Anti-Vascular Endothelial Growth Factor Therapy in Breast Cancer

Abstract
:1. Introduction
2. Anti-Angiogenic Therapy
2.1. Angiogenesis
2.1.1. Definition of Angiogenesis
2.1.2. Spouting, Intussusception, Vascular Mimicry, Vascular Co-Option and Regulation of These Processes
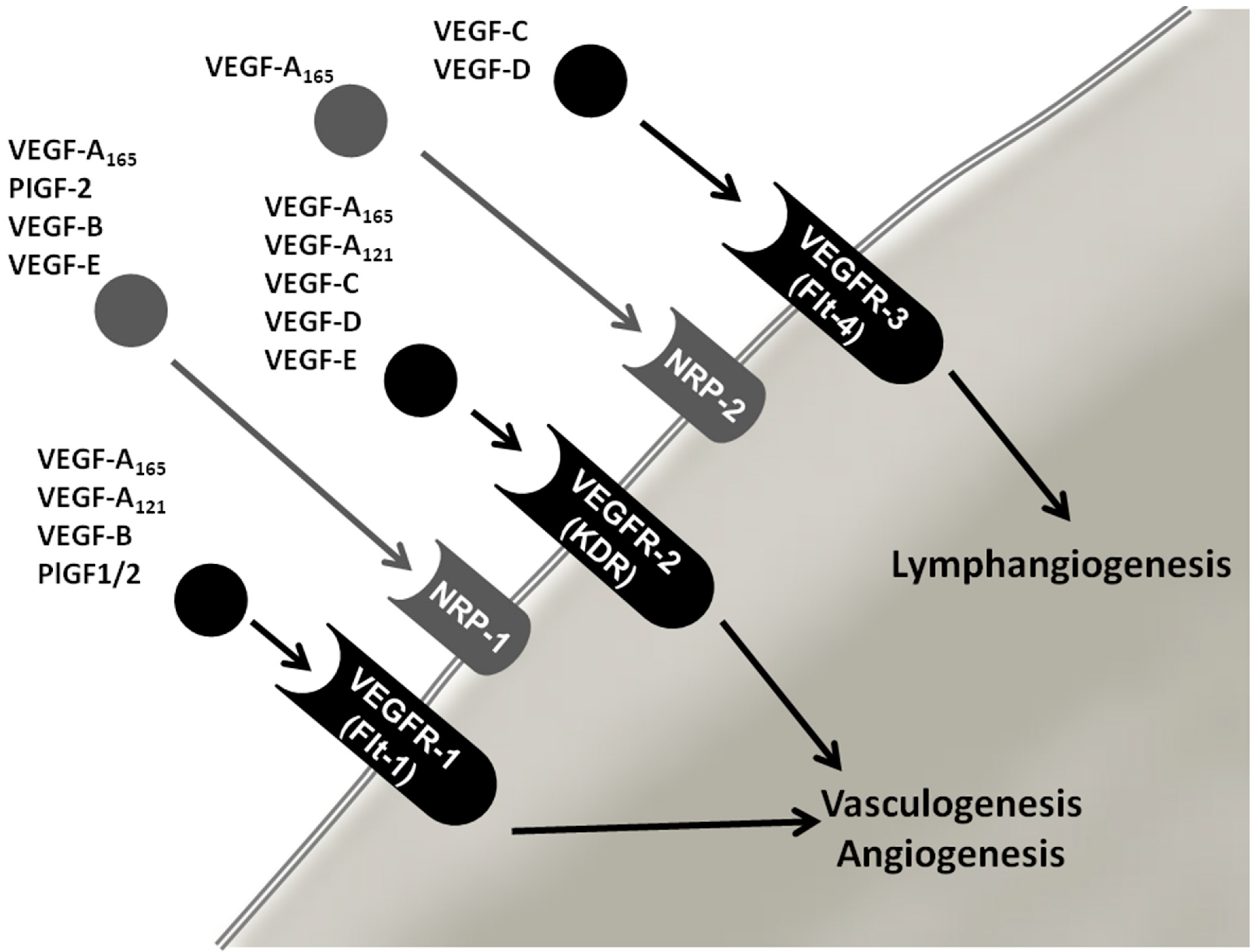
2.2. Vascular Endothelial Growth Factor (VEGF) Family

3. Overview of Anti-Angiogenic Drugs Targeting the VEGF System

{kind=link}
{kind=link}
| Drug | Trial/Reference | Treatment | Drugs Used | PFS | ORR | pCR | OS |
|---|---|---|---|---|---|---|---|
| bevacizumab | AVF2119g | Second-line | Capecitabine +/− bevacizumab | NS | Significant | Not reported | NS |
| bevacizumab | ECOG-E2100 | First-line | Paclitaxel +/− bevacizumab | Significant | Significant | Not reported | NS |
| bevacizumab | AVADO | First-line | Docetaxel +/− bevacizumab (arm treated with highest dosage bevacizumab) | Significant | Significant | Not reported | NS |
| bevacizumab | RIBBON-1 | First-line | Capecitabine/taxane/Anthracycline based chemotherapy +/− bevacizumab | Significant | Significant | Not reported | NS |
| bevacizumab | RIBBON-2 | Second-line | Capecitabine/taxane/gemcitabine/vinorelbine based chemotherapy +/− bevacizumab | Significant | Significant | Not reported | NS |
| bevacizumab | GBG44/clinicaltrials.gov ID: NCT00567554 | Neoadjuvant therapy | Epirubicin/cyclophosphamide/docetaxel +/− bevacizumab | Not reported | Not reported | Significant | Data under way |
| bevacizumab | NSABP | Neoadjuvant therapy | Docetaxel/capecitabine/gemcitabine +/− bevacizumab | Not reported | Not reported | Significant | Data under way |
| bevacizumab | AVEREL | First-line | Trastuzumab/docetaxel +/− bevacizumab | NS | NS | Not reported | NS |
| sorafenib | SOLTI0701 | First-line/second-line | Capecitabine +/− sorafenib | Significant | NS | - | NS |
| sorafenib | AB01B07 | Second-line | Capecitabine and gemcitabine +/− sorafenib | Significant | NS | - | NS |
| sorafenib | NU07B1 | First-line | Paclitaxel +/− sorafenib | NS | Significant | - | NS |
| sorafenib | FMB0701 | First-line | Docetaxel and/or letrozole +/− sorafenib | NS | NS | - | NS |
| ramucirumab | TRIO-012 | - | Doceraxel +/− ramucirumab | NS | NS | - | NS at interim analysis |
| ramucirumab | clinicaltrials.gov ID: NCT01427933 | Second-line | Eribulin +/− ramucirumab | Not reported | Not reported | Not reported | Not reported |

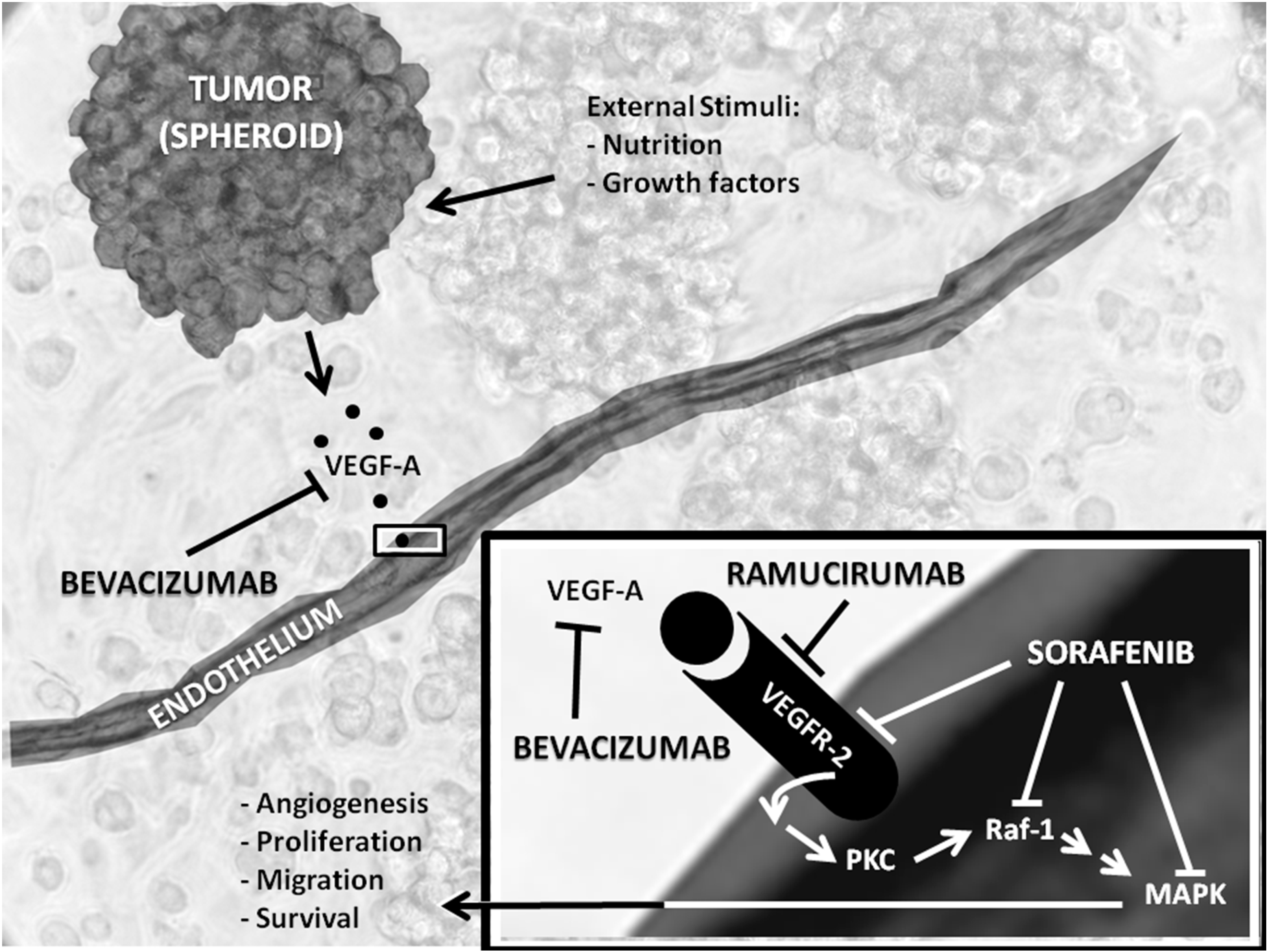
3.1. Bevacizumab
3.2. Ramucirumab
| Protocol Title | Phase | Condition | Intervention | Clinicaltrials.gov |
|---|---|---|---|---|
| Patient Preference for Everolimus in Combination with Exemestane or Capecitabine in Combination with Bevacizumab (IMPROVE) | IV | Advanced (Inoperable or Metastatic) HER2-negative Hormone Receptor Positive Breast Cancer | Everolimus + Exemestane vs. Capecitabine + Bevacizumab | NCT02248571 |
| Trastuzumab or Bevacizumab with Combination Chemotherapy in Treating Patients with Stage II–III Breast Cancer | II | Stage II Breast Cancer; Stage IIIA Breast Cancer; Stage IIIB Breast Cancer; Stage IIIC Breast Cancer | Trastuzumab vs. Bevacizumab + Chemotherapy (Docetaxel; Carboplatin; Doxorubicin Hydrochloride; Cyclophosphamide, Paclitaxel) | NCT01959490 |
| Bevacizumab in Combination with Chemotherapy in the Neo-adjuvant Setting for HER2 (−) Breast Cancer | II | Breast Cancer | Neoadjuvant Treatment of Bevacizumab + Chemotherapy (5-Fluorouracil, Epirubicin; Cyclophosphamide; Docetaxel) | NCT01985841 |
| Bevacizumab, Etoposide and Cisplatin Followed by Whole Brain Radiotherapy in Breast Cancer with Brain Metastases | II | Breast Cancer; Brain Metastases | BEEP (bevacizumab preconditioning followed by etoposide and cisplatin) Regimen Prior to Radiotherapy | NCT02185352 |
| Safety and Efficacy Study of Eribulin in Combination with Bevacizumab for Second-line Treatment HER2-MBC Patients (GIM11-BERGI) | II | Metastatic Breast Cancer; Human Epidermal Growth Factor 2 Negative Carcinoma of Breast | Bevacizumab and Eribulin | NCT02175446 |
| Intrapleural Bevacizumab After Pleural Drainage in the Context of Breast Cancer | I | Pleural Effusion, Malignant; Breast Cancer | Bevacizumab | NCT02250118 |
| Bevacizumab Plus Paclitaxel Optimization Study with Interventional Maintenance Endocrine Therapy in Advanced or Metastatic ER-positive Human Epidermal Growth Factor Receptor 2(HER2)-Negative Breast Cancer (BOOSTER) | II | Metastatic Breast Cancer | Weekly Paclitaxel + Bevacizumab vs. Weekly Paclitaxel + Bevacizumab Followed By Hormone Therapy + Bevacizumab Then back to Weekly Paclitaxel + Bevacizumab | NCT01989780 |
| Triple-B Study; Carboplatin-cyclophosphamide vs. Paclitaxel with or without Bevacizumab as First-line Treatment in Advanced Triple Negative Breast Cancer | II | Breast Cancer | Carboplatin/Cyclophosphamide vs. Carboplatin/Cyclophosphamide + Bevacizumab vs. Paclitaxel vs. Paclitaxel + Bevacizumab | NCT01898117 |
| Phase I Study of Lurbinectedin (PM01183) in Combination with Paclitaxel, with or without Bevacizumab, in Selected Advanced Solid Tumors | I | Breast Cancer; Ovarian Cancer; Gynecological Cancer; Head and Neck Carcinoma; Non-Small-Cell-Lung Cancer; Small-Cell-Lung Cancer; Non-Squamous-Cell-Lung Cancer | PM01183 + Paclitaxel vs. PM01183 + Paclitaxel + Bevacizumab | NCT01831089 |
3.3. Sorafenib
3.4. Adverse Effects
4. Biomarkers
5. Conclusions and Future Developments
Author Contributions
Abbreviation
| EC | Endothelial cell |
| ECM | Extracellular matrix |
| EMEA | European Medicines Agency |
| FDA | Food and Drug Administration |
| HER2 | Human epidermal growth receptor 2 |
| HER2-positive | Tumor shows overexpression of HER2-receptors |
| HER2-negative | Tumor does not show overexpression of HER2-receptors |
| HIF | Hypoxia induced factor |
| MAPK | Mitogen activated protein kinase |
| MMP | Matrix metalloproteinases |
| NPLD | Non-PEGylated liposome-encapsulated doxorubicin |
| ORR | Overall response rate |
| OS | Overall survival |
| pCR | Pathological complete response |
| PDGFB | Platelet-derived growth factor-b |
| PFS | Progression-free survival |
| PHD | Prolyl hydroxylase domain |
| PKC | Protein kinase C |
| PLGF-1/-2 | Placental growth factor-1/-2 |
| Raf-1 | Proto-oncogene, serine/threonine kinase |
| SNP | Single nucleotide polymorphism |
| TIES | Trials to Investigate the Efficacy of Sorafenib |
| TNBC | Triple negative breast cancer: the tumor is HER2-negative, ER-negative and PR-negative |
| VEGF | Vascular endothelial growth factor |
| VEGF-A | Vascular endothelial growth factor A |
| VEGFR-2 | Vascular endothelial growth factor receptor subtype 2 |
Conflicts of Interest
References
- GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012. Available online: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx (accessed on 1 December 2014).
- Grimm, D.; Wehland, M.; Pietsch, J.; Infanger, M.; Bauer, J. Drugs interfering with apoptosis in breast cancer. Curr. Pharm. Des. 2011, 17, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Grimm, D.; Bauer, J.; Schönberger, J. Blockade of neoangiogenesis, a new and promising technique to control the growth of malignant tumors and its metastases. Curr. Vasc. Pharmacol. 2009, 7, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Miklos, G.L. Bevacizumab in neoadjuvant treatment for breast cancer. N. Engl. J. Med. 2012, 366, 1637–1640. [Google Scholar] [CrossRef] [PubMed]
- Bear, H.D.; Tang, G.; Rastogi, P.; Geyer, C.E., Jr.; Robidoux, A.; Atkins, J.N.; Baez-Diaz, L.; Brufsky, A.M.; Mehta, R.S.; Fehrenbacher, L.; et al. Bevacizumab added to neoadjuvant chemotherapy for breast cancer. N. Engl. J. Med. 2012, 366, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Fan, F.; Schimming, A.; Jaeger, D.; Podar, K. Targeting the tumor microenvironment: Focus on angiogenesis. J. Oncol. 2012, 2012, 281261. [Google Scholar] [CrossRef] [PubMed]
- Jelkmann, W. Pitfalls in the measurement of circulating vascular endothelial growth factor. Clin. Chem. 2001, 47, 617–623. [Google Scholar] [PubMed]
- Carmeliet, P.; Jain, R.K. Molecular mechanisms and clinical applications of angiogenesis. Nature 2011, 473, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Claesson-Welsh, L.; Welsh, M. VEGFA and tumour angiogenesis. J. Intern. Med. 2013, 273, 114–127. [Google Scholar] [CrossRef] [PubMed]
- Wehland, M.; Bauer, J.; Magnusson, N.E.; Infanger, M.; Grimm, D. Biomarkers for anti-angiogenic therapy in cancer. Int. J. Mol. Sci. 2013, 14, 9338–9364. [Google Scholar] [CrossRef] [PubMed]
- Leite de Oliveira, R.; Hamm, A.; Mazzone, M. Growing tumor vessels: More than one way to skin a cat—Implications for angiogenesis targeted cancer therapies. Mol. Aspects Med. 2011, 32, 71–87. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J. Tumor angiogenesis: Therapeutic implications. N. Engl. J. Med. 1971, 285, 1182–1186. [Google Scholar] [CrossRef] [PubMed]
- Niu, G.; Chen, X. Vascular endothelial growth factor as an anti-angiogenic target for cancer therapy. Curr. Drug Targets 2010, 11, 1000–1017. [Google Scholar] [CrossRef] [PubMed]
- Leenders, W.P.; Kusters, B.; de Waal, R.M. Vessel co-option: How tumors obtain blood supply in the absence of sprouting angiogenesis. Endothelium 2002, 9, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Donnem, T.; Hu, J.; Ferguson, M.; Adighibe, O.; Snell, C.; Harris, A.L.; Gatter, K.C.; Pezzella, F. Vessel co-option in primary human tumors and metastases: An obstacle to effective anti-angiogenic treatment? Cancer Med. 2013, 2, 427–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrara, N. The role of VEGF in the regulation of physiological and pathological angiogenesis. In Mechanisms of Angiogenesis; Clauss, M., Breier, G., Eds.; Birkhäuser: Basel, Switzerland, 2005; pp. 209–231. [Google Scholar]
- Ferrara, N. Vascular endothelial growth factor: Basic science and clinical progress. Endocr. Rev. 2004, 25, 581–611. [Google Scholar] [CrossRef] [PubMed]
- Grimm, D.; Bauer, J.; Ulbrich, C.; Westphal, K.; Wehland, M.; Infanger, M.; Aleshcheva, G.; Pietsch, J.; Gardi, M.; Beck, M.; et al. Different responsiveness of endothelial cells to Vascular Endothelial Growth Factor and Basic Fibroblast Growth Factor added to culture media under gravity and simulated microgravity. Tissue Eng. Part A 2010, 16, 1559–1573. [Google Scholar] [CrossRef] [PubMed]
- Infanger, M.; Grosse, J.; Westphal, K.; Leder, A.; Ulbrich, C.; Paul, M.; Grimm, D. Vascular Endothelial Growth Factor induces extracellular matrix proteins and osteopontin in the umbilical artery. Ann. Vasc. Surg. 2008, 22, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Infanger, M.; Faramarzi, S.; Grosse, J.; Kurth, E.; Ulbrich, C.; Bauer, J.; Wehland, M.; Kreutz, R.; Kossmehl, P.; Paul, M.; et al. Expression of Vascular endothelial growth factor and receptor tyrosine kinases in cardiac ischemia-reperfusion injury. Cardiovasc. Pathol. 2007, 16, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Infanger, M.; Shakibaei, M.; Kossmehl, P.; Hollenberg, S.M.; Grosse, J.; Faramarzi, S.; Schulze-Tanzil, G.; Paul, M.; Grimm, D. Intraluminal application of VEGF enhances healing of microvascular anastomosis in a rat model. J. Vasc. Res. 2005, 42, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Infanger, M.; Schmidt, O.; Kossmehl, P.; Grad, S.; Ertel, W.; Grimm, D. Vascular endothelial growth factor serum level is strongly enhanced after burn injury and correlated with local and general tissue edema. Burns 2004, 30, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Grothey, A.; Ellis, L.M. Targeting angiogenesis driven by vascular endothelial growth factors using antibody-based therapies. Cancer J. 2008, 14, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Bergers, G.; Hanahan, D. Modes of resistance to anti-angiogenic therapy. Nat. Rev. Cancer 2008, 8, 592–603. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Chap, L.I.; Holmes, F.A.; Cobleigh, M.A.; Marcom, P.K.; Fehrenbacher, L.; Dickler, M.; Overmoyer, B.A.; Reimann, J.D.; Sing, A.P.; et al. Randomized phase III trial of capecitabine compared with bevacizumab plus capecitabine in patients with previously treated metastatic breast cancer. J. Clin. Oncol. 2005, 23, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Mackey, J.; Gelmon, K.; Martin, M.; McCarthy, N.; Pinter, T.; Rupin, M.; Youssoufian, H. TRIO-012: A multicenter, multinational, randomized, double-blind phase III study of IMC-1121B plus docetaxel vs. placebo plus docetaxel in previously untreated patients with HER2-negative, unresectable, locally recurrent or metastatic breast cancer. Clin. Breast Cancer 2009, 9, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Wehland, M.; Bauer, J.; Infanger, M.; Grimm, D. Target-based anti-angiogenic therapy in breast cancer. Curr. Pharm. Des. 2012, 18, 4244–4257. [Google Scholar] [CrossRef] [PubMed]
- Von Minckwitz, G.; Eidtmann, H.; Rezai, M.; Fasching, P.A.; Tesch, H.; Eggemann, H.; Schrader, I.; Kittel, K.; Hanusch, C.; Kreienberg, R.; et al. Neoadjuvant chemotherapy and bevacizumab for her2-negative breast cancer. N. Engl. J. Med. 2012, 366, 299–309. [Google Scholar] [CrossRef]
- Miller, K.; Wang, M.; Gralow, J.; Dickler, M.; Cobleigh, M.; Perez, E.A.; Shenkier, T.; Cella, D.; Davidson, N.E. Paclitaxel plus bevacizumab vs. paclitaxel alone for metastatic breast cancer. N. Engl. J. Med. 2007, 357, 2666–2676. [Google Scholar] [CrossRef] [PubMed]
- Refaat, T.; Choi, M.; Gaber, G.; Kiel, K.; Mehta, M.; Gradishar, W.; Small, W., Jr. Markov model and cost-effectiveness analysis of bevacizumab in her2-negative metastatic breast cancer. Am. J. Clin. Oncol. 2014, 37, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Miles, D.W.; Diéras, V.; Cortés, J.; Duenne, A.A.; Yi, J.; O’Shaughnessy, J. First-line bevacizumab in combination with chemotherapy for her2-negative metastatic breast cancer: Pooled and subgroup analyses of data from 2447 patients. Ann. Oncol. 2013, 24, 2773–2780. [Google Scholar] [CrossRef] [PubMed]
- Robert, N.J.; Dieras, V.; Glaspy, J.; Brufsky, A.M.; Bondarenko, I.; Lipatov, O.N.; Perez, E.A.; Yardley, D.A.; Chan, S.Y.; Zhou, X.; et al. RIBBON-1: Randomized, double-blind, placebo-controlled, phase iii trial of chemotherapy with or without bevacizumab for first-line treatment of human epidermal growth factor receptor 2-negative, locally recurrent or metastatic breast cancer. J. Clin. Oncol. 2011, 29, 1252–1260. [Google Scholar] [CrossRef] [PubMed]
- Gligorov, J.; Doval, D.; Bines, J.; Alba, E.; Cortes, P.; Pierga, J.Y.; Gupta, V.; Costa, R.; Srock, S.; de Ducla, S.; et al. Maintenance capecitabine and bevacizumab vs. bevacizumab alone after initial first-line bevacizumab and docetaxel for patients with her2-negative metastatic breast cancer (imelda): A randomised, open-label, phase 3 trial. Lancet Oncol. 2014, 15, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Brufsky, A.M.; Hurvitz, S.; Perez, E.; Swamy, R.; Valero, V.; O’Neill, V.; Rugo, H.S. RIBBON-2: A randomized, double-blind, placebo-controlled, phase iii trial evaluating the efficacy and safety of bevacizumab in combination with chemotherapy for second-line treatment of human epidermal growth factor receptor 2-negative metastatic breast cancer. J. Clin. Oncol. 2011, 29, 4286–4293. [Google Scholar] [CrossRef] [PubMed]
- Von Minckwitz, G.; Puglisi, F.; Cortes, J.; Vrdoljak, E.; Marschner, N.; Zielinski, C.; Villanueva, C.; Romieu, G.; Lang, I.; Ciruelos, E.; et al. Bevacizumab plus chemotherapy vs. chemotherapy alone as second-line treatment for patients with her2-negative locally recurrent or metastatic breast cancer after first-line treatment with bevacizumab plus chemotherapy (TANIA): An open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Montero, A.J.; Avancha, K.; Gluck, S.; Lopes, G. A cost-benefit analysis of bevacizumab in combination with paclitaxel in the first-line treatment of patients with metastatic breast cancer. Breast Cancer Res. Treat. 2012, 132, 747–751. [Google Scholar] [CrossRef] [PubMed]
- Gianni, L.; Romieu, G.H.; Lichinitser, M.; Serrano, S.V.; Mansutti, M.; Pivot, X.; Mariani, P.; Andre, F.; Chan, A.; Lipatov, O.; et al. AVEREL: A randomized phase iii trial evaluating bevacizumab in combination with docetaxel and trastuzumab as first-line therapy for her2-positive locally recurrent/metastatic breast cancer. J. Clin. Oncol. 2013, 31, 1719–1725. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Mayer, E.L.; Je, Y.; Rosenberg, J.E.; Nguyen, P.L.; Azzi, G.R.; Bellmunt, J.; Burstein, H.J.; Schutz, F.A. Congestive heart failure risk in patients with breast cancer treated with bevacizumab. J. Clin. Oncol. 2011, 29, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Spratlin, J.L.; Cohen, R.B.; Eadens, M.; Gore, L.; Camidge, D.R.; Diab, S.; Leong, S.; O’Bryant, C.; Chow, L.Q.; Serkova, N.J.; et al. Phase I pharmacologic and biologic study of ramucirumab (imc-1121b), a fully human immunoglobulin g1 monoclonal antibody targeting the vascular endothelial growth factor receptor-2. J. Clin. Oncol. 2010, 28, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Phase III Study of Docetaxel + Ramucirumab or Placebo in Breast Cancer. Available online: http://clinicaltrials.gov/ct2/show/NCT00703326 (accessed on 1 December 2014).
- ClinicalTrial.gov. Available online: http://clinicaltrials.gov (accessed on 25 October 2014).
- Gradishar, W.J. Sorafenib in locally advanced or metastatic breast cancer. Expert Opin. Investig. Drugs 2012, 21, 1177–1191. [Google Scholar] [CrossRef] [PubMed]
- Schwartzberg, L.S.; Tauer, K.W.; Hermann, R.C.; Makari-Judson, G.; Isaacs, C.; Beck, J.T.; Kaklamani, V.; Stepanski, E.J.; Rugo, H.S.; Wang, W.; et al. Sorafenib or placebo with either gemcitabine or capecitabine in patients with her-2-negative advanced breast cancer that progressed during or after bevacizumab. Clin. Cancer Res. 2013, 19, 2745–2754. [Google Scholar] [CrossRef] [PubMed]
- Huober, J.; Fasching, P.A.; Hanusch, C.; Rezai, M.; Eidtmann, H.; Kittel, K.; Hilfrich, J.; Schwedler, K.; Blohmer, J.U.; Tesch, H.; et al. Neoadjuvant chemotherapy with paclitaxel and everolimus in breast cancer patients with non-responsive tumours to epirubicin/cyclophosphamide (ec) +/− bevacizumab—Results of the randomised geparquinto study (GBG 44). Eur. J. Cancer 2013, 49, 2284–2293. [Google Scholar] [CrossRef] [PubMed]
- Gampenrieder, S.P.; Romeder, F.; Muss, C.; Pircher, M.; Ressler, S.; Rinnerthaler, G.; Bartsch, R.; Sattlberger, C.; Mlineritsch, B.; Greil, R. Hypertension as a predictive marker for bevacizumab in metastatic breast cancer: Results from a retrospective matched-pair analysis. Anticancer Res. 2014, 34, 227–233. [Google Scholar] [PubMed]
- Bertolini, F. Response to anti-angiogenesis: An ever changing feature. Breast 2011, 20, S61–S62. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, A.; Pharoah, P.D.; Narod, S.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Loman, N.; Olsson, H.; Johannsson, O.; Borg, A.; et al. Average risks of breast and ovarian cancer associated with brca1 or brca2 mutations detected in case series unselected for family history: A combined analysis of 22 studies. Am. J. Hum. Genet. 2003, 72, 1117–1130. [Google Scholar] [CrossRef] [PubMed]
- Mahdi, K.M.; Nassiri, M.R.; Nasiri, K. Hereditary genes and snps associated with breast cancer. Asian Pac. J. Cancer Prev. 2013, 14, 3403–3409. [Google Scholar] [CrossRef] [PubMed]
- Nelen, M.R.; Kremer, H.; Konings, I.B.; Schoute, F.; van Essen, A.J.; Koch, R.; Woods, C.G.; Fryns, J.P.; Hamel, B.; Hoefsloot, L.H.; et al. Novel PTEN mutations in patients with cowden disease: Absence of clear genotype-phenotype correlations. Eur. J. Hum. Genet. 1999, 7, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Schneider, B.P.; Wang, M.; Radovich, M.; Sledge, G.W.; Badve, S.; Thor, A.; Flockhart, D.A.; Hancock, B.; Davidson, N.; Gralow, J.; et al. Association of vascular endothelial growth factor and vascular endothelial growth factor receptor-2 genetic polymorphisms with outcome in a trial of paclitaxel compared with paclitaxel plus bevacizumab in advanced breast cancer: ECOG 2100. J. Clin. Oncol. 2008, 26, 4672–4678. [Google Scholar] [CrossRef] [PubMed]
- Miles, D.W.; Chan, A.; Dirix, L.Y.; Cortes, J.; Pivot, X.; Tomczak, P.; Delozier, T.; Sohn, J.H.; Provencher, L.; Puglisi, F.; et al. Phase III study of bevacizumab plus docetaxel compared with placebo plus docetaxel for the first-line treatment of human epidermal growth factor receptor 2-negative metastatic breast cancer. J. Clin. Oncol. 2010, 28, 3239–3247. [Google Scholar] [CrossRef] [PubMed]
- Miles, D.W.; de Haas, S.L.; Dirix, L.Y.; Romieu, G.; Chan, A.; Pivot, X.; Tomczak, P.; Provencher, L.; Cortes, J.; Delmar, P.R.; et al. Biomarker results from the avado phase 3 trial of first-line bevacizumab plus docetaxel for her2-negative metastatic breast cancer. Br. J. Cancer 2013, 108, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Keyhani, E.; Muhammadnejad, A.; Behjati, F.; Sirati, F.; Khodadadi, F.; Karimlou, M.; Moghaddam, F.A.; Pazhoomand, R. Angiogenesis markers in breast cancer—Potentially useful tools for priority setting of anti-angiogenic agents. Asian Pac. J. Cancer Prev. 2013, 14, 7651–7656. [Google Scholar] [CrossRef] [PubMed]
- Jubb, A.M.; Miller, K.D.; Rugo, H.S.; Harris, A.L.; Chen, D.; Reimann, J.D.; Cobleigh, M.A.; Schmidt, M.; Langmuir, V.K.; Hillan, K.J.; et al. Impact of exploratory biomarkers on the treatment effect of bevacizumab in metastatic breast cancer. Clin. Cancer Res. 2011, 17, 372–381. [Google Scholar]
- Ohtsu, A.; Shah, M.A.; van Cutsem, E.; Rha, S.Y.; Sawaki, A.; Park, S.R.; Lim, H.Y.; Yamada, Y.; Wu, J.; Langer, B.; et al. Bevacizumab in combination with chemotherapy as first-line therapy in advanced gastric cancer: A randomized, double-blind, placebo-controlled phase III study. J. Clin. Oncol. 2011, 29, 3968–3976. [Google Scholar] [CrossRef] [PubMed]
- Saltz, L.B.; Clarke, S.; Diaz-Rubio, E.; Scheithauer, W.; Figer, A.; Wong, R.; Koski, S.; Lichinitser, M.; Yang, T.S.; Rivera, F.; et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: A randomized phase III study. J. Clin. Oncol. 2008, 26, 2013–2019. [Google Scholar] [CrossRef] [PubMed]
- Errico, A. Combining bevacizumab with chemotherapy—From maintenance to second-line treatment. Nat. Rev. Clin. Oncol. 2014. [Google Scholar] [CrossRef]
- Pepin, F.; Bertos, N.; Laferriere, J.; Sadekova, S.; Souleimanova, M.; Zhao, H.; Finak, G.; Meterissian, S.; Hallett, M.T.; Park, M. Gene-expression profiling of microdissected breast cancer microvasculature identifies distinct tumor vascular subtypes. Breast Cancer Res. 2012, 14. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Wang, Z.Y.; Mo, S.L.; Loo, T.Y.; Wang, D.M.; Luo, H.B.; Yang, D.P.; Chen, Y.L.; Shen, J.G.; Chen, J.P. Ellagic acid, a phenolic compound, exerts anti-angiogenesis effects via vegfr-2 signaling pathway in breast cancer. Breast Cancer Res. Treat. 2012, 134, 943–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purdue, M.P.; Johansson, M.; Zelenika, D.; Toro, J.R.; Scelo, G.; Moore, L.E.; Prokhortchouk, E.; Wu, X.; Kiemeney, L.A.; Gaborieau, V.; et al. Genome-wide association study of renal cell carcinoma identifies two susceptibility loci on 2p21 and 11q13.3. Nat. Genet. 2011, 43, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Sledge, G.W. Anti-vascular endothelial growth factor therapy in breast cancer: Game over? J. Clin. Oncol. 2014. [Google Scholar] [CrossRef]
- De Luca, A.; Lamura, L.; Gallo, M.; Maffia, V.; Normanno, N. Mesenchymal stem cell-derived interleukin-6 and vascular endothelial growth factor promote breast cancer cell migration. J. Cell Biochem. 2012, 113, 3363–3370. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kristensen, T.B.; Knutsson, M.L.T.; Wehland, M.; Laursen, B.E.; Grimm, D.; Warnke, E.; Magnusson, N.E. Anti-Vascular Endothelial Growth Factor Therapy in Breast Cancer. Int. J. Mol. Sci. 2014, 15, 23024-23041. https://doi.org/10.3390/ijms151223024
Kristensen TB, Knutsson MLT, Wehland M, Laursen BE, Grimm D, Warnke E, Magnusson NE. Anti-Vascular Endothelial Growth Factor Therapy in Breast Cancer. International Journal of Molecular Sciences. 2014; 15(12):23024-23041. https://doi.org/10.3390/ijms151223024
Chicago/Turabian StyleKristensen, Tina Bøgelund, Malin L. T. Knutsson, Markus Wehland, Britt Elmedal Laursen, Daniela Grimm, Elisabeth Warnke, and Nils E. Magnusson. 2014. "Anti-Vascular Endothelial Growth Factor Therapy in Breast Cancer" International Journal of Molecular Sciences 15, no. 12: 23024-23041. https://doi.org/10.3390/ijms151223024