The Use of Positron Emission Tomography in Soft Tissue Sarcoma Patients under Therapy with Trabectedin


Abstract
:Background
Patients and Methods
Results
Conclusion
1. Introduction
2. Patients and Methods
Patients
Ecteinascidin-743
Imaging studies
Statistical analysis
3. Results and Discussion
Clinical response based on RECIST criteria
Clinical response based on PET imaging
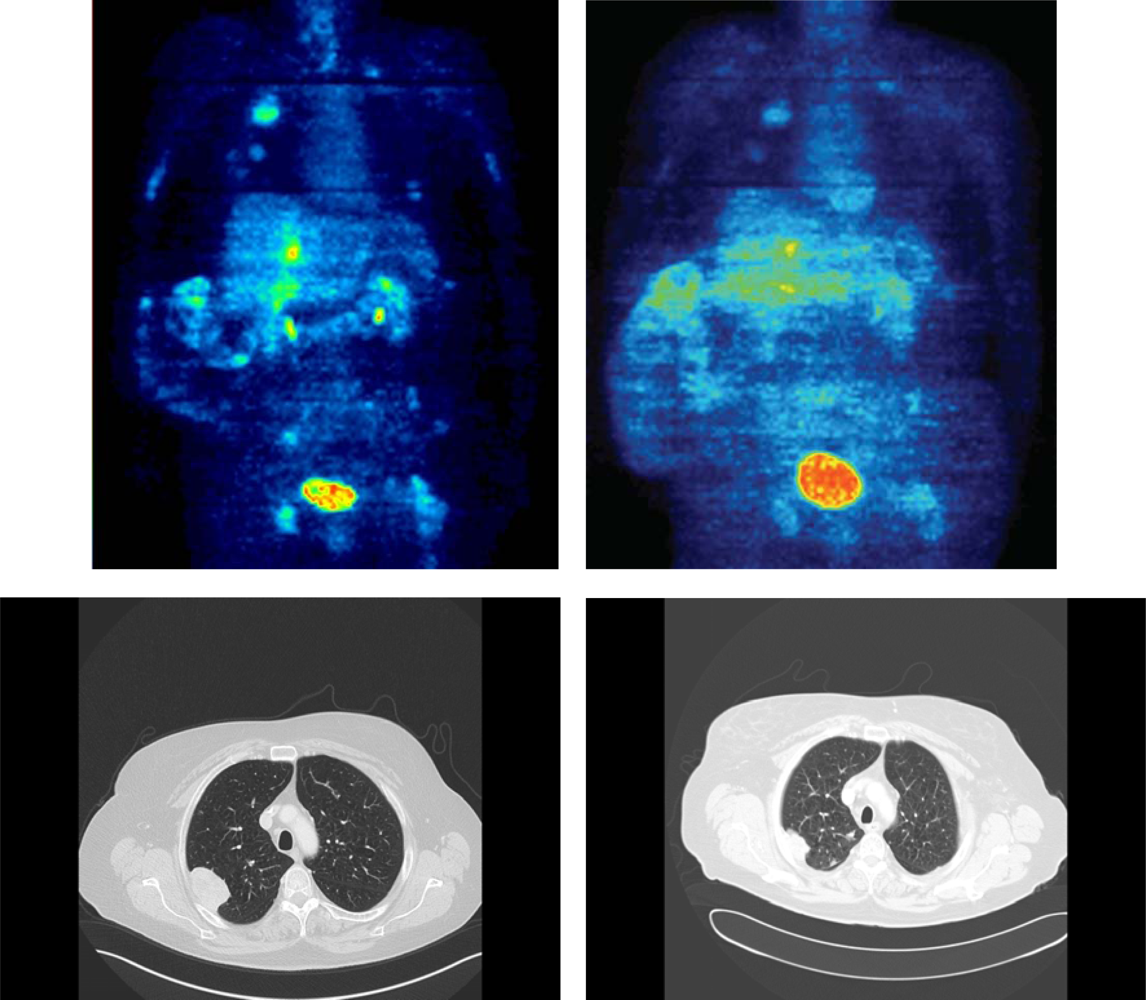
Example
Discussion
4. Conclusions
References
- Pisters, P. Pollock, RE, Ed.; Staging and Prognosis. In American Cancer Society Atlas of Clinical Oncology: Soft Tissue Sar comas; BC Decker, Inc: Hamilton, ON, Canada, 2002; pp. 80–88. [Google Scholar]
- Standard-Options-Recommandations. In Sarcome des T issus Mous et Ostéosarcomes; Arnette Blackwell: Paris, France, 1995; Volume 1, pp. 1–113.
- Verweij, J; Mouridsen, HT; Nielsen, OS; Woll, PJ; Somers, R; van Oosterom, AT; van Glabbeke, M; Tursz, T. The present state of the art in chemotherapy for soft tissue sarcomas in adults: The EORTC point of view. Crit Rev Oncol Hematol 1995, 20, 193–201. [Google Scholar]
- Frustaci, S; de Paoli, A; Bidoli, E. Ifosfamide in the adjuvant therapy of soft tissue sarcomas. Oncology 2003, 65, 80–84. [Google Scholar]
- Grobmyer, SR; Maki, RG; Demetri, GD; Mazumdar, M; Riedel, E; Brennan, MF; Singer, S. Neo-adjuvant chemotherapy for primary high-grade extremity soft tissue sarcoma. Ann Oncol 2004, 15, 1667–1672. [Google Scholar]
- Pisters, PW; Patel, SR; Varma, DG; Cheng, SC; Chen, NP; Nguyen, HT; Feig, BW; Pollack, A; Pollock, RE; Benjamin, RS. Preoperative chemotherapy for stage IIIB extremity soft tissue sarcoma: long-term results from a single institution. J Clin Oncol 1997, 15, 3481–3487. [Google Scholar]
- Wendtner, CM; Abdel-Rahman, S; Krych, M; Baumert, J; Lindner, LH; Baur, A; Hiddemann, W; Issels, RD. Response to neoadjuvant chemotherapy combined with regional hyperthermia predicts long-term survival for adult patients with retroperitoneal and visceral high-risk soft tissue sarcomas. J Clin Oncol 2002, 20, 3156–3164. [Google Scholar]
- Strauss, LG; Conti, PS. The applications of PET in clinical oncology. J Nucl Med 1991, 32, 623–648. [Google Scholar]
- Schulte, M; Brecht-Krauss, D; Heymer, B; Guhlmann, A; Hartwig, G; Sarkar, MR; Diederichs, CG; Schultheiss, M; Kotzerke, J; Reske, SN. Fluorodeoxyglucose positron emission tomography of soft tissue tumors: is a non-invasive determination of biological activity possible? Eur J Nucl Med 1999, 26, 599–605. [Google Scholar]
- Schwarzbach, M; Dimitrakopoulou-Strauss, A; Willeke, F; Hinz, U; Strauss, LG; Zhang, YM; Mechtersheimer, G; Attigah, N; Lehnert, T; Herfarth, C. Clinical value of [18F]fluorodeoxyglucose positron emission tomography imaging in soft tissue sarcomas. Ann Surg 2000, 231, 380–386. [Google Scholar]
- Eary, JF; Mankoff, DA. Tumor metabolic rates in sarcoma using FDG PET. J Nucl Med 1998, 39, 250–254. [Google Scholar]
- Schelling, M; Avril, N; Nahrig, J; Kuhn, W; Romer, W; Sattler, D; Werner, M; Dose, J; Janicke, F; Graeff, H; Schwaiger, M. Positron emission tomography using [18F]fluorodeoxyglucose for monitoring primary chemotherapy in breast cancer. J Clin Oncol 2000, 18, 1689–1695. [Google Scholar]
- Gretschel, S; Moesta, KT; Hünerbein, M; Lange, T; Gebauer, B; Stroszczinsk, C; Bembenek, A; Schlag, PM. New concepts of staging in gastrointestinal tumors as a basis of diagnosis and multimodal therapy. Onkologie 2004, 27, 23–30. [Google Scholar]
- Dimitrakopoulou-Strauss, A; Strauss, LG; Burger, C; Ruhl, A; Irngartinger, G; Stremmel, W; Rudi, J. Prognostic aspects of 18F-FDG PET kinetics in patients with metastatic colorectal carcinoma receiving FOLFOX chemotherapy. J Nucl Med 2004, 45, 1480–1487. [Google Scholar]
- Stroobants, S; Goeminne, J; Seegers, M; Dimitrijevic, S; Dupont, P; Nuyts, J; Martens, M; van den Borne, B; Cole, P; Sciot, R; Dumez, H; Silberman, S; Mortelmans, L; van Oosterom, A. 18FDG-Positron emission tomography for the early prediction of response in advanced soft tissue sarcoma treated with imatinib mesylate (Glivec). Eur J Cancer 2003, 39, 2012–2020. [Google Scholar]
- Schuetze, SM; Rubin, BP; Vernon, C; Hawkins, DS; Bruckner, JD; Conrad, EU, 3rd; Eary, JF. Use of positron emission tomography in localized extremity soft tissue sarcoma treated with neoadjuvant chemotherapy. Cancer 2005, 103, 339–348. [Google Scholar]
- Schuetze, SM. Utility of positron emission tomography in sarcomas. Curr Opin Oncol 2006, 18, 369–373. [Google Scholar]
- Verweij, J. Ecteinascidin-743 (ET-743): Early test or effective treatment in soft tissue sarcomas? J Clin Oncol 2005, 24, 5420–5423. [Google Scholar]
- Fayette, J; Coquard, IR; Alberti, L; Ranchère, D; Boyle, H; Blay, JY. ET-743: A novel agent with activity in soft-tissue sarcomas. Curr Opin Oncol 2006, 18, 347–353. [Google Scholar]
- Grosso, F; Forni, C; Frapolli, R; Greco, A; Gronchi, A; Jimeno, J; Mantovani, R; D'Incalci, M; Pilotti, S; Casali, PG. Sensitivity of myxoid-round cell liposarcoma (MRCL) to trabectedin (T) may be related to a direct effect on the fusion transcript. Proc Am Soc Clin Oncol 2007, 25, 18S, (abstract 10000). [Google Scholar]
- Ryan, DP; Supko, JG; Eder, JP; Seiden, MV; Demetri, G; Lynch, TJ; Fischman, AJ; Davis, J; Jimeno, J; Clark, JW. Phase I and pharmacokinetic study of ecteinascidin 743 administerd as a 72-hour continuous intravenous infusion in patients with solid malignancies. Clin Cancer Res 2001, 7, 231–242. [Google Scholar]
- Trojani, M; Contesso, G; Coindre, JM; Rouesse, J; Bui, NB; de Mascarel, A; Goussot, JF; David, M; Bonichon, F; Lagarde, C. Soft-tissue sarcomas of adults; study of pathological prognostic variables and definition of a histopathological grading system. Int J Cancer 1984, 33, 37–42. [Google Scholar]
- Schwarzbach, MH; Hinz, U; Dimitrakopoulou-Strauss, A; Willeke, F; Cardona, S; Mechtersheimer, G; Lehnert, T; Strauss, LG; Herfarth, C; Buchler, MW. Prognostic significance of preoperative [18-F] fluorodeoxyglucose (FDG) positron emission tomography (PET) imaging in patients with resectable soft tissue sarcomas. Ann Surg 2005, 241, 286–294. [Google Scholar]
- Burger, C; Buck, A. Requirements and implementation of a flexible kinetic modelling tool. J Nucl Med 1997, 38, 1818–1823. [Google Scholar]
- Cheng, EY; Froelich, JW; Manivel, JC; Weigel, BJ; Skubitz, KM. Correlation of FDG-PET with histologic response after neoadjuvant chemotherapy for soft tissue sarcomas. Proc Am Soc Clin Oncol 2009, 25, 18S, (abstract 10583). [Google Scholar]
- Dimitrakopoulou-Strauss, A; Strauss, LG; Schwarzbach, M; Burger, C; Heichel, T; Willeke, F; Mechtersheimer, G; Lehnert, T. Dynamic PET 18F-FDG studies in patients with primary and recurrent soft tissue sarcomas: impact on diagnosis and correlation with grading. J Nucl Med 2001, 42, 713–720. [Google Scholar]
- Jager, PL; Gietema, JA; van der Graaf, WT. Imatinib mesylate for the treatment of gastrointestinal stromal tumours: best monitored with FDG PET. Nucl Med Commun 2004, 25, 433–438. [Google Scholar]
- Kasper, B; Dietrich, S; Dimitrakopoulou-Strauss, A; Strauss, LG; Haberkorn, U; Ho, AD; Egerer, G. Early prediction of therapy outcome in patients with high risk soft tissue sarcoma using positron emission tomography. Onkologie 2008, 31, 107–112. [Google Scholar]


{kind=link}
| Gender | ||
| Female | 6 | |
| Male | 3 | |
| Age | ||
| Median (years) | 52 [range: 26–73] | |
| Histology | ||
| Synovial sarcoma | 2 | |
| Leiomyosarcoma | 7 | |
| Grading | ||
| II | 2 | |
| III | 7 | |
| Tumour site at initial diagnosis | ||
| None | 1 | |
| Extremities | 3 | |
| Trunk | 5 | |
| Metastatic sites | ||
| Lung | 8 | |
| Liver | 3 | |
| Lymph nodes | 3 | |
| Soft tissue | 2 | |
| Line of Treatment | ||
| 2nd line | 4 | |
| 3rd line or more | 5 | |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kasper, B.; Schmitt, T.; Wuchter, P.; Dimitrakopoulou-Strauss, A.; Ho, A.D.; Egerer, G. The Use of Positron Emission Tomography in Soft Tissue Sarcoma Patients under Therapy with Trabectedin. Mar. Drugs 2009, 7, 331-340. https://doi.org/10.3390/md7030331
Kasper B, Schmitt T, Wuchter P, Dimitrakopoulou-Strauss A, Ho AD, Egerer G. The Use of Positron Emission Tomography in Soft Tissue Sarcoma Patients under Therapy with Trabectedin. Marine Drugs. 2009; 7(3):331-340. https://doi.org/10.3390/md7030331
Chicago/Turabian StyleKasper, Bernd, Thomas Schmitt, Patrick Wuchter, Antonia Dimitrakopoulou-Strauss, Anthony D. Ho, and Gerlinde Egerer. 2009. "The Use of Positron Emission Tomography in Soft Tissue Sarcoma Patients under Therapy with Trabectedin" Marine Drugs 7, no. 3: 331-340. https://doi.org/10.3390/md7030331