessel disease | 146 (29.7) | 12 (22.6) | |
| BMI | 25.3 ± 3.5 | 26.6 ± 5.0 | 0.074 |
| Previous ACS | 30 (9.4) | 23 (10.1) | 0.768 |
| Medication | |||
| Aspirin | 210 (42.5) | 25 (47.2) | 0.515 |
| Clopidogrel | 48 (9.7) | 7 (13.2) | 0.422 |
| β-blocker | 177 (35.8) | 20 (37.7) | 0.784 |
| Nitrate | 143 (28.9) | 17 (32.1) | 0.634 |
| ACEI | 99 (20.0) | 11 (20.8) | 0.902 |
| ARB | 101 (20.4) | 11 (20.8) | 0.958 |
| CCB | 138 (27.9) | 13 (24.5) | 0.598 |
| Diuretic | 79 (16.0) | 7 (13.2) | 0.597 |
| Statin | 98 (19.8) | 9 (17.0) | 0.618 |
| Ectasia location | N (%) |
|---|---|
| Right coronary artery | 29 (5.3) |
| Left anterior descending artery | 1 (0.2) |
| Left circumflex artery | 12 (2.2) |
| Right coronary artery + left anterior descending artery | 5 (0.9) |
| Right coronary artery + left circumflex artery | 3 (0.5) |
| Left anterior descending artery + left circumflex artery | 0 |
| All three vessels | 3 (0.5) |
| Number of ectatic vessels in patients with coronary ectasia | |
| 1 | 42 (7.7) |
| 2 | 8 (1.4) |
| 3 | 3 (0.5) |
| Polymorphism site | Non-CE N (%) | CE N (%) | OR (95% CI) | p-value | aOR * (95% CI) | p-value |
|---|---|---|---|---|---|---|
| Allele frequency | ||||||
| G | 609 (61.6) | 54 (50.9) | 1 | 1 | ||
| C | 379 (38.4) | 52 (49.1) | 1.55 (1.04–2.31) | 0.033 | 1.55 (1.03–2.33) | 0.037 |
| Genotype | ||||||
| GG | 182 (36.8) | 10 (18.9) | 1 | 1 | ||
| CG | 245 (49.6) | 34 (64.2) | 2.45 (0.95–6.28) | 0.063 | 2.41 (0.92–6.29) | 0.074 |
| CC | 67 (13.6) | 9 (17.0) | 2.53 (1.22–5.25) | 0.013 | 2.624 (1.24–5.53) | 0.011 |
| Dominant model | ||||||
| GG | 182 (36.8) | 10 (18.9) | 1 | 1 | ||
| CG + CC | 312 (63.2) | 43 (81.1) | 2.51 (1.23–5.11) | 0.011 | 2.57 (1.25–5.32) | 0.011 |
| Polymorphism site | Control group N (%) | CE group N (%) | OR (95% CI) | p-value | aOR * (95% CI) | p-value |
|---|---|---|---|---|---|---|
| Allele frequency | ||||||
| G | 196 (62.8) | 54 (50.9) | 1 | 1 | ||
| C | 116 (37.2) | 52 (49.1) | 1.63 (1.04–2.54) | 0.032 | 1.64 (1.00–2.68) | 0.049 |
| Genotype | ||||||
| GG | 61 (39.1) | 10 (18.9) | 1 | 1 | ||
| CG | 74 (47.4) | 34 (64.2) | 2.61 (0.94–7.31) | 0.067 | 2.65 (0.84–8.34) | 0.097 |
| CC | 21 (13.5) | 9 (17.0) | 2.80 (1.28–6.13) | 0.010 | 2.941 (1.24–7.00) | 0.015 |
| Dominant model | ||||||
| GG | 61 (39.1) | 10 (18.9) | 1 | 1 | ||
| CG + CC | 95 (60.9) | 43 (81.1) | 2.76 (1.29–5.90) | 0.009 | 2.88 (1.24–6.67) | 0.014 |
| Variables | OR | 95% CI | p-value |
|---|---|---|---|
| Age | 1.02 | 0.99–1.05 | 0.132 |
| Sex (male vs. female) | 1.57 | 0.64–3.81 | 0.325 |
| Hypertension | 1.86 | 0.94–3.71 | 0.077 |
| Diabetes | 0.53 | 0.27–1.01 | 0.055 |
| Hypercholesterolemia | 0.56 | 0.31–1.03 | 0.062 |
| Body mass index | 1.11 | 1.03–1.20 | 0.009 |
| Smoking | 0.88 | 0.42–1.85 | 0.736 |
| Family history of premature CAD | 1.27 | 0.15–10.59 | 0.826 |
| hOGG1 CG + CC vs. GG | 2.57 | 1.25–5.32 | 0.011 |
© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Hsu, P.-C.; Wang, C.-L.; Su, H.-M.; Juo, S.-H.; Lin, T.-H.; Voon, W.-C.; Shin, S.-J.; Lai, W.-T.; Sheu, S.-H. The hOGG1 Ser326Cys Gene Polymorphism and the Risk of Coronary Ectasia in the Chinese Population. Int. J. Mol. Sci. 2014, 15, 1671-1682. https://doi.org/10.3390/ijms15011671
Hsu P-C, Wang C-L, Su H-M, Juo S-H, Lin T-H, Voon W-C, Shin S-J, Lai W-T, Sheu S-H. The hOGG1 Ser326Cys Gene Polymorphism and the Risk of Coronary Ectasia in the Chinese Population. International Journal of Molecular Sciences. 2014; 15(1):1671-1682. https://doi.org/10.3390/ijms15011671
Chicago/Turabian StyleHsu, Po-Chao, Chiao-Ling Wang, Ho-Ming Su, Suh-Hang Juo, Tsung-Hsien Lin, Wen-Chol Voon, Shyi-Jang Shin, Wen-Ter Lai, and Sheng-Hsiung Sheu. 2014. "The hOGG1 Ser326Cys Gene Polymorphism and the Risk of Coronary Ectasia in the Chinese Population" International Journal of Molecular Sciences 15, no. 1: 1671-1682. https://doi.org/10.3390/ijms15011671