Combined MicroRNA-340 and ROCK1 mRNA Profiling Predicts Tumor Progression and Prognosis in Pediatric Osteosarcoma

Abstract
:1. Introduction
2. Results
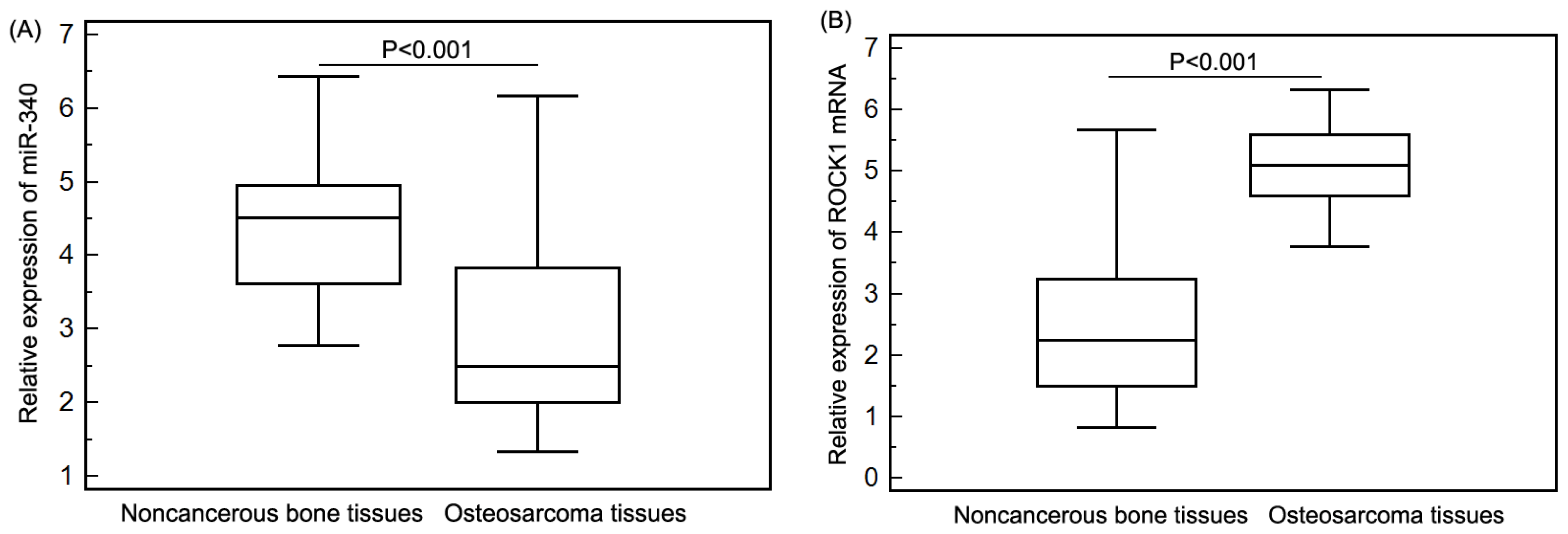
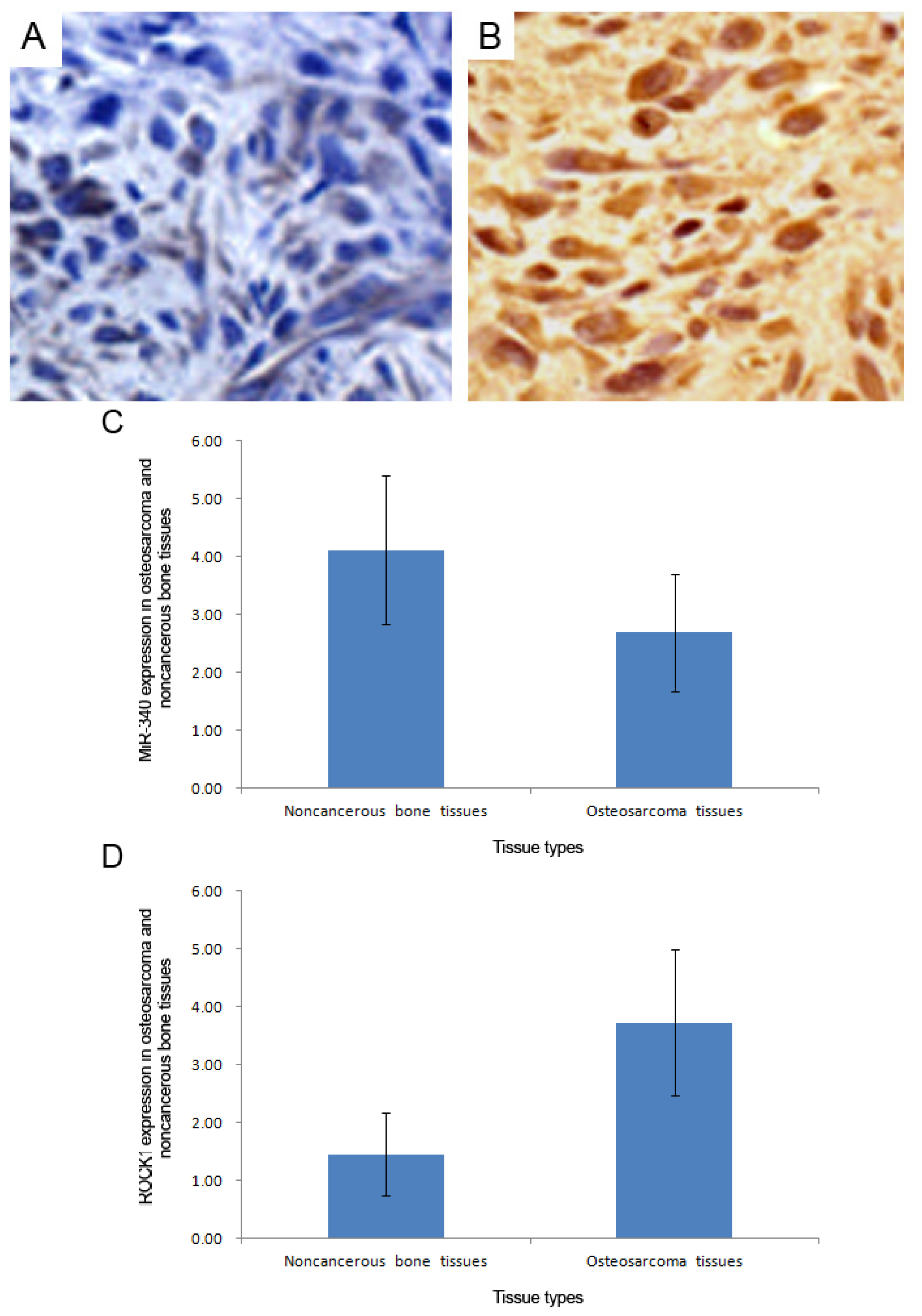
2.1. Expression Patterns of miR-340 and ROCK1 in Pediatric Osteosarcoma Tissues
2.2. miR-340 Downregulation and ROCK1 Upregulation Associate with Aggressive Clinicopathological Features of Pediatric Osteosarcoma
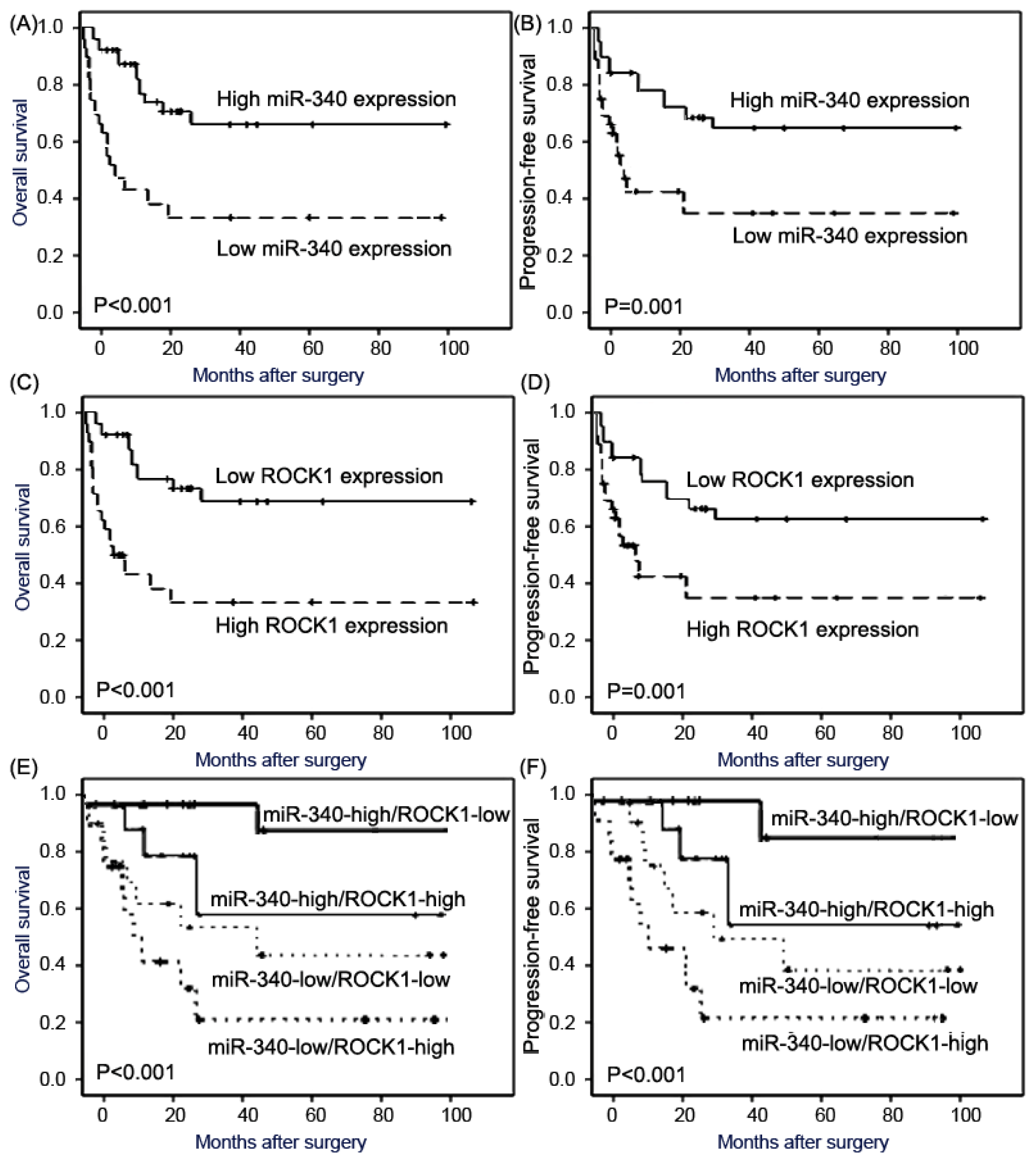
2.3. miR-340 Downregulation and ROCK1 Upregulation Confer Poor Prognosis in Pediatric Osteosarcoma
3. Discussion
4. Materials and Methods
4.1. Patients and Tissue Samples
4.2. RNA Extraction
4.3. miRNA and mRNA qRT-PCR Assay
4.4. In Situ Hybridization
4.5. Immunohistochemistry Analysis
4.6. Evaluation of in Situ Hybridization and Immunostaining
4.7. Statistical Analysis
5. Conclusions
Conflicts of Interest
References
- Broadhead, M.L.; Clark, J.C.; Myers, D.E. The molecular pathogenesis of osteosarcoma: A review. Sarcoma 2011, 2011, 959248. [Google Scholar]
- Ottaviani, G.; Jaffe, N. The epidemiology of osteosarcoma. Cancer Treat. Res 2009, 152, 3–13. [Google Scholar]
- Gorlick, R. Current concepts on the molecular biology of osteosarcoma. Cancer Treat. Res 2009, 152, 467–478. [Google Scholar]
- Clark, J.C.; Dass, C.R.; Choong, P.F. A review of clinical and molecular prognostic factors in osteosarcoma. J. Cancer Res. Clin. Oncol 2008, 134, 281–297. [Google Scholar]
- Papachristou, D.J.; Papavassiliou, A.G. Osteosarcoma and chondrosarcoma: New signaling pathways as targets for novel therapeutic interventions. Int. J. Biochem. Cell Biol 2007, 39, 857–862. [Google Scholar]
- Miao, J.; Wu, S.; Peng, Z.; Tania, M.; Zhang, C. MicroRNAs in osteosarcoma: Diagnostic and therapeutic aspects. Tumor Biol 2013, 34, 2093–2098. [Google Scholar]
- Nana-Sinkam, S.P.; Croce, C.M. Clinical applications for microRNAs in cancer. Clin. Pharmacol. Ther 2013, 93, 98–104. [Google Scholar]
- Shen, J.; Stass, S.A.; Jiang, F. MicroRNAs as potential biomarkers in human solid tumors. Cancer Lett 2013, 329, 125–136. [Google Scholar]
- Osman, A. MicroRNAs in health and disease—Basic science and clinical applications. Clin. Lab 2012, 58, 393–402. [Google Scholar]
- Amiel, J.; de Pontual, L.; Henrion-Caude, A. miRNA, development and disease. Adv. Genet 2012, 80, 1–36. [Google Scholar]
- Fabbri, M.; Calore, F.; Paone, A.; Galli, R.; Calin, G.A. Epigenetic regulation of miRNAs in cancer. Adv. Exp. Med. Biol 2013, 754, 137–148. [Google Scholar]
- Jones, K.B.; Salah, Z.; Del Mare, S.; Galasso, M.; Gaudio, E.; Nuovo, G.J.; Lovat, F.; LeBlanc, K.; Palatini, J.; Lor Randall, R.; et al. miRNA signatures associate with pathogenesis and progression of osteosarcoma. Cancer Res 2012, 72, 1865–1877. [Google Scholar]
- Cai, H.; Lin, L.; Cai, H.; Tang, M.; Wang, Z. Prognostic evaluation of microRNA-210 expression in pediatric osteosarcoma. Med. Oncol 2013, 30, 499. [Google Scholar]
- Wang, Z.; Cai, H.; Lin, L.; Tang, M.; Cai, H. Upregulated expression of microRNA-214 is linked to tumor progression and adverse prognosis in pediatric osteosarcoma. Pediatr. Blood Cancer 2013, in press. [Google Scholar]
- Novello, C.; Pazzaglia, L.; Cingolani, C.; Conti, A.; Quattrini, I.; Manara, M.C.; Tognon, M.; Picci, P.; Benassi, M.S. miRNA expression profile in human osteosarcoma, role of miR-1 and miR-133b in proliferation and cell cycle control. Int. J. Oncol 2013, 42, 667–675. [Google Scholar]
- Sun, Y.; Zhao, X.; Zhou, Y.; Hu, Y. miR-124, miR-137 and miR-340 regulate colorectal cancer growth via inhibition of the Warburg effect. Oncol. Rep 2012, 28, 1346–1352. [Google Scholar]
- Wu, Z.S.; Wu, Q.; Wang, C.Q.; Wang, X.N.; Huang, J.; Zhao, J.J.; Mao, S.S.; Zhang, G.H.; Xu, X.C.; Zhang, N. miR-340 inhibition of breast cancer cell migration and invasion through targeting of oncoprotein c-Met. Cancer 2011, 117, 2842–2852. [Google Scholar]
- Yao, Y.; Suo, A.L.; Li, Z.F.; Liu, L.Y.; Tian, T.; Ni, L.; Zhang, W.G.; Nan, K.J.; Song, T.S.; Huang, C. MicroRNA profiling of human gastric cancer. Mol. Med. Rep 2009, 2, 963–970. [Google Scholar]
- Zhou, X.; Wei, M.; Wang, W. MicroRNA-340 suppresses osteosarcoma tumor growth and metastasis by directly targeting ROCK1. Biochem. Biophys. Res. Commun 2013, 437, 653–658. [Google Scholar]
- Wang, Y.; Zhao, W.; Fu, Q. miR-335 suppresses migration and invasion by targeting ROCK1 in osteosarcoma cells. Mol. Cell. Biochem 2013, 384, 105–111. [Google Scholar]
- Li, F.; Jiang, Q.; Shi, K.J.; Luo, H.; Yang, Y.; Xu, C.M. RhoA modulates functional and physical interaction between ROCK1 and Erk1/2 in selenite-induced apoptosis of leukaemia cells. Cell Death Dis 2013, 4, e708. [Google Scholar]
- Schofield, A.V.; Bernard, O. Rho-associated coiled-coil kinase (ROCK) signaling and disease. Crit. Rev. Biochem. Mol. Biol 2013, 48, 301–316. [Google Scholar]
- Patel, R.A.; Liu, Y.; Wang, B.; Li, R.; Sebti, S.M. Identification of novel ROCK inhibitors with anti-migratory and anti-invasive activities. Oncogene 2013. [Google Scholar] [CrossRef]
- Vigil, D.; Kim, T.Y.; Plachco, A.; Garton, A.J.; Castaldo, L.; Pachter, J.A.; Dong, H.; Chen, X.; Tokar, B.; Campbell, S.L.; et al. ROCK1 and ROCK2 are required for non-small cell lung cancer anchorage-independent growth and invasion. Cancer Res 2012, 72, 5338–5347. [Google Scholar]
- Wu, Y.J.; Tang, Y.; Li, Z.F.; Li, Z.; Zhao, Y.; Wu, Z.J.; Su, Q. Expression and significance of Rac1, Pak1 and Rock1 in gastric carcinoma. Asia Pac. J. Clin. Oncol 2013. [Google Scholar] [CrossRef]
- Majid, S.; Dar, A.A.; Saini, S.; Shahryari, V.; Arora, S.; Zaman, M.S.; Chang, I.; Yamamura, S.; Chiyomaru, T.; Fukuhara, S.; et al. MicroRNA-1280 inhibits invasion and metastasis by targeting ROCK1 in bladder cancer. PLoS One 2012, 7, e46743. [Google Scholar]
- Liu, X.; Choy, E.; Hornicek, F.J.; Yang, S.; Yang, C.; Harmon, D.; Mankin, H.; Duan, Z. ROCK1 as a potential therapeutic target in osteosarcoma. J. Orthop. Res 2011, 29, 1259–1266. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological features | No. of cases | miR-340-low (n, %) | p | ROCK1-high (n, %) | p | miR-340-low/ROCK1-high (n, %) | p |
|---|---|---|---|---|---|---|---|
| Age | |||||||
| <13 | 52 | 28 (53.85) | NS | 30 (57.69) | NS | 24 (46.15) | NS |
| ≥13 | 40 | 22 (55.00) | 22 (55.00) | 18 (45.00) | |||
| Gender | |||||||
| Male | 56 | 32 (57.14) | NS | 32 (57.14) | NS | 25 (44.64) | NS |
| Female | 36 | 18 (50.00) | 20 (55.56) | 17 (47.22) | |||
| Tumor size (cm) | |||||||
| >8 | 50 | 32 (64.00) | 0.02 | 30 (60.00) | NS | 25 (50.00) | NS |
| ≤8 | 42 | 18 (42.86) | 22 (52.38) | 17 (40.48) | |||
| Localization of the primary tumor | |||||||
| Femur | 53 | 30 (56.60) | NS | 32 (60.38) | NS | 27 (50.94) | NS |
| Tibia | 25 | 15 (60.00) | 15 (60.00) | 10 (40.00) | |||
| Humeral bone | 9 | 3 (33.33) | 3 (33.33) | 3 (33.33) | |||
| Other | 5 | 2 (40.00) | 2 (40.00) | 2 (40.00) | |||
| Pathological facture | |||||||
| Present | 10 | 6 (60.00) | NS | 6 (60.00) | NS | 4 (40.00) | NS |
| Absent | 82 | 44 (53.66) | 46 (56.10) | 38 (46.34) | |||
| Subtype of osteosarcoma | |||||||
| Conventional | 38 | 20 (52.63) | NS | 22 (57.89) | NS | 16 (42.11) | NS |
| Non-conventional | 54 | 30 (55.56) | 30 (55.56) | 26 (48.15) | |||
| Chemotherapy | |||||||
| ADM/DDP | 58 | 32 (55.17) | NS | 32 (55.17) | NS | 26 (44.83) | NS |
| ADM/MTX | 34 | 18 (52.94) | 20 (58.82) | 16 (47.06) | |||
| Metastasis | |||||||
| Present | 31 | 25 (80.65) | 0.00 | 25 (80.65) | 0.00 | 24 (77.42) | <0.001 |
| Absent | 61 | 25 (40.98) | 1 | 27 (44.26) | 1 | 18 (29.51) | |
| Response to pre-operative chemotherapy | |||||||
| Good | 50 | 32 (64.00) | 0.00 | 34 (68.00) | 0.00 | 28 (56.00) | 0.002 |
| Poor | 42 | 18 (42.86) | 2 | 18 (42.86) | 2 | 14 (33.33) | |
| Variables | Overall survival | Progression-free survival | ||||
|---|---|---|---|---|---|---|
| RR | 95% CI | p | RR | 95% CI | p | |
| miR-340 expression | 6.2 | 1.4–13.9 | 0.006 | 4.5 | 1.0–9.2 | 0.01 |
| ROCK1 expression | 5.8 | 1.2–12.6 | 0.008 | 3.2 | 1.0–8.8 | 0.02 |
| miR-340/ROCK1 expression | 7.6 | 1.5–16.2 | 0.002 | 6.5 | 1.0–8.2 | 0.005 |
| Tumor size | 3.5 | 1.0–8.4 | 0.01 | 2.9 | 0.8–7.6 | 0.02 |
| Metastasis status | 4.2 | 1.6–10.3 | 0.006 | 3.9 | 1.3–9.6 | 0.008 |
| Response to pre-operative chemotherapy | 2.5 | 0.9–7.3 | 0.02 | 2.1 | 0.6–6.6 | 0.03 |
© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Cai, H.; Lin, L.; Cai, H.; Tang, M.; Wang, Z. Combined MicroRNA-340 and ROCK1 mRNA Profiling Predicts Tumor Progression and Prognosis in Pediatric Osteosarcoma. Int. J. Mol. Sci. 2014, 15, 560-573. https://doi.org/10.3390/ijms15010560
Cai H, Lin L, Cai H, Tang M, Wang Z. Combined MicroRNA-340 and ROCK1 mRNA Profiling Predicts Tumor Progression and Prognosis in Pediatric Osteosarcoma. International Journal of Molecular Sciences. 2014; 15(1):560-573. https://doi.org/10.3390/ijms15010560
Chicago/Turabian StyleCai, Haiqing, Lijun Lin, Haikang Cai, Mingjie Tang, and Zhigang Wang. 2014. "Combined MicroRNA-340 and ROCK1 mRNA Profiling Predicts Tumor Progression and Prognosis in Pediatric Osteosarcoma" International Journal of Molecular Sciences 15, no. 1: 560-573. https://doi.org/10.3390/ijms15010560