
Detection of Circulating Tumor Cells Using Negative Enrichment Immunofluorescence and an In Situ Hybridization System in Pancreatic Cancer

Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Stability Test of Electronic Microscope
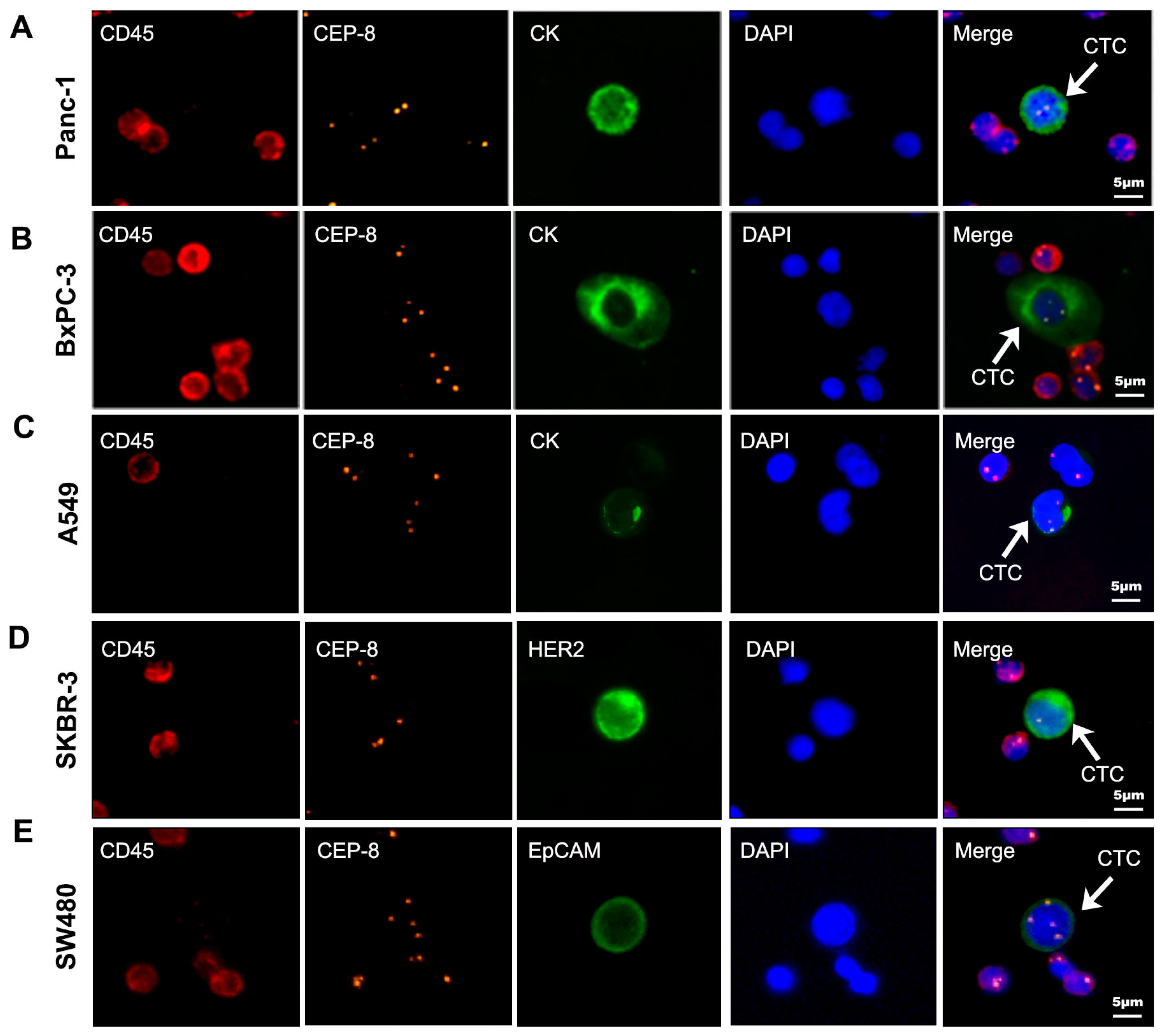
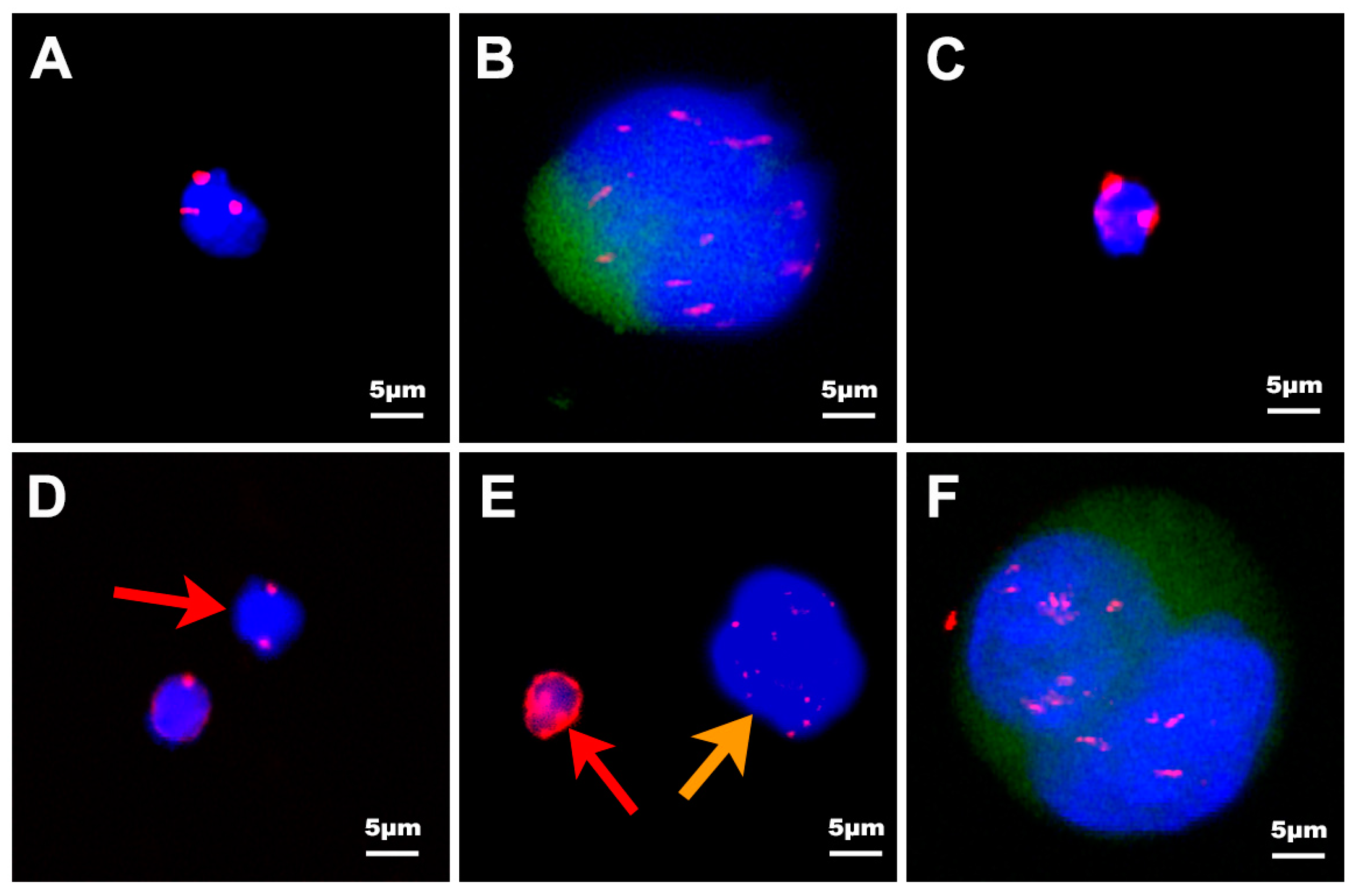
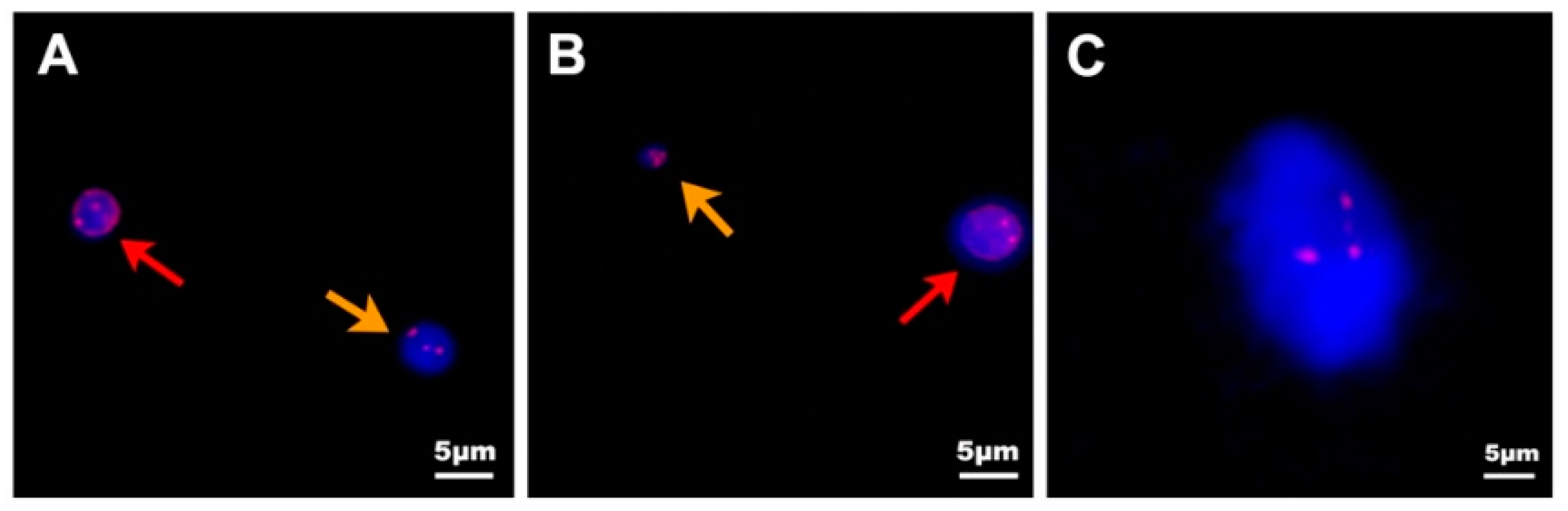
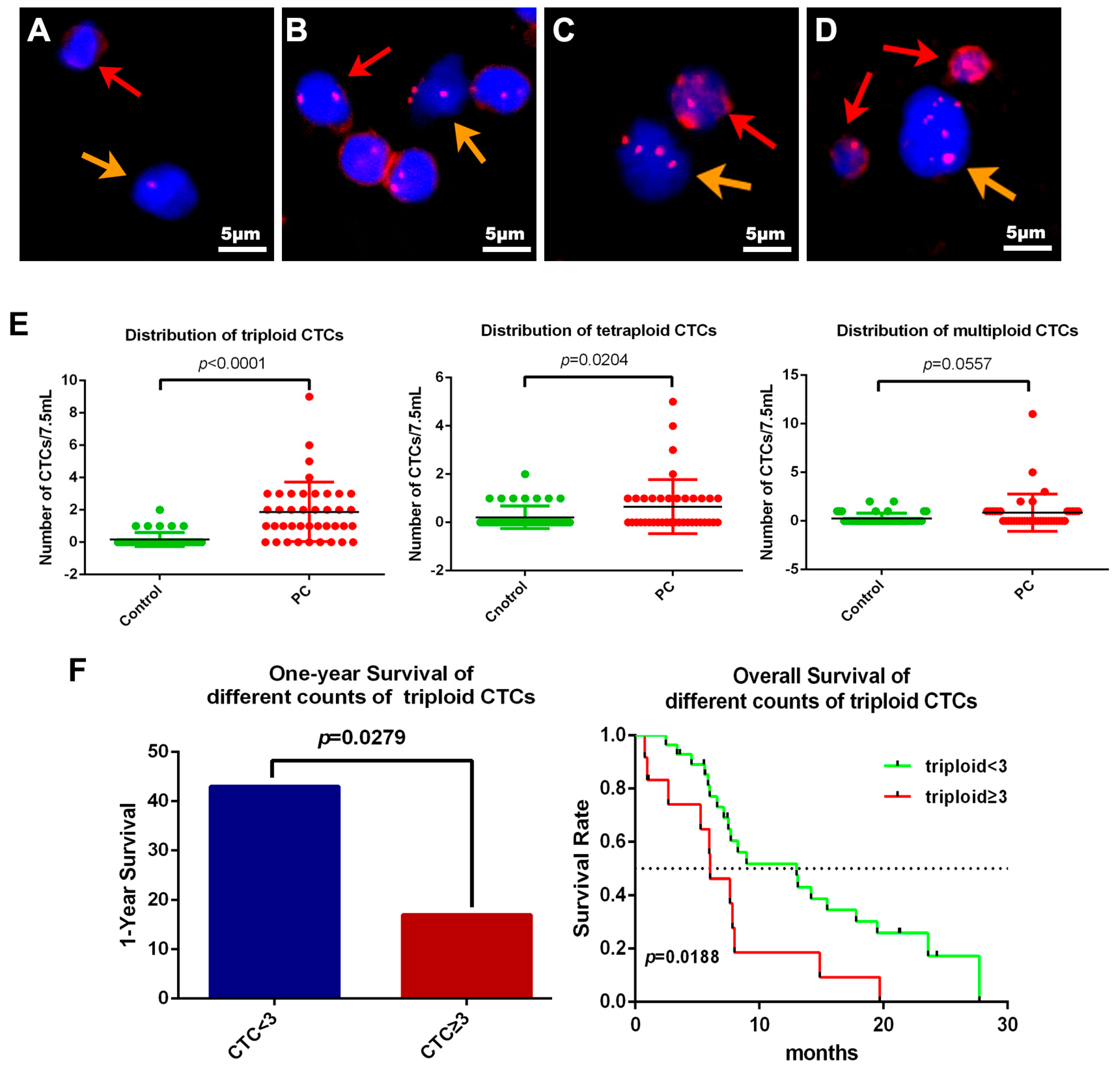
2.3. Definition of Circulating Tumor Cells (CTC) by Negative Enrichment Immunofluorescence and an In Situ Hybridization (NE-iFISH) System
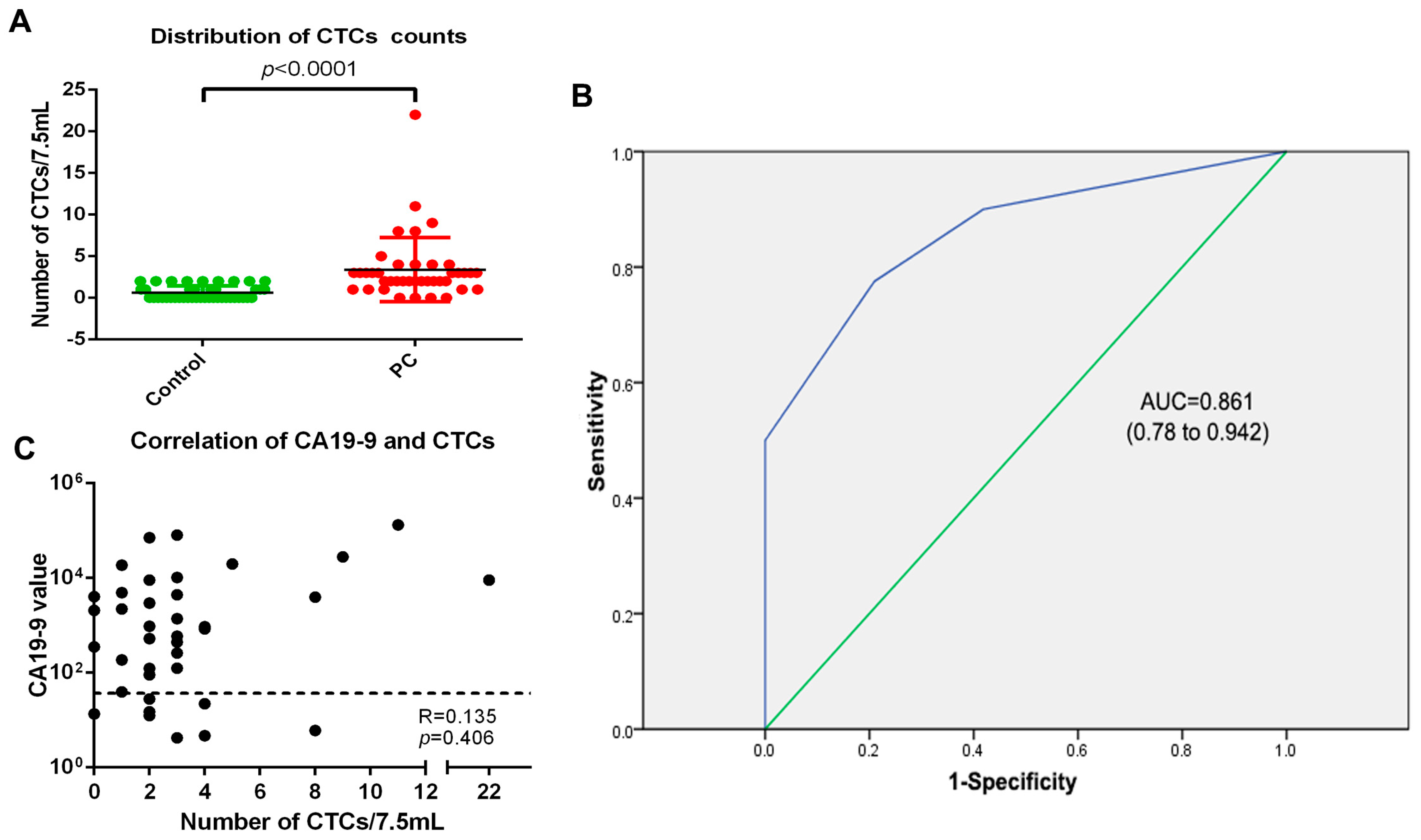
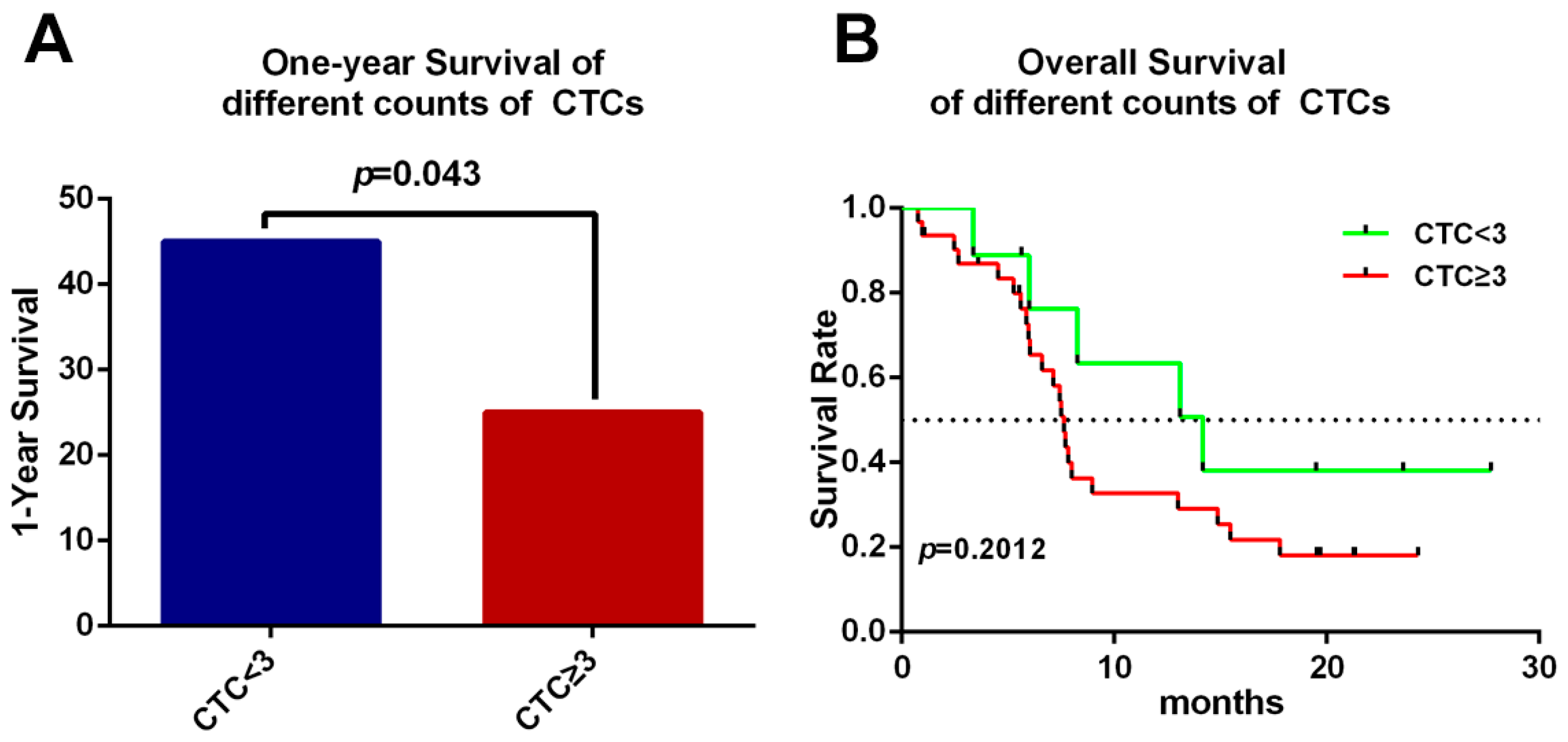
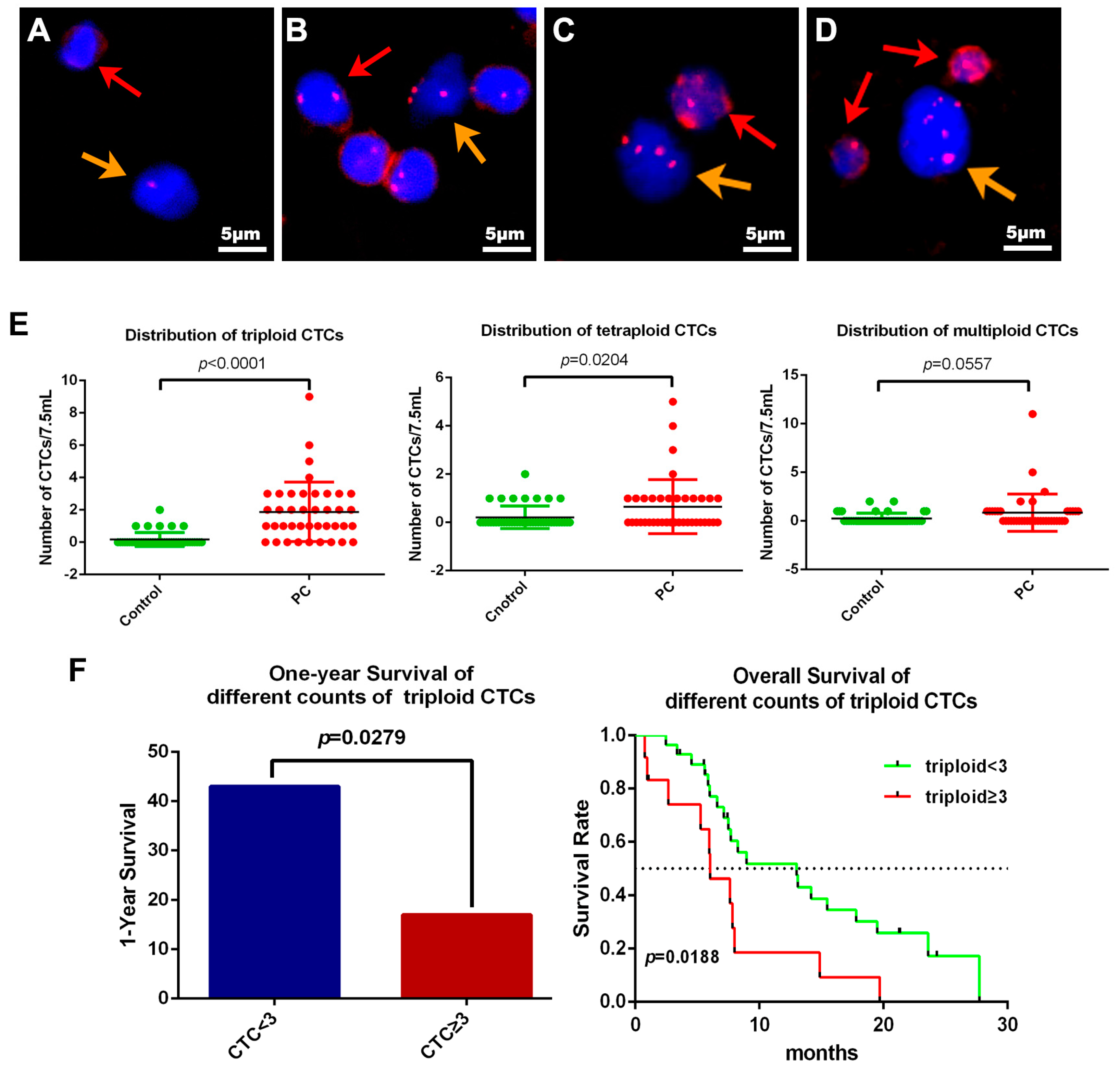
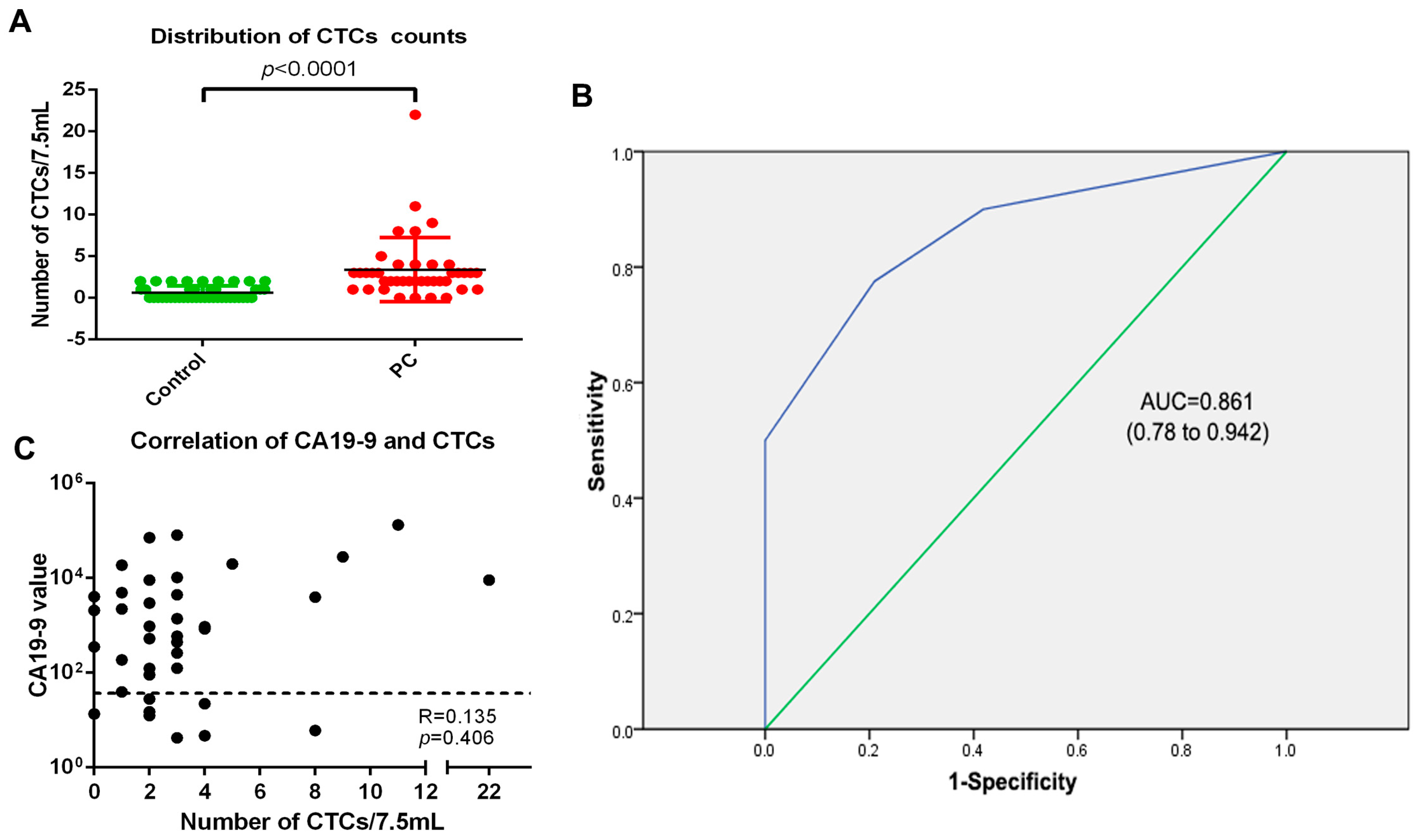
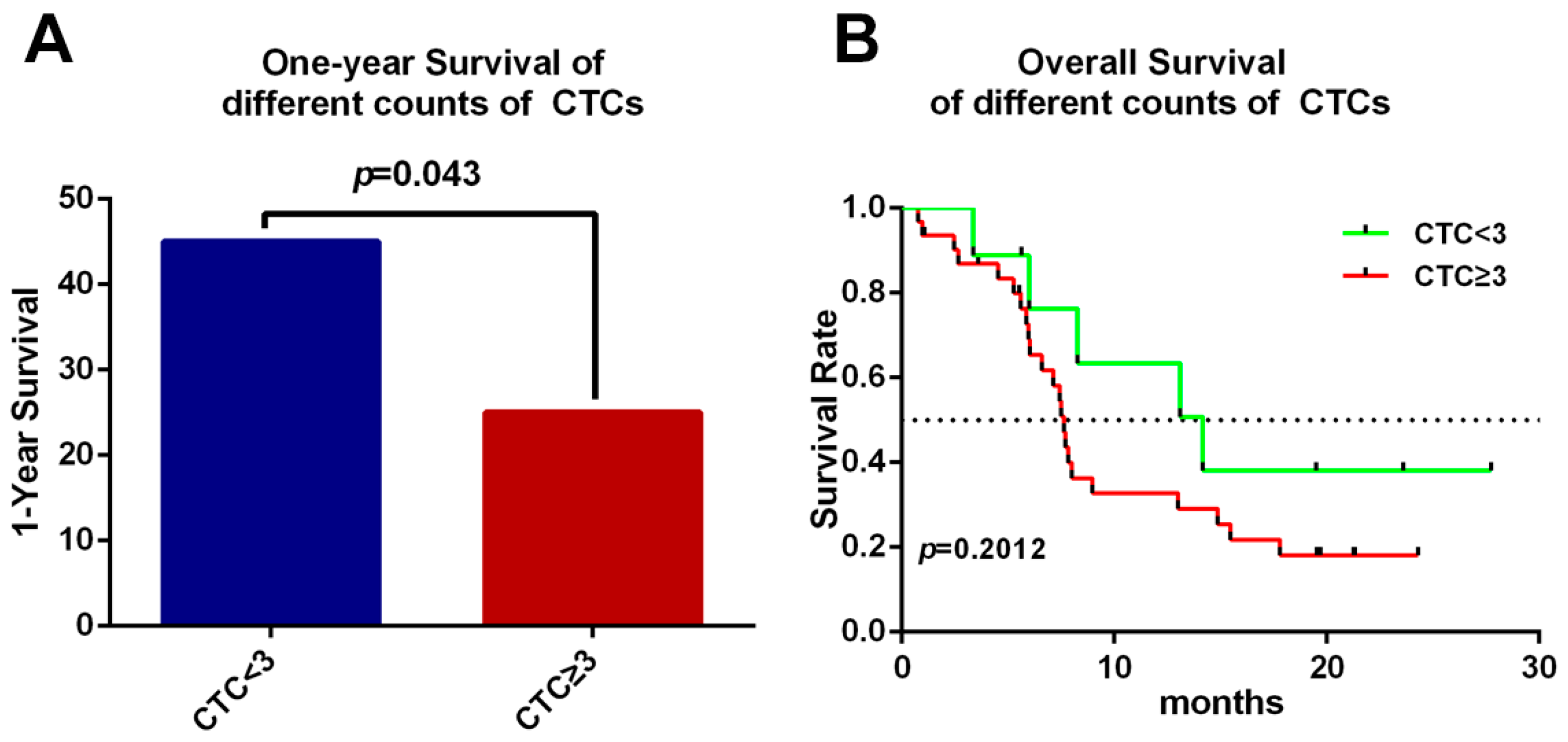
2.4. Clinical Significance of CTCs in PC
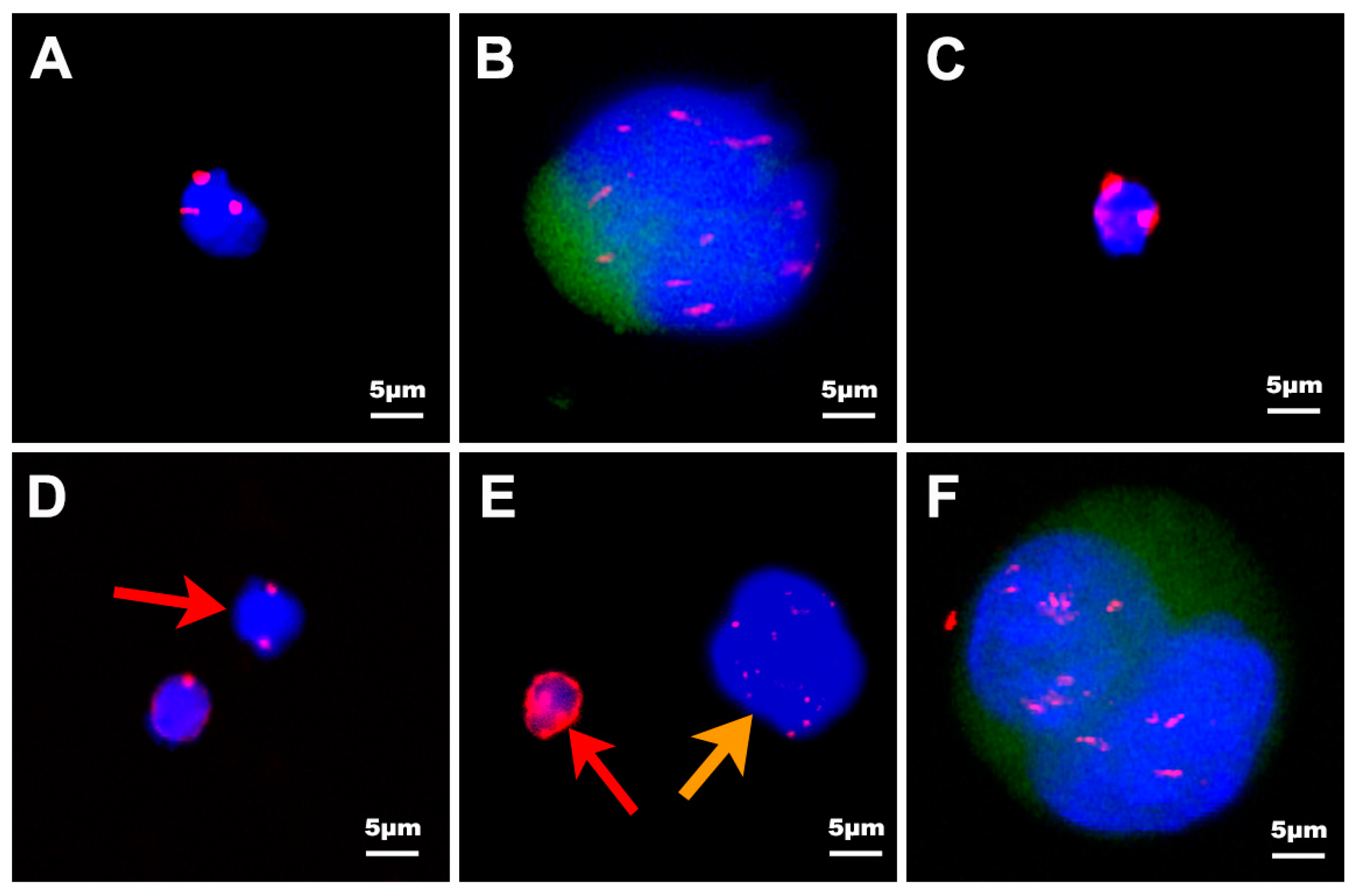
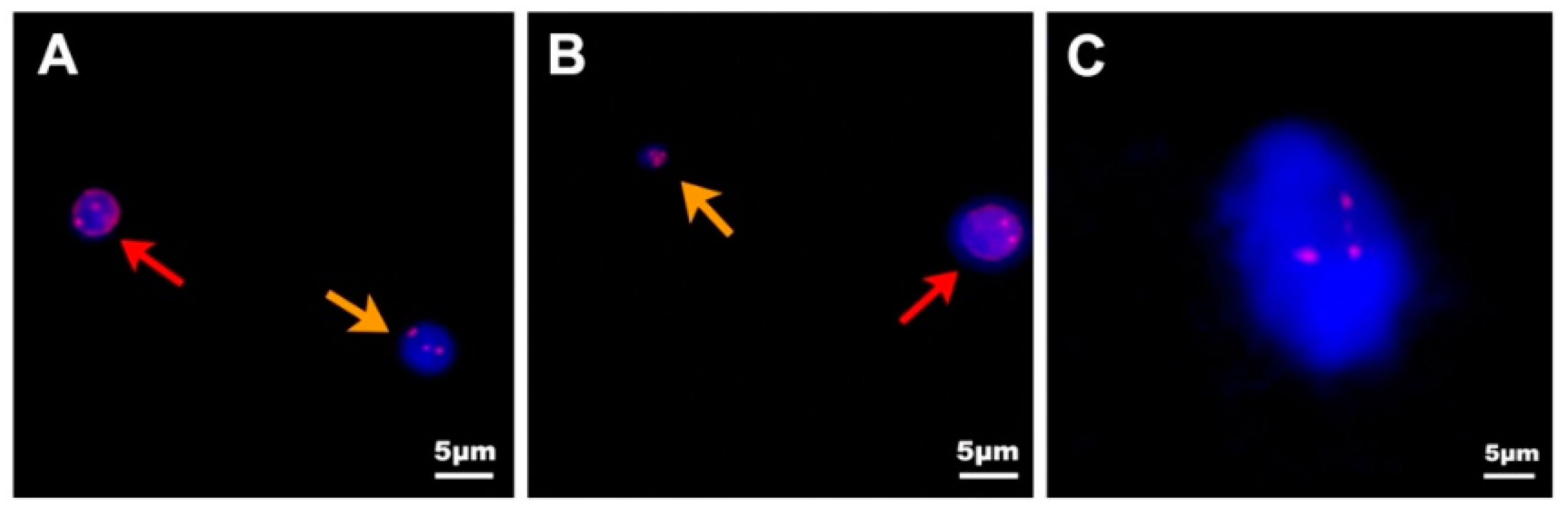
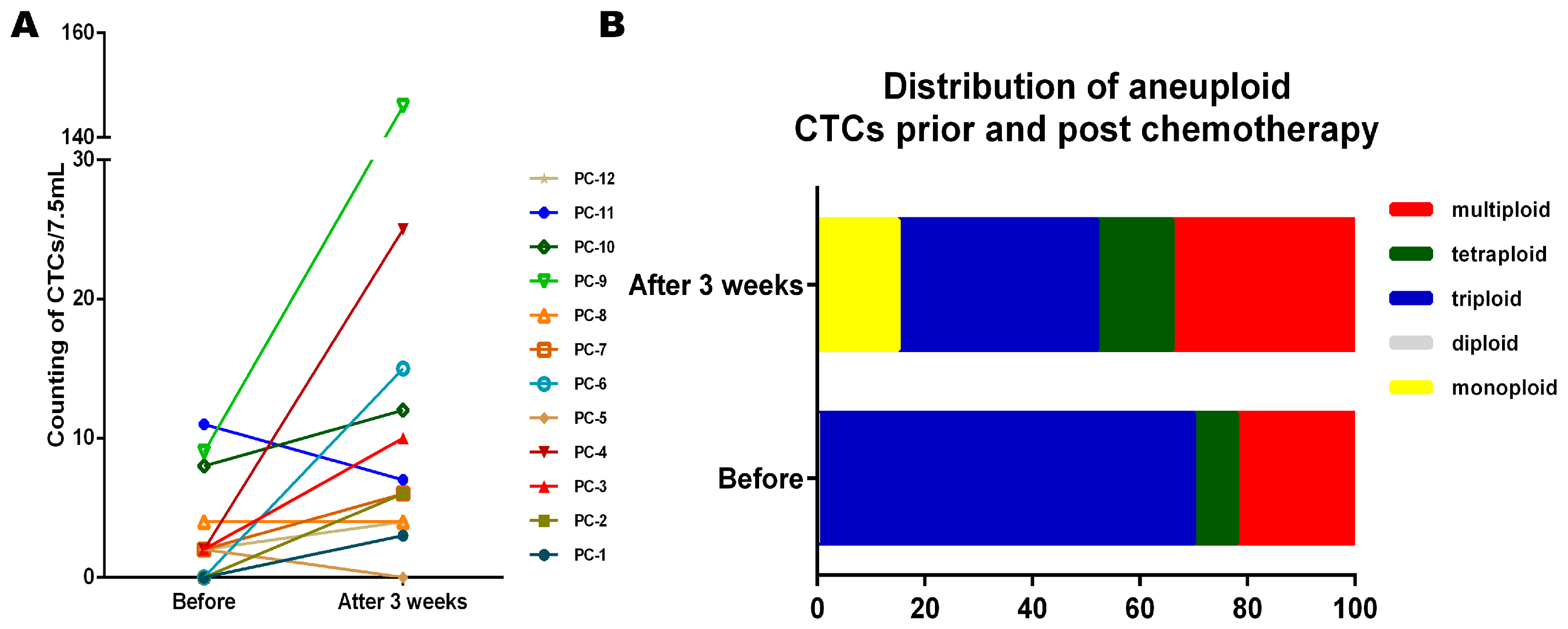
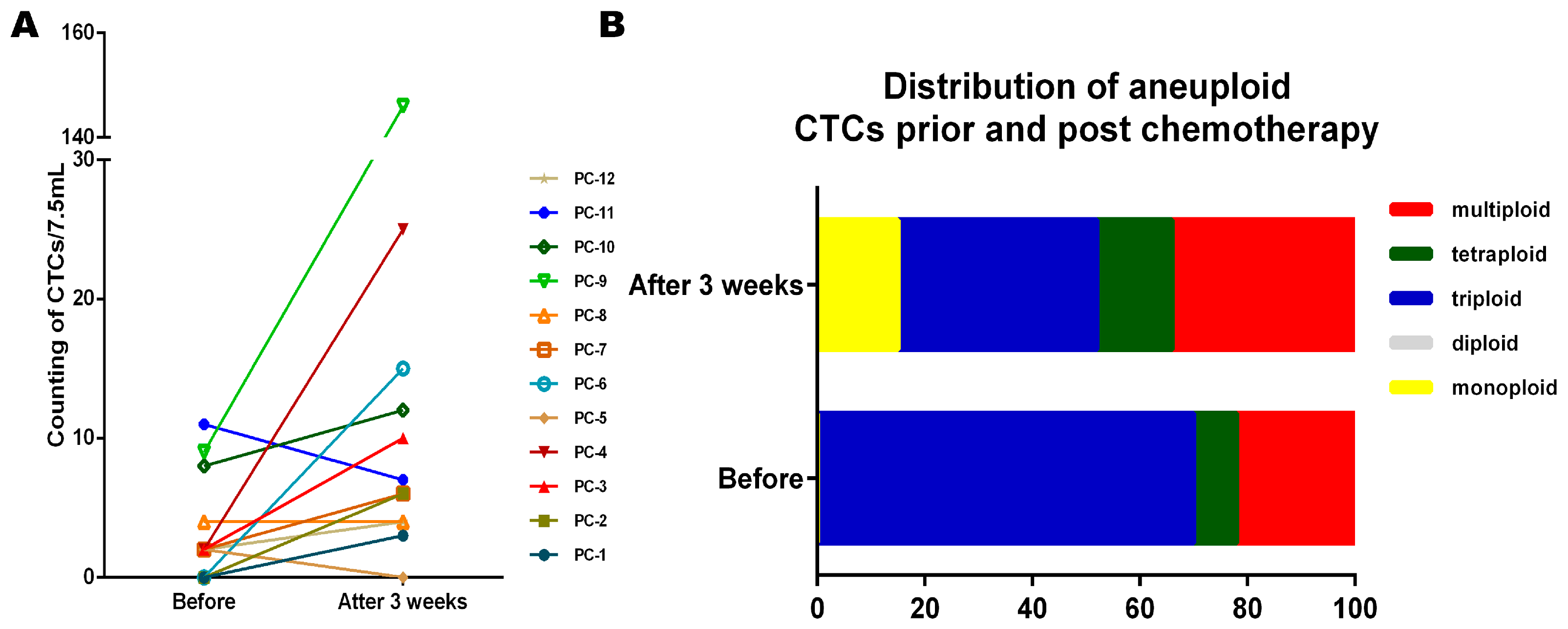
2.5. Dynamically Monitored CTC Counts and Aneuploidy in PC Patients
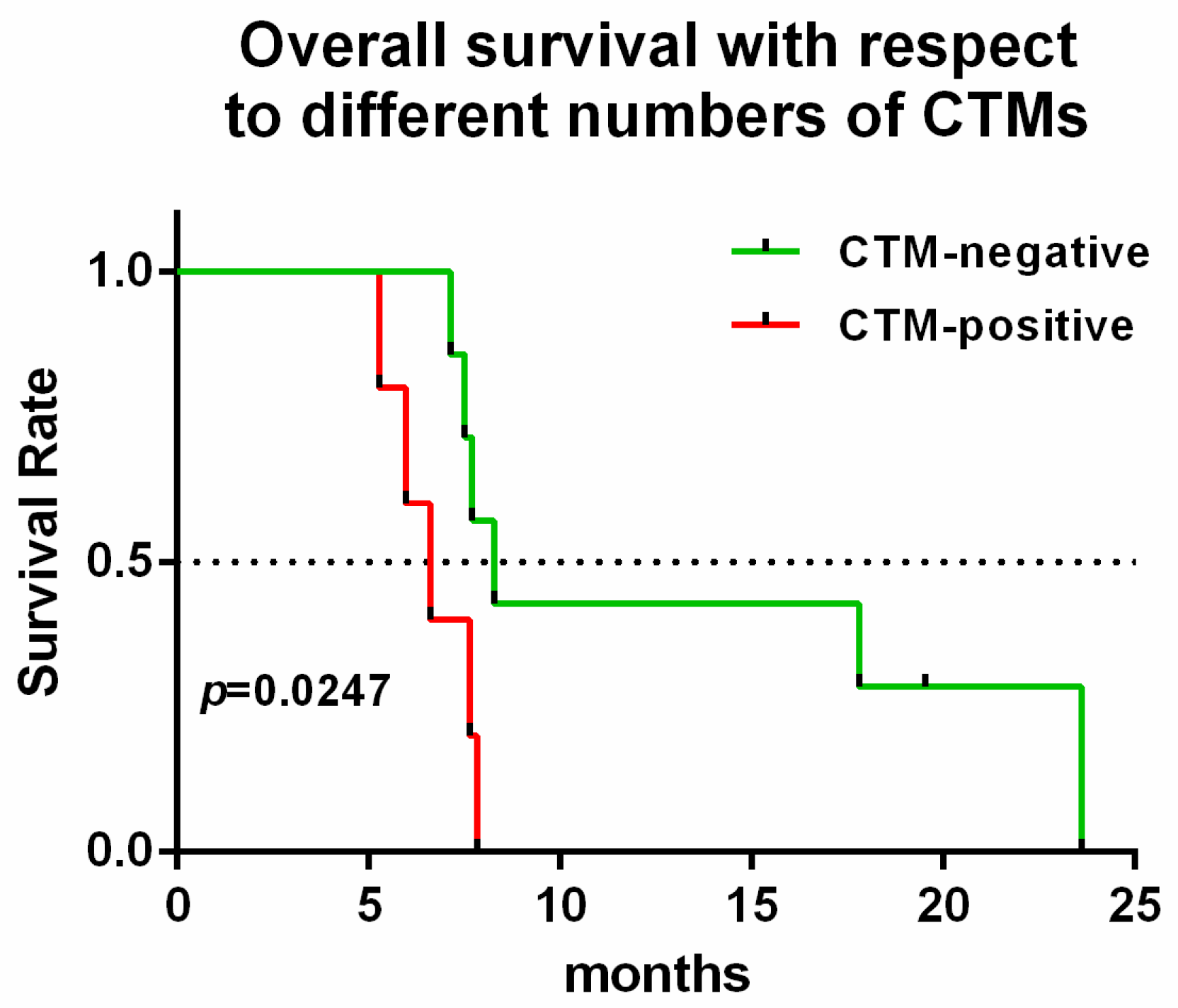
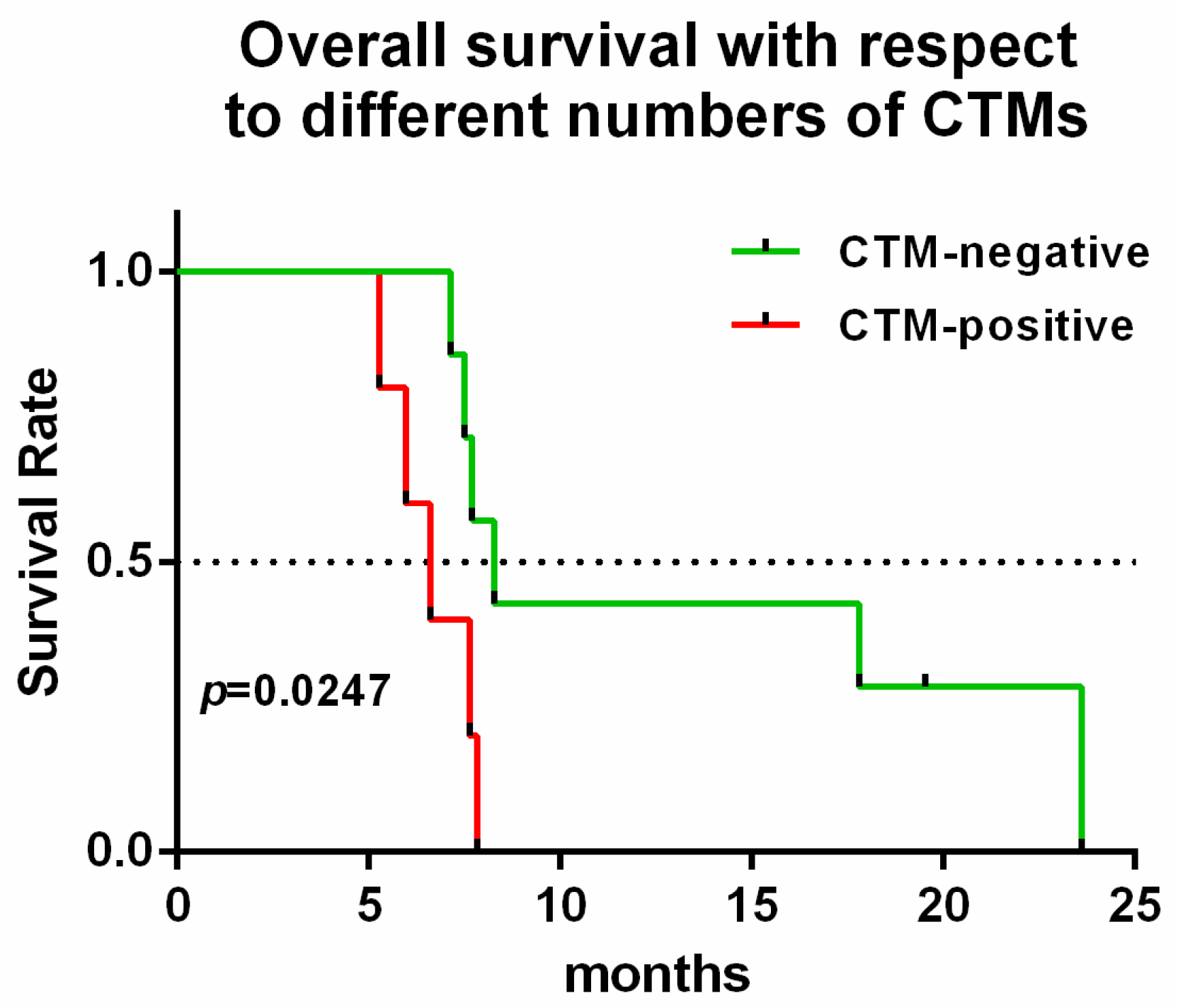
2.6. CTM Indicates Chemo-Resistance and a Poor Prognosis
3. Discussion
4. Materials and Methods
4.1. Cell Culture
4.2. Patients and Sample Collection
4.3. CTC Determination by NE-iFISH System
4.4. Detection of Carbohydrate Antigen 19-9
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CTCs | Circulating tumor cells |
| CTMs | Circulating tumor microembolus |
| PC | Pancreatic cancer |
| BTP | Benign tumors of the pancreas |
| HC | Healthy control |
| PDAC | Pancreatic ductal adenocarcinoma |
| PNET | Pancreatic neuroendocrine tumors |
| PCN | Pancreatic cystic neoplasms |
| AIP | Autoimmune pancreatitis |
| IPMN | Pancreatic intraductal papillary mucinous neoplasms |
| AC | Acute pancreatitis |
| CA19-9 | Carbohydrate antigen 19-9 |
| ASCO | American Society of Clinical Oncology |
References
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Shirai, Y.; Nakamura, N.; Sudo, K.; Nakamura, K.; Hironaka, S.; Hara, T.; Denda, T. Usefulness of brush cytology combined with pancreatic juice cytology in the diagnosis of pancreatic cancer: Significance of pancreatic juice cytology after brushing. Pancreas 2012, 41, 1225–1229. [Google Scholar] [CrossRef] [PubMed]
- Mollberg, N.; Rahbari, N.N.; Koch, M.; Hartwig, W.; Hoeger, Y.; Buchler, M.W.; Weitz, J. Arterial resection during pancreatectomy for pancreatic cancer: A systematic review and meta-analysis. Ann. Surg. 2011, 254, 882–893. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.G.; Bois, J.P.; Sarr, M.G.; Wood, C.M.; Qin, R.; Thomsen, K.M.; Kendrick, M.L.; Farnell, M.B. Predictive and prognostic value of CA 19-9 in resected pancreatic adenocarcinoma. J. Gastrointest. Surg. 2009, 13, 2050–2058. [Google Scholar] [CrossRef] [PubMed]
- Hata, S.; Sakamoto, Y.; Yamamoto, Y.; Nara, S.; Esaki, M.; Shimada, K.; Kosuge, T. Prognostic impact of postoperative serum CA 19-9 levels in patients with resectable pancreatic cancer. Ann. Surg. Oncol. 2012, 19, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Tang, S.J.; Sreenarasimhaiah, J.; Lara, L.F.; Siddiqui, A. The clinical utility and limitations of serum carbohydrate antigen (CA19-9) as a diagnostic tool for pancreatic cancer and cholangiocarcinoma. Dig. Dis. Sci. 2011, 56, 2491–2496. [Google Scholar] [CrossRef] [PubMed]
- Hayes, D.F.; Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Miller, M.C.; Matera, J.; Allard, W.J.; Doyle, G.V.; Terstappen, L.W. Circulating tumor cells at each follow-up time point during therapy of metastatic breast cancer patients predict progression-free and overall survival. Clin. Cancer Res. 2006, 12, 4218–4224. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.J.; Punt, C.J.; Iannotti, N.; Saidman, B.H.; Sabbath, K.D.; Gabrail, N.Y.; Picus, J.; Morse, M.; Mitchell, E.; Miller, M.C.; et al. Relationship of circulating tumor cells to tumor response, progression-free survival, and overall survival in patients with metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 3213–3221. [Google Scholar] [CrossRef] [PubMed]
- De Bono, J.S.; Scher, H.I.; Montgomery, R.B.; Parker, C.; Miller, M.C.; Tissing, H.; Doyle, G.V.; Terstappen, L.W.; Pienta, K.J.; Raghavan, D. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin. Cancer Res. 2008, 14, 6302–6309. [Google Scholar] [CrossRef] [PubMed]
- Grover, P.K.; Cummins, A.G.; Price, T.J.; Roberts-Thomson, I.C.; Hardingham, J.E. Circulating tumour cells: The evolving concept and the inadequacy of their enrichment by EpCAM-based methodology for basic and clinical cancer research. ESMO 2014, 25, 1506–1516. [Google Scholar] [CrossRef] [PubMed]
- Pecot, C.V.; Bischoff, F.Z.; Mayer, J.A.; Wong, K.L.; Pham, T.; Bottsford-Miller, J.; Stone, R.L.; Lin, Y.G.; Jaladurgam, P.; Roh, J.W.; et al. A novel platform for detection of CK+ and CK-CTCs. Cancer Discov. 2011, 1, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Thiery, J.P.; Acloque, H.; Huang, R.Y.; Nieto, M.A. Epithelial-mesenchymal transitions in development and disease. Cell 2009, 139, 871–890. [Google Scholar] [CrossRef] [PubMed]
- Satelli, A.; Mitra, A.; Brownlee, Z.; Xia, X.; Bellister, S.; Overman, M.J.; Kopetz, S.; Ellis, L.M.; Meng, Q.H.; Li, S. Epithelial-mesenchymal transitioned circulating tumor cells capture for detecting tumor progression. Clin. Cancer Res. 2015, 21, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Wang, D.D.; Yang, M.; Chen, D.; Pang, L.; Guo, S.; Cai, J.; Wery, J.P.; Li, L.; Li, H.Q.; et al. Comprehensive characterization of chemotherapeutic efficacy on metastases in the established gastric neuroendocrine cancer patient derived xenograft model. Oncotarget 2015, 6, 15639–15651. [Google Scholar] [CrossRef] [PubMed]
- Kops, G.J.; Weaver, B.A.; Cleveland, D.W. On the road to cancer: Aneuploidy and the mitotic checkpoint. Nat. Rev. Cancer 2005, 5, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Passerini, V.; Ozeri-Galai, E.; de Pagter, M.S.; Donnelly, N.; Schmalbrock, S.; Kloosterman, W.P.; Kerem, B.; Storchova, Z. The presence of extra chromosomes leads to genomic instability. Nat. Commun. 2016, 7, 10754. [Google Scholar] [CrossRef] [PubMed]
- Habermann, J.K.; Doering, J.; Hautaniemi, S.; Roblick, U.J.; Bundgen, N.K.; Nicorici, D.; Kronenwett, U.; Rathnagiriswaran, S.; Mettu, R.K.; Ma, Y.; et al. The gene expression signature of genomic instability in breast cancer is an independent predictor of clinical outcome. Int. J. Cancer 2009, 124, 1552–1564. [Google Scholar] [CrossRef] [PubMed]
- Smid, M.; Hoes, M.; Sieuwerts, A.M.; Sleijfer, S.; Zhang, Y.; Wang, Y.; Foekens, J.A.; Martens, J.W. Patterns and incidence of chromosomal instability and their prognostic relevance in breast cancer subtypes. Breast Cancer Res. Treat. 2011, 128, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; Endesfelder, D.; Rowan, A.J.; Walther, A.; Birkbak, N.J.; Futreal, P.A.; Downward, J.; Szallasi, Z.; Tomlinson, I.P.; Howell, M.; et al. Chromosomal instability confers intrinsic multidrug resistance. Cancer Res. 2011, 71, 1858–1870. [Google Scholar] [CrossRef] [PubMed]
- McGranahan, N.; Burrell, R.A.; Endesfelder, D.; Novelli, M.R.; Swanton, C. Cancer chromosomal instability: Therapeutic and diagnostic challenges. EMBO Rep. 2012, 13, 528–538. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.W.; Seo, K.W.; Jang, S.J.; Oh, Y.M.; Shim, T.S.; Kim, W.S.; Lee, D.S.; Lee, S.D.; Choi, C.M. The relationship between the presence of chromosomal instability and prognosis of squamous cell carcinoma of the lung: Fluorescence in situ hybridization analysis of paraffin-embedded tissue from 47 Korean patients. J. Korean Med. Sci. 2010, 25, 863–867. [Google Scholar] [CrossRef] [PubMed]
- Mettu, R.K.; Wan, Y.W.; Habermann, J.K.; Ried, T.; Guo, N.L. A 12-gene genomic instability signature predicts clinical outcomes in multiple cancer types. Int. J. Biol. Markers 2010, 25, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Kronenwett, U.; Huwendiek, S.; Ostring, C.; Portwood, N.; Roblick, U.J.; Pawitan, Y.; Alaiya, A.; Sennerstam, R.; Zetterberg, A.; Auer, G. Improved grading of breast adenocarcinomas based on genomic instability. Cancer Res. 2004, 64, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Uzawa, N.; Takahashi, K.; Myo, K.; Ohyama, Y.; Amagasa, T. Prognostic utility of chromosomal instability detected by fluorescence in situ hybridization in fine-needle aspirates from oral squamous cell carcinomas. BMC Cancer 2010, 10, 182. [Google Scholar] [CrossRef] [PubMed]
- Vona, G.; Sabile, A.; Louha, M.; Sitruk, V.; Romana, S.; Schutze, K.; Capron, F.; Franco, D.; Pazzagli, M.; Vekemans, M.; et al. Isolation by size of epithelial tumor cells: A new method for the immunomorphological and molecular characterization of circulatingtumor cells. Am. J. Pathol. 2000, 156, 57–63. [Google Scholar] [CrossRef]
- Amato, R.J.; Melnikova, V.; Zhang, Y.; Liu, W.; Saxena, S.; Shah, P.K.; Jensen, B.T.; Torres, K.E.; Davis, D.W. Epithelial cell adhesion molecule-positive circulating tumor cells as predictive biomarker in patients with prostate cancer. Urology 2013, 81, 1303–1307. [Google Scholar] [CrossRef] [PubMed]
- Mostert, B.; Sleijfer, S.; Foekens, J.A.; Gratama, J.W. Circulating tumor cells (CTCs): Detection methods and their clinical relevance in breast cancer. Cancer Treat. Rev. 2009, 35, 463–474. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, X.; Ge, S.; Gao, J.; Gong, J.; Lu, M.; Zhang, Q.; Cao, Y.; Wang, D.D.; Lin, P.P.; Shen, L. Clinical significance of phenotyping and karyotyping of circulating tumor cells in patients with advanced gastric cancer. Oncotarget 2014, 5, 6594–6602. [Google Scholar] [CrossRef] [PubMed]
- Hiltermann, T.J.N.; Pore, M.M.; van den Berg, A.; Timens, W.; Boezen, H.M.; Liesker, J.J.W.; Schouwink, J.H.; Wijnands, W.J.A.; Kerner, G.S.M.A.; Kruyt, F.A.E.; et al. Circulating tumor cells in small-cell lung cancer: A predictive and prognostic factor. Ann. Oncol. 2012, 23, 2937–2942. [Google Scholar] [CrossRef] [PubMed]
- Janni, W.J.; Rack, B.; Terstappen, L.W.; Pierga, J.Y.; Taran, F.A.; Fehm, T.; Hall, C.; de Groot, M.R.; Bidard, F.C.; Friedl, T.W.; et al. Pooled Analysis of the Prognostic Relevance of Circulating Tumor Cells in Primary Breast Cancer. Clin. Cancer Res. 2016, 22, 2583–2593. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.; Fritsche, H.; Mennel, R.; Norton, L.; Ravdin, P.; Taube, S.; Somerfield, M.R.; Hayes, D.F.; Bast, R.C., Jr. American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer. J. Clin. Oncol. 2007, 25, 5287–5312. [Google Scholar] [CrossRef] [PubMed]
- Tjensvoll, K.; Nordgard, O.; Smaaland, R. Circulating tumor cells in pancreatic cancer patients: Methods of detection and clinical implications. Int. J. Cancer 2014, 134, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Deneve, E.; Riethdorf, S.; Ramos, J.; Nocca, D.; Coffy, A.; Daures, J.P.; Maudelonde, T.; Fabre, J.M.; Pantel, K.; Alix-Panabieres, C. Capture of viable circulating tumor cells in the liver of colorectal cancer patients. Clin. Chem. 2013, 59, 1384–1392. [Google Scholar] [CrossRef] [PubMed]
- Went, P.T.; Lugli, A.; Meier, S.; Bundi, M.; Mirlacher, M.; Sauter, G.; Dirnhofer, S. Frequent EpCam protein expression in human carcinomas. Hum. Pathol. 2004, 35, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.C.; Huguet, F.; Louvet, C.; Mineur, L.; Bouche, O.; Chibaudel, B.; Artru, P.; Desseigne, F.; Bachet, J.B.; Mathiot, C.; et al. Circulating tumor cells in locally advanced pancreatic adenocarcinoma: The ancillary CirCe 07 study to the LAP 07 trial. ESMO 2013, 24, 2057–2061. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Inoue, H.; Kimura, S.; Ohmori, T.; Ishikawa, F.; Gohda, K.; Sato, J. Prognostic impact of the number of viable circulating cells with high telomerase activity in gastric cancer patients: A prospective study. Int. J. Oncol. 2014, 45, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Koopmann, J.; Rosenzweig, C.N.; Zhang, Z.; Canto, M.I.; Brown, D.A.; Hunter, M.; Yeo, C.; Chan, D.W.; Breit, S.N.; Goggins, M. Serum markers in patients with resectable pancreatic adenocarcinoma: Macrophage inhibitory cytokine 1 versus CA19-9. Clin. Cancer Res. 2006, 12, 442–446. [Google Scholar] [CrossRef] [PubMed]
- Ehmann, M.; Felix, K.; Hartmann, D.; Schnolzer, M.; Nees, M.; Vorderwulbecke, S.; Bogumil, R.; Buchler, M.W.; Friess, H. Identification of potential markers for the detection of pancreatic cancer through comparative serum protein expression profiling. Pancreas 2007, 34, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.T.; Tao, H.Q.; Zou, S.C. Detection of serum tumor markers in the diagnosis and treatment of patients with pancreatic cancer. Hepatobiliary Pancreat. Dis. Int. 2004, 3, 464–468. [Google Scholar] [PubMed]
- Safi, F.; Schlosser, W.; Falkenreck, S.; Beger, H.G. Prognostic value of CA 19-9 serum course in pancreatic cancer. Hepato Gastroenterol. 1998, 45, 253–259. [Google Scholar]
- Chang, M.C.; Chang, Y.T.; Su, T.C.; Yang, W.S.; Chen, C.L.; Tien, Y.W.; Liang, P.C.; Wei, S.C.; Wong, J.M. Adiponectin as a potential differential marker to distinguish pancreatic cancer and chronic pancreatitis. Pancreas 2007, 35, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Duraker, N.; Hot, S.; Polat, Y.; Hobek, A.; Gencler, N.; Urhan, N. CEA, CA 19-9, and CA 125 in the differential diagnosis of benign and malignant pancreatic diseases with or without jaundice. J. Surg. Oncol. 2007, 95, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Liao, Q.; Zhao, Y.P.; Yang, Y.C.; Li, L.J.; Long, X.; Han, S.M. Combined detection of serum tumor markers for differential diagnosis of solid lesions located at the pancreatic head. Hepatobiliary Pancreat. Dis. Int. 2007, 6, 641–645. [Google Scholar] [PubMed]
- Ni, X.G.; Bai, X.F.; Mao, Y.L.; Shao, Y.F.; Wu, J.X.; Shan, Y.; Wang, C.F.; Wang, J.; Tian, Y.T.; Liu, Q.; et al. The clinical value of serum CEA, CA19-9, and CA242 in the diagnosis and prognosis of pancreatic cancer. Eur. J. Surg. Oncol. Assoc. Surg. Oncol. 2005, 31, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Kuusela, P.; Haglund, C.; Roberts, P.J. Comparison of a new tumour marker CA 242 with CA 19-9, CA 50 and carcinoembryonic antigen (CEA) in digestive tract diseases. Br. J. Cancer 1991, 63, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Brand, R.E.; Nolen, B.M.; Zeh, H.J.; Allen, P.J.; Eloubeidi, M.A.; Goldberg, M.; Elton, E.; Arnoletti, J.P.; Christein, J.D.; Vickers, S.M.; et al. Serum biomarker panels for the detection of pancreatic cancer. Clin. Cancer Res. 2011, 17, 805–816. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, F.; Ning, N.; Chen, Q.; Yang, Z.; Guo, Y.; Xu, D.; Zhang, D.; Zhan, T.; Cui, W. Patterns of circulating tumor cells identified by CEP8, CK and CD45 in pancreatic cancer. Int. J. Cancer 2015, 136, 1228–1233. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Zhu, Y.; Zhang, Z.; Zhang, C.; Huang, X.; Yuan, Z. Clinical significance of pancreatic circulating tumor cells using combined negative enrichment and immunostaining-fluorescence in situ hybridization. J. Exp. Clin. Cancer Res. 2016, 35, 66. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.M.; Krebs, M.G.; Lancashire, L.; Sloane, R.; Backen, A.; Swain, R.K.; Priest, L.J.; Greystoke, A.; Zhou, C.; Morris, K.; et al. Clinical significance and molecular characteristics of circulating tumor cells and circulating tumor microemboli in patients with small-cell lung cancer. J. Clin. Oncol. 2012, 30, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.M.; Krebs, M.; Ward, T.; Sloane, R.; Priest, L.; Hughes, A.; Clack, G.; Ranson, M.; Blackhall, F.; Dive, C. Circulating tumor cells as a window on metastasis biology in lung cancer. Am. J. Pathol. 2011, 178, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Aceto, N.; Bardia, A.; Miyamoto, D.T.; Donaldson, M.C.; Wittner, B.S.; Spencer, J.A.; Yu, M.; Pely, A.; Engstrom, A.; Zhu, H.; et al. Circulating tumor cell clusters are oligoclonal precursors of breast cancer metastasis. Cell 2014, 158, 1110–1122. [Google Scholar] [CrossRef] [PubMed]
- Khoja, L.; Backen, A.; Sloane, R.; Menasce, L.; Ryder, D.; Krebs, M.; Board, R.; Clack, G.; Hughes, A.; Blackhall, F.; et al. A pilot study to explore circulating tumour cells in pancreatic cancer as a novel biomarker. Br. J. Cancer 2012, 106, 508–516. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Code | Gender | Age | Location | Histological Type | Stage | Before Treatment | Treatment after 3 Weeks | Outcome (Follow Up for 28 Months) | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CA19-9 (U/ML) | CK+, CD45−, DAPI+ | CK−, CD45−, DAPI+ | CTM | CA19-9 (U/ML) | CK+, CD45−, DAPI+ | CK−, CD45−, DAPI+ | CTM | |||||||||||||||||||||||||||
| Monoploid | Diploid | Triploid | Tetraploid | Multiploid | Sum | Monoploid | Diploid | Triploid | Tetraploid | Multiploid | Sum | Monoploid | Diploid | Triploid | Tetraploid | Multiploid | Sum | Monoploid | Diploid | Triploid | Tetraploid | Multiploid | Sum | |||||||||||
| PC-1 | M | 65 | H | PDAC | IV | 4050 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | 934.8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 2 | 0 | 1 | 3 | 0 | Died |
| PC-2 | M | 51 | BT | PDAC | IV | 13.59 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | 13.59 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | / | 3 | 1 | 0 | 6 | 0 | Died |
| PC-3 | F | 55 | BT | PDAC | IV | 9080 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 0 | 1 | 2 | 0 | 10361 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 5 | 5 | 10 | 0 | Died |
| PC-4 | M | 54 | BT | PDAC | IV | 28.12 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 2 | 0 | 0 | 2 | 0 | 727.9 | 0 | 0 | 0 | 0 | 0 | 0 | 13 | / | 10 | 1 | 1 | 25 | 0 | Died |
| PC-5 | M | 39 | H | PDAC | IV | 527.7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 0 | 1 | 2 | 0 | 423.2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 2 | 0 | 0 | 2 | 0 | Died |
| PC-6 | M | 36 | BT | PDAC | IV | 591.4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 2 | 1 | 0 | 3 | 0 | 1700 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 0 | 14 | 15 | 0 | Died |
| PC-7 | M | 62 | H | PDAC | IV | 964.4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 2 | 0 | 0 | 2 | 0 | 155 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 5 | 0 | 1 | 6 | 0 | Alive |
| PC-8 | M | 59 | H | PDAC | IV | 22.18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 3 | 1 | 0 | 4 | 0 | 6.9 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 3 | 1 | 0 | 4 | 1 | Died |
| PC-9 | M | 50 | BT | PDAC | IV | 28068 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 3 | 1 | 5 | 9 | 0 | 78,182 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 146 | 146 | 5 | Died |
| PC-10 | F | 70 | BT | PDAC | IV | 3954 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 5 | 0 | 3 | 8 | 2 | 11,356 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 5 | 0 | 7 | 12 | 1 | Died |
| PC-11 | F | 51 | H | PDAC | IV | 132,070 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 9 | 0 | 2 | 11 | 1 | 173,664 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 4 | 0 | 4 | 8 | 1 | Died |
| PC-12 | M | 64 | H | PDAC | IV | 71,019 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 1 | 1 | 2 | 0 | 73,780 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 3 | 1 | 0 | 4 | 1 | Died |
| PC-13 | M | 59 | H | PDAC | IV | 4925 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 0 | 0 | 1 | 0 | Died | ||||||||||||||
| PC-14 | M | 65 | H | PDAC | IV | 2222 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 1 | 0 | 1 | 0 | Died | ||||||||||||||
| PC-15 | M | 74 | BT | PDAC | IV | 28.33 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 1 | 0 | 2 | 0 | Lost | ||||||||||||||
| PC-16 | M | 76 | BT | PDAC | IV | 15.13 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 2 | 0 | 0 | 2 | 0 | Died | ||||||||||||||
| PC-17 | M | 50 | H | PDAC | IV | 4423 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 2 | 1 | 3 | 0 | Died | ||||||||||||||
| PC-18 | M | 75 | H | PDAC | IV | 4.25 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 3 | 0 | 0 | 3 | 0 | Died | ||||||||||||||
| PC-19 | F | 48 | H | PDAC | IV | 10,313 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 3 | 0 | 0 | 3 | 0 | Died | ||||||||||||||
| PC-20 | F | 48 | H | PDAC | IV | 442 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 1 | 1 | 3 | 0 | Died | ||||||||||||||
| PC-21 | M | 39 | BT | PDAC | IV | 80,749 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 3 | 0 | 0 | 3 | 0 | Died | ||||||||||||||
| PC-22 | M | 76 | BT | PDAC | IV | 19,764 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 4 | 0 | 1 | 5 | 0 | Died | ||||||||||||||
| PC-23 | M | 36 | H | PDAC | IV | 6.09 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 2 | 4 | 2 | 8 | 0 | Died | ||||||||||||||
| PC-24 | F | 73 | H | PDAC | IV | 9038 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 6 | 5 | 11 | 22 | 4 | Alive | ||||||||||||||
| PC-25 | F | 64 | H | PDAC | III | 187.9 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 1 | 0 | 1 | 0 | Died | ||||||||||||||
| PC-26 | M | 70 | BT | PDAC | III | 39.40 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 0 | 0 | 1 | 0 | Alive | ||||||||||||||
| PC-27 | M | 50 | H | PDAC | III | 12.50 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 0 | 1 | 2 | 0 | Alive | ||||||||||||||
| PC-28 | F | 21 | H | PDAC | III | 4.68 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | / | 1 | 1 | 1 | 4 | 0 | Died | ||||||||||||||
| PC-29 | M | 72 | BT | PDAC | III | 848.4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 3 | 1 | 0 | 4 | 0 | Died | ||||||||||||||
| PC-30 | F | 58 | H | PDAC | II | 2956 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 2 | 0 | 0 | 2 | 0 | Died | ||||||||||||||
| PC-31 | F | 71 | H | PDAC | II | 18,834 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 1 | 1 | 0 | Died | ||||||||||||||
| PC-32 | M | 56 | BT | PDAC | II | 124.5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 3 | 0 | 0 | 3 | 0 | Died | ||||||||||||||
| PC-33 | F | 68 | BT | PDAC | II | 124.20 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 0 | 1 | 2 | 0 | Alive | ||||||||||||||
| PC-34 | F | 58 | H | PDAC | II | 1393 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 2 | 1 | 0 | 3 | 0 | Lost | ||||||||||||||
| PC-35 | M | 62 | H | PDAC | II | 942.7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 3 | 0 | 4 | 0 | Alive | ||||||||||||||
| PC-36 | M | 71 | H | PDAC | II | 354.1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | Died | ||||||||||||||
| PC-37 | M | 65 | BT | PDAC | I | 262.1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 3 | 0 | 0 | 3 | 0 | Died | ||||||||||||||
| PC-38 | F | 59 | BT | PDAC | I | 124.5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 2 | 1 | 0 | 3 | 0 | Lost | ||||||||||||||
| PC-39 | F | 64 | H | PDAC | I | 2088 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | Died | ||||||||||||||
| PC-40 | F | 49 | H | PDAC | I | 90.52 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 0 | 1 | 2 | 0 | Died | ||||||||||||||
| BTP-1 | F | PCN | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 2 | 0 | 2 | 0 | |||||||||||||||||||
| BTP-2 | M | AIP | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||
| BTP-3 | M | PCN | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 1 | 0 | 1 | 0 | |||||||||||||||||||
| BTP-4 | M | IPMN | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||
| BTP-5 | F | IPMN | 0 | 0 | 0 | 0 | 1 | 1 | 0 | / | 0 | 0 | 1 | 1 | 0 | |||||||||||||||||||
| BTP-6 | F | PCN | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 0 | 1 | 2 | 0 | |||||||||||||||||||
| BTP-7 | M | IPMN | 0 | 0 | 0 | 0 | 1 | 1 | 0 | / | 1 | 0 | 0 | 1 | 0 | |||||||||||||||||||
| BTP-8 | M | AC | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 1 | 1 | 2 | 0 | |||||||||||||||||||
| HC-1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 1 | 2 | 0 | |||||||||||||||||||||
| HC-3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 1 | 0 | 1 | 0 | |||||||||||||||||||||
| HC-6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-9 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-11 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-12 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-13 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-14 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-15 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 1 | 1 | 0 | |||||||||||||||||||||
| HC-16 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-17 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 1 | 0 | 1 | 0 | |||||||||||||||||||||
| HC-19 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 1 | 1 | 2 | 0 | |||||||||||||||||||||
| HC-20 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 2 | 0 | 0 | 2 | 0 | |||||||||||||||||||||
| HC-21 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-22 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 0 | 0 | 1 | 0 | |||||||||||||||||||||
| HC-23 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 1 | 1 | 0 | |||||||||||||||||||||
| HC-24 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-25 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-26 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-27 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 1 | 0 | 1 | 0 | |||||||||||||||||||||
| HC-28 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 1 | 1 | 0 | |||||||||||||||||||||
| HC-29 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-30 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 0 | 0 | 1 | 0 | |||||||||||||||||||||
| HC-31 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-32 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-33 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| HC-34 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 1 | 1 | 0 | 2 | 0 | |||||||||||||||||||||
| HC-35 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||||
| Cell Line | Cells Found by Technologist | Cells Found by the Electronic Microscope | Average | ||
|---|---|---|---|---|---|
| Cycle 1 | Cycle 2 | Cycle 3 | |||
| Bxpc-3 | 0 | 0 | 0 | 0 | 0 |
| 6 | 6 | 6 | 6 | 6 | |
| 12 | 12 | 12 | 12 | 12 | |
| 186 | 193 | 191 | 191 | 191 | |
| PANC-1 | 0 | 0 | 0 | 0 | 0 |
| 5 | 5 | 5 | 5 | 5 | |
| 10 | 10 | 10 | 10 | 10 | |
| 172 | 186 | 182 | 178 | 182 | |
| A549 | 11 | 11 | 11 | 10 | 10 |
| 32 | 32 | 32 | 31 | 31 | |
| 118 | 120 | 118 | 119 | 119 | |
| SW480 | 5 | 5 | 5 | 5 | 5 |
| 34 | 34 | 34 | 33 | 33 | |
| 98 | 98 | 98 | 96 | 97 | |
| SK-BR3 | 7 | 7 | 7 | 7 | 7 |
| 41 | 43 | 43 | 43 | 43 | |
| 140 | 145 | 143 | 143 | 143 | |
| Patients Codes | Stage | Before Chemotherapy | After 3 Weeks | ||
|---|---|---|---|---|---|
| The Number of CTMs | CA19-9 Value (U/mL) | The Number of CTMs | CA19-9 Value (U/mL) | ||
| PC-8 | IV | 0 | 22.18 | 1 | 6.9 |
| PC-9 | IV | 0 | 13,162 | 5 | 78,182 |
| PC-10 | IV | 2 | 3954 | 1 | 11,356 |
| PC-11 | IV | 1 | 132,070 | 1 | 173,664 |
| PC-12 | IV | 0 | 71,019 | 1 | 73,780 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, Y.; Qin, T.; Li, J.; Wang, X.; Gao, C.; Xu, C.; Hao, J.; Liu, J.; Gao, S.; Ren, H. Detection of Circulating Tumor Cells Using Negative Enrichment Immunofluorescence and an In Situ Hybridization System in Pancreatic Cancer. Int. J. Mol. Sci. 2017, 18, 622. https://doi.org/10.3390/ijms18040622
Xu Y, Qin T, Li J, Wang X, Gao C, Xu C, Hao J, Liu J, Gao S, Ren H. Detection of Circulating Tumor Cells Using Negative Enrichment Immunofluorescence and an In Situ Hybridization System in Pancreatic Cancer. International Journal of Molecular Sciences. 2017; 18(4):622. https://doi.org/10.3390/ijms18040622
Chicago/Turabian StyleXu, Yu, Tai Qin, Jing Li, Xiuchao Wang, Chuntao Gao, Chao Xu, Jihui Hao, Jingcheng Liu, Song Gao, and He Ren. 2017. "Detection of Circulating Tumor Cells Using Negative Enrichment Immunofluorescence and an In Situ Hybridization System in Pancreatic Cancer" International Journal of Molecular Sciences 18, no. 4: 622. https://doi.org/10.3390/ijms18040622