The Pathophysiology of Post-Traumatic Glioma

 , , , and
, , , and
Abstract
:1. Introduction
2. Brain Injury and Repair Processes
3. The Role of IL-6 Secreted by Macrophages
4. The Role of Eosinophil Peroxidase and Reactive Oxygen Species (ROS)
5. Inflow of Stem Cells
6. The Role of Microglia Cells
7. Interruption of the Blood–Brain Barrier
8. Epidemiological and Experimental Research on Post-Traumatic Glioma
9. Strategy for Further Study and at the Clinical Approach
10. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Li, W.; Graeber, M.B. The molecular profile of microglia under the influence of glioma. Neuro Oncol. 2012, 14, 958–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyagi, V.; Theobald, J.; Barger, J.; Bustoros, M.; Bayin, N.S.; Modrek, A.S.; Kader, M.; Anderer, E.G.; Donahue, B.; Fatterpekar, G.; et al. Traumatic brain injury and subsequent glioblastoma development: Review of the literature and case reports. Surg. Neurol. Int. 2016, 26, 77–78. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Gittleman, H.; Liao, P.; Rouse, C.; Chen, Y.; Dowling, J.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2007–2011. Neuro Oncol. 2014, 16, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Schwartzbaum, J.A.; Fisher, J.L.; Aldape, K.D.; Wrensch, M. Epidemiology and molecular pathology of glioma. Nat. Clin. Pract. Neurol. 2006, 2, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Munch, T.N.; Gørtz, S.; Wohlfahrt, J.; Melbye, M. The long-term risk of malignant astrocytic tumors after structural brain injury—A nationwide cohort study. Neuro Oncol. 2015, 17, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Han, Z.; Du, Y.; Qi, H.; Yin, W. Post-traumatic malignant glioma in a pregnant woman: Case report and review of the literature. Neurol. Med. Chir. 2013, 53, 630–634. [Google Scholar] [CrossRef]
- Zhou, B.; Liu, W. Post-traumatic glioma: Report of one case and review of the literature. Int. J. Med. Sci. 2010, 7, 248–250. [Google Scholar] [CrossRef] [PubMed]
- Bohman, L.E.; Swanson, K.R.; Moore, J.L.; Rockne, R.; Mandigo, C.; Hankinson, T.; Assanah, M.; Canoll, P.; Bruce, J.N. Magnetic Resonance Imaging Characteristics of Glioblastoma Multiforme: Implications for Understanding Gliomna Ontogeny. Neurosurgery 2010, 67, 1319–1328. [Google Scholar] [CrossRef] [PubMed]
- Moorthy, R.K.; Rajshekhar, V. Development of glioblastoma multiforme following traumatic cerebral contusion: Case report and review of literature. Surg. Neurol. 2004, 61, 180–184. [Google Scholar] [CrossRef]
- Xu, B.; Yu, D.M.; Liu, F.S. Effect of siRNA induced inhibition of IL 6 expression in rat cerebral gliocytes on cerebral edema following traumatic brain injury. Mol. Med. Rep. 2014, 10, 1863–1868. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, G.T.; Pereira, R.A.; Koifman, R.J.; Koifman, S. Head injury and brain tumours in adults: A case-control study in Rio de Janeiro, Brazil. Eur. J. Cancer 2006, 42, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Xu, Y.; Luo, Y.; Zheng, D.; Song, Y.; Yu, K.; Li, H.; Zhang, L.; Zhong, W.; Ji, Y. Down-regulation of Stat3 decreases invasion activity and induces apoptosis of human glioma cells. J. Mol. Neurosci. 2010, 40, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Iwamaru, A.; Szymanski, S.; Iwado, E.; Aoki, H.; Yokoyama, T.; Fokt, I.; Hess, K.; Conrad, C.; Madden, T.; Sawaya, R.; Kondo, S.; et al. A novel inhibitor of the STAT3 pathway induces apoptosis in malignant glioma cells both in vitro and in vivo. Oncogene 2007, 26, 2435–2444. [Google Scholar] [CrossRef] [PubMed]
- Sroka, J.; Madeja, Z. Reactive oxygen species in regulation of cell migration. The role of thioredoxin reductase. Postepy Biochem. 2009, 55, 145–152. [Google Scholar] [PubMed]
- Coskun, S.; Coskun, A.; Gursan, N.; Aydin, M.D. Post-traumatic glioblastoma multiforme: A case report. Eurasian J. Med. 2011, 43, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Sofroniew, M.V.; Vinters, H.V. Astrocytes: Biology and pathology. Acta Neuropathol. 2010, 119, 7–35. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.K.; Hawkins, C.; Clarke, I.D.; Squire, J.A.; Bayani, J.; Hide, T.; Henkelman, R.M.; Cusimano, M.D.; Dirks, P.B. Identification of Human brain tumour initiating cells. Nature 2004, 432, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Brantley, E.C.; Nabors, L.B.; Gillespie, G.Y.; Choi, Y.H.; Palmer, C.A.; Harrison, K.; Roarty, K.; Benveniste, E.N. Loss of protein inhibitors of activated STAT-3 expression in glioblastoma multiforme tumors: Implications for STAT 3 activation and gene expression. Clin. Cancer Res. 2008, 14, 4694–4704. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, J.E.; Imura, T.; Song, B.; Qi, J.; Ao, Y.; Nguyen, T.K.; Korsak, R.A.; Takeda, K.; Akira, S.; Sofroniew, M.V. STAT 3 is a critical regulator of astrogliosis and scar formation after spinal cord injury. J. Neurosci. 2008, 28, 7231–7243. [Google Scholar] [CrossRef] [PubMed]
- Korbecki, J.; Gutowska, I.; Kojder, I.; Jeżewski, D.; Goschorska, M.; Łukomska, A.; Lubkowska, A.; Chlubek, D.; Baranowska-Bosiacka, I. New extracellular factors in glioblastoma multiforme development: Neurotensin, growth differentiation factor-15, sphingosine-1-phosphate and cytomegalovirus infection. Oncotarget 2018, 9, 7219–7270. [Google Scholar] [CrossRef] [PubMed]
- Gil-Perotin, S.; Marin-Husstege, M.; Li, J.; Soriano-Navarro, M.; Zindy, F.; Roussel, M.F.; Garcia-Verdugo, J.M.; Casaccia-Bonnefil, P. Loss of p53 induces changes in the behavior of subventricular zone cells: Implication for the genesis of glial tumors. J. Neurosci. 2006, 26, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Jackson, E.L.; Garcia-Verdugo, J.M.; Gil-Perotin, S.; Roy, M.; Quinones-Hinojosa, A.; VandenBerg, S.; Alvarez-Buylla, A. PDGFR alpha–positive B cells are neural stem cells in the adults SVZ that form glioma- like growths in response to increased PDGF signaling. Neuron 2006, 51, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Assanah, M.; Lochhead, R.; Ogden, A.; Bruce, J.; Goldman, J.; Canoll, P. Glial progenitors in adult white matter are driven to form malignant gliomas by platelet-derived growth factor-expressing retroviruses. J. Naurosci. 2006, 26, 6781–6790. [Google Scholar] [CrossRef] [PubMed]
- Larysz, M.; Becht, R.; Falco, M.; Nowacki, P.; Kojder, K. Glioblastoma multiforme in a patient with common variable immunodeficiency and multiple malignanies—A case report. Pomeranian J. Life Sci. 2017, 63, 46–49. [Google Scholar] [CrossRef]
- Madden, J.R.; Addo-Yobo, S.O.; Donson, A.M.; Liu, A.K.; McNatt, S.A.; Kleinschmidt-Demasters, B.K.; Fenton, L.Z.; Foreman, N.K.; Smith, A.A. Radiation-induced glioblastoma multiforme in children treated for medulloblastoma with characteristics of both medulloblastoma and glioblastoma multiforme. Pediatr. Hematol. Oncol. 2010, 32, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Furuta, T.; Nakada, M.; Ueda, F.; Watanabe, T.; Arakawa, Y.; Higashi, R.; Hashimoto, M.; Nitta, H.; Hayashi, Y.; Hamada, J. Prognostic paradox: Brain damage around the glioblastoma resection cavity. J. Neurooncol. 2014, 118, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Markovic, D.S.; Vinnakota, K.; Chirasani, S.; Synowitz, M.; Raguet, H.; Stock, K.; Sliwa, M.; Lehmann, S.; Kälin, R.; van Rooijen, N.; et al. Gliomas induce and exploit microglial MT1-MMP expression for tumor expansion. Proc. Natl. Acad. Sci. USA 2009, 106, 12530–12535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, H.; Heppner, F.L.; Tsirka, S.E. Microglia/macrophages promote glioma progression. Glia 2011, 59, 472–485. [Google Scholar] [CrossRef] [PubMed]
- Sawamura, Y.; Diserens, A.C.; de Tribolet, N. In vitro prostaglandin E2 production by glioblastoma cells and ist effect on IL2 activation of oncolytic lymphocytes. J. Neuroncol. 1990, 9, 125–130. [Google Scholar] [CrossRef]
- Patel, J.P.; Frey, B.N. Disruption in the Blood-Brain Barrier: The Missing Link between Brain and Body Inflammation in Bipolar Disorder? Neural. Plast. 2015, 708306. [Google Scholar] [CrossRef] [PubMed]
- Annegers, J.F.; Laws, E.R.; Kurland, L.T.; Grabow, J.D. Head trauma and subsequent brain tumors. Neurosurgery 1979, 4, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Inskip, P.D.; Mellemkjaer, L.; Gridley, G.; Olsen, J.H. Incidence of intracranial tumors following hospitalization for head injuries (Denmark). Cancer Causes Control 1998, 9, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Klein, C.F.; Gørtz, S.; Wohlfahrt, J.; Munch, T.N.; Melbye, M.; Bundgaard, H.; Iversen, K.K. Long-term risk of hemorrhagic stroke in patients with infective endocarditis: A Danish nationwide cohort study. Clin. Infect Dis. 2018. [Google Scholar] [CrossRef] [PubMed]
- Bunin, G.R.; Buckley, J.D.; Boesel, C.P.; Rorke, L.B.; Meadows, A.T. Risk factors for astrocytic glioma and primitive neuroectodermal tumor of the brain in young children: A report from the Children’s Cancer Group. Cancer Epidemiol. Biomarkers Prev. 1994, 3, 197–204. [Google Scholar] [PubMed]
- Hochberg, F.; Toniolo, P.; Cole, P. Head trauma and seizures as risk factors of glioblastoma. Neurology 1984, 34, 1511–1514. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Johnson, K.C.; Mao, Y.; Guo, L.; Zhao, X.; Jia, X.; Bi, D.; Huang, G.; Liu, R. Risk factors for glioma in adults: A case-control study in northeast China. Cancer Detect Prev. 1998, 22, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.H.; Keller, J.J.; Kang, J.H.; Lin, H.C. Association between traumatic brain injury and the subsequent risk of brain cancer. J. Neurotrauma 2012, 29, 1328–1333. [Google Scholar] [CrossRef] [PubMed]
- Salvati, M.; Caroli, E.; Rocchi, G.; Frati, A.; Brogna, C.; Orlando, E.R. Post-traumatic glioma. Report of four cases and review of the literature. Tumori J. 2004, 90, 416–419. [Google Scholar] [CrossRef] [PubMed]
- Henry, P.T.; Rajshekhar, V. Post-traumatic malignant glioma: Case report and review of the literature. Br. J. Neurosurg. 2000, 14, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Di Trapani, G.; Carnevale, A.; Scerrati, M.; Colosimo, C.; Vaccario, M.L.; Mei, D. Post-traumatic malignant glioma. Report of a case. Ital. J. Neurol. Sci. 1996, 17, 283–286. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
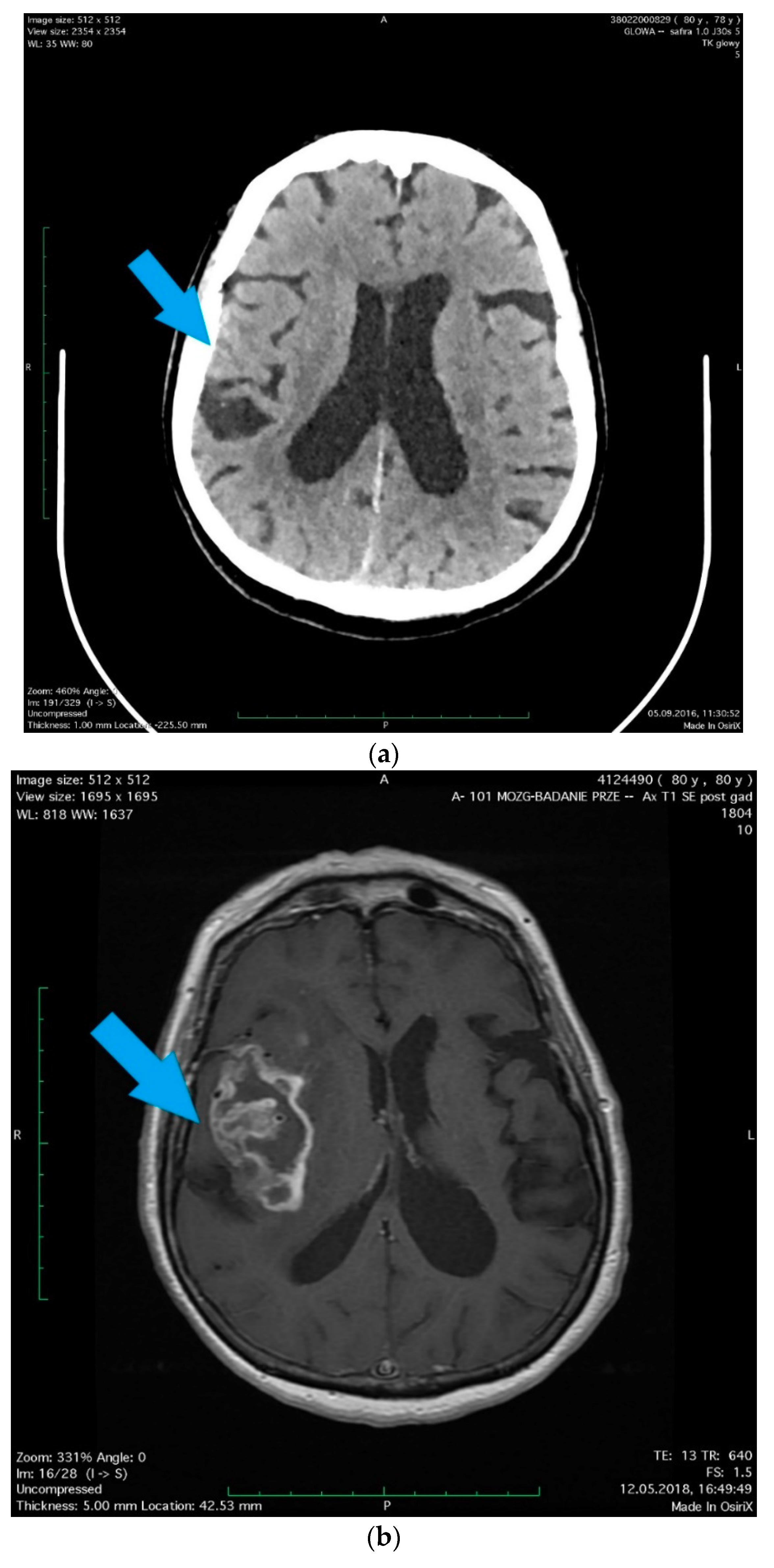
| Sex | Woman |
| Age | 78-year-old |
| Comorbidity | hypertension and hypercholesterolemia |
| Reason for admission to the hospital | head injury (after falling in moving bus) |
| CT test result | A little amount of blood along the falx of the brain, on the tent of the cerebellum on the right side in a fissure of the right parietal lobe with scant concussion in it. |
| The patient, without neurological deficits, except diminishing post-traumatic headaches, was discharged after the observation period in a good condition | |
| Readmission to the hospital | 2 years later |
| Reason for readmission to the hospital | diagnosed brain tumor |
| Symptoms | 1.5-month history of memory and orientation disorders |
| MRI test result | the right brain hemisphere tumor was found, the position of which corresponded to previous post-traumatic lesions |
| Treatment | right temporoparietal craniotomy was performed and the cytoreduction of the tumor was extended |
| Changes in the histopathological picture | characteristic necrosis, surrounded by a pseudopalisade, visible cell mitosis, large cell density, mitosis, lumen of the vessel with erythrocytes |
| Histopathological result | Glioblastoma multiforme |
| Further treatment | radiotherapy with chemotherapy |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simińska, D.; Kojder, K.; Jeżewski, D.; Kojder, I.; Skórka, M.; Gutowska, I.; Chlubek, D.; Baranowska-Bosiacka, I. The Pathophysiology of Post-Traumatic Glioma. Int. J. Mol. Sci. 2018, 19, 2445. https://doi.org/10.3390/ijms19082445
Simińska D, Kojder K, Jeżewski D, Kojder I, Skórka M, Gutowska I, Chlubek D, Baranowska-Bosiacka I. The Pathophysiology of Post-Traumatic Glioma. International Journal of Molecular Sciences. 2018; 19(8):2445. https://doi.org/10.3390/ijms19082445
Chicago/Turabian StyleSimińska, Donata, Klaudyna Kojder, Dariusz Jeżewski, Ireneusz Kojder, Marta Skórka, Izabela Gutowska, Dariusz Chlubek, and Irena Baranowska-Bosiacka. 2018. "The Pathophysiology of Post-Traumatic Glioma" International Journal of Molecular Sciences 19, no. 8: 2445. https://doi.org/10.3390/ijms19082445