1. Introduction
In 2012, 14.1 million new cancer cases were diagnosed worldwide and 8.2 million cancer patients passed away and more than 32.6 million people were living with cancer (within 5 years of diagnosis). About 57% (approximately 8 million) of new arising cancer cases, 65% (approximately 5.3 million) deaths of cancer and 48% (approximately 15.6 million) of the 5-year prevalent cancer cases have taken place in underdeveloped areas [
1]. Surgery, radiotherapy and chemotherapy have been the main approaches for treating cancer in previous decades. Since Dana R. Leach first proposed an immune checkpoint blockade in 1996 [
2], the first immune checkpoint inhibitor was approved by the FDA in 2011. By 2013, the cover report of science showed the new weapon of immunotherapy against cancer and the new therapeutic approach of using immune checkpoint inhibitors as anticancer agents was a landmark innovation. Undoubtedly, PD-1(Programmed cell death protein 1)/PD-L1(Programmed death-ligand 1) became the brightest star in 2015, after president Carter’s tumor was cured using anti-PD-1 antibody.
At least two signaling pathways need to be stimulated for the activation of cytotoxic T lymphocytes (CTLs) in secondary lymphoid tissues: Firstly, the binding occurs between peptide-MHC (major histocompatibility complex) complex with the availability of antigen presenting cells (APCs) and T cell receptors (TCRs). Then, the B7 molecules on APC interact with the CD28 receptors of T cells. It is noticeable that some experimental data suggests that a third necessary signal (such as IL-12, Type I IFN and adjuvant) plays a very important role in determining the fate of naïve CD8 T cells, tolerance or full activation [
3]. Although less well studied, there is evidences of naïve CD4 T cells requiring a cytokine-dependent ′signal 3′ for a productive response to Ag and may be complementary to IL-1 [
4]. Cellular immunity mediated by T cell is strictly supervised and controlled by a check/balance system performed though many stimulatory and inhibitory molecules. The inhibitory receptors, also called immune checkpoints, regulate CTLs activation and effector function to maintain self-tolerance and limit bystander tissue damage as an indirect consequence of immune response against pathogenic invasion [
5]. Targeting PD-1 and PD-L1, the immune checkpoint blockade agents could reactivate cytotoxic T cells to eliminate tumor cells.
This review will introduce PD-1, PD-L1 as well as the signaling pathway. It will also highlight the clinical development and research progress of the anti-PD-1 and anti-PD-L1 mAbs for managing categories of cancers. Except that, we interpret the aptamer that may become the next generation of PD-1/PD-L1 inhibitors and update the progress of tolerance mechanisms on PD-1/PD-L1 antibodies.
3. Programmed Death 1 Inhibitors
In 1996, Jim Allison’s group found that anti-CTLA-4 could boost anti-tumor response of T cell, which proved the immune checkpoint blocking in tumor therapy for the first time [
2]. Through 10 years’ tough clinical research, the FDA finally approved the ipilimumab in 2011. Except for the different efficacy profile, the immune-related adverse events (irAEs), which were studied in-depth and accepted by the FDA, were regarded as an example of a new immunotherapy safety [
41] which drove the clinical trials of the PD1 and PD-L1 antibody. Because of the lessons learned from ipilimumab and tremelimumab, nivolumab and pembrolizumab was marketed without difficulty in 2014.
3.1. Nivolumab
Nivolumab (BMS-936558 or MDX1106b) is a human IgG4 antibody against PD-1, lacking detectable antibody-dependent cellular toxicity (ADCC). It is manufactured by Bristol-Myers Squibb Company Princeton and has been approved by the FDA for the use of unresectable or metastatic melanoma, metastatic NSCLC and advanced renal cell carcinoma (
Table 1).
3.1.1. Unresectable or Metastatic Melanoma
3.1.2. Metastatic Non-Small Cell Lung Cancer
3.1.3. Renal Cell Carcinoma
A phase 3 study in 821 renal-cell carcinoma patients who have experienced previous treatment was completed in comparing nivolumab(OS 25.0 months) with everolimus(OS 19.6 months). OS benefit was significantly confirmed even if the expression of PD-L1 could not be detected. The hazard ratio for death was 0.73 (98.5% CI, 0.57 to 0.93;
p = 0.002) when nivolumab was combined with everolimus [
45].
Table 6 displays further information.
3.1.4. Adverse Reactions
After the immune checkpoints were blocked, the balance between the autoimmunity and immune tolerance were broken as well. Newly generated dysimmune toxicities created immune-meditated adverse reactions (IMARs) caused by the new immunotherapy. For instance, immune-mediated pneumonitis, colitis, hepatitis, endocrinopathies, rash, encephalitis and other immune-mediated adverse reactions were observed as IMARs. Immune-mediated pneumonitis, colitis, hepatitis, nephritis and renal dysfunction, meant patients required the use of corticosteroids and had no clear alternative etiology, which can occur with nivolumab treatment. Immune-mediated edocrinopathies and rash mainly occurred in combination with ipilimumab. A total of 8,490 patients received nivolumab as a single agent or in combination with ipilimumab in all clinical trials. Fortunately, less than 1.0% of them were confirm as having encephalitis. As well as less than 1.0% of patients were regarded as having severe in fusion when using nivolumab as a single-agent. In only one patient (0.3%) did fatal limbic encephalitis occur, after receiving nivolumab after 7.2 months of exposure. Others were administered with corticosteroids. In addition, the fetus could be harmed when pregnant woman received nivolumab treatment, based on data from animal studies.
In clinical trials, the most common adverse reactions experienced (≥20%) in melanoma were fatigue, musculoskeletal pain, rash and pruritus when nivolumab acted as a single-agent. Patient symptoms when Nivolumab was used in combination with ipilimumab were rash, pruritus, headache, vomiting and colitis.
The most common adverse reactions (≥20%) in patients with metastatic NSCLC were fatigue, musculoskeletal pain, decreased appetite, cough and constipation, based on clinical trials experience.
Just like other therapeutic proteins, nivolumab also has the potential of immunogenicity. 73 patients (11.4%) was tested positive for anti-nivolumab antibodies because of the treatment and using an electrochemiluminescent (ECL) assay in all 639 patients. In five patients (0.8%), anti-nivolumab neutralizing antibodies were detected as well. In combinational therapy with ipilimumab, 23 patients were tested positive for treatment-arising anti-nivolumab antibodies though ECL assay and neutralizing antibodies, anti-nivolumab were inspected at one patient.
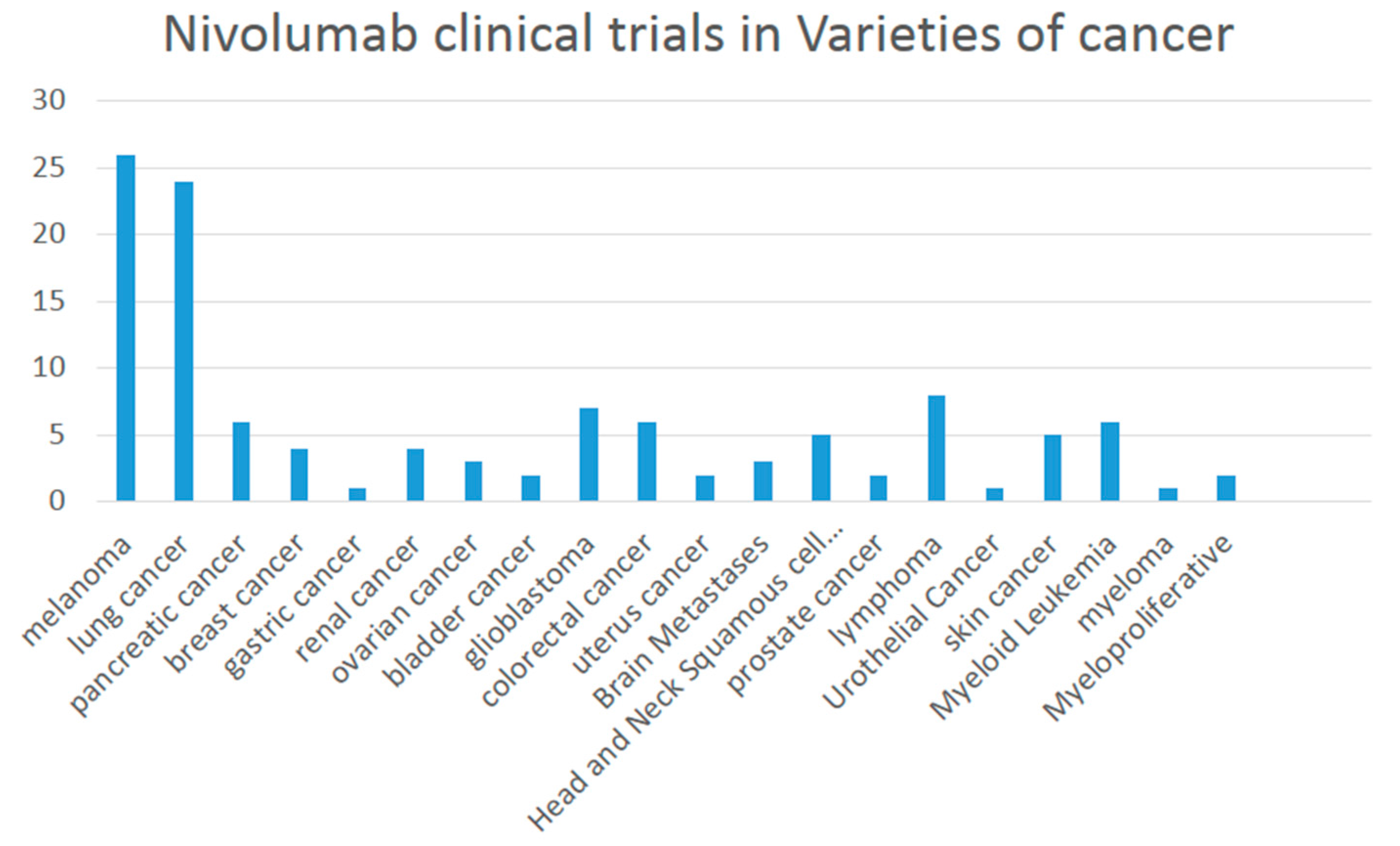
3.1.5. Recruiting Clinical Trials of Nivolumab
There are 121 studies found in ClinicalTrials.gov searching for “Nivolumab | Recruiting”. A variety of melanoma are involved including lung cancer, breast cancer, bladder cancer and renal cancer (
Figure 1) when combined or compared with multiple medicines such as Ipilimumab, Pembrolizumab, Dabrafenib, Trametinib, Placebo, Omaveloxolone Capsules, sunitinib, BMS-936558 (MDX1106-04), Fotemustine and HyperAcute
®-Melanoma (HAM) Immunotherapy.
3.2. Pembrolizumab
Pembrolizumab (MK-3475, lambrolizumab, KEYTRUDA) is an highly specific anti-PD-1 humanized IgG4 κ isotype antibody that contains a mutation at C228P designed to prevent Fc-mediated cytotoxicity. It can disrupt the engagement of PD-1 and PD-L1, resulting in tumor recognition by cytotoxic T cells.
It is approved by the FDA for the treatment of the patients suffering with unresectable or metastatic melanoma and patients with metastatic NSCLC. Accordingly, the PD-L1 expression level has to be detected in determining whether the patients receive pembrolizumab or not. Otherwise, their disease continued to progress on or after chemotherapy platinum. In the case of patients with EGFR or ALK, genomic aberrations had disease progression on other prior FDA-approved therapy before receiving pembrolizumab.
3.2.1. Pembrolizumab in Melanoma
Ipilimumab-Naive Melanoma
The safety and efficacy of pembrolizumab were well demonstrated in Ipilimumab-Naive Melanoma. The affirmed 6-month PFS rates were 47.3% for the patients receiving pembrolizumab every 2 weeks contrasting with 46.4% for every 3 weeks and 26.5% for ipilimumab, with 12-month survival rates: 74.1%, 68.4% and 58.2%, respectively. The improving response rate, regardless of the interval of pembrolizumab being administered; whether every 2 weeks (33.7%) or every 3 weeks (32.9%), as compared with ipilimumab (11.9%). The response rates were ongoing in 89.4%, 96.7%, and 87.9% of patients, respectively. All the data supports the efficiencies were similar in two pembrolizumab patients groups. The adverse events rates referring to treatment of grade 3 to 5 severity were lower in the pembrolizuma patients (13.3% and 10.1%) than in the ipilimumab patients (19.9%) [
46,
47] (
Table 7). These clinical trials suggests there are statistically significant improvements in OS and PFS for patients receiving pembrolizumab in Ipilimumab-Naive Melanoma.
Ipilimumab-Refractory Melanoma
A safety and efficacy phase II trial of pembrolizumab were evaluated in Ipilimumab-Refractory Melanoma. In this trial by active comparator arms, the pembrolizumab group had significantly improved PFS and ORR but not OS (although OS data are immature), when compared with BRAF/MEK inhibiting chemotherapy in ipilimumab-refractory patients with BRAF-mutation positive [
47,
48,
49,
50,
51] (
Table 8). After an analysis of 220 deaths, there was no statistically significant difference between pembrolizumab and chemotherapy, regardless of the dosage of pembrolizumabpembrolizumab, 2 mg/kg or 10 mg/kg (
Table 8).
3.2.2. Pembrolizumab in Non-Small Cell Lung Cancer
Altogether, 280 patients were involved in a multi-center, open-label multi-cohort, activity-estimating study. The sub-group defining was retrospectively analyzed using an analytically validated assay for PD-L1 expression TPS (tumor proportion score). Of a total of 280 patients, 61 were defined as highly expressed for PD-L1 with partial response, consequently the confirmed ORR reached to 41% (
Table 9). In 25 ORR patients, 21 (84%) had duration response, as well as 11 patients (44%) who had ongoing response to ≥6 months [
52].
3.2.3. Adverse Reactions
In clinical trials research, the adverse reactions reported in ≥20% of patients were fatigue, pruritus, rash, constipation, diarrhea, nausea with decreased appetite and fatigue, dyspnea and cough in NSCLC.
In total, 2117 patients with melanoma, 1567 NSCLC 550 patients, pembrolizumab caused some immune-mediated adverse reaction such as immune-mediated pneumonitis, colitis, hepatitis, endocrinopathies, nephritis and renal dysfunction. The exact percentage is shown in (
Table 10).
Similar to other therapeutic proteins, the immunogenicity risk for pembrolizumab was observed in clinical studies. The anti-pembrolizumab antibody were detected in 1 (0.3%) of 392 patients which were verified positively in the neutralizing assay.
3.2.4. Clinical Trials on Recruiting
There were 178 studies in the ClinicalTrials.gov with recruited participants distributed throughout the world. The 178 clinical trials used pembrolizumab in many varieties of cancer, including melanoma, lung, ovarian, breast, glioma, renal, adrenocortical carcinoma, colorectal, pancreatic, gastric, endometrial, mesothelioma, bladder cancer and so on (
Figure 2).
3.3. Pidilizumab
Pidilizumab targeting PD-1 is derived from BAT, a the mouse monoclonal antibody, and it was humanized to IgG 1κ [
53]. In preclinical studies, CT-011 and BAT had successfully suppressed the tumor growth within melanoma, lymphoma, lung, colon and breast tumors and furthermore it extended the survival of tumor-bearing mice, both NK and T cell involved [
54,
55,
56,
57]. The Phase I study has affirmed the safety and pharmacokinetic of pidilizumab in advanced ematologic malignancies. Fortunately, there was no observed treatment or infusion-related serious adverse events [
58]. Pharmacokinetic analyses show the Cmax (maximum concentration) and the AUC (area under the curve) of CT-011 in serum increasing dose with a median of t1/2 from 217 to 410 h. The peripheral blood CD4+ lymphocytes rose unremittingly until the 21st. day after CT-011 treatment.
Researchers designed a single group, open-label phase 2 trial, for assessing the safety and activity of the combination between Pidilizumab and Rituximab in relapsed Follicular Lymphoma patients. It was demonstrated that no autoimmune or therapy-related grade 3/4 toxicities were observed. Anemia (14 patients) and fatigue (13 patients) were the most frequent grade 1 adverse symptoms and 5 patients were defined as having respiratory infection with a grade 2 adverse event. Overall response rates were 66% (19/29), 15 being complete response rates. In total, 25/29 (86%) of the patients had tumor regression within 18.8 months (95% CI: 14.7 months to not reach) of median progression-free survival. Nineteen responders had 20.2 months (95% CI: 13.9 months to not reached) of median response duration [
53].
The clinical activity of PD-1 blockade was confirmed in diffused large B-cell lymphoma (DLBCL) using a phase II trial (NCT00532259). After autologous hematopoietic stem-cell transplantation for DLBCL, the overall response rate of pidilizumab treatment has been reported as reaching 51% which presents a promising strategy of PD-1 blockade therapy. It is demonstrated in DLBCL for the first time. A total of 613 adverse events took place in 69 (96%) patients and 135 were regarded as treatment-related. Neutropenia (19%) and thrombocytopenia (8%) became the most common grade 3 to 4 adverse events but the neutropenia could be managed by growth factor treatment and remaining in asymptomatic. Sadly, one patient died due to herpes zoster infection after the third dose of pidilizumab, but is not related to this study treatment. At least 32% (23/72) of patients suffered one serious adverse event each with three undergoing a related serious adverse event. The evidence of significant autoimmune toxicity, infusion reactions and treatment related mortality have not yet been found [
59].
Pidilizumab was studied in another two Phase 2 clinic trials on aggressive and indolent lymphomas which appeared in clinical activity of PD-1/PD-L1 positive lymphocytes. Then Michael B etc. initiated a large Phase 2 study to assess the safety and efficacy of pidilizumab in metastatic melanoma (MM) patients. It resulted in a substantial 12 month survival rate in heavily pretreated patients and was very well tolerated. It appears comparable to other anti- PD-1 MAbs in 12 months survival [
60].
There were also two clinical trials but these were suspended due to a Pidilizumab (CT-011) licensing transfer and Pharmaceutical Companies decision. Two further clinical trials with Chronic Hepatitis C Genotype and Hepatocellular Carcinoma were terminated. The study of PD-1 blockading in combination with DC/AML vaccine and subsequent chemotherapy to induce remission is being sought. A Stage III-IV diffuse large B-cell lymphoma trial is requesting volunteer patients as well.
3.4. AMP-224
The curative effects of nivolumab and pembrolizumab are very encouraging [
61]. However, targeting the PD-1 has the potential to prevent differentiated development [
62,
63]. Amplimmune and GlaxoSmithKline are assessing the safety and efficiency of a new arising PD-1 targeting agent, AMP-224. It is a fusion protein consist of the extracellular domain of PD-L2 and the Fc region of human IgG [
64]. Contrasting to nivolumab and pembrolizumab, AMP-224 does not just perform as a blockading agent. It is hypothesized that AMP-224 could deplete PD-1 highly expressed T-cells, which referred to as exhausted effector cells, ADCC or CDC. Following restoration of the T-cell cohort with normal function may reestablish immune ability [
2,
3]. AMP-224 was well-tolerated up to its maximum administered dose of 30 mg/kg, with manageable infusion reactions in the majority of patients. The trial is ongoing, including monitoring for clinical activity [
65].
Preclinical studies utilizing a murine AMP-224 in syngeneic murine tumor models show anti-tumor activity as a single agent which could be enhanced after the combination of low dose cyclophosphamide (unpublished data Amplimmune, Inc, Gaithersburg, MD, USA).
A pilot research of AMP-224 combined with stereotactic body radiation therapy (SBRT) in patients with metastatic colorectal cancer was reported at the 2015 Gastrointestinal Cancers Symposium. A few other preclinical studies have reported an increase in peripheral anti-tumor immune activity, consequently with radiation for “abscopal effect”. The PD-L1 expression of tumor cells could also been induced by radiation, so the aim of this study is to assess whether the radiation therapy enhanced anti-tumor immunity of anti-PD-1 therapy (with AMP-224) or not. However, the clinical trial information is not yet complete [
66].
3.5. MEDI0680
MEDI0680 (AMP-514) is a humanized IgG monoclonal antibody targeting human PD-1. It could also improve the cytotoxicity of T cells though inducing the internalization of PD-1 [
67,
68]. There are three ongoing clinic trails: NCT02271945 is a Phase 1b/2 open-label study to evaluate the safety/efficacy of MEDI-551 + AMP-514 in participants with relapsed or refractory aggressive B-cell lymphomas who have failed 1–2 prior lines of therapy; NCT02013804 is a dose-escalation study to test the safety, tolerability, PK, immunogenicity and anti-tumor activity in adult patients bearing solid tumors; NCT02118337 is a combinational trail to assess the safety and tolerability of AMP-514, with MEDI4736 (Anti-PD-L1 Antibody).
3.6. REGN2810
REGN2810 is a fully human hinge-stabilized IgG4 monoclonal Ab that binds to the extracellular domain of human PD-1 with high affinity and specificity inhibiting interaction of PD-1 with its ligands [
69]. Elena Burova et al. generated a mouse with human PD-1 gene knock-in allowing direct testing of our anti-human PD-1 Ab. Human PD-1 knock-in mice express a hybrid protein containing the extracellular portion of human PD-1 with transmembrane and intracellular domains of mouse PD-1. We demonstrated functional PD-1/PD-L1 signaling and immune responses in this model and confirmed REGN2810 binding to hybrid PD-1 receptor on mouse T cells in vivo, following REGN2810 injections. Prophylactic and therapeutic treatments of subcutaneous syngeneic tumors with REGN2810 in human PD-1 knock-in mice resulted in a dose-dependent suppression of tumor growth [
69,
70].
Three phase I clinic trials are commencing at clinicaltrials.gov. NCT02383212 is an open-label, multi-center, ascending-dose escalation study of REGN2810, alone and in combination with other anti-cancer therapies in patients with advanced malignancies on recruiting. NCT02651662 is calling for participants in patients with lymphoma. It is an open-label, multi-center, dose escalation study of REGN2810 as single-agent. NCT02520245 has been designed to collect long-term follow-up information for patients who received REGN2810 in other clinical studies and to allow re-treatment for eligible patients not yet recruiting.
3.7. PDR001
PDR001 is a high-affinity, ligand-blocking, humanized anti-PD-1 IgG4 antibody that blocks the binding of PD-L1 and PD-L2 to PD-1. As a signal agent, NCT02678260, NCT02605967 and NCT02404441 are on phase I/II. NCT02404441 and is the “first-in-human” study of PDR001 to characterize the safety, tolerability, pharmacokinetics (PK), pharmacodynamics (PD) and anti-tumor activity of PDR001 administered i.v. as a single agent, to adult patients with solid tumors. The purpose of NCT02678260 is to characterize the safety, tolerability, Pharmacokinetics (PK) and anti-tumor activity of PDR001 administered intravenous as a single agent to Japanese patients. The randomized controlled of NCT02605967 Phase II study is to assess the efficacy of PDR001 versus investigator's choice of chemotherapy in patients with advanced NPC. Another two agents (NCT02608268 and NCT02460224) were in combination with MBG453 or LAG525.
3.8. PD-1 Antibody in China
China has overtaken India becoming the largest biosimilar discovering country from Cortellis Competitive Intelligence, according to Thomson Reuters report in 2015. It mirror the investment environment’s expectation to Chinese biosimilars. There is no doubt that the development of biosimilar will make up for the massive unsatisfied clinic demand in diabetes, tumor and immunological diseases.
Nivolumab and pembrolizumab have submitted an application for clinic trials, but most are in assessing, except for a clinic trial of nivolumab (JXSL1300032). As expected, there are many ongoing PD-1 antibodies discoveries in China. According to incomplete statistics, two have reached clinical trials and a further two are in assessment (
Table 11).
5. Prospects
To date, three therapeutic antibodies targeting the PD-1/PD-L1 signal pathway have been approved by the FDA in the use of metastatic melanoma, NSCLC, renal cell cancer or urothelial carcinoma, with several others in clinical trials in preparation for release to the open market (
Table 15) [
84]. It is predicted that some will be approved.
Varied response towards immunotherapy has resulted from the different immune backgrounds of patients. The immune background is dependent on many substances with the immunogenicity a person has in their immune system being determined in the womb. However, the gut microbiota plays a most important role in shaping the systemic immune responses [
85,
86,
87]. Ayelet Sivan demonstrate the commensal Bifidobacterium could promote antitumor immunity and facilitate anti-PD-L1 activity in cancer [
88]. So, it is possible to manipulate microbiota to modulate cancer immunotherapy. On the other hand, it has been a long journey for Ipilimumab due to the low responsible rate compared to small molecular drugs or other therapeutic antibodies. Similarly, the responsible rate of PD-1/PD-L1 antibodies were still low as immunotherapeutic antibodies. Most researchers view that the different performances in a variety of people are due to the individual immune system and tumor driven mutation. However, which gene has been a mystery, until recently. A researcher from University of California, Los Angeles found that highly mutational loads co-related with optimistic survival and the responding patients’ tumors are abundant with mutations in BRCA2. Similarly, mitogen-activated protein kinase (MAPK) inhibited therapy induces similar characteristics in melanoma, which indicate that non-genomic MAPK inhibitor resistance has the cross-resistance within anti-PD-1 therapy [
89].
To address the immune-related adverse effects of mAbs and get more penetration in solid tumors, some peptides based on immune checkpoint blockers were discovered. A therapeutic peptide targeting PD-1/PD-L1 signal pathway for cancer immunotherapy, AUNP-12 (AUR-12/Aurigene-012) was co-developed by Aurigene Discovery Technologies and Pierre Fabre Laboratories and is currently undegoing preclinical study [
84]. The sequence is still secret. Although it has shown valid antitumor activity, the druggability pharmacokinetic profile was too short. Some hydrolysis-resistant D-peptides were discovered as PD-L1 antagonists developed by using mirror-image phage display [
90]. The highest affinity of Kd = 0.51 μM has shown inhibited tumor growth and prolonged animal survival.
Otherwise, there was one patent relating to small drug-like inhibitors. It was filed by Bristol-Myers Squibb in 2015 WO 2015/034820 A1 (priority to US 61/873,398). The compound and its ramification could inhibit the interactions between PD-1 and PD-L1 having IC50 values between 0.006 and 0.10 mM. It should be noted that Curis, Inc. (Nasdaq:CRIS, Lexington, MA, USA) announced the FDA has accepted the company’s Investigational New Drug (IND) application for CA-170 at 1 June 2016. CA-170 is the first orally available small molecule targeting and inhibiting the immune checkpoints, PD-L1 and V-domain Immunoglobulin Suppressor of T-cell Activation (VISTA).
Since the regulatory approval of ipilimumab in 2011, immuno-oncology has not only grown rapidly but also inspired the entire pharmaceutical industry. Dozens of new technologies and investments in immune-oncology have soared overnight, especially since
Science magazine in 2013 reported cancer immunotherapy as the breakthrough of the year [
91]. Between 2014 and 2015, immune-oncology technologies and business deals led to extreme valuations and the market is expected to reach US $35 billion by 2023 [
92]. Axel Hoos also reviewed or forecast three generations of immuno-oncology drugs. Generation 1 encompasses the initiating antibodies of the immune-oncology era, such as ipilimumab and sipuleucel‑T (autologous dendritic cell therapy developed by Dendreon), which were approved respectively in 2011 and 2010 [
93,
94]; and then immune-oncology drugs rapidly develop to next generation agents against new targets and new emerging mechanisms, which are represented by the PD-1 and PD-L1 antibodies. A bi‑specific T cell adaptor (BITE), blinatumomab (Amgen) targeting CD19 + B cell malignancies and T cell, was also approved in 2015 [
95,
96,
97]. Generation 3 will be various immune-oncology modalities combined with adaptive immunity and innate immunity. In other words, establishing the best combination of therapies and drugs is under development. Further development of PD-1/PD-L1 pathway inhibitors are expected to be a powerful weapon in the fight against cancers.
We expected more PD-1 (or PD-L1) inhibitors to show excellent results at immune checkpoints in reactivating the adaptive or innate immunity for defeating cancers. However, antibody drugs have some insurmountable disadvantages, such as high immunogenicity [
98], high cost, low stability and low production [
99]. Undoubtedly, the marketed two PD-1 antibodies have been reported with anti-antibodies which weaken the therapeutic effect. The anti-antibody of nivolumab (OPDIVO) has reached up to 12.6% (67/532) and so a new solution may be required. The aptamer with minimal immunogenicity [
100], low cost [
101], high production [
101] and high stability [
99] may became the key to solving the puzzle. More and more anti-tumor drugs will be investigated until we overcome cancer.






{kind=link}
{kind=link}