Effects of β2-Adrenergic Receptor Gene Polymorphisms on Ritodrine Therapy in Pregnant Women with Preterm Labor: Prospective Follow-Up Study

Abstract
:1. Introduction
2. Results
2.1. Effects of Patient Characteristics on Time to Delivery

{kind=link}
| Characteristic | Number | Time to Delivery Median (95% CI) | p Value |
|---|---|---|---|
| Age | 0.582 | ||
| <35 years | 109 | 772.0 (388.58–1155.42) | |
| ≥35 years | 28 | 491.5 (5.47–977.47) | |
| Gestational age at admission | <0.001 | ||
| <32 weeks | 87 | 1344.0 (1033.17–1654.83) | |
| ≥32 weeks | 50 | 231.0 (112.66–349.35) | |
| Modified Bishop score * | <0.001 | ||
| <3 | 78 | 978.5 (386.48–1570.52) | |
| ≥3 | 29 | 161.0 (32.46–289.54) | |
| Mode of delivery | 0.567 | ||
| Normal delivery | 58 | 614.0 (325.33–902.67) | |
| Cesarean-section | 64 | 539.9 (0.00–1229.55) |
2.2. Effects of Genotypes on Time to Delivery
| Gene Polymorphism | Minor Allele Frequency (%) | Grouped Genotype | Number of Patients | Time to Delivery (h) Median (95% CI) | p Value |
|---|---|---|---|---|---|
| ADRB2 rs1042713 | 49.6% | AA, AG | 101 | 828.0 (472.39–1183.61) | 0.089 |
| (c.46 A>G, Arg16Gly) | GG | 34 | 287.1 (28.35–545.91) | ||
| ADRB2 rs1042714 | 9.7% | CC | 109 | 684.5 (415.17–953.83) | 0.932 |
| (c.79 C>G, Gln27Glu) | CG, GG | 25 | 1030.3 (0.00–2109.88) | ||
| ADRB2 rs1042717 | 39.2% | GG | 48 | 1319.0 (330.50–2307.50) | 0.098 |
| (c.252 G>A, Leu84Leu) | GA, AA | 86 | 566.0 (304.13–827.87) | ||
| ADRB2 rs1042718 | 39.8% | CC | 48 | 1319 (199.56–2438.44) | 0.061 |
| (c.523 C>A, Arg175Arg) | CA, AA | 89 | 539.9 (330.39–749.45) | ||
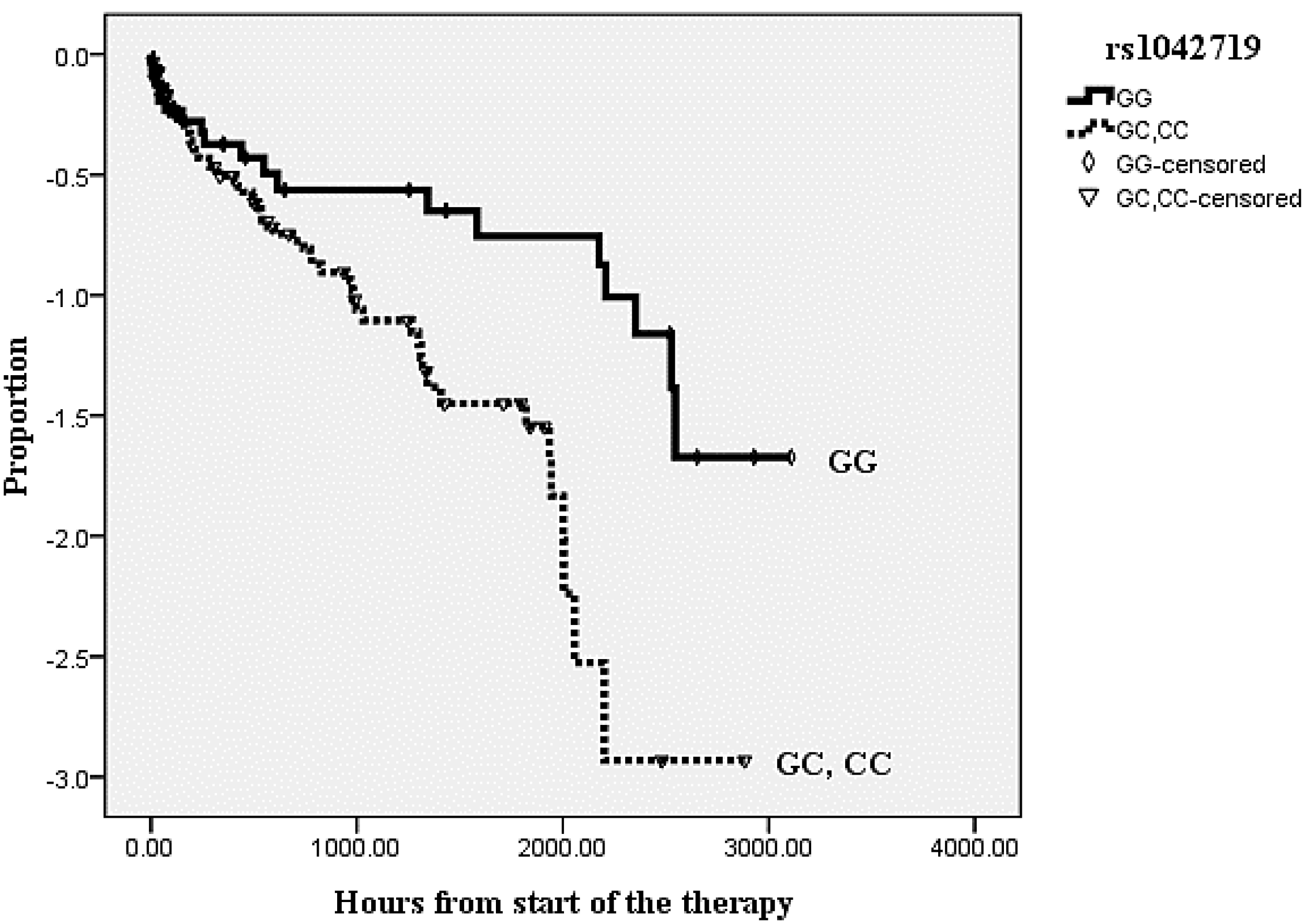
| ADRB2 rs1042719 | 47.4% | GG | 35 | 1584.0 (0.00–3597.95) | 0.019 |
| (c.1053 G>C, Gly351Gly) | GC, CC | 102 | 566.0 (314.53–817.47) |

| Factor | Odds Ratio (95% CI) | p Value |
|---|---|---|
| Age (≥35 years) | 0.51 (0.28–0.93) | 0.027 |
| Modified Bishop score (≥3) | 0.31 (0.18–0.55) | <0.00 |
| Gestational age at admission (≥32 weeks) | 0.25 (0.14–0.46) | <0.00 |
| ADRB2 rs1042719 | 0.36 (0.15–0.85) | 0.020 |
2.3. Effects of Genotypes on Proportions of Patients Who Remained Undelivered
| Gene Polymorphism | Genotype | 24 h | 48 h | 10 day | |||
|---|---|---|---|---|---|---|---|
| Proportion (%) | p Value | Proportion (%) | p Value | Proportion (%) | p Value | ||
| ADRB2 rs1042713 | AA, AG | 54/62 (87.1) | 0.860 | 50/62 (80.6) | 0.693 | 39/62 (62.9) | 0.035 |
| GG | 23/26 (88.5) | 20/26 (76.9) | 10/26 (38.5) | ||||
| ADRB2 rs1042714 | CC | 69/79 (87.3) | 0.359 | 64/79 (81.0) | 0.819 | 42/74 (56.8) | 0.807 |
| CG, GG | 18/19 (94.7) | 15/18 (83.3) | 8/15 (53.3) | ||||
| ADRB2 rs1042717 | GG, GA | 73/83 (88.0) | 0.499 | 65/82 (79.3) | 0.171 | 43/74 (58.1) | 0.295 |
| AA | 15/16 (93.8) | 15/16 (93.8) | 7/16 (43.8) | ||||
| ADRB2 rs1042718 | CC, CA | 74/84 (88.1) | 0.508 | 66/83 (79.5) | 0.177 | 44/75 (58.7) | 0.275 |
| AA | 15/16 (93.8) | 15/16 (93.8) | 7/16 (43.8) | ||||
| ADRB2 rs1042719 | GG, GC | 70/79 (88.6) | 0.808 | 63/78 (80.8) | 0.602 | 42/70 (60.0) | 0.165 |
| CC | 19/21 (90.5) | 18/21 (85.7) | 9/21 (42.9) | ||||
3. Discussion
4. Materials and Methods
4.1. Study Patients
4.2. Drug Administration
4.3. Outcomes and Data Collection
4.4. Genotyping Methods
4.5. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hamilton, B.E.; Hoyert, D.L.; Martin, J.A.; Strobino, D.M.; Guyer, B. Annual summary of vital statistics: 2010–2011. Pediatrics 2013, 131, 548–558. [Google Scholar] [CrossRef]
- Mathews, T.J.; MacDorman, M.F. Infant mortality statistics from the 2003 period linked birth/infant death data set. Natl. Vital Stat. Rep. 2006, 54, 1–29. [Google Scholar]
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar]
- Shim, J.Y.; Park, Y.W.; Yoon, B.H.; Cho, Y.K.; Yang, J.H.; Lee, Y.; Kim, A. Multicentre, parallel group, randomised, single-blind study of the safety and efficacy of atosiban vs. ritodrine in the treatment of acute preterm labour in Korean women. BJOG 2006, 113, 1228–1234. [Google Scholar] [CrossRef]
- The canadian preterm labor investigators group. Treatment of preterm labor with the β-adrenergic agonist ritodrine. N. Engl. J. Med. 1992, 327, 308–312. [Google Scholar] [CrossRef]
- Weinberg, C.R.; Shi, M. The genetics of preterm birth: Using what we know to design better association studies. Am. J. Epidemiol. 2009, 170, 1373–1381. [Google Scholar] [CrossRef]
- Liggett, S.B. Polymorphisms of the β2-adrenergic receptor. N. Engl. J. Med. 2002, 346, 536–538. [Google Scholar] [CrossRef]
- Lanfear, D.E.; Jones, P.G.; Marsh, S.; Cresci, S.; McLeod, H.L.; Spertus, J.A. β2-Adrenergic receptor genotype and survival among patients receiving β-blocker therapy after an acute coronary syndrome. JAMA 2005, 294, 1526–1533. [Google Scholar]
- Lanfear, D.E.; Jones, P.G.; Marsh, S.; Cresci, S.; McLeod, H.L.; Spertus, J.A. β1- and β2-adrenergic receptor gene variation, β-blocker use and risk of myocardial infarction and stroke. Am. J. Hypertens. 2008, 21, 290–296. [Google Scholar] [CrossRef]
- Palmer, C.N.; Lipworth, B.J.; Lee, S.; Ismail, T.; Macgregor, D.F.; Mukhopadhyay, S. Arginine-16 β2 adrenoceptor genotype predisposes to exacerbations in young asthmatics taking regular salmeterol. Thorax 2006, 61, 940–944. [Google Scholar] [CrossRef]
- Basu, K.; Palmer, C.N.; Tavendale, R.; Lipworth, B.J.; Mukhopadhyay, S. Adrenergic β2-receptor genotype predisposes to exacerbations in steroid-treated asthmatic patients taking frequent albuterol or salmeterol. J. Allergy Clin. Immunol. 2009, 124, 1188–1194. [Google Scholar] [CrossRef]
- Martinez, F.D.; Graves, P.E.; Baldini, M.; Solomon, S.; Erickson, R. Association between genetic polymorphisms of the β2-adrenoceptor and response to albuterol in children with and without a history of wheezing. J. Clin. Investig. 1997, 100, 3184–3188. [Google Scholar] [CrossRef]
- Eichelbaum, M.; Ingelman-Sundberg, M.; Evans, W.E. Pharmacogenomics and individualized drug therapy. Annu. Rev. Med. 2006, 57, 119–137. [Google Scholar] [CrossRef]
- Hamada, Y.; Nakaya, Y.; Hamada, S.; Kamada, M.; Aono, T. Activation of K+ channels by ritodrine hydrochloride in uterine smooth muscle cells from pregnant women. Eur. J. Pharmacol. 1994, 288, 45–51. [Google Scholar] [CrossRef]
- Ahles, A.; Engelhardt, S. Polymorphic variants of adrenoceptors: Pharmacology, physiology, and role in disease. Pharmacol. Rev. 2014, 66, 598–637. [Google Scholar] [CrossRef]
- Adams, K.M.; Eschenbach, D.A. The genetic contribution towards preterm delivery. Semin. Fetal Neonatal. Med. 2004, 9, 445–452. [Google Scholar] [CrossRef]
- Crider, K.S.; Whitehead, N.; Buus, R.M. Genetic variation associated with preterm birth: A HuGE review. Genet. Med. 2005, 7, 593–604. [Google Scholar]
- Shin, J.; Johnson, J.A. Pharmacogenetics of β-blockers. Pharmacotherapy 2007, 27, 874–887. [Google Scholar] [CrossRef]
- Landau, R.; Xie, H.; Dishy, V.; Stein, C.M.; Wood, A.J.J.; Emala, C.W.; Smiley, R.M. β2-Adrenergic receptor genotype and preterm delivery. Am. J. Obstet. Gynecol. 2002, 187, 1294–1298. [Google Scholar]
- Ozkur, M.; Dogulu, F.; Ozkur, A.; Gokmen, B.; Inaloz, S.S.; Aynacioglu, A.S. Association of the Gln27Glu polymorphism of the β2-adrenergic receptor with preterm labor. Int. J. Gynaecol. Obstet. 2002, 77, 209–215. [Google Scholar] [CrossRef]
- Landau, R.; Morales, M.A.; Antonarakis, S.E.; Blouin, J.L.; Smiley, R.M. Arg16 homozygosity of the β2-adrenergic receptor improves the outcome after β2-agonist tocolysis for preterm labor. Clin. Pharmacol. Ther. 2005, 78, 656–663. [Google Scholar] [CrossRef]
- Liggett, S.B. β2-Adrenergic receptor pharmacogenetics. Am. J. Respir. Crit. Care Med. 2000, 161, S197–S201. [Google Scholar] [CrossRef]
- Drysdale, C.M.; McGraw, D.W.; Stack, C.B.; Stephens, J.C.; Judson, R.S.; Nandabalan, K.; Arnold, K.; Ruano, G.; Liggett, S.B. Complex promoter and coding region β2-adrenergic receptor haplotypes alter receptor expression and predict in vivo responsiveness. Proc. Natl. Acad. Sci. USA 2000, 97, 10483–10488. [Google Scholar] [CrossRef]
- Park, H.S.; Shin, E.S.; Lee, J.E. Genotypes and haplotypes of β2-adrenergic receptor and parameters of the metabolic syndrome in Korean adolescents. Metabolism 2008, 57, 1064–1070. [Google Scholar] [CrossRef]
- Chu, X.; Dong, Y.; Shen, M.; Sun, L.; Dong, C.; Wang, Y.; Wang, B.; Zhang, K.; Hua, Q.; Xu, S.; et al. Polymorphisms in the ADRB2 gene and graves disease: A case-control study and a meta-analysis of available evidence. BMC Med. Genet. 2009, 10, 26. [Google Scholar]
- Kimchi-Sarfaty, C.; Oh, J.M.; Kim, I.W.; Sauna, Z.E.; Calcagno, A.M.; Ambudkar, S.V.; Gottesman, M.M. A “silent” polymorphism in the MDR1 gene changes substrate specificity. Science 2007, 315, 525–528. [Google Scholar] [CrossRef]
- Zhang, F.; Saha, S.; Shabalina, S.A.; Kashina, A. Differential arginylation of actin isoforms is regulated by coding sequence-dependent degradation. Science 2010, 329, 1534–1537. [Google Scholar] [CrossRef]
- Koukouritaki, S.B.; Poch, M.T.; Cabacungan, E.T.; McCarver, D.G.; Hines, R.N. Discovery of novel flavin-containing monooxygenase 3 (FMO3) single nucleotide polymorphisms and functional analysis of upstream haplotype variants. Mol. Pharmacol. 2005, 68, 383–392. [Google Scholar]
- Michel, M.C.; Pingsmann, A.; Nohlen, M.; Siekmann, U.; Brodde, O. Decresaes myometrial β-adrenoceptors in women receiving β2-adrenergic tocolytic therapy: Correlation with lymphocyte β-adrenoceptors. Clin. Pharmacol. Ther. 1989, 45, 1–8. [Google Scholar] [CrossRef]
- Frambach, T.; Müller, T.; Freund, S.; Engelhardt, S.; Sütterlin, M.; Lohse, M.J.; Dietl, J. Self-limitation of intravenous tocolysis with β2-adrenergic agonists is mediated through receptor G protein uncoupling. J. Clin. Endocrinol. Metab. 2005, 90, 2882–2887. [Google Scholar] [CrossRef]
- Engelhardt, S.; Zieger, W.; Kassubek, J.; Michel, M.C.; Lohse, M.J.; Brodde, O.E. Tocolytic therapy with fenoterol induces selective down-regulation of β-adrenergic receptors in human myometrium. J. Clin. Endocrinol. Metab. 1997, 82, 1235–1242. [Google Scholar]
- Dishy, V.; Sofowora, G.G.; Xie, H.G.; Kim, R.B.; Byrne, D.W.; Stein, C.M.; Wood, A.J. The effect of common polymorphisms of the β2-adrenergic receptor on agonist-mediated vascular desensitization. N. Engl. J. Med. 2001, 345, 1030–1035. [Google Scholar] [CrossRef]
- Bruck, H.; Leineweber, K.; Beilfuss, A.; Weber, M.; Heusch, G.; Philipp, T.; Brodde, O.E. Genotype-dependent time course of lymphocyte β2-adrenergic receptor down-regulation. Clin. Pharmacol. Ther. 2003, 74, 255–263. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Park, J.Y.; Lee, N.R.; Lee, K.E.; Park, S.; Kim, Y.J.; Gwak, H.S. Effects of β2-Adrenergic Receptor Gene Polymorphisms on Ritodrine Therapy in Pregnant Women with Preterm Labor: Prospective Follow-Up Study. Int. J. Mol. Sci. 2014, 15, 12885-12894. https://doi.org/10.3390/ijms150712885
Park JY, Lee NR, Lee KE, Park S, Kim YJ, Gwak HS. Effects of β2-Adrenergic Receptor Gene Polymorphisms on Ritodrine Therapy in Pregnant Women with Preterm Labor: Prospective Follow-Up Study. International Journal of Molecular Sciences. 2014; 15(7):12885-12894. https://doi.org/10.3390/ijms150712885
Chicago/Turabian StylePark, Jin Young, Na Ra Lee, Kyung Eun Lee, Sunny Park, Young Ju Kim, and Hye Sun Gwak. 2014. "Effects of β2-Adrenergic Receptor Gene Polymorphisms on Ritodrine Therapy in Pregnant Women with Preterm Labor: Prospective Follow-Up Study" International Journal of Molecular Sciences 15, no. 7: 12885-12894. https://doi.org/10.3390/ijms150712885