
Melatonin and Female Hormone Secretion in Postmenopausal Overweight Women

Abstract
:1. Introduction
2. Results





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Correlation | Correlation Coefficient r | ||
|---|---|---|---|
| Group I | Group II | Group III | |
| Melatonin/BMI | −0.3319 | −0.3158 | −0.2829 |
| 17-β-estradiol/BMI | 0.3232 | 0.3682 | 0.4206 |
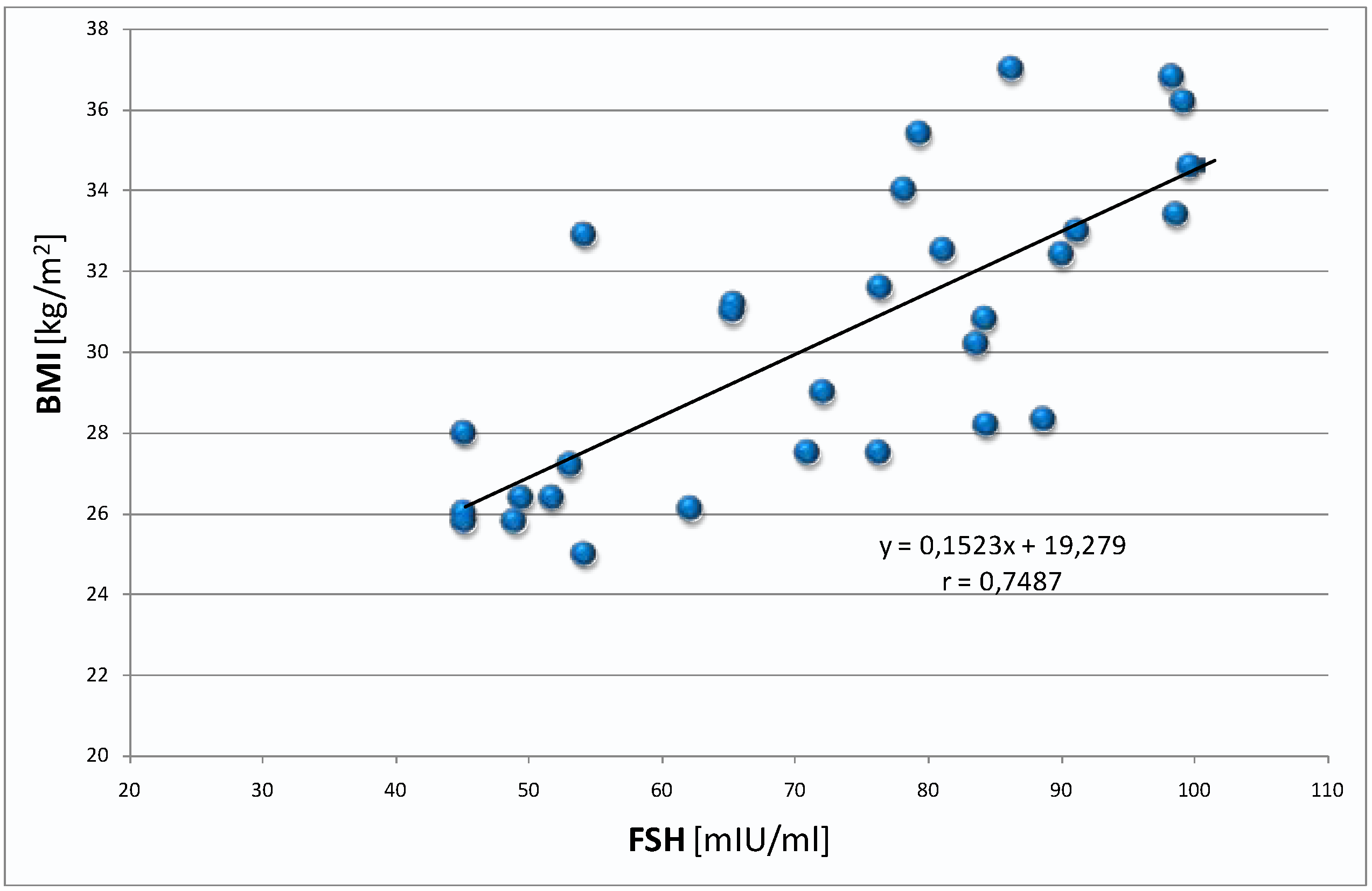
| FSH/BMI | −0.1567 | −0.2478 | 0.7487 *** |
| aMT6s/BMI | −0.3774 | −0.4564 | −0.8272 *** |


3. Discussion
4. Experimental Section
| Feature | Group I | Group II | Group III |
|---|---|---|---|
| Age (years) | 32.4 ± 3.1 | 57.3 ± 2.1 | 58.0 ± 4.3 |
| BMI (kg/m2) | 21.7 ±.1.7 | 21.8 ± 1.8 | 30.4 ± 3.7 ** |
| HARS (points) | 10.5 ±.6.1 | 19.7 ±.3.5 | 18.6 ± 3.1 |
| BDI (points) | 6.6 ± 2.9 | 16.8 ± 2.5 | 17.0 ± 2.1 |
| GFR (mL/min) | 104.8 ± 10.2 | 96.5 ± 7.1 | 92.0 ± 11.9 |
Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Freeman, E.W.; Sammel, M.D.; Lin, H.; Nelson, D.B. Associations of hormones and menopausal status with depressed mood in women with no history of depression. Arch. Gen. Psychiatry 2006, 63, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Frey, B.N.; Lord, C.; Soares, C.N. Depression during menopausal transition, a review of treatment strategies and pathophysiological correlates. Menopause Int. 2008, 14, 123–128. [Google Scholar] [PubMed]
- Freeman, E.W. Associations of depression with the transition to menopause. Menopause 2010, 17, 823–827. [Google Scholar] [CrossRef] [PubMed]
- Everson-Rose, S.A.; Lewis, T.T.; Karavolos, K.; Dugan, S.A.; Wesley, D.; Powell, L.H. Depressive symptoms and increased visceral fat in middle-aged women. Psychosom. Med. 2009, 71, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Murabito, J.M.; Massaro, J.M.; Clifford, B.; Hoffmann, U.; Fox, C.S. Depressive symptoms are associated with visceral adiposity in a community-based sample of middle-aged women and men. Obesity 2013, 21, 1713–1719. [Google Scholar] [CrossRef] [PubMed]
- Wiltink, J.; Michal, M.; Wild, P.S.; Zwiener, I.; Blettner, M.; Münzel, T.; Schulz, A.; Kirschner, Y.; Beutel, M.E. Associations between depression and different measures of obesity (BMI, WC, WHtR, WHR). BMC Psychiatry 2013, 13, 223. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.J.; Wu, C.H.; Yao, W.J.; Yang, Y.C.; Wu, J.S.; Lu, F.H. Relationships of age, menopause and central obesity on cardiovascular disease risk factors in Chinese women. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1699–1704. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, S.; Salman, M.; Lokesh, S.; Xaviour, D.; Saheb, S.Y.; Prasad, B.V.; Sarkar, B. Menopause versus aging. The predictor of obesity and metabolic aberrations among menopausal women of Karnataka, South India. J. Midlife Health 2012, 3, 24–30. [Google Scholar] [PubMed]
- Zedler, B.; von Lengerke, T.; Emeny, R.; Heier, M.; Lacruz, M.E.; Ladwig, K.H. Obesity and symptoms of depression and anxiety in pre- and post-menopausal women, a comparison of different obesity indicators. Psychother. Psychosom. Med. Psychol. 2014, 64, 128–135. [Google Scholar] [PubMed]
- Asarian, L.; Geary, N. Cyclic estradiol treatment normalizes body weight and restores physiological patterns of spontaneous feeding and sexual receptivity in ovariectomized rats. Horm. Behav. 2002, 42, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Geary, N.; Corwin, R.L. Ovarian hormones inhibit fat intake under binge-type conditions in ovariectomized rats. Physiol. Behav. 2008, 95, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Benmansour, S.; Privratsky, A.A.; Adeniji, O.S.; Frazer, A. Signaling mechanisms involved in the acute effects of estradiol on 5-HT clearance. Int. J. Neuropsychopharmacol. 2014, 17, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Butera, P.C.; Bradway, D.M.; Cataldo, N.J. Modulation of the satiety effect of cholecystokinin by estradiol. Physiol. Behav. 1993, 53, 1235–1238. [Google Scholar] [CrossRef] [PubMed]
- Geary, N. The effect of estrogen on appetite. Medscape Women’s Health 1998, 3, 3. [Google Scholar] [PubMed]
- Asarian, L.; Geary, N. Modulation of appetite by gonadal steroid hormones. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2006, 361, 1251–1263. [Google Scholar] [CrossRef] [PubMed]
- Hutson, W.R.; Roehrkasse, R.L.; Wald, A. Influence of gender and menopause on gastric emptying and motility. Gastroenterology 1989, 96, 11–17. [Google Scholar] [PubMed]
- Bond, E.F.; Heitkemper, M.M.; Bailey, S.L. Estrogen suppresses gastric motility response to thyrotropin-releasing hormone and stress in awake rats. Res. Nurs. Health 1998, 21, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Amure, B.O.; Omole, A.A. Sex hormones, and acid gastric secretion induced with carbachol, histamine, and gastrin. Gut 1970, 11, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Tuo, B.; Wen, G.; Wei, J.; Liu, X.; Wang, X.; Zhang, Y.; Wu, H.; Dong, X.; Chow, J.Y.; Vallon, V.; Dong, H. Estrogen regulation of duodenal bicarbonate secretion and sex-specific protection of human duodenum. Gastroenterology 2011, 141, 854–863. [Google Scholar] [CrossRef] [PubMed]
- De Villiers, T.J.; Gass, M.L.; Haines, C.J.; Hall, J.E.; Lobo, R.A.; Pierroz, D.D.; Rees, M. Global Consensus Statement on menopausal hormone therapy. Climacteric 2013, 16, 203–204. [Google Scholar] [CrossRef] [PubMed]
- Rossouw, J.E.; Prentice, R.L.; Manson, J.E.; Wu, L.; Barad, D.; Barnabei, V.M.; Ko, M.; LaCroix, A.Z.; Margoli,s, K.L.; Stefanick, M.L. Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA 2007, 297, 1465–1477. [Google Scholar] [CrossRef] [PubMed]
- Archer, D.F.; Oger, E. Estrogen and progestogen effect on venous thromboembolism in menopausal women. Climacteric 2012, 15, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Speroff, L. Transdermal hormone therapy and the risk of stroke and venous thrombosis. Climacteric 2010, 13, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Lobo, R.A. Menopause and stroke and the effects of hormonal therapy. Climacteric 2007, 10, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Antoine, C.; Ameye, L.; Paesmans, M.; Rozenberg, S. Treatment of climacteric symptoms in breast cancer patients: A retrospective study from a medication databank. Maturitas 2014, 78, 228–232. [Google Scholar] [CrossRef] [PubMed]
- De Villiers, T.J.; Pines, A.; Panay, N.; Gambacciani, M.; Archer, D.F.; Baber, R.J.; Davis, S,R.; Gompel, A.A.; Henderson, V.W.; Langer, R.; et al. Updated 2013 International Menopause Society recommendations on menopausal hormone therapy and preventive strategies for midlife health. Climacteric 2013, 16, 316–337. [Google Scholar] [CrossRef] [PubMed]
- North American Menopause Society. The 2012 hormone therapy position statement of The North American Menopause Society. Menopause 2012, 19, 257–271. [Google Scholar]
- Voelker, R. FDA expands warning on diet products. JAMA 2009, 301, 1646. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, F.; Fraschini, F.; Esposti, G.; Bossolo, P.A.; Marelli, G.; Ferrari, E. Melatonin circadian rhythm in anorexia nervosa and obesity. Psychiatry Res. 1988, 23, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, E.; Foppa, S.; Bossolo, P.A.; Comis, S.; Esposti, G.; Licini, V.; Fraschini, F.; Brambilla, F. Melatonin and pituitary-gonadal function in disorders of eating behavior. J. Pineal Res. 1989, 7, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Lima, F.B.; Machado, U.F.; Bartol, I.; Seraphim, P.M.; Sumida, D.H.; Moraes, S.M.; Hell, N.S.; Okamoto, M.M.; Saad, M.J.; Carvalho, C.R.; et al. Pinealectomy causes glucose intolerance and decreases adipose cell responsiveness to insulin in rats. Am. J. Physiol. 1998, 275, E934–E941. [Google Scholar] [PubMed]
- Picinato, M.C.; Haber, E.P.; Carpinelli, A.R.; Cipolla-Neto, J. Daily rhythm of glucose-induced insulin secretion by isolated islets from intact and pinealectomized rat. J. Pineal Res. 2002, 33, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, D.D.; Boldt, B.M.; Wilkinson, C.W.; Yellon, S.M.; Matsumoto, A.M. Daily melatonin administration at middle age suppresses male rat visceral fat, plasma leptin, and plasma insulin to youthful levels. Endocrinology 1999, 140, 1009–1012. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Vale, M.I.; Andreotti, S.; Peres, S.B.; Anhê, G.F.; das Neves Borges-Silva, C.; Neto, J.C.; Lima, F.B. Melatonin enhances leptin expression by rat adipocytes in the presence of insulin. J. Appl. Physiol. 2005, 98, 1037–1043. [Google Scholar] [PubMed]
- Ríos-Lugo, M.J.; Cano, P.; Jiménez-Ortega, V.; Fernández-Mateos, M.P.; Scacchi, P.A.; Cardinali, D.P.; Esquifino, A.I. Melatonin effect on plasma adiponectin, leptin, insulin, glucose, triglycerides and cholesterol in normal and high fat-fed rats. J. Pineal Res. 2010, 49, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Agil, A.; Navarro-Alarcón, M.; Ruiz, R.; Abuhamadah, S.; El-Mir, M.Y.; Vázquez, G.F. Beneficial effects of melatonin on obesity and lipid profile in young Zucker diabetic fatty rats. J. Pineal Res. 2011, 50, 207–212. [Google Scholar] [PubMed]
- Favero, G.; Lonati, C.; Giugno, L.; Castrezzati, S.; Rodella, L.F.; Rezzani, R. Obesity-related dysfunction of the aorta and prevention by melatonin treatment in ob/ob mice. Acta Histochem. 2013, 115, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Zanuto, R.; Siqueira-Filho, M.A.; Caperuto, L.C.; Bacurau, R.F.; Hirata, E.; Peliciari-Garcia, R.A.; do Amaral, F.G.; Marçal, A.C.; Ribeiro, L.M.; Camporez, J.P.; et al. Melatonin improves insulin sensitivity independently of weight loss in old obese rats. J. Pineal Res. 2013, 55, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Cardinali, D.P.; Cano, P.; Jiménez-Ortega, V.; Esquifino, A.I. Melatonin and the metabolic syndrome, physiopathologic and therapeutical implications. Neuroendocrinology 2011, 93, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Walecka-Kapica, E.; Klupińska, G.; Chojnacki, J.; Tomaszewska-Warda, K.; Błońska, A.; Chojnacki, C. The effect of melatonin on the quality of sleep and nutritional status in postmenopausam women. Menopausal Rev. 2014, in press. [Google Scholar]
- Cipolla-Neto, J.; Amaral, F.G.; Afeche, S.C.; Tan, D.X.; Reiter, R.J. Melatonin, energy metabolism, and obesity, a review. J. Pineal Res. 2014, 56, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Kennaway, D.J.; Lushington, K.; Dawson, D.; Lack, L.; van den Heuvel, C.; Rogers, N. Urinary 6-sulfatoxymelatonin excretion and aging, new results and a critical review of the literature. J. Pineal Res. 1999, 27, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Toffol, E.; Kalleinen, N.; Haukka, J.; Vakkuri, O.; Partonen, T.; Polo-Kantola, P. Melatonin in perimenopausal and postmenopausal women, associations with mood, sleep, climacteric symptoms, and quality of life. Menopause 2014, 21, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.J.; Tan, D.X.; Fuentes-Broto, L. Melatonin, a multitasking molecule. Prog. Brain Res. 2010, 181, 127–151. [Google Scholar] [PubMed]
- Bódis, J.; Koppán, M.; Kornya, L.; Tinneberg, H.R.; Török, A. Influence of melatonin on basal and gonadotropin-stimulated progesterone and estradiol secretion of cultured human granulosa cells and in the superfused granulosa cell system. Gynecol. Obstet. Investig. 2001, 52, 198–202. [Google Scholar] [CrossRef]
- Luboshitzky, R.; Herer, P.; Shen-Orr, Z. Cyproterone acetate-ethinyl estradiol treatment alters urinary 6-sulfatoxymelatonin excretion in hyperandrogenic women. Neuro Endocrinol. Lett. 2002, 23, 309–313. [Google Scholar] [PubMed]
- Gruber, D.M.; Schneeberger, C.; Laml, T.; Sator, M.O.; Huber, J.C. 6-sulfatoxymelatonin in women with secondary amenorrhea. Wien. Klin. Wochenschr. 1997, 109, 750–752. [Google Scholar] [PubMed]
- Okatani, Y.; Morioka, N.; Wakatsuki, A. Changes in nocturnal melatonin secretion in perimenopausal women, correlation with endogenous estrogen concentrations. J. Pineal Res. 2000, 28, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Vakkuri, O.; Kivelä, A.; Leppäluoto, J.; Valtonen, M.; Kauppila, A. Decrease in melatonin precedes follicle-stimulating hormone increase during perimenopause. Eur. J. Endocrinol. 1996, 135, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Blaicher, W.; Imhof, M.H.; Gruber, D.M.; Schneeberger, C.; Sator, M.O.; Huber, J.C. Endocrinological disorders: Focusing on melatonin’s interactions. Gynecol. Obstet. Investig. 1999, 48, 179–182. [Google Scholar] [CrossRef]
- Sanchez-Mateos, S.; Alonso-Gonzalez, C.; Gonzalez, A.; Martinez-Campa, C,M.; Mediavilla, M.D.; Cos, S.; Sanchez-Barcelo, E.J. Melatonin and estradiol effects on food intake, body weight, and leptin in ovariectomized rats. Maturitas 2007, 58, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Sartori, C.; Dessen, P.; Mathieu, C.; Monney, A.; Bloch, J.; Nicod, P.; Scherrer, U.; Duplain, H. Melatonin improves glucose homeostasis and endothelial vascular function in high-fat diet-fed insulin-resistant mice. Endocrinology 2009, 150, 5311–5317. [Google Scholar] [CrossRef] [PubMed]
- Nduhirabandi, F.; Du Toit, E.F.; Blackhurst, D.; Marais, D.; Lochner, A. Chronic melatonin consumption prevents obesity-related metabolic abnormalities and protects the heart against myocardial ischemia and reperfusion injury in a prediabetic model of diet-induced obesity. J. Pineal Res. 2011, 50, 171–182. [Google Scholar] [PubMed]
- Srinivasan, V.; Ohta, Y.; Espino, J.; Pariente, J.A.; Rodriguez, A.B.; Mohamed, M.; Zakaria, R. Metabolic syndrome, its pathophysiology and the role of melatonin. Recent Pat. Endocr. Metab. Immune Drug Discov. 2013, 7, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Wolden-Hanson, T.; Mitton, D.R.; McCants, R.L.; Yellon, S.M.; Wilkinson, C.W.; Matsumoto, A.M.; Rasmussen, D.D. Daily melatonin administration to middle-aged male rats suppresses body weight, intraabdominal adiposity, and plasma leptin and insulin independent of food intake and total body fat. Endocrinology 2000, 141, 487–497. [Google Scholar] [PubMed]
- Prunet-Marcassus, B.; Desbazeille, M.; Bros, A.; Louche, K..; Delagrange, P.; Renard, P.; Casteilla, L.; Pénicaud, L. Melatonin reduces body weight gain in Sprague Dawley rats with diet-induced obesity. Endocrinology 2003, 144, 5347–5352. [Google Scholar] [CrossRef] [PubMed]
- Hussein, M.R.; Ahmed, O.G.; Hassan, A.F.; Ahmed, M.A. Intake of melatonin is associated with amelioration of physiological changes, both metabolic and morphological pathologies associated with obesity, an animal model. Int. J. Exp. Pathol. 2007, 88, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.J.; Tan, D.X.; Korkmaz, A.; Ma, S. Obesity and metabolic syndrome, association with chronodisruption, sleep deprivation, and melatonin suppression. Ann. Med. 2012, 44, 564–577. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, A.; Topal, T.; Tan, D.X.; Reiter, R.J. Role of melatonin in metabolic regulation. Rev. Endocr. Metab. Disord. 2009, 10, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Blaicher, W.; Speck, E.; Imhof, M.H.; Gruber, D.M.; Schneeberger, C.; Sator, M.O.; Huber, J.C. Melatonin in postmenopausal females. Arch. Gynecol. Obstet. 2000, 263, 116–118. [Google Scholar] [CrossRef] [PubMed]
- Nduhirabandi, F.; du Toit, E.F.; Lochner, A. Melatonin and the metabolic syndrome: A tool for effective therapy in obesity-associated abnormalities? Acta Physiol. (Oxf.) 2012, 205, 209–223. [Google Scholar] [CrossRef]
- Rastmanesh, R.; de Bruin, P.F. Potential of melatonin for the treatment or prevention of obesity, an urgent need to include weight reduction as a secondary outcome in clinical trials of melatonin in obese patients with sleep disorders. Contemp. Clin. Trials 2012, 33, 574–575. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Murai, I.; Asai, S.; Takahashi, Y.; Matsuno, Y.; Komuro, S.; Kurosaka, H.; Iwasaki, A.; Ishikawa, K.; Arakawa, Y. Central nervous system action of melatonin on gastric acid and pepsin secretion in pylorus-ligated rats. Neuroreport 1998, 9, 2447–2450. [Google Scholar] [CrossRef] [PubMed]
- Sjöblom, M.; Flemström, G. Melatonin in the duodenal lumen is a potent stimulant of mucosal bicarbonate secretion. J. Pineal Res. 2003, 34, 288–293. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walecka-Kapica, E.; Chojnacki, J.; Stępień, A.; Wachowska-Kelly, P.; Klupińska, G.; Chojnacki, C. Melatonin and Female Hormone Secretion in Postmenopausal Overweight Women. Int. J. Mol. Sci. 2015, 16, 1030-1042. https://doi.org/10.3390/ijms16011030
Walecka-Kapica E, Chojnacki J, Stępień A, Wachowska-Kelly P, Klupińska G, Chojnacki C. Melatonin and Female Hormone Secretion in Postmenopausal Overweight Women. International Journal of Molecular Sciences. 2015; 16(1):1030-1042. https://doi.org/10.3390/ijms16011030
Chicago/Turabian StyleWalecka-Kapica, Ewa, Jan Chojnacki, Agnieszka Stępień, Patrycja Wachowska-Kelly, Grażyna Klupińska, and Cezary Chojnacki. 2015. "Melatonin and Female Hormone Secretion in Postmenopausal Overweight Women" International Journal of Molecular Sciences 16, no. 1: 1030-1042. https://doi.org/10.3390/ijms16011030