PSMA, EpCAM, VEGF and GRPR as Imaging Targets in Locally Recurrent Prostate Cancer after Radiotherapy

Abstract
:1. Introduction
2. Results and Discussion
2.1. Results
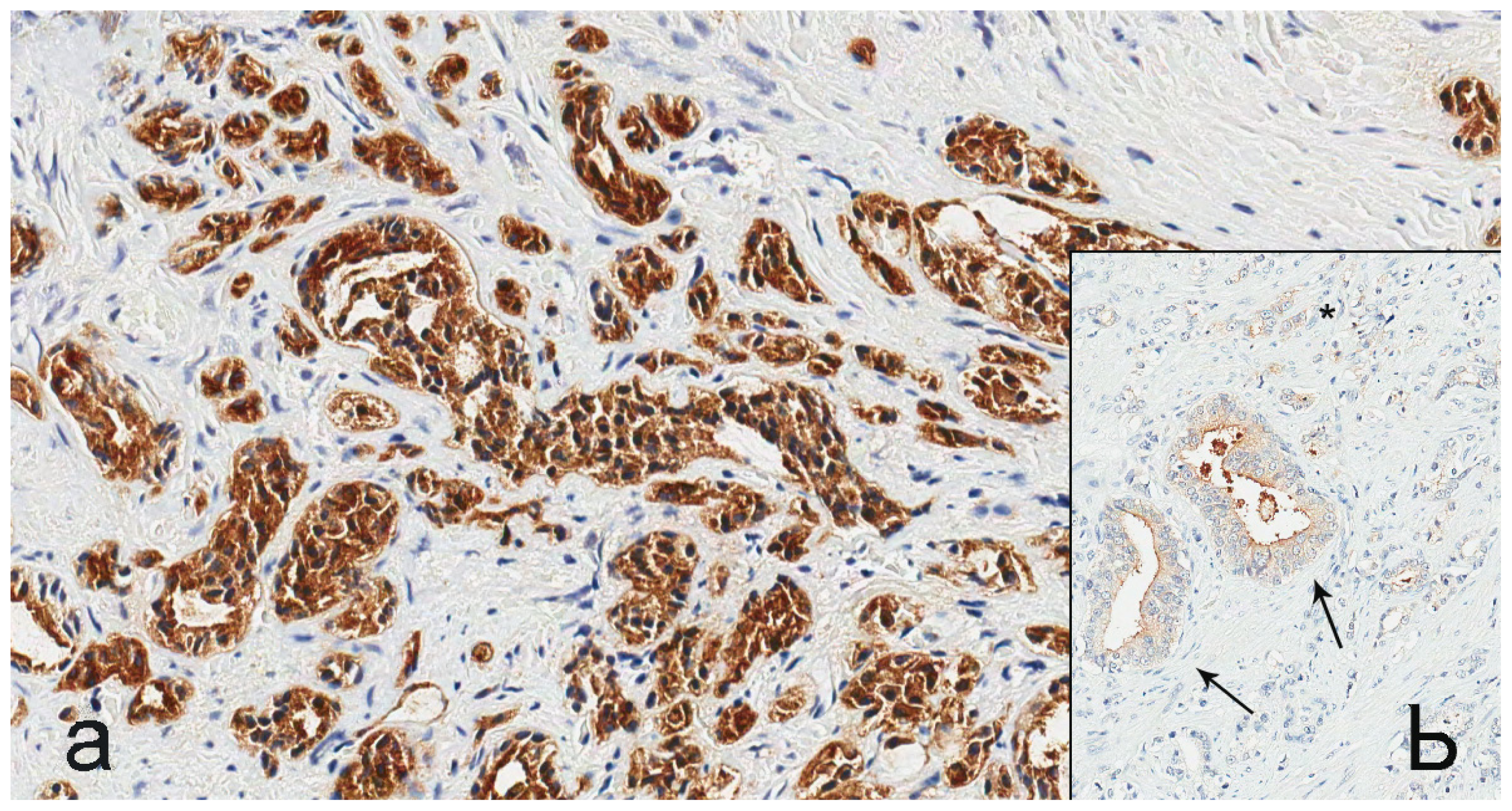
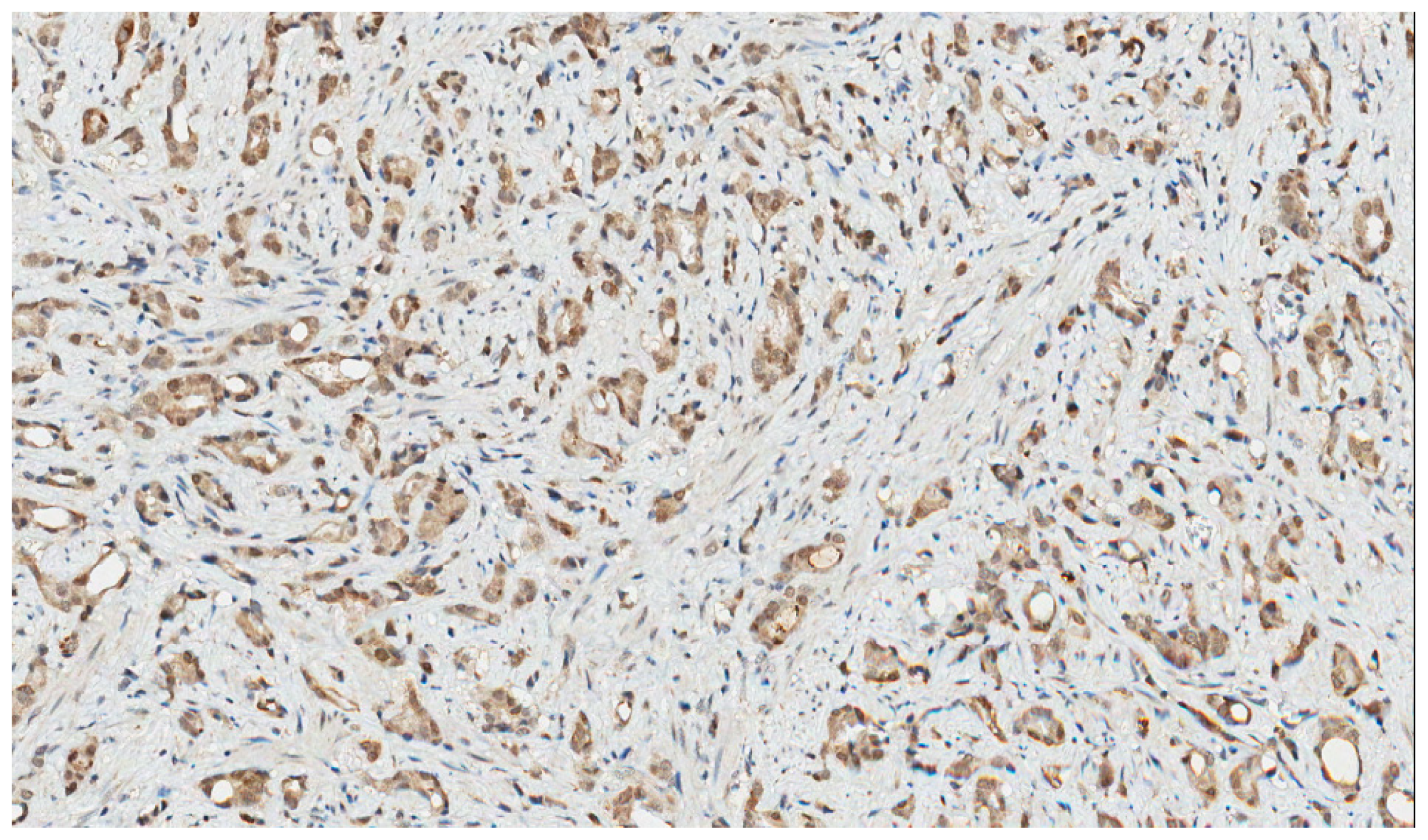
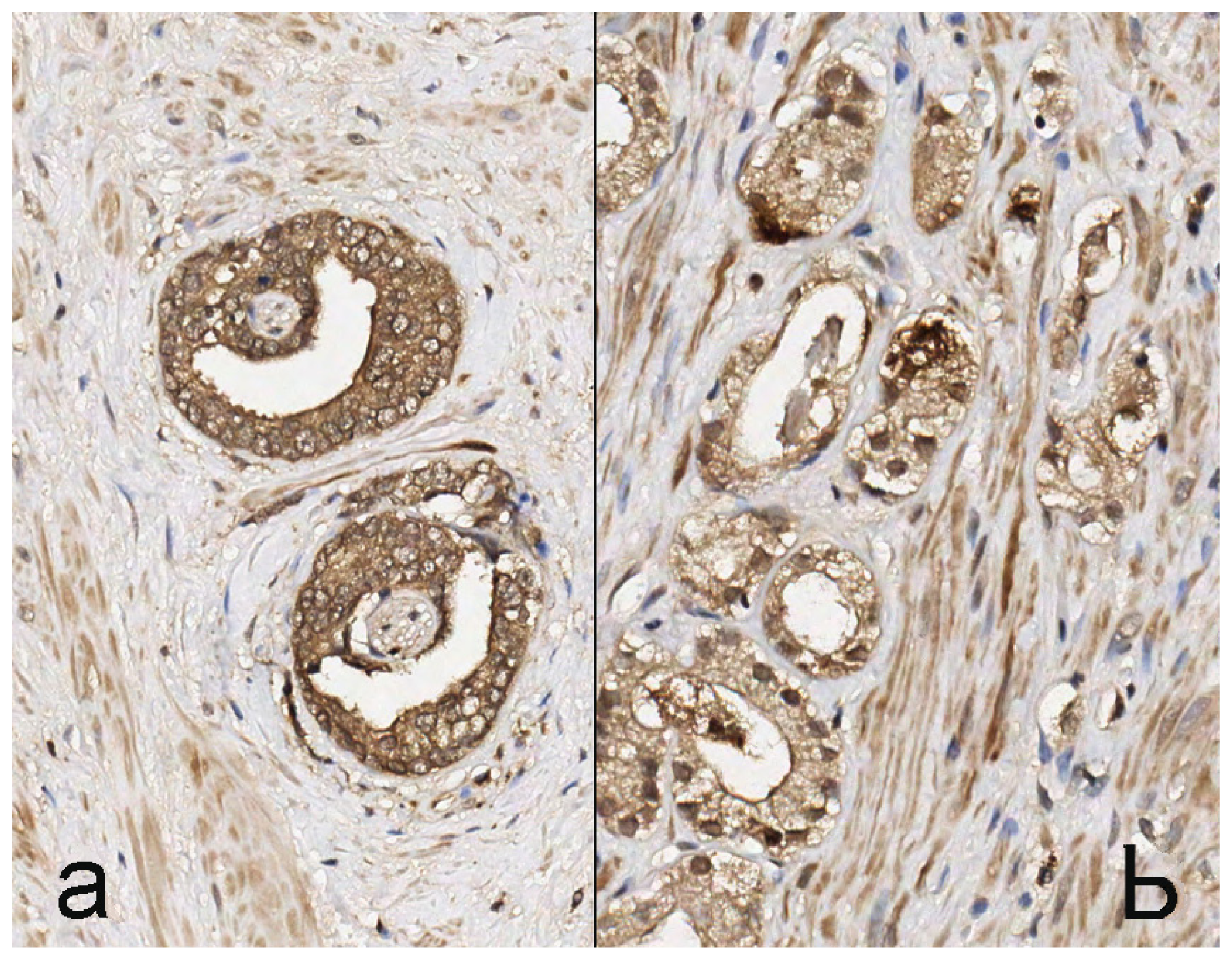
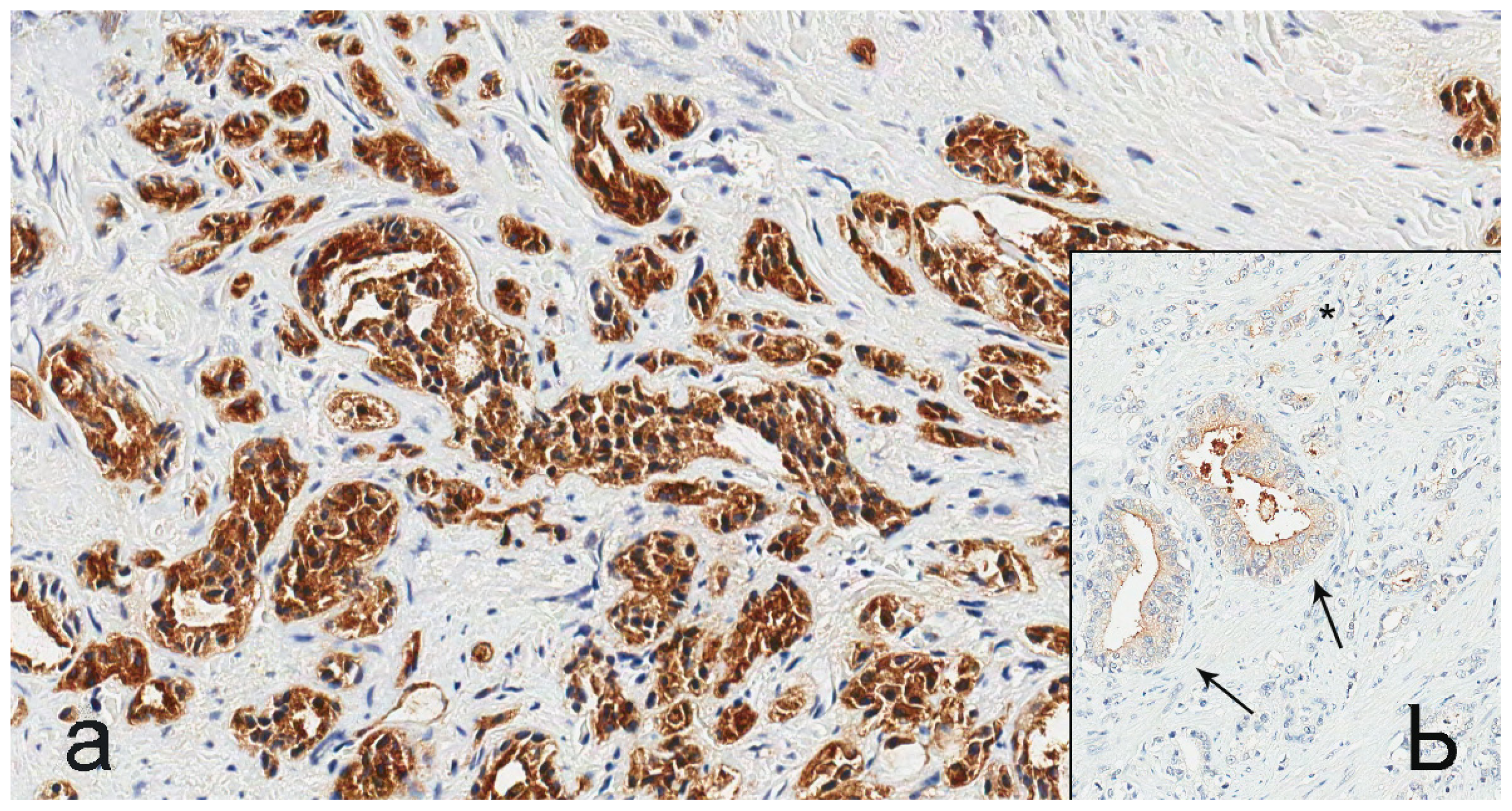
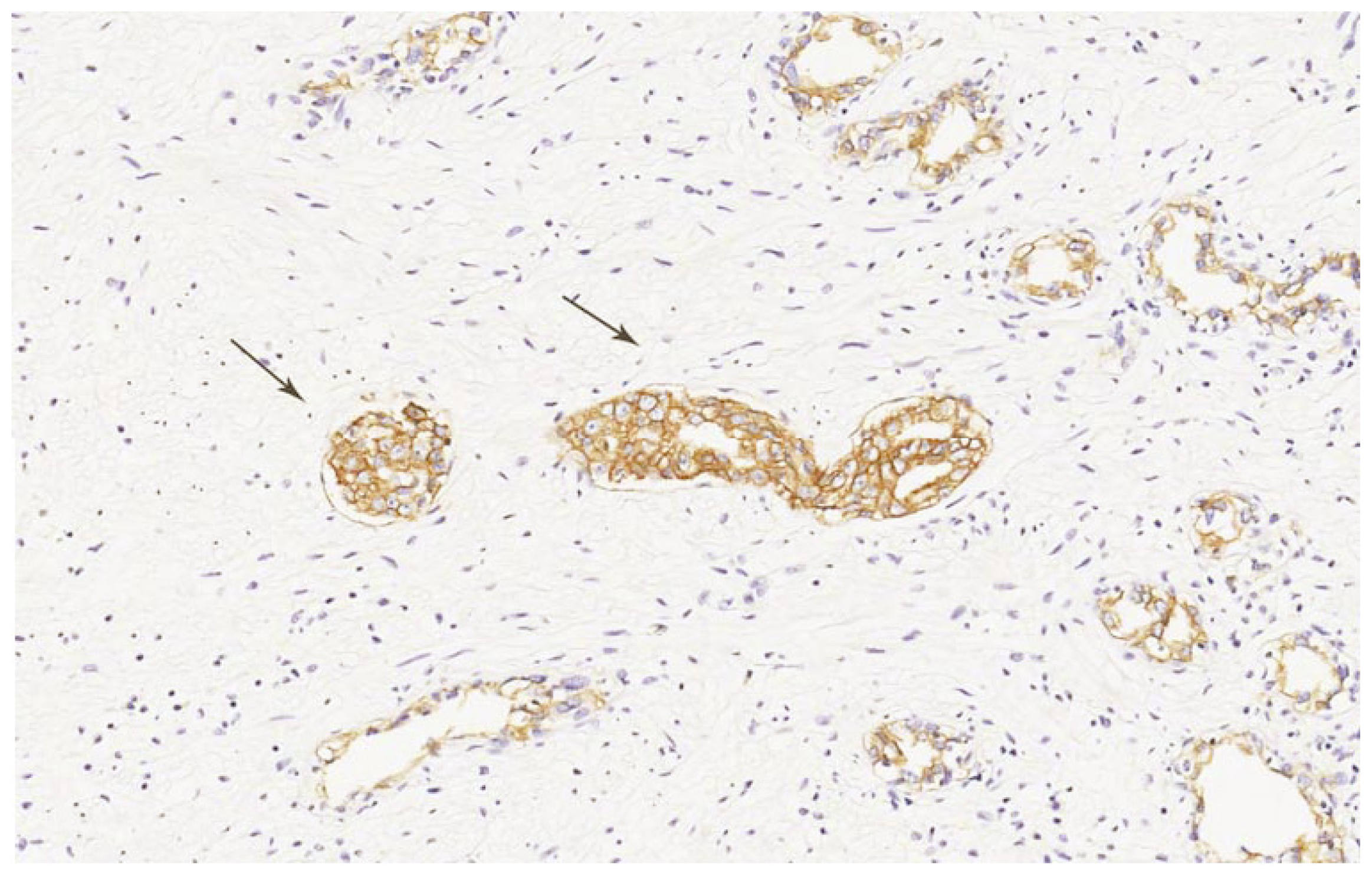
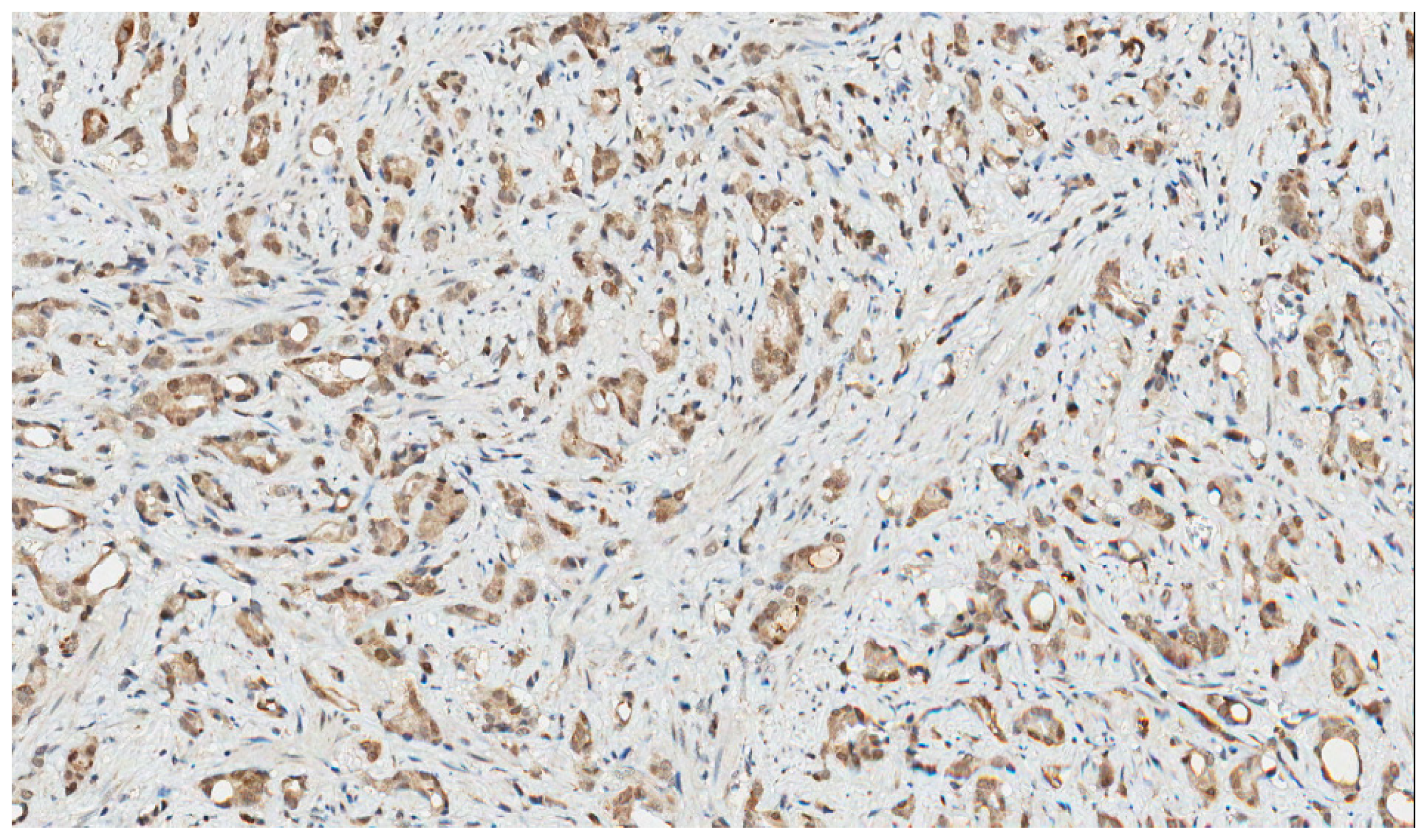
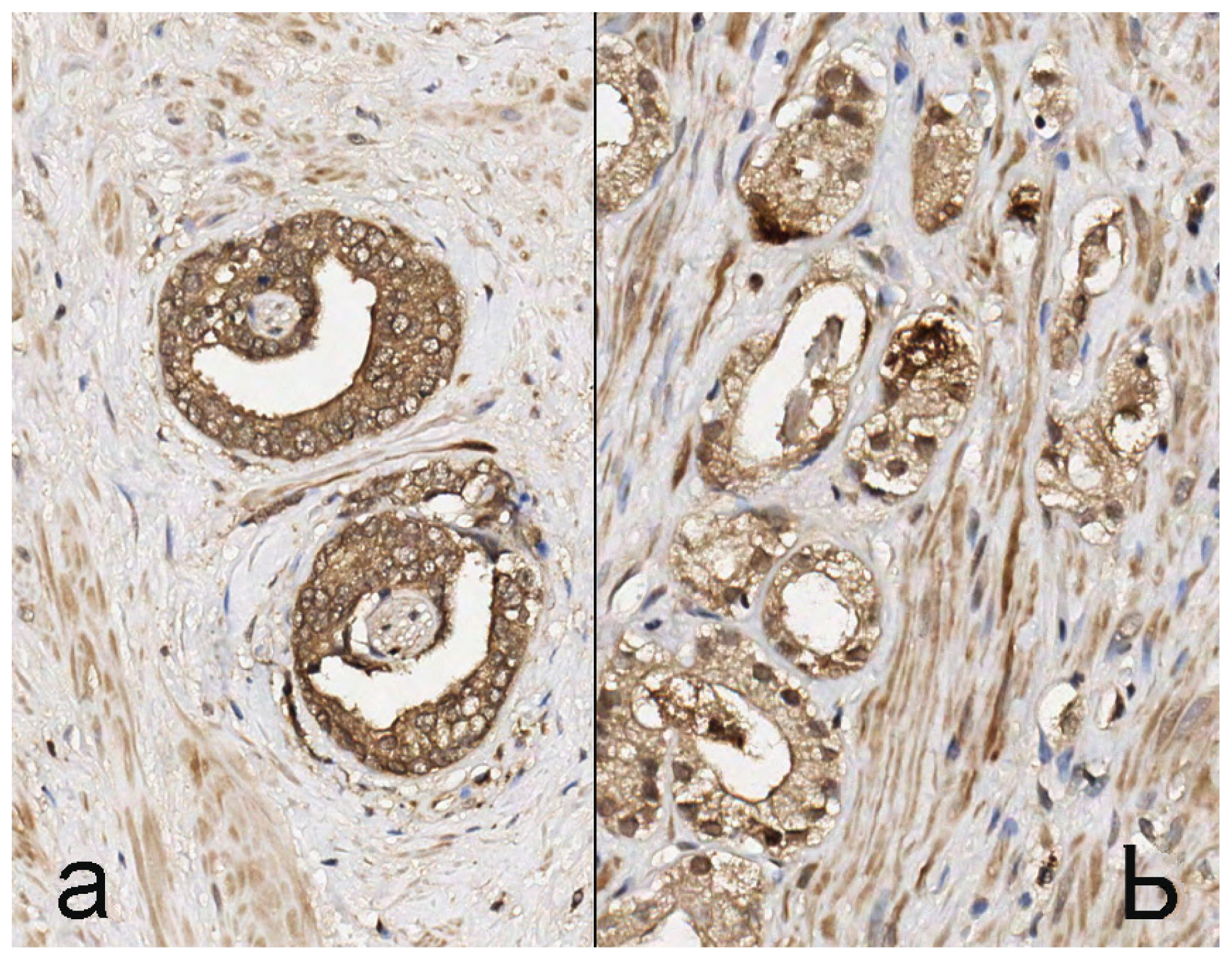
2.2. Staining Pattern
2.3. Discussion
3. Experimental Section
3.1. Materials
3.2. Immunohistochemistry
3.2.1. PSMA
3.2.2. GRPR
3.2.3. EpCAM
3.2.4. VEGF
3.3. Assessment of Staining Patterns
4. Conclusions
Acknowledgments
Conflicts of Interest
References
- Center, M.M.; Jemal, A.; Lortet-Tieulent, J.; Ward, E.; Ferlay, J.; Brawley, O.; Bray, F. International variation in prostate cancer incidence and mortality rates. Eur. Urol 2012, 61, 1079–1092. [Google Scholar]
- Kupelian, P.A.; Potters, L.; Khuntia, D.; Ciezki, J.P.; Reddy, C.A.; Reuther, A.M.; Carlson, T.P.; Klein, E.A. Radical prostatectomy, external beam radiotherapy <72 Gy, external beam radiotherapy > or =72 Gy, permanent seed implantation, or combined seeds/external beam radiotherapy for stage T1-T2 prostate cancer. Int. J. Radiat. Oncol. Biol. Phys 2004, 58, 25–33. [Google Scholar]
- Bellmunt, J.; Attard, G.; Bahl, A.; Huland, H.; Klotz, L.; Kuban, D.; Oudard, S.; Watson, W. Advances in the management of high-risk localised and metastatic prostate cancer. BJU Int 2012, 109, 8–13. [Google Scholar]
- Hillier, S.M.; Maresca, K.P.; Femia, F.J.; Marquis, J.C.; Foss, C.A.; Nguyen, N.; Zimmerman, C.N.; Barrett, J.A.; Eckelman, W.C.; Pomper, M.G.; et al. Preclinical evaluation of novel glutamate-urea-lysine analogues that target prostate-specific membrane antigen as molecular imaging pharmaceuticals for prostate cancer. Cancer Res 2009, 69, 6932–6940. [Google Scholar]
- Kularatne, S.A.; Wang, K.; Santhapuram, H.K.; Low, P.S. Prostate-specific membrane antigen targeted imaging and therapy of prostate cancer using a PSMA inhibitor as a homing ligand. Mol. Pharm 2009, 6, 780–789. [Google Scholar]
- Entwistle, J.; Brown, J.G.; Chooniedass, S.; Cizeau, J.; MacDonald, G.C. Preclinical evaluation of VB6-845: An anti-EpCAM immunotoxin with reduced immunogenic potential. Cancer Biother. Radiopharm 2012, 27, 582–592. [Google Scholar]
- Köllermann, J.; Helpap, B. Expression of vascular endothelial growth factor (VEGF) and VEGF receptor Flk-1 in benign, premalignant, and malignant prostate tissue. Am. J. Clin. Pathol 2001, 116, 115–121. [Google Scholar]
- Ananias, H.J.; van den Heuvel, M.C.; Helfrich, W.; de Jong, I.J. Expression of the gastrin-releasing peptide receptor, the prostate stem cell antigen and the prostate-specific membrane antigen in lymph node and bone metastases of prostate cancer. Prostate 2009, 69, 1101–1108. [Google Scholar]
- Bouchelouche, K.; Choyke, P.L.; Capala, J. Prostate specific membrane antigen—A target for imaging and therapy with radionuclides. Discov. Med 2010, 9, 55–61. [Google Scholar]
- Ghosh, A.; Heston, W.D. Tumor target prostate specific membrane antigen (PSMA) and its regulation in prostate cancer. J. Cell. Biochem 2004, 91, 528–539. [Google Scholar]
- Ross, J.S.; Sheehan, C.E.; Fisher, H.A.; Kaufman, R.P., Jr.; Kaur, P.; Gray, K.; Webb, I.; Gray, G.S.; Mosher, R.; Kallakury, B.V. Correlation of primary tumor prostate-specific membrane antigen expression with disease recurrence in prostate cancer. Clin. Cancer Res 2003, 9, 6357–6362. [Google Scholar]
- Elsasser-Beile, U.; Buhler, P.; Wolf, P. Targeted therapies for prostate cancer against the prostate specific membrane antigen. Curr. Drug Targets 2009, 10, 118–125. [Google Scholar]
- Bouchelouche, K.; Capala, J. Image and treat—An individualized approach to urological tumors. Curr. Opin. Oncol 2010, 22, 274–280. [Google Scholar]
- Bostwick, D.G.; Pacelli, A.; Blute, M.; Roche, P.; Murphy, G.P. Prostate specific membrane antigen expression in prostatic intraepithelial neoplasia and adenocarcinoma: A study of 184 cases. Cancer 1998, 82, 2256–2261. [Google Scholar]
- Lapidus, R.G.; Tiffany, C.W.; Isaacs, J.T.; Slusher, B.S. Prostate-specific membrane antigen (PSMA) enzyme activity is elevated in prostate cancer cells. Prostate 2000, 45, 350–354. [Google Scholar]
- Liu, H.; Moy, P.; Kim, S.; Xia, Y.; Rajasekaran, A.; Navarro, V.; Knudsen, B.; Bander, N.H. Monoclonal antibodies to the extracellular domain of prostate-specific membrane antigen also react with tumor vascular endothelium. Cancer Res 1997, 57, 3629–3634. [Google Scholar]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res 1997, 3, 81–85. [Google Scholar]
- Minner, S.; Wittmer, C.; Graefen, M.; Salomon, G.; Steuber, T.; Haese, A.; Huland, H.; Bokemeyer, C.; Yekebas, E.; Dierlamm, J.; et al. High level PSMA expression is associated with early PSA recurrence in surgically treated prostate cancer. Prostate 2011, 71, 281–288. [Google Scholar]
- Rajasekaran, A.K.; Anilkumar, G.; Christiansen, J.J. Is prostate-specific membrane antigen a multifunctional protein? Am. J. Physiol. Cell Physiol 2005, 288, C975–C981. [Google Scholar]
- Bermejo, C.E.; Coursey, J.; Basler, J.; Austenfeld, M.; Thompson, I. Histologic confirmation of lesions identified by Prostascint scan following definitive treatment. Urol. Oncol 2003, 21, 349–352, discussion 353. [Google Scholar]
- Lau, H.Y.; Kindrachuk, G.; Carter, M.; Prestage, K.; Webber, D.; Stauffer, E.; Haseman, M. Surgical confirmation of ProstaScint abnormalities in two patients with high risk prostate cancer. Can. J. Urol 2001, 8, 1199–1202. [Google Scholar]
- Hinkle, G.H.; Burgers, J.K.; Olsen, J.O.; Williams, B.S.; Lamatrice, R.A.; Barth, R.F.; Rogers, B.; Maguire, R.T. Prostate cancer abdominal metastases detected with indium-111 capromab pendetide. J. Nucl. Med 1998, 39, 650–652. [Google Scholar]
- Manyak, M.J.; Hinkle, G.H.; Olsen, J.O.; Chiaccherini, R.P.; Partin, A.W.; Piantadosi, S.; Burgers, J.K.; Texter, J.H.; Neal, C.E.; Libertino, J.A.; et al. Immunoscintigraphy with indium-111-capromab pendetide: Evaluation before definitive therapy in patients with prostate cancer. Urology 1999, 54, 1058–1063. [Google Scholar]
- Taneja, S.S. ProstaScint® Scan: Contemporary use in clinical practice. Rev. Urol 2004, 6, S19–S28. [Google Scholar]
- Trzpis, M.; McLaughlin, P.M.; de Leij, L.M.; Harmsen, M.C. Epithelial cell adhesion molecule: More than a carcinoma marker and adhesion molecule. Am. J. Pathol 2007, 171, 386–395. [Google Scholar]
- Went, P.; Vasei, M.; Bubendorf, L.; Terracciano, L.; Tornillo, L.; Riede, U.; Kononen, J.; Simon, R.; Sauter, G.; Baeuerle, P.A. Frequent high-level expression of the immunotherapeutic target Ep-CAM in colon, stomach, prostate, and lung cancers. Br. J. Cancer 2006, 94, 128–135. [Google Scholar]
- Van der Gun, B.T.; Melchers, L.J.; Ruiters, M.H.; de Leij, L.F.; McLaughlin, P.M.; Rots, M.G. EpCAM in carcinogenesis: The good, the bad, or the ugly. Carcinogenesis 2010, 31, 1913–1921. [Google Scholar]
- Stoecklein, N.H.; Siegmund, A.; Scheunemann, P.; Luebke, A.M.; Erbersdobler, A.; Verde, P.E.; Eisenberger, C.F.; Peiper, M.; Rehders, A.; Esch, J.S.; et al. Ep-CAM expression in squamous cell carcinoma of the esophagus: A potential therapeutic target and prognostic marker. BMC Cancer 2006, 6, 165. [Google Scholar]
- Went, P.T.; Lugli, A.; Meier, S.; Bundi, M.; Mirlacher, M.; Sauter, G.; Dirnhofer, S. Frequent EpCam protein expression in human carcinomas. Hum. Pathol 2004, 35, 122–128. [Google Scholar]
- Poczatek, R.B.; Myers, R.B.; Manne, U.; Oelschlager, D.K.; Weiss, H.L.; Bostwick, D.G.; Grizzle, W.E. Ep-Cam levels in prostatic adenocarcinoma and prostatic intraepithelial neoplasia. J. Urol 1999, 162, 1462–1466. [Google Scholar]
- Varga, M.; Obrist, P.; Schneeberger, S.; Mühlmann, G.; Felgel-Farnholz, C.; Fong, D.; Zitt, M.; Brunhuber, T.; Schäfer, G.; Gastl, G.; et al. Overexpression of epithelial cell adhesion molecule antigen in gallbladder carcinoma is an independent marker for poor survival. Clin. Cancer Res 2004, 10, 3131–3136. [Google Scholar]
- Ni, J.; Cozzi, P.J.; Duan, W.; Shigdar, S.; Graham, P.H.; John, K.H.; Li, Y. Role of the EpCAM (CD326) in prostate cancer metastasis and progression. Cancer Metastasis Rev 2012, 31, 779–791. [Google Scholar]
- Patriarca, C.; Macchi, R.M.; Marschner, A.K.; Mellstedt, H. Epithelial cell adhesion molecule expression (CD326) in cancer: A short review. Cancer Treat. Rev 2012, 38, 68–75. [Google Scholar]
- Benko, G.; Spajić, B.; Krušlin, B.; Tomas, D. Impact of the EpCAM expression on biochemical recurrence-free survival in clinically localized prostate cancer. Urol. Oncol 2013, 31, 468–474. [Google Scholar]
- Ferrara, N. Molecular and biological properties of vascular endothelial growth factor. J. Mol. Med 1999, 77, 527–543. [Google Scholar]
- Ferrara, N.; Gerber, H.P.; LeCouter, J. The biology of VEGF and its receptors. Nat. Med 2003, 9, 669–676. [Google Scholar]
- Ferrara, N. Vascular endothelial growth factor: Basic science and clinical progress. Endocr. Rev 2004, 25, 581–611. [Google Scholar]
- Kaushal, V.; Mukunyadzi, P.; Dennis, R.A.; Siegel, E.R.; Johnson, D.E.; Kohli, M. Stage-specific characterization of the vascular endothelial growth factor axis in prostate cancer: Expression of lymphangiogenic markers is associated with advanced-stage disease. Clin. Cancer Res 2005, 11, 584–593. [Google Scholar]
- Peyromaure, M.; Badoual, C.; Camparo, P.; Grabar, S.; Goulvestre, C.; Fulla, Y.; Vieillefond, A.; Mao, K.; Dinh-Xuan, A.T. Plasma levels and expression of vascular endothelial growth factor-A in human localized prostate cancer. Oncol. Rep 2007, 18, 145–149. [Google Scholar]
- Borre, M.; Nerstrøm, B.; Overgaard, J. Association between immunohistochemical expression of vascular endothelial growth factor (VEGF), VEGF-expressing neuroendocrine-differentiated tumor cells, and outcome in prostate cancer patients subjected to watchful waiting. Clin. Cancer Res 2000, 6, 1882–1890. [Google Scholar]
- Jackson, M.W.; Bentel, J.M.; Tilley, W.D. Vascular endothelial growth factor (VEGF) expression in prostate cancer and benign prostatic hyperplasia. J. Urol 1997, 157, 2323–2328. [Google Scholar]
- Ferrer, F.A.; Miller, L.J.; Andrawis, R.I.; Kurtzman, S.H.; Albertsen, P.C.; Laudone, V.P.; Kreutzer, D.L. Vascular endothelial growth factor (VEGF) expression in human prostate cancer: In situ and in vitro expression of VEGF by human prostate cancer cells. J. Urol 1997, 157, 2329–2333. [Google Scholar]
- El-Gohary, Y.M.; Silverman, J.F.; Olson, P.R.; Liu, Y.L.; Cohen, J.K.; Miller, R.; Saad, R.S. Endoglin (CD105) and vascular endothelial growth factor as prognostic markers in prostatic adenocarcinoma. Am. J. Clin. Pathol 2007, 127, 572–579. [Google Scholar]
- Pasquali, D.; Rossi, V.; Staibano, S.; de Rosa, G.; Chieffi, P.; Prezioso, D.; Mirone, V.; Mascolo, M.; Tramontano, D.; Bellastella, A.; et al. The endocrine-gland-derived vascular endothelial growth factor (EG-VEGF)/prokineticin 1 and 2 and receptor expression in human prostate: Up-regulation of EG-VEGF/prokineticin 1 with malignancy. Endocrinology 2006, 147, 4245–4251. [Google Scholar]
- Pallares, J.; Rojo, F.; Iriarte, J.; Morote, J.; Armadans, L.I.; de Torres, I. Study of microvessel density and the expression of the angiogenic factors VEGF, bFGF and the receptors Flt-1 and FLK-1 in benign, premalignant and malignant prostate tissues. Histol. Histopathol 2006, 21, 857–865. [Google Scholar]
- Walsh, K.; Sriprasad, S.; Hopster, D.; Codd, J.; Mulvin, D. Distribution of vascular endothelial growth factor (VEGF) in prostate disease. Prostate Cancer Prostatic Dis 2002, 5, 119–122. [Google Scholar]
- Kwak, C.; Jin, R.J.; Lee, C.; Park, M.S.; Lee, S.E. Thrombospondin-1, vascular endothelial growth factor expression and their relationship with p53 status in prostate cancer and benign prostatic hyperplasia. BJU Int 2002, 89, 303–309. [Google Scholar]
- Strohmeyer, D.; Rössing, C.; Bauerfeind, A.; Kaufmann, O.; Schlechte, H.; Bartsch, G.; Loening, S. Vascular endothelial growth factor and its correlation with angiogenesis and p53 expression in prostate cancer. Prostate 2000, 45, 216–224. [Google Scholar]
- Mazzucchelli, R.; Montironi, R.; Santinelli, A.; Lucarini, G.; Pugnaloni, A.; Biagini, G. Vascular endothelial growth factor expression and capillary architecture in high-grade PIN and prostate cancer in untreated and androgen-ablated patients. Prostate 2000, 45, 72–79. [Google Scholar]
- Mao, K.; Badoual, C.; Camparo, P.; Delongchamps, N.B.; Vieillefond, A.; Dinh-Xuan, A.T.; Peyromaure, M. The prognostic value of vascular endothelial growth factor (VEGF)-A and its receptor in clinically localized prostate cancer: A prospective evaluation in 100 patients undergoing radical prostatectomy. Can. J. Urol 2008, 15, 4257–4262. [Google Scholar]
- Boddy, J.L.; Fox, S.B.; Han, C.; Campo, L.; Turley, H.; Kanga, S.; Malone, P.R.; Harris, A.L. The androgen receptor is significantly associated with vascular endothelial growth factor and hypoxia sensing via hypoxia-inducible factors HIF1a, HIF2a, and the prolyl hydroxylases in human prostate cancer. Clin. Cancer Res 2005, 11, 7658–7663. [Google Scholar]
- Jans, J.; van Dijk, J.H.; van Schelven, S.; van der Groep, P.; Willems, S.H.; Jonges, T.N.; van Diest, P.J.; Bosch, J.L. Expression and localization of hypoxia proteins in prostate cancer: Prognostic implications after radical prostatectomy. Urology 2010, 75, 786–792. [Google Scholar]
- Mao, K.; Camparo, P.; Badoual, C.; Peyromaure, M.; Delongchamps, N.B.; Vieillefond, A.; Dinh-Xuan, A.T. The association of vascular endothelial growth factor receptor-1 with the risk of cancer progression following radical prostatectomy. Oncol. Rep 2008, 19, 171–175. [Google Scholar]
- Aprikian, A.G.; Cordon-Cardo, C.; Fair, W.R.; Reuter, V.E. Characterization of neuroendocrine differentiation in human benign prostate and prostatic adenocarcinoma. Cancer 1993, 71, 3952–3965. [Google Scholar]
- Cutz, E.; Chan, W.; Track, N.S. Bombesin, calcitonin and leuenkephalin immunoreactivity in endocrine cells of human lung. Experientia 1981, 37, 765–767. [Google Scholar]
- Price, J.; Penman, E.; Wass, J.A.; Rees, L.H. Bombesin-like immunoreactivity inhumangastrointestinal tract. Regul. Pept 1984, 9, 1–10. [Google Scholar]
- Spindel, E.R.; Chin, W.W.; Price, J.; Rees, L.H.; Besser, G.M.; Habener, J.F. Cloning and characterization of cDNAs encoding human gastrin-releasing peptide. Proc. Natl. Acad. Sci. USA 1984, 81, 5699–5703. [Google Scholar]
- Track, N.S.; Cutz, E. Bombesin-like immunoreactivity in developing human lung. Life Sci 1982, 30, 1553–1556. [Google Scholar]
- Xiao, D.; Wang, J.; Hampton, L.L.; Weber, H.C. The human gastrinreleasing peptide receptor gene structure, its tissue expression and promoter. Gene 2001, 264, 95–103. [Google Scholar]
- Beer, M.; Montani, M.; Gerhardt, J.; Wild, P.J.; Hany, T.F.; Hermanns, T.; Müntener, M.; Kristiansen, G. Profiling gastrin-releasing peptide receptor in prostate tissues: Clinical implications and molecular correlates. Prostate 2012, 72, 318–325. [Google Scholar]
- Bartholdi, M.F.; Wu, J.M.; Pu, H.; Troncoso, P.; Eden, P.A.; Feldman, R.I. In situ hybridization for gastrin-releasing peptide receptor (GRP receptor) expression in prostatic carcinoma. Int. J. Cancer 1998, 79, 82–90. [Google Scholar]
- Markwalder, R.; Reubi, J.C. Gastrin-releasing peptide receptors in the human prostate: Relation to neoplastic transformation. Cancer Res 1999, 59, 1152–1159. [Google Scholar]
- Bologna, M.; Festuccia, C.; Muzi, P.; Biordi, L.; Ciomei, M. Bombesin stimulates growth of human prostatic cancer cellsin vitro. Cancer 1989, 63, 1714–1720. [Google Scholar]
- Shimoda, J. Effects of bombesin and its antibody on growth of human prostatic carcinoma cell lines. Nihon Hinyokika Gakkai Zasshi 1992, 83, 1459–1468. [Google Scholar]
- Zellweger, T.; Ninck, C.; Bloch, M.; Mirlacher, M.; Koivisto, P.A.; Helin, H.J.; Mihatsch, M.J.; Gasser, T.C.; Bubendorf, L. Expression patterns of potential therapeutic targets in prostate cancer. Int. J. Cancer 2005, 113, 619–628. [Google Scholar]
- Li, R.; Younes, M.; Wheeler, T.M.; Scardino, P.; Ohori, M.; Frolov, A.; Ayala, G. Expression of vascular endothelial growth factor receptor-3 (VEGFR-3) in human prostate. Prostate 2004, 58, 193–199. [Google Scholar]
- Inoue, Y.; Ojima, E.; Watanabe, H.; Hiro, J.; Toiyama, Y.; Kobayashi, M.; Miki, C.; Kusunoki, M. Does preoperative chemo-radiotherapy enhance the expression of vascular endothelial growth factor in patients with rectal cancer? Oncol. Rep 2007, 18, 369–375. [Google Scholar]
- Bellone, S.; Siegel, E.R.; Cocco, E.; Cargnelutti, M.; Silasi, D.A.; Azodi, M.; Schwartz, P.E.; Rutherford, T.J.; Pecorelli, S.; Santin, A.D. Overexpression of epithelial cell adhesion molecule in primary, metastatic, and recurrent/chemotherapy-resistant epithelial ovarian cancer: Implications for epithelial cell adhesion molecule-specific immunotherapy. Int. J. Gynecol. Cancer 2009, 19, 860–866. [Google Scholar]
- Koomagi, R.; Zintl, F.; Sauerbrey, A.; Volm, M. Vascular endothelial growth factor in newly diagnosed and recurrent childhood acute lymphoblastic leukemia as measured by real-time quantitative polymerase chain reaction. Clin. Cancer Res 2001, 7, 3381–3384. [Google Scholar]
- Ananias, H.J.; de Jong, I.J.; Dierckx, R.A.; van de Wiele, C.; Helfrich, W.; Elsinga, P.H. Nuclear imaging of prostate cancer with gastrin-releasing-peptide-receptor targeted radiopharmaceuticals. Curr. Pharm. Des 2008, 14, 3033–3047. [Google Scholar]
- Afshar-Oromieh, A.; Malcher, A.; Eder, M.; Eisenhut, M.; Linhart, H.G.; Hadaschik, B.A.; Holland-Letz, T.; Giesel, F.L.; Kratochwil, C.; Haufe, S.; et al. PET imaging with a [68Ga]gallium-labelled PSMA ligand for the diagnosis of prostate cancer: Biodistribution in humans and first evaluation of tumour lesions. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 486–495. [Google Scholar]
- Cho, S.Y.; Gage, K.L.; Mease, R.C.; Senthamizhchelvan, S.; Holt, D.P.; Jeffrey-Kwanisai, A.; Endres, C.J.; Dannals, R.F.; Sgouros, G.; Lodge, M.; et al. Biodistribution, tumor detection, and radiation dosimetry of 18F-DCFBC, a low-molecular-weight inhibitor of prostate-specific membrane antigen, in patients with metastatic prostate cancer. J. Nucl. Med 2012, 53, 1883–1891. [Google Scholar]
- Cai, W.; Chen, X. Multimodality molecular imaging of tumor angiogenesis. J. Nucl. Med 2008, 49, 113S–128S. [Google Scholar]
- Hsieh, W.J.; Liang, C.J.; Chieh, J.J.; Wang, S.H.; Lai, I.R.; Chen, J.H.; Chang, F.H.; Tseng, W.K.; Yang, S.Y.; Wu, C.C.; et al. In vivo tumor targeting and imaging with anti-vascular endothelial growth factor antibody-conjugated dextran-coated iron oxide nanoparticles. Int. J. Nanomed 2012, 7, 2833–2842. [Google Scholar]
- Song, Y.; Zhu, Z.; An, Y.; Zhang, W.; Zhang, H.; Liu, D.; Yu, C.; Duan, W.; Yang, C.J. Selection of DNA aptamers against epithelial cell adhesion molecule for cancer cell imaging and circulating tumor cell capture. Anal. Chem 2013, 85, 4141–4149. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No. | Radiotherapy (Dose in Gy) | Hormonal Status Prior to Salvage Prostatectomy | Interval between Radiotherapy and Salvage Prostatectomy (Months) | Stage | Gleason | PSMA | EpCAM | VEGF | GRPR |
|---|---|---|---|---|---|---|---|---|---|
| 1 | EBRT (Dose unknown) | LHRH + AA | 51 | pT3b | 7 | ++ | + | ++ | +++ |
| 2 | Brachytherapy (HDR) | None | 45 | pT2c | 8 | + | ++ | ++ | +++ |
| 3 | EBRT (70) | LHRH + AA | 58 | pT3b | 8 | + | − | + | +++ |
| 4 | EBRT (70) | None | 24 | pT3a | 7 | + | + | − | ++ |
| 5 | EBRT (Dose unknown) | None | 80 | pT2c | 7 | ++ | + | − | + |
| 6 | Brachytherapy (LDR) | None | 47 | pT2c | cnd | + | + | − | +++ |
| 7 | EBRT (70) | LHRH + AA | 120 | pT3a | 7 | +++ | − | + | + |
| 8 | EBRT (66) | None | 31 | pT3b | 8 | + | − | + | + |
| 9 | EBRT (66) | None | 78 | pT4 | 7 | +++ | +++ | + | +++ |
| 10 | EBRT (66) | None | 48 | pT3b | 8 | +++ | ++ | ++ | +++ |
| 11 | EBRT (Dose unknown) | Unknown | 63 | pT3b | 7 | +++ | +++ | +++ | ++ |
| 12 | Brachytherapy (LDR) | None | 41 | pT4 | 7 | +++ | +++ | + | ++ |
| 13 | EBRT (70) | None | 49 | pT3a | 8 | + | ++ | ++ | ++ |
| 14 | EBRT (68) | LHRH | 58 | pT3a | 6 | +++ | +++ | ++ | +++ |
| 15 | Brachytherapy (LDR) | AA | 88 | pT3b | 8 | +++ | ++ | ++ | +++ |
| 16 | EBRT (68) | None | 13 | pT3b | 6 | + | ++ | + | ++ |
| 17 | EBRT (70) | LHRH | 34 | pT3b | 10 | +++ | ++ | + | ++ |
| Staining Intensity | PSMA Prostate Cancer | PSMA Stroma | EpCAM Prostate Cancer | EpCAM Stroma | VEGF Prostate Cancer | VEGF Stroma | GRPR Prostate Cancer | GRPR Stroma |
|---|---|---|---|---|---|---|---|---|
| 0 | 0 (0%) | 17 (100%) | 3 (17.7%) | 17 (100%) | 3 (17.7%) | 17 (100%) | 0 (0%) | 0 (0%) |
| 1+ | 7 (41.2%) | - | 4 (23.5%) | - | 7 (41.2%) | - | 3 (17.7%) | 3 (17.7%) |
| 2+ | 2 (11.8%) | - | 6 (35.3%) | - | 6 (35.3%) | - | 6 (35.3%) | 8 (47.0%) |
| 3+ | 8 (47.0%) | - | 4 (23.5%) | - | 1 (5.8%) | - | 8 (47.0%) | 6 (35.3%) |
| Overall+ | 17/17 (100%) | 0/17 (0%) | 14/17 (82.3%) | 0/17 (0%) | 14/17 (82.3%) | 0/17 (0%) | 17/17 (100%) | 17/17 (100%) |
| Tumor distinctiveness | PSMA | EpCAM | VEGF | GRPR |
|---|---|---|---|---|
| 0 | - | 3 (17.7%) | 3 (17.7%) | 15 (88.2%) |
| 1 | 7 (41.2%) | 4 (23.5%) | 7 (41.2%) | 2 (11.8%) |
| 2 | 2 (11.8%) | 6 (35.3%) | 6 (35.3%) | - |
| 3 | 8 (47.0%) | 4 (23.5%) | 1 (5.8%) | - |
© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Rybalov, M.; Ananias, H.J.K.; Hoving, H.D.; Van der Poel, H.G.; Rosati, S.; De Jong, I.J. PSMA, EpCAM, VEGF and GRPR as Imaging Targets in Locally Recurrent Prostate Cancer after Radiotherapy. Int. J. Mol. Sci. 2014, 15, 6046-6061. https://doi.org/10.3390/ijms15046046
Rybalov M, Ananias HJK, Hoving HD, Van der Poel HG, Rosati S, De Jong IJ. PSMA, EpCAM, VEGF and GRPR as Imaging Targets in Locally Recurrent Prostate Cancer after Radiotherapy. International Journal of Molecular Sciences. 2014; 15(4):6046-6061. https://doi.org/10.3390/ijms15046046
Chicago/Turabian StyleRybalov, Maxim, Hildo J. K. Ananias, Hilde D. Hoving, Henk G. Van der Poel, Stefano Rosati, and Igle J. De Jong. 2014. "PSMA, EpCAM, VEGF and GRPR as Imaging Targets in Locally Recurrent Prostate Cancer after Radiotherapy" International Journal of Molecular Sciences 15, no. 4: 6046-6061. https://doi.org/10.3390/ijms15046046