
Cytidine 5′-Diphosphocholine (Citicoline) in Glaucoma: Rationale of Its Use, Current Evidence and Future Perspectives

 , , ,
, , , 
Abstract
:
1. Introduction
Cytidine 5′-Diphosphocholine (Citicoline): Mechanism of Action

2. Evidence on the Effects of Citicoline in Ocular and Non-Ocular Neurological Conditions
2.1. Citicoline and Brain Ischemia
2.2. Citicoline and Alzheimer’s Disease (AD)
2.3. Citicoline and Parkinson’s Disease (PD)
2.4. Citicoline in Amblyopia and Non-Arteritic Ischaemic Optic Neuropathy
3. Glaucoma as a Central Nervous System (CNS) Disease
4. Glaucoma Physiopathology and Neuroprotection
5. Role of Citicoline in Glaucoma: Current Evidence
5.1. Experimental Studies on Citicoline as a Neuroprotectant

{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Study Design | Animal | Citicoline Concentration | Citicoline Administration | Outcomes |
|---|---|---|---|---|---|---|
| Rejdak R et al. [62] | 2002 | case-control | Albino rabbits | 50 mg/kg/twice day | Intraperitoneal injection | Retinal catecholamine levels |
| Park CH et al. [65] | 2005 | case-control | Spraue-Dawley rats | 50 mg·kg−1 | Intraperitoneal injection | Thickness of retinal layers and expression of ChAT and TH |
| Schuettauf F et al. [64] | 2006 | case-control | Rats | 1 g/kg/daily and 300 mg/kg/daily | Intraperitomeal injection | Retinal ganglion cells density and expression of the antiapoptotic protein Bcl-2 |
| Oshitari T et al. [63]. | 2010 | case-control | Cultures from Spraue-Dawley rats | 1 μM | Added to high glucose medium in retinal culture | Apoptosis evaluation by TUNEL assay and Caspase-3 and Caspase-9 activity |
| Matteucci A et al. [66]. | 2014 | case-control | Cultures from embryonic rat retina | 10, 100 and 1000 μM | Treated for 96 h and 24 h before glutamate-induced excitotoxic insult and high glucose-promoted neuronal cell damage | Apoptosis evaluation by TUNEL assay and caspase activation |
5.2. Clinical Studies

| Authors | Year | Study Design | Study Population | Adm | Dosage | Schedule of Treatment | Follow-up | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Pecori Giraldi et al. [69] | 1989 | cohort | Open Angle Glaucoma (OAG) | IM | 1 g/day | 10 days | 3 months | Reduction in the scotomatous area (computerized central perimetry) and decrease in mean defect (automated perimetry) |
| Parisi V et al. [71] | 1999 | case-control | OAG −3 dB > Mean Deviation (MD) < −6 dB | IM | 1 g/day | 60 days 120 days of washout (2 cycles) | 360 days | Visual Evoked Potential (VEP) and Pattern Electroretinogram (PERG) parameters |
| Virno M et al. [70] | 2000 | case-control | OAG | IM | 1 g/day | 15 days 180 days of washout (20 cycles) | 10 years | Visual field worsening (increase of non-perception area >500 mm2) |
| Rejdak et al. [73] | 2003 | cohort | OAG | Oral | 1 g/day | 14 days 2 days of washout (2 cycles) | 56 days | VEP parameters |
| Parisi V [72] | 2005 | case-control | OAG −3 dB > MD < −6 dB | IM | 1 g/day | 60 days 120 days of washout (14 cycles) | 8 years | VEP and PERG parameters |
| Parisi V et al. [74] | 2008 | case-control | OAG −2 dB > MD < −14 dB | IM Oral | 1 g/day 1600 mg/day | 60 days 120 days of washout (2 cycles) | 360 days | VEP and PERG parameters |
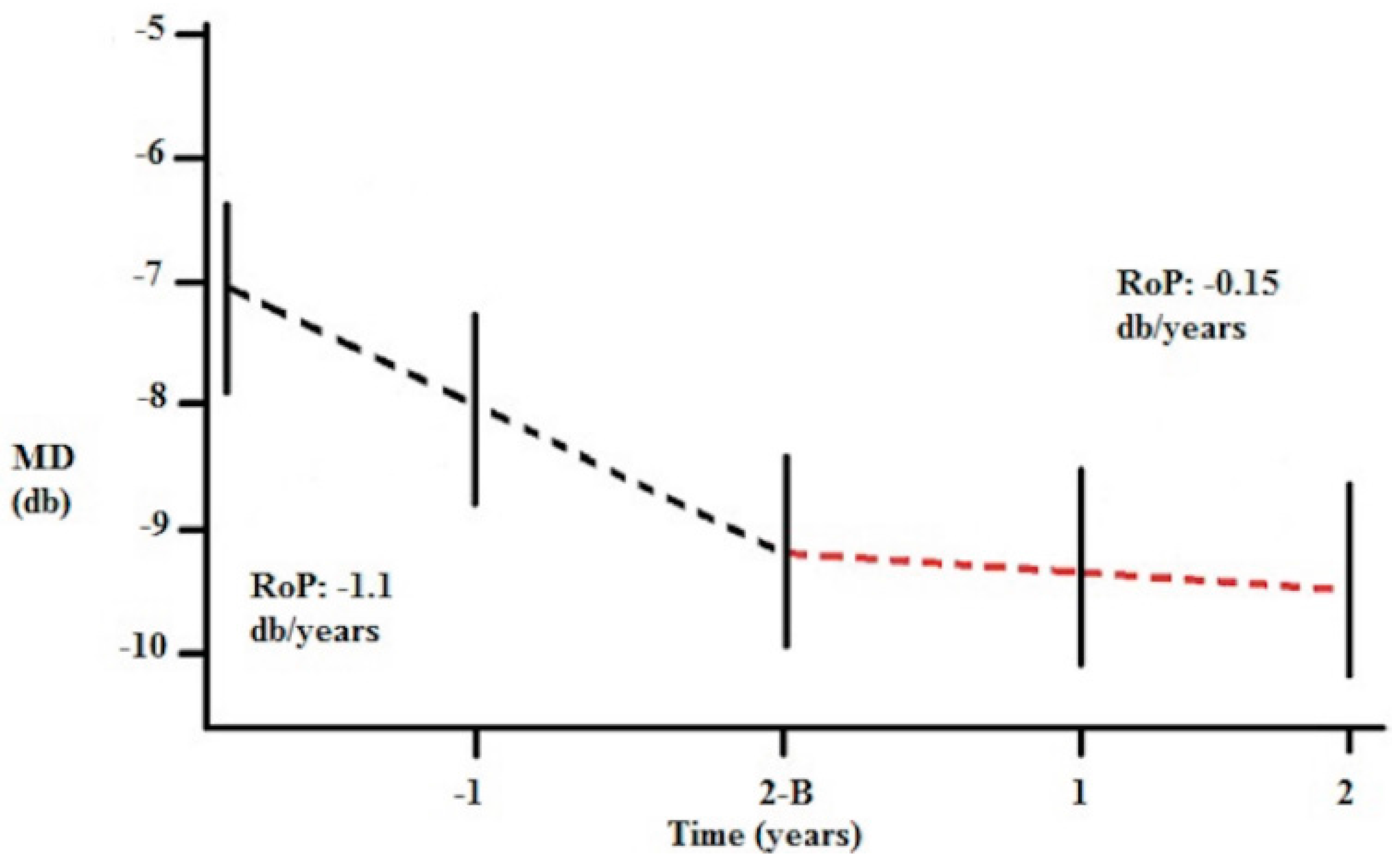
| Ottobelli L et al. [75] | 2013 | retrospective cohort | progressing OAG | Oral (solution) | 500 mg/day | 120 days 60 days of washout (4 cycles) | 2 years | Rate of visual field progression |
| Roberti et al. [78] | 2014 | experimental and clinical (case-control) | OAG −3 dB > MD < −12 dB | Topic (eye drops) | 3 drops/day | 60 days | 90 days | VEP and PERG parameters |
| Parisi V et al. [79] | 2015 | case-control | OAG MD > −10 dB | Topic (eye drops) | 3 drops/day | 120 days 60 days of washout | 180 days | VEP and PERG parameters |
5.3. Citicoline Eye Drops in Glaucoma
6. Comments and Future Perspectives
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- De la Morena, E.; Goldberg, D.M.; Werner, M. Citidín difosfato de colina y biosíntesis de fosfolípidos. In Citicolina: Bioquímica, Neurofarmacología y Clínica; De la Morena, E., Ed.; Salvat: Barcelona, Spain, 1985; pp. 25–38. [Google Scholar]
- Saver, J.L. Citicoline: Update on a promising and widely available agent for neuroprotection and neurorepair. Rev. Neurol. Dis. 2008, 5, 167–177. [Google Scholar] [PubMed]
- Fagone, P.; Jackowski, S. Phosphatidylcholine and the CDP-choline cycle. Biochim. Biophys. Acta 2013, 1831, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Secades, J.J. Citicoline: Pharmacological and clinical review, 2010 update. Rev. Neurol. 2011, 52, S1–S62. [Google Scholar] [PubMed]
- Rao, A.M.; Hatcher, J.F.; Dempsey, R.J. Does CDP-choline modulate phospholipase activities aftertransient forebrain ischemia? Brain Res. 2001, 893, 268–272. [Google Scholar] [CrossRef]
- Martinet, M.; Fonlupt, P.; Pacheco, H. Effects of cytidine-5′-diphosphocholine on norepinephrine, dopamine and serotonin synthesis in various regions of the rat brain. Arch. Int. Pharmacodyn. Ther. 1979, 239, 52–61. [Google Scholar] [PubMed]
- Skripuletz, T.; Manzel, A.; Gropengießer, K.; Schäfer, N.; Gudi, V.; Singh, V.; Salinas Tejedor, L.; Jörg, S.; Hammer, A.; Voss, E.; et al. Pivotal role of choline metabolites in remyelination. Brain 2015, 138, 398–413. [Google Scholar] [CrossRef] [PubMed]
- Schauss, A.G.; Somfai-Relle, S.; Financsek, I.; Glavits, R.; Parent, S.C.; Endres, J.R.; Varga, T.; Szücs, Z.; Clewell, A. Single- and repeated-dose oral toxicity studies of citicoline free-base (choline cytidine 5′-pyrophosphate) in Sprague-Dawley rats. Int. J. Toxicol. 2009, 28, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Lozano, F.R. Efficacy and safety of oral CDP-choline. Drug surveillance study in 2817 cases. Arzneimittelforschung 1983, 33, 1073–1080. [Google Scholar]
- Grieb, P. Neuroprotective properties of citicoline: Facts, doubts and unresolved issues. CNS Drugs 2014, 28, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Grieb, P.; Rejdak, R. Pharmacodynamics of citicoline relevant to the treatment of glaucoma. J. Neurosci. Res. 2002, 67, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Sabín, J.; Román, G.C. The role of citicoline in neuroprotection and neurorepair in ischemic stroke. Brain Sci. 2013, 3, 1395–1414. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Fernández, M.; Rodríguez-Frutos, B.; Fuentes, B.; Vallejo-Cremades, M.T.; Alvarez-Grech, J.; Expósito-Alcaide, M.; Díez-Tejedor, E. CDP-choline treatment induces brain plasticity markers expression in experimental animal stroke. Neurochem. Int. 2012, 60, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Dávalos, A.; Alvarez-Sabín, J.; Castillo, J.; Díez-Tejedor, E.; Ferro, J.; Martínez-Vila, E.; Serena, J.; Segura, T.; Cruz, V.T.; Masjuan, J.; et al. Citicoline in the treatment of acute ischaemic stroke: An international, randomised, multicentre, placebo-controlled study (ICTUS trial). Lancet 2012, 380, 349–357. [Google Scholar] [CrossRef]
- Overgaard, K. The effects of citicoline on acute ischemic stroke: A review. J. Stroke Cerebrovasc. Dis. 2014, 23, 1764–1769. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R.; Caamaño, J.; Gómez, M.J.; Fernández-Novoa, L.; Franco-Maside, A.; Alvarez, X.A. Therapeutic effects of CDP-choline in Alzheimer’s disease. Cognition, brain mapping, cerebrovascular hemodynamics, and immune factors. Ann. N. Y. Acad. Sci. 1996, 777, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, X.A.; Sampedro, C.; Lozano, R.; Cacabelos, R. Citicoline protects hippocampal neurons against apoptosis induced by brain beta-amyloid deposits plus cerebral hypoperfusion in rats. Methods Find Exp. Clin. Pharmacol. 1999, 21, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Sheng, W.; He, Y.; Cui, J.; Haidekker, M.A.; Sun, G.Y.; Lee, J.C.-M. Secretory phospholipase A2 type III enhances αsecretase-dependent amyloid precursor protein processing through alterations in membrane fluidity. J. Lipid Res. 2010, 51, 957–966. [Google Scholar] [CrossRef] [PubMed]
- Brender, J.R.; Lee, E.L.; Cavitt, M.A.; Gafni, A.; Steel, D.G.; Ramamoorthy, A. Amyloid fiber formation and membrane disruption are separate processes localized in two distinct regions of IAPP, the type-2-diabetes-related peptide. J. Am. Chem. Soc. 2008, 130, 6424–6429. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, X.A.; Mouzo, R.; Pichel, V.; Pérez, P.; Laredo, M.; Fernández-Novoa, L.; Corzo, L.; Zas, R.; Alcaraz, M.; Secades, J.J.; et al. Double-blind placebo-controlled study with citicoline in APOE genotyped Alzheimer’s disease patients. Effects on cognitive performance, brain bioelectrical activity and cerebral perfusion. Methods Find Exp. Clin. Pharmacol. 1999, 21, 633–644. [Google Scholar] [PubMed]
- Franco-Maside, A.; Caamaño, J.; Gómez, M.J.; Cacabelos, R. Brain mapping activity and mental performance after chronic treatment with CDP-choline in Alzheimer’s disease. Methods Find Exp. Clin. Pharmacol. 1994, 16, 597–607. [Google Scholar] [PubMed]
- Fioravanti, M.; Yanagi, M. Cytidinediphosphocholine (CDP-choline) for cognitive and behavioural disturbances associated with chronic cerebral disorders in the elderly. Cochrane Database Syst. Rev. 2005, 18, CD000269. [Google Scholar] [CrossRef]
- Agnoli, A.; Ruggieri, S.; Denaro, A.; Bruno, G. New strategies in the management of Parkinson’s disease: A biological approach using a phospholipid precursor (CDP-choline). Neuropsychobiology 1982, 8, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Saligaut, C.; Daoust, M.; Moore, N.; Boismare, F. Circling behaviour in rats with unilateral lesions of the nigrostriatum induced by 6-hydroxydopamine: Changes induced by oral administration of cytidine-5′-diphosphocholine. Neuropharmacology 1987, 26, 1315–1319. [Google Scholar] [CrossRef]
- Eberhardt, R.; Birbamer, G.; Gerstenbrand, F.; Rainer, E.; Traegner, H. Citicoline in the treatment of Parkinson’s disease. Clin. Ther. 1990, 12, 489–495. [Google Scholar] [PubMed]
- Campos, E.C.; Bolzani, R.; Schiavi, C.; Baldi, A.; Porciatti, V. Cytidin-5′-diphosphocholine enhances the effect of part-time occlusion in amblyopia. Doc. Ophthalmol. 1996–1997, 93, 247–263. [Google Scholar] [CrossRef]
- Fresina, M.; Dickmann, A.; Salerni, A.; de Gregorio, F.; Campos, E.C. Effect of oral CDP-choline on visual function in young amblyopic patients. Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Pawar, P.V.; Mumbare, S.S.; Patil, M.S.; Ramakrishnan, S. Effectiveness of the addition of citicoline to patching in the treatment of amblyopia around visual maturity: A randomized controlled trial. Indian J. Ophthalmol. 2014, 62, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Porciatti, V.; Schiavi, C.; Benedetti, P.; Baldi, A.; Campos, E.C. Cytidine-5′-diphosphocholine improves visual acuity, contrast sensitivity and visually-evoked potentials of amblyopic subjects. Curr. Eye Res. 1998, 17, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Parisi, V.; Coppola, G.; Ziccardi, L.; Gallinaro, G.; Falsini, B. Cytidine-5′-diphosphocholine (Citicoline): A pilot study in patients with non-arteritic ischaemic optic neuropathy. Eur. J. Neurol. 2008, 15, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2890. [Google Scholar] [CrossRef] [PubMed]
- Gordon, M.O.; Beiser, J.A.; Brandt, J.D.; Heuer, D.K.; Higginbotham, E.J.; Johnson, C.A.; Keltner, J.L.; Miller, J.P.; Parrish, R.K., 2nd; Wilson, M.R.; et al. The Ocular Hypertension Treatment Study: Baseline factors that predict the onset of primary open-angle glaucoma. Arch. Ophthalmol. 2002, 120, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Collaborative Normal-Tension Glaucoma Study Group. Comparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with therapeutically reduced intraocular pressures. Am. J. Ophthalmol. 1998, 126, 487–497. [Google Scholar]
- Heijl, A.; Leske, M.C.; Bengtsson, B.; Hyman, L.; Bengtsson, B.; Hussein, M.; Early Manifest Glaucoma Trial Group. Reduction of intraocular pressure and glaucoma progression: Results from the Early Manifest Glaucoma Trial. Arch. Ophthalmol. 2002, 120, 1268–1279. [Google Scholar] [CrossRef] [PubMed]
- Kass, M.A.; Heuer, D.K.; Higginbotham, E.J.; Johnson, C.A.; Keltner, J.L.; Miller, J.P.; Parrish, R.K., 2nd; Wilson, M.R.; Gordon, M.O. The Ocular Hypertension Treatment Study: A randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch. Ophthalmol. 2002, 120, 701–713. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Ophthalmology (AAO). Primary angle closure glaucoma. In Preferred Practice Patterns Guidelines; American Academy of Opthalmology: San Francisco, CA, USA, 2010. [Google Scholar]
- European Glaucoma Society. Terminology and Guidelines for Glaucoma, 4th ed.; Publicomm: Savona, Italy, 2014. [Google Scholar]
- Gupta, N.; Ang, L.C.; Noël de Tilly, L.; Bidaisee, L.; Yücel, Y.H. Human glaucoma and neural degeneration in intracranial optic nerve, lateral geniculate nucleus, and visual cortex. Br. J. Ophthalmol. 2006, 90, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Weber, A.J.; Chen, H.; Hubbard, W.C.; Kaufman, P.L. Experimental glaucoma and cell size, density, and number in the primate lateral geniculate nucleus. Investig. Ophthalmol. Vis. Sci. 2000, 41, 1370–1379. [Google Scholar]
- Yücel, Y.H.; Zhang, Q.; Weinreb, R.N.; Kaufman, P.L.; Gupta, N. Atrophy of relay neurons in magno- and parvocellular layers in the lateral geniculate nucleus in experimental glaucoma. Investig. Ophthalmol. Vis. Sci. 2001, 42, 3216–3222. [Google Scholar]
- Schumer, R.A.; Podos, S.M. The nerve of glaucoma! Arch. Ophthalmol. 1994, 112, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Buckingham, B.P.; Inman, D.M.; Lambert, W.; Oglesby, E.; Calkins, D.J.; Steele, M.R.; Vetter, M.L.; Marsh-Armstrong, N.; Horner, P.J. Progressive ganglion cell degeneration precedes neuronal loss in a mouse model of glaucoma. J. Neurosci. 2008, 28, 2735–2744. [Google Scholar] [CrossRef] [PubMed]
- Tamm, E.R.; Schmetterer, L.; Grehn, F. Status and perspectives of neuroprotective therapies in glaucoma: The European Glaucoma Society White Paper. Cell Tissue Res. 2013, 353, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Nickells, R.W. Retinal ganglion cell death in glaucoma: The how, the why, and the maybe. J. Glaucoma 1996, 5, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Corredor, R.G.; Goldberg, J.L. Electrical activity enhances neuronal survival and regeneration. J. Neural Eng. 2009, 6, 055001. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, R.N. Glaucoma neuroprotection: What is it? Why is it needed? Can. J. Ophthalmol. 2007, 42, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, R.N.; Levin, L.A. Is neuroprotection a viable therapy for glaucoma? Arch. Ophthalmol. 1999, 117, 1540–1544. [Google Scholar] [CrossRef] [PubMed]
- Rudzinski, M.; Wong, T.P.; Saragovi, H.U. Changes in retinal expression of neurotrophins and neurotrophin receptors induced by ocular hypertension. J. Neurobiol. 2004, 58, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Hayreh, S.S.; March, W.; Anderson, D.R. Pathogenesis of block of rapid orthograde axonal transport by elevated intraocular pressure. Exp. Eye Res. 1979, 28, 515–523. [Google Scholar] [CrossRef]
- Quigley, H.A.; McKinnon, S.J.; Zack, D.J.; Pease, M.E.; Kerrigan-Baumrind, L.A.; Kerrigan, D.F.; Mitchell, R.S. Retrograde axonal transport of BDNF in retinal ganglion cells is blocked by acute IOP elevation in rats. Investig. Ophthalmol. Vis. Sci. 2000, 41, 3460–3466. [Google Scholar]
- Colafrancesco, V.; Parisi, V.; Sposato, V.; Rossi, S.; Russo, M.A.; Coassin, M.; Lambiase, A.; Aloe, L. Ocular application of nerve growth factor protects degenerating retinal ganglion cells in a rat model of glaucoma. J. Glaucoma 2011, 20, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Pease, M.E.; Zack, D.J.; Berlinicke, C.; Bloom, K.; Cone, F.; Wang, Y.; Klein, R.L.; Hauswirth, W.W.; Quigley, H.A. Effect of CNTF on retinal ganglion cell survival in experimental glaucoma. Investig. Ophthalmol. Vis. Sci. 2009, 50, 2194–200. [Google Scholar] [CrossRef] [PubMed]
- Lipton, S.A.; Rosenberg, P.A. Excitatory amino acids as a final common pathway for neurologic disorders. N. Engl. J. Med. 1994, 330, 613–622. [Google Scholar] [PubMed]
- Guo, L.; Salt, T.E.; Maass, A.; Luong, V.; Moss, S.E.; Fitzke, F.W.; Cordeiro, M.F. Assessment of neuroprotective effects of glutamate modulation on glaucoma-related retinal ganglion cell apoptosis in vivo. Investig. Ophthalmol. Vis. Sci. 2006, 47, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Baltmr, A.; Duggan, J.; Nizari, S.; Salt, T.E.; Cordeiro, M.F. Neuroprotection in glaucoma—Is there a future role? Exp. Eye Res. 2010, 91, 554–566. [Google Scholar] [CrossRef] [PubMed]
- Cheung, W.; Guo, L.; Cordeiro, M.F. Neuroprotection in glaucoma: Drug-based approaches. Optom. Vis. Sci. 2008, 85, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Payne, A.J.; Kaja, S.; Sabates, N.R.; Koulen, P. Neuroprotection in eye disease: Developments in translational research. Mo Med. 2013, 110, 429–436. [Google Scholar] [PubMed]
- Prokai-Tatrai, K.; Xin, H.; Nguyen, V.; Szarka, S.; Blazics, B.; Prokai, L.; Koulen, P. 17β-Estradiol eye drops protect the retinal ganglion cell layer and preserve visual function in an in vivo model of glaucoma. Mol. Pharm. 2013, 10, 3253–3261. [Google Scholar] [CrossRef] [PubMed]
- Areosa, S.A.; Sherriff, F. Memantine for dementia. Cochrane Database Syst. Rev. 2003, 3, CD003154. [Google Scholar] [CrossRef] [PubMed]
- Bensimon, G.; Lacomblez, L.; Meininger, V. A controlled trial of riluzole in amyotrophic lateral sclerosis. ALS/Riluzole Study Group. N. Engl. J. Med. 1994, 330, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Rejdak, R.; Toczolowski, J.; Solski, J.; Duma, D.; Grieb, P. Citicoline treatment increases retinal dopamine content in rabbits. Ophthalmic Res. 2002, 34, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Oshitari, T.; Fujimoto, N.; Adachi-Usami, E. Citicoline has a protective effect on damaged retinal ganglion cells in mouse culture retina. Neuroreport 2002, 13, 2109–2111. [Google Scholar] [CrossRef] [PubMed]
- Schuettauf, F.; Rejdak, R.; Thaler, S.; Bolz, S.; Lehaci, C.; Mankowska, A.; Zarnowski, T.; Junemann, A.; Zagorski, Z.; Zrenner, E.; et al. Citicoline and lithium rescue retinal ganglion cells following partial optic nerve crush in the rat. Exp. Eye Res. 2006, 83, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Kim, Y.S.; Noh, H.S.; Cheon, E.W.; Yang, Y.A.; Yoo, J.M.; Choi, W.S.; Cho, G.J. Neuroprotective effect of citicoline against KA-induced neurotoxicity in the rat retina. Exp. Eye Res. 2005, 81, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Matteucci, A.; Varano, M.; Gaddini, L.; Mallozzi, C.; Villa, M.; Pricci, F.; Malchiodi-Abedi, F. Neuroprotective effects of citicoline in in vitro models of retinal neurodegeneration. Int. J. Mol. Sci. 2014, 15, 6286–6297. [Google Scholar] [CrossRef] [PubMed]
- Zerbini, G.; Bandello, F.; Lattanzio, R.; Gabellini, D.; Zucchiatti, I.; Spinello, A.; Capuano, V.; Preziosa, C.; Maestroni, S. In vivo evaluation of retinal and choroidal structure in a mouse model of long-lasting diabetes. Effect of topical treatment with citicoline. J. Ocul. Dis. Ther. 2015, 3, 1–8. [Google Scholar] [CrossRef]
- Oshitari, T.; Yoshida-Hata, N.; Yamamoto, S. Effect of neurotrophic factors on neuronal apoptosis and neurite regeneration in cultured rat retinas exposed to high glucose. Brain Res. 2010, 1346, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Pecori Giraldi, J.; Virno, M.; Covelli, G.; Grechi, G.; de Greforio, F. Therapeutic value of citicoline in the treatment of glaucoma (computerized and automated perimetric investigation). Int. Ophthalmol. 1989, 13, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Virno, M.; Pecori-Giraldi, J.; Liguori, A.; de Gregorio, F. The protective effect of Citicoline on the progression of the perimetric defects in glaucomatous patients (perimetric study with a 10-year follow up). Acta Ophthalmol. Scand. 2000, 232, 56–57. [Google Scholar] [CrossRef]
- Parisi, V.; Manni, G.; Colacino, G.; Bucci, M.G. Cytidine-5′-diphpsphocholine (citicoline) improves retinal and cortical responses in patients with glaucoma. Ophthalmology 1999, 106, 1126–1134. [Google Scholar] [CrossRef]
- Parisi, V. Electrophysiological assessment of glaucomatous visual dysfunction during treatment with cytidine-5′-diphosphocholine (citicoline): A study of 8 years of follow-up. Doc. Ophthalmol. 2005, 110, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Rejdak, R.; Toczolowski, J.; Krukowski, J.; Kaminski, M.; Rejdak, K.; Stelmasiak, Z.; Grieb, P. Oral citicoline treatment improves visual pathway function in glaucoma. Med. Sci. Monit. 2003, 9, PI24–PI28. [Google Scholar] [PubMed]
- Parisi, V.; Coppola, G.; Centofanti, M.; Oddone, F.; Angrisani, A.M.; Ziccardi, L.; Ricci, B.; Quaranta, L.; Manni, G. Evidence of the neuroprotective role of citicoline in glaucoma patients. Prog. Brain Res. 2008, 173, 541–554. [Google Scholar] [PubMed]
- Ottobelli, L.; Manni, G.L.; Centofanti, M.; Iester, M.; Allevena, F.; Rossetti, L. Citicoline oral solution in glaucoma: Is there a role in slowing disease progression? Ophthalmologica 2013, 29, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Roda, A.; Fini, A.; Grigolo, B.; Scapini, G. Routes of administration and serum levels of [Methyl-14C]-Cytidine Diphosphocholine. Curr. Ther. Res. 1983, 34, 1049–1053. [Google Scholar]
- Agut, J.; Font, E.; Sacrist, A.; Ortiz, J.A. Bioavailability of Methyl-14C CDP-Choline by Oral Route. Arzneimittelforschung 1983, 33, 1045–1047. [Google Scholar] [PubMed]
- Roberti, G.; Tanga, L.; Parisi, V.; Sampalmieri, M.; Centofanti, M.; Manni, G. A preliminary study of the neuroprotective role of Citicoline eye drops in glaucomatous optic neuropathy. Indian J. Ophthalmol. 2014, 62, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Parisi, V.; Centofanti, M.; Ziccardi, L.; Tanga, L.; Michelessi, M.; Roberti, G.; Manni, G. Treatment with Citicoline eye drops enhances retinal function and neural conduction along the visual pathways in open angle glaucoma. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 1327–1340. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.E.; Goldberg, J.L. Glaucoma 2.0: Neuroprotection, neuroregeneration, neuroenhancement. Ophthalmology 2012, 119, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.L. The optic nerve. In Adler’s Physiology of the Eye, 11th ed.; Levin, L.A., Nilsson, S.F., Ver Hoeve, J., Wu, S., Kaufman, P.L., Alm, A., Eds.; Saunders/Elsevier: New York, NY, USA, 2011. [Google Scholar]
- Fredette, M.J.; Anderson, D.R.; Porciatti, V.; Feuer, W. Reproducibility of pattern electroretinogram in glaucoma patients with a range of severity of disease with the new glaucoma paradigm. Ophthalmology 2008, 115, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Quigley, H.A. Clinical trials for glaucoma neuroprotection are not impossible. Curr. Opin. Ophthalmol. 2012, 23, 144–154. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roberti, G.; Tanga, L.; Michelessi, M.; Quaranta, L.; Parisi, V.; Manni, G.; Oddone, F. Cytidine 5′-Diphosphocholine (Citicoline) in Glaucoma: Rationale of Its Use, Current Evidence and Future Perspectives. Int. J. Mol. Sci. 2015, 16, 28401-28417. https://doi.org/10.3390/ijms161226099
Roberti G, Tanga L, Michelessi M, Quaranta L, Parisi V, Manni G, Oddone F. Cytidine 5′-Diphosphocholine (Citicoline) in Glaucoma: Rationale of Its Use, Current Evidence and Future Perspectives. International Journal of Molecular Sciences. 2015; 16(12):28401-28417. https://doi.org/10.3390/ijms161226099
Chicago/Turabian StyleRoberti, Gloria, Lucia Tanga, Manuele Michelessi, Luciano Quaranta, Vincenzo Parisi, Gianluca Manni, and Francesco Oddone. 2015. "Cytidine 5′-Diphosphocholine (Citicoline) in Glaucoma: Rationale of Its Use, Current Evidence and Future Perspectives" International Journal of Molecular Sciences 16, no. 12: 28401-28417. https://doi.org/10.3390/ijms161226099