
Diagnostic Value of Serum Angiogenesis Markers in Ovarian Cancer Using Multiplex Immunoassay

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Usefulness of Angiogenesis Factors in Diagnosing Ovarian Cancer
2.2. Usefulness of Angiogenesis Factors in Distinguishing Ovarian Cancer Types
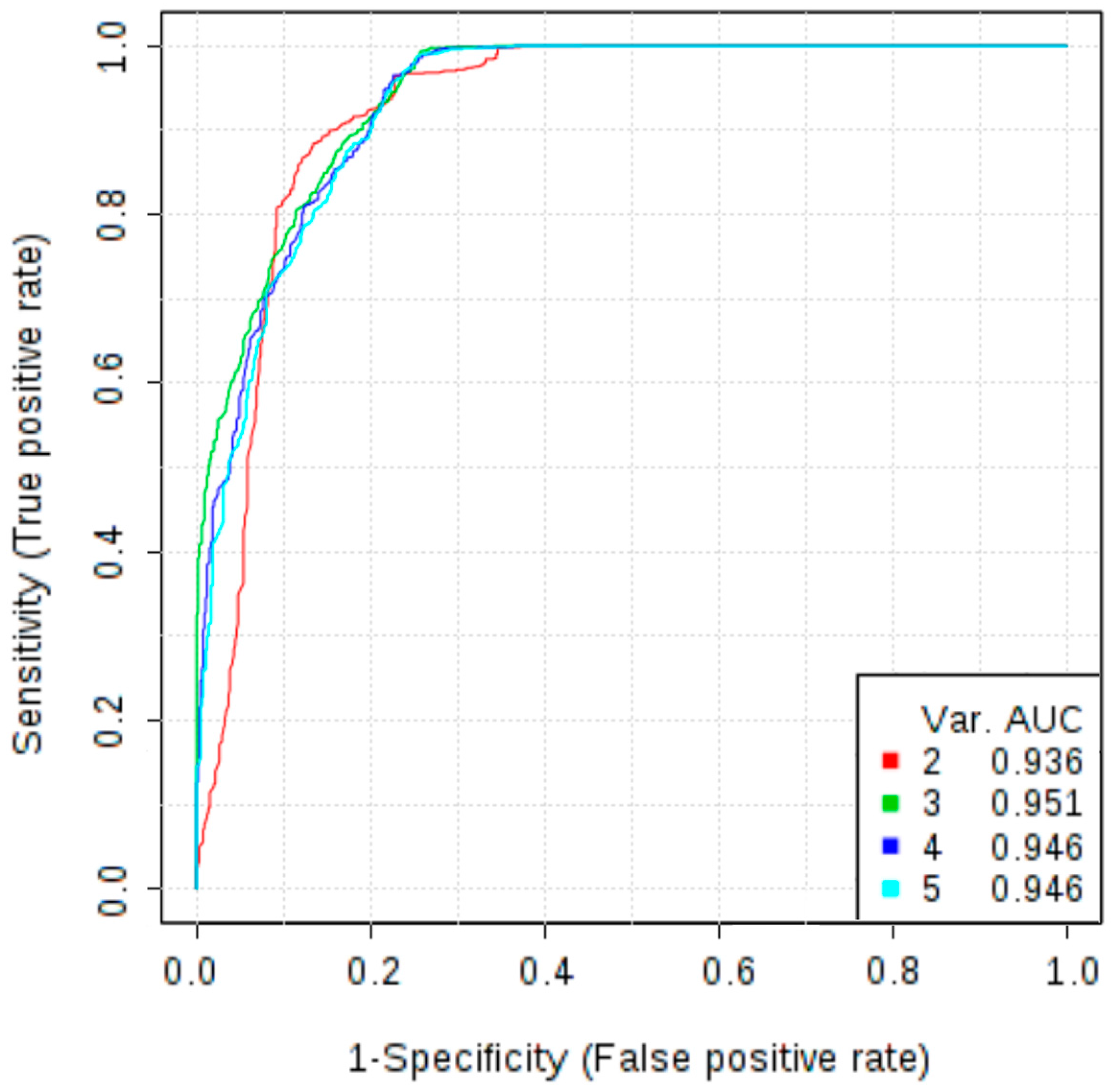
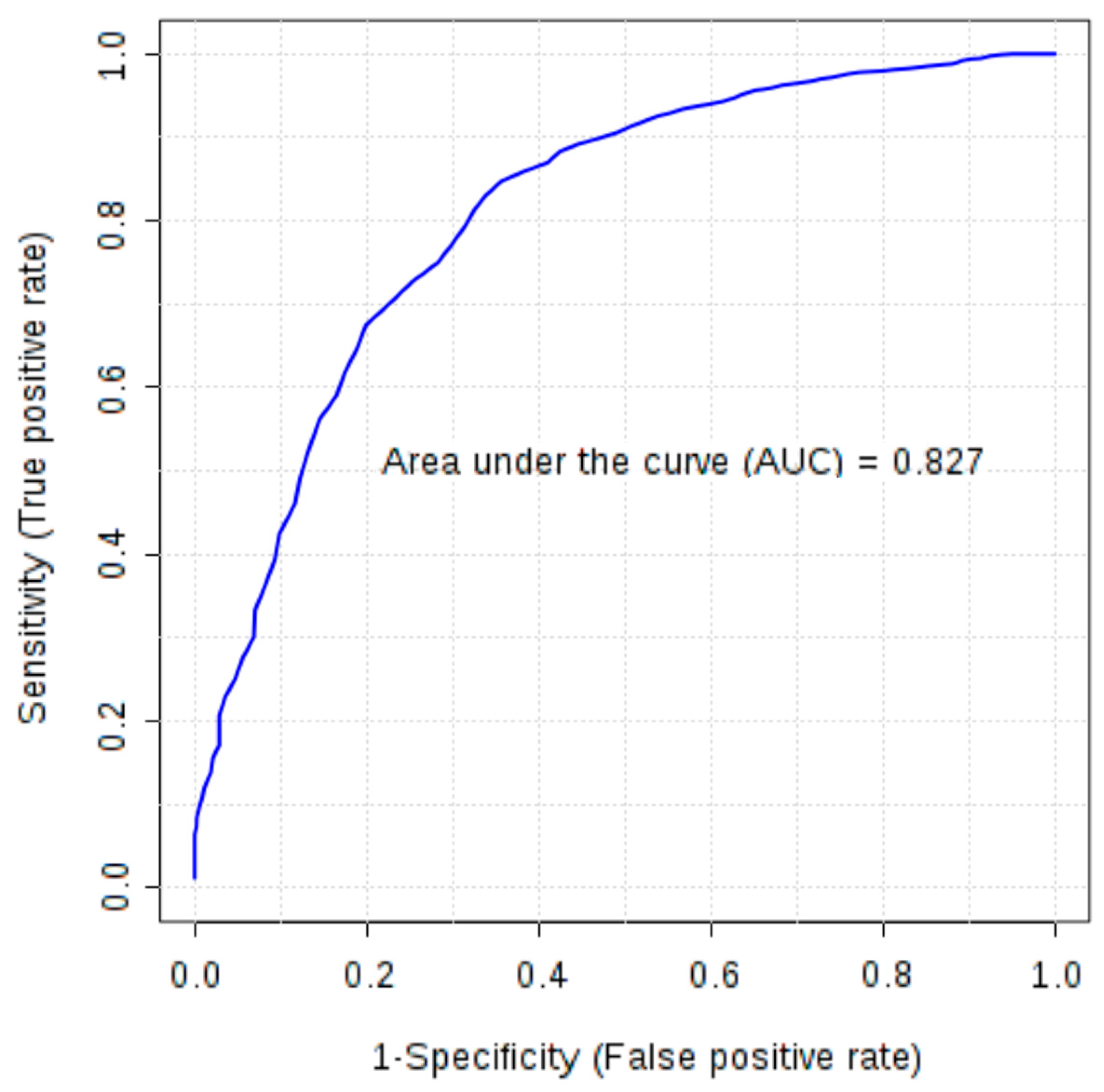
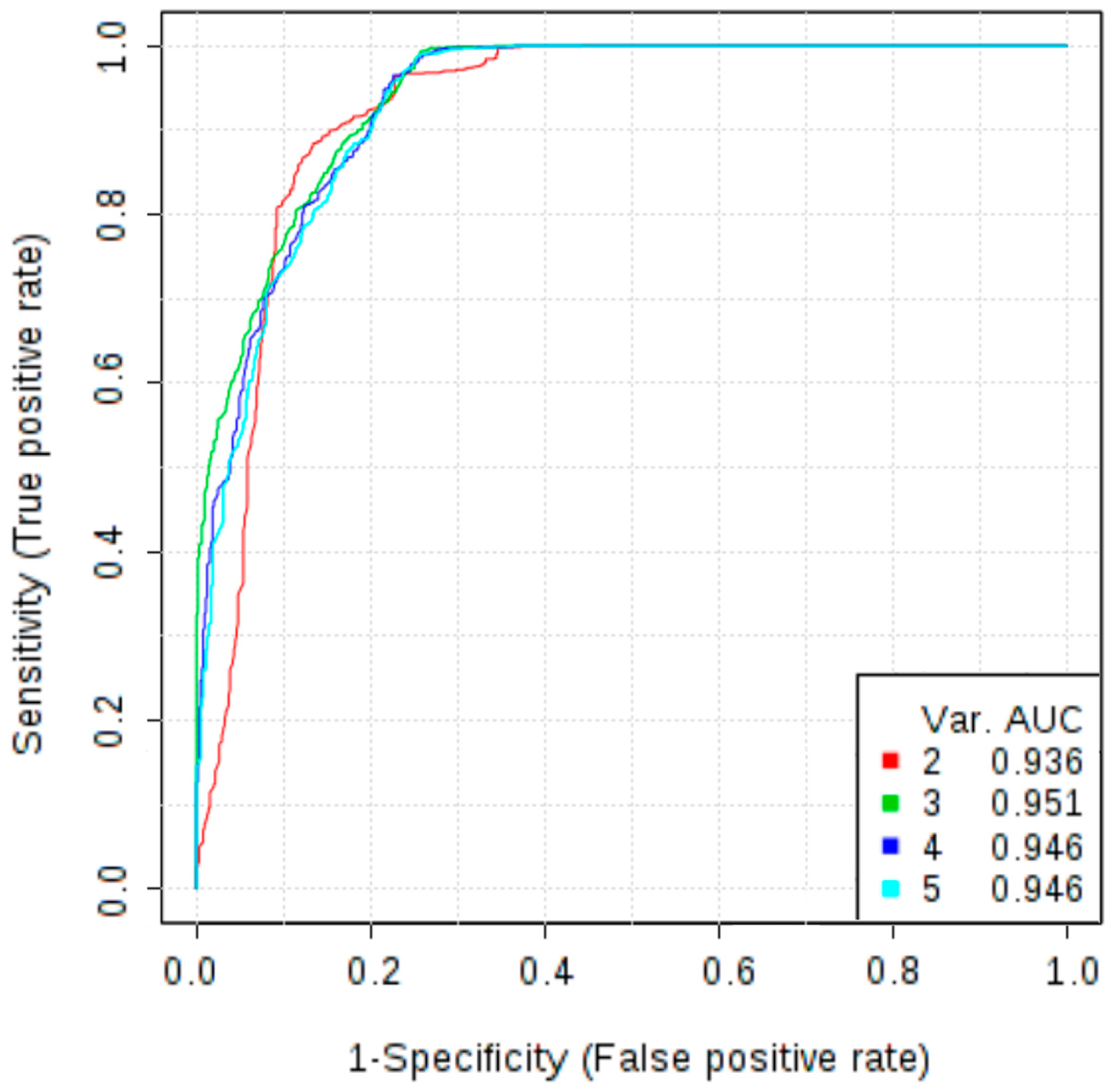
2.3. Usefulness of Angiogenesis Factors in Differential Diagnosis of Ovarian Tumours
3. Discussion
4. Methods
4.1. Patient Characteristics
4.2. Measurement of Angiogenesis Panel
4.3. Data Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of interest
References
- Ferlay, J.; Shin, H.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D. GLOBOCAN 2008 v2.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 10. Available online: https://www.iarc.fr/en/media-centre/iarcnews/2010/globocan2008.php (accessed on 1 September 2016).
- Heintz, A.P.M.; Odicino, F.; Maisonneuve, P.; Quinn, M.A.; Benedet, J.L.; Creasman, W.T.; Ngan, H.Y. S.; Pecorelli, S.; Beller, U. Carcinoma of the ovary. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int. J. Gynaecol. Obstet. 2006, 95, 161–192. [Google Scholar] [CrossRef]
- Doubeni, C.A.; Doubeni, A.R.; Myers, A.E. Diagnosis and Management of Ovarian Cancer. Am. Fam. Physician 2016, 93, 937–944. [Google Scholar] [PubMed]
- Enakpene, C.A.; Omigbodun, A.O.; Goecke, T.W.; Odukogbe, A.-T.; Beckmann, M.W. Preoperative evaluation and triage of women with suspicious adnexal masses using risk of malignancy index. J. Obstet. Gynaecol. Res. 2009, 35, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Kurman, R.J.; Shih, I.-M. The Origin and Pathogenesis of Epithelial Ovarian Cancer: A Proposed Unifying Theory. Am. J. Surg. Pathol. 2010, 34, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, J.A.; Goddard, J.C.; Al-Taan, O.; Dennison, A.R.; Morgan, B.; Stephenson, J.A.; Goddard, J.C.; Al-Taan, O.; Dennison, A.R.; Morgan, B. Tumour Angiogenesis: A Growth Area—From John Hunter to Judah Folkman and Beyond. J. Cancer Res. 2013, 2013, 1–6. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Schmidt, T.; Falk, C.S.; Hinz, U.; Herber, M.; Bork, U.; Büchler, M.W.; Weitz, J.; Koch, M.; Jemal, A.; et al. Expression and prognostic value of circulating angiogenic cytokines in pancreatic cancer. BMC Cancer 2011, 11, 286. [Google Scholar] [CrossRef] [PubMed]
- Lawicki, S.; Będkowska, G.E.; Gacuta-Szumarska, E.; Szmitkowski, M. The plasma concentration of VEGF, HE4 and CA125 as a new biomarkers panel in different stages and sub-types of epithelial ovarian tumors. J. Ovarian Res. 2013, 6, 45. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Chiu, H.; Gupta, V.; Chan, D.W. Validation of a multiplex immunoassay for serum angiogenic factors as biomarkers for aggressive prostate cancer. Clin. Chim. Acta 2012, 413, 1506–1511. [Google Scholar] [CrossRef] [PubMed]
- Mousa, L.; Salem, M.E.; Mikhail, S. Biomarkers of Angiogenesis in Colorectal Cancer. Biomark. Cancer 2015, 7, 13–19. [Google Scholar] [PubMed]
- Rykala, J.; Przybylowska, K.; Majsterek, I.; Pasz-Walczak, G.; Sygut, A.; Dziki, A.; Kruk-Jeromin, J. Angiogenesis markers quantification in breast cancer and their correlation with clinicopathological prognostic variables. Pathol. Oncol. Res. 2011, 17, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Bremnes, R.M.; Camps, C.; Sirera, R. Angiogenesis in non-small cell lung cancer: The prognostic impact of neoangiogenesis and the cytokines VEGF and bFGF in tumours and blood. Lung Cancer 2006, 51, 143–158. [Google Scholar] [CrossRef] [PubMed]
- Avastin (Bevacizumab) Official Patient & Caregiver Website. Available online: http://www.avastin.com/patient (accessed on 1 September 2016).
- Kodera, Y.; Katanasaka, Y.; Kitamura, Y.; Tsuda, H.; Nishio, K.; Tamura, T.; Koizumi, F. Sunitinib inhibits lymphatic endothelial cell functions and lymph node metastasis in a breast cancer model through inhibition of vascular endothelial growth factor receptor 3. Breast Cancer Res. 2011, 13, R66. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.; Visintin, I.; Lai, Y.; Zhao, H.; Schwartz, P.; Rutherford, T.; Yue, L.; Bray-Ward, P.; Ward, D.C. Serum protein markers for early detection of ovarian cancer. Proc. Natl. Acad. Sci. USA 2005, 102, 7677–7682. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.U.; Li, H.; Zhang, B. The diagnostic value of serum HE4 and CA-125 and ROMA index in ovarian cancer. Biomed. Rep. 2016, 5, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Sa, M.; Huang, M.; Yang, J.; Xiang, Z.; Liu, B.; Tang, A. The reference intervals for HE4, CA125 and ROMA in healthy female with electrochemiluminescence immunoassay. Clin. Biochem. 2013, 46, 1705–1708. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.; Stordal, B. Erlotinib or gefitinib for the treatment of relapsed platinum pretreated non-small cell lung cancer and ovarian cancer: A systematic review. Drug Resist. Update 2011, 14, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Secord, A.A.; Blessing, J.A.; Armstrong, D.K.; Rodgers, W.H.; Miner, Z.; Barnes, M.N.; Lewandowski, G.; Mannel, R.S. Gynecologic Oncology Group Phase II trial of cetuximab and carboplatin in relapsed platinum-sensitive ovarian cancer and evaluation of epidermal growth factor receptor expression: A Gynecologic Oncology Group study. Gynecol. Oncol. 2008, 108, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.; Guastalla, J.P.; Allouache, D.; Combe, M.; Weber, B.; Cretin, J.; Curé, H.; Nunhuck, S.; Paraiso, D.; Mousseau, M.; et al. HER2 Overexpression/Amplification and Trastuzumab Treatment in Advanced Ovarian Cancer: A GINECO Phase II Study. Clin. Ovarian Cancer 2008, 1, 54–59. [Google Scholar] [CrossRef]
- Martin, L.P.; Sill, M.; Shahin, M.S.; Powell, M.; di Silvestro, P.; Landrum, L.M.; Gaillard, S.L.; Goodheart, M.J.; Hoffman, J.; Schilder, R.J. A phase II evaluation of AMG 102 (rilotumumab) in the treatment of persistent or recurrent epithelial ovarian, fallopian tube or primary peritoneal carcinoma: A Gynecologic Oncology Group study. Gynecol. Oncol. 2014, 132, 526–530. [Google Scholar] [CrossRef] [PubMed]
- Ivy, S.P.; Wick, J.Y.; Kaufman, B.M. An overview of small-molecule inhibitors of VEGFR signaling. Nat. Rev. Clin. Oncol. 2009, 6, 569–579. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.-J.; Armaiz Pena, G.N.; Pradeep, S.; Cho, M.S.; Coleman, R.L.; Sood, A.K. Anti-vascular therapies in ovarian cancer: Moving beyond anti-VEGF approaches. Cancer Metastasis Rev. 2015, 34, 19–40. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, A.; Sawai, H.; Takahashi, H.; Ochi, N.; Matsuo, Y.; Funahashi, H.; Sato, M.; Okada, Y.; Takeyama, H.; Manabe, T. The stem cell factor/c-kit receptor pathway enhances proliferation and invasion of pancreatic cancer cells. Mol. Cancer 2006, 5, 46. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Peng, L.; Fan, K.; Wang, H.; Wei, R.; Ji, G.; Cai, J.; Lu, B.; Li, B.; Zhang, D.; et al. Osteopontin induces angiogenesis through activation of PI3K/AKT and ERK1/2 in endothelial cells. Oncogene 2009, 28, 3412–3422. [Google Scholar] [CrossRef] [PubMed]
- Weber, G.F.; Lett, G.S.; Haubein, N.C. Categorical meta-analysis of Osteopontin as a clinical cancer marker. Oncol. Rep. 2011, 25, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Tilli, T.M.; Franco, V.F.; Robbs, B.K.; Wanderley, J.L.M.; da Silva, F.R.A.; de Mello, K.D.; Viola, J.P.B.; Weber, G.F.; Gimba, E.R. Osteopontin-c splicing isoform contributes to ovarian cancer progression. Mol. Cancer Res. 2011, 9, 280–293. [Google Scholar] [CrossRef] [PubMed]
- Bao, L.H.; Sakaguchi, H.; Fujimoto, J.; Tamaya, T. Osteopontin in metastatic lesions as a prognostic marker in ovarian cancers. J. Biomed. Sci. 2007, 14, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-D.; Chen, H.; Liu, H.-Q.; Hao, M. Correlation between ovarian neoplasm and serum levels of osteopontin: a meta-analysis. Tumour Biol. 2014, 35, 11799–11808. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.-D.; Wei, T.-T.; Yang, M.; Ma, N.; Tang, Q.-Q.; Qin, B.-D.; Fu, H.-T.; Zhong, R.-Q. Diagnostic value of osteopontin in ovarian cancer: A meta-analysis and systematic review. PLoS ONE 2015, 10, 0126444. [Google Scholar] [CrossRef] [PubMed]
- Lan, Z.; Fu, D.; Yu, X.; Xi, M. Diagnostic values of osteopontin combined with CA125 for ovarian cancer: A meta-analysis. Fam. Cancer 2016, 15, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Welt, C.K.; Lambert-Messerlian, G.; Zheng, W.; Crowley, W.F.; Schneyer, A.L. Presence of activin, inhibin, and follistatin in epithelial ovarian carcinoma. J. Clin. Endocrinol. Metab. 1997, 82, 3720–3727. [Google Scholar] [CrossRef] [PubMed]
- Florio, P.; Reis, F.M.; Torres, P.B.; Calonaci, F.; Abrao, M.S.; Nascimento, L.L.; Franchini, M.; Cianferoni, L.; Petraglia, F. High serum follistatin levels in women with ovarian endometriosis. Hum. Reprod. 2009, 24, 2600–2666. [Google Scholar] [CrossRef]
- Ren, P.; Chen, F.-F.; Liu, H.-Y.; Cui, X.-L.; Sun, Y.; Guan, J.-L.; Liu, Z.-H.; Liu, J.-G.; Wang, Y.-N. High serum levels of follistatin in patients with ovarian cancer. J. Int. Med. Res. 2012, 40, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Cao, R.; Björndahl, M.A.; Religa, P.; Clasper, S.; Garvin, S.; Galter, D.; Meister, B.; Ikomi, F.; Tritsaris, K.; Dissing, S.; et al. PDGF-BB induces intratumoral lymphangiogenesis and promotes lymphatic metastasis. Cancer Cell 2004, 6, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Abdollahi, A.; Folkman, J. Evading tumor evasion: current concepts and perspectives of anti-angiogenic cancer therapy. Drug Resist. Update 2010, 13, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Matei, D.; Emerson, R.E.; Lai, Y.-C.; Baldridge, L.A.; Rao, J.; Yiannoutsos, C.; Donner, D.D. Autocrine activation of PDGFRalpha promotes the progression of ovarian cancer. Oncogene 2006, 25, 2060–2069. [Google Scholar] [CrossRef] [PubMed]
- Burger, R.A. Overview of anti-angiogenic agents in development for ovarian cancer. Gynecol. Oncol. 2011, 121, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Madsen, C.V.; Steffensen, K.D.; Olsen, D.A.; Waldstrøm, M.; Søgaard, C.H.; Brandslund, I.; Jakobsen, A. Serum platelet-derived growth factor and fibroblast growth factor in patients with benign and malignant ovarian tumors. Anticancer Res. 2012, 32, 3817–3825. [Google Scholar] [PubMed]
- Madsen, C.; Steffensen, K.; Olsen, D.; Waldstrøm, M.; Smerdel, M.; Adimi, P.; Brandslund, I.; Jakobsen, A.; Folkman, J.; Ferrara, N.; et al. Serial measurements of serum PDGF-AA, PDGF-BB, FGF2, and VEGF in multiresistant ovarian cancer patients treated with bevacizumab. J. Ovarian Res. 2012, 5, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korc, M.; Friesel, R.E. The role of fibroblast growth factors in tumor growth. Curr. Cancer Drug Targets 2009, 9, 639–651. [Google Scholar] [CrossRef] [PubMed]
- Le Page, C.; Ouellet, V.; Madore, J.; Hudson, T.J.; Tonin, P.N.; Provencher, D.M.; Mes-Masson, A.-M. From gene profiling to diagnostic markers: IL-18 and FGF-2 complement CA125 as serum-based markers in epithelial ovarian cancer. Int. J. Cancer 2006, 118, 1750–1758. [Google Scholar] [CrossRef] [PubMed]
- Aune, G.; Lian, A.-M.; Tingulstad, S.; Torp, S.H.; Forsmo, S.; Reseland, J.E.; Stunes, A.K.; Syversen, U. Increased circulating hepatocyte growth factor (HGF): A marker of epithelial ovarian cancer and an indicator of poor prognosis. Gynecol. Oncol. 2011, 121, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Kong, B.; Yang, Q.; Qu, X. Hepatocyte growth factor enhances ovarian cancer cell invasion through down-regulation of thrombospondin-1. Cancer Biol. Ther. 2010, 9, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Ono, Y.J.; Kanemura, M.; Tanaka, T.; Hayashi, M.; Terai, Y.; Ohmichi, M. Hepatocyte growth factor secreted by ovarian cancer cells stimulates peritoneal implantation via the mesothelial-mesenchymal transition of the peritoneum. Gynecol. Oncol. 2015, 139, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Grabowski, J.P.; Markowska, A.; Markowska, J. Evaluation of leptin serum concentrations during surgery and first-line chemotherapy in primary epithelial ovarian cancer patients. Contemp. Oncol. 2014, 18, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Abarzua-Catalan, L.; Trigo, C.; Delpiano, A.; Sanhueza, C.; García, K.; Ibañez, C.; Hormazábal, K.; Diaz, D.; Brañes, J.; et al. Leptin stimulates migration and invasion and maintains cancer stem-like properties in ovarian cancer cells: An explanation for poor outcomes in obese women. Oncotarget 2015, 6, 21100–21119. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Konishi, I.; Mandai, M.; Kuroda, H.; Komatsu, T.; Nanbu, K.; Sakahara, H.; Mori, T. Expression of vascular endothelial growth factor (VEGF) in epithelial ovarian neoplasms: Correlation with clinicopathology and patient survival, and analysis of serum VEGF levels. Br. J. Cancer 1997, 76, 1221–1227. [Google Scholar] [CrossRef] [PubMed]
- Bednarek, W. Markers and modulators of angiogenesis in ovarian cancer. Ginekol. Pol. 2007, 1, 754–763. [Google Scholar]
- Spannuth, W.A.; Nick, A.M.; Jennings, N.B.; Armaiz-Pena, G.N.; Mangala, L.S.; Danes, C.G.; Lin, Y.G.; Merritt, W.M.; Thaker, P.H.; Kamat, A.A.; et al. Functional significance of VEGFR-2 on ovarian cancer cells. Int. J. Cancer 2009, 124, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhu, S.; Hong, C.; Cai, H. Angiogenesis inhibitors for patients with ovarian cancer: A meta-analysis of 12 randomized controlled trials. Curr. Med. Res. Opin. 2016, 32, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Kotowicz, B.; Fuksiewicz, M.; Sobiczewski, P.; Spiewankiewicz, B.; Jonska-Gmyrek, J.; Skrzypczak, M.; Kowalska, M. Clinical value of human epididymis protein 4 and the risk of ovarian malignancy algorithm in differentiating borderline pelvic tumors from epithelial ovarian cancer in early stages. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 194, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Fotopoulou, C.; Sehouli, J.; Ewald-Riegler, N.; de Gregorio, N.; Reuss, A.; Richter, R.; Mahner, S.; Kommoss, F.; Schmalfeldt, B.; Fehm, T.; et al. The Value of Serum CA125 in the Diagnosis of Borderline Tumors of the Ovary. Int. J. Gynecol. Cancer 2015, 25, 1248–1252. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, K.; Shinozaki, H.; Takada, A. A retrospective study of 1069 epithelial borderline malignancies of the ovary treated in Japan. In Proceedings of the Annual Meeting of the American Society of Clinical Oncology, Los Angeles, CA, USA, 16–19 May 1998; p. 17:A1429.
- Darai, E.; Fauvet, R.; Uzan, C.; Gouy, S.; Duvillard, P.; Morice, P. Fertility and borderline ovarian tumor: A systematic review of conservative management, risk of recurrence and alternative options. Hum. Reprod. Update 2013, 19, 151–166. [Google Scholar] [CrossRef] [PubMed]
- Palermo, G.; Piraino, P.; Zucht, H.-D. Performance of PLS regression coefficients in selecting variables for each response of a multivariate PLS for omics-type data. Adv. Appl. Bioinform. Chem. 2009, 2, 57–70. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Angiogenesis Marker | Ovarian Cancer | Control Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Type I | Type II | Total | Non-Malignant Tumor | Healthy Subjects | Total | |||||||
| Average | SD | Average | SD | Average | SD | Average | SD | Average | SD | Average | SD | |
| sEGFR | 20,342.13 | 5845.31 | 20,295.90 | 8421.43 | 20,309.43 | 20,309.43 | 21,309.90 | 6318.37 | 22,883.43 | 9007.22 | 22,009.25 | 7633.25 |
| FGF-basic | 180.48 | 44.22 | 203.77 | 63.91 | 196.95 | 196.95 | 179.00 | 52.12 | 180.85 | 52.60 | 179.82 | 52.10 |
| Follistatin | 685.78 | 317.57 | 1042.48 | 844.22 | 938.08 | 938.08 | 547.91 | 232.49 | 629.53 | 322.66 | 584.19 | 277.84 |
| G-CSF | 92.53 | 26.26 | 109.25 | 49.04 | 104.36 | 104.36 | 88.79 | 23.68 | 87.51 | 25.59 | 88.22 | 24.44 |
| sHER2/neu | 3320.85 | 948.04 | 4091.06 | 2061.63 | 3865.63 | 3865.63 | 3563.75 | 1273.51 | 4428.57 | 2414.32 | 3948.11 | 1908.16 |
| HGF | 1440.99 | 779.83 | 1936.05 | 1028.92 | 1791.16 | 1791.16 | 1305.13 | 544.67 | 1444.71 | 711.23 | 1367.17 | 625.01 |
| sIL-6Rα | 15,154.04 | 4441.99 | 17,100.30 | 9621.15 | 16,530.66 | 16,530.66 | 14,733.51 | 5632.62 | 17,920.81 | 12,282.34 | 16,150.09 | 9289.22 |
| Leptin | 7928.88 | 7133.65 | 5892.49 | 6349.54 | 6488.51 | 6488.51 | 11,162.45 | 9759.36 | 12,370.69 | 14,333.84 | 11,699.44 | 11,963.72 |
| Osteopontin | 46,882.40 | 19,429.79 | 73,250.94 | 34,155.80 | 65,533.32 | 65,533.32 | 34816.71 | 15,300.22 | 38,185.47 | 20,838.74 | 36,313.94 | 17,962.64 |
| PDGF-AB/BB | 4396.93 | 2274.18 | 5397.20 | 2941.45 | 5104.44 | 5104.44 | 3653.87 | 1517.89 | 4007.50 | 2120.66 | 3811.04 | 1810.25 |
| PECAM-1 | 4411.84 | 996.33 | 4748.20 | 1674.27 | 4649.75 | 4649.75 | 4461.57 | 1524.40 | 4981.73 | 2088.27 | 4692.75 | 1806.74 |
| Prolactin | 11,688.28 | 9112.09 | 8920.90 | 5128.69 | 9730.87 | 9730.87 | 13,006.48 | 14,247.64 | 8799.15 | 6513.54 | 11,136.55 | 11,618.07 |
| SCF | 183.67 | 56.25 | 201.16 | 84.71 | 196.04 | 196.04 | 191.02 | 64.48 | 208.57 | 108.36 | 198.82 | 86.76 |
| sTIE-2 | 7697.06 | 2707.86 | 8890.87 | 4578.14 | 8541.46 | 8541.46 | 7824.73 | 2841.97 | 7886.31 | 3240.18 | 7852.10 | 3011.00 |
| sVEGFR-1 | 323.51 | 200.50 | 373.64 | 237.94 | 358.96 | 358.96 | 288.61 | 122.69 | 292.56 | 150.46 | 290.37 | 135.08 |
| sVEGFR-2 | 2906.88 | 1024.60 | 3347.97 | 1631.41 | 3218.87 | 3218.87 | 3128.36 | 1127.17 | 3520.94 | 1827.38 | 3302.84 | 1485.19 |
| CA125 | 344.68 | 536.27 | 1053.88 | 1312.09 | 853.85 | 1184.66 | 44.75 | 82.41 | - | - | - | - |
| HE4 | 258.78 | 399.07 | 760.70 | 942.74 | 619.14 | 851.91 | 50.22 | 13.88 | - | - | - | - |
| Angiogenesis Marker | OC vs. Control Group | Type I OC vs. Healthy Controls | Type II OC vs. Healthy Controls | OC vs. Benign Ovarian Tumours | ||||
|---|---|---|---|---|---|---|---|---|
| p-Value | AUC | p-Value | AUC | p-Value | AUC | p-Value | AUC | |
| FGF-basic | 0.0288 | 0.617 | - | - | 0.035 | 0.642 | 0.026 | 0.636 |
| Follistatin | 0.002 | 0.668 | - | - | 0.013 | 0.675 | <0.001 | 0.713 |
| G-CSF | - | - | - | - | 0.048 | 0.643 | - | - |
| sHER2/neu | - | - | 0.035 | 0.704 | - | - | - | - |
| HGF | 0.02 | 0.619 | - | - | 0.036 | 0.645 | 0.020 | 0.643 |
| Leptin | 0.001 | 0.669 | - | - | 0.005 | 0.696 | <0.001 | 0.715 |
| Osteopontin | <0.001 | 0.791 | - | - | <0.001 | 0.82 | <0.001 | 0.825 |
| PDGF-AB/BB | 0.008 | 0.636 | - | - | 0.019 | 0.645 | 0.001 | 0.652 |
| CA125 | - | - | - | - | - | - | <0.001 | 0.935 |
| HE4 | - | - | - | - | - | - | <0.001 | 0.946 |
| Marker | Full Name | Target Drugs | Citation |
|---|---|---|---|
| sEGFR | soluble epidermal growth factor receptor | Gefitinib; Erlotinib; Cetuximab | Murphy et al. [18]; Secord et al. [19] |
| sHER-2/neu | human epidermal growth factor receptor 2 erbB-2, ERBB2 | Trastuzumab (Herceptin) | Ray-Coquard et al. [20] |
| HGF | hepatocyte growth factor | Rilotumumab | Martin et al. [21] |
| FGF-basic | basic fibroblast growth factor | Nintedanib (VEGFR, PDGFR, FGFR inhibitor); Pazopanib (VEGFR, PDGFR, FGFR inhibitor); Lucitanib (VEGFR 1–3 and FGFR 1–2 inhibitor) | Ivy et al. [22] |
| PDGF-AB/BB | platelet-derived growth factor—a dimeric glycoprotein composed of two A (-AA) or two B (-BB) chains or a combination of the two (-AB) | Cediranib (VEGFR 1–3, PDGFR inhibitor); Sorafenib (VEGFR, PDGFR inhibitor); Sunitinib (VEGFR, PDGFR, SCF inhibitor); Nintedanib (VEGFR, PDGFR, FGFR inhibitor); Pazopanib (VEGFR, PDGFR, FGFR inhibitor); Imatinib (PDGFRs and SCF inhibitor) | Ivy et al. [22]; Choi et al. [23] |
| sVEGFR-1 (sVEGFR1/sFLT1) | soluble vascular endothelial growth factor receptor 1 | Cediranib (VEGFR 1–3, PDGFR inhibitor); Sorafenib (VEGFR, PDGFR inhibitor); Sunitinib (VEGFR, PDGFR inhibitor); Nintedanib (VEGFR, PDGFR, FGFR inhibitor); Pazopanib (VEGFR, PDGFR, FGFR inhibitor); Lucitanib (VEGFR 1–3 and FGFR 1–2 inhibitor) | Ivy et al. [22] |
| sVEGFR-2 | soluble vascular endothelial growth factor receptor 2 | ||
| SCF | stem cell factor | Imatinib (PDGFRs and SCF inhibitor); Sunitinib (VEGFR, PDGFR, SCF inhibitor) | Choi et al. [23]; Yasuda et al. [24] |
| Patient Group | Number of Samples (%) | Median Age (Min–Max) | Median BMI (Min–Max) | % of Postmenopausal |
|---|---|---|---|---|
| OC | 38 (24.36) | 60 (32–78) | 25.12 (18.55–38.37) | 79 |
| Type I | 7 (4.49) | |||
| Type II | 31 (19.87) | |||
| Borderline | 6 (3.85) | 48 (37–52) | 27.26 (17.29–31.64) | 33 |
| Benign ovarian tumour | 62 (39.74) | 40.5 (17–72) | 24.31 (17.85–39.89) | 26 |
| Healty controls | 50 (32.05) | 56 (19–73) | 25.80 (18.96–40.06) | 60 |
| Histopathological Type | Number of Samples | Percentage (%) |
|---|---|---|
| Serous | 16 | 42.11 |
| Endometrioid | 4 | 10.53 |
| Mucinous | 1 | 2.63 |
| Clear cell | 3 | 7.89 |
| Undifferentiated | 10 | 26.32 |
| Non identified | 4 | 10.53 |
| FIGO stage at diagnosis | ||
| I | 10 | 26.32 |
| II | 2 | 5.26 |
| III | 25 | 65.79 |
| IV | 1 | 2.63 |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horala, A.; Swiatly, A.; Matysiak, J.; Banach, P.; Nowak-Markwitz, E.; Kokot, Z.J. Diagnostic Value of Serum Angiogenesis Markers in Ovarian Cancer Using Multiplex Immunoassay. Int. J. Mol. Sci. 2017, 18, 123. https://doi.org/10.3390/ijms18010123
Horala A, Swiatly A, Matysiak J, Banach P, Nowak-Markwitz E, Kokot ZJ. Diagnostic Value of Serum Angiogenesis Markers in Ovarian Cancer Using Multiplex Immunoassay. International Journal of Molecular Sciences. 2017; 18(1):123. https://doi.org/10.3390/ijms18010123
Chicago/Turabian StyleHorala, Agnieszka, Agata Swiatly, Jan Matysiak, Paulina Banach, Ewa Nowak-Markwitz, and Zenon J. Kokot. 2017. "Diagnostic Value of Serum Angiogenesis Markers in Ovarian Cancer Using Multiplex Immunoassay" International Journal of Molecular Sciences 18, no. 1: 123. https://doi.org/10.3390/ijms18010123