
Age-Related Renal Microvascular Changes: Evaluation by Three-Dimensional Digital Imaging of the Human Renal Microcirculation Using Virtual Microscopy

Abstract
:1. Introduction
2. Results
2.1. Clinical and Pathological Characteristics of Four Cases
2.2. Original 2D Images
2.3. Three-Dimensional Reconstruction of the Vascular Tree in the Presence of Minimal Vascular Damage (Case 1)
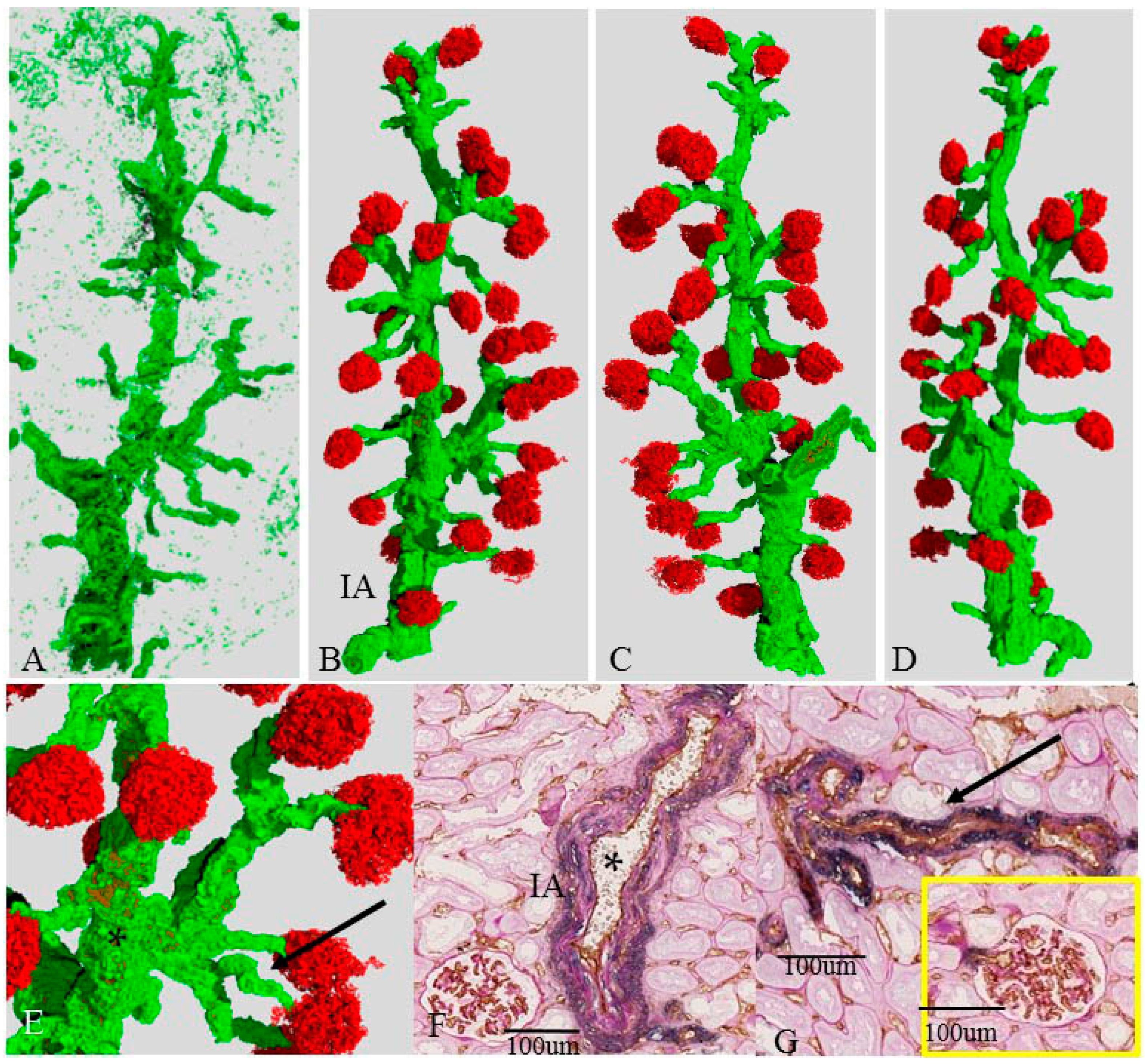
2.4. Three-Dimensional Reconstruction of the Vascular Tree in the Presence of Mildly Damaged Arteries (Case 2)
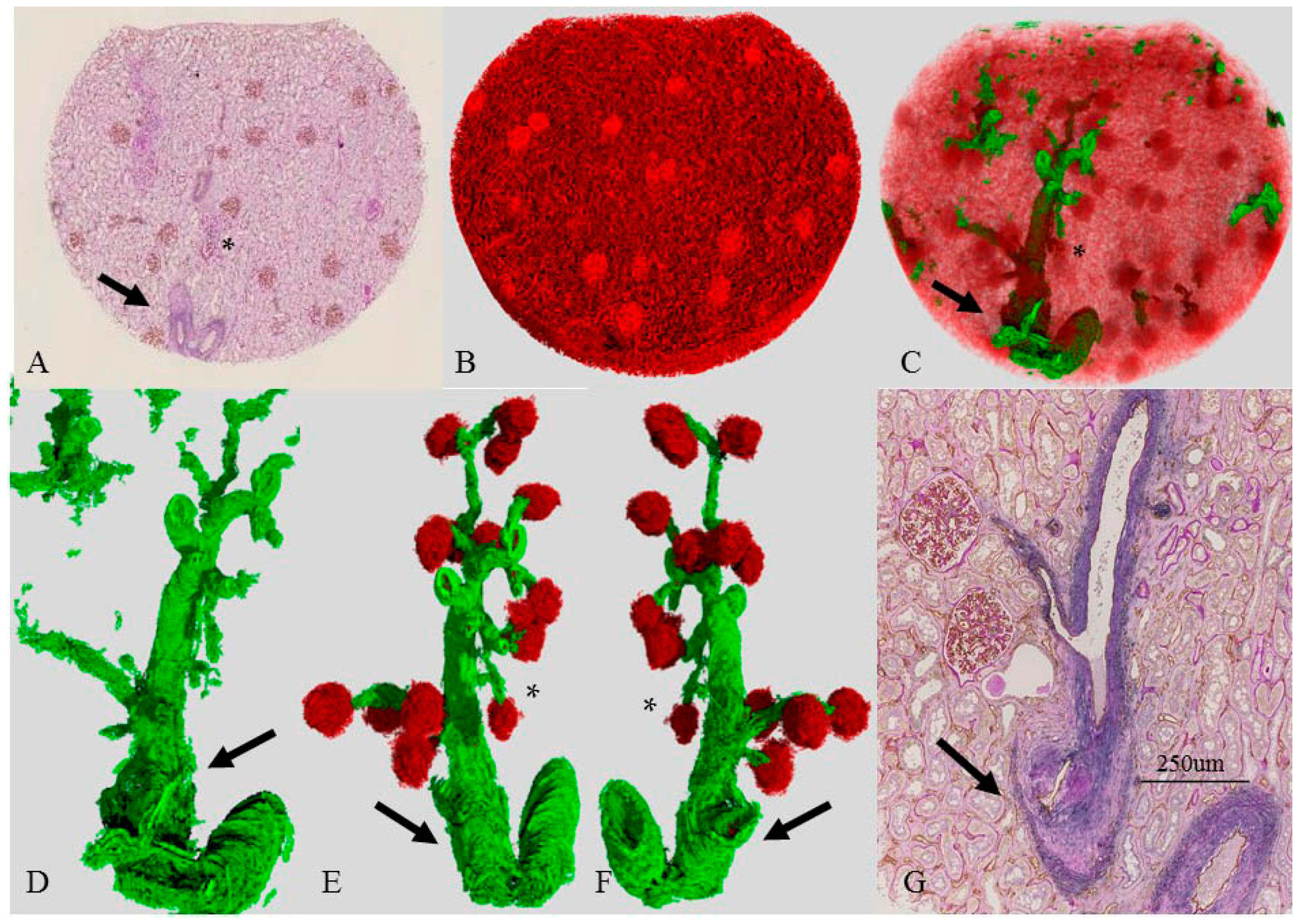
2.5. Three-Dimensional Reconstruction of the Vascular Tree in an Older Patient (Case 3)
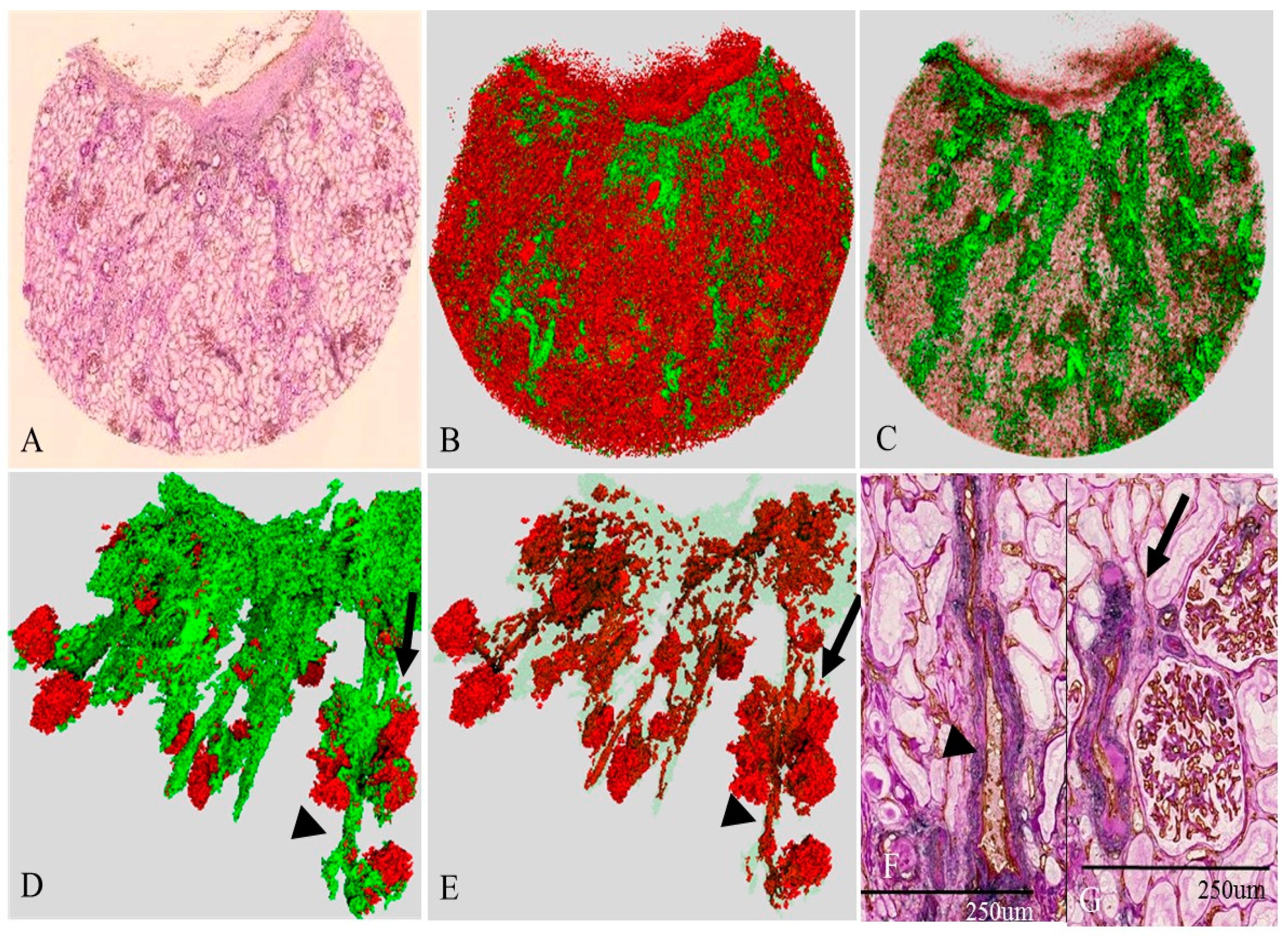
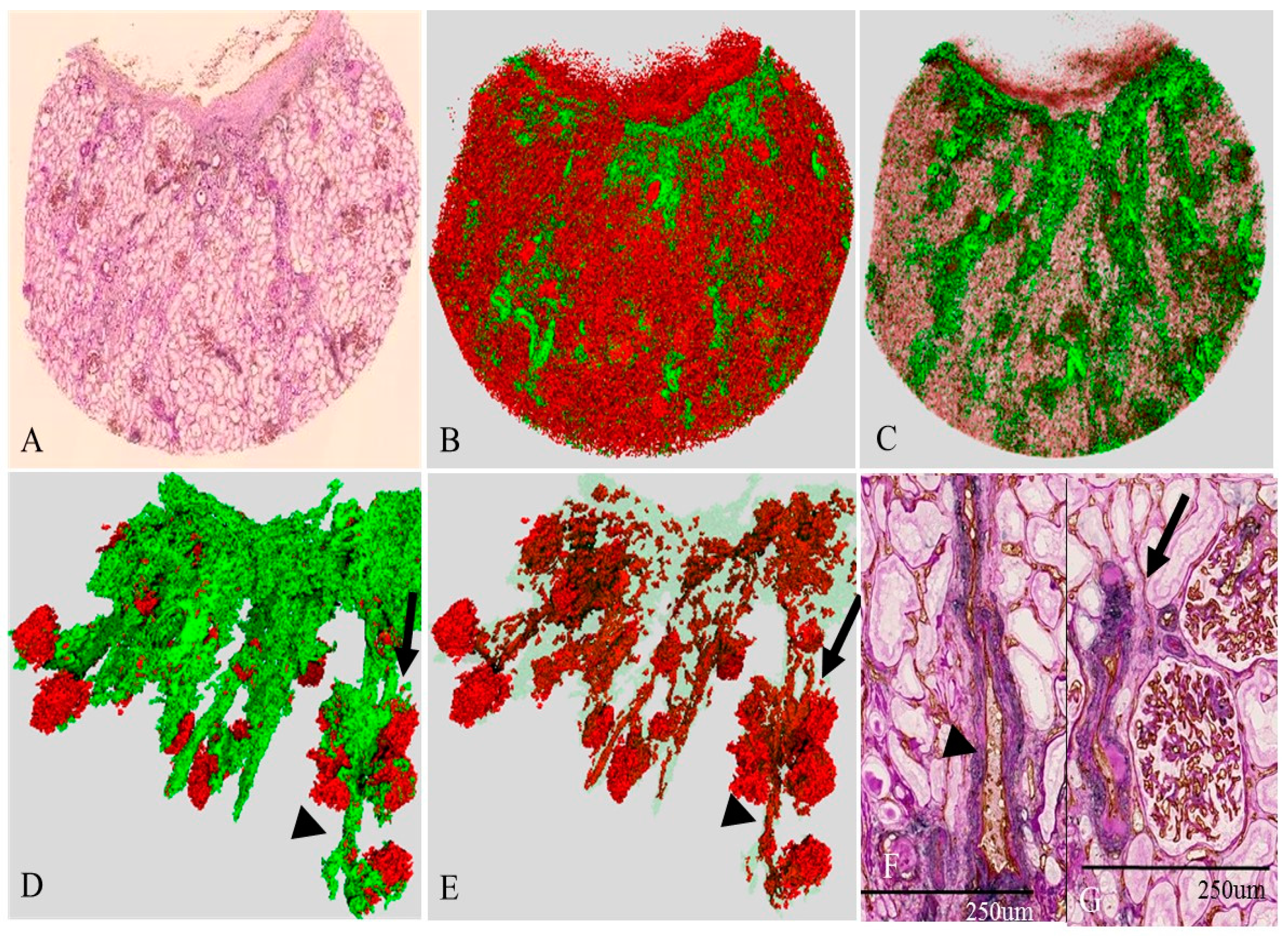
2.6. Three-Dimensional Reconstruction of the Vascular Tree in the Presence of Nephrosclerosis (Case 4)
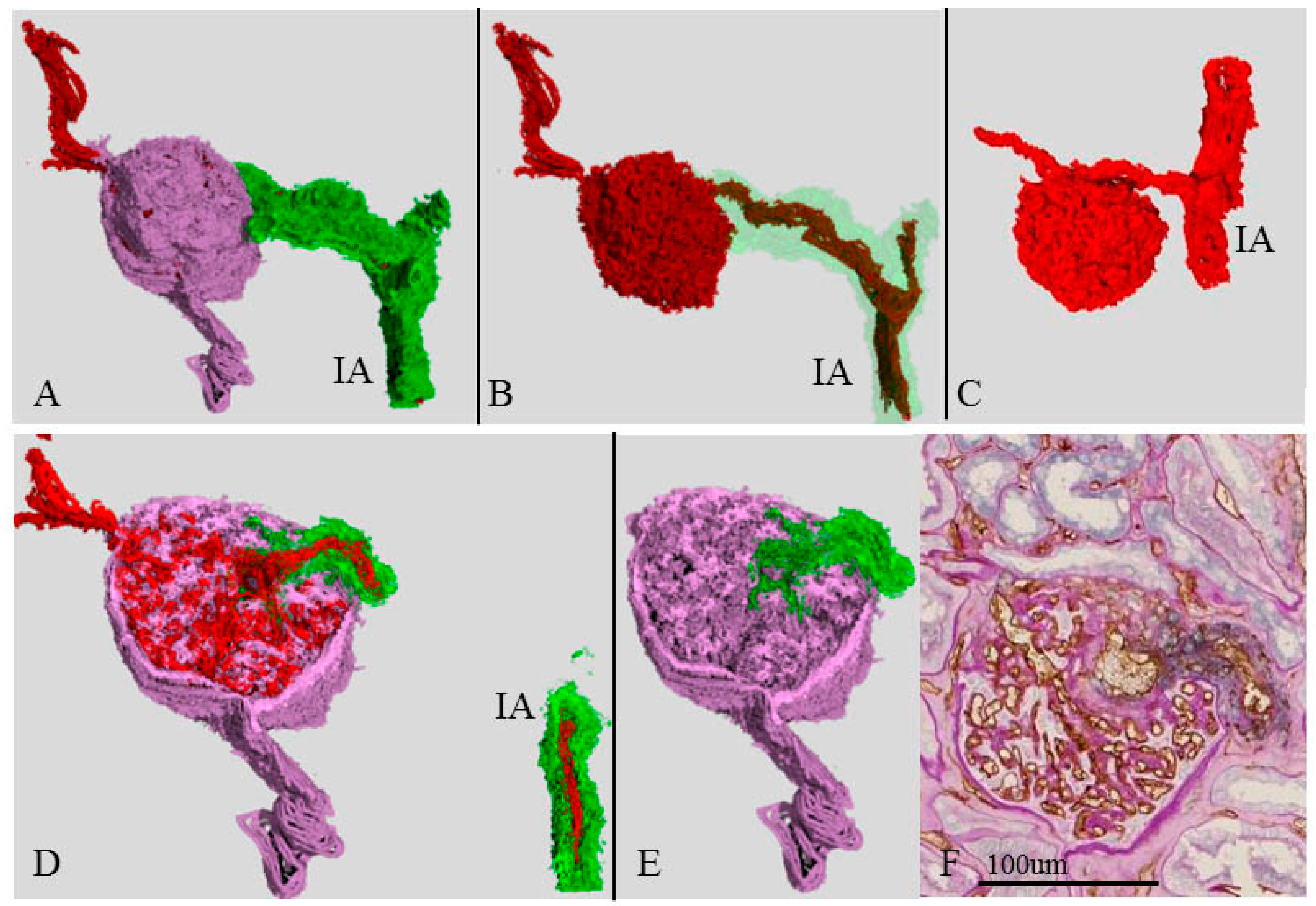
2.7. Three-Dimensional Image of an Atubular Glomerulus (Case 3D)
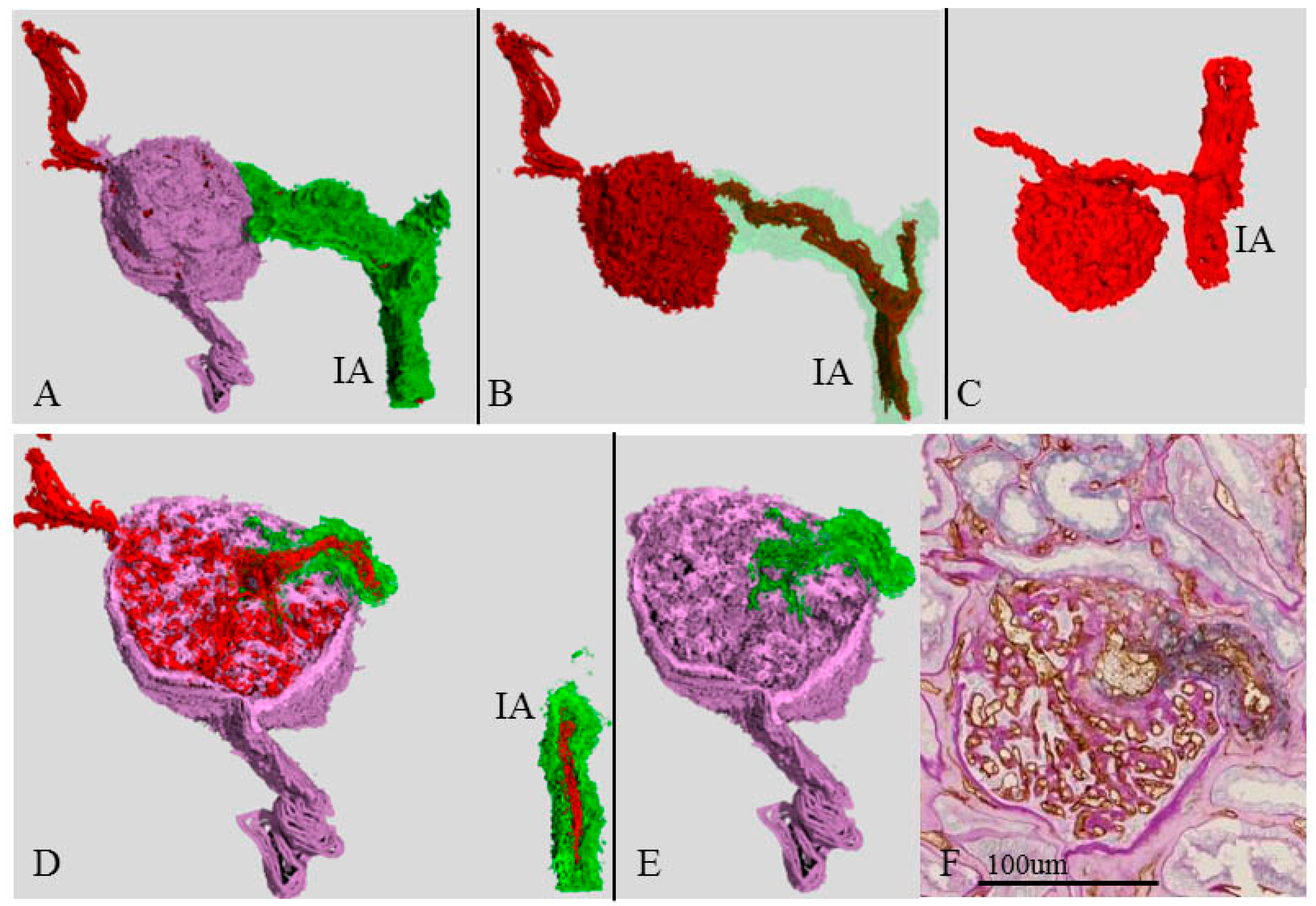
2.8. Three-Dimensional Image of a Single Glomerulus and Cystic Dilation of an Afferent Arteriole (Case 3) near the Atubular Glomerulus
3. Discussion
4. Materials and Methods
4.1. Tissue Preparation
4.2. Immunohistochemistry and Microscopic Image Digitization
4.3. Image Registration, Segmentation of Tissue Components, Geometric Reconstruction
4.4. Conventional Histological Analysis of Surgical Specimens
4.5. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CKD | Chronic Kidney Disease |
| 3D | Three-Dimensional |
| 2D | Two-Dimensional |
| SMA | α-Smooth Muscle Actin |
References
- Navar, L.G.; Arendshorst, W.J.; Pallone, T.L.; Inscho, E.W.; Imig, J.D.; Bell, P.D. The renal microcirculation. In Comprehensive Physiology; Pollock, D.M., Ed.; Wiley: Hoboken, NJ, USA, 2011; pp. 550–683. [Google Scholar]
- Alpers, C.E.; Fogo, A.B. Kidney and its collecting system. In Robbibs Basic Pathology, 9th ed.; Kumar, V., Abbas, A.K., Aster, J.C., Eds.; Elsevier: Philadelphia, PA, USA, 2013; pp. 539–540. [Google Scholar]
- Ljungqvist, A.; Lagergren, C. Normal intrarenal arterial pattern in adult and ageing human kidney: A microangiographical and histological study. J. Anat. Lond. 1962, 96, 285–300. [Google Scholar]
- Schaeffner, E.S.; Ebert, N.; Delanaye, P.; Frei, U.; Gaedeke, J.; Jakob, O.; Kuhlmann, M.K.; Schuchardt, M.; Tölle, M.; Ziebig, R.; et al. Two novel equations to estimate kidney function in persons aged 70 years or older. Ann. Intern. Med. 2012, 157, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Rule, A.D.; Amer, H.; Cornell, L.D.; Taler, S.J.; Cosio, F.G.; Kremers, W.K.; Textor, S.C.; Stegall, M.D. The association between age and nephrosclerosis on renal biopsy among healthy adults. Ann. Intern. Med. 2010, 152, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, R.; Glassock, R.; Doust, J. Chronic kidney disease controversy: How expanding definitions are unnecessarily labelling many people as diseased. BMJ 2013, 347, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Uesugi, N.; Shimazu, Y.; Aoba, T.; Kikuchi, K.; Nagata, M. High-resolution three-dimensional digital imaging of human renal microcirculation: An aid to evaluate microvascular alterations in chronic kidney disease. Pathol. Int. 2015, 65, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Kudo, T.; Shimazu, Y.; Yagishita, H.; Izumo, T.; Soeno, Y.; Sato, K.; Taya, Y.; Aoba, T. Three-dimensional reconstruction of oral tongue squamous cell carcinoma at invasion front. Int. J. Dent. 2013, 13, 424–440. [Google Scholar] [CrossRef] [PubMed]
- Kurata, M.; Nose, M.; Shimazu, Y.; Aoba, T.; Kohada, Y.; Yorioka, S.; Suehiro, S.; Fukuoka, E.; Matsumoto, S.; Watanabe, H.; et al. Microvasculature of carotid atheromatous plaques: Hemorrhagic plaques have dense microvessels with fenestrations to the arterial lumen. J. Stroke Cerebrovasc. Dis. 2014, 23, 1440–1446. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, S.; Shimazu, Y.; Kudo, T.; Sato, K.; Yamazaki, M.; Abé, T.; Babkair, H.; Cheng, J.; Aoba, T.; Saku, T. Three-dimensional visualization of perlecan-rich neoplastic stroma induced concurrently with the invasion of oral squamous cell carcinoma. J. Oral Pathol. Med. 2014, 43, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Shimazu, Y.; Kudo, T.; Yagishita, H.; Aoba, T. Three-dimensional visualization and quantification for the growth and invasion of oral squamous cell carcinoma. Jpn. Dent. Sci. Rev. 2010, 46, 17–25. [Google Scholar] [CrossRef]
- Kubo, M.; Kiyohara, Y.; Kato, I.; Tanizaki, Y.; Katafuchi, R.; Hirakata, H.; Okuda, S.; Tsuneyoshi, M.; Sueishi, K.; Fujishima, M.; et al. Risk factors for renal glomerular and vascular changes in an autopsy-based population survey: The Hisayama study. Kidney Int. 2003, 63, 1508–1515. [Google Scholar] [CrossRef] [PubMed]
- Ninomiya, T.; Kubo, M.; Doi, Y.; Yonemoto, K.; Tanizaki, Y.; Tsuruya, K.; Sueishi, K.; Tsuneyoshi, M.; Iida, M.; Kiyohara, Y. Prehypertension increases the risk for renal arteriosclerosis in autopsies: The Hisayama Study. J. Am. Soc. Nephrol. 2007, 18, 2135–2142. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.C.; Busque, S.; Workeneh, B.; Ho, B.; Derby, G.; Blouch, K.L.; Sommer, F.G.; Edwards, B.; Myers, B.D. Effects of aging on glomerular function and number in living kidney donors. Kidney Int. 2010, 78, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Elsherbiny, H.E.; Alexander, M.P.; Kremers, W.K.; Park, W.D.; Poggio, E.D.; Prieto, M.; Lieske, J.C.; Rule, A.D. Nephron hypertrophy and glomerulosclerosis and their association with kidney function and risk factors among living kidney donors. Clin. J. Am. Soc. Nephrol. 2014, 9, 1892–1902. [Google Scholar] [CrossRef] [PubMed]
- Kappel, B.; Olsen, S. Cortical interstitial tissue and sclerosed glomeruli in the normal human kidney, related to age and sex. A quantitative study. Virchows Arch. A Pathol. Anat. Histol. 1980, 387, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Haas, M.; Segev, D.L.; Racusen, L.C.; Bagnasco, S.M.; Melancon, J.K.; Tan, M.; Kraus, E.S.; Rabb, H.; Ugarte, R.M.; Burdick, J.F.; et al. Arteriosclerosis in kidneys from healthy live donors: Comparison of wedge and needle core perioperative biopsies. Arch. Pathol. Lab. Med. 2008, 132, 37–42. [Google Scholar] [PubMed]
- Samuel, T.; Hoy, W.E.; Douglas-Denton, R.; Hughson, M.D.; Bertram, J.F. Determinants of glomerular volume in different cortical zones of the human kidney. J. Am. Soc. Nephrol. 2005, 16, 3102–3109. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, R.L.; Forbes, M.S. Generation and evolution of atubular glomeruli in the progression of renal disorders. J. Am. Soc. Nephrol. 2008, 19, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, R.L. The proximal tubule is the primary target of injury and progression of kidney disease: Role of the glomerulotubular junction. Am. J. Physiol. Ren. Physiol. 2016, 311, F145–F161. [Google Scholar] [CrossRef] [PubMed]
- Ramot, Y.; Brauner, R.; Kang, K.; Heymach, J.V.; Furtado, S.; Nyska, A. Quantitative evaluation of drug-induced microvascular constriction in mice kidney using a novel tool for 3D geometrical analysis of ex vivo organ vasculature. Toxicol. Pathol. 2014, 42, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Advani, A.; Connelly, K.A.; Yuen, D.A.; Zhang, Y.; Advani, S.L.; Trogadis, J.; Kabir, M.G.; Shachar, E.; Kuliszewski, M.A.; Leong-Poi, H.; et al. Fluorescent microangiography is a novel and widely applicable technique for delineating the renal microvasculature. PLoS ONE 2011, 7, e24695. [Google Scholar] [CrossRef] [PubMed]
- Scruggs, B.S.; Zuo, Y.; Donnert, E.; Ma, L.; Bertram, J.F.; Fogo, A.B. Increased capillary branching contributes to angiotensin type 1 receptor blocker (ARB)-induced regression of sclerosis. Am. J. Pathol. 2011, 178, 1891–1898. [Google Scholar] [CrossRef] [PubMed]
- Torres, R.; Velazquez, H.; Chang, J.J.; Levene, M.J.; Moeckel, G.; Desir, G.V.; Safirstein, R. Three-Dimensional Morphology by Multiphoton Microscopy with Clearing in a Model of Cisplatin-Induced CKD. J. Am. Soc. Nephrol. 2016, 27, 1102–1112. [Google Scholar] [CrossRef] [PubMed]
- Giuvărăşteanu, I. Scanning electron microscopy of vascular corrosion casts-standard method for studying microvessels. Rom. J. Morphol. Embryol. 2007, 48, 257–261. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Case 1 | Case 2 | Case 3 | Case 4 |
|---|---|---|---|---|
| Age (years) | 78 | 78 | 86 | 71 |
| Height (cm) | 171 | 164 | 160 | 168 |
| Weight (kg) | 63 | 53 | 54 | 68 |
| BMI (kg/m2) | 21 | 20 | 21 | 24 |
| BUN (md/dL) | 17 | 15 | 18 | 18 |
| Creatinine (mg/dL) | 0.91 | 0.96 | 0.80 | 1.27 |
| eGFR (mL/min/1.73 m2) | 61 | 59 | 69 | 43 |
| CKD stage | 2 | 3a | 3a | 3b |
| %Glomerular sclerosis | 9 | 17 | 11 | 32 |
| Creatinine at 6 month after surgery (mg/dL) | 1.3 | 1.5 | 1.2 | 2.1 |
| %Interstitial fibrosis | 5 | 7 | 11 | 14 |
| Mean Gl diameter (µm) | 158 ± 18 | 161 ± 10 | 187 ± 22 * | 162 ± 28 |
| Gl density (/mm2 cortex) | 4.4 | 3.7 | 2.5 | 2.7 |
| Tumor pathology | Clear cell ca. 3.0 × 3.0 cm | Clear cell ca. 4.7 × 4.7 cm | Clear cell ca. 3.8 × 3.9 cm | Chromophobe ca. 2.6 × 2.4 cm |
| Stage of tumor (UICC) | Stage I | Stage I | Stage I | Stage I |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uesugi, N.; Shimazu, Y.; Kikuchi, K.; Nagata, M. Age-Related Renal Microvascular Changes: Evaluation by Three-Dimensional Digital Imaging of the Human Renal Microcirculation Using Virtual Microscopy. Int. J. Mol. Sci. 2016, 17, 1831. https://doi.org/10.3390/ijms17111831
Uesugi N, Shimazu Y, Kikuchi K, Nagata M. Age-Related Renal Microvascular Changes: Evaluation by Three-Dimensional Digital Imaging of the Human Renal Microcirculation Using Virtual Microscopy. International Journal of Molecular Sciences. 2016; 17(11):1831. https://doi.org/10.3390/ijms17111831
Chicago/Turabian StyleUesugi, Noriko, Yoshihito Shimazu, Kazunori Kikuchi, and Michio Nagata. 2016. "Age-Related Renal Microvascular Changes: Evaluation by Three-Dimensional Digital Imaging of the Human Renal Microcirculation Using Virtual Microscopy" International Journal of Molecular Sciences 17, no. 11: 1831. https://doi.org/10.3390/ijms17111831