Measuring Gait Quality in Parkinson’s Disease through Real-Time Gait Phase Recognition

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
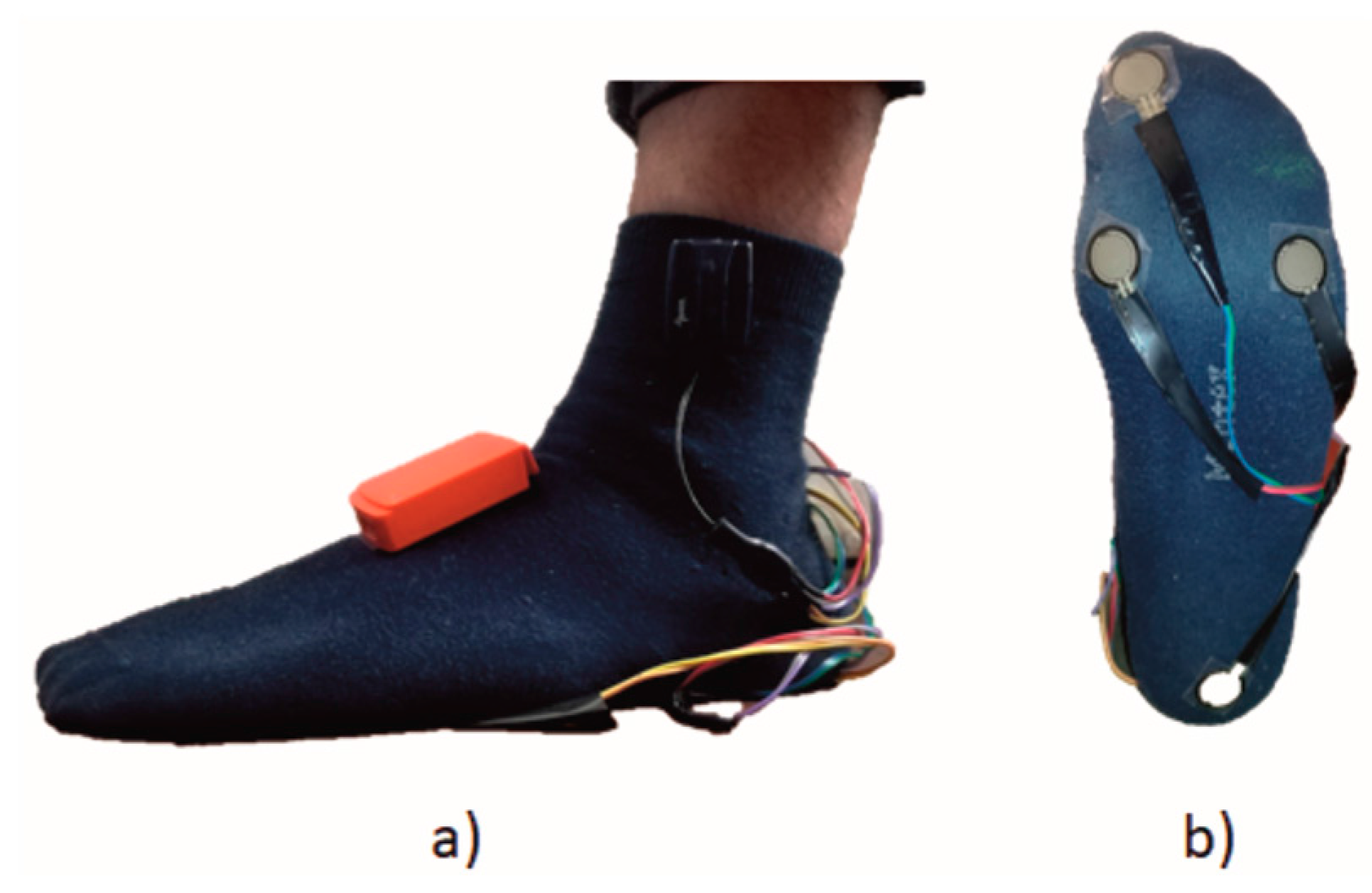
2.2. Experimental Setup
2.3. Experimental Procedure
2.4. Data Processing and Tested Methods
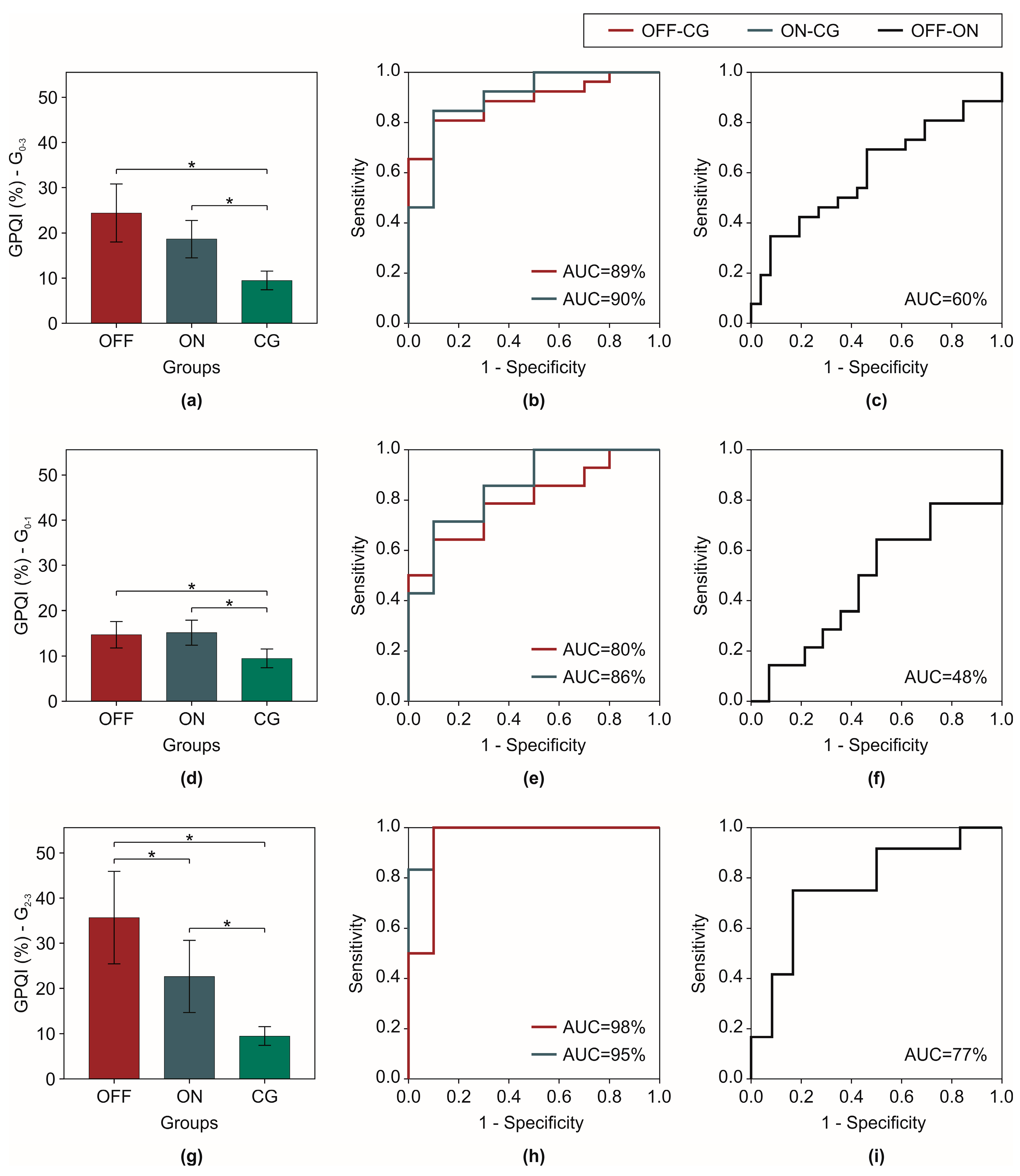
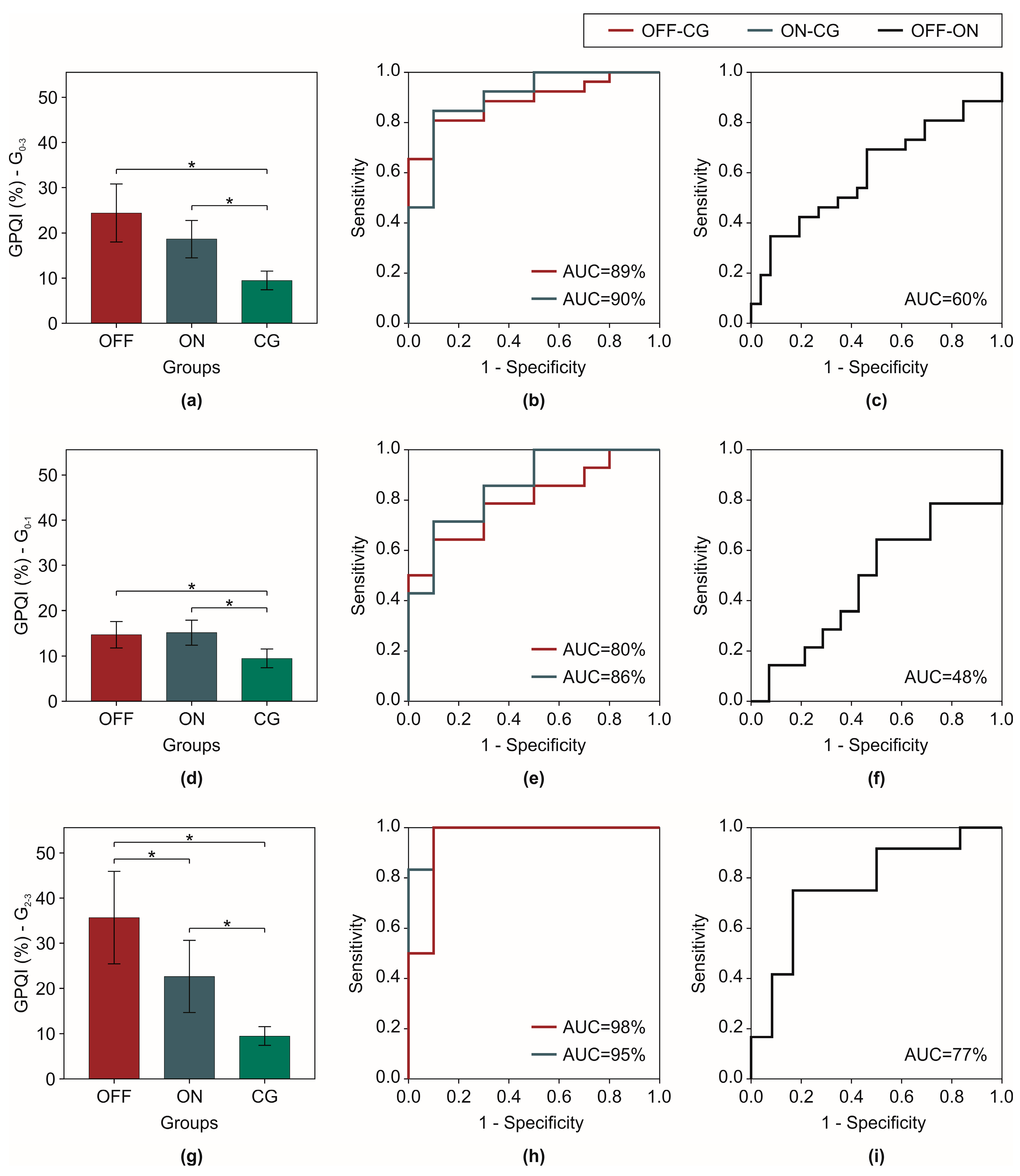
2.5. Gait Phases Quality Index
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. Technical Validity of Gait Partitioning Methods
4.2. Clinical Validity of GPQI
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Taborri, J.; Palermo, E.; Rossi, S.; Cappa, P. Gait Partitioning Methods: A Systematic Review. Sensors 2016, 16, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hegde, N.; Bries, M.; Sazonov, E. A Comparative Review of Footwear-Based Wearable Systems. Electronics 2016, 5, 48. [Google Scholar] [CrossRef]
- Salarian, A.; Russmann, H.; Vingerhoets, F.J.G.; Dehollain, C.; Blanc, Y.; Burkhard, P.R.; Aminian, K. Gait assessment in Parkinson’s disease: Toward an ambulatory system for long-term monitoring. IEEE Trans. Biomed. Eng. 2004, 51, 1434–1443. [Google Scholar] [CrossRef] [PubMed]
- Mileti, I.; Taborri, J.; Rossi, S.; Petrarca, M.; Patane, F.; Cappa, P. Evaluation of the effects on stride-to-stride variability and gait asymmetry in children with Cerebral Palsy wearing the WAKE-up ankle module. In Proceedings of the 2016 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Benevento, Italy, 15–18 May 2016; pp. 1–6. [Google Scholar] [CrossRef]
- Hundza, S.; Hook, W.; Harris, C.; Mahajan, S.; Leslie, P.; Spani, C.; Spalteholz, L.; Birch, B.; Commandeur, D.; Livingston, N. Accurate and Reliable Gait Cycle Detection in Parkinson’s Disease. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 22, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Lorincz, K.; Hughes, R.; Huggins, N.; Growdon, J.; Standaert, D.; Akay, M.; Dy, J.; Welsh, M.; Bonato, P. Monitoring motor fluctuations in patients with Parkinson’s disease using wearable sensors. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 864–873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kestenbaum, M.; Fahn, S. Safety of IPX066, an extended release carbidopa-levodopa formulation, for the treatment of Parkinson’s disease. Expert Opin. Drug Saf. 2015, 14, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Zesiewicz, T.A.; Sullivan, K.L.; Hauser, R.A. Levodopa-induced dyskinesia in Parkinson’s disease: Epidemiology, etiology, and treatment. Curr. Neurol. Neurosci. Rep. 2007, 7, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Thanvi, B.; Lo, N.; Robinson, T. Levodopa-induced dyskinesia in Parkinson’s disease: Clinical features, pathogenesis, prevention and treatment. Postgrad. Med. J. 2007, 83, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Movement Disorder Society Task Force on Rating Scales for Parkinson’s Movement Disorder Society Task Force on Rating Scales for Parkinson’s Disease. The Unified Parkinson’s Disease Rating Scale (UPDRS): Status and recommendations. Mov. Disord. 2003, 18, 738–750. [Google Scholar] [CrossRef]
- Haji Ghassemi, N.; Hannink, J.; Martindale, C.; Gaßner, H.; Müller, M.; Klucken, J.; Eskofier, B. Segmentation of Gait Sequences in Sensor-Based Movement Analysis: A Comparison of Methods in Parkinson’s Disease. Sensors 2018, 18, 145. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Lowenthal, J.; Herman, T.; Gruendlinger, L.; Peretz, C.; Giladi, N. Rhythmic auditory stimulation modulates gait variability in Parkinson’s disease. Eur. J. Neurosci. 2007, 26, 2369–2375. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Plotnik, M.; Giladi, N.; Balash, Y.; Peretz, C.; Hausdorff, J.M. Is freezing of gait in Parkinson’s disease related to asymmetric motor function? Ann. Neurol. 2005, 57, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Mariani, B.; Rouhani, H.; Crevoisier, X.; Aminian, K. Quantitative estimation of foot-flat and stance phase of gait using foot-worn inertial sensors. Gait Posture 2013, 37, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.S.; Wertsch, J.J.; Harris, G.F.; Loftsgaarden, J.D.; Price, M.B. Foot pressure distribution during walking and shuffling. Arch. Phys. Med. Rehabil. 1991, 72, 390–397. [Google Scholar] [PubMed]
- Pacilli, A.; Mileti, I.; Germanotta, M.; Di Sipio, E.; Imbimbo, I.; Aprile, I.; Padua, L.; Rossi, S.; Palermo, E.; Cappa, P. A wearable setup for auditory cued gait analysis in patients with Parkinson’s Disease. In Proceedings of the 2016 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Benevento, Italy, 15–18 May 2016; pp. 1–6. [Google Scholar] [CrossRef]
- Hughes, J.; Bowes, S.; Leeman, A.; O’Neill, C.; Deshmukh, A.; Nicholson, P.; Dobbs, S.; Dobbs, R. Parkinsonian abnormality of foot strike: A phenomenon of ageing and/or one responsive to levodopa therapy? Br. J. Clin. Pharmacol. 1990, 29, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Nieuwboer, A.; De Weerdt, W.; Peeraer, L.; Lesaffre, E.; Hilde, F.; Baunach, B. Plantar force distribution in Parkinsonian gait: A comparison between patients and age-matched control subjects. Scand. J. Rehabil. Med. 1999, 31, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Koller, W.C.; Glatt, S.; Vetere-Overfield, B.; Hassanein, R. Falls and Parkinson’s disease. Clin. Neuropharmacol. 1989, 12, 98–105. [Google Scholar] [PubMed]
- Rueterbories, J.; Spaich, E.G.; Andersen, O.K. Gait event detection for use in FES rehabilitation by radial and tangential foot accelerations. Med. Eng. Phys. 2014, 36, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Mannini, A.; Sabatini, A.M. Gait phase detection and discrimination between walking–jogging activities using hidden Markov models applied to foot motion data from a gyroscope. Gait Posture 2012, 36, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Taborri, J.; Scalona, E.; Palermo, E.; Rossi, S.; Cappa, P. Validation of inter-subject training for hidden markov models applied to gait phase detection in children with Cerebral Palsy. Sensors 2015, 15, 24514–24529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taborri, J.; Scalona, E.; Rossi, S.; Palermo, E.; Patanè, F.; Cappa, P. Real-time gait detection based on Hidden Markov Model: Is it possible to avoid training procedure? In Proceedings of the 2015 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Turin, Italy, 7–9 May 2015; pp. 141–144. [Google Scholar]
- Sabatini, A.M.; Martelloni, C.; Scapellato, S.; Cavallo, F. Assessment of walking features from foot inertial sensing. IEEE Trans. Biomed. Eng. 2005, 52, 486–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannini, A.; Trojaniello, D.; Della Croce, U.; Sabatini, A.M. Hidden Markov model-based strategy for gait segmentation using inertial sensors: Application to elderly, hemiparetic patients and Huntington’s disease patients. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; Volume 2015, pp. 5179–5182. [Google Scholar] [CrossRef]
- Taborri, J.; Rossi, S.; Palermo, E.; Patanè, F.; Cappa, P. A Novel HMM Distributed Classifier for the Detection of Gait Phases by Means of a Wearable Inertial Sensor Network. Sensors 2014, 16212–16234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galli, M.; Cimolin, V.; De Pandis, M.F.; Schwartz, M.H.; Albertini, G. Use of the Gait Deviation Index for the Evaluation of Patients With Parkinson’s Disease. J. Mot. Behav. 2012, 44, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Schutte, L.M.; Narayanan, U.; Stout, J.L.; Selber, P.; Gage, J.R.; Schwartz, M.H. An index for quantifying deviations from normal gait. Gait Posture 2000, 11, 25–31. [Google Scholar] [CrossRef]
- Malt, M.A.; Aarli, Å.; Bogen, B.; Fevang, J.M. Correlation between the Gait Deviation Index and gross motor function (GMFCS level) in children with cerebral palsy. J. Child. Orthop. 2016, 10, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.; McGinley, J.L.; Schwartz, M.H.; Beynon, S.; Rozumalski, A.; Graham, H.K.; Tirosh, O. The Gait Profile Score and Movement Analysis Profile. Gait Posture 2009, 30, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Gouelle, A.; Mégrot, F.; Presedo, A.; Husson, I.; Yelnik, A.; Penneçot, G.-F. The Gait Variability Index: A new way to quantify fluctuation magnitude of spatiotemporal parameters during gait. Gait Posture 2013, 38, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, C.K.; Clark, D.J.; Gouelle, A. Validity of the Gait Variability Index in older adults: Effect of aging and mobility impairments. Gait Posture 2015, 41, 941–946. [Google Scholar] [CrossRef] [PubMed]
- Rennie, L.; Dietrichs, E.; Moe-Nilssen, R.; Opheim, A.; Franzén, E. The validity of the Gait Variability Index for individuals with mild to moderate Parkinson’s disease. Gait Posture 2017, 54, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Gelb, D.J.; Oliver, E.; Gilman, S. Diagnostic criteria for Parkinson disease. Arch. Neurol. 1999, 56, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Tests, D. Basic Principles of ROC Analysis. Semin. Nucl. Med. 1978, 8, 283–298. [Google Scholar]
- Dancey, C.P.; Reidy, J. Statistics without Maths for Psychology: Using SPSS for Windows; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2007; ISBN 0132051605. [Google Scholar]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Di Fabio, R.P. Essentials of Rehabilitation Research: A Statistical Guide to Clinical Practice; F.A. Davis Co.: Philadelphia, PA, USA, 2013; ISBN 9780803625648. [Google Scholar]
- Mileti, I.; Germanotta, M.; Alcaro, S.; Pacilli, A.; Imbimbo, I.; Petracca, M.; Erra, C.; Di Sipio, E.; Aprile, I.; Rossi, S.; et al. Gait partitioning methods in Parkinson’s disease patients with motor fluctuations: A comparative analysis. In Proceedings of the 2017 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Rochester, MN, USA, 7–10 May 2017. [Google Scholar] [CrossRef]
- Motta, C.; Palermo, E.; Studer, V.; Germanotta, M.; Germani, G.; Centonze, D.; Cappa, P.; Rossi, S.; Rossi, S. Disability and Fatigue Can Be Objectively Measured in Multiple Sclerosis. PLoS ONE 2016, 11, e0148997. [Google Scholar] [CrossRef] [PubMed]
- Casamassima, F.; Ferrari, A.; Milosevic, B.; Ginis, P.; Farella, E.; Rocchi, L. A Wearable System for Gait Training in Subjects with Parkinson’s Disease. Sensors 2014, 14, 6229–6246. [Google Scholar] [CrossRef] [PubMed]
- Magrinelli, F.; Picelli, A.; Tocco, P.; Federico, A.; Roncari, L.; Smania, N.; Zanette, G.; Tamburin, S. Pathophysiology of Motor Dysfunction in Parkinson’s Disease as the Rationale for Drug Treatment and Rehabilitation. Park. Dis. 2016. [Google Scholar] [CrossRef] [PubMed]
- Medley, A.R.; Powell, T. Motivational Interviewing to promote self-awareness and engagement in rehabilitation following acquired brain injury: A conceptual review. Neuropsychol. Rehabil. 2010, 20, 481–508. [Google Scholar] [CrossRef] [PubMed]
- Thaut, M.H.; Abiru, M. Rhythmic Auditory Stimulation in Rehabilitation of Movement Disorders: A Review of Current Research. Music Percept. 2010, 27, 263–269. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Patients | Gender | Age | OFF State | ON State | ||
|---|---|---|---|---|---|---|
| UPDRS-III | GAIT | UPDRS-III | GAIT | |||
| 1 | M | 68 | 23 | 0 | 14 | 0 |
| 2 | M | 74 | 25 | 0 | 10 | 0 |
| 3 | F | 71 | 14 | 0 | 10 | 0 |
| 4 | M | 68 | 32 | 1 | 19 | 1 |
| 5 | M | 66 | 10 | 1 | 6 | 0 |
| 6 | F | 78 | 26 | 1 | 23 | 1 |
| 7 | F | 73 | 25 | 1 | 18 | 1 |
| 8 | F | 71 | 15 | 1 | 12 | 0 |
| 9 | M | 78 | 32 | 1 | 23 | 1 |
| 10 | M | 70 | 18 | 1 | 8 | 0 |
| 11 | M | 74 | 33 | 1 | 28 | 1 |
| 12 | F | 69 | 27 | 1 | 20 | 1 |
| 13 | M | 64 | 40 | 1 | 25 | 0 |
| 14 | F | 79 | 36 | 1 | 26 | 1 |
| 15 | M | 81 | 24 | 2 | 18 | 1 |
| 16 | M | 76 | 33 | 2 | 22 | 1 |
| 17 | F | 51 | 18 | 2 | 15 | 2 |
| 18 | M | 63 | 38 | 2 | 20 | 2 |
| 19 | M | 77 | 40 | 2 | 32 | 2 |
| 20 | M | 71 | 42 | 2 | 31 | 1 |
| 21 | M | 74 | 31 | 2 | 19 | 1 |
| 22 | M | 79 | 30 | 2 | 19 | 1 |
| 23 | F | 71 | 29 | 2 | 19 | 1 |
| 24 | F | 76 | 43 | 3 | 20 | 1 |
| 25 | M | 75 | 37 | 3 | 26 | 2 |
| 26 | M | 64 | 36 | 3 | 28 | 2 |
| Typology | Sensor | Signals | Filters | Method Description | |
|---|---|---|---|---|---|
| S-method [26] | Threshold | Single gyroscope | Sagittal angular velocity of foot | 2nd order low-pass Butterworth filter with 15 Hz cut off frequency | Absolute value of the reference signal is used for identifying gait events. Starting from FS, the HO/TS time instants occurred when the absolute value of angular velocity exceed/was less than 30°/s, respectively. TO was the maximum value of the angular velocity in the clockwise direction after HO. After mid-swing, HS was identified as the second maximum value of the angular velocity in the clockwise direction. |
| R-method [22] | Threshold | Single 3-axes accelerometer | Radial and tangential component of foot acceleration | 2nd order low-pass Butterworth filter with 6 Hz cut off frequency and two low pass moving average filters. | Gait events are identified by processing five reference signals: (i) the resultant acceleration filtered with the 2nd order low-pass Butterworth with 6 Hz cut off frequency (c50); (ii) its 1st and (iii) 2nd derivatives; and, the resultant acceleration filtered with low pass moving average filter with 1.25 s (iv) and 0.30 s (v) of window length (cA200 and cA50, respectively). The 1st and 2nd derivatives of resultant acceleration provide turning and inflection points needed to gait events identification. The two moving average filtered signals provide constraining ranges allowing the correct identification of turning and inflection points identification. |
| HMMsst [28] | Machine learning | Single gyroscope | Sagittal angular velocity of foot | 2nd order low-pass Butterworth filter with 17 Hz cut off frequency | This method processes the sagittal angular velocity of the foot, based on the scalar continuous Hidden Model Markov (cHMM). Gait phases are obtained as the likely sequence of the hidden states. The starting point is the training procedure involving the Baum-Welch algorithm and a set of model parameters: (i) the probability distribution matrix of the transition state, chosen as a left-right model; (ii) the initial state vector distribution, chosen giving the same probability for all phases, (iii) a vector of mixture coefficients, i.e., the weights used to estimate the sequence of states; and (iv) the mean and the standard deviation of the signal. This algorithm is trained with signals gathered from two trials of a patient in a specific pharmacological condition (OFF or ON), and tested with leaved out trial of the same patient. |
| HMMspt [24] | Machine learning | Single gyroscope | Sagittal angular velocity of foot | 2nd order low-pass Butterworth filter with 17 Hz cut off frequency | Similar to the previous method, a scalar continuous Hidden Model Markov is used to estimate gait sequence as the likely sequence. For patients with motor deficit, the training procedure involves mean and standard deviation of foot sagittal angular velocity of all trials of control group. Afterwards, foot sagittal angular velocity of all trials of patients is tested to estimate likely gait sequence. |
| OFF State | ON State | |||||||
|---|---|---|---|---|---|---|---|---|
| S-Method | R-Method | HMMsst | HMMspt | S-Method | R-Method | HMMsst | HMMspt | |
| TPR | 0.9 (0.1) | 0.8 (0.2) | 0.9 (0.1) | 0.9 (0.1) | 1.0 (0.1) | 0.8 (0.1) | 1.0 (0.1) | 0.9 (0.1) |
| TNR | 0.9 (0.0) | 0.7 (0.1) | 0.9 (0.1) | 0.9 (0.0) | 0.9 (0.1) | 0.7 (0.1) | 0.9 (0.1) | 0.9 (0.0) |
| G | 0.1 (0.1) | 0.4 (0.2) | 0.1 (0.1) | 0.1 (0.1) | 0.1 (0.1) | 0.4 (0.2) | 0.1 (0.1) | 0.1 (0.1) |
| OFF State | ON State | |||||||
|---|---|---|---|---|---|---|---|---|
| S-Method | R-Method | HMMsst | HMMspt | S-Method | R-Method | HMMsst | HMMspt | |
| LRe (%) | 0.7 (1.2) | 4.7 (4.2) | 2.5 (1.8) | 3.8 (2.0) | 0.5 (0.6) | 5.4 (5.1) | 2.6 (1.8) | 3.7 (2.0) |
| FFe (%) | 5.4 (3.5) | 10.4 (7.9) | 3.9 (3.0) | 2.8 (2.2) | 6.0 (4.3) | 11.7 (11.6) | 3.8 (2.8) | 3.0 (2.0) |
| PSe (%) | 5.9 (3.5) | 9.2 (5.6) | 3.2 (2.3) | 3.3 (3.9) | 6.2 (4.6) | 9.6 (6.2) | 3.5 (3.0) | 2.8 (2.9) |
| Swe (%) | 2.3 (2.6) | 8.0 (5.1) | 2.4 (1.8) | 1.6 (1.8) | 1.8 (1.7) | 9.1 (6.5) | 2.1 (1.4) | 1.1 (0.9) |
| GPQIe (%) | 4.7 (3.8) | 10.0 (12.0) | 3.2 (3.9) | 3.2 (2.3) | 5.6 (3.6) | 10.1 (13.1) | 3.7 (4.4) | 4.1 (4.1) |
| OFF State | ON State | |||
|---|---|---|---|---|
| UPDRS-III | GAIT | UPDRS-III | GAIT | |
| GPQI | p = 0.09 r = 0.33 | p < 0.01 * r = 0.60 | p = 0.17 r = 0.30 | p = 0.03 * r = 0.43 |
| OFF State | ON State | |||
|---|---|---|---|---|
| ICC3,k | MDC95% | ICC3,k | MDC95% | |
| G0–3 | 0.99 | 4.87 | 0.99 | 3.78 |
| G0–1 | 0.97 | 3.28 | 0.98 | 2.89 |
| G2–3 | 0.99 | 5.95 | 0.99 | 4.50 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mileti, I.; Germanotta, M.; Di Sipio, E.; Imbimbo, I.; Pacilli, A.; Erra, C.; Petracca, M.; Rossi, S.; Del Prete, Z.; Bentivoglio, A.R.; et al. Measuring Gait Quality in Parkinson’s Disease through Real-Time Gait Phase Recognition. Sensors 2018, 18, 919. https://doi.org/10.3390/s18030919
Mileti I, Germanotta M, Di Sipio E, Imbimbo I, Pacilli A, Erra C, Petracca M, Rossi S, Del Prete Z, Bentivoglio AR, et al. Measuring Gait Quality in Parkinson’s Disease through Real-Time Gait Phase Recognition. Sensors. 2018; 18(3):919. https://doi.org/10.3390/s18030919
Chicago/Turabian StyleMileti, Ilaria, Marco Germanotta, Enrica Di Sipio, Isabella Imbimbo, Alessandra Pacilli, Carmen Erra, Martina Petracca, Stefano Rossi, Zaccaria Del Prete, Anna Rita Bentivoglio, and et al. 2018. "Measuring Gait Quality in Parkinson’s Disease through Real-Time Gait Phase Recognition" Sensors 18, no. 3: 919. https://doi.org/10.3390/s18030919