New Insights into the Role of Matrix Metalloproteinases in Preeclampsia


{kind=link}
Abstract
:1. Introduction
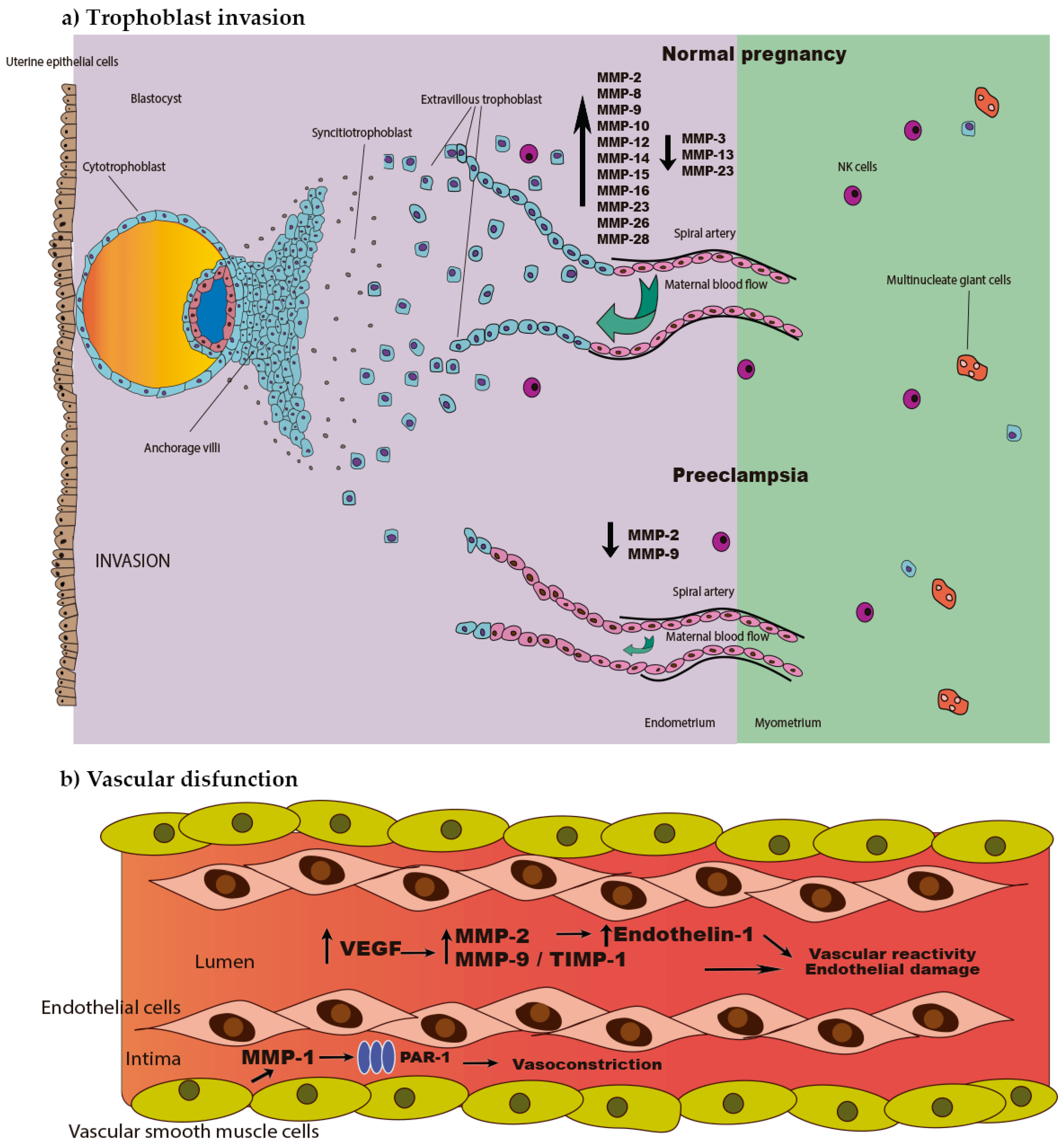
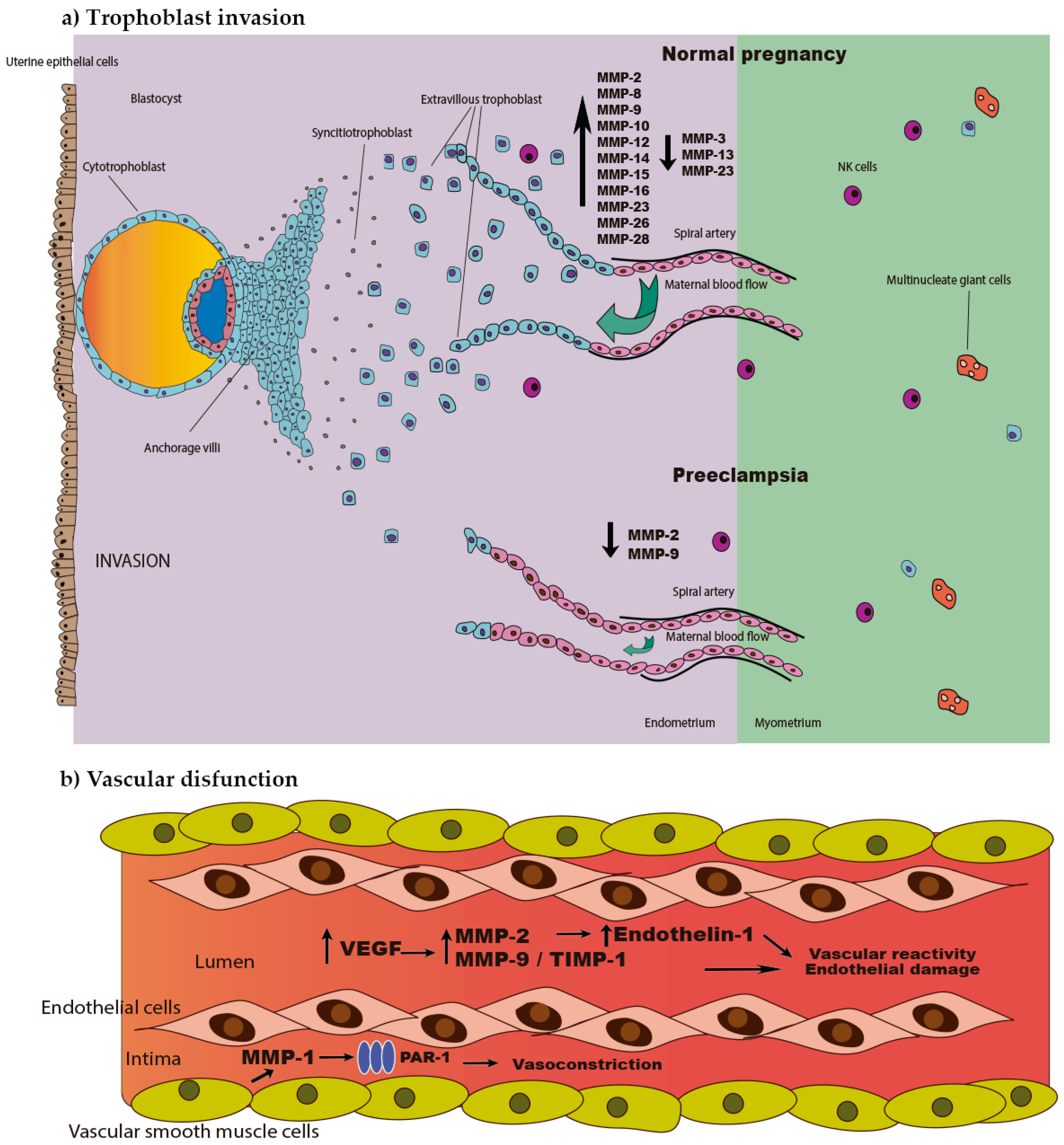
2. MMPs in Trophoblast Implantation and Invasion in Normal Pregnancy and Preeclampsia
3. MMPs and Endothelial Dysfunction in Preeclampsia
4. MMPs as New Biomarkers and Potential Biological Targets in Preeclampsia
Conflicts of Interest
References
- Bonnans, C.; Chou, J.; Werb, Z. Remodelling the extracellular matrix in development and disease. Nat. Rev. Mol. Cell Biol. 2014, 15, 786–801. [Google Scholar] [CrossRef] [PubMed]
- Nagase, H.; Visse, R.; Murphy, G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc. Res. 2006, 69, 562–573. [Google Scholar] [CrossRef] [PubMed]
- Bode, W.; Maskos, K. Structural basis of the matrix metalloproteinases and their physiological inhibitors, the tissue inhibitors of metalloproteinases. Biol. Chem. 2003, 384, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Massova, I.; Kotra, L.P.; Fridman, R.; Mobashery, S. Matrix metalloproteinases: Structures, evolution, and diversification. FASEB J. 1998, 12, 1075–1095. [Google Scholar] [PubMed]
- Vincenti, M.P. The matrix metalloproteinase (MMP) and tissue inhibitor of metalloproteinase (TIMP) genes. Transcriptional and posttranscriptional regulation, signal transduction and cell-type-specific expression. Methods Mol. Biol. 2001, 151, 121–148. [Google Scholar] [PubMed]
- Ra, H.J.; Parks, W.C. Control of matrix metalloproteinase catalytic activity. Matrix Biol. 2007, 26, 587–596. [Google Scholar] [CrossRef] [PubMed]
- Gomez, D.E.; Alonso, D.F.; Yoshiji, H.; Thorgeirsson, U.P. Tissue inhibitors of metalloproteinases: Structure, regulation and biological functions. Eur. J. Cell Biol. 1997, 74, 111–122. [Google Scholar] [PubMed]
- Yamamoto, K.; Murphy, G.; Troeberg, L. Extracellular regulation of metalloproteinases. Matrix Biol. 2015, 44–46, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Tjaderhane, L.; Salo, T. Matrix metalloproteinases (MMPs) in oral diseases. Oral Dis. 2004, 10, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Avila, V.; Spencer, J.V. Methods for Detection of Matrix Metalloproteinases as Biomarkers in Cardiovascular Disease. Clin. Med. Insights Cardiol. 2008, 2, 75–87. [Google Scholar]
- Klein, T.; Bischoff, R. Physiology and pathophysiology of matrix metalloproteases. Amino Acids 2011, 41, 271–290. [Google Scholar] [CrossRef] [PubMed]
- Strauss, J.F., III. Extracellular matrix dynamics and fetal membrane rupture. Reprod. Sci. 2013, 20, 140–153. [Google Scholar] [CrossRef] [PubMed]
- Vadillo-Ortega, F.; Gonzalez-Avila, G.; Furth, E.E.; Lei, H.; Muschel, R.J.; Stetler-Stevenson, W.G.; Strauss, J.F., III. 92-Kd type IV Collagenase (matrix metalloproteinase-9) activity in human amniochorion increases with labor. Am. J. Pathol. 1995, 146, 148–156. [Google Scholar] [PubMed]
- Parry, S.; Strauss, J.F., III. Premature rupture of the fetal membranes. N. Engl. J. Med. 1998, 338, 663–670. [Google Scholar] [PubMed]
- Vadillo-Ortega, F.; Estrada-Gutierrez, G. Role of matrix metalloproteinases in preterm labour. BJOG Int. J. Obst. Gynaecol. 2005, 112, 19–22. [Google Scholar] [CrossRef] [PubMed]
- ACOG Practice Bulletin. Diagnosis and management of preeclampsia and eclampsia. Obstet. Gynecol. 2002, 99, 159–167. [Google Scholar]
- Sahay, A.S.; Sundrani, D.P.; Joshi, S.R. Regional changes of placental vascularization in preeclampsia: A review. IUBMB Life 2015, 67, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Merchant, S.J.; Davidge, S.T. The role of matrix metalloproteinases in vascular function: Implications for normal pregnancy and pre-eclampsia. BJOG Int. J. Obst. Gynaecol. 2004, 111, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.E.; Merchant, S.J.; Macleod, M.; Mires, G.J.; Baker, P.N.; Davidge, S.T. MMP-2 levels are elevated in the plasma of women who subsequently develop preeclampsia. Hypertens. Pregnancy 2005, 24, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Pollheimer, J.; Fock, V.; Knofler, M. Review: The ADAM metalloproteinases—Novel regulators of trophoblast invasion? Placenta 2014, 35, S57–S63. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.M.; Enders, A.C.; Pijnenborg, R. The role of invasive trophoblast in implantation and placentation of primates. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2015, 370, 20140070. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.Y.; Pang, Z.J.; Yu, Y.H. Regulation of trophoblast invasion: The role of matrix metalloproteinases. Rev. Obstet. Gynecol. 2012, 5, e137–e143. [Google Scholar] [PubMed]
- Staun-Ram, E.; Goldman, S.; Gabarin, D.; Shalev, E. Expression and importance of matrix metalloproteinase 2 and 9 (MMP-2 and -9) in human trophoblast invasion. Reprod. Biol. Endocrinol. 2004, 2, 59. [Google Scholar] [CrossRef] [PubMed]
- Plaks, V.; Rinkenberger, J.; Dai, J.; Flannery, M.; Sund, M.; Kanasaki, K.; Ni, W.; Kalluri, R.; Werb, Z. Matrix metalloproteinase-9 deficiency phenocopies features of preeclampsia and intrauterine growth restriction. Proc. Natl. Acad. Sci. USA 2013, 110, 11109–11114. [Google Scholar] [CrossRef] [PubMed]
- Anacker, J.; Segerer, S.E.; Hagemann, C.; Feix, S.; Kapp, M.; Bausch, R.; Kammerer, U. Human decidua and invasive trophoblasts are rich sources of nearly all human matrix metalloproteinases. Mol. Hum. Reprod. 2011, 17, 637–652. [Google Scholar] [CrossRef] [PubMed]
- Seval, Y.; Akkoyunlu, G.; Demir, R.; Asar, M. Distribution patterns of matrix metalloproteinase (MMP)-2 and -9 and their inhibitors (TIMP-1 and TIMP-2) in the human decidua during early pregnancy. Acta Histochem. 2004, 106, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Rahat, B.; Sharma, R.; Bagga, R.; Hamid, A.; Kaur, J. Imbalance between matrix metalloproteinases and their tissue inhibitors in preeclampsia and gestational trophoblastic diseases. Reproduction 2016, 152, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Nissi, R.; Talvensaari-Mattila, A.; Kotila, V.; Niinimaki, M.; Jarvela, I.; Turpeenniemi-Hujanen, T. Circulating matrix metalloproteinase MMP-9 and MMP-2/TIMP-2 complex are associated with spontaneous early pregnancy failure. Reprod. Biol. Endocrinol. 2013, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Long, Q.; Ling, L.; Gao, A.; Li, H.; Lin, Q. Elevated expression of KiSS-1 in placenta of preeclampsia and its effect on trophoblast. Reprod. Biol. 2011, 11, 99–115. [Google Scholar] [CrossRef]
- Shokry, M.; Omran, O.M.; Hassan, H.I.; Elsedfy, G.O.; Hussein, M.R. Expression of matrix metalloproteinases 2 and 9 in human trophoblasts of normal and preeclamptic placentas: Preliminary findings. Exp. Mol. Pathol. 2009, 87, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Zhong, M.; Pang, Z.; Yu, Y. Dysregulated expression of matrix metalloproteinases and their inhibitors may participate in the pathogenesis of pre-eclampsia and fetal growth restriction. Early Hum. Dev. 2014, 90, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.; Ribaux, P.; Epiney, M.; Irion, O. Expression of metalloproteinases 1, 2, 7, 9, and 12 in human cytotrophoblastic cells from normal and preeclamptic placentas. Neuro Endocrinol. Lett. 2012, 33, 406–411. [Google Scholar] [PubMed]
- Raffetto, J.D.; Khalil, R.A. Matrix metalloproteinases and their inhibitors in vascular remodeling and vascular disease. Biochem. Pharmacol. 2008, 75, 346–359. [Google Scholar] [CrossRef] [PubMed]
- Palei, A.C.; Sandrim, V.C.; Amaral, L.M.; Machado, J.S.; Cavalli, R.C.; Duarte, G.; Tanus-Santos, J.E. Association between matrix metalloproteinase (MMP)-2 polymorphisms and MMP-2 levels in hypertensive disorders of pregnancy. Exp. Mol. Pathol. 2012, 92, 217–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narumiya, H.; Zhang, Y.; Fernandez-Patron, C.; Guilbert, L.J.; Davidge, S.T. Matrix metalloproteinase-2 is elevated in the plasma of women with preeclampsia. Hypertens. Pregnancy 2001, 20, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Montagnana, M.; Lippi, G.; Albiero, A.; Scevarolli, S.; Salvagno, G.L.; Franchi, M.; Guidi, G.C. Evaluation of metalloproteinases 2 and 9 and their inhibitors in physiologic and pre-eclamptic pregnancy. J. Clin. Lab. Anal. 2009, 23, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Palei, A.C.; Sandrim, V.C.; Amaral, L.M.; Machado, J.S.; Cavalli, R.C.; Lacchini, R.; Duarte, G.; Tanus-Santos, J.E. Matrix metalloproteinase-9 polymorphisms affect plasma MMP-9 levels and antihypertensive therapy responsiveness in hypertensive disorders of pregnancy. Pharmacogenom. J. 2012, 12, 489–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karampas, G.; Eleftheriades, M.; Panoulis, K.; Rizou, M.; Haliassos, A.; Hassiakos, D.; Vitoratos, N.; Rizos, D. Maternal serum levels of neutrophil gelatinase-associated lipocalin (NGAL), matrix metalloproteinase-9 (MMP-9) and their complex MMP-9/NGAL in pregnancies with preeclampsia and those with a small for gestational age neonate: A longitudinal study. Prenat. Diagn. 2014, 34, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Palei, A.C.; Sandrim, V.C.; Cavalli, R.C.; Tanus-Santos, J.E. Comparative assessment of matrix metalloproteinase (MMP)-2 and MMP-9, and their inhibitors, tissue inhibitors of metalloproteinase (TIMP)-1 and TIMP-2 in preeclampsia and gestational hypertension. Clin. Biochem. 2008, 41, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Tayebjee, M.H.; Karalis, I.; Nadar, S.K.; Beevers, D.G.; MacFadyen, R.J.; Lip, G.Y. Circulating matrix metalloproteinase-9 and tissue inhibitors of metalloproteinases-1 and -2 levels in gestational hypertension. Am. J. Hypertens. 2005, 18, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Estrada-Gutierrez, G.; Cappello, R.E.; Mishra, N.; Romero, R.; Strauss, J.F., III; Walsh, S.W. Increased expression of matrix metalloproteinase-1 in systemic vessels of preeclamptic women: A critical mediator of vascular dysfunction. Am. J. Pathol. 2011, 178, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Nugent, W.H.; Mishra, N.; Strauss, J.F., III; Walsh, S.W. Matrix Metalloproteinase 1 Causes Vasoconstriction and Enhances Vessel Reactivity to Angiotensin II via Protease-Activated Receptor 1. Reprod. Sci. 2016, 23, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Mousa, A.A.; Cappello, R.E.; Estrada-Gutierrez, G.; Shukla, J.; Romero, R.; Strauss, J.F., III; Walsh, S.W. Preeclampsia is associated with alterations in DNA methylation of genes involved in collagen metabolism. Am. J. Pathol. 2012, 181, 1455–1463. [Google Scholar] [CrossRef] [PubMed]
- Mousa, A.A.; Archer, K.J.; Cappello, R.; Estrada-Gutierrez, G.; Isaacs, C.R.; Strauss, J.F., III; Walsh, S.W. DNA methylation is altered in maternal blood vessels of women with preeclampsia. Reprod. Sci. 2012, 19, 1332–1342. [Google Scholar] [CrossRef] [PubMed]
- Ab Hamid, J.; Mohtarrudin, N.; Osman, M.; Andi Asri, A.A.; Wan Hassan, W.H.; Aziz, R. Matrix metalloproteinase-9 and tissue inhibitors of metalloproteinases 1 and 2 as potential biomarkers for gestational hypertension. Singap. Med. J. 2012, 53, 681–683. [Google Scholar]
- Feng, H.; Wang, L.; Zhang, M.; Zhang, Z.; Guo, W.; Wang, X. Ratio of matrix metalloproteinase-2 to -9 is a more accurate predictive biomarker in women with suspected preeclampsia. Biosci. Rep. 2017, 37, BSR20160508. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.C.; Nekrasova, E.; Anastassopoulos, P.; Livanos, P.; Nicolaides, K.H. First-trimester maternal serum matrix metalloproteinase-9 (MMP-9) and adverse pregnancy outcome. Prenat. Diagn. 2009, 29, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Fierro, M.L.; Perez-Favila, A.; Garza-Veloz, I.; Espinoza-Juarez, M.A.; Avila-Carrasco, L.; Delgado-Enciso, I.; Ortiz-Castro, Y.; Cardenas-Vargas, E.; Cid-Baez, M.A.; Ramirez-Santoyo, R.M.; et al. Matrix metalloproteinase multiplex screening identifies increased MMP-2 urine concentrations in women predicted to develop preeclampsia. Biomarkers 2017, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Gu, Y.; Loyd, S.; Jia, X.; Groome, L.J. Increased urinary levels of podocyte glycoproteins, matrix metallopeptidases, inflammatory cytokines, and kidney injury biomarkers in women with preeclampsia. Am. J. Phys. Ren. Phys. 2015, 309, F1009–F1017. [Google Scholar] [CrossRef] [PubMed]
- Coolman, M.; de Maat, M.; van Heerde, W.L.; Felida, L.; Schoormans, S.; Steegers, E.A.; Bertina, R.M.; de Groot, C.J. Matrix metalloproteinase-9 gene-1562C/T polymorphism mitigates preeclampsia. Placenta 2007, 28, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, Z.; Rahimi, Z.; Shahsavandi, M.O.; Bidoki, K.; Rezaei, M. MMP-9 (-1562 C:T) polymorphism as a biomarker of susceptibility to severe pre-eclampsia. Biomark. Med. 2013, 7, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Zhang, Q.; Hu, B.; Zhang, K. Investigation of the association between matrix metalloproteinase-9 genetic polymorphisms and development of pre-eclampsia in Chinese pregnant women. Genet. Mol. Res. 2016, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- Luizon, M.R.; Sandrim, V.C.; Palei, A.C.; Lacchini, R.; Cavalli, R.C.; Duarte, G.; Tanus-Santos, J.E. Epistasis among eNOS, MMP-9 and VEGF maternal genotypes in hypertensive disorders of pregnancy. Hypertens. Res. 2012, 35, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Fraser, R.; Walker, J.J.; Ekbote, U.V.; Martin, K.L.; McShane, P.; Orsi, N.M. Interleukin-4 -590 (C > T), toll-like receptor-2 +2258 (G > A) and matrix metalloproteinase-9 -1562 (C > T) polymorphisms in pre-eclampsia. BJOG Int. J. Obstet. Gynaecol. 2008, 115, 1052–1056. [Google Scholar] [CrossRef] [PubMed]
- Leonardo, D.P.; Albuquerque, D.M.; Lanaro, C.; Baptista, L.C.; Cecatti, J.G.; Surita, F.G.; Parpinelli, M.A.; Costa, F.F.; Franco-Penteado, C.F.; Fertrin, K.Y.; Costa, M.L. Association of Nitric Oxide Synthase and Matrix Metalloprotease Single Nucleotide Polymorphisms with Preeclampsia and Its Complications. PLoS ONE 2015, 10, e0136693. [Google Scholar] [CrossRef] [PubMed]
- Gong, L.L.; Liu, H.; Liu, L.H. Lack of association between matrix metalloproteinase-9 gene-1562C/T polymorphism and preeclampsia: A meta-analysis. Hypertens. Pregnancy 2014, 33, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.M.; Zhang, S.L. Non-association of MMP-9 -1562C/T polymorphism with preeclampsia risk: Evidence from a meta-analysis. Clin. Exp. Obstet. Gynecol. 2015, 42, 730–735. [Google Scholar] [PubMed]
- Palei, A.C.; Sandrim, V.C.; Amaral, L.M.; Machado, J.S.; Cavalli, R.C.; Lacchini, R.; Duarte, G.; Tanus-Santos, J.E. Effects of matrix metalloproteinase (MMP)-2 polymorphisms on responsiveness to antihypertensive therapy of women with hypertensive disorders of pregnancy. Basic Clin. Pharmacol. Toxicol. 2012, 111, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Kaitu’u-Lino, T.J.; Palmer, K.R.; Whitehead, C.L.; Williams, E.; Lappas, M.; Tong, S. MMP-14 is expressed in preeclamptic placentas and mediates release of soluble endoglin. Am. J. Pathol. 2012, 180, 888–894. [Google Scholar] [CrossRef] [PubMed]
- Kaitu’u-Lino, T.J.; Tuohey, L.; Ye, L.; Palmer, K.; Skubisz, M.; Tong, S. MT-MMPs in pre-eclamptic placenta: Relationship to soluble endoglin production. Placenta 2013, 34, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Majali-Martinez, A.; Velicky, P.; Pollheimer, J.; Knofler, M.; Yung, H.W.; Burton, G.J.; Tabrizi-Wizsy, N.G.; Lang, U.; Hiden, U.; Desoye, G.; Dieber-Rotheneder, M. Endothelin-1 down-regulates matrix metalloproteinase 14 and 15 expression in human first trimester trophoblasts via endothelin receptor type B. Hum. Reprod. 2017, 32, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Cim, N.; Kurdoglu, M.; Ege, S.; Yoruk, I.; Yaman, G.; Yildizhan, R. An analysis on the roles of angiogenesis-related factors including serum vitamin D, soluble endoglin (sEng), soluble fms-like tyrosine kinase 1 (sFlt1), and vascular endothelial growth factor (VEGF) in the diagnosis and severity of late-onset preeclampsia. J. Matern. Fetal Neonatal Med. 2017, 30, 1602–1607. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Patron, C.; Zouki, C.; Whittal, R.; Chan, J.S.; Davidge, S.T.; Filep, J.G. Matrix metalloproteinases regulate neutrophil-endothelial cell adhesion through generation of endothelin-1 [1–32]. FASEB J. 2001, 15, 2230–2240. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Patron, C.; Radomski, M.W.; Davidge, S.T. Vascular matrix metalloproteinase-2 cleaves big endothelin-1 yielding a novel vasoconstrictor. Circ. Res. 1999, 85, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, M.M.; Khalil, R.A. Matrix metalloproteinase inhibitors as investigative tools in the pathogenesis and management of vascular disease. EXS 2012, 103, 209–279. [Google Scholar] [PubMed]
- Palei, A.C.; Sandrim, V.C.; Duarte, G.; Cavalli, R.C.; Gerlach, R.F.; Tanus-Santos, J.E. Matrix metalloproteinase (MMP)-9 genotypes and haplotypes in preeclampsia and gestational hypertension. Clin. Chim. Acta Int. J. Clin. Chem. 2010, 411, 874–877. [Google Scholar] [CrossRef] [PubMed]
- Pillar, N.; Yoffe, L.; Hod, M.; Shomron, N. The possible involvement of microRNAs in preeclampsia and gestational diabetes mellitus. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Biro, O.; Nagy, B.; Rigo, J., Jr. Identifying miRNA regulatory mechanisms in preeclampsia by systems biology approaches. Hypertens. Pregnancy 2017, 36, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Mayor-Lynn, K.; Toloubeydokhti, T.; Cruz, A.C.; Chegini, N. Expression profile of microRNAs and mRNAs in human placentas from pregnancies complicated by preeclampsia and preterm labor. Reprod. Sci. 2011, 18, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Pan, Q.; Niu, H.; Cheng, L.; Li, X.; Zhang, Q.; Ning, Y. Invasion of trophoblast cell lines is inhibited by miR-93 via MMP-2. Placenta 2017, 53, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Su, M.T.; Tsai, P.Y.; Tsai, H.L.; Chen, Y.C.; Kuo, P.L. miR-346 and miR-582–3p-regulated EG-VEGF expression and trophoblast invasion via matrix metalloproteinases 2 and 9. BioFactors 2017, 43, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Sandrim, V.C.; Luizon, M.R.; Palei, A.C.; Tanus-Santos, J.E.; Cavalli, R.C. Circulating microRNA expression profiles in pre-eclampsia: Evidence of increased miR-885–5p levels. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 2120–2128. [Google Scholar] [CrossRef] [PubMed]
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espino Y. Sosa, S.; Flores-Pliego, A.; Espejel-Nuñez, A.; Medina-Bastidas, D.; Vadillo-Ortega, F.; Zaga-Clavellina, V.; Estrada-Gutierrez, G. New Insights into the Role of Matrix Metalloproteinases in Preeclampsia. Int. J. Mol. Sci. 2017, 18, 1448. https://doi.org/10.3390/ijms18071448
Espino Y. Sosa S, Flores-Pliego A, Espejel-Nuñez A, Medina-Bastidas D, Vadillo-Ortega F, Zaga-Clavellina V, Estrada-Gutierrez G. New Insights into the Role of Matrix Metalloproteinases in Preeclampsia. International Journal of Molecular Sciences. 2017; 18(7):1448. https://doi.org/10.3390/ijms18071448
Chicago/Turabian StyleEspino Y. Sosa, Salvador, Arturo Flores-Pliego, Aurora Espejel-Nuñez, Diana Medina-Bastidas, Felipe Vadillo-Ortega, Veronica Zaga-Clavellina, and Guadalupe Estrada-Gutierrez. 2017. "New Insights into the Role of Matrix Metalloproteinases in Preeclampsia" International Journal of Molecular Sciences 18, no. 7: 1448. https://doi.org/10.3390/ijms18071448