
Expression and Diagnostic Value of HE4 in Pancreatic Adenocarcinoma

Abstract
:1. Introduction
2. Result
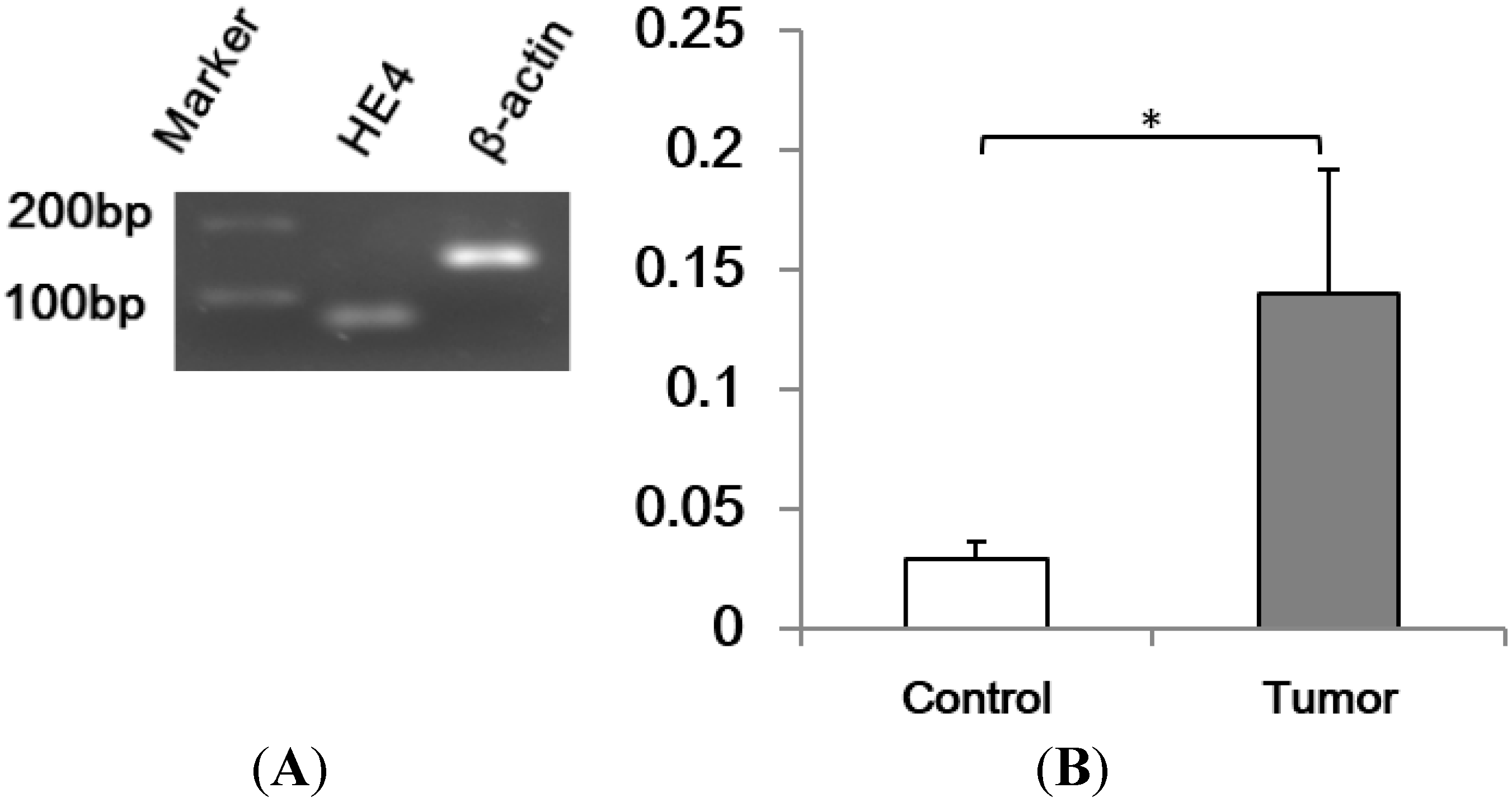
2.1. Human Epididymis Protein 4 (HE4) mRNA Level Increased in Pancreatic Adenocarcinoma

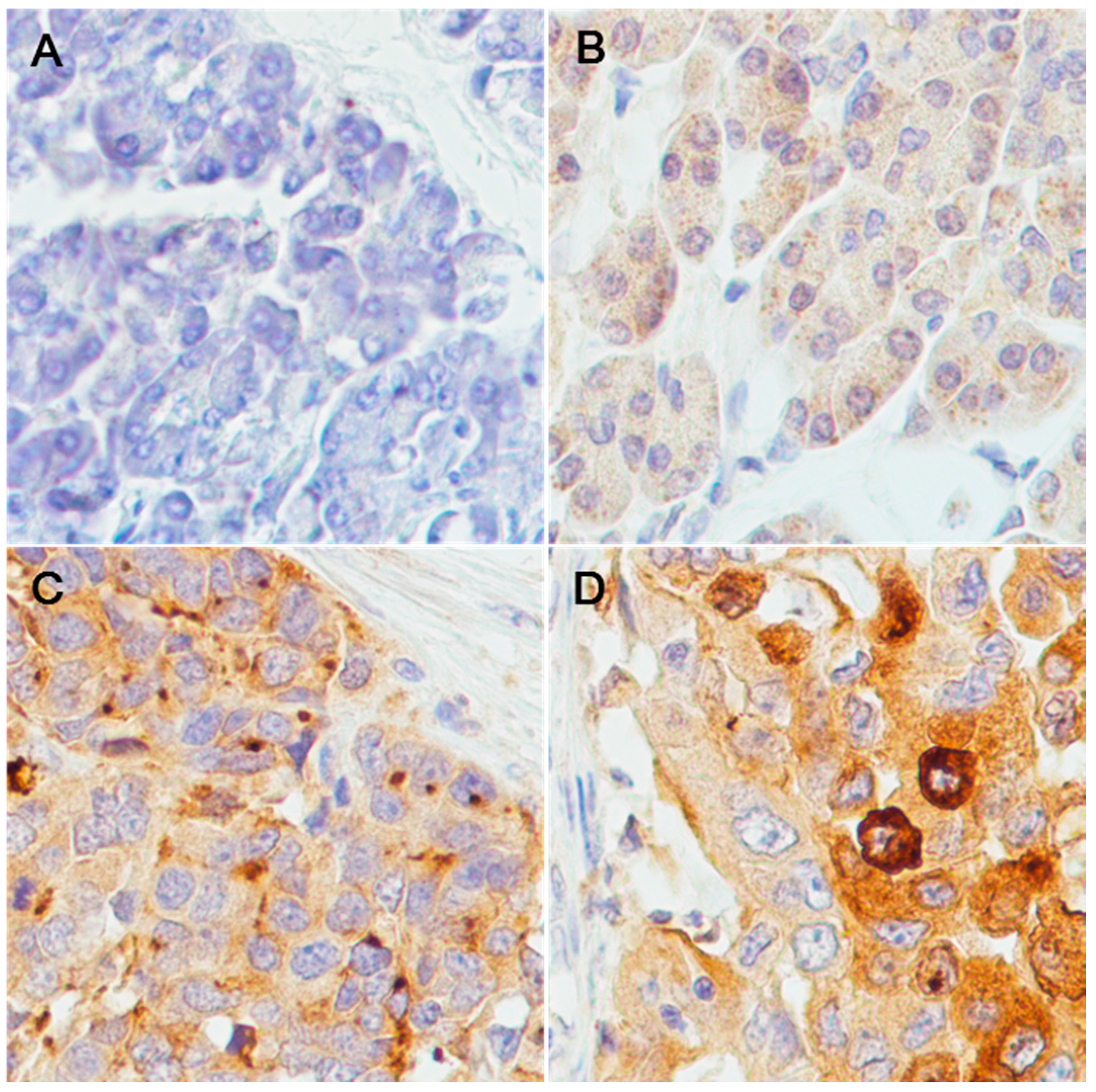
2.2. Over-Expression of HE4 Protein in Pancreatic Adenocarcinoma Tissues

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis | − | + | ++ | +++ | Total |
|---|---|---|---|---|---|
| Normal | 4 | 6 | 0 | 0 | 10 |
| Tumor | 6 | 20 | 17 | 10 | 53 |
| Adjacent | 4 | 6 | 0 | 0 | 10 |
| Total | 14 | 32 | 17 | 10 | 73 |

| Level | − | + | ++ | +++ | Total | Correlation | |
|---|---|---|---|---|---|---|---|
| Stage | I | 1 | 3 | 5 | 5 | 14 | |
| II | 2 | 13 | 7 | 5 | 28 | ||
| III | 3 | 5 | 2 | 0 | 10 | ||
| IV | 0 | 0 | 2 | 0 | 2 | ||
| total | 6 | 21 | 16 | 10 | 53 | r = −0.31, p = 0.02 | |
| Grade | 1 | 2 | 1 | 2 | 0 | 5 | |
| 2 | 0 | 10 | 9 | 3 | 22 | ||
| 3 | 4 | 9 | 6 | 7 | 26 | ||
| total | 6 | 20 | 17 | 10 | 53 | r = 0.08, p = 0.59 | |
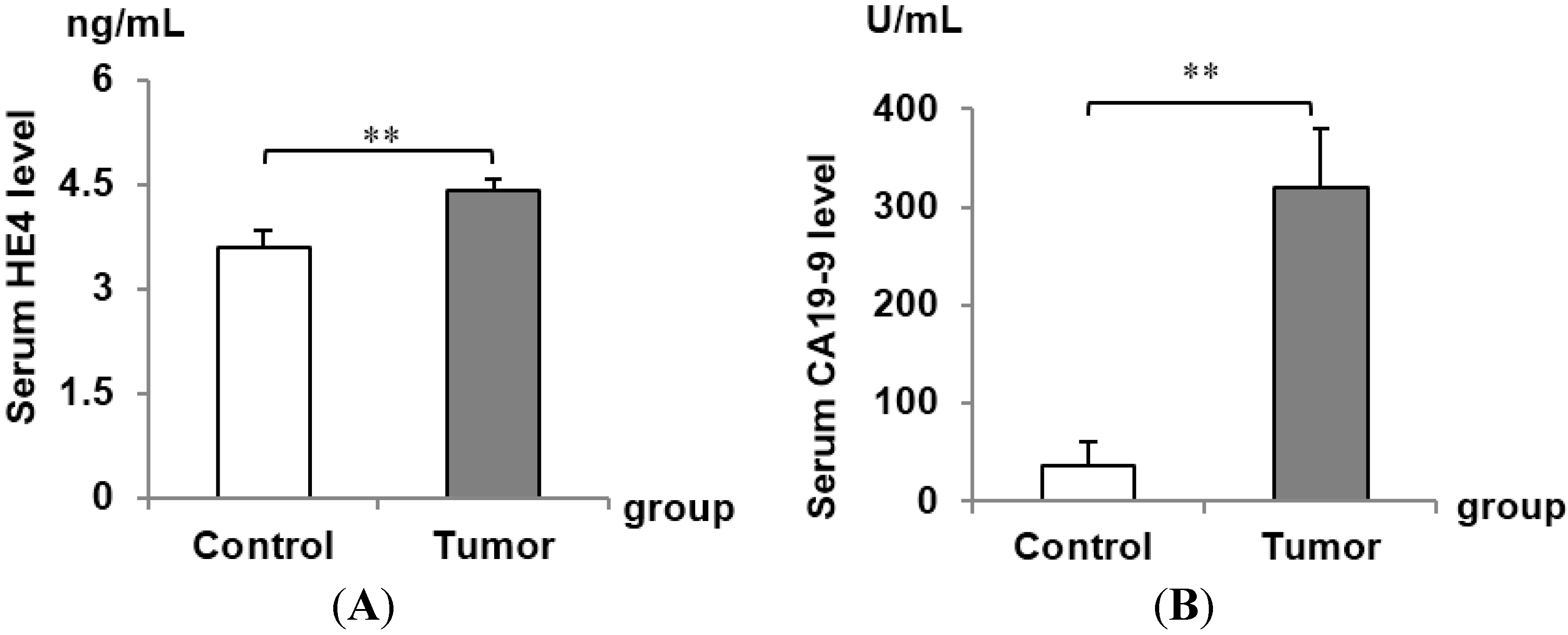
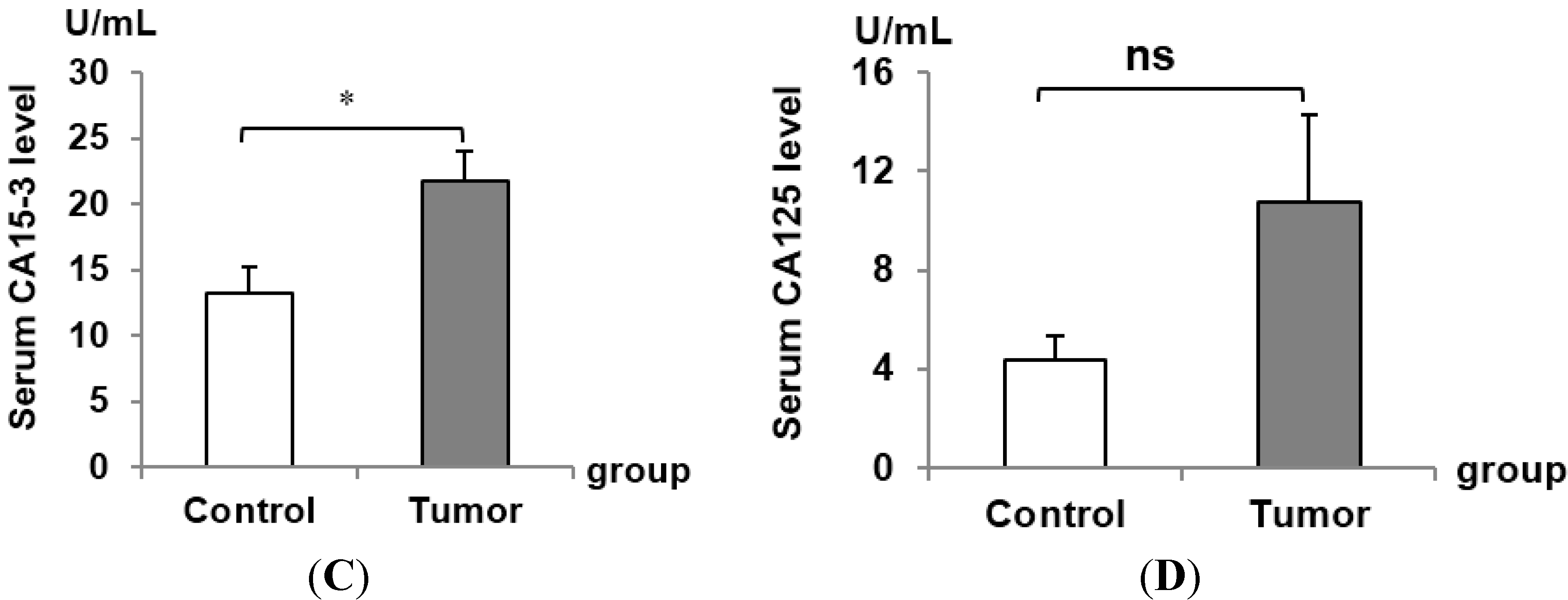
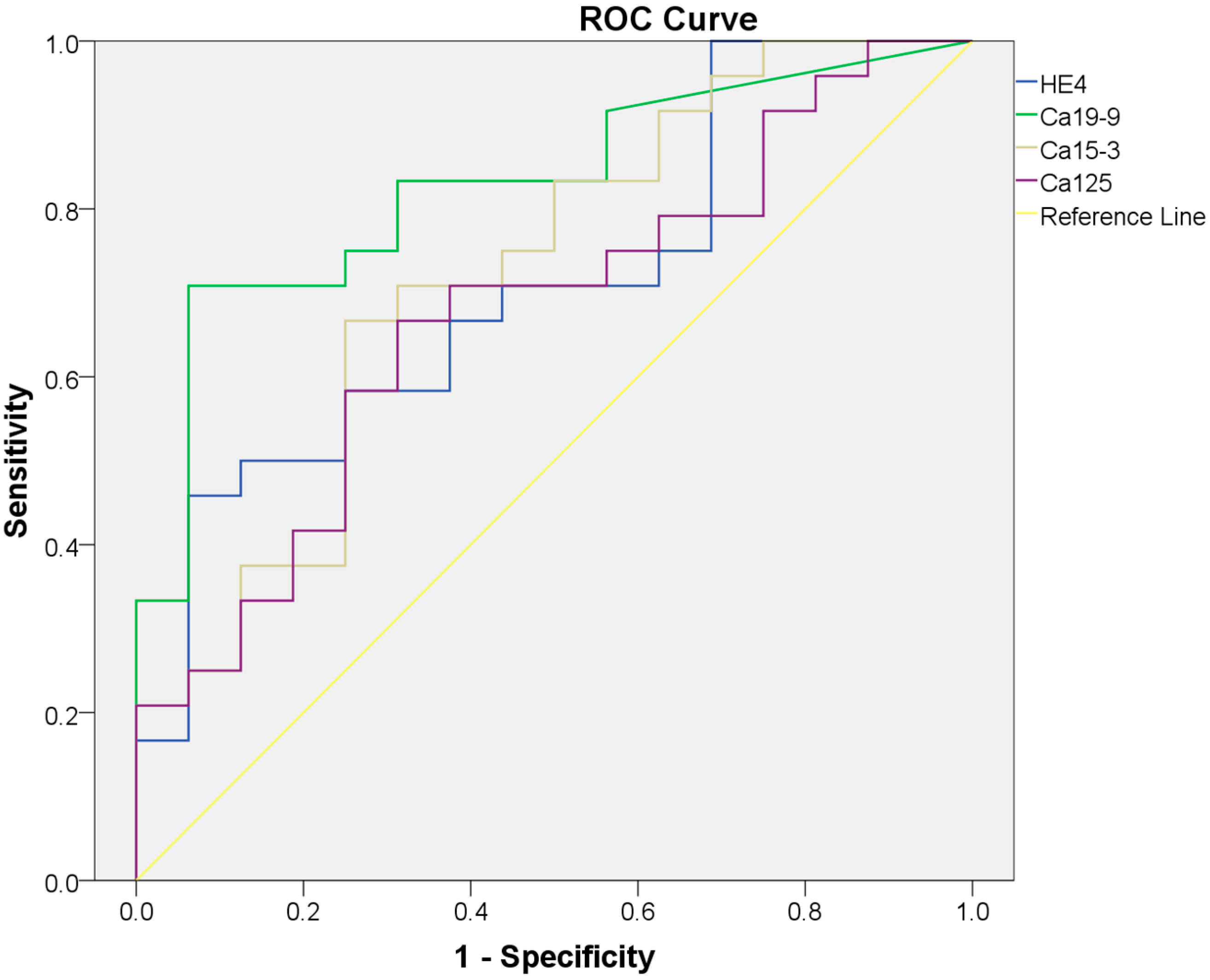
2.3. Serum HE4 Is a Potential Biomarker for Pancreatic Adenocarcinoma Alone or in Combination with Classical Pancreatic Adenocarcinoma Biomarkers



| Marker | AUC | 95% CI | Cutoff | Sensitivity | Specificity |
|---|---|---|---|---|---|
| HE4 | 0.71 | 0.55–0.87 | 4.59 | 45.83% | 93.75% |
| CA19-9 | 0.83 | 0.70–0.96 | 62.85 | 70.83% | 93.75% |
| CA15-3 | 0.72 | 0.56–0.89 | 18.08 | 66.67% | 75.00% |
| CA125 | 0.67 | 0.51–0.84 | 4.52 | 66.67% | 68.75% |
| Marker | CA199 | CA153 | CA125 |
|---|---|---|---|
| HE4 | r = 0.095, p = 0.785 | r = −0.365, p = 0.079 | r = 0.123, p = 0.568 |
| CA199 | r = −0.230, p = 0.280 | r = −0.239, p = 0.260 | |
| CA153 | r = 0.217, p = 0.308 |
| Marker | Detectable Status | Patient | Normal | Sensitivity | Specificity | Accuracy |
|---|---|---|---|---|---|---|
| HE4 | + | 11 | 1 | 45.83% | 93.75% | 65% |
| − | 13 | 15 | ||||
| CA19-9 | + | 17 | 1 | 70.83% | 93.75% | 80% |
| − | 7 | 15 | ||||
| CA15-3 | + | 16 | 4 | 66.67% | 75% | 70% |
| − | 8 | 12 | ||||
| CA125 | + | 16 | 5 | 66.67% | 68.75% | 67.5% |
| − | 8 | 11 | ||||
| HE4/CA19-9 | + | 20 | 2 | 83.33% | 87.5% | 85% |
| − | 4 | 14 | ||||
| HE4/CA15-3 | + | 21 | 4 | 87.5% | 75% | 82.5% |
| − | 3 | 12 | ||||
| HE4/CA125 | + | 19 | 5 | 79.17% | 68.75% | 75% |
| − | 5 | 11 |
3. Discussion
4. Experimental Section
4.1. Patients and Tissue Samples
4.2. Quantitative RT-PCR
4.3. Immunohistochemistry
4.4. ELISA
4.5. Statistical Analyses
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Seufferlein, T.; Bachet, J.B.; van Cutsem, E.; Rougier, P. Pancreatic adenocarcinoma: ESMO–ESDO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2012, 23, vii33–vii40. [Google Scholar] [CrossRef] [PubMed]
- Elebro, J.; Heby, M.; Gaber, A.; Nodin, B.; Jonsson, L.; Fristedt, R.; Uhlen, M.; Jirstrom, K.; Eberhard, J. Prognostic and treatment predictive significance of SATB1 and SATB2 expression in pancreatic and periampullary adenocarcinoma. J. Transl. Med. 2014, 12, 289. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.T.; Tao, H.Q.; Zou, S.C. Detection of serum tumor markers in the diagnosis and treatment of patients with pancreatic cancer. Hepatobiliary Pancreat. Dis. Int. 2004, 3, 464–468. [Google Scholar] [PubMed]
- Nakai, Y.; Isayama, H.; Sasaki, T.; Takahara, N.; Hamada, T.; Uchino, R.; Mizuno, S.; Miyabayashi, K.; Yamamoto, K.; Mohri, D.; et al. A retrospective analysis of early CA199 change in salvage chemotherapy for refractory pancreatic cancer. Cancer Chemother. Pharmacol. 2013, 72, 1291–1297. [Google Scholar] [CrossRef]
- Liu, L.; Xu, H.; Wang, W.; Wu, C.; Chen, Y.; Yang, J.; Cen, P.; Xu, J.; Liu, C.; Long, J.; et al. A Preoperative serum signature of CEA/CA125/CA19-9 ≥ 1000 U/mL indicates poor outcome to pancreatectomy for pancreatic cancer. Int. J. Cancer 2014. [Google Scholar] [CrossRef]
- Lee, K.J.; Yi, S.W.; Chung, M.J.; Park, S.W.; Song, S.Y.; Chung, J.B.; Park, J.Y. Serum CA19-9 and CEA levels as a prognostic factor in pancreatic adenocarcinoma. Yonsei Med. J. 2013, 54, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.; Chiu, D.; Qin, D.; Niu, L.; Cai, J.; He, L.; Huang, W.; Xu, K. The efficacy evaluation of cryosurgery in pancreatic cancer patients with the expression of CD44v6, integrin-β1, CA199, and CEA. Mol. Biotechnol. 2012, 52, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Gold, D.V.; Modrak, D.E.; Ying, Z.; Cardillo, T.M.; Sharkey, R.M.; Goldenberg, D.M. New MUC1 serum immunoassay differentiates pancreatic cancer from pancreatitis. J. Clin. Oncol. 2006, 24, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yi, C.; Wen, Y.; Radhakrishnan, P.; Tremayne, J.R.; Dao, T.; Johnson, K.R.; Hollingsworth, M.A. Interactions between MUC1 and p120 catenin regulate dynamic features of cell adhesion, motility, and metastasis. Cancer Res. 2014, 74, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Drapkin, R.; von Horsten, H.H.; Lin, Y.; Mok, S.C.; Crum, C.P.; Welch, W.R.; Hecht, J.L. Human epididymis protein 4 (HE4) is a secreted glycoprotein that is overexpressed by serous and endometrioid ovarian carcinomas. Cancer Res. 2005, 65, 2162–2169. [Google Scholar] [CrossRef] [PubMed]
- LeBleu, V.S.; Teng, Y.; O’Connell, J.T.; Charytan, D.; Muller, G.A.; Muller, C.A.; Sugimoto, H.; Kalluri, R. Identification of human epididymis protein-4 as a fibroblast-derived mediator of fibrosis. Nat. Med. 2013, 19, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Nozaki, K.; Ogawa, M.; Williams, J.A.; Lafleur, B.J.; Ng, V.; Drapkin, R.I.; Mills, J.C.; Konieczny, S.F.; Nomura, S.; Goldenring, J.R.; et al. A molecular signature of gastric metaplasia arising in response to acute parietal cell loss. Gastroenterology 2008, 134, 511–522. [Google Scholar] [CrossRef]
- Hough, C.D.; Sherman-Baust, C.A.; Pizer, E.S.; Montz, F.J.; Im, D.D.; Rosenshein, N.B.; Cho, K.R.; Riggins, G.J.; Morin, P.J. Large-scale serial analysis of gene expression reveals genes differentially expressed in ovarian cancer. Cancer Res. 2000, 60, 6281–6287. [Google Scholar] [PubMed]
- Nagy, B.; Bhattoa, H.P.; Steiber, Z.; Csoban, M.; Szilasi, M.; Mehes, G.; Muller, M.; Lazar, J.; Kappelmayer, J.; Antal-Szalmas, P.; et al. Serum human epididymis protein 4 (HE4) as a tumor marker in men with lung cancer. Clin. Chem. Lab. Med. 2014, 52, 1639–1648. [Google Scholar] [CrossRef]
- Mutz-Dehbalaie, I.; Egle, D.; Fessler, S.; Hubalek, M.; Fiegl, H.; Marth, C.; Widschwendter, A. HE4 is an independent prognostic marker in endometrial cancer patients. Gynecol. Oncol. 2012, 126, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Urban, N. Designing early detection programs for ovarian cancer. Ann. Oncol. 2011, 22, viii6–viii18. [Google Scholar] [CrossRef] [PubMed]
- Granato, T.; Midulla, C.; Longo, F.; Colaprisca, B.; Frati, L.; Anastasi, E. Role of HE4, CA72.4, and CA125 in monitoring ovarian cancer. Tumour Biol. 2012, 33, 1335–1339. [Google Scholar] [CrossRef] [PubMed]
- Midulla, C.; Manganaro, L.; Longo, F.; Viggiani, V.; Frati, L.; Granato, T.; Anastasi, E. HE4 combined with MDCT imaging is a good marker in the evaluation of disease extension in advanced epithelial ovarian carcinoma. Tumour Biol. 2012, 33, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Anastasi, E.; Porpora, M.G.; Pecorella, I.; Bernardo, S.; Frati, L.; Benedetti Panici, P.; Manganaro, L. May increased CA125 in borderline ovarian tumor be indicative of a poor prognosis? A case report. Tumour Biol. 2014, 35, 6969–6971. [Google Scholar] [CrossRef] [PubMed]
- Saarelainen, S.K.; Peltonen, N.; Lehtimaki, T.; Perheentupa, A.; Vuento, M.H.; Maenpaa, J.U. Predictive value of serum human epididymis protein 4 and cancer antigen 125 concentrations in endometrial carcinoma. Am. J. Obstet. Gynecol. 2013, 209, 142. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Fan, Y.; Wang, J.; Wang, H.; Liu, W. Evaluating the expression and diagnostic value of human epididymis protein 4 (HE4) in small cell lung cancer. Tumour Biol. 2014, 35, 6847–6853. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, H.; Hu, Z.; Tan, M.; Zhu, L.; Liu, J.; Liu, D.; Yan, L.; Lin, B. Overexpression of Lewis y antigen promotes human epididymis protein 4-mediated invasion and metastasis of ovarian cancer cells. Biochimie 2014, 105, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Lu, R.; Sun, X.; Xiao, R.; Zhou, L.; Gao, X.; Guo, L. Human epididymis protein 4 (HE4) plays a key role in ovarian cancer cell adhesion and motility. Biochem. Biophys. Res. Commun. 2012, 419, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, H.; Mariani, A.; Chen, D.; Klatt, E.; Podratz, K.; Drapkin, R.; Broaddus, R.; Dowdy, S.; Jiang, S.W.; et al. HE4 (WFDC2) promotes tumor growth in endometrial cancer cell lines. Int. J. Mol. Sci. 2013, 14, 6026–6043. [Google Scholar] [CrossRef]
- O’Neal, R.L.; Nam, K.T.; LaFleur, B.J.; Barlow, B.; Nozaki, K.; Lee, H.J.; Kim, W.H.; Yang, H.K.; Shi, C.; Maitra, A.; et al. Human epididymis protein 4 is up-regulated in gastric and pancreatic adenocarcinomas. Hum. Pathol. 2013, 44, 734–742. [Google Scholar] [CrossRef] [PubMed]
- Galgano, M.T.; Hampton, G.M.; Frierson, H.F., Jr. Comprehensive analysis of HE4 expression in normal and malignant human tissues. Mod. Pathol. 2006, 19, 847–853. [Google Scholar] [PubMed]
- Faca, V.M.; Song, K.S.; Wang, H.; Zhang, Q.; Krasnoselsky, A.L.; Newcomb, L.F.; Plentz, R.R.; Gurumurthy, S.; Redston, M.S.; Pitteri, S.J.; et al. A mouse to human search for plasma proteome changes associated with pancreatic tumor development. PLoS Med. 2008, 5, e123. [Google Scholar] [CrossRef]
- Brand, R.E.; Nolen, B.M.; Zeh, H.J.; Allen, P.J.; Eloubeidi, M.A.; Goldberg, M.; Elton, E.; Arnoletti, J.P.; Christein, J.D.; Vickers, S.M.; et al. Serum biomarker panels for the detection of pancreatic cancer. Clin. Cancer Res. 2011, 17, 805–816. [Google Scholar] [CrossRef]
- Chen, K.T.; Kim, P.D.; Jones, K.A.; Devarajan, K.; Patel, B.B.; Hoffman, J.P.; Ehya, H.; Huang, M.; Watson, J.C.; Tokar, J.L.; et al. Potential prognostic biomarkers of pancreatic cancer. Pancreas 2014, 43, 22–27. [Google Scholar] [CrossRef]
- Wang, J.; Raimondo, M.; Guha, S.; Chen, J.; Diao, L.; Dong, X.; Wallace, M.B.; Killary, A.M.; Frazier, M.L.; Woodward, T.A.; et al. Circulating microRNAs in pancreatic juice as candidate biomarkers of pancreatic cancer. J. Cancer 2014, 5, 696–705. [Google Scholar] [CrossRef]
- Ballehaninna, U.K.; Chamberlain, R.S. Biomarkers for pancreatic cancer: Promising new markers and options beyond CA19-9. Tumour Biol. 2013, 34, 3279–3292. [Google Scholar] [CrossRef] [PubMed]
- Kondalsamy-Chennakesavan, S.; Hackethal, A.; Bowtell, D.; Obermair, A. Differentiating stage 1 epithelial ovarian cancer from benign ovarian tumours using a combination of tumour markers HE4, CA125, and CEA and patient’s age. Gynecol. Oncol. 2013, 129, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Bast, R.C., Jr.; Brewer, M.; Zou, C.; Hernandez, M.A.; Daley, M.; Ozols, R.; Lu, K.; Lu, Z.; Badgwell, D.; Mills, G.B.; et al. Prevention and early detection of ovarian cancer: Mission impossible? Recent Results Cancer Res. 2007, 174, 91–100. [Google Scholar]
- Chan, A.; Prassas, I.; Dimitromanolakis, A.; Brand, R.E.; Serra, S.; Diamandis, E.P.; Blasutig, I.M. Validation of biomarkers that complement CA19.9 in detecting early pancreatic cancer. Clin. Cancer Res. 2014, 20, 5787–5795. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, H.; Suzuki, M.; Takeshima, N.; Takizawa, K.; Kimura, E.; Nakanishi, T.; Yamada, K.; Takano, H.; Sasaki, H.; Koyama, K.; et al. Evaluation of human epididymis protein 4 (HE4) and Risk of Ovarian Malignancy Algorithm (ROMA) as diagnostic tools of type I and type II epithelial ovarian cancer in Japanese women. Tumour Biol. 2014. [Google Scholar] [CrossRef]
- Lenhard, M.; Stieber, P.; Hertlein, L.; Kirschenhofer, A.; Furst, S.; Mayr, D.; Nagel, D.; Hofmann, K.; Krocker, K.; Burges, A.; et al. The diagnostic accuracy of two human epididymis protein 4 (HE4) testing systems in combination with CA125 in the differential diagnosis of ovarian masses. Clin. Chem. Lab. Med. 2011, 49, 2081–2088. [Google Scholar] [CrossRef] [Green Version]
- Lokich, E.; Singh, R.K.; Han, A.; Romano, N.; Yano, N.; Kim, K.; Moore, R.G. HE4 expression is associated with hormonal elements and mediated by importin-dependent nuclear translocation. Sci. Rep. 2014, 4, 5500. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, T.; Jiang, S.-W.; Qin, L.; Senkowski, C.; Lyle, C.; Terry, K.; Brower, S.; Chen, H.; Glasgow, W.; Wei, Y.; et al. Expression and Diagnostic Value of HE4 in Pancreatic Adenocarcinoma. Int. J. Mol. Sci. 2015, 16, 2956-2970. https://doi.org/10.3390/ijms16022956
Huang T, Jiang S-W, Qin L, Senkowski C, Lyle C, Terry K, Brower S, Chen H, Glasgow W, Wei Y, et al. Expression and Diagnostic Value of HE4 in Pancreatic Adenocarcinoma. International Journal of Molecular Sciences. 2015; 16(2):2956-2970. https://doi.org/10.3390/ijms16022956
Chicago/Turabian StyleHuang, Tianhe, Shi-Wen Jiang, Liangyi Qin, Christopher Senkowski, Christian Lyle, Karen Terry, Steven Brower, Haibin Chen, Wayne Glasgow, Yongchang Wei, and et al. 2015. "Expression and Diagnostic Value of HE4 in Pancreatic Adenocarcinoma" International Journal of Molecular Sciences 16, no. 2: 2956-2970. https://doi.org/10.3390/ijms16022956