
Association between ADIPOQ +45T>G Polymorphism and Type 2 Diabetes: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Results
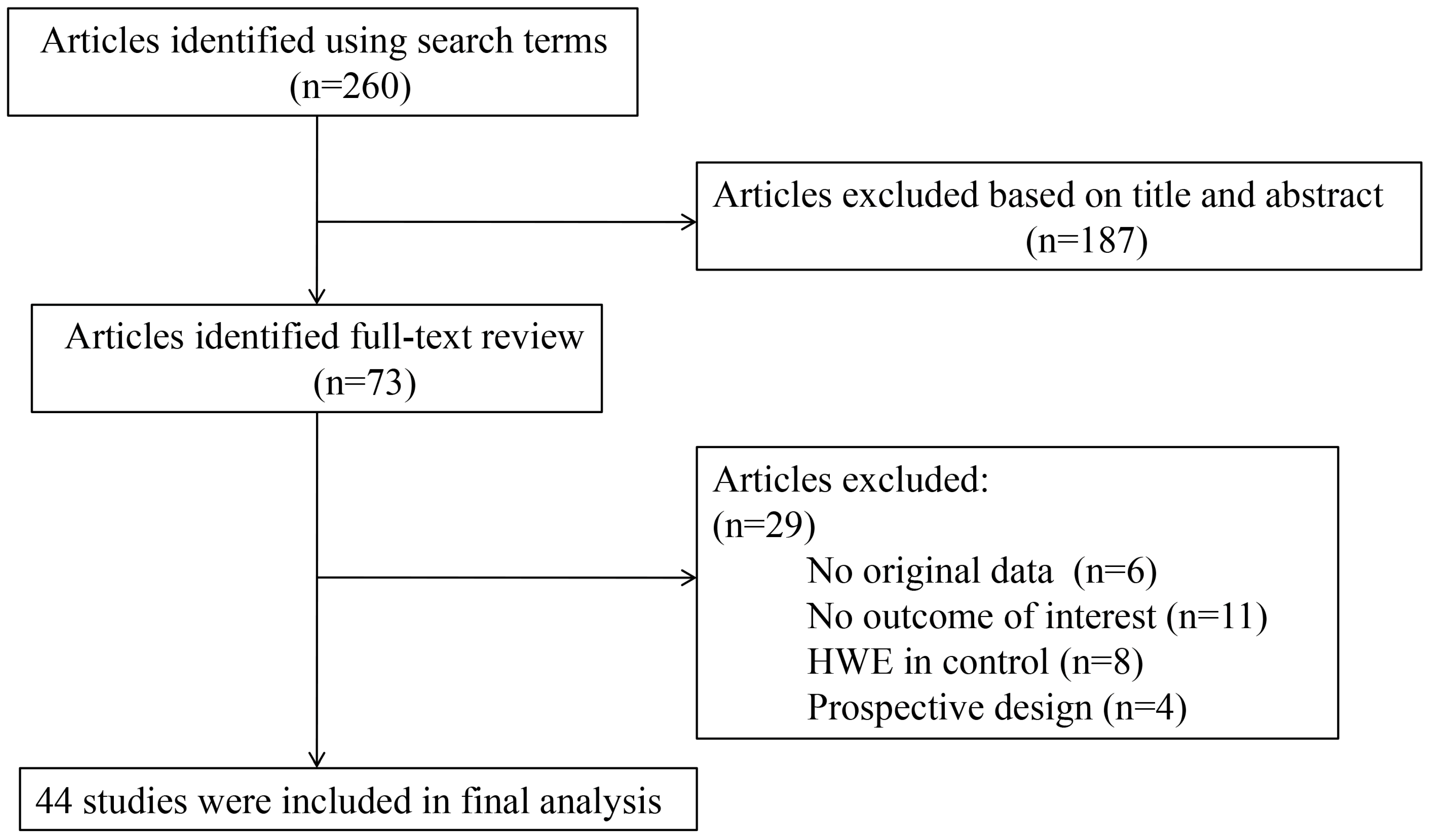
2.1. Description of the Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country/Ethnicity | Study Design | Genotyping Method | Cases | Controls | HWE | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TT | TG | GG | Allele G | Allele T | TT | TG | GG | Allele G | Allele T | χ2 Control Population | Cases | Controls | |||||
| [6] | 2009 | Chinese/Asian | Population-based | ARMS-PCR | 480 | 362 | 74 | 510 | 1322 | 483 | 389 | 98 | 585 | 1355 | 2.23 | 0.62 | 0.14 |
| [12] | 2010 | Italy/Caucasian | Cohort | RT-PCR | 370 | 117 | 16 | 149 | 857 | 359 | 126 | 18 | 162 | 844 | 2.68 | 0.08 | 0.1 |
| [13] | 2002 | Japanese/Asian | Population-based | PCR-DS | 164 | 169 | 51 | 271 | 497 | 251 | 183 | 46 | 275 | 685 | 2.18 | 0.48 | 0.14 |
| [14] | 2003 | Japanese/Asian | Population-based | PCR-DS | 78 | 66 | 20 | 106 | 222 | 90 | 74 | 15 | 104 | 254 | <0.01 | 0.31 | 0.97 |
| [15] | 2004 | Chinese/Asian | Population-based | PCR-RFLP | 104 | 71 | 20 | 111 | 279 | 98 | 74 | 15 | 104 | 270 | 0.04 | 0.14 | 0.84 |
| [16] | 2004 | Chinese/Asian | Population-based | PCR-RFLP | 8 | 46 | 24 | 94 | 62 | 39 | 35 | 11 | 57 | 113 | 0.49 | 0.04 | 0.48 |
| [17] | 2005 | Korean/Asian | Hospital-based | SBE | 252 | 202 | 39 | 280 | 706 | 201 | 181 | 45 | 271 | 583 | 0.2 | 0.87 | 0.65 |
| [18] | 2005 | Chinese/Asian | Hospital-based | PCR-RFLP | 56 | 36 | 12 | 60 | 148 | 48 | 38 | 4 | 46 | 134 | 1.08 | 0.11 | 0.3 |
| [19] | 2005 | Chinese/Asian | Population-based | PCR-RFLP | 53 | 46 | 16 | 78 | 152 | 46 | 44 | 5 | 54 | 136 | 1.82 | 0.25 | 0.18 |
| [20] | 2006 | Chinese/Asian | Population-based | PCR-RFLP | 103 | 69 | 23 | 115 | 275 | 78 | 57 | 4 | 65 | 213 | 2.9 | 0.04 | 0.09 |
| [21] | 2007 | Chinese/Asian | Population-based | PCR-RFLP | 36 | 19 | 2 | 23 | 91 | 75 | 16 | 3 | 22 | 166 | 2.92 | 0.79 | 0.09 |
| [22] | 2007 | Chinese/Asian | Hospital-based | PCR-RFLP | 67 | 36 | 17 | 70 | 170 | 60 | 45 | 15 | 75 | 165 | 1.94 | <0.01 | 0.16 |
| [23] | 2007 | Chinese/Asian | Hospital-based | PCR-RFLP | 80 | 92 | 28 | 148 | 252 | 122 | 72 | 6 | 84 | 316 | 1.44 | 0.85 | 0.23 |
| [24] | 2007 | Chinese/Asian | Population-based | PCR-RFLP | 39 | 48 | 13 | 74 | 126 | 58 | 40 | 3 | 46 | 156 | 1.6 | 0.77 | 0.21 |
| [25] | 2007 | Chinese/Asian | Population-based | RT-PCR | 20 | 94 | 54 | 202 | 134 | 68 | 60 | 22 | 104 | 196 | 2.05 | 0.03 | 0.15 |
| [26] | 2007 | Chinese/Asian | Population-based | PCR-RFLP | 89 | 79 | 12 | 103 | 257 | 152 | 114 | 20 | 154 | 418 | 0.05 | 0.32 | 0.83 |
| [27] | 2007 | Chinese/Asian | Population-based | RT-PCR | 90 | 36 | 12 | 60 | 216 | 48 | 64 | 20 | 104 | 160 | 0.03 | <0.01 | 0.86 |
| [28] | 2008 | Chinese/Asian | Hospital-based | PCR–RFLP | 134 | 135 | 20 | 175 | 403 | 59 | 38 | 6 | 50 | 156 | <0.01 | 0.07 | 0.97 |
| [29] | 2008 | Chinese/Asian | Population-based | PCR-RFLP | 126 | 115 | 14 | 143 | 367 | 76 | 40 | 4 | 48 | 192 | 0.21 | 0.06 | 0.65 |
| [30] | 2008 | Chinese/Asian | Hospital-based | PCR-RFLP | 103 | 75 | 17 | 109 | 281 | 79 | 53 | 6 | 65 | 211 | 0.61 | 0.53 | 0.43 |
| [31] | 2008 | Chinese/Asian | Population-based | PCR-RFLP | 55 | 26 | 16 | 58 | 136 | 53 | 41 | 4 | 49 | 147 | 1.31 | <0.01 | 0.25 |
| [32] | 2008 | Chinese/Asian | Population-based | PCR-RFLP | 167 | 123 | 22 | 167 | 457 | 85 | 75 | 7 | 89 | 245 | 3.7 | 0.92 | 0.05 |
| [33] | 2009 | Chinese/Asian | Population-based | PCR-RFLP | 44 | 44 | 18 | 80 | 132 | 28 | 24 | 6 | 36 | 80 | 0.06 | 0.23 | 0.8 |
| [34] | 2009 | Chinese/Asian | Population-based | PCR-RFLP | 71 | 44 | 11 | 66 | 186 | 47 | 54 | 11 | 76 | 148 | 0.64 | 0.28 | 0.42 |
| [35] | 2009 | Chinese/Asian | Population-based | PCR-RFLP | 68 | 52 | 11 | 74 | 188 | 59 | 42 | 4 | 50 | 160 | 1.1 | 0.81 | 0.29 |
| [36] | 2010 | Chinese/Asian | Hospital-based | PCR-RFLP | 38 | 47 | 15 | 77 | 123 | 60 | 37 | 3 | 43 | 157 | 0.92 | 0.94 | 0.34 |
| [37] | 2011 | Chinese/Asian | Population-based | PCR-RFLP | 209 | 99 | 19 | 137 | 517 | 206 | 103 | 20 | 143 | 515 | 2.09 | 0.12 | 0.15 |
| [38] | 2012 | Chinese/Asian | Population-based | PCR-RFLP | 88 | 54 | 11 | 76 | 230 | 88 | 62 | 8 | 78 | 238 | 0.48 | 0.5 | 0.49 |
| [39] | 2012 | Chinese/Asian | Population-based | PCR-RFLP | 97 | 46 | 4 | 54 | 240 | 135 | 52 | 2 | 56 | 322 | 1.53 | 0.6 | 0.22 |
| [40] | 2012 | Chinese/Asian | Hospital-based | PCR-SSCP | 114 | 134 | 26 | 186 | 362 | 84 | 50 | 7 | 64 | 218 | 0.02 | 0.13 | 0.9 |
| [41] | 2013 | Chinese/Asian | Hospital-based | PCR-DS | 75 | 79 | 26 | 131 | 229 | 64 | 48 | 8 | 64 | 176 | 0.06 | 0.49 | 0.8 |
| [42] | 2002 | Italy/Caucasian | Hospital-based | ARMS-PCR | 242 | 61 | 7 | 75 | 545 | 220 | 75 | 9 | 93 | 515 | 0.7 | 0.19 | 0.4 |
| [43] | 2004 | French/Caucasian | Population-based | RT-PCR | 24 | 6 | 1 | 8 | 54 | 2816 | 847 | 56 | 959 | 6479 | 0.72 | 0.44 | 0.4 |
| [44] | 2005 | Finland/Caucasian | Cohort | - | 235 | 23 | 0 | 23 | 493 | 255 | 26 | 2 | 30 | 536 | 2.04 | 0.45 | 0.15 |
| [45] | 2005 | Spain/Caucasian | Population-based | PCR-SSCP | 35 | 24 | 2 | 28 | 94 | 346 | 166 | 18 | 202 | 858 | 0.12 | 0.38 | 0.73 |
| [46] | 2006 | Mexico/- | Population-based | PCR-RFLP | 262 | 123 | 11 | 145 | 647 | 582 | 261 | 30 | 321 | 1425 | 0.01 | 0.44 | 0.91 |
| [47] | 2006 | German/Caucasian | Cohort | RT-PCR | 299 | 60 | 6 | 72 | 658 | 263 | 53 | 7 | 67 | 579 | 4.45 | 0.15 | 0.03 |
| [48] | 2007 | UK/Caucasian | Population-based | PCR-RFLP | 116 | 25 | 7 | 39 | 257 | 1968 | 536 | 35 | 606 | 4472 | 0.05 | <0.01 | 0.83 |
| [49] | 2008 | Polish/Caucasian | Population-based | PCR-RFLP | 117 | 10 | 2 | 14 | 244 | 108 | 8 | 1 | 10 | 224 | 3.16 | <0.01 | 0.08 |
| [50] | 2009 | Russian/Caucasian | Population-based | PCR–RFLP | 427 | 67 | 1 | 69 | 921 | 368 | 66 | 1 | 68 | 802 | 1.21 | 0.33 | 0.27 |
| [51] | 2009 | Iranian/Caucasian | Population-based | PCR-RFLP | 31 | 17 | 4 | 25 | 79 | 42 | 10 | 0 | 10 | 94 | 0.59 | 0.5 | 0.44 |
| [52] | 2010 | Brazilian/Asian | Population-based | PCR-DS | 93 | 95 | 12 | 119 | 281 | 100 | 85 | 15 | 115 | 285 | 0.28 | 0.05 | 0.6 |
| [53] | 2010 | Iranian/Caucasian | Population-based | PCR-RFLP | 171 | 63 | 7 | 77 | 405 | 117 | 47 | 9 | 65 | 281 | 2.08 | 0.68 | 0.15 |
| [54] | 2012 | Saudi Arabia/ Caucasian | Population-based | ARMS-PCR | 220 | 72 | 6 | 84 | 512 | 209 | 80 | 9 | 98 | 498 | 0.16 | 0.96 | 0.69 |

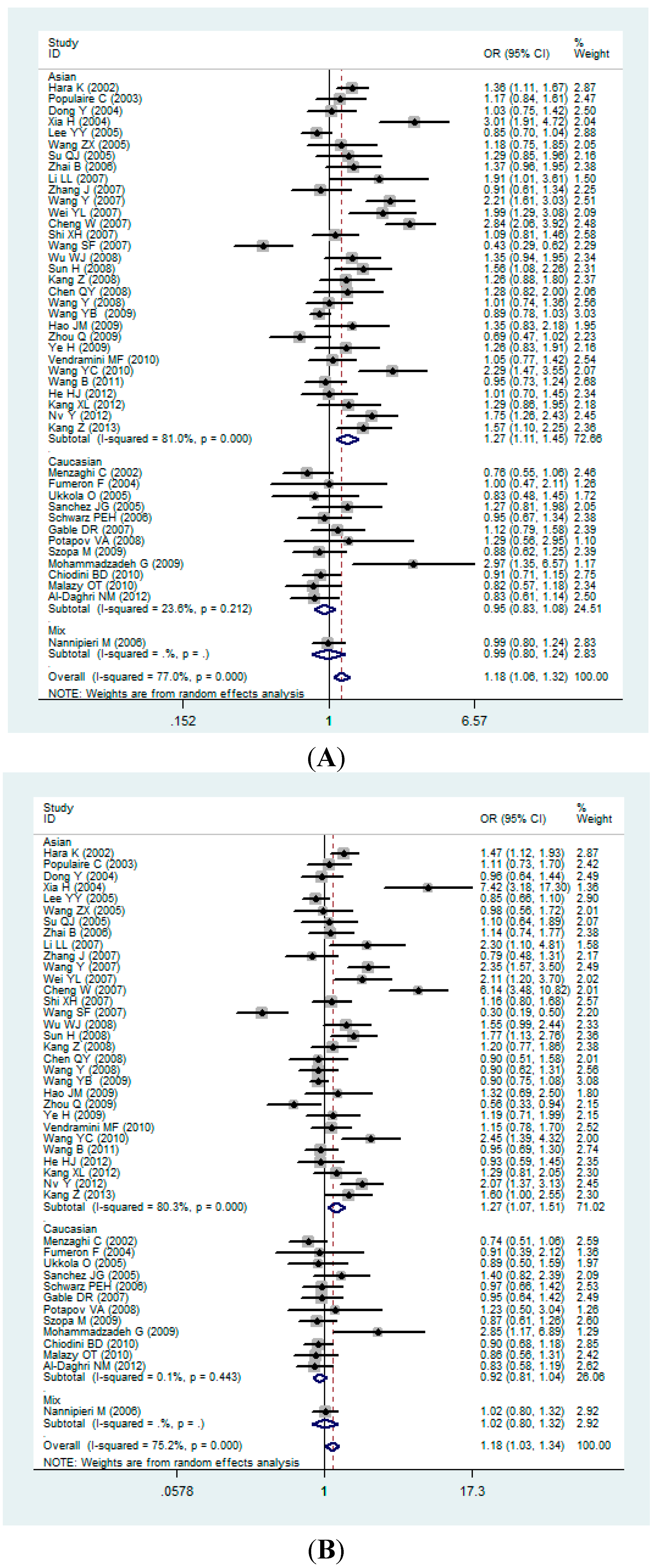
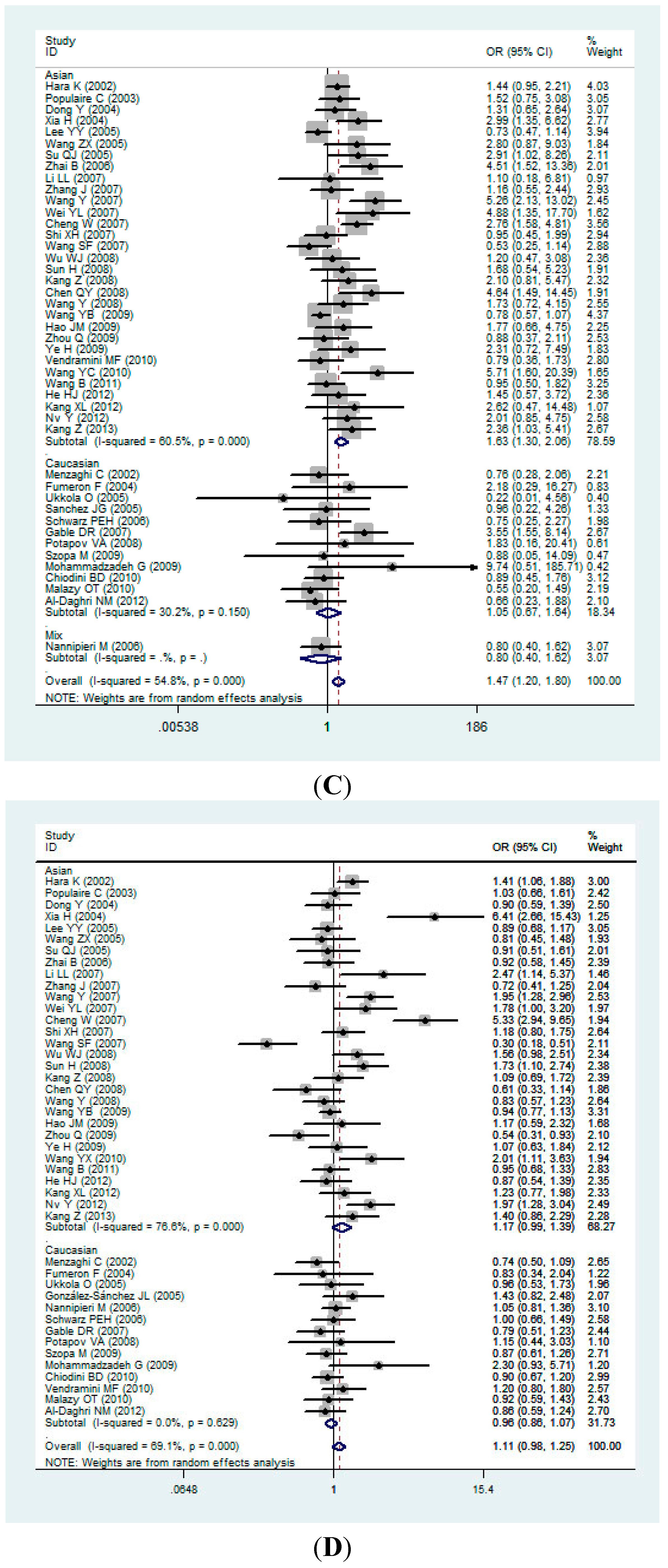
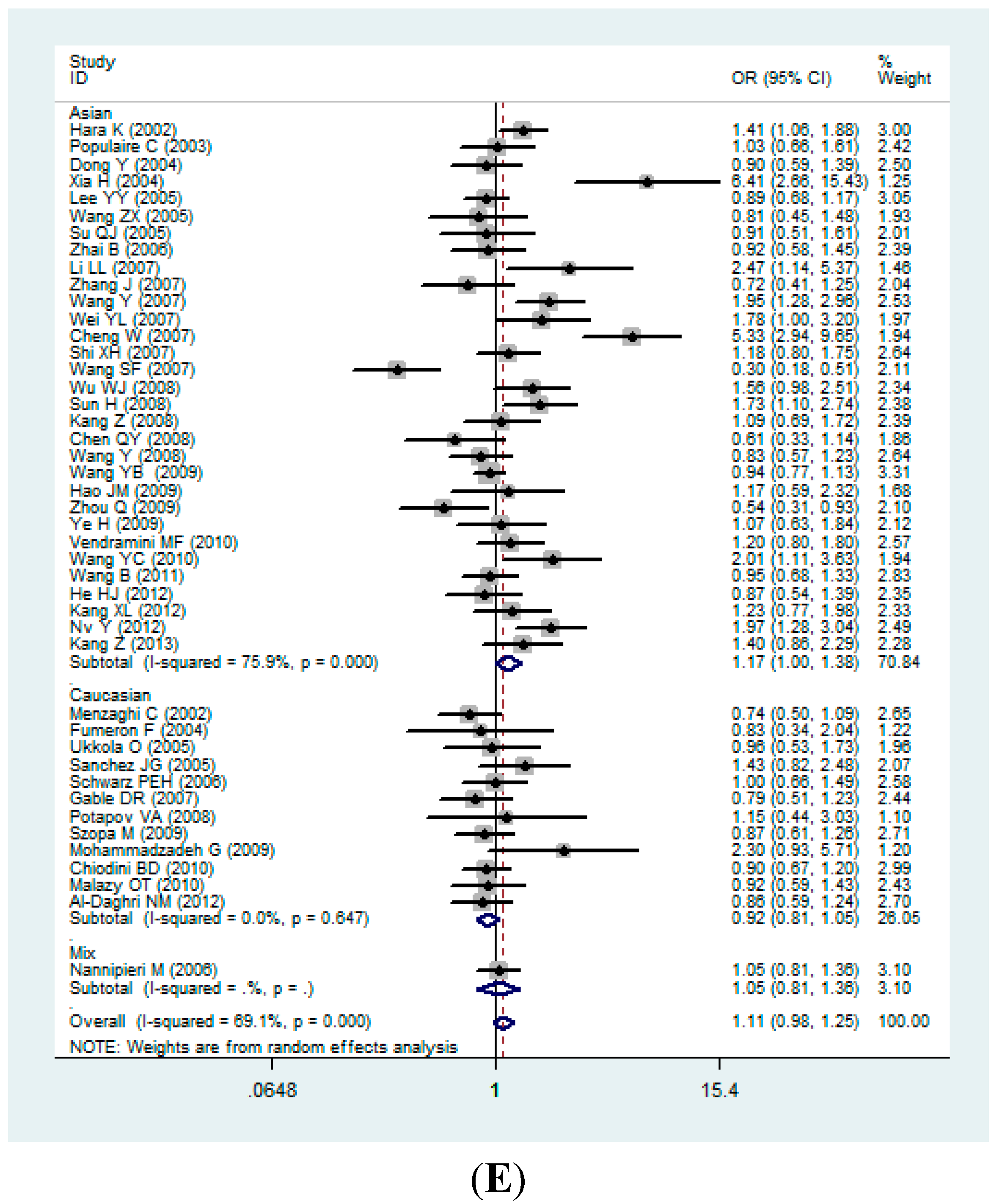
2.2. Pooled Analyses



2.3. Sensitivity Analysis
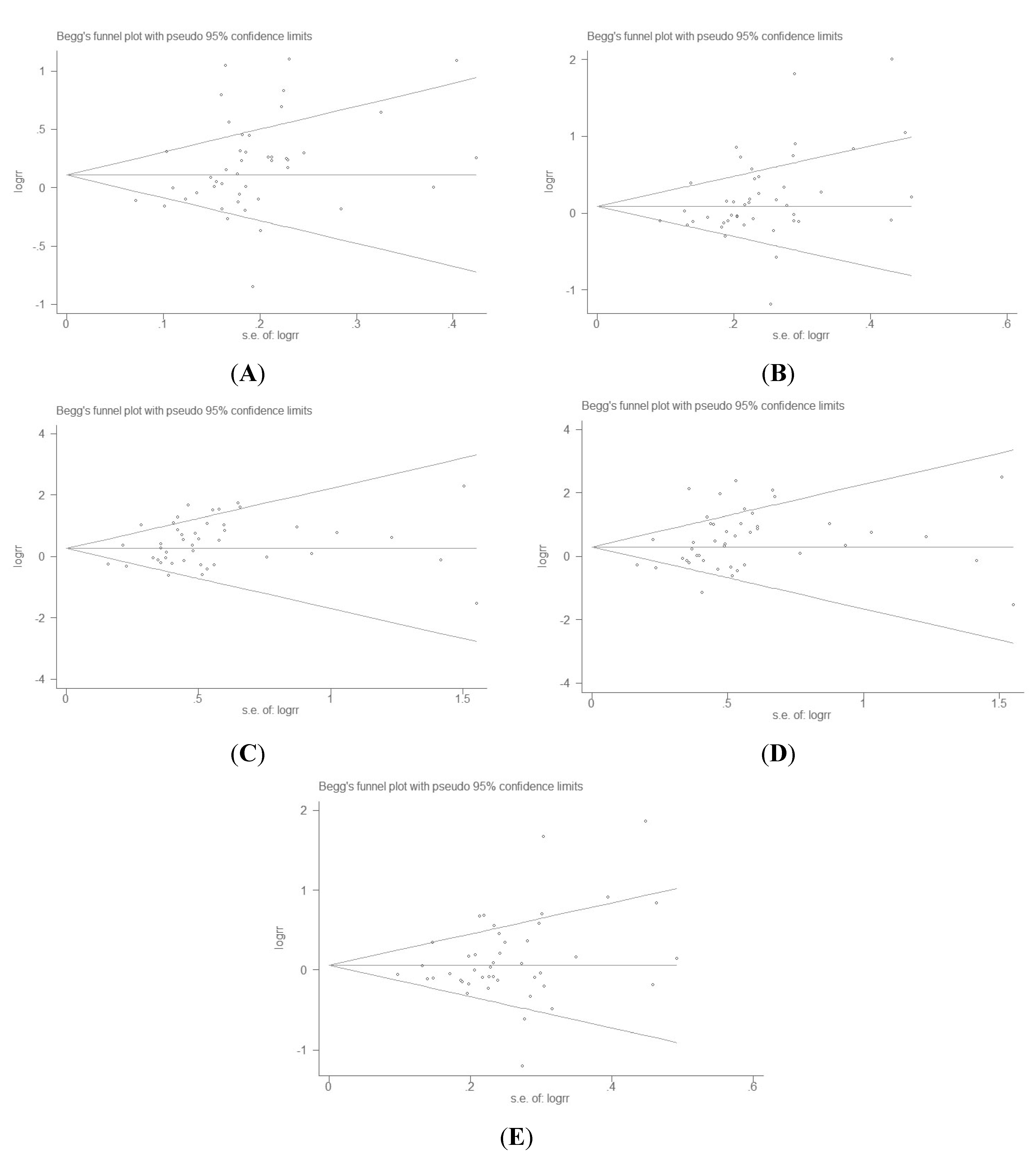
2.4. Publication Bias Analysis

3. Discussion
4. Materials and Methods
4.1. Literature Search Strategy
4.2. Inclusion and Exclusion Criteria
4.3. Data Extraction
4.4. Statistical Methods
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Matharoo, K.; Arora, P.; Bhanwer, A.J. Association of adiponectin (ADIPOQ) and sulphonylurea receptor (ABCC8) gene polymorphisms with Type 2 diabetes in North Indian population of Punjab. Gene 2013, 527, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, F.; Chu, J.W.; Lamendola, C.; McLaughlin, T.; Hayden, J.; Reaven, G.M.; Reaven, P.D. Discrimination between obesity and insulin resistance in the relationship with adiponectin. Diabetes 2004, 53, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Kern, P.A.; di Gregorio, G.B.; Lu, T.; Rassouli, N.; Ranganathan, G. Adiponectin expression from human adipose tissue: Relation to obesity, insulin resistance, and tumor necrosis factor-α expression. Diabetes 2003, 52, 1779–1785. [Google Scholar] [CrossRef] [PubMed]
- Tschritter, O.; Fritsche, A.; Thamer, C.; Haap, M.; Shirkavand, F.; Rahe, S.; Staiger, H.; Maerker, E.; Häring, H.; Stumvoll, M. Plasma adiponectin concentrations predict insulin sensitivity of both glucose and lipid metabolism. Diabetes 2003, 52, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Arita, Y.; Yamagata, K.; Matsukawa, Y.; Okutomi, K.; Horie, M.; Shimomura, I.; Hotta, K.; Kuriyama, H.; Kihara, S.; et al. Genomic structure and mutations in adipose-specific gene, adiponectin. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, D.; Liu, Y.; Yang, Y.; Zhao, T.; Xu, J.; Li, S.; Zhang, Z.; Feng, G.; He, L.; et al. Association study of the single nucleotide polymorphisms in adiponectin-associated genes with type 2 diabetes in Han Chinese. J. Genet. Genomics 2009, 36, 417–423. [Google Scholar] [CrossRef]
- Suriyaprom, K.; Phonrat, B.; Namjuntra, P.; Harnroongroj, T.; Tungtrongchitr, R. The −11377C>G adiponectin gene polymorphism alters the adiponectin concentration and the susceptibility to type 2 diabetes in Thais. Int. J. Vitam. Nutr. Res. 2010, 80, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Khadqawat, R.; Nq, HK.; Kumar, S.; Aggarwal, A.; Rao, V.R.; Sachdeva, M.P. A validation study of type 2 diabetes-related variants of the TCF7L2, HHEX, KCNJ11, and ADIPOQ genes in one endogamous ethnic group of North India. Ann. Hum. Genet. 2010, 74, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Mousavinasab, F.; Tahtinen, T.; Jokelainen, J.; Koskela, P.; Vanhala, M.; Oikarinen, J.; Keinänen-Kiukaanniemi, S.; Laakso, M. Common polymorphisms (single-nucleotide polymorphisms SNP+45 and SNP+276) of the adiponectin gene regulate serum adiponectin concentrations and blood pressure in young Finnish men. Mol. Genet. Metab. 2006, 87, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Arikoglu, H.; Ozdemir, H.; Kaya, D.E.; Ipekci, S.H.; Arslan, A.; Kayis, S.A.; Gonen, M.S. The Adiponectin variants contribute to the genetic background of type 2 diabetes in Turkish population. Gene. 2014, 534, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Peters, K.E.; Beilby, J.; Cadby, G.; Warrington, N.M.; Bruce, D.G.; Davis, W.A.; Davis, T.M.; Wiltshire, S.; Knuiman, M.; McQuillan, B.M.; et al. A comprehensive investigation of variants in genes encoding adiponectin (ADIPOQ) and its receptors (ADIPOR1/R2), and their association with serum adiponectin, type 2 diabetes, insulin resistance and the metabolic syndrome. BMC. Med. Genet. 2013, 14, 15. [Google Scholar] [CrossRef] [PubMed]
- Chiodini, B.D.; Specchia, C.; Gori, F.; Barlera, S.; D’Orazio, A.; Pietri, S.; Crociati, L.; Nicolucci, A.; Franciosi, M.; Signorini, S.; et al. Adiponectin gene polymorphisms and their effect on the risk of myocardial infarction and type 2 diabetes: An association study in an Italian population. Ther. Adv. Cardiovasc. Dis. 2010, 4, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Hara, K.; Boutin, P.; Mori, Y.; Tobe, K.; Dina, C.; Yasuda, K.; Yamauchi, T.; Otabe, S.; Okada, T.; Eto, K.; et al. Genetic variation in the gene encoding adiponectin is associated with an increased risk of type 2 diabetes in the Japanese population. Diabetes 2002, 51, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Populaire, C.; Mori, Y.; Dina, C.; Vasseur, F.; Vaxillaire, M.; Kadowaki, T.; Froguel, P. Does the −11377 promoter variant of APM1 gene contribute to the genetic risk for type 2 diabetes mellitus in Japanese families? Diabetologia 2003, 46, 443–445. [Google Scholar] [PubMed]
- Dong, Y.; Li, G.; Luo, T.H.; Wu, G.; Huang, W.; Luo, M. Relationship between adiponectin gene polymorphisms and type 2 diabetes. Acad. J. Shanghai Second. Med. Univ. 2004, 12, 008. [Google Scholar]
- Xia, H.; Mo, Y.Z.; Bian, R.W. Correlation between single nucleotide polymorphism of adiponectin gene and type 2 diabetes in Chinese. Chin. J. Endocrinol. Metab. 2004, 20, 236–237. [Google Scholar]
- Lee, Y.Y.; Lee, N.S.; Cho, Y.M.; Moon, M.K.; Jung, H.S.; Park, Y.J.; Park, H.J.; Youn, B.S.; Lee, H.K.; Park, K.S.; et al. Genetic association study of adiponectin polymorphisms with risk of type 2 diabetes mellitus in Korean population. Diabet. Med. 2005, 22, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.X. Study on Serum Adiponectin Level and Its Gene Polymorphism in Different Glucose Tolerance Humans. Master’s Thesis, Hebei Medical University, Shijiazhuang, China, 10 March 2005. [Google Scholar]
- Su, Q.J. Association of the T-G Polymorphism in Adiponectin (Exon 2) with Diabetes and Related Risk Factors. Master’s Thesis, Guangxi Medical University, Nanning, China, 25 May 2005. [Google Scholar]
- Zhai, B.; Ye, L.; Liu, J.W. Interaction of adiponectin and peroxisome proliferator-activated receptor γ 2 gene polymorphisms and their relationship with type 2 diabetes in population from Beijing communities. Chin. J. Clin. Rehabil. 2006, 10, 28–31. [Google Scholar]
- Li, L.L.; Kang, X.L.; Ran, X.J.; Wang, Y.; Wang, C.H.; Huang, L.; Ren, J.; Luo, X.; Mao, X.M. Associations between 45T/G polymorphism of the adiponectin gene and plasma adiponectin levels with type 2 diabetes. Clin. Exp. Pharmacol. Physiol. 2007, 34, 1287–1290. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J. Correlation between Single Nucleotide Polymorphism (+45, 276) of Adiponectin Gene and Type 2 Diabetes in Xinjiang Uigur Population. Master’s Thesis, Shihezi University, Shihezi, China, 15 June 2007. [Google Scholar]
- Wang, Y.; He, L.; Huang, C.L. Correlation of adiponectin gene polymorphism and type 2 diabetes Mellitusin Han Population of Guangdong. J. Trop. Med. 2007, 7, 651–653. [Google Scholar]
- Wei, Y.L.; Huo, Z.H.; Zhao, W. The relationship of the adiponectin +45 nucleotide T/G polymorphism with insulin resistance, obesity and type 2 diabetes. Chin. J. Diabetes 2007, 15, 583–585. [Google Scholar]
- Cheng, W.; Yi, H.Z.; Ma, X.W. Single nucleotide polymorphism of adiponectin gene 45 site in patientswith type 2 diabetes in the south of Henan province. J. Zhengzhou Univ. 2007, 42, 1145–1147. [Google Scholar]
- Shi, X.H.; Jin, F.; Sun, L.; Li, H.; Wang, L.; Yang, Z. Association of the polymorphism of SNP+45 (T/G) in adiponectin gene with type 2 diabetes. J. Clin. Rehabil. Tissue Eng. Res. 2007, 11, 4941–4944. [Google Scholar]
- Wang, S.F.; Zhao, J.J.; Jiang, Q. The correlation between adiponectin gene polymorphism and type 2 diabetes. Chin. J. Endocrinol. Metab. 2007, 23, 51–52. [Google Scholar]
- Wu, W.J.; Bu, R.F.; Liu, G.P. Study on serum adiponectin level and SNP45 in adiponectin gene in type 2 diabetes patients with hypertriglyceridemia. Chin. J. Diabetes 2008, 16, 402–404. [Google Scholar]
- Sun, H.; Gong, Z.C.; Yin, J.Y.; Liu, H.L.; Liu, Y.Z.; Guo, Z.W.; Zhou, H.H.; Wu, J.; Liu, Z.Q. The association of adiponectin allele 45T/G and −11377C/G polymorphisms with type 2 diabetes and rosiglitazone response in Chinese patients. Br. J. Clin. Pharmacol. 2008, 65, 917–926. [Google Scholar] [CrossRef] [PubMed]
- Kang, Z.; Sun, C.K.; Zhao, H.Z.; Sha, Y.; Yu, D.; Liu, D.; Yan, X.; Xue, Y. Correlation between polymorphism of adiponectin gene and type 2 diabetes mellitus in Bai and Han population at Daliarea. Chin. J. Diabetes 2008, 16, 718–720. [Google Scholar]
- Chen, Q.Y.; Su, Q.J.; Tan, W.W. Association of the T–G polymorphism in adiponectin (exon 2) with diabetes in Zhuang people in Guangxi. J. Guangxi Med. Univ. 2008, 25, 821–824. [Google Scholar]
- Wang, Y.; Wang, T.; Zhong, H.T. An association research of adiponectin gene SNP45 T/G polymorphism and type 2 diabetes mellitus. Prog. Mod. Biomed. 2008, 8, 84–86. [Google Scholar]
- Hao, J.M.; Diao, Z.H.; Liu, J.X. Correlation between single nucleotide polymorphism of adiponectin gene and type 2 diabetes in Han population of Hainan. Hainan Med. J. 2009, 20, 1–3. [Google Scholar]
- Zhou, Q.; Yang, J.; Luo, M.S. Research on adiponectin’s single nucleotide polymorphism (SNP+45) site expression in type 2 diabetes mellitus. Int. J. Lab. Med. 2009, 30, 105–107. [Google Scholar]
- Ye, H.; Zhuang, J. Association research of adiponectin gene T45G polymorphism and type 2 diabetes mellitusin Han Chinese. Pharm. Care. Res. 2009, 9, 158–160. (In Chinese) [Google Scholar]
- Wang, Y.X.; Zhao, L.; Yu, S.G. Correlation of adiponectin gene polymorphism and type 2 diabetes mellitus. Shandong Med. J. 2010, 50, 1–2. [Google Scholar]
- Wang, B.; Wang, C.; Wei, D.; Zhang, J.; He, H.; Ma, M.; Li, X.; Pan, L.; Xue, F.; Jonasson, J.M.; et al. An association study of SNP +45T>G of the ADIPOQ gene with type 2 diabetes in Yi and Han people in China. Int. J. Vitam. Nutr. Res. 2011, 81, 392–397. [Google Scholar] [CrossRef] [PubMed]
- He, H.J.; Wei, D.Y.; Wang, C.X. Association between single nucleotide polymorphism of adiponectin gene and type 2 diabetes in Han people in Liangshan, Sichuan province. Chin. J. Public Health 2012, 28, 302–304. [Google Scholar]
- Kang, X.L.; Kang, X.L.; He, C.H. Correlation of 45T/G polymorphism adiponectin gene with type 2 diabetes in Kazaks of Xinjiang. J. China Med. Univ. 2012, 41, 454–457. [Google Scholar]
- Nv, Y.; Ye, S.D.; Hu, H.L. The association of between the polymorphism of the adiponectin gene rs2241766 and rs1501299 and the metabolic traits of type 2 diabetes in Han Chinese. Chin. J. Clin. Healthc. 2012, 15, 337–339. [Google Scholar]
- Kang, Z.; Su, H.; Zhang, Y. Genetic association analysis of the adiponectin polymorphisms in type 2 diabetes of Bai nationality at Dali area. Lab. Med. Clin. 2013, 10, 3122–3124. [Google Scholar]
- Menzaghi, C.; Ercolino, T.; Di Paola, R.; Berg, A.H.; Warram, J.H.; Scherer, P.E.; Trischitta, V.; Doria, A. A haplotype at the adiponectin locus is associated with obesity and other features of the insulin resistance syndrome. Diabetes 2002, 51, 2306–2312. [Google Scholar] [CrossRef] [PubMed]
- Fumeron, F.; Aubert, R.; Siddig, A.; Betoulle, D.; Péan, F.; Hadjadj, S.; Tichet, J.; Wilpart, E.; Chesnier, MC.; Balkau, B.; et al. Adiponectin gene polymorphisms and adiponectin levels are independently associated with the development of hyperglycemia during a 3-year period: The epidemiologic data on the insulin resistance syndrome prospective study. Diabetes. 2004, 53, 1150–1157. [Google Scholar] [CrossRef] [PubMed]
- Ukkola, O.; Santaniemi, M.; Rankinen, T.; Leon, A.S.; Skinner, J.S.; Wilmore, J.H.; Rao, D.C.; Bergman, R.; Kesäniemi, Y.A.; Bouchard, C. Adiponectin polymorphisms, adiposity and insulin metabolism: HERITAGE family study and Oulu diabetic study. Ann. Med. 2005, 37, 141–150. [Google Scholar] [CrossRef] [PubMed]
- González-Sánchez, J.L.; Zabena, C.A.; Martínez-Larrad, M.T.; Fernández-Pérez, C.; Pérez-Barba, M.; Laakso, M.; Serrano-Ríos, M. An SNP in the adiponectin gene is associated with decreased serum adiponectin levels and risk for impaired glucose tolerance. Obes. Res. 2005, 13, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Nannipieri, M.; Posadas, R.; Bonotti, A.; Williams, K.; Gonzalez-Villalpando, C.; Stern, M.P.; Ferrannini, E. Polymorphism of the 3'-untranslated region of the leptin receptor gene, but not the adiponectin SNP45 polymorphism, predicts type 2 diabetes. Diabetes Care. 2006, 29, 2509–2511. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, P.E.; Govindarajalu, S.; Towers, W.; Schwanebeck, U.; Fischer, S.; Vasseur, F.; Bornstein, S.R.; Schulze, J. Haplotypes in the promoter region of the ADIPOQ gene are associated with increased diabetes risk in a German Caucasian population. Horm. Metab. Res. 2006, 38, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Gable, D.R.; Matin, J.; Whittall, R.; Cakmak, H.; Li, K.W.; Cooper, J.; Miller, G.J.; Humphries, S.E. HIFMECH investigators. Common adiponectin gene variants show different effects on risk of cardiovascular disease and type 2 diabetesin European subjects. Ann. Hum. Genet. 2007, 71, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Potapov, V.A.; Chistiakov, D.A.; Dubinina, A.; Shamkhalova, M.S.; Shestakova, M.V.; Nosikov, V.V. Adiponectin andadiponectin receptor gene variants in relation to type 2 diabetes and insulin resistance related phenotypes. Rev. Diabet. Stud. 2008, 5, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Szopa, M.; Malczewska-Malec, M.; Kiec-Wilk, B.; Skupien, J.; Wolkow, P.; Malecki, M.T.; Sieradzki, J. Variants of the adiponectin gene and type 2 diabetes in a Polish population. Acta Diabetol. 2009, 46, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Mohammadzadeh, G.; Zarghami, N. Associations between single nucleotide polymorphisms of the adiponectin gene, serum adiponectin levels and increased risk of type 2 diabetes mellitus in Iranian obese individuals. Scand. J. Clin. Lab. Investig. 2009, 69, 764–771. [Google Scholar] [CrossRef]
- Vendramini, M.F.; Pereira, A.C.; Ferreira, S.R.; Kasamatsu, T.S.; Moisés, R.S. Japanese Brazilian Diabetes Study Group. Association of genetic variants in the adiponectin encoding gene (ADIPOQ) with type 2 diabetes in Japanese Brazilians. J. Diabetes Complicat. 2010, 24, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Tabatabaei-Malazy, O.; Hasani-Ranjbar, S.; Amoli, M.M.; Heshmat, R.; Sajadi, M.; Derakhshan, R.; Amiri, P.; Namakchian, M.; Rezazadeh, E.; Tavakkoly-Bazzaz, J.; et al. Genderspecific differences in the association of adiponectin gene polymorphisms with body mass index. Rev. Diabet. Stud. 2010, 7, 241–246. [Google Scholar] [PubMed]
- Al-Daghri, N.M.; Al-Attas, O.S.; Alokail, M.S.; Alkharfy, K.M.; Hussain, T.; Yakout, S.; Vinodson, B.; Sabico, S. Adiponectin gene polymorphisms (T45G and G276T), adiponectin levels and risk formetabolic diseases in an Arab population. Gene 2012, 493, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Vionnet, N.; Hani, E.H.; Dupont, S.; Gallina, S.; Francke, S.; Dotte, S.; de Matos, F.; Durand, E.; Leprêtre, F.; Lecoeur, C.; et al. Genomewide search for type 2 diabetes-susceptibility genes in French whites: Evidence for a novel susceptibility locus for early-onset diabetes on chromosome 3q27-qter and independent replication of a type 2-diabetes locus on chromosome 1q21–q24. Am. J. Genet. 2000, 67, 1470–1480. [Google Scholar] [CrossRef]
- Mori, Y.; Otabe, S.; Dina, C.; Yasuda, K.; Populaire, C.; Lecoeur, C.; Vatin, V.; Durand, E.; Hara, K.; Okada, T.; et al. Genome-wide search for type 2 diabetes in Japanese affected sib-pairs confirms susceptibility genes on 3q, 15q, and 20q and identifies two new candidate Loci on 7p and 11p. Diabetes 2002, 51, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Kissebah, A.H.; Sonnenberg, G.E.; Myklebust, J.; Goldstein, M.; Broman, K.; James, R.G.; Marks, J.A.; Krakower, G.R.; Jacob, H.J.; Weber, J.; et al. Quantitative trait loci on chromosomes 3 and 17 influence phenotypes of the metabolic syndrome. Proc. Natl. Acad. Sci. USA 2000, 97, 14478–14483. [Google Scholar] [CrossRef] [PubMed]
- Borges, A.P.; Guidoni, C.M.; Freitas, O.D.; Pereira, L.R. Economic evaluation of outpatients with type 2 diabetes mellitus assisted by a pharmaceutical care service. Arg. Bras. Endocrinol. Metabol. 2011, 55, 686–691. [Google Scholar] [CrossRef]
- Lin, Y.; Sun, Z. Current views on type 2 diabetes. J. Endocrinol. 2010, 204, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gong, M.; Long, J.; Liu, Q.; Deng, H.C. Association of the ADIPOQ rs17360539 and rs266729 polymorphisms with type 2 diabetes: A meta-analysis. Mol. Cell. Endocrinol. 2010, 325, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Han, L.Y.; Wu, Q.H.; Jiao, M.L.; Kumar, S.; Aggarwal, A.; Rao, V.R.; Sachdeva, M.P. Associations between single-nucleotide polymorphisms (+45T>G, +276G>T, −11377C>G, −11391G>A) of adiponectin gene and type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetologia 2011, 54, 2303–2314. [Google Scholar] [CrossRef] [PubMed]
- Menzaghi, C.; Trischitta, V.; Doria, A. Genetic influences of adiponectin on insulin resistance, type 2 diabetes, and cardiovascular disease. Diabetes 2007, 56, 1198–1209. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, X.; Shi, L.; Yang, M.; Yang, Y.; Tao, W.; Shi, L.; Xiong, Y.; Zhang, Y.; Yao, Y. Association of adiponectin SNP+45 and SNP+276 with type 2 diabetes in Han Chinese populations: A meta-Analysis of 26 case-control studies. PLoS One 2011, 6, e19686. [Google Scholar] [CrossRef] [PubMed]
- Thompson, S.G. Why sources of heterogeneity in meta-analysis should be investigated. BMJ 1994, 309, 1351–1355. [Google Scholar] [CrossRef] [PubMed]
- Munafò, M.R.; Flint, J. Meta-analysis of genetic association studies. Trends Genet. 2004, 20, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Nair, M. Diabetes mellitus, part 1: Physiology and complications. Br. J. Nurs. 2007, 16, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Liao, N.; Xie, Z.K.; Huang, J.; Xie, Z.F. Association between the ghrelin Leu72Met polymorphism and type 2 diabetes risk: A meta-analysis. Gene 2013, 517, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Kadowaki, T.; Yamauchi, T.; Kubota, N.; Hara, K.; Ueki, K.; Tobe, K. Adiponectin and adiponectin receptors in insulin resistance, diabetes, and the metabolic syndrome. J. Clin. Investig. 2006, 116, 1784–1792. [Google Scholar] [CrossRef] [PubMed]
- Xita, N.; Tsatsoulis, A. Adiponectin in diabetes mellitus. Curr. Med. Chem. 2012, 19, 5451–5458. [Google Scholar] [CrossRef] [PubMed]
- Heidemann, C.; Sun, Q.; van Dam, R.M.; Meigs, J.B.; Zhang, C.; Tworoger, S.S.; Mantzoros, C.; Hu, F.B. Total and high-molecular-weight adiponectin and resistin in relation to the risk for type 2 diabetes in women. Ann. Intern. Med. 2008, 149, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Von Eynatten, M.; Humpert, P.M.; Bluemm, A.; Lepper, P.M.; Hamann, A.; Allolio, B.; Nawroth, P.P.; Bierhaus, A.; Dugi, K.A. High-molecular weight adiponectin is independently associated with the extent of coronary artery disease in men. Atherosclerosis 2008, 199, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Seino, Y.; Hirose, H.; Saito, I.; Itoh, H. High-molecular-weight adiponectin is a predictor of progression to metabolic syndrome: A population-based 6-year follow-up study in Japanese men. Metabolism 2009, 58, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Fasshauer, M.; Klein, J.; Neumann, S.; Eszlinger, M.; Paschke, R. Hormonal regulation of adiponectin gene expression in 3T3-L1 adipocytes. Biochem. Biophys. Res. Commun. 2002, 290, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Koerner, A.; Kratzsch, J.; Kiess, W. Adipocytokines: Leptin—the classical, resistin—the controversical, adiponectin—the promising, and more to come. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 525–546. [Google Scholar] [CrossRef] [PubMed]
- Cochran, W.G. The effectiveness of adjustment by subclassification in removing bias in observational studies. Biometrics 1968, 24, 295–313. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, Y.; Wang, K.; Xu, S.; Chen, G.; Di, H.; Cao, M.; Liu, C. Association between ADIPOQ +45T>G Polymorphism and Type 2 Diabetes: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2015, 16, 704-723. https://doi.org/10.3390/ijms16010704
Fan Y, Wang K, Xu S, Chen G, Di H, Cao M, Liu C. Association between ADIPOQ +45T>G Polymorphism and Type 2 Diabetes: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2015; 16(1):704-723. https://doi.org/10.3390/ijms16010704
Chicago/Turabian StyleFan, Yaofu, Kun Wang, Shuhang Xu, Guofang Chen, Hongjie Di, Meng Cao, and Chao Liu. 2015. "Association between ADIPOQ +45T>G Polymorphism and Type 2 Diabetes: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 16, no. 1: 704-723. https://doi.org/10.3390/ijms16010704