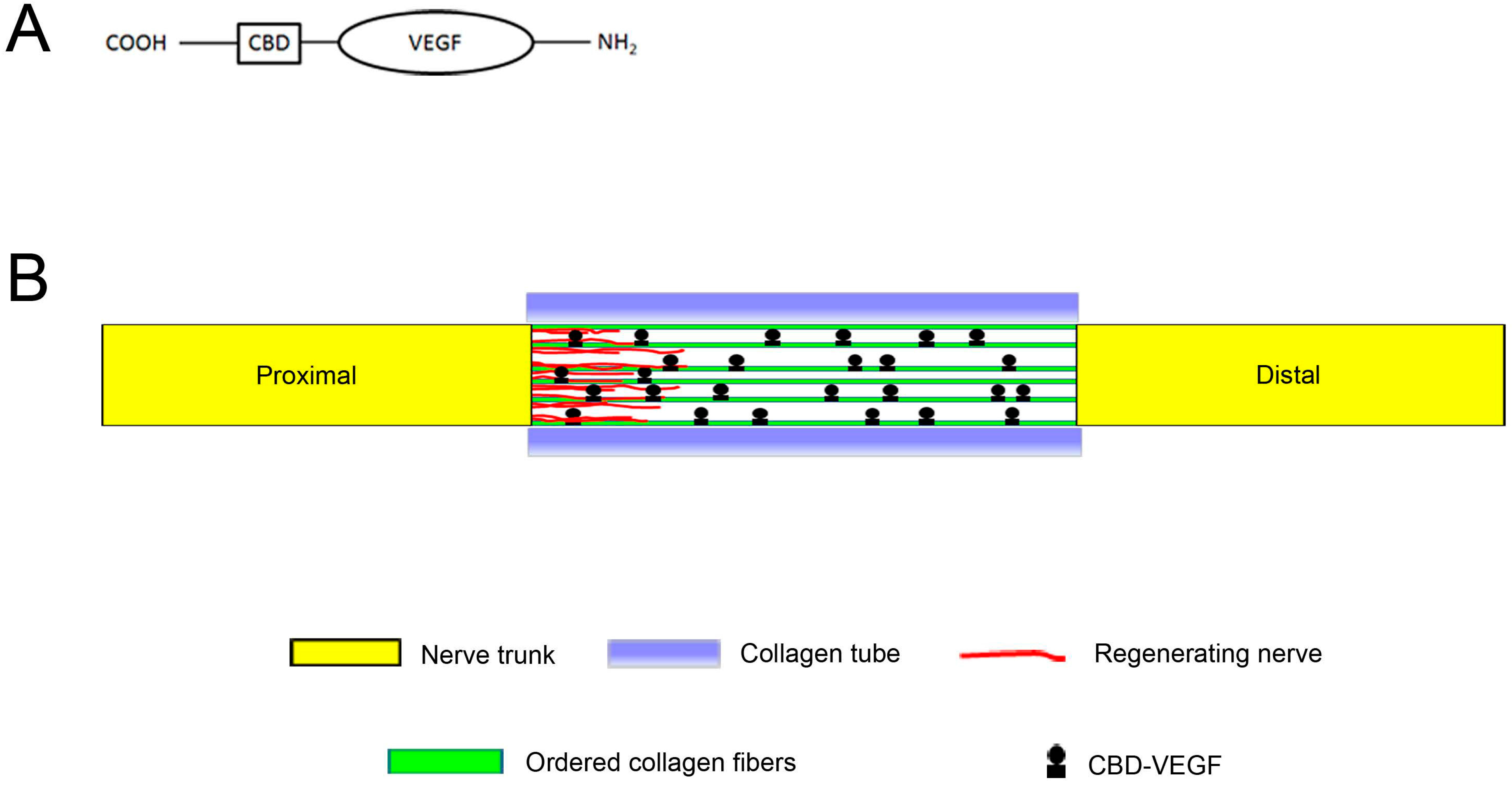
Use of Natural Neural Scaffolds Consisting of Engineered Vascular Endothelial Growth Factor Immobilized on Ordered Collagen Fibers Filled in a Collagen Tube for Peripheral Nerve Regeneration in Rats

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction

2. Results
2.1. General Observation of the Regenerated Nerve
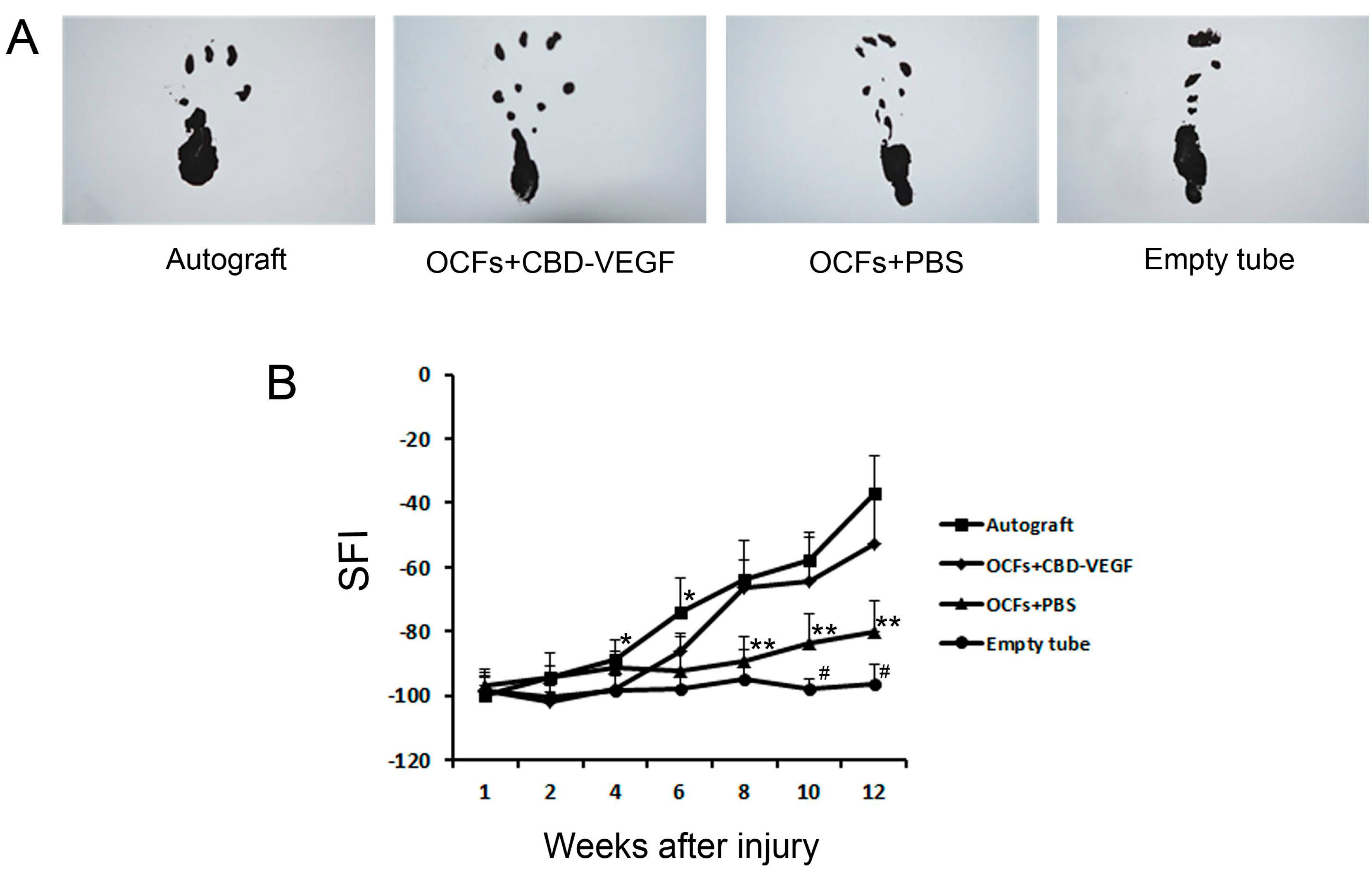
2.2. Motor Functional Assessment of Nerve Regeneration

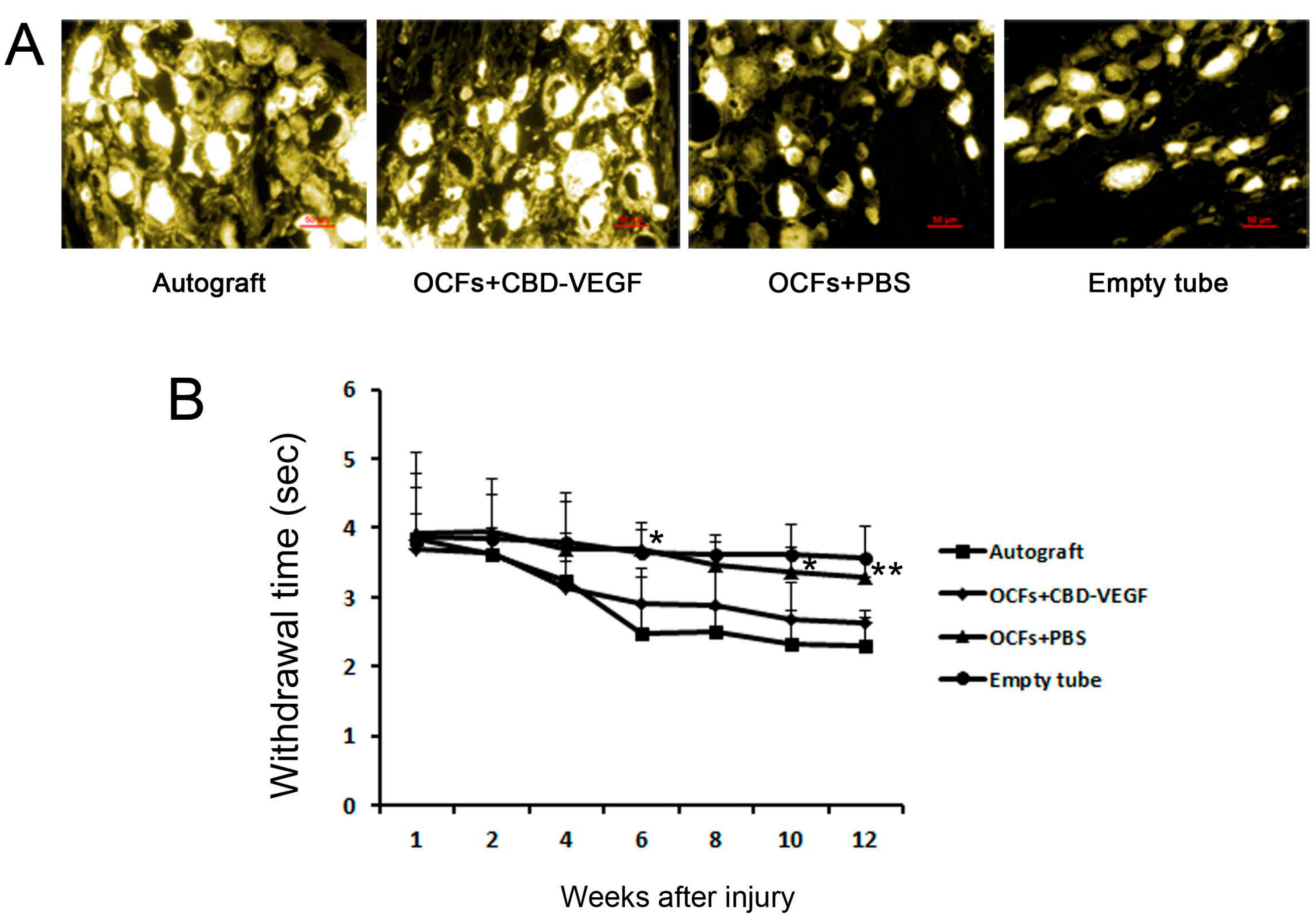
2.3. Sensory Function and Retrograde Tracing Findings

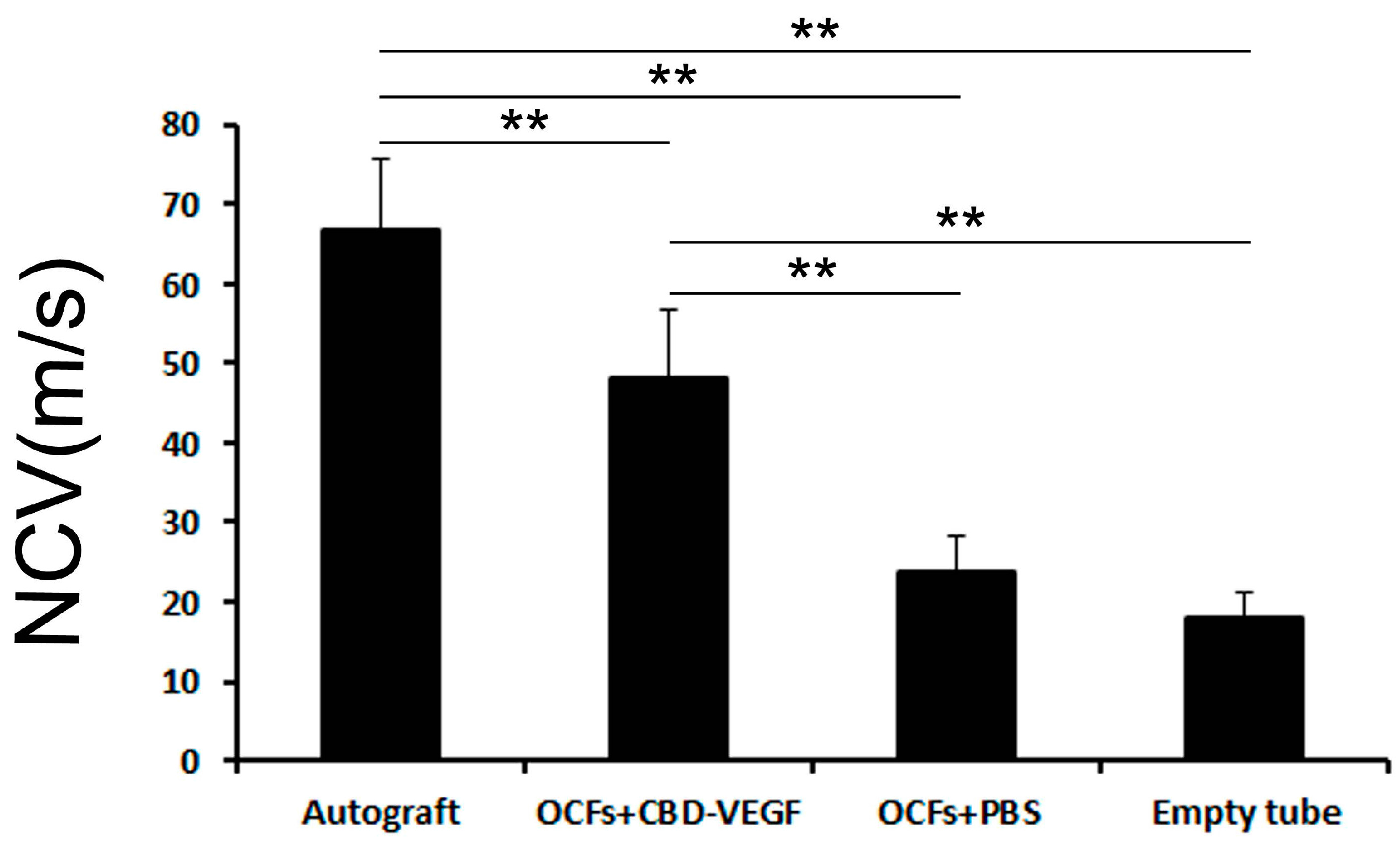
2.4. Electrophysiological Analysis

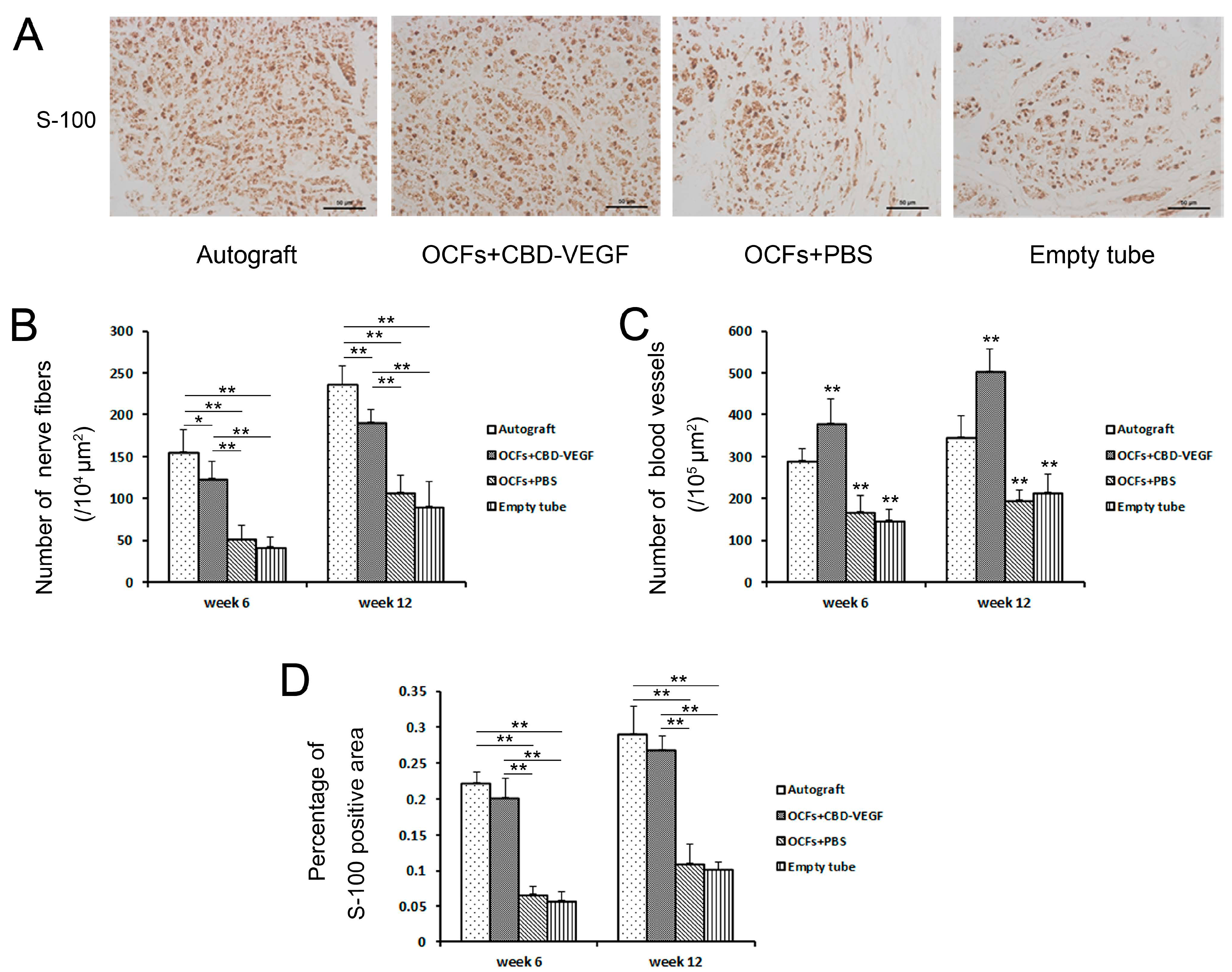
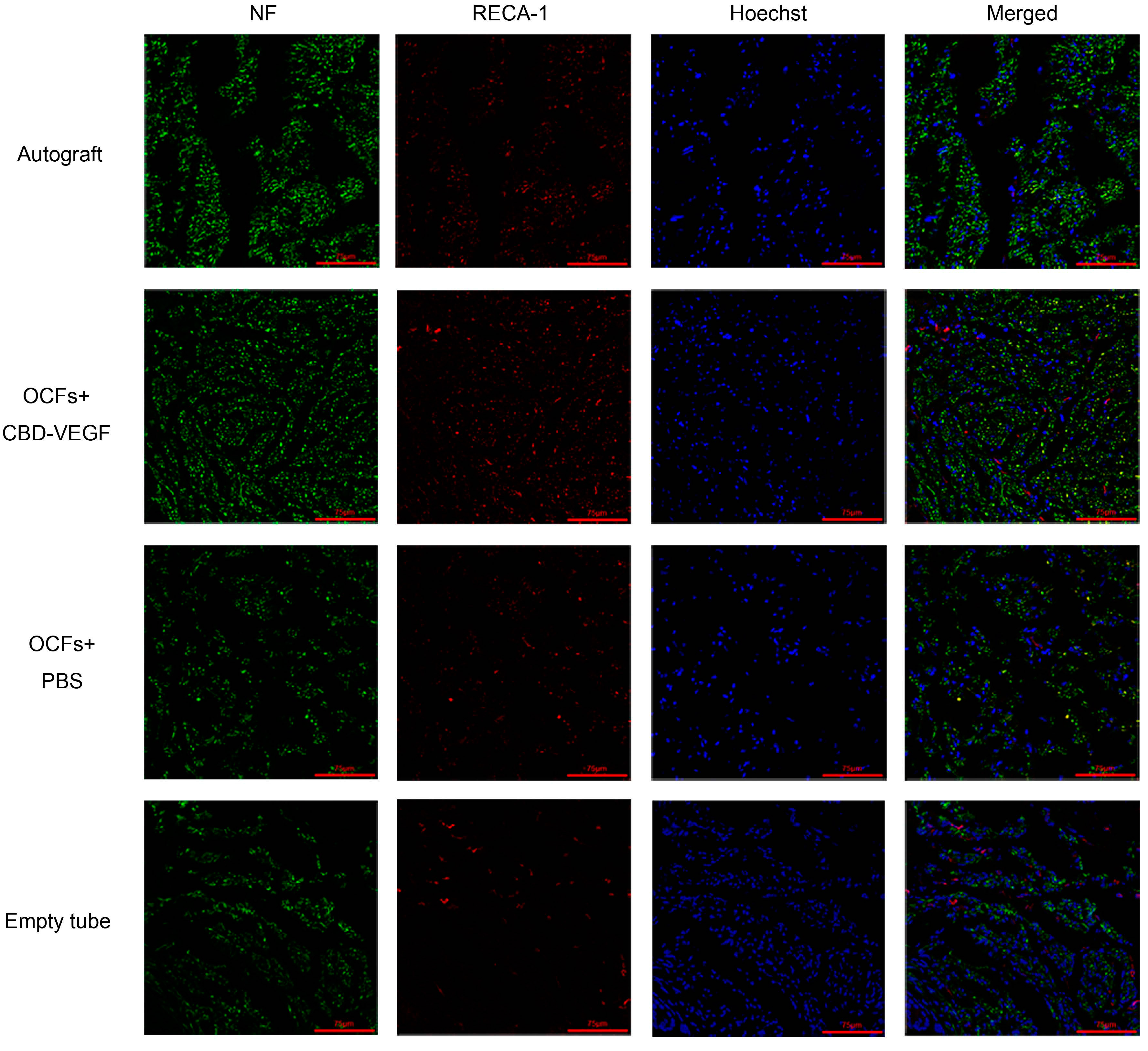
2.5. Immunohistochemical Evaluation

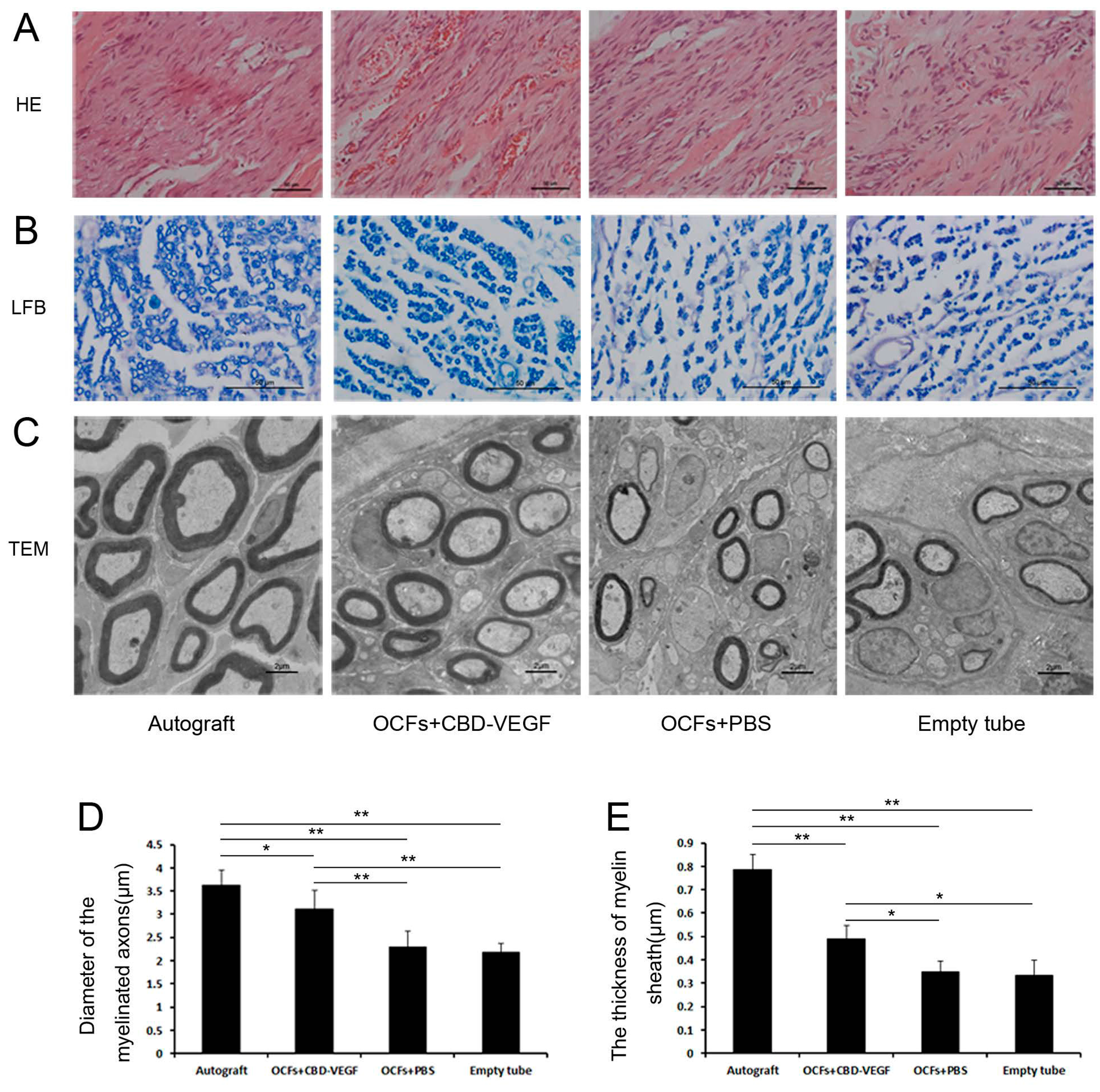
2.6. Histological Assessment
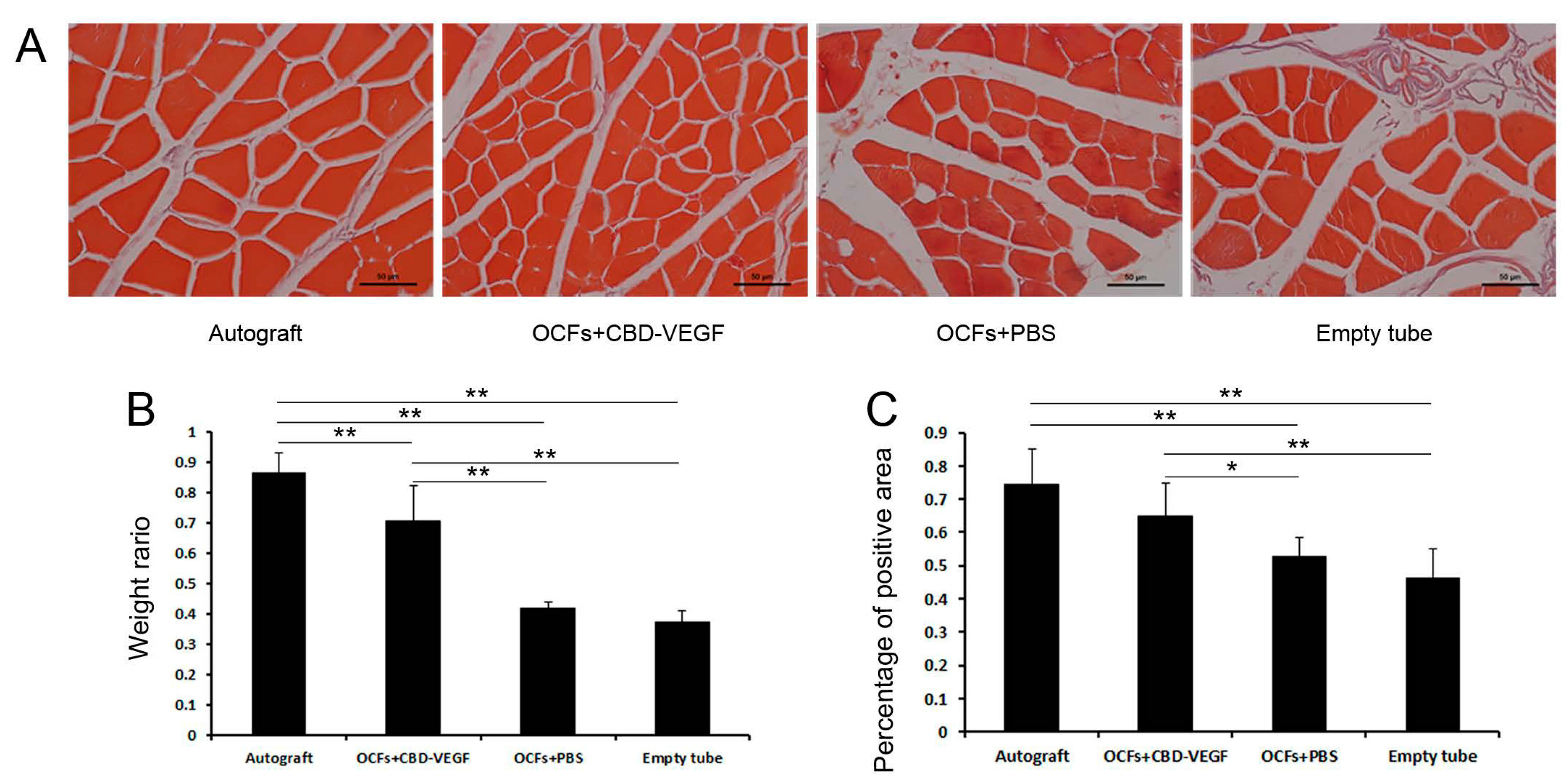
2.7. Muscle-Mass Ratio and Masson’s Trichrome Staining


3. Discussion
4. Material and Methods
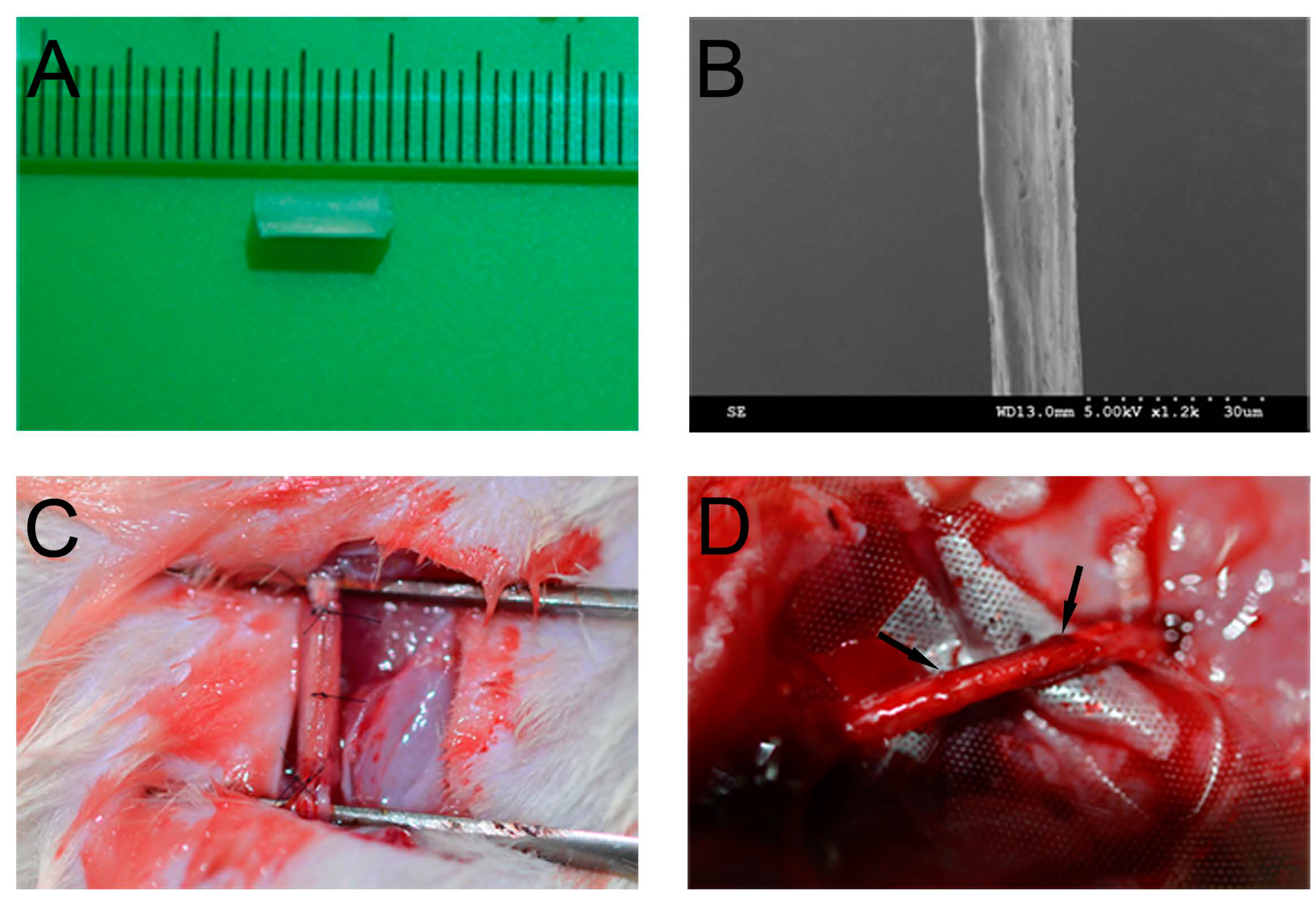
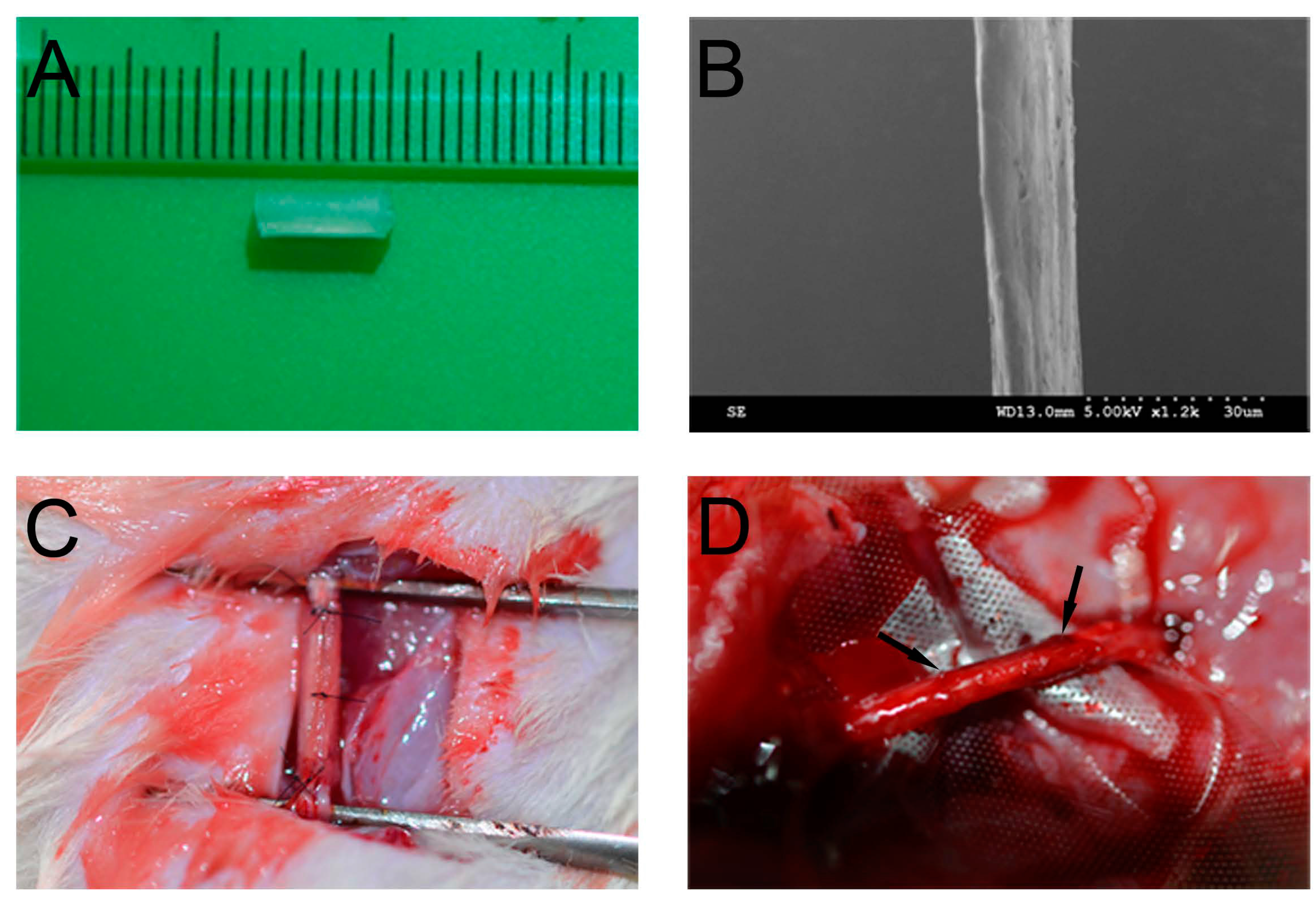
4.1. Preparation of OCFs and Collagen Tubes
4.2. Production of CBD-VEGF
4.3. Animals and Surgical Procedure
4.4. Functional Assessment of Nerve Regeneration
4.5. Assessment of Sensory Recovery
4.6. Fluorogold Retrograde Tracing
4.7. Electrophysiological Assessment
4.8. Immunohistochemical Evaluation
4.9. Histological Evaluation
4.10. Muscle-Mass Ratio and Masson’s Trichrome Staining
4.11. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kemp, S.W.; Walsh, S.K.; Midha, R. Growth factor and stem cell enhanced conduits in peripheral nerve regeneration and repair. Neurol. Res. 2008, 30, 1030–1038. [Google Scholar]
- Huang, J.; Zhang, Y.; Lu, L.; Hu, X.; Luo, Z. Electrical stimulation accelerates nerve regeneration and functional recovery in delayed peripheral nerve injury in rats. Eur. J. Neurosci. 2013, 38, 3691–3701. [Google Scholar]
- Gu, X.; Ding, F.; Yang, Y.; Liu, J. Construction of tissue engineered nerve grafts and their application in peripheral nerve regeneration. Prog. Neurobiol. 2011, 93, 204–230. [Google Scholar]
- English, A.W.; Cucoranu, D.; Mulligan, A.; Rodriguez, J.A.; Sabatier, M.J. Neurotrophin-4/5 is implicated in the enhancement of axon regeneration produced by treadmill training following peripheral nerve injury. Eur. J. Neurosci. 2011, 33, 2265–2271. [Google Scholar]
- Campbell, W.W. Evaluation and management of peripheral nerve injury. Clin. Neurophysiol. 2008, 119, 1951–1965. [Google Scholar]
- Lundborg, G.; Richard, P. Bunge memorial lecture. Nerve injury and repair—A challenge to the plastic brain. JPNS 2003, 8, 209–226. [Google Scholar]
- Chalfoun, C.T.; Wirth, G.A.; Evans, G.R. Tissue engineered nerve constructs: Where do we stand? J. Cell. Mol. Med. 2006, 10, 309–317. [Google Scholar]
- Yurchenco, P.D.; Smirnov, S.; Mathus, T. Analysis of basement membrane self-assembly and cellular interactions with native and recombinant glycoproteins. Methods Cell Biol. 2002, 69, 111–144. [Google Scholar]
- Longo, F.M.; Hayman, E.G.; Davis, G.E.; Ruoslahti, E.; Engvall, E.; Manthorpe, M.; Varon, S. Neurite-promoting factors and extracellular matrix components accumulating in vivo within nerve regeneration chambers. Brain Res. 1984, 309, 105–117. [Google Scholar]
- Li, X.; Feng, Q.; Liu, X.; Dong, W.; Cui, F. Collagen-based implants reinforced by chitin fibres in a goat shank bone defect model. Biomaterials 2006, 27, 1917–1923. [Google Scholar]
- Ribeiro-Resende, V.T.; Koenig, B.; Nichterwitz, S.; Oberhoffner, S.; Schlosshauer, B. Strategies for inducing the formation of bands of Bungner in peripheral nerve regeneration. Biomaterials 2009, 30, 5251–5259. [Google Scholar]
- Koh, H.S.; Yong, T.; Teo, W.E.; Chan, C.K.; Puhaindran, M.E.; Tan, T.C.; Lim, A.; Lim, B.H.; Ramakrishna, S. In vivo study of novel nanofibrous intra-luminal guidance channels to promote nerve regeneration. J. Neural Eng. 2010, 7, 046003. [Google Scholar]
- Chew, S.Y.; Mi, R.; Hoke, A.; Leong, K.W. Aligned protein-polymer composite fibers enhance nerve regeneration: A potential tissue-engineering platform. Adv. Funct. Mater. 2007, 17, 1288–1296. [Google Scholar]
- Sondell, M.; Lundborg, G.; Kanje, M. Vascular endothelial growth factor stimulates Schwann cell invasion and neovascularization of acellular nerve grafts. Brain Res. 1999, 846, 219–228. [Google Scholar]
- Frey, S.P.; Jansen, H.; Raschke, M.J.; Meffert, R.H.; Ochman, S. VEGF improves skeletal muscle regeneration after acute trauma and reconstruction of the limb in a rabbit model. Clin. Orthop. Relat. Res. 2012, 470, 3607–3614. [Google Scholar]
- Tan, A.; Rajadas, J.; Seifalian, A.M. Biochemical engineering nerve conduits using peptide amphiphiles. J. Control. Release 2012, 163, 342–352. [Google Scholar]
- Mukhatyar, V.; Karumbaiah, L.; Yeh, J.; Bellamkonda, R. Tissue engineering strategies designed to realize the endogenous regenerative potential of peripheral nerves. Adv. Mater. 2009, 21, 4670–4679. [Google Scholar]
- Belkas, J.S.; Shoichet, M.S.; Midha, R. Peripheral nerve regeneration through guidance tubes. Neurol. Res. 2004, 26, 151–160. [Google Scholar]
- Hoffman-Kim, D.; Mitchel, J.A.; Bellamkonda, R.V. Topography, cell response, and nerve regeneratio. Annu. Rev. Biomed. Eng. 2010, 12, 203–231. [Google Scholar]
- Bellamkonda, R.V. Peripheral nerve regeneration: An opinion on channels, scaffolds and anisotropy. Biomaterials 2006, 27, 3515–3518. [Google Scholar]
- Pereira Lopes, F.R.; Frattini, F.; Marques, S.A.; Almeida, F.M.; de Moura Campos, L.C.; Langone, F.; Lora, S.; Borojevic, R.; Martinez, A.M. Transplantation of bone-marrow-derived cells into a nerve guide resulted in transdifferentiation into Schwann cells and effective regeneration of transected mouse sciatic nerve. Micron 2010, 41, 783–790. [Google Scholar]
- De Souza, S.J.; Brentani, R. Collagen binding site in collagenase can be determined using the concept of sense-antisense peptide interactions. J. Biol. Chem. 1992, 267, 13763–13767. [Google Scholar]
- Hu, X.; Huang, J.; Ye, Z.; Xia, L.; Li, M.; Lv, B.; Shen, X.; Luo, Z. A novel scaffold with longitudinally oriented microchannels promotes peripheral nerve regeneration. Tissue Eng. Part A 2009, 15, 3297–3308. [Google Scholar]
- Brushart, T.M.; Mathur, V.; Sood, R.; Koschorke, G.M. Dispersion of regenerating axons across enclosed neural gaps. J. Hand Surg. 1995, 20, 557–564. [Google Scholar]
- Madison, R.D.; Archibald, S.J.; Lacin, R.; Krarup, C. Factors contributing to preferential motor reinnervation in the primate peripheral nervous system. J. Neurosci. 1999, 19, 11007–11016. [Google Scholar]
- Hamilton, S.K.; Hinkle, M.L.; Nicolini, J.; Rambo, L.N.; Rexwinkle, A.M.; Rose, S.J.; Sabatier, M.J.; Backus, D.; English, A.W. Misdirection of regenerating axons and functional recovery following sciatic nerve injury in rats. J. Comp. Neurol. 2011, 519, 21–33. [Google Scholar]
- Silva, E.A.; Mooney, D.J. Spatiotemporal control of vascular endothelial growth factor delivery from injectable hydrogels enhances angiogenesis. J. Thromb. Haemost. 2007, 5, 590–598. [Google Scholar]
- Eppler, S.M.; Combs, D.L.; Henry, T.D.; Lopez, J.J.; Ellis, S.G.; Yi, J.H.; Annex, B.H.; McCluskey, E.R.; Zioncheck, T.F. A target-mediated model to describe the pharmacokinetics and hemodynamic effects of recombinant human vascular endothelial growth factor in humans. Clin. Pharmacol. Ther. 2002, 72, 20–32. [Google Scholar]
- Lee, R.J.; Springer, M.L.; Blanco-Bose, W.E.; Shaw, R.; Ursell, P.C.; Blau, H.M. VEGF gene delivery to myocardium: Deleterious effects of unregulated expression. Circulation 2000, 102, 898–901. [Google Scholar]
- Liu, G.; Sun, X.; Bian, J.; Wu, R.; Guan, X.; Ouyang, B.; Huang, Y.; Xiao, H.; Luo, D.; Atala, A.; et al. Correction of diabetic erectile dysfunction with adipose derived stem cells modified with the vascular endothelial growth factor gene in a rodent diabetic model. PLoS One 2013, 8, e72790. [Google Scholar]
- Nauta, A.; Seidel, C.; Deveza, L.; Montoro, D.; Grova, M.; Ko, S.H.; Hyun, J.; Gurtner, G.C.; Longaker, M.T.; Yang, F. Adipose-derived stromal cells overexpressing vascular endothelial growth factor accelerate mouse excisional wound healing. Mol. Ther. 2013, 21, 445–455. [Google Scholar]
- Saeed, M.; Saloner, D.; Martin, A.; Do, L.; Weber, O.; Ursell, P.C.; Jacquier, A.; Lee, R.; Higgins, C.B. Adeno-associated viral vector-encoding vascular endothelial growth factor gene: Effect on cardiovascular MR perfusion and infarct resorption measurements in swine. Radiology 2007, 243, 451–460. [Google Scholar]
- Galeano, M.; Deodato, B.; Altavilla, D.; Cucinotta, D.; Arsic, N.; Marini, H.; Torre, V.; Giacca, M.; Squadrito, F. Adeno-associated viral vector-mediated human vascular endothelial growth factor gene transfer stimulates angiogenesis and wound healing in the genetically diabetic mouse. Diabetologia 2003, 46, 546–555. [Google Scholar]
- Boodhwani, M.; Mieno, S.; Voisine, P.; Feng, J.; Sodha, N.; Li, J.; Sellke, F.W. High-dose atorvastatin is associated with impaired myocardial angiogenesis in response to vascular endothelial growth factor in hypercholesterolemic swine. J. Thorac. Cardiovasc. Surg. 2006, 132, 1299–1306. [Google Scholar]
- Davies, N.H.; Schmidt, C.; Bezuidenhout, D.; Zilla, P. Sustaining neovascularization of a scaffold through staged release of vascular endothelial growth factor-A and platelet-derived growth factor-BB. Tissue Eng. Part A 2012, 18, 26–34. [Google Scholar]
- Lin, H.; Chen, B.; Wang, B.; Zhao, Y.; Sun, W.; Dai, J. Novel nerve guidance material prepared from bovine aponeurosis. J. Biomed. Mater. Res. Part A 2006, 79, 591–598. [Google Scholar]
- Zhang, J.; Ding, L.; Zhao, Y.; Sun, W.; Chen, B.; Lin, H.; Wang, X.; Zhang, L.; Xu, B.; Dai, J. Collagen-targeting vascular endothelial growth factor improves cardiac performance after myocardial infarction. Circulation 2009, 119, 1776–1784. [Google Scholar]
- Bain, J.R.; Mackinnon, S.E.; Hunter, D.A. Functional evaluation of complete sciatic, peroneal, and posterior tibial nerve lesions in the rat. Plast. Reconstr. Surg. 1989, 83, 129–138. [Google Scholar]
- Derby, A.; Engleman, V.W.; Frierdich, G.E.; Neises, G.; Rapp, S.R.; Roufa, D.G. Nerve growth factor facilitates regeneration across nerve gaps: Morphological and behavioral studies in rat sciatic nerve. Exp. Neurol. 1993, 119, 176–191. [Google Scholar]
- Young, C.; Miller, E.; Nicklous, D.M.; Hoffman, J.R. Nerve growth factor and neurotrophin-3 affect functional recovery following peripheral nerve injury differently. Restor. Neurol. Neurosci. 2001, 18, 167–175. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, F.; Xiao, Z.; Meng, D.; Hou, X.; Zhu, J.; Dai, J.; Xu, R. Use of Natural Neural Scaffolds Consisting of Engineered Vascular Endothelial Growth Factor Immobilized on Ordered Collagen Fibers Filled in a Collagen Tube for Peripheral Nerve Regeneration in Rats. Int. J. Mol. Sci. 2014, 15, 18593-18609. https://doi.org/10.3390/ijms151018593
Ma F, Xiao Z, Meng D, Hou X, Zhu J, Dai J, Xu R. Use of Natural Neural Scaffolds Consisting of Engineered Vascular Endothelial Growth Factor Immobilized on Ordered Collagen Fibers Filled in a Collagen Tube for Peripheral Nerve Regeneration in Rats. International Journal of Molecular Sciences. 2014; 15(10):18593-18609. https://doi.org/10.3390/ijms151018593
Chicago/Turabian StyleMa, Fukai, Zhifeng Xiao, Danqing Meng, Xianglin Hou, Jianhong Zhu, Jianwu Dai, and Ruxiang Xu. 2014. "Use of Natural Neural Scaffolds Consisting of Engineered Vascular Endothelial Growth Factor Immobilized on Ordered Collagen Fibers Filled in a Collagen Tube for Peripheral Nerve Regeneration in Rats" International Journal of Molecular Sciences 15, no. 10: 18593-18609. https://doi.org/10.3390/ijms151018593