
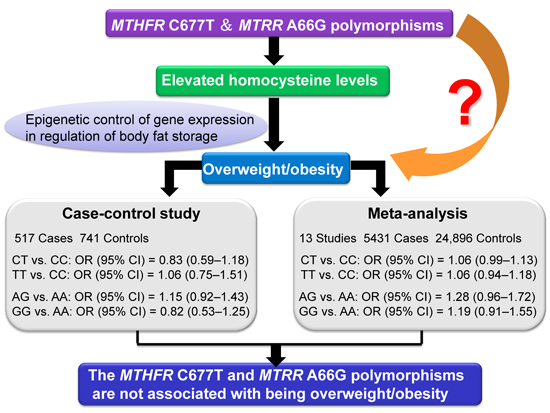
Are MTHFR C677T and MTRR A66G Polymorphisms Associated with Overweight/Obesity Risk? From a Case-Control to a Meta-Analysis of 30,327 Subjects

 ,
,
Abstract
:
1. Introduction
2. Results
2.1. Population Characteristics in Our Case-Control Study
2.2. Genotype Distribution and Association Analysis in Our Case-Control Study

{kind=link}
{kind=link}
| Characteristics | Controls | Overweight/Obesity | p-Value |
|---|---|---|---|
| Number of subjects | 741 | 517 | - |
| Gender (male/female) | 369/372 | 261/256 | 0.819 |
| Age (year) | 44.57 ± 9.71 | 47.4 ± 9.72 | <0.001 |
| Height (cm) | 166.81 ± 7.41 | 166.74 ± 8.23 | 0.877 |
| Weight (kg) | 61.14 ± 6.94 | 75.31 ± 10.34 | <0.001 |
| BMI (kg/m2) | 21.92 ± 1.39 | 27.02 ± 2.56 | <0.001 |
| WC (cm) | 78.16 ± 6.67 | 90.22 ± 8.32 | <0.001 |
| SBP (mmHg) | 122.36 ± 17.17 | 133.89 ± 19.08 | <0.001 |
| DBP (mmHg) | 77.25 ± 10.77 | 84.33 ± 12.63 | <0.001 |
| FBG (mmol/L) | 5.03 ± 0.70 | 5.27 ± 0.88 | <0.001 |
| TC (mmol/L) | 4.85 ± 1.02 | 5.05 ± 0.99 | 0.001 |
| TG (mmol/L) | 1.01 ± 1.00 | 1.56 ± 0.98 | <0.001 |
| HDL-C (mmol/L) | 1.31 ± 0.35 | 1.19 ± 0.30 | <0.001 |
| LDL-C (mmol/L) | 2.67 ± 0.93 | 2.80 ± 0.94 | 0.016 |
| Polymorphism | Cases (n = 517) | Controls (n = 741) | Crude OR (95% CI) | p-Value | Adjusted OR a | p-Value |
|---|---|---|---|---|---|---|
| MTHFR C677T | ||||||
| CC | 115 (22.2) | 160 (21.6) | 1.00 | - | 1.00 | - |
| CT | 244 (47.2) | 375 (50.6) | 0.91 (0.68–1.21) | 0.499 | 0.83 (0.59–1.18) | 0.308 |
| TT | 158 (30.6) | 206 (27.8) | 1.07 (0.78–1.47) | 0.688 | 1.06 (0.75–1.51) | 0.738 |
| Allelic model | - | - | 1.04 (0.89–1.22) | 0.602 | 1.05 (0.85–1.30) | 0.626 |
| Dominant model | - | - | 0.96 (0.73–1.26) | 0.783 | 0.92 (0.65–1.32) | 0.655 |
| Recessive model | - | - | 1.14 (0.89–1.46) | 0.288 | 1.21 (0.88–1.67) | 0.245 |
| MTRR A66G | ||||||
| AA | 298 (57.6) | 437 (59.0) | 1.00 | - | 1.00 | - |
| AG | 186 (36.0) | 251 (33.9) | 1.09 (0.86–1.38) | 0.497 | 1.15 (0.92–1.43) | 0.216 |
| GG | 33 (6.4) | 53 (7.1) | 0.91 (0.58–1.45) | 0.698 | 0.82 (0.53–1.25) | 0.344 |
| Allelic model | - | - | 1.02 (0.84–1.22) | 0.871 | 1.11 (0.87–1.41) | 0.403 |
| Dominant model | - | - | 1.06 (0.84–1.33) | 0.637 | 1.17 (0.87–1.58) | 0.291 |
| Recessive model | - | - | 0.89 (0.56–1.39) | 0.595 | 0.99 (0.56–1.76) | 0.968 |
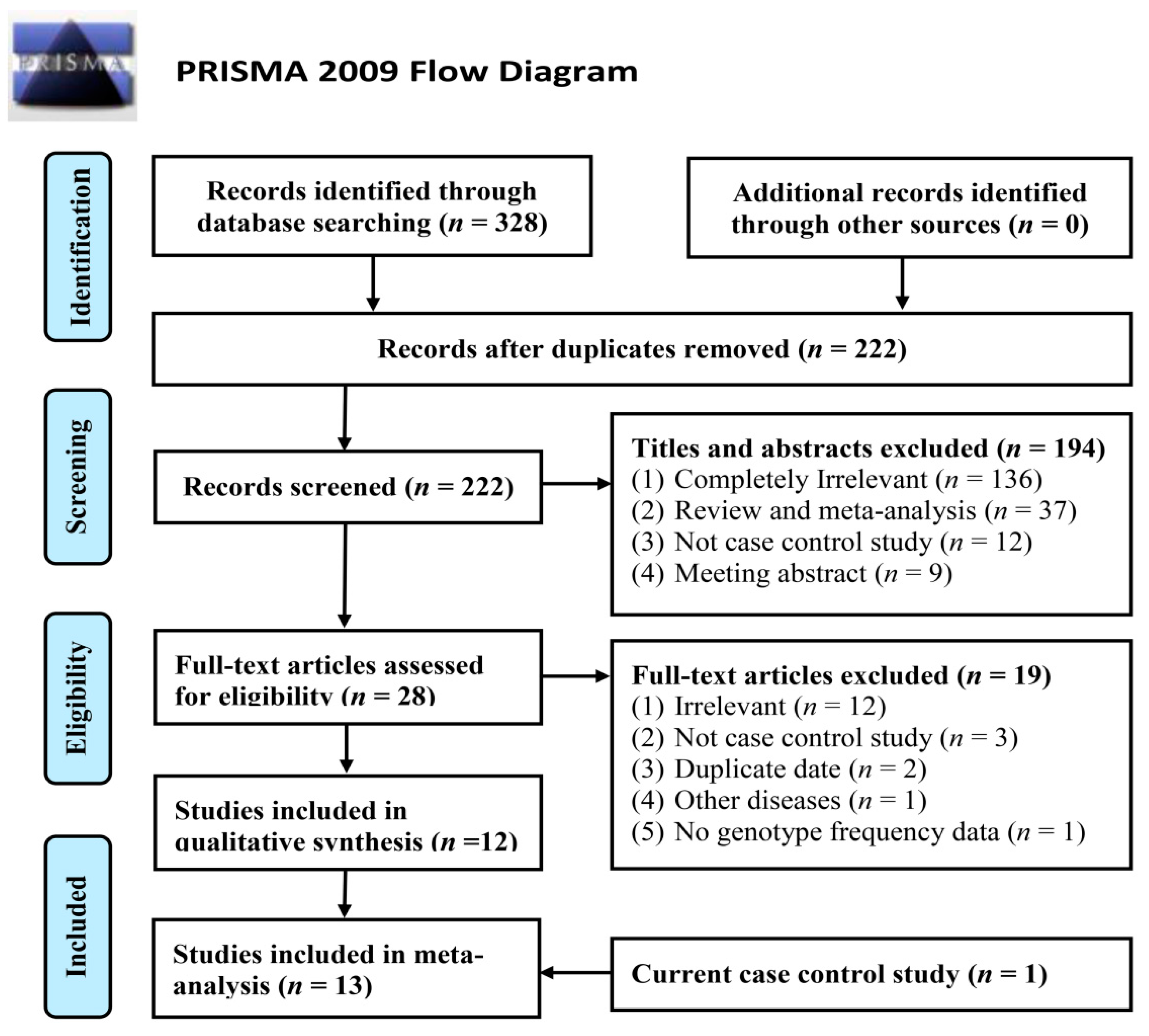
2.3. Meta-Analysis Results

| Study | Genotype Distribution | Allele Frequency | HWE Test | Number of Cases/Controls | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Author (Year) | Cases | Controls | Cases | Controls | χ2 | p | |||||||
| MTHFR C677T | CC | CT | TT | CC | CT | TT | C | T | C | T | - | - | - |
| Thawnashom et al. (2005) [4] | 67 | - | 23 e | 34 | - | 16 e | NA | NA | NA | NA | NA | NA | 90/50 |
| Terruzzi et al. (2007) [5] | 18 | 54 | 12 | 14 | 33 | 5 | 90 | 78 | 61 | 43 | 4.9466 | 0.026 | 84/52 |
| Lewis et al. (2008) [6] a | 360 | 410 | 112 | 1165 | 1086 | 283 | 1130 | 634 | 3416 | 1652 | 1.5459 | 0.214 | 882/2534 |
| Lewis et al. (2008) [6] b | 163 | 155 | 38 | 2707 | 2713 | 715 | 481 | 231 | 8127 | 4143 | 0.7882 | 0.375 | 356/6135 |
| Lewis et al. (2008) [6] c | 115 | 93 | 25 | 2155 | 2190 | 552 | 323 | 143 | 6500 | 3294 | 0.0153 | 0.902 | 233/4897 |
| Lewis et al. (2008) [6] d | 588 | 574 | 107 | 3812 | 3356 | 736 | 1750 | 788 | 10,980 | 4828 | 0.0045 | 0.946 | 1269/7904 |
| Settin et al. (2009) [7] | 89 | 34 | 5 | 69 | 36 | 5 | 212 | 44 | 174 | 46 | 0.0121 | 0.912 | 128/110 |
| Bazzaz et al. (2010) [8] | 44 | 21 | 9 | 113 | 80 | 14 | 109 | 39 | 306 | 108 | 0.0009 | 0.975 | 74/207 |
| Gara et al. (2011) [9] | 15 | 14 | 2 | 9 | 12 | 1 | 44 | 18 | 30 | 14 | 1.4550 | 0.228 | 31/22 |
| Chauhan et al. (2012) [10] | 348 | 185 | 29 | 272 | 148 | 16 | 881 | 243 | 692 | 180 | 0.5680 | 0.451 | 562/436 |
| Yin et al. (2012) [11] | 354 | 341 | 56 | 471 | 441 | 66 | 1049 | 453 | 1383 | 573 | 7.6608 | 0.006 | 751/978 |
| Tabassum et al. (2012) [12] | 290 | 144 | 20 | 581 | 218 | 31 | 724 | 184 | 1380 | 280 | 0.8313 | 0.068 | 454/830 |
| Our study | 115 | 244 | 158 | 160 | 375 | 206 | 474 | 560 | 695 | 787 | 0.1911 | 0.662 | 517/741 |
| MTRR A66G | AA | AG | GG | AA | AG | GG | A | G | A | G | - | - | - |
| Terruzzi et al. (2007) [5] | 39 | 42 | 0 | 36 | 16 | 1 | 120 | 42 | 88 | 18 | 0.2649 | 0.607 | 81/53 |
| Tabassum et al. (2012) [12] | 110 | 231 | 106 | 244 | 407 | 169 | 451 | 443 | 895 | 745 | 0.0009 | 0.976 | 447/820 |
| Our study | 298 | 186 | 33 | 437 | 251 | 53 | 782 | 252 | 1125 | 357 | 4.0366 | 0.045 | 517/741 |
| Subgroup | Recessive | Dominant | Homozygous Codominant | Heterozygous Codominant | Allelic Model | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph | |
| MTHFR C677T polymorphism | ||||||||||
| Overall | 1.05 (0.94–1.16) | 0.730 | 1.05 (0.99–1.13) | 0.140 | 1.06 (0.94–1.18) | 0.664 | 1.06 (0.99–1.13) | 0.095 | 1.05 (1.00–1.10) | 0.284 |
| Ethnicity | ||||||||||
| Asian | 1.18 (0.99–1.41) | 0.862 | 1.04 (0.93–1.16) | 0.304 | 1.16 (0.95–1.42) | 0.880 | 1.02 (0.91–1.15) | 0.155 | 1.07 (0.98–1.16) | 0.513 |
| Caucasian | 0.99 (0.86–1.13) | 0.477 | 1.04 (0.90–1.20) | 0.049 | 1.02 (0.89–1.18) | 0.209 | 1.05 (0.91–1.21) | 0.080 | 1.02 (0.92-1.13) | 0.077 |
| African | 1.45 (0.12–17.04) | - | 0.74 (0.25–2.23) | - | 1.20 (0.10–15.20) | - | 0.70 (0.23–2.17) | - | 0.88 (0.38–2.03) | - |
| Source of control | ||||||||||
| Population based | 1.02 (0.90–1.45) | 0.581 | 1.07 (1.00–1.18) | 0.057 | 1.05 (0.93–1.20) | 0.356 | 1.07 (0.96–1.19) | 0.076 | 1.05 (0.97–1.13) | 0.088 |
| Hospital based | 1.19 (0.95–1.49) | 0.786 | 0.90 (0.74–1.10) | 0.810 | 1.13 (0.85–1.50) | 0.782 | 0.85 (0.68–1.06) | 0.722 | 1.02 (0.89–1.17) | 0.736 |
| Genotyping method | ||||||||||
| PCR-RFLP | 0.98 (0.82–1.17) | 0.261 | 1.01 (0.85–1.20) | 0.596 | 1.02 (0.85–1.23) | 0.434 | 1.07 (0.97–1.19) | 0.397 | 1.03 (0.96–1.11) | 0.911 |
| TaqMan | 1.07 (0.93–1.24) | 0.729 | 0.96 (0.80–1.16) | 0.026 | 1.07 (0.91–1.25) | 0.356 | 0.95 (0.79–1.15) | 0.040 | 1.00 (0.88–1.13) | 0.054 |
| Others | 1.30 (0.86–1.97) | 0.909 | 1.10 (1.00–1.23) | 0.377 | 1.35 (0.88–2.05) | 0.974 | 1.13 (0.94–1.36) | 0.191 | 1.15 (0.99–1.33) | 0.450 |
| Sample size | ||||||||||
| Large study | 1.04 (0.93–1.16) | 0.615 | 1.06 (0.96–1.16) | 0.075 | 1.06 (0.94–1.19) | 0.468 | 1.05 (0.95–1.16) | 0.077 | 1.05 (1.00–1.10) | 0.138 |
| Small study | 1.48 (0.82–2.67) | 0.788 | 0.83 (0.61–1.12) | 0.782 | 1.39 (0.75–2.59) | 0.762 | 0.78 (0.55–1.11) | 0.642 | 0.98 (0.76–1.25) | 0.616 |
| MTRR A66G polymorphism | ||||||||||
| Overall | 1.09 (0.86–1.38) | 0.476 | 1.27 (0.95–1.70) | 0.106 | 1.19 (0.91–1.55) | 0.246 | 1.28 (0.96–1.72) | 0.116 | 1.14 (0.95–1.35) | 0.194 |
3. Discussion
4. Experimental Section
4.1. Study Subjects
4.2. Clinical Measurements and Laboratory Tests
4.3. Genotyping Analysis
4.4. Statistical Analysis
4.5. Meta-Analysis
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Van Gal, L.F.; Maggioni, A.P. Overweight, obesity, and outcomes: Fat mass and beyond. Lancet 2014, 383, 935–936. [Google Scholar] [CrossRef] [PubMed]
- International Obesity Taskforce. Obesity: The global epidemic (2010). Available online: http://www.iaso.org/iotf/obesity/obesitytheglobalepidemic (accessed on 19 July 2014).
- Bell, C.G.; Walley, A.J.; Froguel, P. The genetics of human obesity. Nat. Rev. Genet. 2005, 6, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Thawnashom, K.; Tungtrongchitr, R.; Petmitr, S.; Pongpaew, P.; Phonrat, B.; Tungtrongchitr, A.; Schelp, F.P. Methylenetetrahydrofolate reductase (MTHFR) polymorphism (C677T) in relation to homocysteine concentration in overweight and obese Thais. Southeast Asian J. Trop. Med. Public Health 2005, 36, 459–466. [Google Scholar] [PubMed]
- Terruzzi, I.; Senesi, P.; Fermo, I.; Lattuada, G.; Luzi, L. Are genetic variants of the methyl group metabolism enzymes risk factors predisposing to obesity? J. Endocrinol. Investig. 2007, 30, 747–753. [Google Scholar] [CrossRef]
- Lewis, S.J.; Lawlor, D.A.; Nordestgaard, B.G.; Tybjaerg-Hansen, A.; Ebrahim, S.; Zacho, J.; Ness, A.; Leary, S.; Smith, G.D. The methylenetetrahydrofolate reductase C677T genotype and the risk of obesity in three large population-based cohorts. Eur. J. Endocrinol. 2008, 159, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Settin, A.A.; Algasham, A.; Dowaidar, M.; Ismail, H. Methylenetetrahydrofolate reductase and angiotensin converting enzyme gene polymorphisms related to overweight/obesity among Saudi subjects from Qassim Region. Dis. Markers 2009, 27, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Bazzaz, J.T.; Shojapoor, M.; Nazem, H.; Amiri, P.; Fakhrzadeh, H.; Heshmat, R.; Parvizi, M.; Hasani-Ranjbar, S.; Amoli, M.M. Methylenetetrahydrofolate reductase gene polymorphism in diabetes and obesity. Mol. Biol. Rep. 2010, 37, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Gara, S.; Ochi, H.; Chango, A.; Najjar, L.; Feki, M.; B’chir, F.; Kaabachi, N.; Ben Becher, S.; Boukthir, S.; Abdennebi, M. C677t polymorphism of MTHFR and G80A polymorphism of RFC genes and their relation with homocysteine levels in obese Tunisian children. Tunis Med. 2011, 89, 565–568. [Google Scholar] [PubMed]
- Chauhan, G.; Kaur, I.; Tabassum, R.; Dwivedi, O.P.; Ghosh, S.; Tandon, N.; Bharadwaj, D. Common Variants of Homocysteine Metabolism Pathway Genes and Risk of Type 2 Diabetes and Related Traits in Indians. Exp. Diabetes Res. 2012, 2012. [Google Scholar] [CrossRef]
- Yin, R.X.; Wu, D.F.; Miao, L.; Aung, L.H.; Cao, X.L.; Yan, T.T.; Long, X.J.; Liu, W.Y.; Zhang, L.; Li, M. Several genetic polymorphisms interact with overweight/obesity to influence serum lipid levels. Cardiovasc. Diabetol. 2012, 11. [Google Scholar] [CrossRef]
- Tabassum, R.; Jaiswal, A.; Chauhan, G.; Dwivedi, O.P.; Ghosh, S.; Marwaha, R.K.; Tandon, N.; Bharadwaj, D. Genetic variant of AMD1 is associated with obesity in urban Indian children. PLoS ONE 2012, 7, e33162. [Google Scholar] [CrossRef] [PubMed]
- Frosst, P.; Blom, H.J.; Milos, R.; Goyette, P.; Sheppard, C.A.; Matthews, R.G.; Boers, G.J.; den Heijer, M.; Kluijtmans, L.A.; van den Heuvel, L.P.; et al. A candidate genetic risk factor for vascular disease: A common mutation in methylenetetrahydrofolate reductase. Nat. Genet. 1995, 10, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Gaughan, D.J.; Kluijtmans, L.A.; Barbaux, S.; McMaster, D.; Young, I.S.; Yarnell, J.W.; Evans, A.; Whitehead, A.S. The methionine synthase reductase (MTRR) A66G polymorphism is a novel genetic determinant of plasma homocysteine concentrations. Atherosclerosis 2001, 157, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, I.; Tran, P.; Christensen, B.; Sibani, S.; Rozen, R. A second genetic polymorphism in methylenetetrahydrofolate reductase (MTHFR) associated with decreased enzyme activity. Mol. Genet. Metab. 1998, 64, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Van der Put, N.M.; Blom, H.J. Neural tube defects and a disturbed folate dependent homocysteine metabolism. Eur. J. Obstet. Gynecol. Reprod. Biol. 2000, 92, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Olteanu, H.; Munson, T.; Banerjee, R. Differences in the efficiency of reductive activation of methionine synthase and exogenous electron acceptors between the common polymorphic variants of human methionine synthase reductase. Biochemistry 2002, 41, 13378–13385. [Google Scholar] [CrossRef] [PubMed]
- Marchesini, G.; Manini, R.; Bianchi, G.; Sassi, S.; Natale, S.; Chierici, S.; Visani, F.; Baraldi, L.; Forlani, G.; Melchionda, N. Homocysteine and psychological traits: A study in obesity. Nutrition 2002, 18, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Jacques, P.F.; Bostom, A.G.; Wilson, P.W.; Rich, S.; Rosenberg, I.H.; Selhub, J. Determinants of plasma total homocysteine concentration in the Framingham Offspring cohort. Am. J. Clin. Nutr. 2001, 73, 613–621. [Google Scholar] [PubMed]
- Martos, R.; Valle, M.; Morales, R.; Cañete, R.; Gavilan, M.I.; Sánchez-Margalet, V. Hyperhomocysteinemia correlates with insulin resistance and low-grade systemic inflammation in obese prepubertal children. Metabolism 2006, 55, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Fuks, F. DNA methylation and histone modifications: Teaming up to silence genes. Curr. Opin. Genet. Dev. 2005, 15, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.T.; Schalinske, K.L. New insignts into the regulation of methyl group and homocysteine metabolism. J. Nutr. 2007, 137, 311–314. [Google Scholar] [PubMed]
- Cooney, C.A.; Dave, A.A.; Wolff, G.L. Maternal methyl supplements in mice affect epigenetic variation and DNA methylation of offspring. J. Nutr. 2002, 132, 2393S–2400S. [Google Scholar] [PubMed]
- Melzner, I.; Scott, V.; Dorsch, K.; Fischer, P.; Wabitsch, M.; Brüderlein, S.; Hasel, C.; Möller, P. Leptin gene expression in human preadipocytes is switched on by maturation-induced demethylation of distinct CpGs in its proximal promoter. J .Biol. Chem. 2002, 277, 45420–45427. [Google Scholar] [CrossRef] [PubMed]
- Newell-Price, J. Proopiomelanocortin gene expression and DNA methylation: implications for Cushing’s syndrome and beyond. J. Endocrinol. 2003, 177, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Scuteri, A.; Sanna, S.; Chen, W.M.; Uda, M.; Albal, G.; Strait, J.; Najiar, S.; Naqaraja, R.; Orru, M.; Usala, G.; et al. Genome-wide association scan shows genetic variants in the FTO gene are associated with obesity-related traits. PLoS Genet. 2007, 3, e115. [Google Scholar] [CrossRef] [PubMed]
- Bokor, S.; Meirhaeghe, A.; Ruiz, J.R.; Zaccaria, M.; Widhalm, K.; Gonzalez-Gross, M.; Amouyel, P.; Moreno, L.A.; Molnàr, D.; Dallongeville, J.; Helena Study Group. Common polymorphisms in six genes of the methyl group metabolism pathway and obesity in European adolescents. Int. J. Pediatr. Obes. 2011, 6, e336–e344. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Liu, Y.; Li, Y.; Fan, S.; Zhi, X.; Lu, X.; Wang, D.; Zheng, Q.; Wang, Y.; Wang, Y.; Sun, G. Geographical Distribution of MTHFR C677T, A1298C and MTRR A66G Gene Polymorphisms in China: Findings from 15,357 Adults of Han Nationality. PLoS ONE 2013, 8, e57917. [Google Scholar] [CrossRef] [PubMed]
- Lambrinoudaki, I.; Kaparos, G.; Papadimitriou, D.; Sergentanis, T.N.; Creatsa, M.; Alexandrou, A.; Logothetis, E.; Christodoulakos, G.; Kouskouni, E. Methylenetetrahydrofolate reductase C677T polymorphism is associated with central adiposity and increased androgenicity in healthy postmenopausal women. Eur. J. Endocrinol. 2008, 159, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane handbook for systematic reviews of interventions 4.2.6 (updated September 2006). Available online: http://www.cochrane.org/resources/handbook/hbook.htm (accessed on 6 October 2014).
- Liu, X.; Zhao, L.J.; Liu, Y.J.; Xiong, D.H.; Recker, R.R.; Deng, H.W. The MTHFR gene polymorphism is associated with lean body mass but not fat body mass. Hum. Genet. 2008, 123, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Swart, K.M.; Enneman, A.W.; van Wijingaarden, J.P.; van Dijk, S.C.; Brouwer-Brolsma, E.M.; Ham, A.C.; Dhonukshe-Rutten, R.A.; van der Velde, N.; Bruq, J.; van Meurs, J.B.; et al. Homocysteine and the methylenetetrahydrofolate reductase 677C-T polymorphism in relation to muscle mass and strength, physical performance and postural sway. Eur. J. Clin. Nutr. 2013, 67, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Zintzaras, E.; Ioannidis, J.P. Heterogeneity testing in meta-analysis of genome searches. Genet. Epidemiol. 2005, 28, 123–137. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Trikalinos, T.A.; Salanti, G.; Zintzaras, E.; Ioannidis, J.P. Meta-analysis methods. Adv. Genet. 2008, 60, 311–334. [Google Scholar] [PubMed]
- Egger, M.; Davey, S.G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, S.-J.; Yang, B.-Y.; Zhi, X.-Y.; He, M.; Wang, D.; Wang, Y.-X.; Wang, Y.-N.; Wei, J.; Zheng, Q.-M.; Sun, G.-F. Are MTHFR C677T and MTRR A66G Polymorphisms Associated with Overweight/Obesity Risk? From a Case-Control to a Meta-Analysis of 30,327 Subjects. Int. J. Mol. Sci. 2015, 16, 11849-11863. https://doi.org/10.3390/ijms160611849
Fan S-J, Yang B-Y, Zhi X-Y, He M, Wang D, Wang Y-X, Wang Y-N, Wei J, Zheng Q-M, Sun G-F. Are MTHFR C677T and MTRR A66G Polymorphisms Associated with Overweight/Obesity Risk? From a Case-Control to a Meta-Analysis of 30,327 Subjects. International Journal of Molecular Sciences. 2015; 16(6):11849-11863. https://doi.org/10.3390/ijms160611849
Chicago/Turabian StyleFan, Shu-Jun, Bo-Yi Yang, Xue-Yuan Zhi, Miao He, Da Wang, Yan-Xun Wang, Yi-Nuo Wang, Jian Wei, Quan-Mei Zheng, and Gui-Fan Sun. 2015. "Are MTHFR C677T and MTRR A66G Polymorphisms Associated with Overweight/Obesity Risk? From a Case-Control to a Meta-Analysis of 30,327 Subjects" International Journal of Molecular Sciences 16, no. 6: 11849-11863. https://doi.org/10.3390/ijms160611849