Role of Leukotrienes and Leukotriene Modifiers in Asthma

Department of Pharmacology, Faculty of Medicine, Catholic University of the Sacred Heart, Largo Francesco Vito, 1-00168 Rome, Italy
Pharmaceuticals 2010, 3(6), 1792-1811; https://doi.org/10.3390/ph3061792
Submission received: 21 April 2010
/
Revised: 13 May 2010
/
Accepted: 31 May 2010
/
Published: 2 June 2010
(This article belongs to the Special Issue Antiasthmatic Drugs)
Abstract
:Leukotrienes (LTs), including cysteinyl LTs (CysLTs) and LTB4, are potent lipid mediators that are pivotal in the pathophysiology of asthma phenotypes. At least two receptor subtypes for CysLTs – CysLT1 and CysLT2 – have been identified. Most of the pathophysiological effects of CysLTs in asthma, including increased airway smooth muscle activity, microvascular permeability and airway mucus secretion, are mediated by the activation of the CysLT1 receptor. LTB4 may have a role in the development of airway hyperresponsiveness, severe asthma and asthma exacerbations. Although generally less effective than inhaled glucocorticoids, CysLT1 receptor antagonists can be given orally as monotherapy in patients with persistent mild asthma. In patients with more severe asthma, CysLT1 receptor antagonists can be combined with inhaled glucocorticoids. This therapeutic strategy improves asthma control and enables the dose of inhaled glucocorticoids to be reduced, while maintaining similar efficacy. The identification of subgroups of patients with asthma who respond to CysLT1 receptor antagonists is relevant for asthma management, as the response to these drugs is variable. The potential anti-remodeling effect of CysLT1 receptor antagonists might be important for preventing or reversing airway structural changes in patients with asthma. This review discusses the role of LTs in asthma and the therapeutic implications of the pharmacological modulation of the LT pathway for asthma.
1. Introduction
Leukotrienes (LTs), including cysteinyl-LTs (LTC4, LTD4, and LTE4) and LTB4, are potent biological lipid mediators derived from arachidonic acid through the 5-lipoxygenase (5-LO) pathway [1,2,3,4,5]. Specific pathways for the synthesis of cysteinyl-LTs from arachidonic acid are present in several types of inflammatory cells and become activated during allergic airway inflammation [3,5]; moreover, other cell types like platelets and endothelial cells have a unique capacity to produce large amounts of cysteinyl-LTs from the chemically reactive intermediate LTA4 via intercellular transfer mechanisms [5].
Leukotrienes play a central pathophysiological role in asthma [1,2,3,4,6], particularly in specific subgroups of patients with asthma. Cysteinyl-LTs induce pathophysiological responses similar to those associated with asthma and elevated cysteinyl-LT concentrations have been detected in biological fluids, including bronchoalveolar lavage (BAL) [7], sputum [8], and exhaled breath condensate (EBC) from patients with asthma [9,10]. The cysteinyl-LTs are likely to contribute to airway remodelling that characterises persistent asthma [11,12].
Two G-protein coupled receptor subtypes for cysteinyl-LTs (CysLT1 and CysLT2) have been identified [13,14]. Most of the effects of cysteinyl-LTs relevant to the pathophysiology of asthma are mediated by activation of the CysLT1 receptor [2,3], which is expressed in different types of inflammatory and structural cells in the airways [13,15].
The most convincing evidence for an etiological role of cysteinyl-LTs in asthma comes from the therapeutic efficacy of CysLT1 receptor antagonists (e.g., montelukast, zafirlukast, pranlukast), commonly known as leukotriene receptor antagonists (LTRAs), and 5-lipoxygenase (5-LO) inhibitors (e.g., zileuton) in patients with asthma [4]. These drugs are effective in preventing asthmatic responses induced by allergen-challenge [16], exercise [17], and aspirin [18]. Moreover, CysLT1 receptor antagonists have a therapeutic role in persistent asthma as they improve pulmonary function, symptoms and quality of life, and reduce β-agonist use, airway and peripheral eosinophilia, asthma exacerbations, and the required dose of inhaled corticosteroids in asthma patients [19,20].
CysLT1 receptor antagonism has anti-remodeling effects in the airways in an animal model of human asthma [21] and inhibitory effects on airway structural cells that are functionally involved in airway remodeling in allergic airway inflammation in patients with asthma [22].
As a potent chemoattractant for neutrophils, LTB4 can have a central role in the neutrophilic inflammation that characterises severe asthma and asthma exacerbations [23], whereas its role in mild to moderate persistent asthma is less known. Elevated LTB4 concentrations in EBC have been reported in adults and children with stable asthma [24,25,26,27,28]. The lack of effect of LTB4 receptor antagonists in allergen-induced early or late phase airway obstruction in patients with asthma [29] argues against an important role for LTB4 in acute bronchoconstriction in asthma. However, a role for LTB4 in airway hyperresponsiveness (AHR) in asthma has been proposed [30,31,32].
This review will examine the role of leukotrienes in asthma and the therapeutic implications of the leukotriene pathway inhibition for asthma.
2. Biosynthesis and Metabolism of Leukotrienes
Leukotrienes derive from 5-LO activity (Scheme 1). Arachidonic acid, that is esterified on plasma membrane phospholipids, is cleaved by the action of different phopsholipase A2 enzymes, released and metabolized into LTA4. This leukotriene is subsequently metabolized by LTA4 hydrolase into LTB4 and, into LTC4 by LTC4 synthase or different members of the membrane-associated proteins in the eicosanoid and glutathione metabolism superfamily (MAPEG), including microsomal glutathione transferase 2 (MGST2) [5]. LTC4 in turn is metabolized by a γ-glutamyl transpeptidase into LTD4 that is then metabolized by a dipeptidase into LTE4. LTA4 is highly reactive, with an estimated half-life < 3 seconds [5]. LTC4 and its metabolites, LTD4 and LTE4, are known as cysteinyl-LTs due to the common cysteine in their side chains. Biosynthesis of LTs requires cellular activation, including IgE receptor cross-binding on mast cell surface, and involves a five-lipoxygenase activating protein (FLAP) that binds 5-LO and facilitates the metabolism of arachidonic acid [2,3,5]. The intracellular distribution of 5-LO varies between different cells. 5-LO is mainly expressed in granulocytes, monocytes, macrophages, mast-cells and B lymphocytes [3]. Mast cells and eosinophils can produce large amounts of LTC4 from an endogenous pool of arachidonic acid. Human bronchial fibroblasts constitutively express 5-LO, FLAP, LTA4 hydrolase, and LTC4 synthase and produce cysteinyl-LTs and LTB4 spontaneously in vitro [33]. Cells that do not express 5-LO, including platelets, erythrocytes, endothelial cells and epithelial cells, also have the capacity to produce cysteinyl-LTs and/or LTB4 through the transcellular metabolism of LTA4 synthesized by activated neutrophils [5]. After their intracellular formation, cysteinyl-LTs and LTB4 are released to the extracellular space through specific carrier-proteins that are potential targets for future antileukotriene drugs [3].
Scheme 1.
Biosynthetic pathway of leukotrienes (LTs), LT receptors, and mechanisms of action of antileukotriene drugs (reproduced with permission from reference [2]).
Scheme 1.
Biosynthetic pathway of leukotrienes (LTs), LT receptors, and mechanisms of action of antileukotriene drugs (reproduced with permission from reference [2]).

3. Receptors and Mechanism of Action of Leukotrienes
Two G-protein coupled receptor subtypes for cysteinyl-LTs (CysLT1 and CysLT2), that have 38% amino acid identity, have been identified [13,14] (Scheme 1). There is evidence that supports the existence of distinct CysLT receptors [34,35,36,37,38]. Increased vascular permeability induced by LTE4 in mice lacking CysLT1 and CysLT2 receptors suggests the existence of a third cysLT receptor that responds preferentially to LTE4 [34]. A G-protein-coupled receptor (GPCR) GPR17, that responds both to cysteinyl-LTs and to uracil nucleotides [38], is a ligand independent, constitutive negative regulator for the CysLT1 receptor and suppresses CysLT1 receptor-mediated function at the cell membrane [35]. Most of the effects of cysteinyl-LTs relevant to the pathophysiology of asthma are mediated by activation of the CysLT1 receptor [1,2] that is expressed in monocytes and macrophages, eosinophils, basophils, mast cells, neutrophils, T cells, B lymphocytes, pluripotent hemopoietic stem cells (CD 34+), airway smooth muscle cells, bronchial fibroblasts, and vascular endothelial cells [13,15,33]. The CysLT2 receptor is expressed in human peripheral basophils [39], endothelial cells [40], cultured mast cells [14], and in nasal eosinophils and mast cells in patients with active seasonal allergic rhinitis [41]. In human cultured mast cells, CysLT2 activation may elicit IL-8 generation with potential neutrophilic inflammation [14] that is a characteristic of acute and severe asthma. Expression of CysLT2 receptors on eosinophils is increased in patients with asthma exacerbations, especially in nonatopic subjects, and is up-regulated by interferon-γ indicating a role for this receptor subtype in acute asthma [42]. At present, the role of the CysLT2 receptor in allergic inflammation is largely unknown [40]. CysLT1 and CysLT2 receptor activation involves increased intracellular calcium [13,43], but the complete signal transduction pathway is not known. In cell lines derived from humans and monkeys, protein kinase C activity is the principal regulator of both rapid agonist-dependent internalization and rapid agonist-dependent desensitization [43].
Two LTB4 receptor subtypes (BLT1 and BLT2), that are cell surface G protein-coupled seven transmembrane domain receptors, have been identified [44,45]. Both receptor subtypes are expressed in a human mast cell line (HMC-1) [46]. BLT1 receptors are expressed in human bronchial fibroblasts [33] and in a subset of effector memory IL-13-producing CD8+ T cells in bronchoalveolar lavage fluid of patients with asthma [47]. BLT1 expression on Ag-primed T cells [48] and dendritic cells [31] is required for the development of AHR in mice, indicating a possible role for LTB4 in AHR in patients with asthma.
4. Biological Effects of Leukotrienes in the Airways
Cysteinyl-LTs induce pathophysiological responses that are observed in patients with asthma [1,2,3]. Cysteinyl-LTs are the most potent endogenous bronchoconstrictors. LTC4, LTD4, and LTE4 have similar contractile activity on human airway smooth muscle in vitro. This effect has been confirmed by bronchoprovocation studies in healthy subjects [3]. Patients with asthma are hyperresponsive to inhalation of LTC4, LTD4, and LTE4 [3]. Cysteinyl-LTs increase mucus secretion in isolated animal and human airways and increase microvascular permeability in the lungs in experimental animals [3]. These effects can contribute to bronchial obstruction in patients with asthma. Cysteinyl-LT inhalation in patients with asthma increases the number of sputum eosinophils and causes recruitment of eosinophils into the airway mucosa [49]. However, the mechanism(s) of the eosinophil chemotactic effect induced by cysteinyl-LTs in not completely known.
In addition to their local effects in the airways, cysteinyl-LTs have several effects that contribute to the inflammatory processes characterising asthma [4,50]. Cysteinyl-LTs (1) modulate leucopoiesis induced by granulocyte-macrophage colony stimulating factor, interleukin (IL)-5, and IL-3 and prime progenitor cells to differentiate into mature blood cells; (2) induce leukocyte migration from the bone marrow into the circulatory system; (3) cause chemotaxis of eosinophils increasing their cellular adhesion and transendothelial migration accross the vessel wall into the airways; (4) increase eosinophil survival in response to mast cell and lymphocyte paracrine signals; (5) activate eosinophils, mast cells, T lymphocytes, monocytes and basophils [4,50]. Cysteinyl-LTs have a central role in lung inflammation induced by allergen challenge as shown by the reduced Th2 cell-dependent inflammatory response in LTC4 synthase null mice [51].
Cysteinyl-LTs are functionally involved in airway remodeling that includes eosinophil cell inflammatory response, airway smooth muscle cell hyperplasia, mucus gland hyperplasia, mucus hypersecretion, and collagen deposition beneath the epithelial layer and in the lung interstitium at sites of leukocytes infiltration [11,12]. Montelukast reduces allergen-induced lung inflammation and fibrosis in an animal model of the airway remodeling changes observed in patients with persistent asthma [21].
LTB4 may contribute to a reduction in airway calibre due to local edema and increasing mucus secretion, although it has no bronchoconstrictor effect in healthy and asthmatic subjects [2,3]. As it is a potent chemoattractant for neutrophils, LTB4 might be functionally involved in the neutrophilic phenotype of asthma that characterizes patients with severe asthma [23] or asthma exacerbations. Persistently elevated LTB4 concentrations in plasma in children with asthma exacerbation at least one month after the acute episode [52], elevated LTB4 concentrations in EBC in adults with mild asthma [24], and elevated LTB4 concentrations in EBC in children with mild-to-moderate persistent asthma [26] could indicate a pathophysiological role of LTB4 in chronic stable asthma of lesser severity [53]. However, the pathophysiological role of LTB4 in mild-to-moderate persistent asthma in not completely known and requires further studies. In mice, LTB4 has an essential role in triggering airway allergic responses by activating BLT1 receptors on a subset of effector CD8+ T cells [47]. The absence of BLT1 receptors or their antagonism on these cells markedly reduces allergen challenge-induced AHR and airway inflammation in mice [31,47,48]. A subset of CD8+ T cells expressing BLT1 receptors have been identified in BAL and lung tissue from subjects with asthma, but not from healthy subjects [47]. The number of this subset of CD8+ T cells is increased in patients with steroid-resistant asthma compared with those with steroid-sensitive asthma [47], indicating a possible role for BLT1 receptors in steroid response. However, the biological significance of LTB4-induced activation of effector CD8+ T cells in patients with asthma needs to be established. A role for LTB4 in AHR is also suggested by the fact that chronic treatment with zileuton, that reduces synthesis of both cysteinyl-LT and LTB4, decreases AHR in asthmatic patients [54,55], concomitant with a reduction of ex vivo LTB4 production [55]. In contrast, selective CysLT1 antagonists have only a modest effect on AHR [4,56]. 5-LO inhibition is very effective in causing chronic improvement in nasal function in patients with aspirin-sensitive asthma (ASA) at baseline [54], whereas CysLT1 receptor antagonists, that significantly reduce bronchospastic response, have only minor effects on ASA-induced upper airway reactions [57]. These data indicate that LTB4 can have a pathophysiological role in nasal symptoms in ASA. Alternatively, or in addition to that, nasal symptoms in patients with ASA could be due to activation of CysLT2 receptors or distinct LTE4 receptors [34,35,36,37,38]. Although LTE4 has little activity at CysLT1 and CysLT2 receptors [37], inhalation of LTE4 increases airway inflammatory cells [58,59] and AHR in asthma patients [60], particularly in those with ASA [37]. In sensitized mice, intranasal LTE4 potentiates pulmonary inflammation in response to low-dose aerosolized antigen [36]. This effect persists in mice lacking both CysLT1 and CysLT2 receptors but not in mice lacking P2Y12 receptors, indicating that the P2Y12 receptor is required for pro-inflammatory effects of LTE4 [36].
5. Measurement of LTs in Biological Fluids in Patients with Asthma
LTs have been measured in exhaled breath condensate (EBC) [9,10,24,25,26,27,28,61,62,63,64], sputum [27,65], BAL fluid [7], and urine [66,67,68] from asthmatic patients. There are several reports of increased LT levels in EBC in both adults and children with asthma [9,10,24,25,26,27,28,61,62,63,64,69], but the methodology used requires standardization [70]. Sputum CysLT concentrations are elevated in patients with asthma, reflecting asthma severity [65]. LT concentrations are increased in BAL fluid in patients with asthma, including those with nocturnal asthma [7]. Measurement of LTs in BAL fluid, sputum and EBC is likely to reflect pulmonary synthesis of LTs.
Urinary measurement of LTE4, the most abundant CysLT excreted in the urine, is used for assessing the systemic synthesis of CysLTs as circulating concentrations of LTs are usually undetectable [66]. No or only slight differences in urinary LTE4 concentrations between healthy and atopic asthmatic subjects have generally been reported under basal conditions [66]. In contrast, urinary LTE4 excretion is elevated after allergen challenge in atopic asthmatics [3,66], in aspirin-sensitive asthmatics under basal conditions [67], in patients with nocturnal asthma [7], in severe asthma [71], and during asthma exacerbations [68].
6. Effects of Leukotriene Receptor Antagonists in Asthma
Selective CysLT1 receptor antagonists that have been approved for clinical use in asthma include montelukast, zafirlukast and pranlukast (Table 1). Zileuton, a 5-LO inhibitor, has been approved for the prevention and chronic treatment of asthma in adults and children 12 years of age and older in the United Kingdom and USA (Table 1). Montelukast is the most prescribed CysLT1 receptor antagonist in Europe and the USA, whereas pranlukast is only marketed in Japan and other Asian countries. Zafirlukast was the first anti-LT that was approved in Europe, but it is not frequently prescribed due to possible food and drug interactions, and its twice daily administration regimen [2,3]. The fact that selective CysLT1 receptor antagonists and 5-LO inhibitors have similar efficacy in short-term treatment studies and challenge models indicates that most of the antiasthmatic effects of anti-LTs are due to CysLT1 antagonism [3]. The use of zileuton is limited because of a small, but distinct, incidence of hepatic enzyme elevation, which is not observed with montelukast, and the short half-life, requiring four daily administrations [3]. A twice-daily controlled-release formulation of zileuton has been approved by the U.S. Food and Drug Administration (FDA) [1].
At least two aspects of selective 5-LO inhibitors concerning the inhibition of LTB4 synthesis deserve further investigation: their effects on AHR in patients with asthma [54,55], that is slightly affected by CysLT1 antagonists [4]; the potential efficacy of 5-LO inhibitors in rhinitis and rhinopolyposis as these drugs are very effective in reducing nasal symptoms in patients with ASA [54].

{kind=link}
{kind=link}
{kind=link}
Table 1.
Main pharmacological characteristics of antileukotrienes (reproduced with permission from reference [2]).
| Drug | Mechanism of action | Indication | Benefits | Side effects | Dose | Comments |
|---|---|---|---|---|---|---|
| Montelukast | CysLT1 receptor antagonism | asthma, allergic rhinitis | as monotherapy in children with mild persistent asthma; particularly effective in exercise-induced asthma, ASA, allergen-induced asthma; as add-on therapy with ICS | headache, abdominal pain; possible association with Churg-Strauss syndrome | adults: 10 mg o.d. children 6 to 14 years of age: 5 mg o.d. children 2 to 5 years of age: 4 mg o.d. | most widely prescribed CysLT1 receptor antagonist |
| Pranlukast | CysLT1 receptor antagonism | asthma, allergic rhinitis | particularly effective in exercise-induced asthma, ASA, allergen-induced asthma; as add-on therapy with ICS | abdominal pain, liver enzymes elevations; possible association with Churg-Strauss syndrome | adults: 225 mg b.i.d. | only marketed in Asia |
| Zafirlukast | CysLT1 receptor antagonism | asthma | particularly effective in exercise-induced asthma, ASA, allergen-induced asthma; as add-on therapy with ICS | headache, abdominal pain, liver enzymes elevations; possible association with Churg-Strauss syndrome | children ≥ 12 years of age and adults: 20 mg b.i.d. children 5 to 11 years of age: 10 mg b.i.d. | first CysLT1 receptor antagonist to be approved; food and drug interactions |
| Zileuton | 5-LO inhibition | asthma | particularly effective in exercise-induced asthma and ASA | headache, abdominal pain; liver enzymes elevations (5%) | adults and children 12 years of age and older: 600 mg q.i.d. | virtually abandoned because of poor compliance and hepatic toxicity |
Abbreviations: ASA = aspirin-sensitive asthma; CysLT = cysteinyl-leukotrienes; ICS = inhaled corticosteroids.
CysLT1 receptor antagonists improve symptoms and lung function, and reduce exacerbation rate, the use of rescue β2 bronchodilators, and airway and blood eosinophilia in adults and children with asthma of different severity [1,2,3,4]. Cys-LT1 receptor antagonists provide a prompt improvement in asthma control, although low-dose inhaled glucocorticoids are generally more effective than Cys-LT1 receptor antagonists as first-line maintenance therapy for patients with persistent asthma who are undertreated and remain symptomatic while taking short-acting β2-agonists alone [20]. When added to standard therapy in adults with asthma exacerbations, intravenous montelukast (7 mg) significantly improves airway obstruction throughout the 2 hours immediately after administration, with an onset of action as early as 10 minutes, indicating a possible therapeutic role for CysLT1 receptor antagonists in severe acute asthma [72,73]. CysLT1 receptor antagonists are effective in reducing early and late asthmatic responses induced by allergen inhalation [16,74]. Unlike budesonide, montelukast inhibits the maximal early asthmatic response, whereas both drugs attenuate the late asthmatic response [16]. However, anti-LTs reduce allergen-induced AHR to a lesser extent than do inhaled glucocorticoids [16]. This could be explained by the fact that AHR is multifactorial and relatively independent of the acute inflammatory response mediated by LTs. Moreover, inhaled glucocorticoids inhibit several airway inflammatory cells and mediators that are pivotal in the AHR pathophysiology, whereas anti-LTs selectively block LT-mediated eosinophilic inflammation [16]. CysLT1 receptor antagonists are also effective in reducing allergen-induced asthmatic response in children [75]. Montelukast given once daily at a dose of 10 mg protected against exercise-induced broncho-constriction over a 12-week period in adults with asthma [17]. Treatment with CysLT1 receptor antagonists reduces the time to recovery from the maximal decrease in FEV1, the maximal decrease in FEV1, and the area under the FEV1 versus time curve after exercise [17]. These effects are observed as soon as two hours after a single oral dose of montelukast (10 mg) and are maintained up to 24 hours [76,77]. Montelukast was superior to salmeterol in the chronic treatment of exercise-induced bronchoconstriction over a period of eight weeks in adults with mild asthma, as demonstrated by effect size, peristence of effect and higher tolerability during the study period [78]. Likewise, CysLT1 receptor antagonists are effective in exercise-induced bronchoconstriction in children [79]. CysLT1 antagonism and 5-LO inhibition protect against the reduction in FEV1 in response to aspirin challenge [3] and improve asthma control in aspirin-sensitive patients over and above the therapeutic response to glucocorticoids, an effect that is independent of baseline urinary LTE4 [18,54].
Some aspects of the clinical pharmacology of CysLT1 receptor antagonists deserve further discussion: (1) their role as monotherapy in patients with asthma; (2) their efficacy and the possibility of reducing the dose of inhaled glucocorticoids when addedd to these drugs; (3) the variability in their therapeutic response; (4) their potential anti-remodeling effect in the airways; (5) their safety.
In the USA, monotherapy with CysLT1 receptor antagonists is a common therapeutic option for patients with mild asthma [80], although inhaled glucocorticoids are generally preferred [81] as in Europe. However, CysLT1 receptor antagonists are less effective than inhaled glucocorticoids as first-line agents in both adults [20] and children with asthma [82].
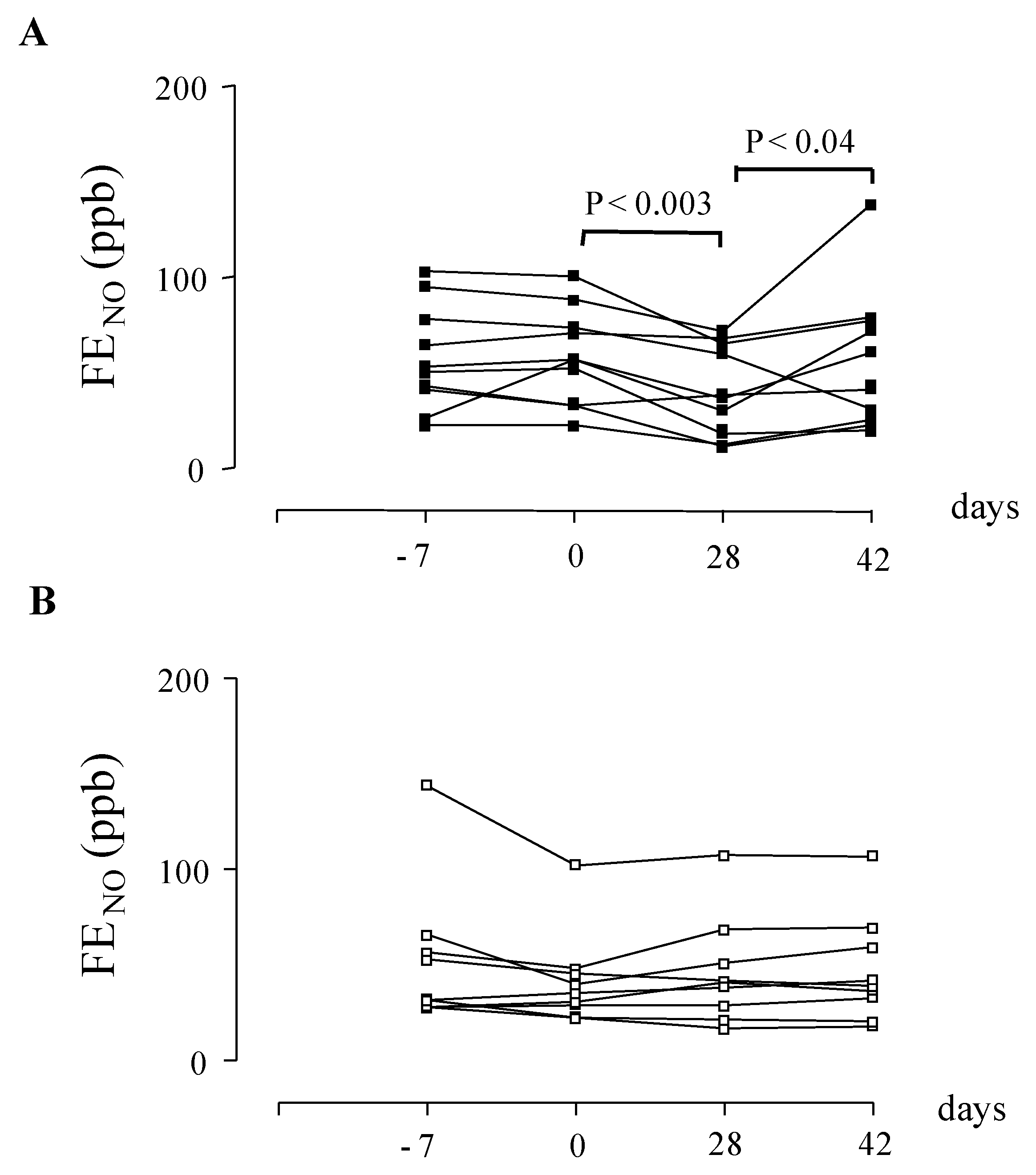
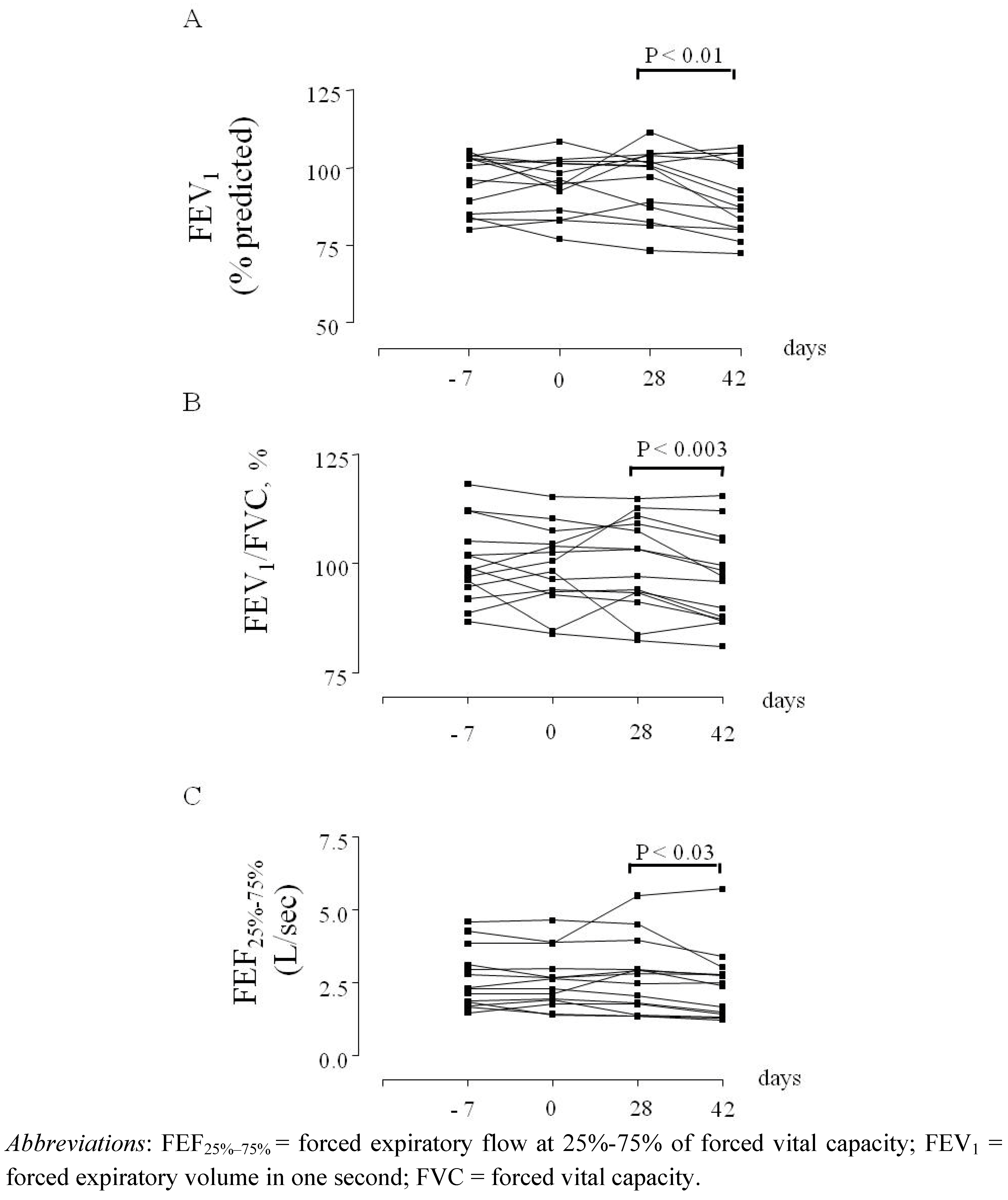
In Europe, CysLT1 receptor antagonists are currently indicated for preventing exercise-induced bronchoconstriction [3]. In patients with asthma who are not sufficiently controlled with a constant dose of inhaled budesonide alone, add-on therapy with montelukast improves asthma control [83] to a level comparable to that achieved by doubling the dose of budesonide [19]. The advantage of this therapeutic strategy would be the reduced risk of side effects due to long-term administration of high-dose inhaled glucocorticoids [19]. In patients whose symptoms remain uncontrolled with inhaled fluticasone alone, the addition of montelukast is a therapeutic option [84], although the addition of a long-acting β2-agonist (LABA) is generally more effective than a CysLT1 receptor antagonist for preventing exacerbations requiring systemic steroids, and for improving lung function, symptoms and the use of rescue β2 agonists [85,86]. In patients with well-controlled asthma based on symptoms and lung function testing, the addition of pranlukast to the combination of inhaled glucocorticoids and LABAs gives better control of airway inflammation compared with therapy with the combination of inhaled glucocorticoid/LABA alone [87,88]. In children with mild persistent asthma, montelukast withdrawal can result in enhanced airway inflammation, as reflected by increased fractional exhaled nitric oxide concentrations (FENO) (Figure 1) and worsening of lung funtion (Figure 2) [89]. Add-on therapy with CysLT1 receptor antagonists enables a reduction in the dose of inhaled glucocorticoids required to control asthma [19,90]. As the LT pathway is relatively steroid-resistant [91], the combination of LTRAs and inhaled glucocorticoids can increase therapeutic efficacy in subgroups of patients with asthma who respond to LTRAs.
Figure 1.
(A) Fractional exhaled nitric oxide (FENO) in children with asthma (n = 14) at baseline (day -7), before treatment with montelukast (filled squares) (day 0), after treatment with oral montelukast (5 mg qd for four weeks) (day 28), and two weeks after montelukast withdrawal (day 42). (B) FENO in children with asthma (n = 12) at baseline (day -7), before treatment with placebo (open squares) (day 0), after treatment with matching placebo (5 mg qd for four weeks) (day 28), and two weeks after placebo withdrawal (day 42). Values are expressed as mean ± SD.
Figure 1.
(A) Fractional exhaled nitric oxide (FENO) in children with asthma (n = 14) at baseline (day -7), before treatment with montelukast (filled squares) (day 0), after treatment with oral montelukast (5 mg qd for four weeks) (day 28), and two weeks after montelukast withdrawal (day 42). (B) FENO in children with asthma (n = 12) at baseline (day -7), before treatment with placebo (open squares) (day 0), after treatment with matching placebo (5 mg qd for four weeks) (day 28), and two weeks after placebo withdrawal (day 42). Values are expressed as mean ± SD.

Figure 2.
FEV1 percentage of predicted values (A), FEV1/FVC ratio values (B), and FEF25%–75% values (C) in children with asthma (n = 14) at baseline (day -7), before treatment with montelukast (day 0), after treatment with oral montelukast (5 mg qd for four weeks) (day 28), and two weeks after montelukast withdrawal (day 42).
Figure 2.
FEV1 percentage of predicted values (A), FEV1/FVC ratio values (B), and FEF25%–75% values (C) in children with asthma (n = 14) at baseline (day -7), before treatment with montelukast (day 0), after treatment with oral montelukast (5 mg qd for four weeks) (day 28), and two weeks after montelukast withdrawal (day 42).

AHR to LTD4, and urinary LTE4 concentrations in adults with mild asthma are not affected by inhaled fluticasone (500 μg b.i.d. for two weeks) [91]. Treatment with inhaled fluticasone (100 μg b.i.d. for four weeks) reduces LTE4 concentrations in EBC by 18% in children with intermittent and mild persistent asthma [10]. Taken together, this evidence indicates that inhaled glucocorticoids have limited, if any, effects on the biosynthesis of Cys-LTs and AHR to Cys-LTs [91].
The therapeutic response to CysLT1 receptor antagonists as well as to inhaled glucocorticoids in both adults [19,92,93] and children with asthma is variable [82,92]. Identification of patients who are most likely to respond to LTRAs and/or inhaled glucocorticoids might have important clinical implications, in view of the fact that a tailored, individualized approach to asthma management and assessment is preferable for asthma control than a strategy directed to the best outcome in a group of patients [82]. Some phenotypic features, including higher FENO concentrations, serum IgE and eosinophil cationic protein concentrations, total blood eosinophil counts, lower levels of methacholine provocative concentration (PC)20 causing a 20% fall in FEV1 and lower levels of pulmonary function, are associated with a therapeutic response to fluticasone in children with asthma [82,92]; a therapeutic response to montelukast is associated with younger age, shorter disease duration, higher urinary LTE4 concentrations [82,92] and elevated LTE4 concentrations in EBC [9]. Studies on biomolecule profiles in biological fluids and genetic polymorphisms of 5-LO pathway and CysLT receptors [94] could help to predict the therapeutic response to CysLT1 receptor antagonists.
In an animal model of asthma, CysLT1 receptor antagonists not only prevent allergen-induced airway changes, but also reverse structural changes including subepithelial fibrosis and airway smooth muscle cell layer thickening that are not affected by glucocorticoid treatment [21]. These findings could clarify the role of Cys-LTs in airway remodeling [12] and have important implications for the management of patients with asthma as they might indicate new therapeutic effects of CysLT1 receptor antagonists. Inhaled glucocorticoids also reduce basal membrane thickening [95] and subepithelial collagen deposition [96], although these effects seem to have limited impact on the clinical evolution of asthma [97]. In one study, montelukast at a dose of 10 mg once daily for eight weeks reduced myofibroblast accumulation in the airways observed in biopsies of patients with asthma following low-dose allergen challenge [22]. However, whether CysLT1 receptor antagonists prevent airway remodeling and/or reverse established airway structural changes in patients with asthma require further research.
CysLT1 receptor antagonists are generally considered to be safe and well tolerated, with headache and gastric discomfort being the most common side effects [3]. However, an association between treatment with CysLT1 receptor antagonists and severe adverse events including Churg–Strauss syndrome [98] and suicidality [99] has been reported. An etiologic role for CysLT1 receptor antagonists in the Churg–Strauss syndrome is generally excluded [3]. However, a recent analysis of the FDA adverse event reporting system database has shown that LTRA therapy was a suspect medication in most confirmed cases of Churg–Strauss syndrome reported [98]. In the majority of cases treated with a LTRA, Churg–Strauss syndrome could not be explained by either glucocorticoid withdrawal or pre-existing Churg–Strauss syndrome [98]. Based on a limited number of postmarketing suicide-related adverse experience reports, the FDA issued a warning raising concerns about the suicidality potential of montelukast and other CysLT1 receptor antagonists, and similar changes were submitted to regulatory agencies around the world in October 2007 [99]. A review of the available clinical trial database on montelukast regarding suicidality showed that no completed suicides were reported in any studies [99]; adverse experiences possibly related to suicidality were rare and were similar between the montelukast and placebo or active-control groups [99]. At present, there is insufficient data to prove that there is a link between montelukast and suicidality [100]. Results from three randomized, double-masked, controlled trials conducted by the American Lung Association Asthma Clinical Research Centers, that included a total of 1469 patients of whom 569 patients were assigned to montelukast, did not show evidence of a negative effect of montelukast on emotional well being as a marker for depression [101]. However, due to the relevance of this safety issue, a close monitoring of suicidality in patients treated with LTRAs is warranted. There are limited prospective, comparative studies examining the safety of CysLT1 receptor antagonists in pregnancy [102]. Montelukast does not appear to increase the baseline rate of major malformations [102,103]. The lower birth weight observed in infants born to women treated with montelukast could be attributed to severity/control of the maternal asthma [102,103].
Oral administration of CysLT1 receptor antagonists provides a single therapeutic approach to allergic rhinitis and asthma. In asthmatic patients with allergic rhinitis, a combined treatment approach that includes montelukast and budesonide is more effective in reducing airflow obstruction compared with doubling the dose of budesonide, indicating that this strategy increases therapeutic efficacy potentially reducing the number of side effects of inhaled glucocorticoids [104].
7. Conclusions
Most of our knowledge of the pathophysiological role of LTs in asthma is currently limited to CysLT1 receptor-mediated effects, whereas the role of the CysLT2 receptor is largely unknown. The identification of responders to CysLT1 receptor antagonists might be relevant for a more rational therapy of patients with asthma. In responders, CysLT1 receptor antagonists provide a therapeutic alternative to inhaled glucocorticoids in patients with persistent mild asthma. However, CysLT1 receptor antagonists are generally less effective than inhaled glucocorticoids. In patients with more severe asthma who respond to CysLT1 receptor antagonists, the addition of these drugs to inhaled glucocorticoids improves asthma control and enables the dose of inhaled glucocorticoids to be reduced while maintaining similar efficacy. The potential effect of CysLT1 receptor antagonists in preventing and reversing structural changes that characterize airway remodeling, as well as the role of LTB4 in asthma, requires further study.
Ackowledgements
This work was supported by the Catholic University of the Sacred Heart, Academic Grant 2009–2010.
References
- Peters-Golden, M.; Henderson, W.R. Leukotrienes. N. Engl. J. Med. 2007, 357, 1841–1854. [Google Scholar]
- Montuschi, P.; Sala, A.; Dahlén, S.-E.; Folco, G. Pharmacological modulation of the leukotriene pathway in allergic airway disease. Drug Discov. Today 2007, 12, 404–412. [Google Scholar]
- Dahlen, S.E. Treatment of asthma with antileukotrienes: First line or last resort therapy? Eur. J. Pharmacol. 2006, 533, 40–56. [Google Scholar] [CrossRef] [PubMed]
- Busse, W.; Kraft, M. Cysteinyl leukotrienes in allergic inflammation: Strategic target for therapy. Chest 2005, 127, 1312–1326. [Google Scholar]
- Folco, G.; Murphy, R.C. Eicosanoid transcellular biosynthesis: From cell-cell interactions to in vivo tissue responses. Pharmacol. Rev. 2006, 58, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hallstrand, T.S.; Henderson, W.R., Jr. An update on the role of leukotrienes in asthma. Curr. Opin. Allergy Clin. Immunol. 2010, 10, 60–66. [Google Scholar]
- Wenzel, S.E.; Trudeau, J.B.; Kaminsky, D.A.; Cohn, J.; Martin, R.J.; Wescott, J.Y. Effect of 5-lipoxygenase inhibition on bronchoconstriction and airway inflammation in nocturnal asthma. Am. J. Respir. Crit. Care Med. 1995, 152, 897–905. [Google Scholar]
- Aggarwal, S.; Moodley, Y.P.; Thompson, P.J.; Misso, N.L. Prostaglandin E2 and cysteinyl leukotriene concentrations in sputum: Association with asthma severity and eosinophilic inflammation. Clin. Exp. Allergy 2010, 40, 85–93. [Google Scholar]
- Montuschi, P.; Mondino, C.; Koch, P.; Barnes, P.J.; Ciabattoni, G. Effect of a leukotriene receptor antagonist on exhaled leukotriene E4 and prostanoids in asthmatic children. J. Allergy Clin. Immunol. 2006, 118, 347–353. [Google Scholar]
- Mondino, C.; Ciabattoni, G.; Koch, P.; Pistelli, R.; Trové, A.; Barnes, P.J.; Montuschi, P. Effects of inhaled corticosteroids on exhaled leukotrienes and prostanoids in asthmatic children. J. Allergy Clin. Immunol. 2004, 114, 761–767. [Google Scholar]
- Holgate, S.T.; Peters-Golden, M.; Panettieri, R.A.; Henderson, W.R. Roles of cysteinyl leukotrienes in airway inflammation, smooth muscle function, and remodeling. J. Allergy Clin. Immunol. 2003, 111, S18–S36. [Google Scholar] [PubMed]
- Mehrotra, A.K.; Henderson, W.R., Jr. The role of leukotrienes in airway remodeling. Curr. Mol. Med. 2009, 9, 383–391. [Google Scholar]
- Lynch, K.R.; O'Neill, G.P.; Liu, Q.; Im, D.S.; Sawyer, N.; Metters, K.M.; Coulombe, N.; Abramovitz, M.; Figueroa, D.J.; Zeng, Z.; Connolly, B.M.; Bai, C.; Austin, C.P.; Chateauneuf, A.; Stocco, R.; Greig, G.M.; Kargman, S.; Hooks, S.B.; Hosfield, E.; Williams, D.L., Jr.; Ford-Hutchinson, A.W.; Caskey, C.T.; Evans, J.F. Characterization of the human cysteinyl leukotriene CysLT1 receptor. Nature 1999, 399, 789–793. [Google Scholar] [PubMed]
- Mellor, E.A.; Frank, N.; Soler, D.; Hodge, M.R.; Lora, J.M.; Austen, K.F.; Boyce, J.A. Expression of the type 2 receptor for cysteinyl leukotrienes (CysLT2R) by human mast cells: Functional distinction from CysLT1R. Proc. Natl. Acad. Sci. USA 2003, 100, 11589–11593. [Google Scholar]
- Figueroa, D.J.; Breyer, R.M.; Defoe, S.K.; Kargman, S.; Daugherty, B.L.; Waldburger, K.; Liu, Q.; Clements, M.; Zeng, Z.; O'Neill, G.P.; Jones, T.R.; Lynch, K.R.; Austin, C.P.; Evans, J.F. Expression of the cysteinyl leukotriene 1 receptor in normal human lung and peripheral blood leukocytes. Am. J. Resp. Crit. Care Med. 2001, 163, 226–233. [Google Scholar]
- Leigh, R.; Vethanayagam, D.; Yoshida, M.; Watson, R.M.; Rerecich, T.; Inman, M.D.; O'Byrne, P.M. Effects of montelukast and budesonide on airway responses and airway inflammation in asthma. Am. J. Resp. Crit. Care Med. 2002, 166, 1212–1217. [Google Scholar]
- Leff, J.A.; Busse, W.W.; Pearlman, D.; Bronsky, E.A.; Kemp, J.; Hendeles, L.; Dockhorn, R.; Kundu, S.; Zhang, J.; Seidenberg, B.C.; Reiss, T.F. Montelukast, a leukotriene-receptor antagonist, for the treatment of mild asthma and exercise-induced bronchoconstriction. N. Engl. J. Med. 1998, 339, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Dahlen, S.E.; Malmström, K.; Nizankowska, E.; Dahlén, B.; Kuna, P.; Kowalski, M.; Lumry, W.R.; Picado, C.; Stevenson, D.D.; Bousquet, J.; Pauwels, R.; Holgate, S.T.; Shahane, A.; Zhang, J.; Reiss, T.F.; Szczeklik, A. Improvement of aspirin-intolerant asthma by montelukast, a leukotriene antagonist: A randomized, double-blind, placebo-controlled trial. Am. J. Resp. Crit. Care Med. 2002, 165, 9–14. [Google Scholar]
- Price, D.B.; Hernandez, D.; Magyar, P.; Fiterman, J.; Beeh, K.M.; James, I.G.; Konstantopoulos, S.; Rojas, R.; van Noord, J.A.; Pons, M.; Gilles, L.; Leff, J.A. Randomised controlled trial of montelukast plus inhaled budesonide versus double dose inhaled budesonide in adult patients with asthma. Thorax 2003, 58, 211–216. [Google Scholar] [PubMed]
- Busse, W.; Raphael, G.D.; Galant, S.; Kalberg, C.; Goode-Sellers, S.; Srebro, S.; Edwards, L.; Rickard, K. Low-dose fluticasone propionate compared with montelukast for first-line treatment of persistent asthma: A randomized clinical trial. J. Allergy Clin. Immunol. 2001, 107, 461–468. [Google Scholar]
- Henderson, W.R., Jr.; Chiang, G.K.; Tien, Y.T.; Chi, E.Y. Reversal of allergen-induced airway remodeling by CysLT1 receptor blockade. Am. J. Resp. Crit. Care Med. 2006, 173, 718–728. [Google Scholar]
- Kelly, M.M.; Chakir, J.; Vethanayagam, D.; Boulet, L.P.; Laviolette, M.; Gauldie, J.; O'Byrne, P.M. Montelukast treatment attenuates the increase in myofibroblasts following low-dose allergen challenge. Chest 2006, 130, 741–753. [Google Scholar]
- Wenzel, S.E.; Szefler, S.J.; Leung, D.Y.; Sloan, S.I.; Rex, M.D.; Martin, R.J. Bronchoscopic evaluation of severe asthma. Persistent inflammation associated with high dose glucocorticoids. Am. J. Resp. Crit. Care Med. 1997, 156, 737–743. [Google Scholar]
- Montuschi, P.; Barnes, P.J. Exhaled leukotrienes and prostaglandins in asthma. J. Allergy Clin. Immunol. 2002, 109, 615–620. [Google Scholar]
- Montuschi, P.; Martello, S.; Felli, M.; Mondino, C.; Chiarotti, M. Ion trap liquid chromatography/tandem mass spectrometry analysis of leukotriene B4 in exhaled breath condensate. Rapid Commun. Mass Spectrom. 2004, 18, 2723–2729. [Google Scholar]
- Montuschi, P.; Martello, S.; Felli, M.; Mondino, C.; Chiarotti, C. Liquid chromatography/mass spectrometry analysis of exhaled leukotriene B4 in asthmatic children. Respir. Res. 2005, 6, 119. [Google Scholar]
- Kostikas, K.; Gaga, M.; Papatheodorou, G.; Karamanis, T.; Orphanidou, D.; Loukides, S. Leukotriene B4 in exhaled breath condensate and sputum supernatant in patients with COPD and asthma. Chest 2005, 127, 1553–1559. [Google Scholar]
- Montuschi, P. New Perspectives in Monitoring Lung Inflammation: Analysis of Exhaled Breath Condensate; Montuschi, P., Ed.; CRC Press: Boca Raton, FL, USA, 2005. [Google Scholar]
- Evans, D.J.; Barnes, P.J.; Spaethe, S.M.; van Alstyne, E.L.; Mitchell, M.I.; O'Connor, B.J. Effect of a leukotriene B4 receptor antagonist, LY293111, on allergen-induced responses in asthma. Thorax 1996, 51, 1178–1184. [Google Scholar] [PubMed]
- Rao, N.L.; Riley, J.P; Banie, H.; Xue, X.; Sun, B.; Crawford, S.; Lundeen, K.A.; Yu, F.; Karlsson, L.; Fourie, A.M.; Dunford, P.J. Leukotriene A4 hydrolase inhibition attenuates allergic airway inflammation and hyperresponsiveness. Am. J. Respir. Crit. Care Med. 2010, 181, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Miyahara, N.; Ohnishi, H.; Matsuda, H.; Miyahara, S.; Takeda, K.; Koya, T.; Matsubara, S.; Okamoto, M.; Dakhama, A.; Haribabu, B.; Gelfand, E.W. Leukotriene B4 receptor 1 expression on dendritic cells is required for the development of Th2 responses and allergen-induced airway hyperresponsiveness. J. Immunol. 2008, 181, 1170–1178. [Google Scholar]
- Ohnishi, H.; Miyahara, N.; Dakhama, A.; Takeda, K.; Mathis, S.; Haribabu, B.; Gelfand, E.W. Corticosteroids enhance CD8+ T cell-mediated airway hyperresponsiveness and allergic inflammation by upregulating leukotriene B4 receptor 1. J. Allergy Clin. Immunol. 2008, 121, 864–871. [Google Scholar]
- James, A.J.; Penrose, J.F.; Cazaly, A.M.; Holgate, S.T.; Sampson, A.P. Human bronchial fibroblasts express the 5-lipoxygenase pathway. Resp. Res. 2006, 7, 102. [Google Scholar]
- Maekawa, A.; Kanaoka, Y.; Xing, W.; Austen, K.F. Functional recognition of a distinct receptor preferential for leukotriene E4 in mice lacking the cysteinyl leukotriene 1 and 2 receptors. Proc. Natl. Acad. Sci. USA 2008, 105, 16695–11700. [Google Scholar]
- Maekawa, C.; Balestrieri, B.; Austen, K.F.; Kanaoka, Y. GPR17 is a negative regulator for the cysteinyl leukotriene 1 receptor response to leukotriene D4. Proc. Natl. Acad. Sci. USA 2009, 106, 11685–11690. [Google Scholar]
- Paruchuri, S.; Tashimo, H.; Feng, C.; Maekawa, A.; Xing, W.; Jiang, Y.; Kanaoka, Y.; Conley, P.; Boyce, J.A. Leukotriene E4-induced pulmonary inflammation is mediated by the P2Y12 receptor. J. Exp. Med. 2009, 206, 2543–2555. [Google Scholar]
- Lee, T.H. Leukotriene E4: Perspective on the forgotten mediator. J. Allergy Clin. Immunol. 2009, 124, 417–421. [Google Scholar]
- Ciana, P.; Fumagalli, M.; Trincavelli, M.L.; Verderio, C.; Rosa, P.; Lecca, D.; Ferrario, S.; Parravicini, C.; Capra, V.; Gelosa, P.; Guerrini, U.; Belcredito, S.; Cimino, M.; Sironi, L.; Tremoli, E.; Rovati, G.E.; Martini, C.; Abbracchio, M.P. The orphan receptor GPR17 identified as a new dual uracil nucleotides/cysteinyl-leukotrienes receptor. EMBO J. 2006, 25, 4615–4627. [Google Scholar]
- Gauvreau, G.M.; Plitt, J.R.; Baatjes, A.; MacGlashan, D.W. Expression of functional cysteinyl leukotriene receptors by human basophils. J. Allergy Clin. Immunol. 2005, 116, 80–87. [Google Scholar]
- Di Gennaro, A.; Carnini, C.; Buccellati, C.; Ballerino, R.; Zarini, S.; Fumagalli, F.; Viappiani, S.; Librizzi, L.; Hernandez, A.; Murphy, R.C.; Constantin, G.; De Curtis, M.; Folco, G.; Sala, A. Cysteinyl-leukotrienes receptor activation in brain inflammatory reactions and cerebral edema formation: A role for transcellular biosynthesis of cysteinyl-leukotrienes. FASEB J. 2004, 18, 842–844. [Google Scholar]
- Figueroa, D.J.; Borish, L.; Barami, D.; Philip, G.; Austin, C.P.; Evans, J.F. Expression of cysteinyl leukotriene synthetic and signalling proteins in inflammatory cells in active seasonal allergic rhinitis. Clin. Exp. Allergy 2003, 33, 1380–1388. [Google Scholar]
- Fujii, M.; Tanaka, H.; Abe, S. Interferon-γ up-regulates expression of cysteinyl leukotriene type 2 receptors on eosinophils in asthmatic patients. Chest 2005, 128, 3148–3155. [Google Scholar]
- Naik, S.; Billington, C.K.; Pascual, R.M.; Deshpande, D.A.; Stefano, F.P.; Kohout, T.A.; Eckman, D.M.; Benovic, J.L.; Penn, R.B. Regulation of cysteinyl leukotriene type 1 receptor internalization and signaling. J. Biol. Chem. 2005, 280, 8722–8732. [Google Scholar]
- Yokomizo, T.; Izumi, T.; Chang, K.; Takuwa, Y.; Shimizu, T. A G-protein-coupled receptor for leukotriene B4 that mediates chemotaxis. Nature 1997, 387, 620–624. [Google Scholar]
- Yokomizo, T.; Kato, K.; Terawaki, K.; Izumi, T.; Shimizu, T. A second leukotriene B4 receptor, BLT2. A new therapeutic target in inflammation and immunological disorders. J. Exp. Med. 2000, 192, 421–432. [Google Scholar] [CrossRef]
- Lundeen, K.A.; Sun, B.; Karlsson, L.; Furie, A.M. Leukotriene B4 receptors BLT1and BLT2: Expression and function in human and murine mast cells. J. Immunol. 2006, 177, 339–347. [Google Scholar]
- Gelfand, E.W.; Dakhama, A. CD8+ T lymphocytes and leukotriene B4: novel interactions in the persistence and progression of asthma. J. Allergy Clin. Immunol. 2006, 117, 577–582. [Google Scholar]
- Miyahara, N.; Takeda, K.; Miyahara, S.; Taube, C.; Joetham, A.; Koya, T.; Matsubara, S.; Dakhama, A.; Tager, A.M.; Lustre, A.D.; Gelfand, E.W. Leukotriene B4 receptor-1 is essential for allergen-mediated recruitment of CD8+ T cells and airway hyperresponsiveness. J. Immunol. 2005, 174, 4979–4984. [Google Scholar]
- Diamant, Z.; Hiltermann, J.T.; van Rensen, E.L.; Callenbach, P.M.; Veselic-Charvat, M.; van der Veen, H.; Sont, J.K.; Sterk, P.J. The effect of inhaled leukotriene D4 and methacholine on sputum cell differentials in asthma. Am. J. Resp. Crit. Care Med. 1997, 155, 1247–1253. [Google Scholar]
- Peters-Golden, M. Expanding roles for leukotrienes in airway inflammation. Curr. Allergy Asthma Rep. 2008, 8, 367–373. [Google Scholar]
- Kim, D.C.; Hsu, F.I.; Barrett, N.A.; Friend, D.S.; Grenningloh, R.; Ho, I.C.; Al-Garawi, A.; Lora, J.M.; Lam, B.K.; Austen, K.F.; Kanaoka, Y. Cysteinyl leukotrienes regulate Th2 cell-dependent pulmonary inflammation. J. Immunol. 2006, 176, 4440–4448. [Google Scholar]
- Sampson, A.P.; Castling, D.P.; Green, C.P.; Price, J.F. Persistent increase in plasma and urinary leukotrienes after acute asthma. Arch. Dis. Chil. 1995, 73, 221–225. [Google Scholar]
- Fourie, A.M. Modulation of inflammatory disease by inhibitors of leukotriene A4 hydrolase. Curr. Opin. Invest. Drugs 2009, 10, 1173–1182. [Google Scholar]
- Dahlen, B.; Nizankowska, E.; Szczeklik, A.; Zetterström, O.; Bochenek, G.; Kumlin, M.; Mastalerz, L.; Pinis, G.; Swanson, L.J.; Boodhoo, T.I.; Wright, S.; Dubé, L.M.; Dahlén, S.E. Benefits from adding the 5-lipoxygenase inhibitor zileuton to conventional therapy in aspirin-intolerant asthmatics. Am. J. Resp. Crit. Care Med. 1998, 157, 1187–1194. [Google Scholar]
- Fischer, A.R.; McFadden, C.A.; Frantz, R.; Awni, W.M.; Cohn, J.; Drazen, J.M.; Israel, E. Effect of chronic 5-lipoxygenase inhibition on airway hyperresponsiveness in asthmatic subjects. Am. J. Resp. Crit. Care Med. 1995, 152, 1203–1207. [Google Scholar]
- Riccioni, G.; Vecchia, R.D.; D'Orazio, N.; Sensi, S.; Guagnano, M.T. Comparison of montelukast and budesonide on bronchial reactivity in subjects with mild-moderate persistent asthma. Pulm. Pharmacol. Ther. 2003, 16, 111–114. [Google Scholar]
- Berges-Gimeno, M.P.; Simon, R.A.; Stevenson, D.D. The effect of leukotriene-modifier drugs on aspirin-induced asthma and rhinitis reactions. Clin. Exp. Allergy 2002, 32, 1491–1496. [Google Scholar]
- Laitinen, L.A.; Laitinen, A.; Haahtela, T.; Vilkka, V.; Spur, B.W.; Lee, T.H. Leukotriene E4 and granulocytic infiltration into asthmatic airways. Lancet 1993, 341, 989–990. [Google Scholar]
- Gauvreau, G.M.; Parameswaran, K.N.; Watson, R.M.; O'Byrne, P.M. Inhaled leukotriene E4, but not leukotriene D4, increased airway inflammatory cells in subjects with aopic asthma. Am. J. Respir. Crit. Care Med. 2001, 164, 1495–1500. [Google Scholar] [PubMed]
- O'Hickey, S.P.; Arm, J.P.; Rees, P.J.; Spur, B.W.; Lee, T.H. The relative responsiveness to inhaled leukotriene E4, methacholine and histamine in normal and asthmatic subjects. Eur. Respir. J. 1988, 1, 913–917. [Google Scholar] [PubMed]
- Antczak, A.; Montuschi, P.; Kharitonov, S.; Gorski, P.; Barnes, P.J. Increased exhaled cysteinyl leukotrienes and 8-isoprostane in aspirin-induced asthma. Am. J. Respir. Crit. Care Med. 2002, 166, 301–306. [Google Scholar]
- Zanconato, S.; Carraro, S.; Corradi, M.; Alinovi, R.; Pasquale, M.F.; Piacentini, G.; Zacchello, F.; Baraldi, E. Leukotrienes and 8-isoprostane in exhaled breath condensate of children with stable and unstable asthma. J. Allergy Clin. Immunol. 2004, 113, 257–263. [Google Scholar]
- Katsunuma, T.; Tomikawa, M.; Tan, A.; Yuki, K.; Akashi, K.; Eto, Y. Increased leukotriene E4 in the exhaled breath condensate of children with mild asthma. Chest 2006, 130, 1718–1722. [Google Scholar]
- Csoma, Z.; Kharitonov, S.A.; Balint, B.; Bush, A.; Wilson, N.M.; Barnes, P.J. Increased leukotrienes in exhaled breath condensate in childhood asthma. Am. J. Respir. Crit. Care Med. 2002, 166, 1345–1349. [Google Scholar]
- Pavord, I.D.; Ward, R.; Woltmann, G.; Wardlaw, A.J.; Sheller, J.R.; Dworski, R. Induced sputum eicosanoid concentrations in asthma. Am. J. Resp. Crit. Care Med. 1999, 160, 1905–1909. [Google Scholar]
- Kumlin, M. Measurement of leukotrienes in humans. Am. J. Resp. Crit. Care Med. 2000, 161, S102–S106. [Google Scholar]
- Higashi, N.; Taniguchi, M.; Mita, H.; Kawagishi, Y.; Ishii, T.; Higashi, A.; Osame, M.; Akiyama, K. Clinical features of asthmatic patients with increased urinary leukotriene E4 excretion (hyperleukotrienuria): Involvement of chronic hyperplastic rhinosinusitis with nasal polyposis. J. Allergy Clin. Immunol. 2004, 113, 277–283. [Google Scholar]
- Green, S.A.; Malice, M.P.; Tanaka, W.; Tozzi, C.A.; Reiss, T.F. Increase in urinary leukotriene LTE4 levels in acute asthma: correlation with airflow limitation. Thorax 2004, 59, 100–104. [Google Scholar]
- Horvath, I.; Hunt, J.; Barnes, P.J.; Alving, K.; Antczak, A.; Baraldi, E.; Becher, G.; van Beurden, W.J.; Corradi, M.; Dekhuijzen, R.; Dweik, R.A.; Dwyer, T.; Effros, R.; Erzurum, S.; Gaston, B.; Gessner, C.; Greening, A.; Ho, L.P.; Hohlfeld, J.; Jöbsis, Q.; Laskowski, D.; Loukides, S.; Marlin, D.; Montuschi, P.; Olin, A.C.; Redington, A.E.; Reinhold, P.; van Rensen, E.L.; Rubinstein, I.; Silkoff, P.; Toren, K.; Vass, G.; Vogelberg, C.; Wirtz, H. ATS/ERS Task Force on exhaled breath condensate. Exhaled breath condensate: Methodological recommendations and unresolved questions. Eur. Resp. J. 2005, 26, 523–548. [Google Scholar]
- Montuschi, P. Analysis of exhaled breath condensate in respiratory medicine: Methodological aspects and potential clinical applications. Ther. Adv. Respir. Dis. 2007, 1, 5–23. [Google Scholar]
- Abraham, B.; Antó, J.M.; Barreiro, E.; Bel, E.H.D.; Bousquet, J.; Castellsagud, J.; Chanez, P.; Dahién, B.; Dahién, S.E.; Dews, Ń.; Djukanovic, R.; Fabbri, L.M.; Folkerts, G.; Gaga, M.; Gratziou, C.; Holgate, S.T.; Howarth, P.H.; Johnston, S.L.; Kanniess, F. The ENFUMOSA cross-sectional European multicentre study of the clinical phenotype of chronic severe asthma. Eur. Resp. J. 2003, 22, 470–477. [Google Scholar]
- Camargo, C.A., Jr.; Smithline, H.A.; Malice, M.P.; Green, S.A.; Reiss, T.F. A randomized controlled trial of intravenous montelukast in acute asthma. Am. J. Resp. Crit. Care Med. 2003, 167, 528–533. [Google Scholar]
- Camargo, C.A., Jr.; Gurner, D.M.; Smithline, H.A.; Chapela, R.; Fabbri, L.M.; Green, S.A.; Malice, M.P.; Legrand, C.; Dass, S.B.; Knorr, B.A.; Reiss, T.F. A randomized placebo-controlled study of intravenous montelukast for the treatment of acute asthma. J. Allergy Clin. Immunol. 2010, 125, 374–380. [Google Scholar]
- Roquet, A.; Dahlén, B.; Kumlin, M.; Ihre, E.; Anstrén, G.; Binks, S.; Dahlén, S.E. Combined antagonism of leukotrienes and histamine produces predominant inhibition of allergen-induced early and late phase airway obstruction in asthmatics. Am. J. Resp. Crit. Care Med. 1997, 155, 1856–1863. [Google Scholar]
- Phipatanakul, W.; Nowak-Wegrzyn, A.; Eggleston, P.A.; Van Natta, M.; Kesavan, J.; Schuberth, K.; Wood, R.A. The efficacy of montelukast in the treatment of cat allergen-induced asthma in children. J. Allergy Clin. Immunol. 2002, 109, 794–799. [Google Scholar]
- Pearlman, D.S.; van Adelsberg, J.; Philip, G.; Tilles, S.A.; Busse, W.; Hendeles, L.; Loeys, T.; Dass, S.B.; Reiss, T.F. Onset and duration of protection against exercise-induced bronchoconstriction by a single oral dose of montelukast. Ann. Allergy Asthma Immunol. 2006, 97, 98–104. [Google Scholar]
- Philip, G.; Pearlman, D.S.; Villarán, C.; Legrand, C.; Loeys, T.; Langdon, R.B.; Reiss, T.F. Single-dose montelukast or salmeterol as protection against exercise-induced bronchoconstriction. Chest 2007, 132, 875–883. [Google Scholar]
- Villaran, C.; O'Neill, S.J.; Helbling, A.; van Noord, J.A.; Lee, T.H.; Chuchalin, A.G.; Langley, S.J.; Gunawardena, K.A.; Suskovic, S.; Laurenzi, M.; Jasan, J.; Menten, J.; Leff, J.A. Montelukast versus salmeterol in patients with asthma and exercise-induced bronchoconstriction. Montelukast/salmeterol exercise study group. J. Allergy Clin. Immunol. 1999, 104, 547–553. [Google Scholar] [PubMed]
- Melo, R.E.; Solé, D.; Naspitz, C.K. Exercise-induced bronchoconstriction in children: Montelukast attenuates the immediate-phase and late-phase responses. J. Allergy Clin. Immunol. 2003, 111, 301–307. [Google Scholar]
- FitzGerald, J.M.; Shahidi, N. Achieving asthma control in patients with moderate disease. J. Allergy Clin. Immunol. 2010, 125, 307–311. [Google Scholar]
- National Asthma Education and Prevention Program. Expert Panel Report (EPR-3): Guidelines for the Diagnosis and Management of Asthma-Summary Report 2007. J. Allergy Clin. Immunol. 2007, 120, S94–S138. [CrossRef] [PubMed]
- Szefler, S.J.; Phillips, B.R.; Martinez, F.D.; Chinchilli, V.M.; Lemanske, R.F.; Strunk, R.C.; Geiger, R.S.; Larsen, G.; Spahn, J.D.; Bacharier, L.B.; Bloomberg, G.R.; Guilbert, T.W.; Heldt, G.; Morgan, W.J.; Moss, M.H.; Sorkness, C.A.; Taussig, L.M. Characterization of within-subject responses to fluticasone and montelukast in childhood asthma. J. Allergy Clin. Immunol. 2005, 115, 233–242. [Google Scholar]
- Vaquerizo, M.J.; Casan, P.; Castello, J.; Perpiña, M.; Sanchis, J.; Sobradillo, V.; Valencia, A.; Verea, H.; Viejo, J.L.; Villasante, C.; Gonzalez-Esteban, J.; Picado, C. Effect of montelukast added to inhaled budesonide on control of mild to moderate asthma. Thorax 2003, 58, 204–210. [Google Scholar]
- Bjermer, L.; Bisgaard, H.; Bousquet, J.; Fabbri, L.M.; Greening, A.P.; Haahtela, T.; Holgate, S.T.; Picado, C.; Menten, J.; Dass, S.B.; Leff, J.A.; Polos, P.G. Montelukast and fluticasone compared with salmeterol and fluticasone in protecting against asthma exacerbation in adults: One year, double blind, randomised, comparative trial. BMJ 2003, 327, 891. [Google Scholar] [PubMed]
- Ducharme, F.M.; Lasserson, T.J.; Cates, C.J. Addition of long-acting β2-agonists vs. anti-leukotrienes as add-on therapy to inhaled corticosteroids for chronic asthma. Cochrane Database Syst. Rev. 2006, (4), CD003137. [Google Scholar]
- Lemanske, R.F., Jr.; Mauger, D.T.; Sorkness, C.A.; Jackson, D.J.; Boehmer, S.J.; Martinez, F.D.; Strunk, R.C.; Szefler, S.J.; Zeiger, R.S.; Bacharier, L.B.; Covar, R.A.; Guilbert, T.W.; Larsen, G.; Morgan, W.J.; Moss, M.H.; Spahn, J.D.; Taussig, L.M. Childhood Asthma Research and Education (CARE) Network of the National Heart, Lung, and Blood Institute. Step-up therapy for children with uncontrolled asthma receiving inhaled corticosteroids. N. Engl. J. Med. 2010, 362, 975–985. [Google Scholar] [PubMed]
- Ohbayashi, H.; Shibata, N.; Hirose, T.; Adachi, M. Additional effects of pranlukast in salmeterol/fluticasone combination therapy for the asthmatic distal airway in a randomized crossover study. Pulm. Pharmacol. Ther. 2009, 22, 574–579. [Google Scholar]
- Tomari, S.; Matsuse, H.; Hirose, H.; Tsuchida, T.; Fukahori, S.; Fukushima, C.; Kawano, T.; Matsuo, N.; Kohno, S. Observational study of the additive effects of pranlukast on inflammatory markers of clinically stable asthma with inhaled corticosteroids and long-acting beta 2 agonists. Respiration 2008, 76, 398–402. [Google Scholar]
- Montuschi, P.; Mondino, C.; Koch, P.; Ciabattoni, G.; Barnes, P.J.; Baviera, G. Effects of montelukast treatment and withdrawal on fractional exhaled nitric oxide and lung function in children with asthma. Chest 2007, 132, 1876–1881. [Google Scholar]
- Lofdahl, C.G.; Reiss, T.F.; Leff, J.A.; Israel, E.; Noonan, M.J.; Finn, A.F.; Seidenberg, B.C.; Capizzi, T.; Kundu, S.; Godard, P. Randomised, placebo controlled trial of effect of a leukotriene receptor antagonist, montelukast, on tapering inhaled corticosteroids in asthmatic patients. BMJ 1999, 319, 87–90. [Google Scholar] [PubMed]
- Gyllfors, P.; Dahlén, S.E.; Kumlin, M.; Larsson, K.; Dahlén, B. Bronchial responsiveness to leukotriene D4 is resistant to inhaled fluticasone propionate. J. Allergy Clin. Immunol. 2006, 118, 78–83. [Google Scholar]
- Szefler, S.J.; Martin, R.J. Lessons learned from variation in response to therapy in clinical trials. J. Allergy Clin. Immunol. 2010, 125, 285–292. [Google Scholar]
- Malmstrom, K.; Rodriguez-Gomez, G.; Guerra, J.; Villaran, C.; Pineiro, A.; Wei, L.X.; Seidenberg, B.C.; Reiss, T.F. Oral montelukast, inhaled beclomethasone, and placebo for chronic asthma. Ann. Intern. Med. 1999, 130, 487–495. [Google Scholar]
- Lima, J.J.; Zhang, S.; Grant, A.; Shao, L.; Tantisira, K.G.; Allayee, H.; Wang, J.; Sylvester, J.; Holbrook, J.; Wise, R.; Weiss, S.T.; Barnes, K. Influence of leukotriene pathway polymorphisms on response to montelukast in asthma. Am. J. Respir. Crit. Care Med. 2006, 173, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Ward, C.; Pais, M.; Bish, R.; Reid, D.; Feltis, B.; Johns, D.; Walter, H. Airway inflammation, basement membrane thickening and bronchial hyperresponsiveness in asthma. Thorax 2002, 57, 309–316. [Google Scholar]
- Hoshino, M.; Takahashi, M.; Takai, Y.; Sim, J. Inhaled corticosteroids decrease subepithelial collagen deposition by modulation of the balance between matrix metalloproteinase-9 and tissue inhibitor of metalloproteinase-1 expression in asthma. J. Allergy Clin. Immunol. 1999, 103, 1054–1061. [Google Scholar]
- Bisgaard, H.; Hermansen, M.N.; Loland, L.; Halkjaer, L.B.; Buchvald, F. Intermittent inhaled corticosteroids in infants with episodic wheezing. N. Engl. J. Med. 2006, 354, 1998–2005. [Google Scholar]
- Bibby, S.; Healy, B.; Steele, R.; Kumareswaran, K.; Nelson, H.; Beasley, R. Association between leukotriene receptor antagonist therapy and Churg-Strauss syndrome: An analysis of the FDA AERS database. Thorax 2010, 65, 132–138. [Google Scholar]
- Philip, G.; Hustad, C.; Noonan, G.; Malice, M.P.; Ezekowitz, A.; Reiss, T.F.; Knorr, B. Reports of suicidality in clinical trials of montelukast. J. Allergy Clin. Immunol. 2009, 124, 691–696. [Google Scholar]
- Manalai, P.; Woo, J.M.; Postolache, T.T. Suicidality and montelukast. Expert. Opin. Drug Saf. 2009, 8, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, J.T.; Harik-Khan, R. Montelukast and emotional well-being as a marker for depression: results from 3 randomized, double-masked clinical trials. J. Allergy Clin. Immunol. 2008, 122, 828–829. [Google Scholar]
- Sarkar, M.; Koren, G.; Kalra, S.; Ying, A.; Smorlesi, C.; De Santis, M.; Diav-Citrin, O.; Avgil, M.; Voyer Lavigne, S.; Berkovich, M.; Einarson, A. Montelukast use during pregnancy: A multicentre, prospective, comparative study of infant outcomes. Eur. J. Clin. Pharmacol. 2009, 65, 1259–1264. [Google Scholar] [CrossRef] [PubMed]
- Bakhireva, L.N.; Jones, K.L.; Schatz, M.; Klonoff-Cohen, H.S.; Johnson, D.; Slymen, D.J.; Chambers, C.D. Organization of Teratology Information Specialists Collaborative Research Group. Safety of leukotriene receptor antagonists in pregnancy. J. Allergy Clin. Immunol. 2007, 119, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Price, D.B.; Swern, A.; Tozzi, C.A.; Philip, G.; Polos, P. Effect of montelukast on lung function in asthma patients with allergic rhinitis: analysis from the COMPACT trial. Allergy 2006, 61, 737–742. [Google Scholar] [CrossRef] [PubMed]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an Open Access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
MDPI and ACS Style
Montuschi, P. Role of Leukotrienes and Leukotriene Modifiers in Asthma. Pharmaceuticals 2010, 3, 1792-1811. https://doi.org/10.3390/ph3061792
AMA Style
Montuschi P. Role of Leukotrienes and Leukotriene Modifiers in Asthma. Pharmaceuticals. 2010; 3(6):1792-1811. https://doi.org/10.3390/ph3061792
Chicago/Turabian StyleMontuschi, Paolo. 2010. "Role of Leukotrienes and Leukotriene Modifiers in Asthma" Pharmaceuticals 3, no. 6: 1792-1811. https://doi.org/10.3390/ph3061792