
A Highly Sensitive Porous Silicon (P-Si)-Based Human Kallikrein 2 (hK2) Immunoassay Platform toward Accurate Diagnosis of Prostate Cancer

Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Derivatized Glass | Filter/Membrane | Gel Pad/Agarose Film | Porous Silicon | |
|---|---|---|---|---|
| Advantages | Cheap | Low cost | High sample capacity | High sample capacity |
| Compatible with most micro-arrayers | Reusable | Spot homogeneity | ||
| Low unspecific binding | ||||
| Disadvantages | Non-uniform spots (Coffee ring effect) | Limit of spot density | Expensive | Laborious procedures |
| Laborious procedures |

2. Experimental Section
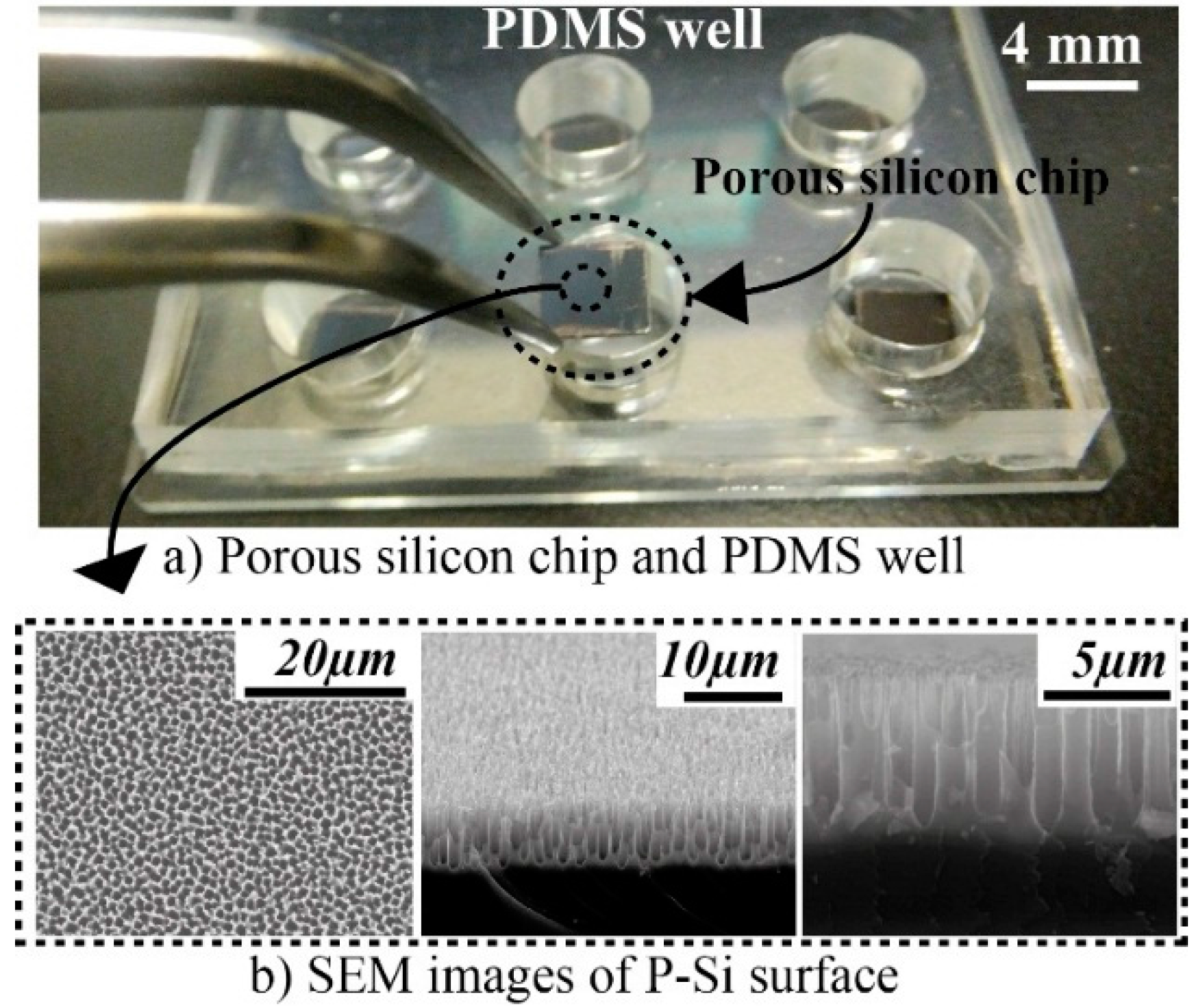
2.1. P-Si Fabrication
2.2. PDMS Well

2.3. Proteins and Reagents
2.4. Analytical Samples
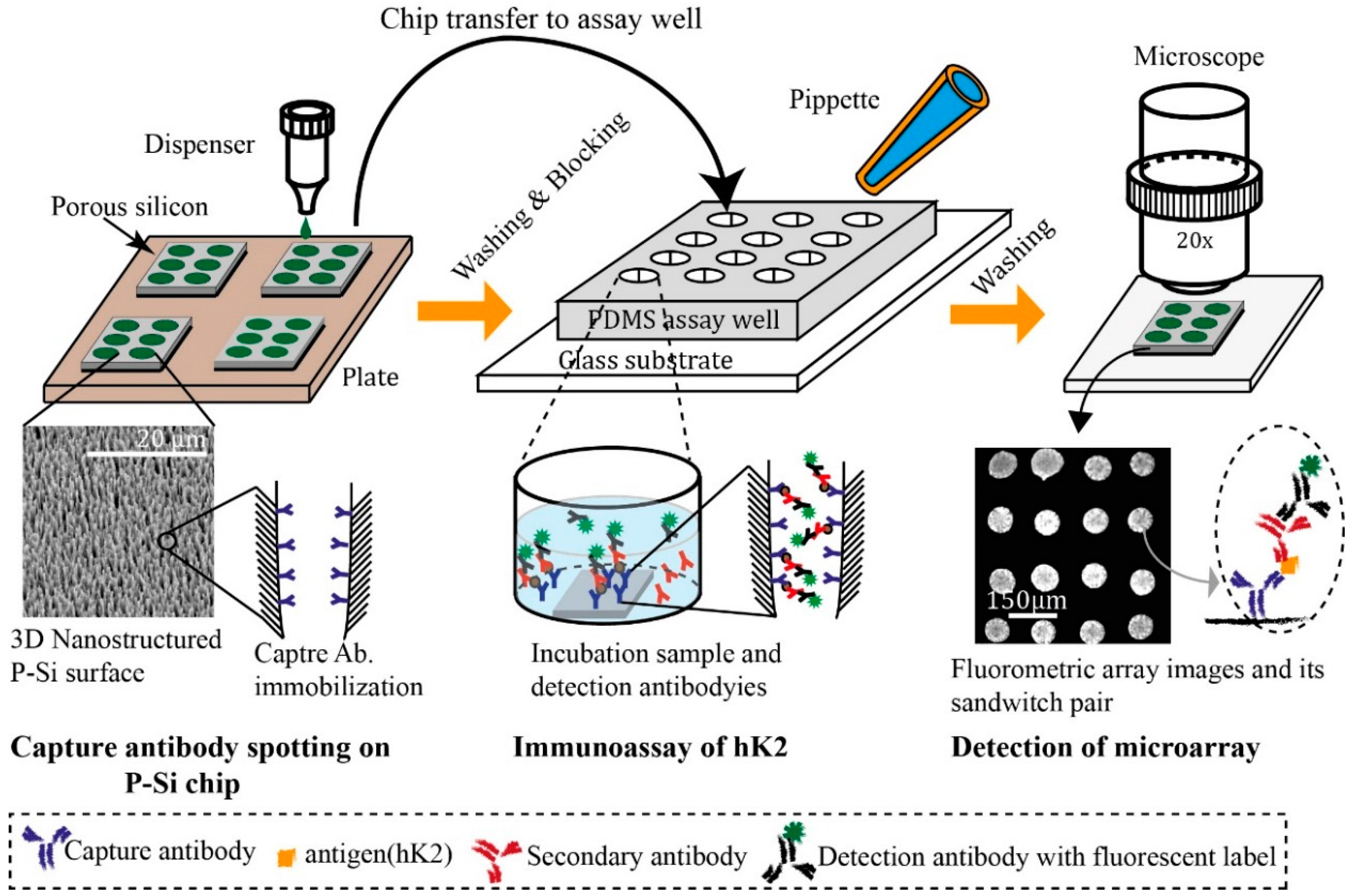
2.5. Sandwich Assay
- 1
- After arraying the antibody, the chips were washed three times using 10 mM PBS to remove loosely bound antibodies.
- 2
- The chips were incubated for 1 h in 100 µL blocking solution (5% (w/v) non-fat dry milk in PBS (Bio-Rad, Hercules, CA, USA)) to prevent non-specific binding and washed 3 times using 0.05% Tween 20 in 10 mM PBS.
- 3
- Following blocking, the chips were incubated with 15 µL of spiked sample for 1 h, then washed (as above) and subsequently incubated with 15 µL of detection antibody (polyclonal goat anti-hK2).
- 4
- After another washing step, 15 µL of AF488 labeled anti-goat polyclonal antibody was added onto the chips and incubated for 1 h.
- 5
- Finally, the chips were washed three times and dried at room temperature.
- 6
- The fluorescent spots images were observed using a eclipse TE2000-U fluorescence microscope (Nikon, Tokyo, Japan).
- 7
- The captured images were analyzed by the open source image-processing tool Image J.
2.6. Mean Spots Intensities and Limits of Detection
3. Results and Discussion
3.1. General Remarks
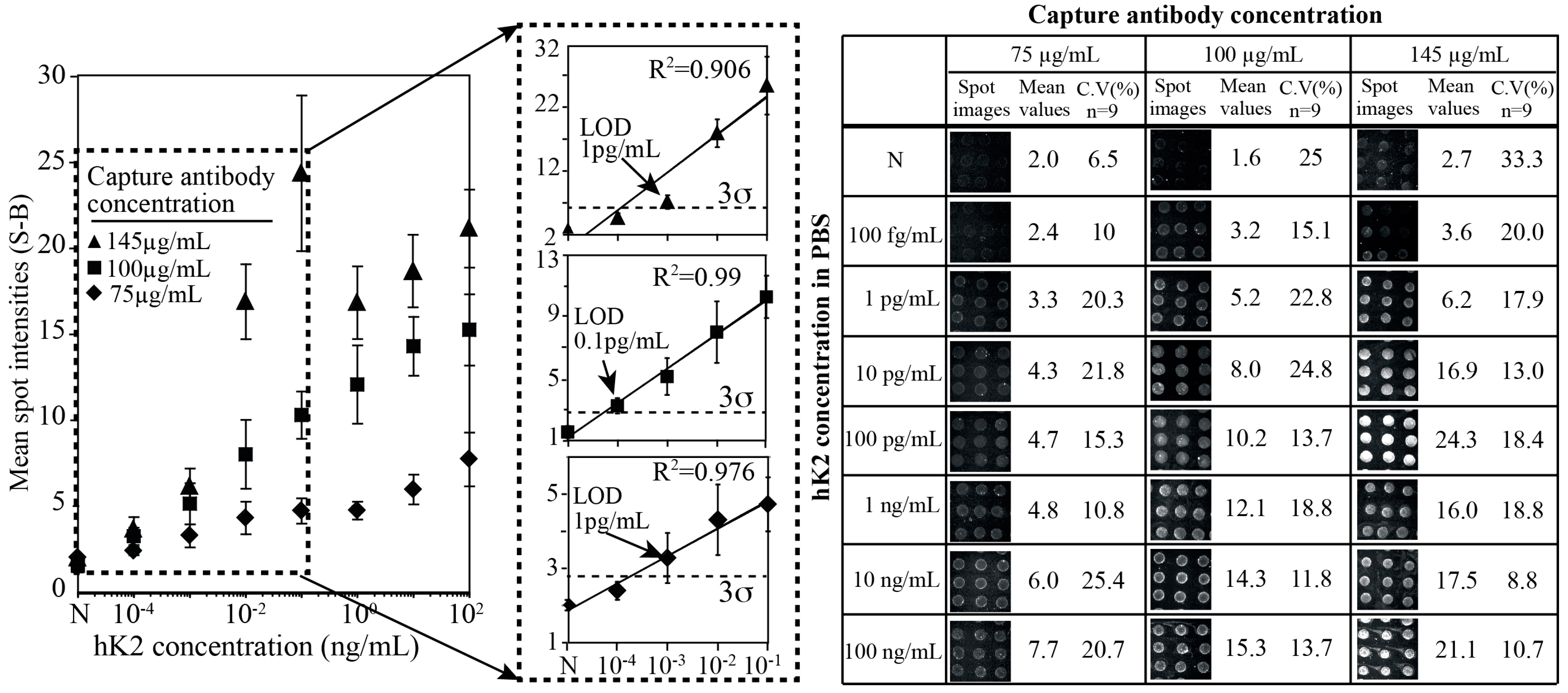
3.2. hK2 Assay Performance against Density of Capture Antibody

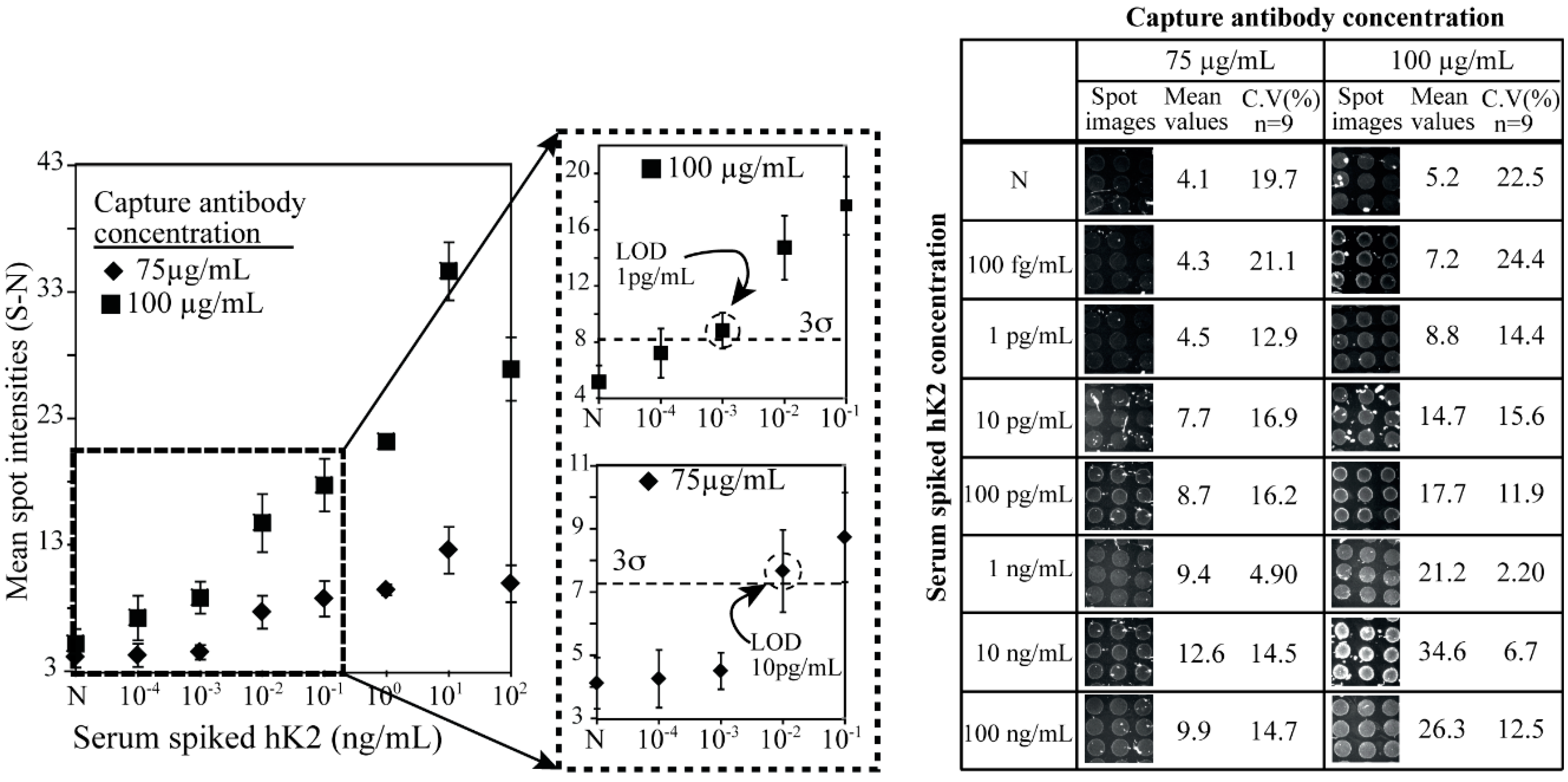
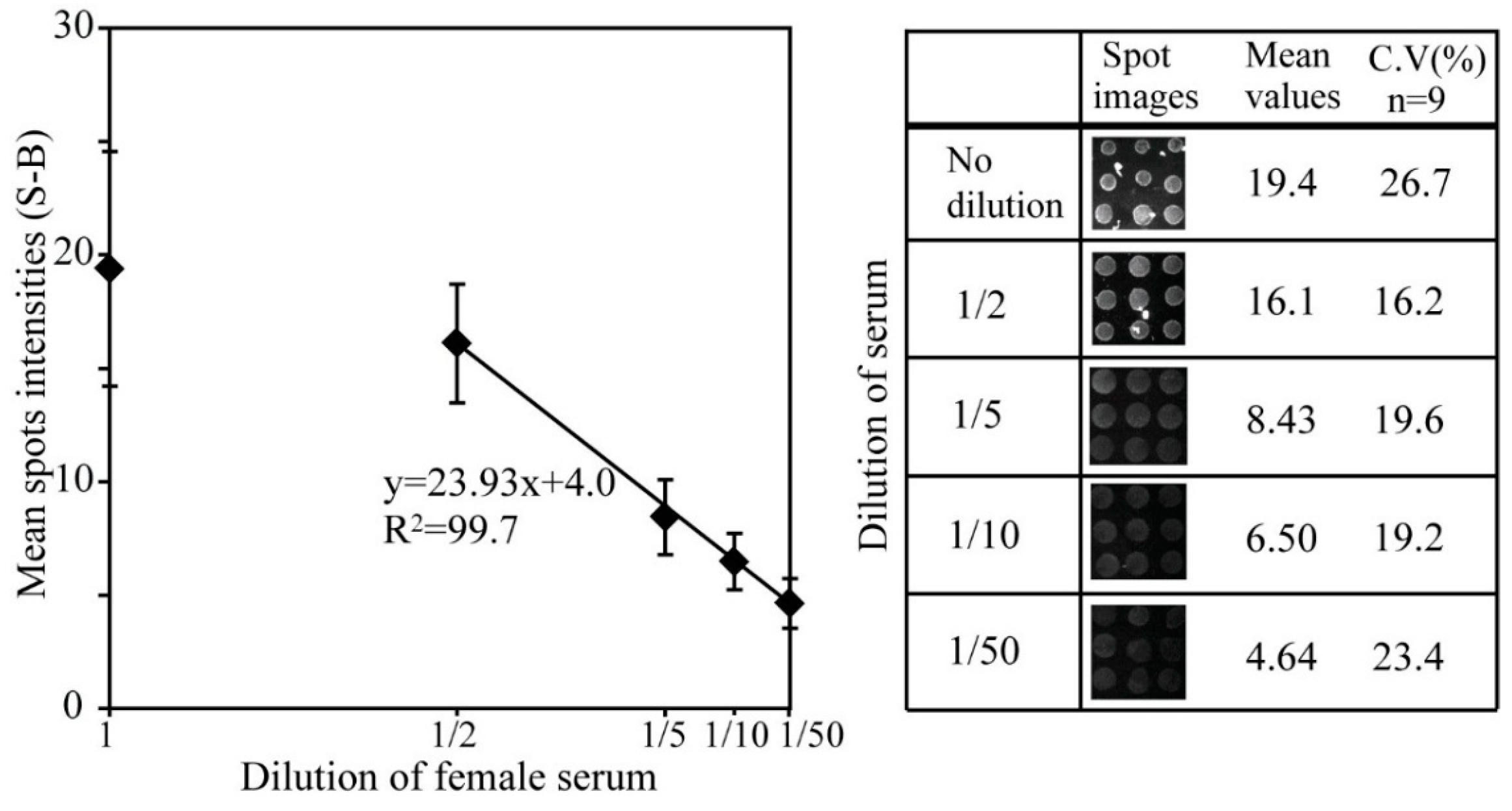
3.3. hK2 Immunoassay in Female Human Serum


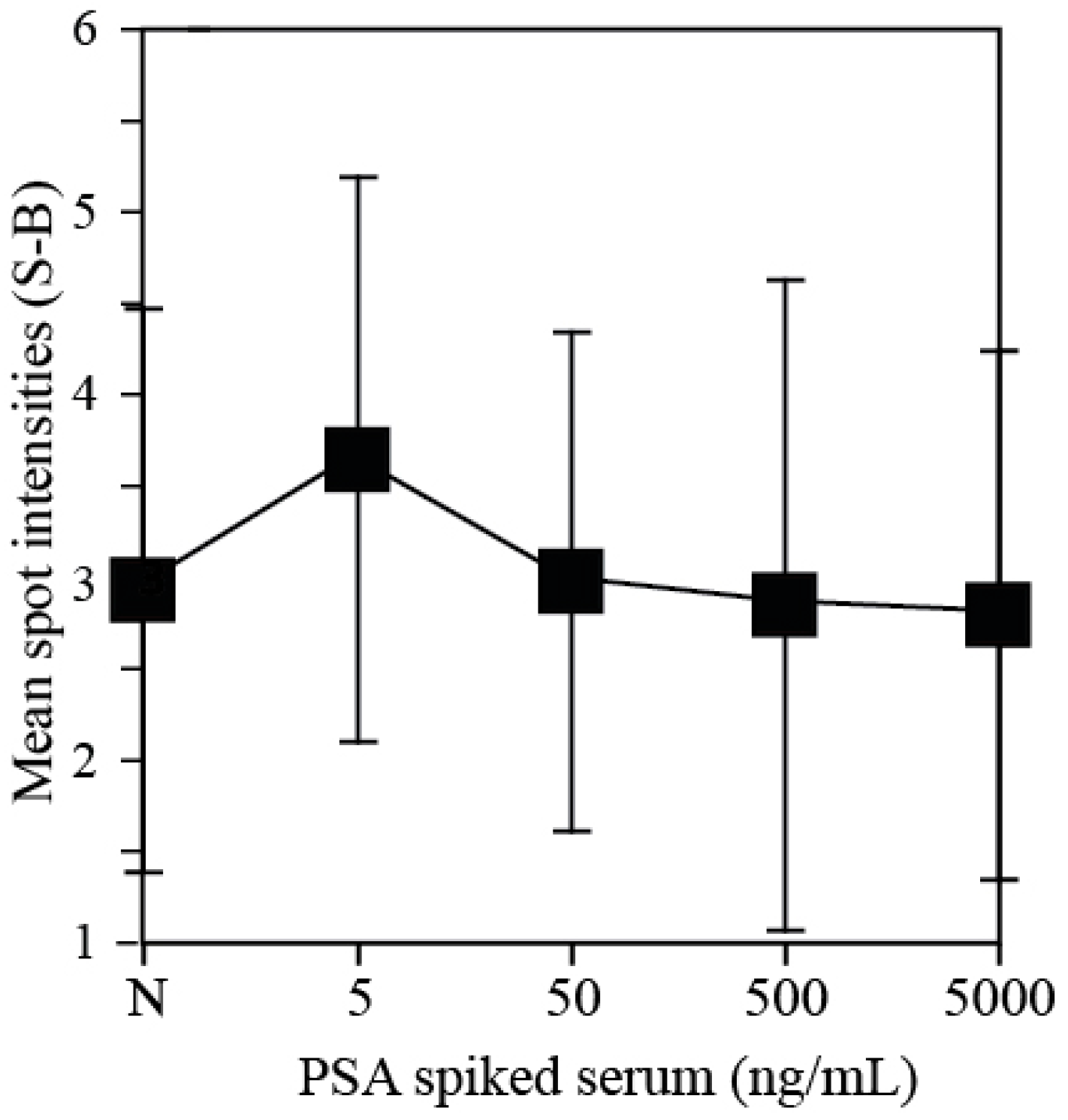
3.4. Cross Reaction of hK2 Antibody against PSA

4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Emami, N.; Diamond, E. Utility of kallikrein-related peptidases (KLKs) as cancer biomarkers. Clin. Chem. 2008, 54, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Carlo, B.; Diamond, E.P. The emerging roles of human tissue kallikreins in cancer. Nat. Rev. Cancer 2004, 4, 876–890. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J.; Ulmert, D.; Serio, A.M.; Bjork, T.; Scardino, P.T.; Eastham, J.A.; Berglund, G.; Lilja, H. The predictive value of prostate cancer biomarkers depends on age and time to diagnosis: Towards a biologically-based screening strategy. Int. J. Cancer 2007, 121, 2212–2217. [Google Scholar] [CrossRef] [PubMed]
- Diamonds, E.F.; Yousef, G.M. Human tissue kallikreins: A family of new cancer biomarkers. Clin. Chem. 2002, 48, 1198–1205. [Google Scholar] [PubMed]
- Vickers, A.; Cronin, A.; Roobol, M.; Savage, C.; Peltola, M.; Pettersson, K.; Scardino, P.T.; Schroder, F.; Lilja, H. Reducing unnecessary biopsy during prostate cancer screening using a four-kallikrein panel: An independent replication. J. Clin. Oncol. 2010, 28, 2493–2498. [Google Scholar] [CrossRef] [PubMed]
- Presner, J.; Rubin, M.; Wei, J.; Chinnaiyan, A. beyond PSA: The next generation of prostate cancer biomarkers. Sci. Transl. Med. 2012, 28, 127rv3. [Google Scholar]
- Avgeris, M.; Mavridis, K.; Scorilas, A. Kallikrein-related peptidase genes as promising biomarkers for prognosis and monitoring of human malignancies. Biol. Chem. 2010, 391, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Kurlender, L.; Yousef, G.M.; Memari, N.; Robb, J.D.; Michael, I.P.; Borgoño, C.; Katsaros, D.; Stephan, C.; Jung, K.; Diamandis, E.P. Differential expression of a human kallikrein 5 (KLK5) splice variant in ovarian and prostate cancer. Tumor Biol. 2004, 25, 149–156. [Google Scholar] [CrossRef]
- Recker, F.; Maciej, F.R.; Kwiatkowski, K.; Piironen, T.; Pettersson, K.; Lümmen, G.; Wernli, M.; Wiefelspütz, J.; Graber, S.F.; Goepel, M.; et al. The importance of human glandular kallikrein and its correlation with different prostate specific antigen serum forms in the detection of prostate carcinoma. Cancer 1998, 83, 2540–2547. [Google Scholar] [CrossRef] [PubMed]
- Vaisanen, V.; Eriksson, S.; Ivaska, K.K.; Lilja, H.; Nurmi, M.; Pettersson, K. Development of sensitive immunoassays for free and total human glandular kallikrein 2. Clin. Chem. 2004, 50, 1607–1617. [Google Scholar] [CrossRef] [PubMed]
- Darson, M.F.; Pacelli, A.; Roche, P.; Rittenhouse, H.G.; Wolfert, R.L.; Young, C.F.; Klee, G.G.; Tindall, D.J.; Bostwick, D.G. Human glandular kallikrein 2 (hK2) expression in prostatic intraepithelial neoplasia and adenocarcinoma: A novel prostate cancer marker. Urology 1997, 49, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.; Piironen, T.; Pettersson, K.; Bjork, T.; Wojno, K.J.; Oesterling, J.E.; Lilja, H. Discrimination of men with prostate cancer from those with benign disease by measurement of human glandular kallikrein 2 (hK2) in serum. J. Urol. 2000, 163, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Lintula, S.; Stenman, J.; Bjartell, A.; Nordling, S.; Stenman, U. Relative concentrations of hK2/PSA mRNA in benign and malignant prostatic tissue. Prostate 2005, 63, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Sutkowski, D.M.; Goode, R.L.; Baniel, J.; Teater, C.; Cohen, P.; McNulty, A.M.; Hsiung, H.M.; Becker, G.W.; Neubauer, B.L. Growth Regulation of Prostatic Stromal Cells by Prostate-Specific Antigen. J. Natl. Cancer Inst. 1999, 91, 1663–1669. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, M.K.; Recker, F.; Piironen, T.; Pettersson, K.; Otto, T.; Wernli, M.; Tscholl, R. In prostatism patients the ratio of human glandular kallikrein to free PSA improves the discrimination between prostate cancer and benign hyperplasia within the diagnostic “gray zone” of total PSA 4 to 10 ng/mL. Urology 1998, 52, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Recker, F.; Kwiatkowski, M.K.; Piironen, T.; Pettersson, K.; Huber, A.; Lümmen, G.; Tscholl, R. Human glandular kallikrein as a tool to improve discrimination of poorly differentiated and non-organ-confined prostate cancer compared with prostate-specific antigen. Urology 2000, 55, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Haese, A.; Graefen, M.; Steuber, T.; Becker, C.; Pettersson, K.; Piironen, T.; Noldus, J.; Huland, H.; Lilja, H. Human glandular kallikrein 2 levels in serum for discrimination of pathologically organ-confined from locally-advanced prostate cancer in total PSA-levels below 10 ng/mL. Prostate 2001, 49, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Henttu, P.; Lukkarinen, O.; Vihko, P. Expression of the gene coding for human prostate-specific antigen and related hGK-1 in benign and malignant tumors of the human prostate. Int. J. Cancer 1990, 45, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Van Gils, M.; Stenman, U.H.; Schalken, J.A.; Schröder, F.H.; Luider, T.M.; Lilja, H.; Bjartell, A.; Hamdy, F.C.; Pettersson, K.S.I.; Bischoff, R.; et al. Innovations in serum and urine markers in prostate cancer current European Research in the P-Mark project. Eur. Urol. 2005, 48, 1031–1041. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Huang, X.; Wang, Z.; Jin, A.; Sun, X.; Zhu, L.; Wang, F.; Ma, Y.; Niu, G.; Walker, A.; Chen, X. Gold Nanoparticle-based activatable probe for sensing ultralow levels of prostate-specific antigen. ACS Nano 2013, 7, 5568–5576. [Google Scholar] [CrossRef] [PubMed]
- Thaxton, C.; Elghanian, R.; Thomas, A.; Stoeva, S.; Lee, J.; Smith, N.; Schaeffer, A.; Klocker, H.; Horninger, W.; Bartsch, G.; Mirkin, C. Nanoparticle-based bio-barcode assay redefines “undetectable” PSA and biochemical recurrence after radical prostatectomy. Proc. Nalt. Acad. Sci. USA 2009, 106, 18437–18442. [Google Scholar] [CrossRef]
- Kim, S.H.; Iwai, S.; Araki, S.; Sakakihara, S.; Iino, R.; Noji, H. Large-scale femtoliter droplet array for digital counting of single biomolecules. Lab Chip 2012, 12, 4986–4991. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.; Hanlon, D.; Provuncher, G.; Chang, L.; Song, L.; Patel, P.; Ferrell, E.; Lepor, H.; Partin, A.; Chan, D.; et al. D. Fifth-generation digital immunoassay for prostate-specific antigen by single molecule array technology. Clin. Chem. 2011, 57, 1712–1721. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Kim, S.; Malm, J.; Jeong, O.C.; Lilja, H.; Laurell, T. Improved porous silicon microarray based prostate specific antigen immunoassay by optimized surface density of the capture antibody. Anal. Chim. Acta 2013, 796, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Stephan, C.; Jung, K.; Nakamura, T.; Yousef, G.M.; Kristiansen, G.; Diamond, E.P. Serum human glandular kallikrein 2 (hK2) for distinguishing stage and grade of prostate cancer. Int. J. Urol. 2006, 13, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Jane, A.; Dronov, R.; Hodges, A.; Voelcker, N.H. Porous silicon biosensors on the advance. Trends Biotechnol. 2009, 4, 230–239. [Google Scholar] [CrossRef]
- Shtenberg, G.; Massad-Ivanir, N.; Moscovitz, O.; Engin, S.; Sharon, M.; Fruk, L.; Segal, E. Picking up the pieces: A generic porous Si biosensor for probing the proteolytic products of enzymes. Anal. Chem. 2013, 83, 1951–1956. [Google Scholar] [CrossRef]
- Finnskog, D.; Ressine, A.; Laurell, T.; Marko-Varga, G. Integrated protein microchip assay with dual fluorescent-, and MALDI read-out. J. Prot. Res. 2004, 3, 988–994. [Google Scholar] [CrossRef]
- Arwin, H.; Gavutis, M.; Gustafsson, J.; Schultzberg, M.; Zangooie, S.; Tengvall, P. Protein adsorption in thin porous silicon layers. Phys. Status Solidi (a) 2000, 182, 515–520. [Google Scholar] [CrossRef]
- Drott, J.; Rosengren, L.; Lindström, K.; Laurell, T. Pore morphology influence on catalytic turn-over for enzyme activated porous silicon matrices. Thin Solid Films 1998, 330, 161–166. [Google Scholar] [CrossRef]
- Hosokawa, K.; Omata, M.; Maeda, M. Immunoassay on a power-free microchip with laminar flow-assisted dendritic amplification. Anal. Chem. 2007, 79, 6000–6004. [Google Scholar] [CrossRef] [PubMed]
- Rapkiewicz, A.; Espina, V.; Zujewski, J.A.; Lebowitz, P.F.; Filie, A.; Wulfkuhle, J.; Camphausen, K.; Petricoin, E.F.; Liotta, L.A.; Abati, A. The needle in the haystack: Application of breast fine-needle aspirate samples to quantitative protein microarray technology. Cancer Cytopathol. 2007, 111, 173–184. [Google Scholar] [CrossRef]
- Nishizuka, S.; Charboneau, L.; Young, L.; Major, S.; Reinhold, W.C.; Waltham, M.; Kouros-Mehr, H.; Bussey, K.J.; Lee, J.K.; Espina, V.; et al. Proteomic profiling of the NCI-60 cancer cell lines using new high-density reverse-phase lysate microarrays. Proc. Nalt. Acad. Sci. USA 2003, 100, 14229–14234. [Google Scholar] [CrossRef]
- Schweitzer, B.; Wiltshire, S.; Lambert, J.; O’Malley, S.; Kukanskis, K.; Zhu, Z.; Kingsmore, S.F.; Lizardi, P.M.; Ward, D.C. Immunoassays with rolling circle DNA amplification: A versatile platform for ultrasensitive antigen detection. Proc. Nalt. Acad. Sci. USA 2000, 97, 10113–10119. [Google Scholar] [CrossRef]
- Lee, S.W.; Silajdžić, E.; Kim, S.; Hansson, O.; Björkqvist, M.; Laurell, T. A porous silicon immunoassay platform for fluorometric determination of α-synuclein in human cerebrospinal fluid. Microchimica. Acta 2014, 181, 1143–1149. [Google Scholar] [CrossRef]
- Finnskog, D.; Järås, K.; Ressine, A.; Malm, J.; Marko-Varga, G.; Lilja, H.; Laurell, T. High-speed biomarker identification utilizing porous silicon nanovial arrays and MALDI-TOF mass spectrometry. Electrophoresis 2006, 27, 1093–1103. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, B.; Roberts, S.; Grimwade, B.; Shao, W.; Wang, M.; Fu, Q. Multiplexed protein profiling on microarrays by rolling-circle amplification. Nat. Biotechnol. 2002, 20, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Michaud, G.A.; Salcius, M.; Zhou, F.; Bangham, R.; Bonin, J.; Guo, H.; Snyder, M.; Predki, P.F.; Schweitzer, B.I. Analyzing antibody specificity with whole proteome microarrays. Nat. Biotechnol. 2003, 21, 1509–1512. [Google Scholar] [CrossRef] [PubMed]
- Ptacek, J.; Devgan, G.; Michaud, G.; Zhu, H.; Zhu, X.; Fasolo, J.; Guo, H.; Jona, G.; Breitkreutz, A.; Sopko, R.; et al. Global analysis of protein phosphorylation in yeast. Nature 2005, 438, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, V.; Leethanakul, C.; Bichsel, V.E.; Worth, J.M.; Prabhu, V.; Gutkind, J.S.; Liotta, L.A.; Munson, P.J.; Petricoin, E.F.; Krizman, D. Proteomic profiling of the cancer microenvironment by antibody arrays. Proteomics 2001, 1, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Tannapfel, A.; Anhalt, K.; Häusermann, P.; Sommerer, F.; Benicke, M.; Uhlmann, D.; Witzigmann, H.; Hauss, J.; Wittekind, C. Identification of novel proteins associated with hepatocellular carcinomas using protein microarrays. J. Pathol. 2003, 201, 238–249. [Google Scholar] [CrossRef] [PubMed]
- Ekins, R.P. Multi-analyte immunoassay. J. Pham Biomed. Anal. 1989, 7, 155–168. [Google Scholar] [CrossRef]
- Pollard, H.B.; Srivastava, M.; Eidelman, O.; Jozwik, C.; Rothwell, S.W.; Mueller, G.P.; Jacobowitz, D.M.; Darling, T.; Guggino, W.B.; Wright, J.; et al. Protein microarray platforms for clinical proteomics. Proteomics Clin. Appl. 2007, 1, 934–952. [Google Scholar] [CrossRef] [PubMed]
- Seidel, M.; Niessner, R. Automated analytical microarrays: A critical review. Anal. Bioanal. Chem. 2008, 391, 1521–1544. [Google Scholar] [CrossRef] [PubMed]
- Sebastiani, V.; Botti, C.; di Tondo, U.; Visca, P.; Pizzuti, L.; Santeusanio, G.; Alo, P.L. Tissue Microarray Analysis of FAS, Bcl-2, Bcl-x, ER, PgR, Hsp60, p53 and Her2-neu in Breast Carcinoma. Anticancer Res. 2006, 26, 2983–2387. [Google Scholar] [PubMed]
- Gembitsky, D.S.; Lawlor, K.; Jacovina, A.; Yaneva, M.; Tempst, P. A prototype antibody microarray platform to monitor changes in protein tyrosine phosphorylation. Mol. Cell. Proteomics 2004, 3, 1102–1118. [Google Scholar] [CrossRef] [PubMed]
- Saviranta, P.; Okon, R.; Brinker, A.; Warashina, M.; Eppinger, J.; Geierstanger, B.H. Evaluating sandwich immunoassays in microarray format in terms of the ambient analyte regime. Clin. Chem. 2004, 50, 1907–1920. [Google Scholar] [CrossRef] [PubMed]
- Foll, H.; Christophersen, M.; Carstensen, J.; Hasse, G. Formation and application of porous silicon. Sci. Eng. R 2002, 39, 93–141. [Google Scholar] [CrossRef]
- Steuber, T.; Vickers, A.; Haese, A.; Becker, C.; Pettersson, K.; Chun, F.; Kattan, M.; Eastham, J.; Scardino, P.; Huland, K.; et al. Risk assessment for biochemical recurrence prior to radical prostatectomy: Significant enhancement contributed by human glandular kallikrein 2 (hK2) and free prostate specific antigen (PSA) in men with moderate PSA-elevation in serum. Int. J. Cancer 2006, 118, 1234–1240. [Google Scholar] [CrossRef] [PubMed]
- Briganti, A. Role of hK2 in prediction clinically insignificant prostate cancer. Eur. Urol. 2007, 52, 1297–1299. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.W.; Hosokawa, K.; Kim, S.; Jeong, O.C.; Lilja, H.; Laurell, T.; Maeda, M. A Highly Sensitive Porous Silicon (P-Si)-Based Human Kallikrein 2 (hK2) Immunoassay Platform toward Accurate Diagnosis of Prostate Cancer. Sensors 2015, 15, 11972-11987. https://doi.org/10.3390/s150511972
Lee SW, Hosokawa K, Kim S, Jeong OC, Lilja H, Laurell T, Maeda M. A Highly Sensitive Porous Silicon (P-Si)-Based Human Kallikrein 2 (hK2) Immunoassay Platform toward Accurate Diagnosis of Prostate Cancer. Sensors. 2015; 15(5):11972-11987. https://doi.org/10.3390/s150511972
Chicago/Turabian StyleLee, Sang Wook, Kazuo Hosokawa, Soyoun Kim, Ok Chan Jeong, Hans Lilja, Thomas Laurell, and Mizuo Maeda. 2015. "A Highly Sensitive Porous Silicon (P-Si)-Based Human Kallikrein 2 (hK2) Immunoassay Platform toward Accurate Diagnosis of Prostate Cancer" Sensors 15, no. 5: 11972-11987. https://doi.org/10.3390/s150511972