Knowledge and Implementation of the New European Guide in the Management of Arterial Hypertension. The Cigema Survey

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Introduction
Results and Discussion
Sample size estimation
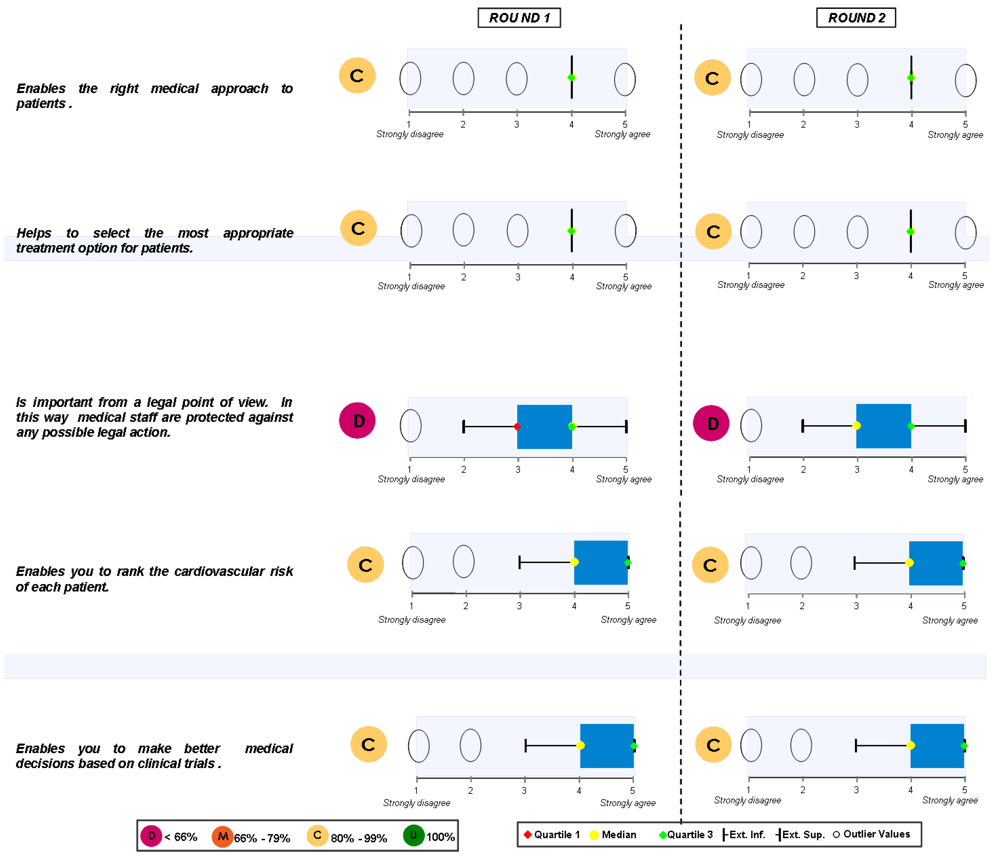
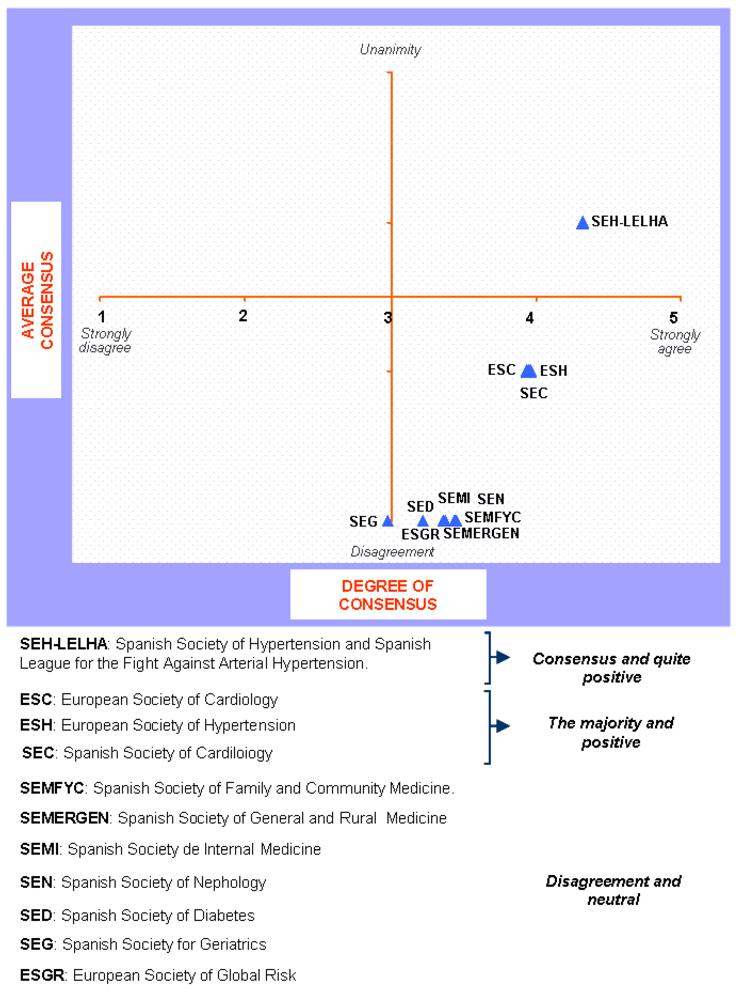
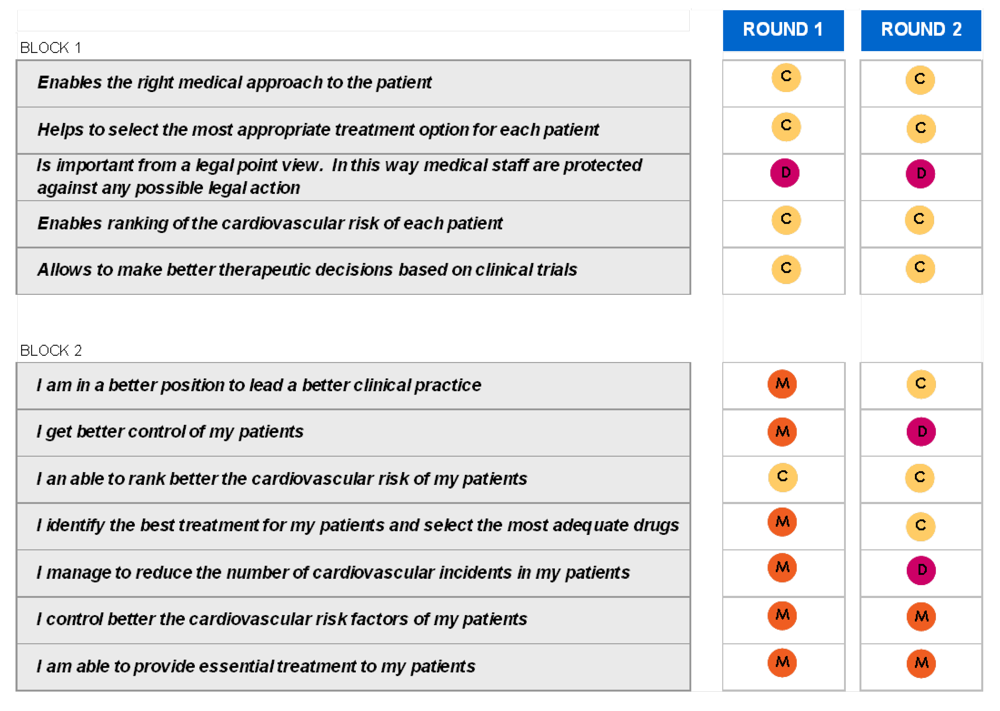
Block 1: Need for the guidelines


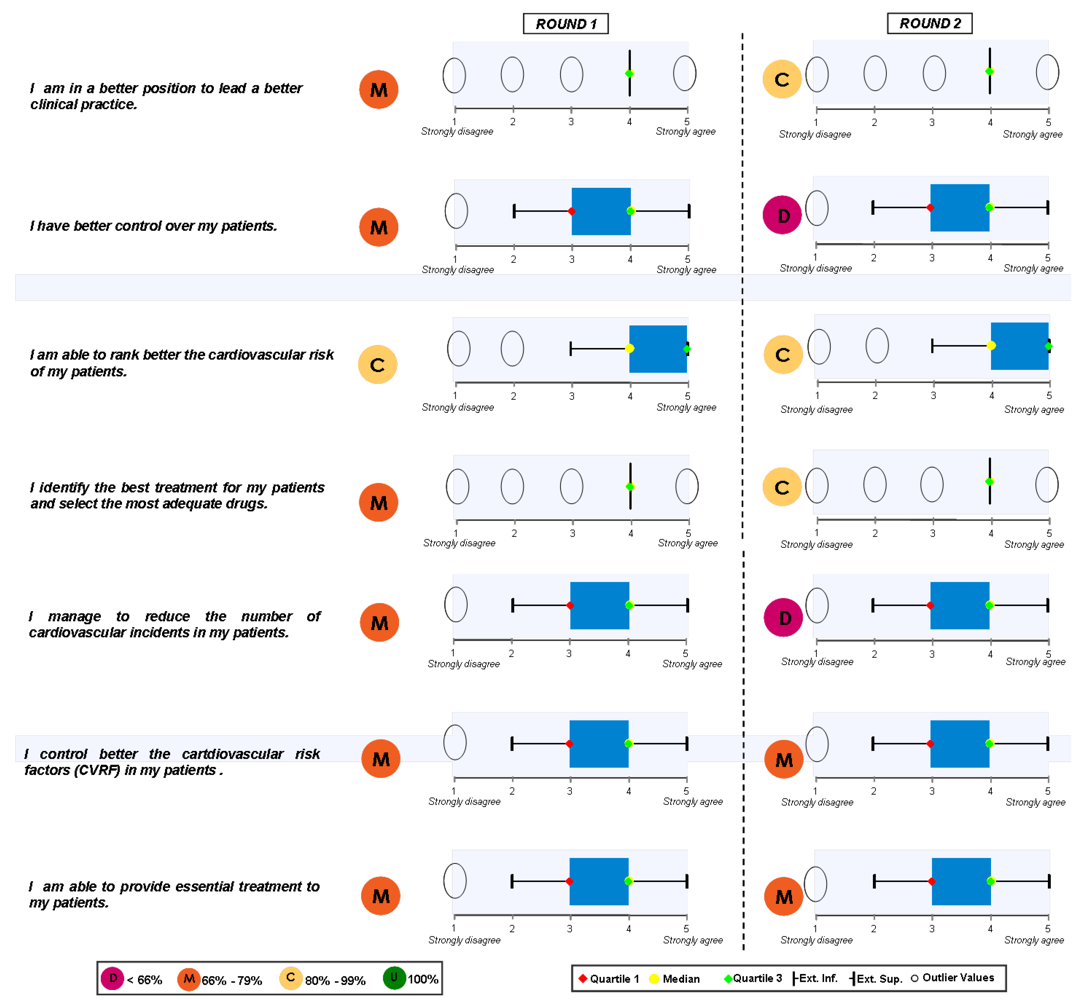
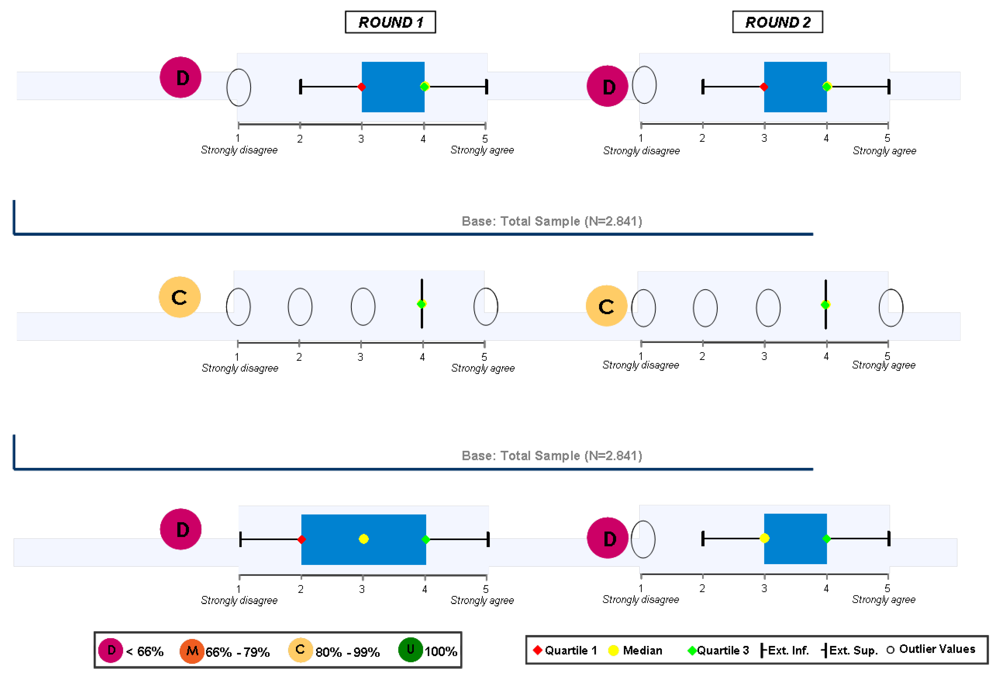
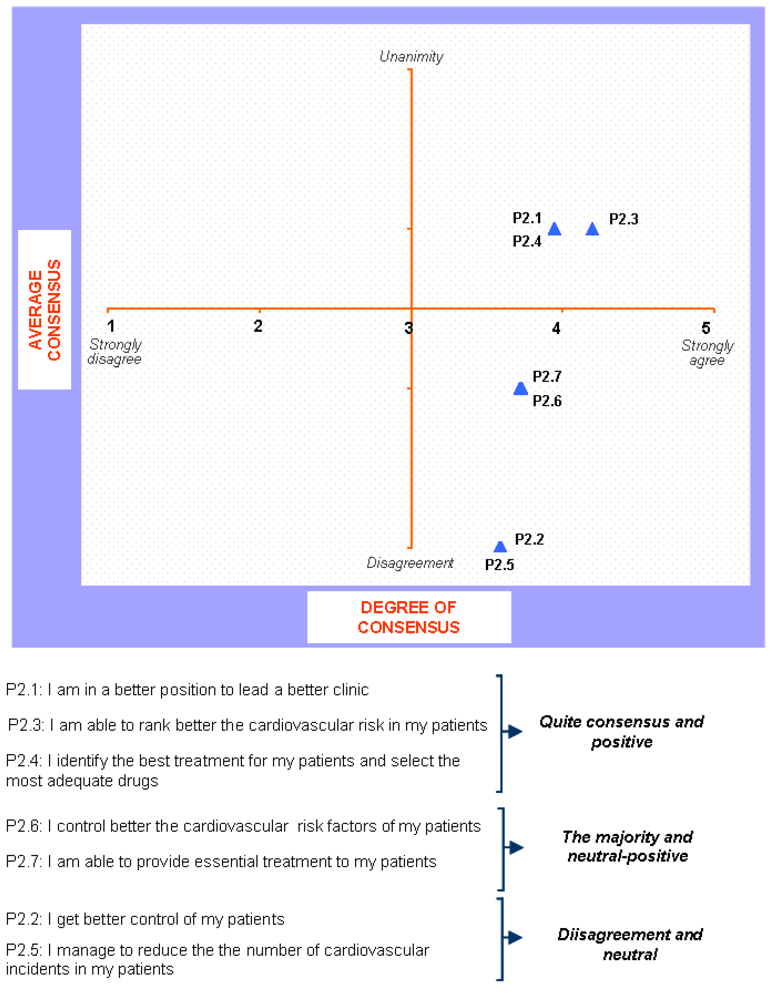
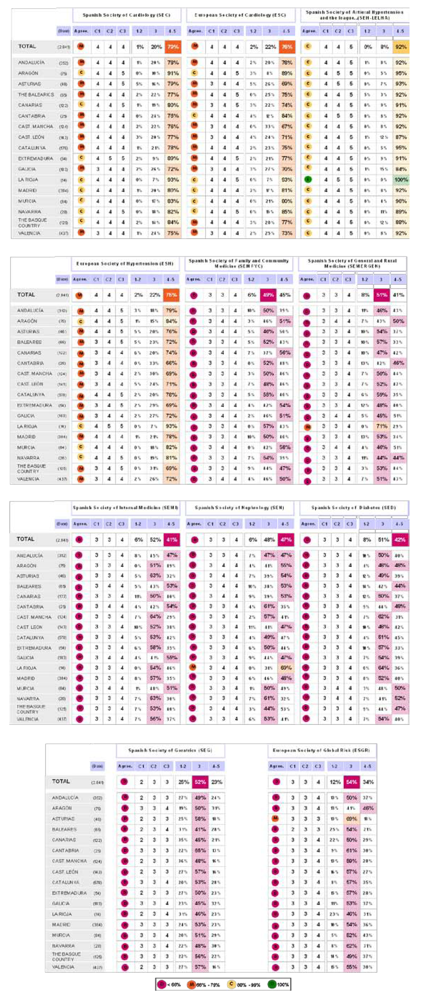
Block 2: Implementation of the Guidelines



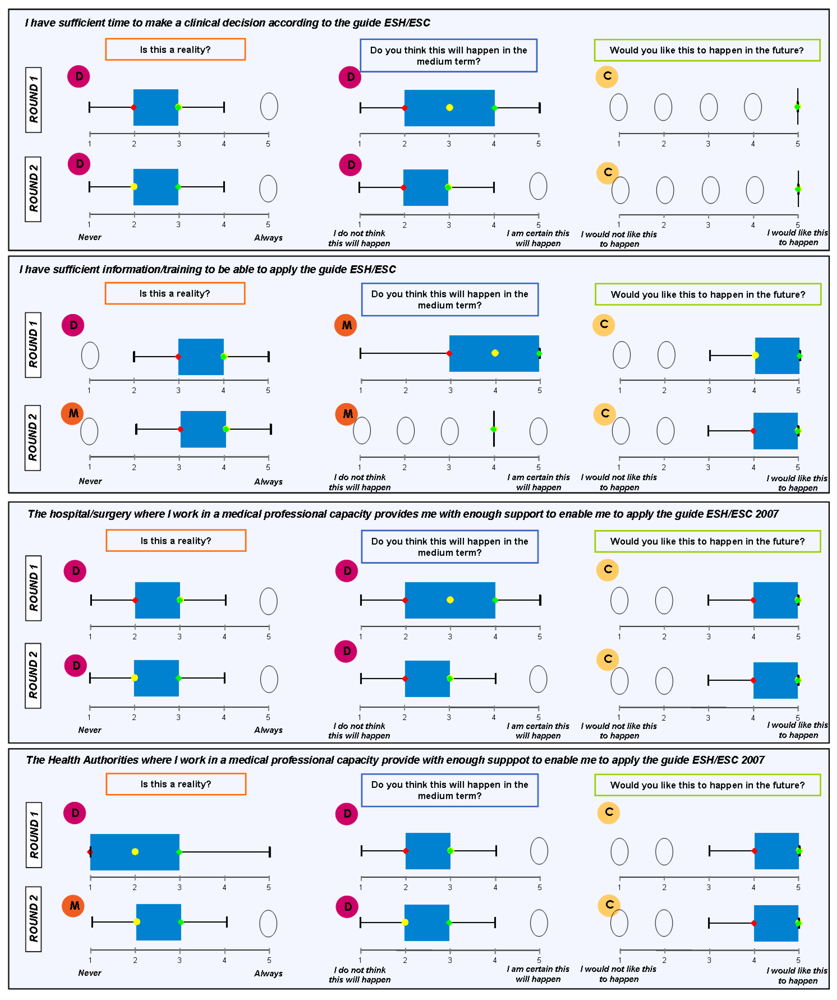
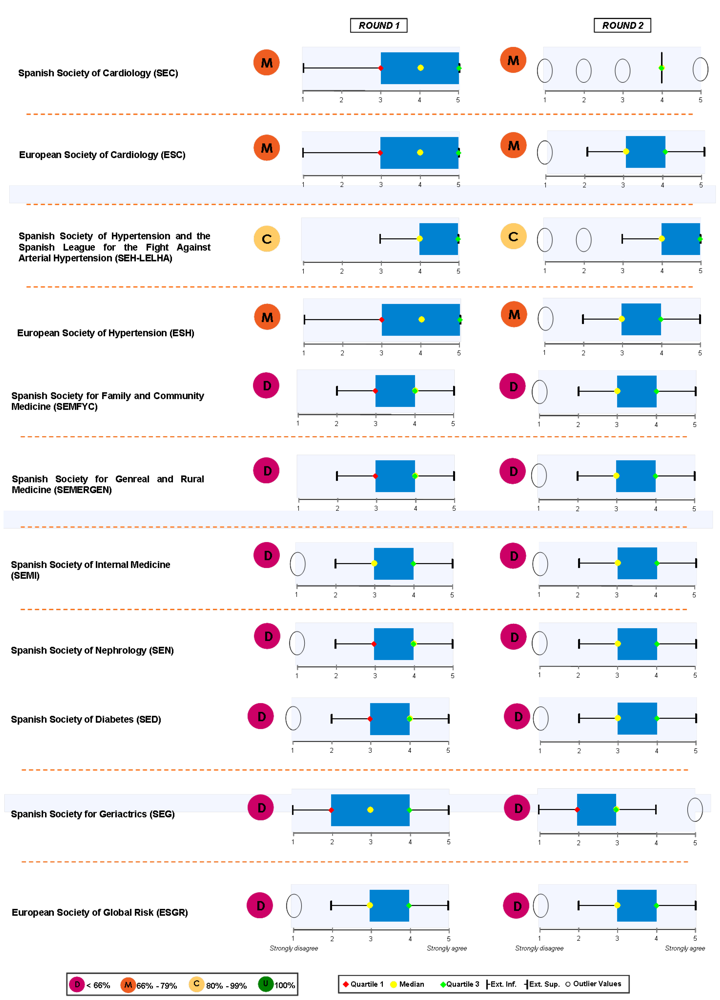
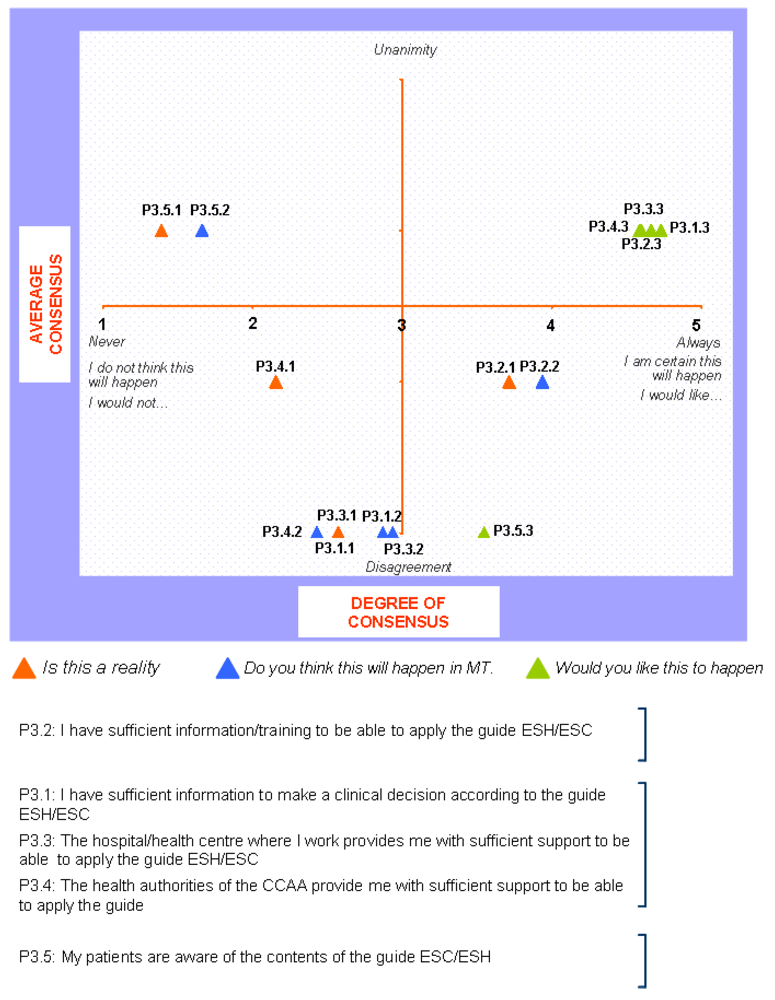
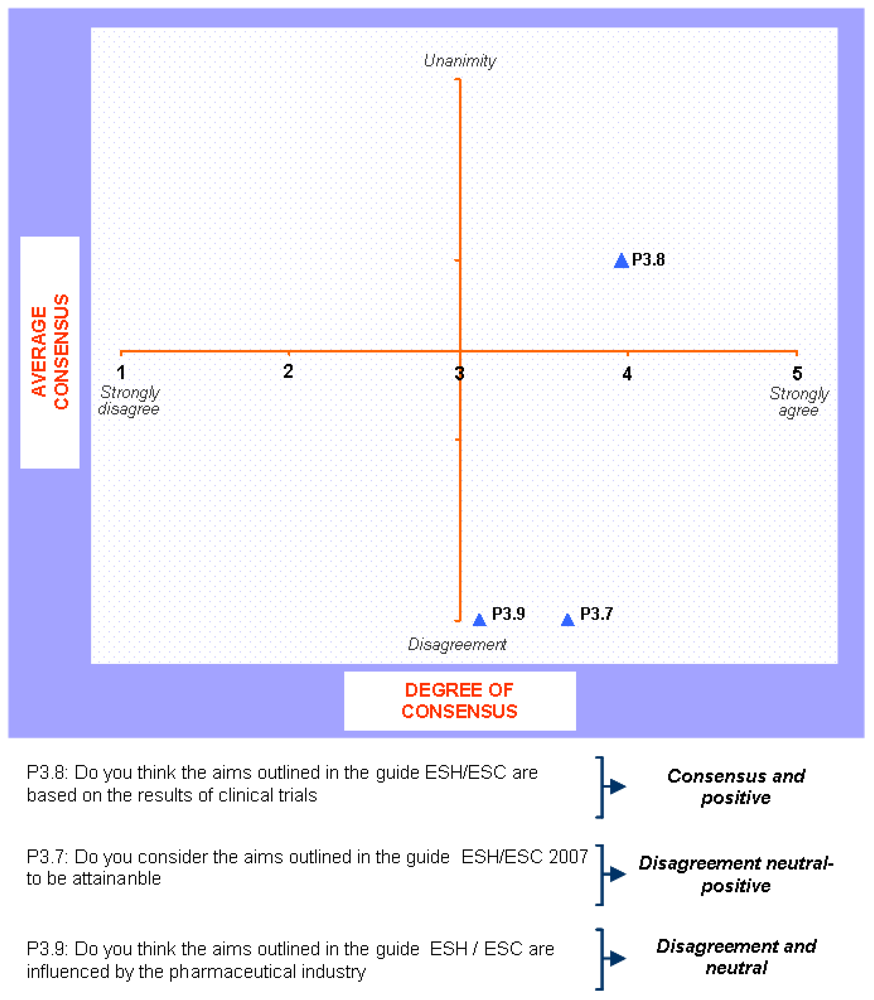
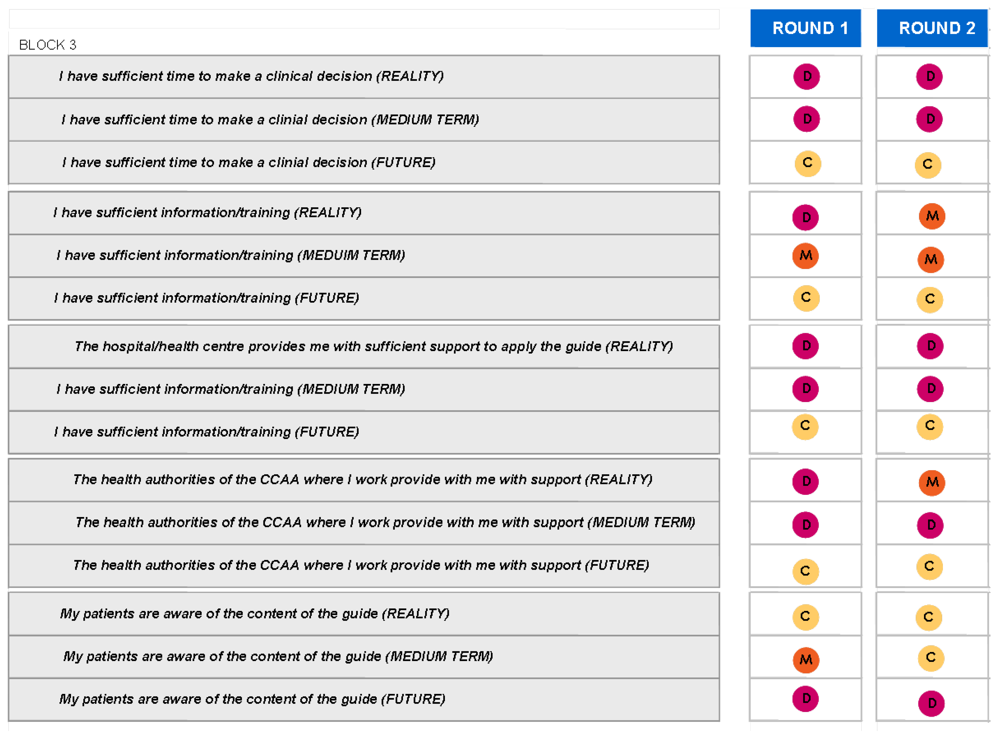
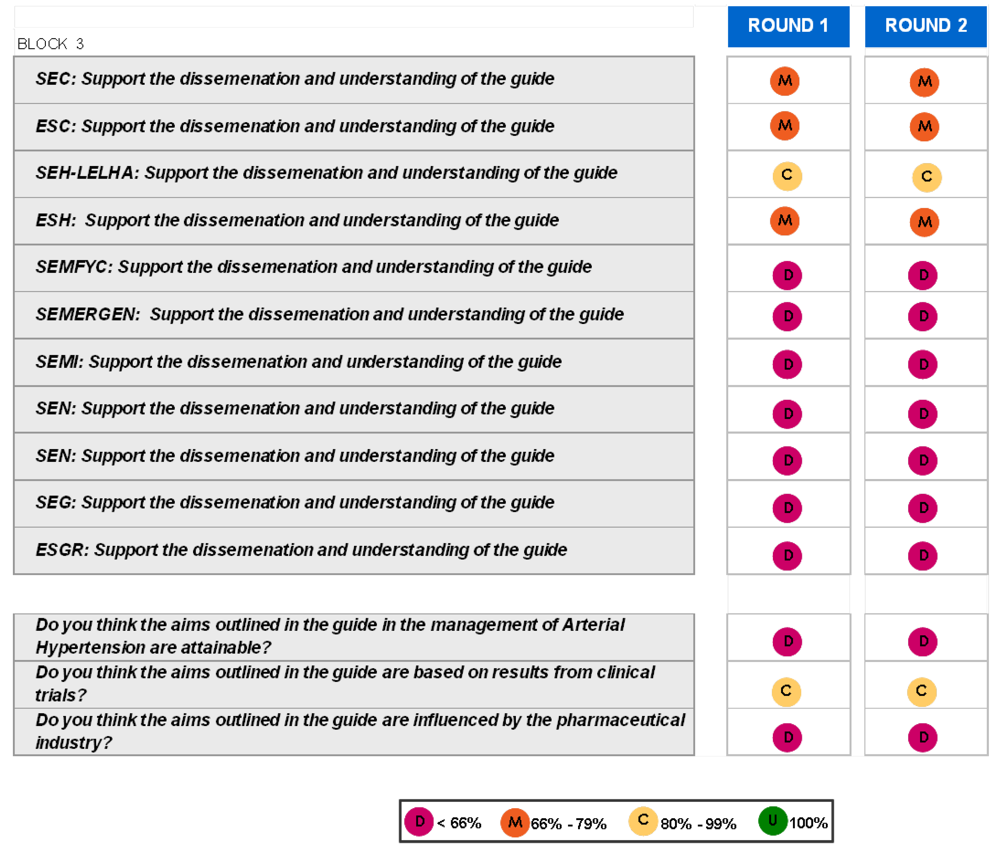
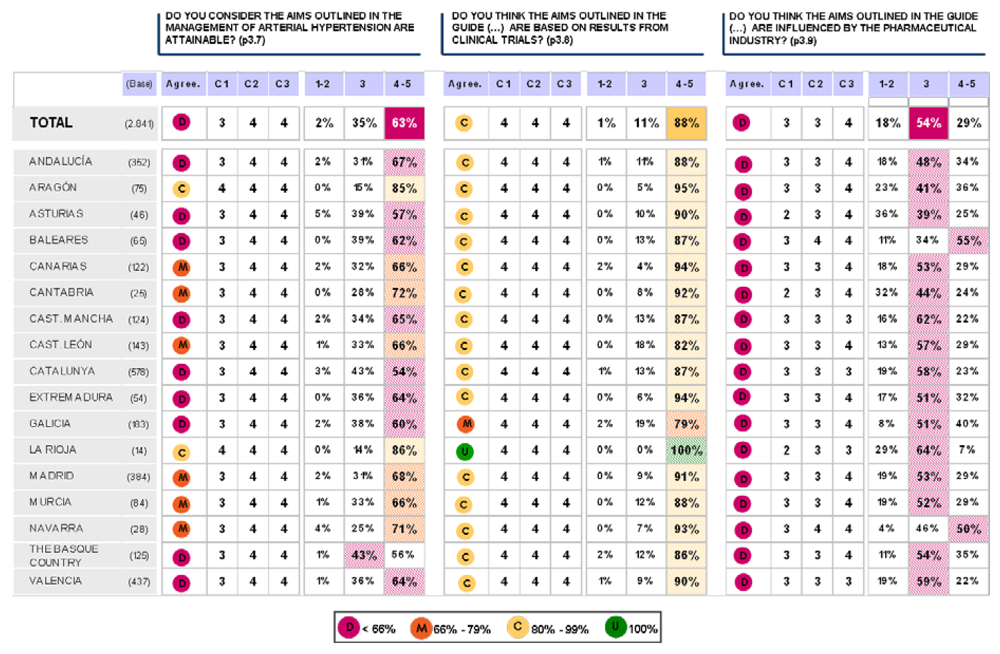
Block 3: Application of the guidelines















Discussion
The Delphi method
- 1)
- Structuring of information flow: The initial contributions from the experts are collected in the form of answers to questionnaires and their comments to these answers. The panel director controls the interactions among the participants by processing the information and filtering out irrelevant content. This avoids the negative effects of face-to-face panel discussions and solves the usual problems of group dynamics.
- 2)
- Regular feedback: Participants comment on their own forecasts, the responses of others and on the progress of the panel as a whole. At any moment they can revise their earlier statements. While in regular group meetings participants tend to stick to previously stated opinions and often conform too much to group leader, the Delphi method prevents it.
- 3)
- Anonymity of the participants: Usually all participants maintain anonymity. Their identity is not revealed even after the completion of the final report. This stops them from dominating others in the process using their authority or personality, frees them to some extent from their personal biases, allows them to express their opinions in a free manner and encourages critique and admitting errors.
Study results
Experimental Section
The Delphi method
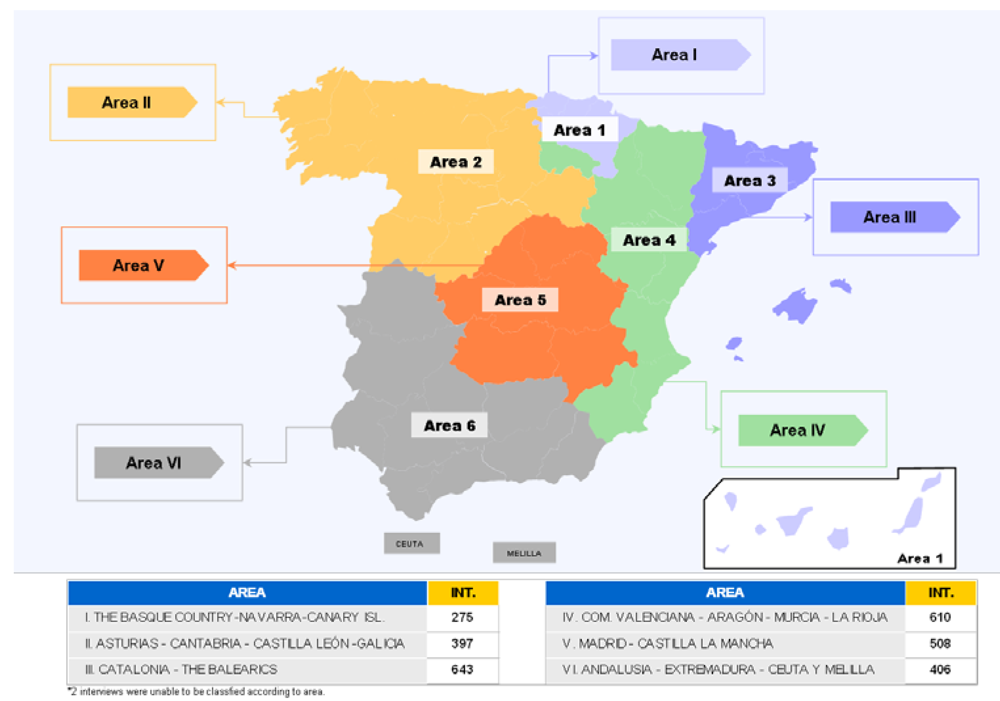
Study population


Conclusions
References and Notes
- Mancia, G.; De Backer, G.; Dominiczak, A.; Cifkova, R.; Fagard, R.; Germano, G.; Grassi, G.; Heagerty, A.M.; Kjeldsen, S.E.; Laurent, S.; Narkiewicz, K.; Ruilope, L.; Rynkiewicz, A.; Schmieder, R.E.; Boudier, H.A.; Zanchetti, A.; Vahanian, A.; Camm, J.; De Caterina, R.; Dean, V.; Dickstein, K.; Filippatos, G.; Funck-Brentano, C.; Hellemans, I.; Kristensen, S.D.; McGregor, K.; Sechtem, U.; Silber, S.; Tendera, M.; Widimsky, P.; Zamorano, J.L.; Erdine, S.; Kiowski, W.; Agabiti-Rosei, E.; Ambrosioni, E.; Lindholm, L.H.; Viigimaa, M.; Adamopoulos, S.; Agabiti-Rosei, E.; Ambrosioni, E.; Bertomeu, V.; Clement, D.; Erdine, S.; Farsang, C.; Gaita, D.; Lip, G.; Mallion, J.M.; Manolis, A.J.; Nilsson, P.M.; O'Brien, E.; Ponikowski, P.; Redon, J.; Ruschitzka, F.; Tamargo, J.; van Zwieten, P.; Waeber, B.; Williams, B.; Management of Arterial Hypertension of the European Society of Hypertension; European Society of Cardiology. 2007 Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 2007, 25, 1105–1187. [Google Scholar]
- Konow, I.; Gonzalo, P. Métodos y Técnicas de Investigación Prospectiva para la toma de Decisiones, 1st ed; Fundación de Estudios Prospectivos (FUNTURO) U. de Chile: Santiago de Chile, Chile, 1990. [Google Scholar]
- Guidelines Committee. 2003 European Society of Hypertension – European Society of Cardiology guidelines for the management of arterial hypertension. J. Hypertens. 2003, 21, 1011–1053.
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Whelton, P.K.; He, J. Worldwide prevalence of hypertension: a systematic review. J. Hypertens. 2004, 22, 11–19. [Google Scholar]
- Fagard, R.H.; Van Den Enden, M.; Leeman, M.; Warling, X. Survey on treatment of hypertension and implementation of World Health Organization/International Society of Hypertension risk stratification in primary care in Belgium. J. Hypertens. 2002, 20, 1927–1302. [Google Scholar]
- Burt, V.L.; Cutler, J.A.; Higgins, M.; Horan, M.J.; Labarthe, D.; Whelton, P.; Brown, C.; Roccella, E.J. Trends in the prevalence, awareness, treatment, and control of hypertension in the adult US population. Data from the health examination surveys, 1960 to 1991. Hypertension 1995, 26, 60–69. [Google Scholar] [PubMed]
- Amar, J.; Chamontin, B.; Genes, N.; Cantet, C.; Salvador, M.; Cambou, J.P. Why is hypertension so frequently uncontrolled in secondary prevention? Hypertens. 2003, 21, 1199–1205. [Google Scholar] [CrossRef]
- Mancia, G.; Ambrosioni, E.; Rosei, E.A.; Leonetti, G.; Trimarco, B.; Volpe, M.; For Life study group. Blood pressure control and risk of stroke in untreated and treated hypertensive patients screened from clinical practice: results of the For Life study. J. Hypertens. 2005, 23, 1575–1581. [Google Scholar]
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pérez de Isla, L.; Ruilope, L.M.; De la Sierra, A.; Zamorano, J. Knowledge and Implementation of the New European Guide in the Management of Arterial Hypertension. The Cigema Survey. Pharmaceuticals 2009, 2, 11-32. https://doi.org/10.3390/ph2020011
Pérez de Isla L, Ruilope LM, De la Sierra A, Zamorano J. Knowledge and Implementation of the New European Guide in the Management of Arterial Hypertension. The Cigema Survey. Pharmaceuticals. 2009; 2(2):11-32. https://doi.org/10.3390/ph2020011
Chicago/Turabian StylePérez de Isla, Leopoldo, Luis Miguel Ruilope, Alejandro De la Sierra, and José Zamorano. 2009. "Knowledge and Implementation of the New European Guide in the Management of Arterial Hypertension. The Cigema Survey" Pharmaceuticals 2, no. 2: 11-32. https://doi.org/10.3390/ph2020011