Discrepancies between VEGF −1154 G>A Polymorphism Analysis Performed in Peripheral Blood Samples and FFPE Tissue

 ,
,
Abstract
:1. Introduction
2. Results and Discussion
2.1. Results

{kind=link}
| VEGF Polymorphisms | Peripheral Blood N = 153 | FFPE Tumor Tissue N = 84 |
|---|---|---|
| VEGF −2578 C>A | ||
| C/C | 39 (25.5) | 24 (28.6) |
| C/A | 74 (48.4) | 46 (54.8) |
| A/A | 40 (26.1) | 14 (16.7) |
| VEGF −1498 C>T | ||
| C/C | 38 (24.8) | 17 (20.2) |
| C/T | 76 (49.7) | 41 (48.8) |
| T/T | 39 (25.5) | 26 (31) |
| VEGF −1154 G>A | ||
| G/G | 72 (47) | 42 (50) * |
| G/A | 59 (38.6) | 20 (23.8) * |
| A/A | 22 (14.4) | 22 (26.2) * |
| VEGF −634 C>G | ||
| G/G | 71 (46.4) | 30 (35.7) |
| G/C | 58 (37.9) | 43 (51.2) |
| C/C | 24 (15.7) | 11 (13.1) |
| VEGF +936 C>T | ||
| C/C | 108 (70.6) | 65 (77.4) |
| C/T | 42 (27.4) | 17 (20.2) |
| T/T | 3 (2) | 1 (1.2) |
| n.e. | - | 1 |
| eNOS −786 T>C | ||
| T/T | 59 (38.6) | 21 (25) |
| T/C | 77 (50.3) | 40 (47.6) |
| C/C | 17 (11.1) | 22 (26.2) |
| n.e. | - | 1 |
| eNOS +894 G>T | ||
| G/G | 69 (45.1) | 35 (41.7) |
| G/T | 63 (41.2) | 39 46.4) |
| T/T | 21 (13.7) | 10 (11.9) |
| eNOS VNTR 4a/b | ||
| 4b/b | 111 (72.5) | 51 (60.7) |
| 4a/b | 42 (27.5) | 26 (30.9) |
| 4a/a | 0 | 3 (3.6) |
| n.e. | - | 4 |
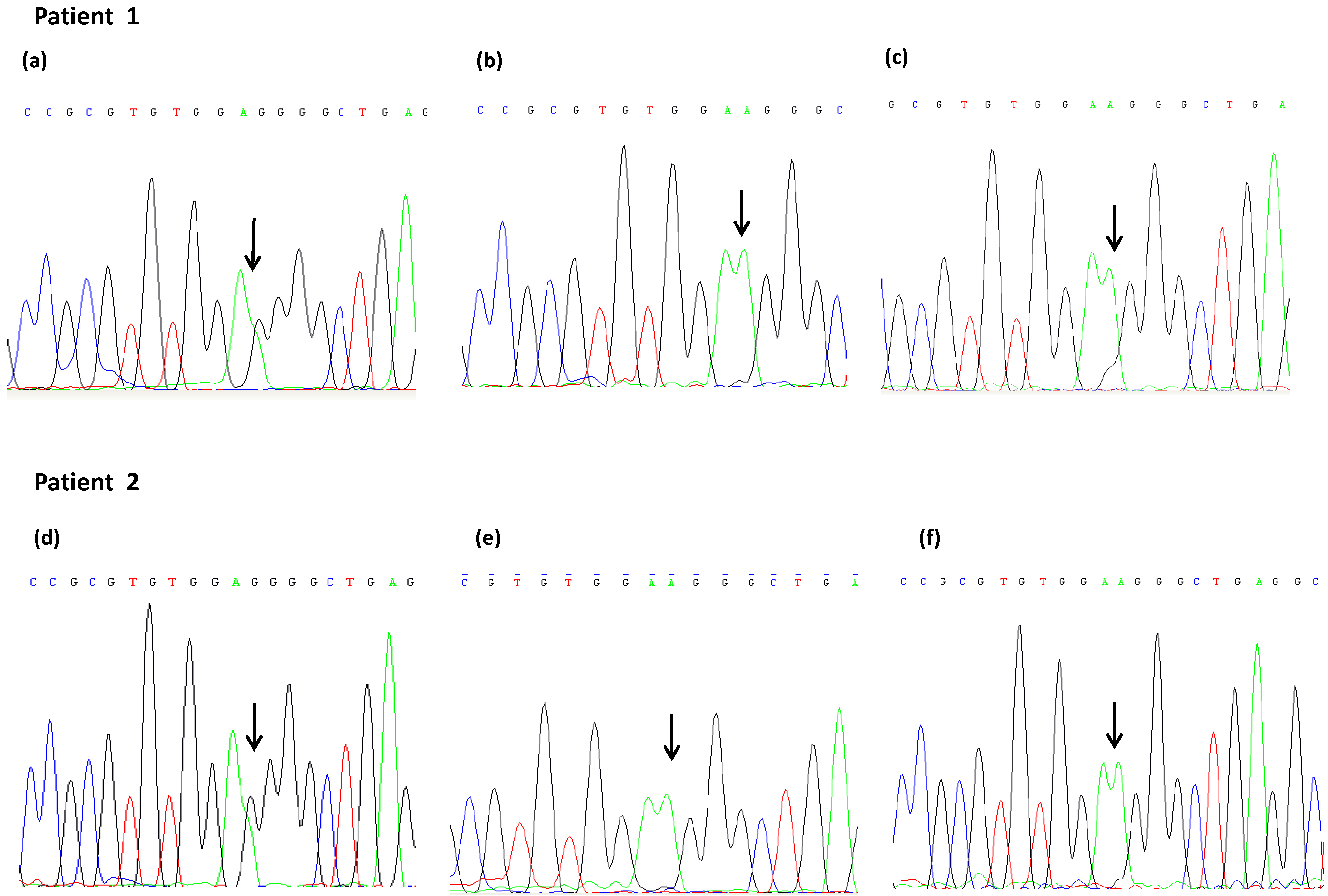
| Samples | VEGF −1154 Peripheral Blood | VEGF −1154 Tumor FFPE Tissue | VEGF −1154 Healthy FFPE Tissue |
|---|---|---|---|
| 1 | G/A | G/A * | G/A * |
| 2 | G/A | A/A | G/A * |
| 3 | G/A | G/A * | A/A |
| 4 | G/A | A/A | A/A |
| 5 | G/A | A/A | G/A * |
| 6 | G/A | A/A | A/A |
| 7 | G/A | G/A * | G/A * |
| 8 | G/A | A/A | n.a. |
| 9 | G/A | G/A * | n.a. |

2.2. Discussion
3. Experimental Section
3.1. Samples and DNA Isolation
3.2. Genotyping
| SNPs | Location | RS-Number | Primers | Annealing Temperature | Product Size |
|---|---|---|---|---|---|
| VEGF −2578C>A | Promoter | rs699947 | F: 5'-AAC-CTA-GCA-CCT-CCA-CCA-AA-3' | 60 °C | 268 bp |
| R: 5'-GCT-GGT-TTC-TGA-CCT-GGC-TA-3' | |||||
| VEGF −1498C>T | Promoter | rs833061 | F: 5'-AAG-CCC-ATT-CCC-TCT-TTA-GC-3' | 60 °C | 303 bp |
| R: 5'-CTG-AGA-GCC-GTT-CCC-TCT-TT-3' | |||||
| VEGF −1498C>T nested * | F: 5'-ACA-GGG-AAG-CTG-GGT-GAA-T-3' | 58 °C | 235 bp | ||
| R: 5'-CTG-AGA-GCC-GTT-CCC-TCT-TT-3' | |||||
| VEGF −1154G>A | Promoter | rs1570360 | F: 5'-TTT-TCA-GGC-TGT-GAA-CCT-TG-3' | 62 °C | 264 bp |
| R: 5'-ACG-ACC-TCC-GAG-CTA-CCC-3' | |||||
| VEGF −1154G>A nested * | F: 5'-TTT-TCA-GGC-TGT-GAA-CCT-TG-3' | 60 °C | 227 bp | ||
| R: 5'-GAT-CCT-CCC-CGC-TAC-CAG-3' | |||||
| VEGF −634C>G | 5'UTR | rs2010963 | F: 5'-GGA-TTT-TGG-AAA-CCA-GCA-GA-3' | 62 °C | 224 bp |
| R: 5'-CTG-TCT-GTC-TGT-CCG-TCA-GC-3' | |||||
| VEGF +936C>T | 3'UTR | rs3025039 | F: 5'-ACA-CCA-TCA-CCA-TCG-ACA-GA-3' | 58 °C | 226 bp |
| R: 5'-CAG-GAA-TCC-CAG-AAA-TAA-AAC-TC-3' | |||||
| eNOS +894G>T | Exon 7 | rs1799983 | F: 5'-AAG-GCA-GGA-GAC-AGT-GGA-TG-3' | 64 °C | 319 bp |
| R: 5'-GTT-GGG-GTG-TGG-GAT-CAG-3' | |||||
| eNOS VNTR 27bp | Intron 4 | - | F: 5'-AAA-CTG-TGG-GGG-AGA-TCC-TT-3' | 62 °C | 544 bp |
| R: 5'-GGG-CAG-CTT-GCT-TCT-CTT-AG-3' |
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kim, J.C.; Ha, Y.J.; Roh, S.A.; Choi, E.Y.; Yoon, Y.S.; Kim, K.P.; Hong, Y.S.; Kim, T.W.; Cho, D.H.; Kim, S.Y.; et al. Feasibility of proposedsingle-nucleotidepolymorphisms aspredictivemarkersfor targeted regimens in metastatic colorectal cancer. Br. J. Cancer 2013, 108, 1862–1869. [Google Scholar] [CrossRef]
- Schneider, B.P.; Shen, F.; Miller, K.D. Pharmacogenetic biomarkers for the prediction ofresponseto antiangiogenic treatment. Lancet Oncol. 2012, 13, e427–e436. [Google Scholar] [CrossRef]
- McWhinney, S.R.; McLeod, H.L. Using germline genotype in cancer pharmacogenetic studies. Pharmacogenomics 2009, 10, 489–493. [Google Scholar] [CrossRef]
- Coura, R.; Prolla, J.C.; Meurer, L.; Ashton-Prolla, P. An alternative protocol for DNA extraction from formalin fixed and paraffin wax embedded tissue. J. Clin. Pathol. 2005, 58, 894–895. [Google Scholar] [CrossRef]
- Okello, J.B.; Zurek, J.; Devault, A.M.; Kuch, M.; Okwi, A.L.; Sewankambo, N.K.; Bimenya, G.S.; Poinar, D.; Poinar, H.N. Comparison of methods in the recovery of nucleic acids from archival formalin-fixed paraffin-embedded autopsy tissues. Anal. Biochem. 2010, 400, 110–117. [Google Scholar]
- Chalkley, R.; Hunter, C. Histone-histone propinquity by aldehyde fixation of chromatin. Proc. Natl. Acad. Sci. USA 1975, 72, 1304–1308. [Google Scholar] [CrossRef]
- Feldman, M.Y. Reaction of nucleic acids and nucleoproteins with formaldehyde. Prog. Nucleic Acid. Res. Mol. Biol. 1973, 13, 1–49. [Google Scholar] [CrossRef]
- Lehmann, U.; Kreipe, H. Real-time PCR analysis of DNA and RNA extracted from formalin-fixed and paraffin-embedded biopsies. Methods 2001, 25, 409–418. [Google Scholar] [CrossRef]
- William, C.; Ponten, F.; Moberg, C.; Soderkvist, P.; Uhlen, M.; Ponten, J.; Sitbon, G.; Lundeberg, J. A high frequency of sequence alteration is due to formalin fixation of archival specimens. Am. J. Pathol. 1999, 155, 1467–1471. [Google Scholar] [CrossRef]
- Rae, J.M.; Cordero, K.E.; Scheys, J.O.; Lippman, M.E.; Flockhart, D.A.; Johnson, M.D. Genotyping for polymorphism drug metabolizing enzymes from paraffin-embedded and immunohistochemically stained tumor samples. Pharmacogenetics 2003, 13, 501–507. [Google Scholar] [CrossRef]
- Xie, B.; Freudenheim, J.L.; Cumming, S.S.; Singh, B.; He, H.; McCann, S.E.; Moysich, K.B.; Shields, P.G. Accurate genotyping from paraffin-embedded normal tissue adjacent to breast cancer. Carcinogenesis 2006, 27, 307–310. [Google Scholar] [CrossRef]
- Hagleitner, M.M.; Coenen, M.J.; Jeuken, J.W.; Flucke, U.; Schreuder, H.W.; te Loo, D.M.; Hoogerbrugge, P.M. Taqman genotyping assays can be used on decalcified and paraffin-embedded tissue from patients with osteosarcoma. Pediatr. Blood Cancer 2011, 56, 35–38. [Google Scholar] [CrossRef]
- Wakatsuki, T.; LaBonte, M.J.; Bohanes, P.O.; Zhang, W.; Yang, D.; Azuma, M.; Barzi, A.; Ning, Y.; Loupakis, F.; Saadat, S.; et al. Prognostic role of lemur tyrosine kinase-3 germline polymorphisms in adjuvant gastric cancer in Japan and the United States. Mol. Cancer Ther. 2013, 12, 2261–2272. [Google Scholar] [CrossRef]
- Rae, J.M.; Regan, M.M.; Thibert, J.N.; Gersch, C.; Thomas, D.; Leyland-Jones, B.; Viale, G.; Pusztai, L.; Hayes, D.F.; Skaar, T.; et al. Concordance between CYP2D6 genotypes obtained from tumor-derived and germline DNA. J. Natl. Cancer Inst. 2013, 105, 1332–1334. [Google Scholar] [CrossRef]
- Van Huis-Tanja, L.; Kweekel, D.; Gelderblom, H.; Koopman, M.; Punt, K.; Guchelaar, H.J.; van der Straaten, T. Concordance of genotype for polymorphism in DNA isolated from peripheral blood and colorectal cancer tumor samples. Pharmacogenomics 2013, 14, 2005–2012. [Google Scholar] [CrossRef]
- Baak-Pablo, R.; Dezentje, V.; Guchelaar, H.J.; van der Straaten, T. Genotyping of DNA samples isolated from formalin-fixed paraffin-embedded tissues using preamplification. J. Mol. Diagn. 2010, 12, 746–749. [Google Scholar] [CrossRef]
- Koutras, A.K.; Antonacopoulou, A.G.; Eleftheraki, A.G.; Dimitrakopoulos, F.I.; Koumarianou, A.; Varthalitis, I.; Fostira, F.; Sgouros, J.; Briasoulis, E.; Bournakis, E.; et al. Vascular endothelial growth factor polymorphisms and clinical outcome in colorectal cancer patients treated with irinotecan-based chemotherapy and bevacizumab. Pharmacogenomics J. 2012, 12, 468–475. [Google Scholar] [CrossRef]
- Hansen, T.F.; Christensen, R.D.; Andersen, R.F.; Spindler, K.L.G.; Johnsson, A.; Jakobsen, A. The predictive value of single nucleotide polymorphisms in the VEGF system to the efficacy of first-line treatment with bevacizumab plus chemiotherapy in patients with metastatic colorectal cancer. Int. J. Colorectal Dis. 2011, 27, 715–720. [Google Scholar]
- Jin, Q.; Hemminki, K.; Enquist, K.; Lenner, P.; Grzybowska, E.; Klaes, R.; Henriksson, R.; Chen, B.; Pamula, J.; Pekala, W.; et al. Vascular endothelial growth factor polymorphisms in relation to breast cancer development and prognosis. Clin. Cancer Res. 2005, 11, 3647–3653. [Google Scholar] [CrossRef]
- Jacobs, E.J.; Feigelson, H.S.; Bain, E.B.; Brady, K.A.; Rodriguez, C.; Stevens, V.L.; Patel, A.V.; Thun, M.J.; Calle, E.E. Polymorphisms in the vascular endothelial growth factor gene and breast cancer in the Cancer Prevention Study II cohort. Breast Cancer Res. 2006, 8. [Google Scholar] [CrossRef]
- Dassoulas, K.; Gazouli, M.; Rizos, S.; Theodoropoulos, G.; Christoni, Z.; Nikiteas, N.; Karakitsos, P. Common polymorphisms in the vascular endothelial growth factor gene and colorectal cancer development, prognosis, and survival. Mol. Carcinog. 2009, 48, 563–569. [Google Scholar] [CrossRef]
- Gilbert, M.T.; Haselkorn, T.; Bunce, M.; Sanchez, J.J.; Lucas, S.B.; Jewell, L.D.; van Marck, E.; Worobey, M. The isolation of nucleic acid from fixed, paraffin-embedded tissues-which methods are useful when? PLoS One 2007, 2, e537. [Google Scholar] [CrossRef]
- Lasko, D.; Cavenee, W.; Nordenskjöld, M. Loss of constitutional heterozygosity in human cancer. Annu. Rev. Genet. 1991, 25, 281–314. [Google Scholar]
- Regan, M.M.; Leyland-Jones, B.; Bouzyk, M.; Pagani, O.; Tang, W.; Kammler, R.; dell’Orto, P.; Biasi, M.O.; Thürlimann, B.; Lyng, M.B.; et al. CYP2D6genotype and tamoxifen response in postmenopausal women with endocrine-responsive breast cancer: The breast international group 1–98 trial. J. Natl. Cancer Inst. 2012, 104, 441–451. [Google Scholar] [CrossRef]
- Huijsmans, C.J.; Damen, J.; van der Linden, J.C.; Savelkoul, P.H.; Hermans, M.H. Comparative analysis of four methods to extract DNA from paraffin-embedded tissues: Effect on downstream molecular applications. BMC Res. Notes 2010, 3. [Google Scholar] [CrossRef]
- Nakamura, Y.; Ratain, M.J.; Cox, N.J.; McLeod, H.L.; Kroetz, D.L.; Flockhart, D.A. Re: CYP2D6 genotype and tamoxifen response in postmenopausal women with endocrine-responsive breast cancer: The Breast International Group 1–98 trial. J. Natl. Cancer Inst 2012, 104. [Google Scholar] [CrossRef]
- Passardi, A.; Nanni, O.; Tassinari, D.; Turci, D.; Cavanna, L.; Fontana, A.; Ruscelli, S.; Mucciarini, C.; Lorusso, V.; Ragazzini, A.; et al. Effectiveness of bevacizumab added to gold standard chemotherapy in metastatic colorectal cancer: Final results for first-line treatment from the ITACA randomized clinical trial. J. Clin. Oncol. 2014, in press. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Marisi, G.; Passardi, A.; Calistri, D.; Zoli, W.; Amadori, D.; Ulivi, P. Discrepancies between VEGF −1154 G>A Polymorphism Analysis Performed in Peripheral Blood Samples and FFPE Tissue. Int. J. Mol. Sci. 2014, 15, 13333-13343. https://doi.org/10.3390/ijms150813333
Marisi G, Passardi A, Calistri D, Zoli W, Amadori D, Ulivi P. Discrepancies between VEGF −1154 G>A Polymorphism Analysis Performed in Peripheral Blood Samples and FFPE Tissue. International Journal of Molecular Sciences. 2014; 15(8):13333-13343. https://doi.org/10.3390/ijms150813333
Chicago/Turabian StyleMarisi, Giorgia, Alessandro Passardi, Daniele Calistri, Wainer Zoli, Dino Amadori, and Paola Ulivi. 2014. "Discrepancies between VEGF −1154 G>A Polymorphism Analysis Performed in Peripheral Blood Samples and FFPE Tissue" International Journal of Molecular Sciences 15, no. 8: 13333-13343. https://doi.org/10.3390/ijms150813333