Brain Metastases in Gastrointestinal Cancers: Is there a Role for Surgery?

Abstract
:1. Introduction

{kind=link}
| Cancer | New Cases per Year [8] | Incidence BM |
|---|---|---|
| Esophageal | 482,000 | 1.4%–3.9% |
| Gastric | 989,000 | 0.2%–0.7% |
| Pancreatic | 277,000 | 0.3% |
| Colorectal | 1,233,000 | 0.6%–4.0% |
2. Brain Metastases of Gastrointestinal Cancers
2.1. Esophageal Cancer
| Inc | n | Age (Years) | Male | ECM | BM > 1 | Resection | OS (Months) | OS Resection (Months) | Reference |
|---|---|---|---|---|---|---|---|---|---|
| 1.4% | 36 | 62 | 92% | 53% | 53% | 33% | 3.9 | 9.6 | [22] |
| 1.7% | 27 | 62 | 100% | 70% | 52% | 37% | 3.8 | 3.8–9.6 | [25] |
| 3.4% | 29 | n/a | n/a | 44% | 52% | 21% | 3.5 | improved | [23] |
| 2.1% | 17 | 58 | n/a | 76% | 35% | 59% | n/a | improved | [26] |
| 2.7% | 12 | 64 | 92% | 75% | 67% | 17% | 2.1 | 1.2–7.0 | [27] |
| 3.9% | 20 | n/a | n/a | 45% | 40% | 60% | 10.5 | n/a | [24] |
| 1.6% | 26 | 62 | 96% | 69% | 54% | 19% | 4.2 | 7.0 | [21] |
2.2. Gastric Cancer
| Inc | n | Age (Years) | Male | ECM | BM > 1 | Resection | OS (Months) | OS Resection (Months) | Reference |
|---|---|---|---|---|---|---|---|---|---|
| 0.7% | 24 | 53 | 75% | 88% | 55% | 21% | 2.4 | 12.5 | [33] |
| 0.2% | 11 | 44 | 54% | n/a | n/a | 0% | 1.4–2.2 | n/a | [34] |
| 0.5% | 11 | 55 | 82% | 20% | 55% | 27% | 2.7 | 6 | [35] |
| n/a | 11 | 61 | 64% | 82% | 45% | 18% | 27.7 | 45.5 | [36] |
| n/a | 56 | 56 | 79% | 91% | 55% | n/a | 2.1–9.3 | n/a | [37] |
2.3. Pancreatic Cancer
| Inc | n | Age (Years) | Male | ECM | BM > 1 | Resection | OS (Months) | OS Resection (Months) | Reference |
|---|---|---|---|---|---|---|---|---|---|
| 0.3% | 4 | 51.5 | 100% | 100% | 50% | 0% | 2.9 | n/a | [43] |
| Inc | n | Age (Years) | Male | ECM | BM > 1 | Resection | OS (Months) | OS Resection (Months) | Reference |
|---|---|---|---|---|---|---|---|---|---|
| n/a | 73 | 62 | 41% | n/a | 11% | 100% | 8.3 | 8.3 | [46] |
| 1.6% | 17 | 59 | 76% | 88% | n/a | 6% | 4.5 | n/a | [47] |
| n/a | 32 | 62 | 66% | n/a | 28% | 88% | 7.5 | 10.6 | [48] |
| n/a | 49 | 66 | 67% | 82% | 53% | 31% | 5.1 | 5.2 | [49] |
| n/a | 30 | 66 | 60% | 87% | 27% | 100% * | n/a | 5.5 | [50] |
| 2.3 | 39 | 59 | 54% | 97% | n/a | 41% | n/a | improved | [51] |
| n/a | 35 | 59–65 | n/a | 56%–78% | 44%–56% | 12%–22% | 3.0–5.0 | 9.0 | [52] |
| 0.6% | 27 | 66 | 52% | 93% | 56% | 26% | 2.4 | n/a | [53] |
| 1.4% | 126 | 62 | 62% | 91% | 60% | 16% | 5.4 | 11.5 | [54] |
| n/a | 118 | 54 | 53% | 90% | 50% | 20% | 4.1 | 7.2 | [55] |
| 0.7 | 60 | 63 | 60% | 88% | 65% | 13% | 8.0 | n/a | [56] |
| n/a | 78 | n/a | 39% | 64% | n/a | 25% | 8.0 | 14.0 | [57] |
| 4.0% | 52 | 61 | 56% | 90% | 27% | 12% | 3.2 | 13.2 | [58] |
| 1.3% | 29 | 58 | 79% | 79% | 69% | 59% | 6.4 | 8.8 | [59] |
| n/a | 39 | 59 | 59% | 97% | 38% | 15% | 5.0 | 15.2 | [60] |
| n/a | 48 | 63 | 52% | 90% | 70% | 38% | 4.0 | 3.0–13.0 | [61] * |
| 1.1% | 47 | n/a | n/a | n/a | n/a | 23% | 6.6 | 16.2 | [62] |
| n/a | 28 | 62 | 46% | 53% | 18% | 100% * | n/a | 12.0 | [63] |
| 2.7% | 113 | n/a | 65% | 78% | 44% | 56% | 5.4 | 15.2 | [64] |
| n/a | 41 | 58 | 61% | 95% | 41% | 29% | 5.0 | 21.4 | [65] |
2.4. Colorectal Cancer

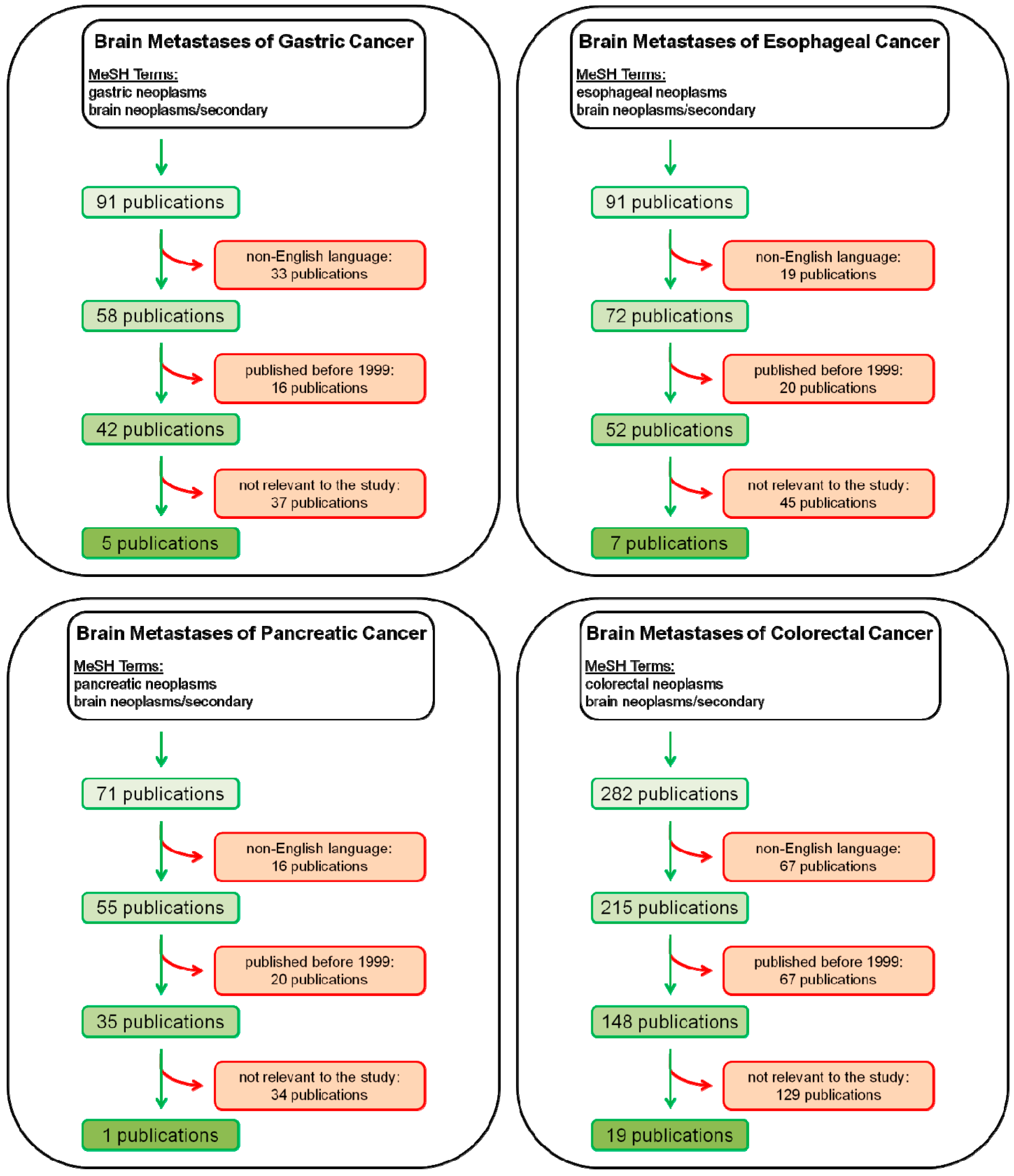
3. Materials and Methods
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2010, 61, 69–90. [Google Scholar]
- Wan, L.; Pantel, K.; Kang, Y. Tumor metastasis: Moving new biological insights into the clinic. Nat. Med. 2013, 19, 1450–1464. [Google Scholar]
- Gavrilovic, I.T.; Posner, J.B. Brain metastases: Epidemiology and pathophysiology. J. Neuro-Oncol. 2005, 75, 5–14. [Google Scholar]
- Barnholtz-Sloan, J.S.; Sloan, A.E.; Davis, F.G.; Vigneau, F.D.; Lai, P.; Sawaya, R.E. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J. Clin. Oncol. 2004, 22, 2865–2872. [Google Scholar]
- Nayak, L.; Lee, E.Q.; Wen, P.Y. Epidemiology of brain metastases. Curr. Oncol. Rep. 2012, 14, 48–54. [Google Scholar]
- Lu-Emerson, C.; Eichler, A.F. Brain metastases. Continuum (Minneap. Minn) 2012, 18, 295–311. [Google Scholar]
- Patel, T.R.; Knisely, J.P.; Chiang, V.L. Management of brain metastases: Surgery, radiation, or both? Hemato. Oncol. Clin. N. Am. 2012, 26, 933–947. [Google Scholar]
- Ferlay, J.; Shin, H.R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer J. Int. Du Cancer 2010, 127, 2893–2917. [Google Scholar]
- Lagerwaard, F.J.; Levendag, P.C.; Nowak, P.J.; Eijkenboom, W.M.; Hanssens, P.E.; Schmitz, P.I. Identification of prognostic factors in patients with brain metastases: A review of 1292 patients. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 795–803. [Google Scholar]
- Patchell, R.A.; Tibbs, P.A.; Walsh, J.W.; Dempsey, R.J.; Maruyama, Y.; Kryscio, R.J.; Markesbery, W.R.; Macdonald, J.S.; Young, B. A randomized trial of surgery in the treatment of single metastases to the brain. N. Engl. J. Med. 1990, 322, 494–500. [Google Scholar]
- Owonikoko, T.K.; Arbiser, J.; Zelnak, A.; Shu, H.K.; Shim, H.; Robin, A.M.; Kalkanis, S.N.; Whitsett, T.G.; Salhia, B.; Tran, N.L.; et al. Current approaches to the treatment of metastatic brain tumours. Nat. Rev. Clin. Oncol. 2014, 11, 203–222. [Google Scholar]
- Eichler, A.F.; Loeffler, J.S. Multidisciplinary management of brain metastases. Oncologist 2007, 12, 884–898. [Google Scholar]
- Stelzer, K.J. Epidemiology and prognosis of brain metastases. Surg. Neurol. Int. 2012, 4, S192–S202. [Google Scholar]
- Barnholtz-Sloan, J.S.; Yu, C.; Sloan, A.E.; Vengoechea, J.; Wang, M.; Dignam, J.J.; Vogelbaum, M.A.; Sperduto, P.W.; Mehta, M.P.; Machtay, M.; et al. A nomogram for individualized estimation of survival among patients with brain metastasis. Neuro Oncol. 2012, 14, 910–918. [Google Scholar]
- Lagergren, J.; Lagergren, P. Oesophageal cancer. BMJ 2010, 341, c6280. [Google Scholar] [CrossRef]
- Zhang, Y. Epidemiology of esophageal cancer. World J. Gastroenterol. 2013, 19, 5598–5606. [Google Scholar]
- Enzinger, P.C.; Mayer, R.J. Esophageal cancer. N. Engl. J. Med. 2003, 349, 2241–2252. [Google Scholar]
- Sundelof, M.; Ye, W.; Dickman, P.W.; Lagergren, J. Improved survival in both histologic types of oesophageal cancer in Sweden. Int. J. Cancer J. Int. Du Cancer 2002, 99, 751–754. [Google Scholar]
- Rouvelas, I.; Zeng, W.; Lindblad, M.; Viklund, P.; Ye, W.; Lagergren, J. Survival after surgery for oesophageal cancer: A population-based study. Lancet Oncol. 2005, 6, 864–870. [Google Scholar]
- Quint, L.E.; Hepburn, L.M.; Francis, I.R.; Whyte, R.I.; Orringer, M.B. Incidence and distribution of distant metastases from newly diagnosed esophageal carcinoma. Cancer 1995, 76, 1120–1125. [Google Scholar]
- Song, Z.; Lin, B.; Shao, L.; Zhang, Y. Brain metastases from esophageal cancer: Clinical review of 26 cases. World Neurosurg. 2014, 81, 131–135. [Google Scholar]
- Ogawa, K.; Toita, T.; Sueyama, H.; Fuwa, N.; Kakinohana, Y.; Kamata, M.; Adachi, G.; Saito, A.; Yoshii, Y.; Murayama, S. Brain metastases from esophageal carcinoma: Natural history, prognostic factors, and outcome. Cancer 2002, 94, 759–764. [Google Scholar]
- Rice, T.W.; Khuntia, D.; Rybicki, L.A.; Adelstein, D.J.; Vogelbaum, M.A.; Mason, D.P.; Murthy, S.C.; Blackstone, E.H. Brain metastases from esophageal cancer: A phenomenon of adjuvant therapy? Ann. Thorac. Surg. 2006, 82, 2042–2049. [Google Scholar]
- Wadhwa, R.; Taketa, T.; Correa, A.M.; Sudo, K.; Campagna, M.C.; Blum, M.A.; Komaki, R.; Skinner, H.; Lee, J.H.; Bhutani, M.S.; et al. Incidence of brain metastases after trimodality therapy in patients with esophageal or gastroesophageal cancer: Implications for screening and surveillance. Oncology 2013, 85, 204–207. [Google Scholar]
- Weinberg, J.S.; Suki, D.; Hanbali, F.; Cohen, Z.R.; Lenzi, R.; Sawaya, R. Metastasis of esophageal carcinoma to the brain. Cancer 2003, 98, 1925–1933. [Google Scholar]
- Yoshida, S. Brain metastasis in patients with esophageal carcinoma. Surg. Neurol. 2007, 67, 288–290. [Google Scholar]
- Kanemoto, A.; Hashimoto, T.; Harada, H.; Asakura, H.; Ogawa, H.; Furutani, K.; Boku, N.; Nakasu, Y.; Nishimura, T. Occurrence and clinical features of brain metastasis after chemoradiotherapy for esophageal carcinoma. J. Radiat. Res. 2011, 52, 509–515. [Google Scholar]
- Nagini, S. Carcinoma of the stomach: A review of epidemiology, pathogenesis, molecular genetics and chemoprevention. World J. Gastrointest. Oncol. 2012, 4, 156–169. [Google Scholar]
- Cammerer, G.; Formentini, A.; Karletshofer, M.; Henne-Bruns, D.; Kornmann, M. Evaluation of important prognostic clinical and pathological factors in gastric cancer. Anticancer Res. 2012, 32, 1839–1842. [Google Scholar]
- Orditura, M.; Galizia, G.; Sforza, V.; Gambardella, V.; Fabozzi, A.; Laterza, M.M.; Andreozzi, F.; Ventriglia, J.; Savastano, B.; Mabilia, A.; et al. Treatment of gastric cancer. World J. Gastroenterol. 2014, 20, 1635–1649. [Google Scholar]
- Dicken, B.J.; Bigam, D.L.; Cass, C.; Mackey, J.R.; Joy, A.A.; Hamilton, S.M. Gastric adenocarcinoma: Review and considerations for future directions. Ann. Surg. 2005, 241, 27–39. [Google Scholar]
- Yang, D.; Hendifar, A.; Lenz, C.; Togawa, K.; Lenz, F.; Lurje, G.; Pohl, A.; Winder, T.; Ning, Y.; Groshen, S.; et al. Survival of metastatic gastric cancer: Significance of age, sex and race/ethnicity. J. Gastrointest. Oncol. 2011, 2, 77–84. [Google Scholar]
- York, J.E.; Stringer, J.; Ajani, J.A.; Wildrick, D.M.; Gokaslan, Z.L. Gastric cancer and metastasis to the brain. Ann. Surg. Oncol. 1999, 6, 771–776. [Google Scholar]
- Kim, M. Intracranial involvement by metastatic advanced gastric carcinoma. J. Neuro-Oncol. 1999, 43, 59–62. [Google Scholar]
- Kasakura, Y.; Fujii, M.; Mochizuki, F.; Suzuki, T.; Takahashi, T. Clinicopathological study of brain metastasis in gastric cancer patients. Surg. Today 2000, 30, 485–490. [Google Scholar]
- Han, J.H.; Kim, D.G.; Chung, H.T.; Kim, C.Y.; Park, C.K.; Chung, Y.S.; Paek, S.H.; Yoo, M.W.; Kim, B.H.; Jung, H.W. Radiosurgery for brain metastasis from advanced gastric cancer. Acta Neurochir. 2010, 152, 605–610. [Google Scholar]
- Park, Y.S.; Chang, J.H.; Chang, J.W.; Park, Y.G. The efficacy of gamma knife radiosurgery for advanced gastric cancer with brain metastases. J. Neuro-Oncol. 2011, 103, 513–521. [Google Scholar]
- Lemke, J.; Schafer, D.; Sander, S.; Henne-Bruns, D.; Kornmann, M. Survival and prognostic factors in pancreatic and ampullary cancer. Anticancer Res. 2014, 34, 3011–3020. [Google Scholar]
- Hidalgo, M. Pancreatic cancer. N. Engl. J. Med. 2010, 362, 1605–1617. [Google Scholar]
- Wolfgang, C.L.; Herman, J.M.; Laheru, D.A.; Klein, A.P.; Erdek, M.A.; Fishman, E.K.; Hruban, R.H. Recent progress in pancreatic cancer. CA Cancer J. Clin. 2013, 63, 318–348. [Google Scholar]
- Burris, H.A., III; Moore, M.J.; Andersen, J.; Green, M.R.; Rothenberg, M.L.; Modiano, M.R.; Cripps, M.C.; Portenoy, R.K.; Storniolo, A.M.; Tarassoff, P.; et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: A randomized trial. J. Clin. Oncol. 1997, 15, 2403–2413. [Google Scholar]
- Yachida, S.; Iacobuzio-Donahue, C.A. The pathology and genetics of metastatic pancreatic cancer. Arch. Pathol. Lab. Med. 2009, 133, 413–422. [Google Scholar]
- Park, K.S.; Kim, M.; Park, S.H.; Lee, K.W. Nervous system involvement by pancreatic cancer. J. Neuro-Oncol. 2003, 63, 313–316. [Google Scholar]
- Lemke, J.; Scheele, J.; Kapapa, T.; Wirtz, C.R.; Henne-Bruns, D.; Kornmann, M. Brain metastasis in pancreatic cancer. Int. J. Mol. Sci. 2013, 14, 4163–4173. [Google Scholar]
- Lemke, J.; Barth, T.F.; Juchems, M.; Kapapa, T.; Henne-Bruns, D.; Kornmann, M. Long-term survival following resection of brain metastases from pancreatic cancer. Anticancer Res. 2011, 31, 4599–4603. [Google Scholar]
- Wronski, M.; Arbit, E. Resection of brain metastases from colorectal carcinoma in 73 patients. Cancer 1999, 85, 1677–1685. [Google Scholar]
- Onodera, H.; Nagayama, S.; Tachibana, T.; Fujimoto, A.; Imamura, M. Brain metastasis from colorectal cancer. Int. J. Colorectal Dis. 2005, 20, 57–61. [Google Scholar]
- Fowler, A.; Cook, R.; Biggs, M.; Little, N.; Assaad, N.; McDonald, K. Survival of patients following neurosurgical treatment of colorectal adenocarcinoma metastasis in the Northern Sydney-Central Coast area. J. Clin. Neurosci. 2008, 15, 998–1004. [Google Scholar]
- Kruser, T.J.; Chao, S.T.; Elson, P.; Barnett, G.H.; Vogelbaum, M.A.; Angelov, L.; Weil, R.J.; Pelley, R.; Suh, J.H. Multidisciplinary management of colorectal brain metastases: A retrospective study. Cancer 2008, 113, 158–165. [Google Scholar]
- Aprile, G.; Zanon, E.; Tuniz, F.; Iaiza, E.; de Pauli, F.; Pella, N.; Pizzolitto, S.; Buffoli, A.; Piga, A.; Skrap, M.; et al. Neurosurgical management and postoperative whole-brain radiotherapy for colorectal cancer patients with symptomatic brain metastases. J. Cancer Res. Clin. Oncol. 2009, 135, 451–457. [Google Scholar]
- Mongan, J.P.; Fadul, C.E.; Cole, B.F.; Zaki, B.I.; Suriawinata, A.A.; Ripple, G.H.; Tosteson, T.D.; Pipas, J.M. Brain metastases from colorectal cancer: Risk factors, incidence, and the possible role of chemokines. Clin. Colorectal Cancer 2009, 8, 100–105. [Google Scholar]
- Nieder, C.; Pawinski, A.; Balteskard, L. Colorectal cancer metastatic to the brain: Time trends in presentation and outcome. Oncology 2009, 76, 369–374. [Google Scholar]
- Tan, W.S.; Ho, K.S.; Eu, K.W. Brain metastases in colorectal cancers. World J. Surg. 2009, 33, 817–821. [Google Scholar]
- Jung, M.; Ahn, J.B.; Chang, J.H.; Suh, C.O.; Hong, S.; Roh, J.K.; Shin, S.J.; Rha, S.Y. Brain metastases from colorectal carcinoma: Prognostic factors and outcome. J. Neuro-Oncol. 2010, 101, 49–55. [Google Scholar]
- Baek, J.Y.; Kang, M.H.; Hong, Y.S.; Kim, T.W.; Kim, D.Y.; Oh, J.H.; Lee, S.H.; Park, J.H.; Kim, J.H.; Kim, S.Y. Characteristics and prognosis of patients with colorectal cancer-associated brain metastases in the era of modern systemic chemotherapy. J. Neuro-Oncol. 2011, 104, 745–753. [Google Scholar]
- Jiang, X.B.; Yang, Q.Y.; Sai, K.; Zhang, X.H.; Chen, Z.P.; Mou, Y.G. Brain metastases from colorectal carcinoma: A description of 60 cases in a single Chinese cancer center. Tumour Biol. 2011, 32, 1249–1256. [Google Scholar]
- Fokas, E.; Henzel, M.; Hamm, K.; Surber, G.; Kleinert, G.; Engenhart-Cabillic, R. Multidisciplinary treatment of brain metastases derived from colorectal cancer incorporating stereotactic radiosurgery: Analysis of 78 patients. Clin. Colorectal Cancer 2011, 10, 121–125. [Google Scholar]
- Byrne, B.E.; Geddes, T.; Welsh, F.K.; John, T.G.; Chandrakumaran, K.; Rees, M. The incidence and outcome of brain metastases after liver resection for colorectal cancer metastases. Colorectal Dis. 2012, 14, 721–726. [Google Scholar]
- Noura, S.; Ohue, M.; Shingai, T.; Fujiwara, A.; Imada, S.; Sueda, T.; Yamada, T.; Fujiwara, Y.; Ohigashi, H.; Yano, M.; et al. Brain metastasis from colorectal cancer: Prognostic factors and survival. J. Surg. Oncol. 2012, 106, 144–148. [Google Scholar]
- Kye, B.H.; Kim, H.J.; Kang, W.K.; Cho, H.M.; Hong, Y.K.; Oh, S.T. Brain metastases from colorectal cancer: The role of surgical resection in selected patients. Colorectal Dis. 2012, 14, e378–e385. [Google Scholar]
- Damiens, K.; Ayoub, J.P.; Lemieux, B.; Aubin, F.; Saliba, W.; Campeau, M.P.; Tehfe, M. Clinical features and course of brain metastases in colorectal cancer: An experience from a single institution. Curr. Oncol. 2012, 19, 254–258. [Google Scholar]
- Kim, H.J.; Huh, J.W.; Jung, T.Y.; Kim, I.Y.; Kim, H.R.; Jung, S.; Kim, Y.J. Clinical outcome with gamma-knife surgery or surgery for brain metastases from colorectal cancer. J. Clin. Neurosci. 2013, 20, 1417–1421. [Google Scholar]
- Mege, D.; Ouaissi, M.; Fuks, D.; Metellus, P.; Peltier, J.; Dufour, H.; Regimbeau, J.M.; Dahan, L.; Sielezneff, I.; Sastre, B. Patients with brain metastases from colorectal cancer are not condemned. Anticancer Res. 2013, 33, 5645–5648. [Google Scholar]
- Suzuki, Y.; Yamaguchi, T.; Matsumoto, H.; Nakano, D.; Honda, G.; Shinoura, N.; Karasawa, K.; Takahashi, K. Prognostic factors and treatment effects in patients with curatively resected brain metastasis from colorectal cancer. Dis. Colon Rectum 2014, 57, 56–63. [Google Scholar]
- Magni, E.; Santoro, L.; Ravenda, P.S.; Leonardi, M.C.; Bonomo, G.; Monfardini, L.; Nole, F.; Zampino, M.G. Brain metastases from colorectal cancer: Main clinical factors conditioning outcome. Int. J. Colorectal Dis. 2014, 29, 201–208. [Google Scholar]
- Ballinger, A.B.; Anggiansah, C. Colorectal cancer. BMJ 2007, 335, 715–718. [Google Scholar]
- O’Connell, J.B.; Maggard, M.A.; Ko, C.Y. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J. Natl. Cancer Inst. 2004, 96, 1420–1425. [Google Scholar]
- Kornmann, M.; Link, K.; Formentini, A. Differences in colon and rectal cancer chemosensitivity. Colorectal Cancer 2014, 3, 93–105. [Google Scholar]
- Goldberg, R.M.; Rothenberg, M.L.; van Cutsem, E.; Benson, A.B., III; Blanke, C.D.; Diasio, R.B.; Grothey, A.; Lenz, H.J.; Meropol, N.J.; Ramanathan, R.K.; et al. The continuum of care: A paradigm for the management of metastatic colorectal cancer. Oncologist 2007, 12, 38–50. [Google Scholar]
- Mintz, A.H.; Kestle, J.; Rathbone, M.P.; Gaspar, L.; Hugenholtz, H.; Fisher, B.; Duncan, G.; Skingley, P.; Foster, G.; Levine, M. A randomized trial to assess the efficacy of surgery in addition to radiotherapy in patients with a single cerebral metastasis. Cancer 1996, 78, 1470–1476. [Google Scholar]
- Vecht, C.J.; Haaxma-Reiche, H.; Noordijk, E.M.; Padberg, G.W.; Voormolen, J.H.; Hoekstra, F.H.; Tans, J.T.; Lambooij, N.; Metsaars, J.A.; Wattendorff, A.R.; et al. Treatment of single brain metastasis: Radiotherapy alone or combined with neurosurgery? Ann. Neurol. 1993, 33, 583–590. [Google Scholar]
- Akgul, O.; Cetinkaya, E.; Ersoz, S.; Tez, M. Role of surgery in colorectal cancer liver metastases. World J. Gastroenterol. 2014, 20, 6113–6122. [Google Scholar]
- Michalski, C.W.; Erkan, M.; Huser, N.; Muller, M.W.; Hartel, M.; Friess, H.; Kleeff, J. Resection of primary pancreatic cancer and liver metastasis: A systematic review. Dig. Surg. 2008, 25, 473–480. [Google Scholar]
- Romano, F.; Garancini, M.; Uggeri, F.; Degrate, L.; Nespoli, L.; Gianotti, L.; Nespoli, A. Surgical treatment of liver metastases of gastric cancer: State of the art. World J. Surg. Oncol. 2012, 10. [Google Scholar] [CrossRef]
- Chen, F.; Sato, K.; Sakai, H.; Miyahara, R.; Bando, T.; Okubo, K.; Hirata, T.; Date, H. Pulmonary resection for metastasis from esophageal carcinoma. Interact. Cardiovasc. Thorac. Surg. 2008, 7, 809–812. [Google Scholar]
- Matsunaga, M.; Wada, S.; Daa, T.; Harada, K.; Okamura, K.; Noguchi, T. Long-term survival after resection of brain metastases from esophagogastric junction adenocarcinoma: Report of two cases and review of the literature. Clin. J. Gastroenterol. 2014, 7, 213–218. [Google Scholar]
- Farnell, G.F.; Buckner, J.C.; Cascino, T.L.; O’Connell, M.J.; Schomberg, P.J.; Suman, V. Brain metastases from colorectal carcinoma. The long term survivors. Cancer 1996, 78, 711–716. [Google Scholar]
- Kesler, K.A.; Hammoud, Z.T.; Helft, P.R.; Rieger, K.M.; Pritz, M.B.; Brown, J.W. Long-term survival after excision of a solitary esophageal cancer brain metastasis. J. Thorac. Cardiovasc. Surg. 2006, 131, 497–498. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lemke, J.; Scheele, J.; Kapapa, T.; Von Karstedt, S.; Wirtz, C.R.; Henne-Bruns, D.; Kornmann, M. Brain Metastases in Gastrointestinal Cancers: Is there a Role for Surgery? Int. J. Mol. Sci. 2014, 15, 16816-16830. https://doi.org/10.3390/ijms150916816
Lemke J, Scheele J, Kapapa T, Von Karstedt S, Wirtz CR, Henne-Bruns D, Kornmann M. Brain Metastases in Gastrointestinal Cancers: Is there a Role for Surgery? International Journal of Molecular Sciences. 2014; 15(9):16816-16830. https://doi.org/10.3390/ijms150916816
Chicago/Turabian StyleLemke, Johannes, Jan Scheele, Thomas Kapapa, Silvia Von Karstedt, Christian Rainer Wirtz, Doris Henne-Bruns, and Marko Kornmann. 2014. "Brain Metastases in Gastrointestinal Cancers: Is there a Role for Surgery?" International Journal of Molecular Sciences 15, no. 9: 16816-16830. https://doi.org/10.3390/ijms150916816