Introduction
Endemic arsenic exposure emerged as a single catastrophe affecting millions of people mostly living in Bangladesh, India, Mexico, Taiwan and South America. In these regions, the concentrations of arsenic amount to several hundred micrograms per liter that considerably exceed the standard of 50 μg/L for drinking water, recommended by the World Health Organization. In Bangladesh, at least 25 million people are drinking arsenic contaminated water [
1]. There is strong evidence from epidemiological studies of an association between chronic exposure to inorganic arsenic and hyperpigmentation, hyperkeratosis, and neoplasia in the skin as well as other diseases [
2]. A higher prevalence rate of arsenical skin lesions with clear dose-response relationship has been found among Bangladeshi populations drinking arsenic contaminated well water [
3]; and callus-like growths all over the extremities with changes in skin pigmentation have been reported [
4].
In humans, the liver rapidly detoxifies inorganic arsenic that is consumed in drinking water by transforming it to organic forms called monomethylarsonic acid (MMA) and dimethylarsenic acid (DMA) that are rapidly excreted in the urine to give an over-all arsenic half-life in the body of about 30 hours [
5]. Thus, following exposure to arsenate (valency state v), the first step in the biotransformation is the reduction to arsenite (valence state iii); a process that may be considered a bioactivation [
6]. There is evidence that the methylating capacity differs among individuals and populations and that different capacities would result in variation in tissue retention of arsenic. Environmental factors, particularly diet, might be important in explaining susceptibility to arsenic toxicity [
7].
Several studies have found that anaemia, leukopenia and thrombocytopenia are common effects of arsenic poisoning in humans following acute [
8] and chronic oral exposures [
9] at doses of 50 μg/Kg/day or more. These effects may be due to both a direct, cytotoxic or hemolytic effect on the blood cells [
8,
10] and a suppression of erythropoiesis [
10]. The magnitude of exposure to patients examined by these researchers is not specified, although arsenic concentration in some of the wells in the area exceeded 1000 μg/L. However, there are reports that hematological effects are not observed in all cases of acute poisoning with arsenic [
11,
12], and the hematological abnormalities are reversible within weeks of termination of exposure [
13].
Patients with arsenic induced Bowen’s disease showed a defected cell mediated immunity and decreased percentages of T cell and T helper cell populations in the peripheral blood mononuclear cells, and arsenic exposure leads to diminution of phytohemagglutinin (PHA) stimulated T cell proliferation [
14,
15]. Electron microscopy study revealed that exposure to sodium arsenite caused alteration in the cytoskeleton, Golgi apparatus, mitochondria and perinuclear membrane of the T lymphocytes which ultimately changed intracellular secretion of proteins including IL–2 that might lead to an impaired proliferation of the cells when stimulated with PHA. It has been reported that both arsenite and arsenate are strongly toxic to macrophages and able to decrease the number of surviving cells to 50% at a concentration of 5 or 500 μM, respectively [
16].
This study was undertaken to determine the relationship of clinical complications of arsenic toxicity with nutritional status based on both measured and self-reported parameters in a randomly selected group of arsenicosis patients and on the profile of their peripheral blood leukocyte.
Materials and Methods
Study Area
The study area of this investigation was the northwestern district of Chapainowabganj where arsenic contamination in drinking water was first detected in Bangladesh in 1993. Samples were collected during November 2001 to August 2003 from patients living in the arsenic endemic rural villages of Rajarampur, Achinpara, Chandnai, and Bottola.
Patient Data Collection
Arsenic exposed subjects whose drinking water contained more than the maximum permissible limit of arsenic (50 μg/L, as recommended by WHO), were enrolled in this study. Their source of drinking water was from tube wells or artisan wells. Prevalence of arsenicosis was based on appearance of skin lesions among the enrolled patients. After informed consent, the researchers with the help of a public health nurse interviewed all the patients personally. The information on symptoms and complications of arsenic toxicity, anthropometric parameters (including age, height, and body weight), monthly income of the family, number of family members, housing, education, and food intake were recorded on a prepared questionnaire. The quality and quantity of food consumed by the patient on three consecutive days starting from the day before sample collection through the following day (from perspective list) were recorded. Since most of the patients were subsistence farmers, land-less farmers, day laborers, and their family members who could not include the monetary value of the produce consumed within the household, the monthly income of the family of all subjects was recorded solely on the basis of self-reported estimate. From the data on questionnaire, the socioeconomic and nutritional status of each subject was determined.
Sample Collection
Blood samples (2 – 3 ml) were collected from the subjects with their full consent to participate in this study. A total of 235 blood samples were collected of which 115 were from patients with arsenic toxicity (arsenicosis), 80 from age-matched subjects living in the same area as the patients but drinking safe water and with no sign of arsenic toxicity, and the remaining from unexposed subjects living in the city. Spot urine and drinking water samples were also collected from each individual. The fresh blood sample was used for blood type determination, total and differential counts of white blood cells.
Analyses of Arsenic
Arsenic content in the water and urine samples was measured at the Laboratory of Analytical Chemistry, School of Environmental Studies, University of Jadavpur, Kolkata, India. Some of the samples were also analyzed at the Analytical Research Division, Dhaka Laboratories, Bangladesh Council of Scientific and Industrial Research (BCSIR) for the content of arsenic. A Flow Injection - Hydride Generation - Atomic Absorption Spectrophotometer (FI-HG-AAS) was used for analysis of the water and urine samples.
Total and Differential Counts of White Blood Cells
The total count of white blood cells (WBC) in a healthy subject usually varies from 4.0 – 11.0 X 106 cells/mL. To find out the effect of high concentrations of arsenic in drinking water on cells of the immune system, the WBC and differential counts were performed for each blood sample. The standard procedures were followed in preparing the samples, and total WBC and differential counts were determined. The percentages of neutrophils, eosinophils, basophils, lymphocytes and monocytes were calculated.
Statistical Analysis of the Data
Data analyses were carried out using the Statistical Package for Social Sciences (version 10.0 for Windows, SPSS Inc., Chicago, USA). The methods used were independent t– test for comparison of two groups (control and patients), correlations and statistical reporting. The results were considered significant when p was ≤ 0.05. Mean ± S.D. values were calculated for each studied parameter.
Results
Socioeconomic Status and Education Levels of Study Subjects
Of the total 115 patients enrolled in this study, there were 36 males and 79 females with age ranging from 14 to 85 years. The age range of males was 14 to 85 years; while that of females was 14 to 75 years. The whole population of patients had an average monthly income of the family of Tk. 4,620 (about $ 80) with a median value of Tk. 4000 while the monthly income of the family varied from Tk. 1,000 - 16,000. A total of 41 patients had no formal education; while 36 had primary; and 27 had high school education. Only 11 patients had passed secondary school certificate examination, of which 2 completed graduation and another one had a master’s degree. The number of family members of the patients varied from 2 to 9 with an average of 5.02 ± 1.53 and median value of 5. A total of 39 patients lived in semi-buildings, 54 in tin-shades, 16 in mud-made houses, and 6 in huts. Of the total 120 unexposed control subjects, there were 81 males and 39 females. Six of them were illiterate, while the education levels of the rest were in the secondary to higher secondary and above. The monthly income of the families of the controls varied from Taka 1,500 – 25,000 with an average of Taka 6,730. Their family members varied from 2 to 6.
Clinical Symptoms and Complications in the Patients
The clinical symptoms based on skin manifestations, complications and duration of arsenic toxicity in the patients are shown in
Table 1. There were diffused and spotted melanoses with black and white appearances, rough and mottled skin, keratosis or hardening of the skin with often formation of nodules. Spotted melanosis was more often seen on the throat, chest, back, or limbs. Many of the patients suffered from severe skin irritation. Prolonged exposure caused the skin to become rough and thickened due to diffused keratosis that usually developed on the soles of feet and palms of both hands with occasional formation of cracks on these areas. Patients with these clinical features were the worst sufferers of arsenic toxicity as they were unable to do their household works.
Arsenicosis patients suffered from other complications like breathing problems including asthma, bronchitis and cough. Gastric and abdominal pain was also very common. Some patients had pain all over the body, while others had backache, headache, palpitation, anaemia and weakness. Anaemia was more prevalent in the females as 26 out of 30 patients identified with anaemia were females. The patients had pain in joints including the knee, burning sensation, tingling, frequent fever and cold. There were some less common complains like sleep disturbances, night blindness, depression, loss of appetite, edema on feet, goiter, tonsillitis, loss of hearing, lesion in mouth, gout and hepatomegaly. These symptoms were more common in the patients than in the control (unexposed) subjects living in the same villages.
Depending upon the clinical symptoms in the patients, arsenicosis was divided into four categories: (i) melanosis (black and white pigmentation on skin), (ii) melanosis, keratosis, rough and mottled skin, (iii) melanosis, keratosis on palms and soles with and without cracks, nodule formation, and (iv) melanosis, keratosis, severe skin irritation, lump formation on feet. It was found that development of these symptoms was related to the duration of exposure as the mean duration was: 5.6 ± 4.1 yrs for (i); 7.2 ± 4.7 yrs for (ii); 8.6 ± 5.4 yrs for (iii) and 9.7 ± 6.6 yrs for (iv) (
Table 1). Further, the duration of exposure in 42 of the patients was at least for 10 yrs, while 15 had the signs of poisoning developed for 2 yrs or so. The whole population of patients had an average duration of exposure for 7.6 ± 5.2 yrs with a median of 6.5 yrs, and varied from 1 – 25 yrs. The average levels of arsenic in the drinking water of the different categories of arsenicosis patients were: (i) 206 μg/L, (ii) 190 μg/L, (iii) 252 μg/L, and (iv) 271 μg/L.
Levels of Arsenic in Drinking Water and Urine Samples
It was found that a total of 13 (11%) patients drank water that contained more than 600 μg/L of arsenic. There were 21 (18%) patients included in this study who switched to safe drinking water following the onset of arsenical skin lesions. The average level of arsenic in the drinking water of the patients was 218.1 ± 218.4 μg/L, with a median value of 156 μg/L. The levels varied from 3.0 – 875.0 μg/L. On the other hand, the mean arsenic concentration in the drinking water of the unexposed (control) population was 11.3 μg/L. The urine samples of only 15 (13%) patients contained arsenic that was within the permissible limit (5 – 40 μg/L). A total of 48 (42%) patients excreted more arsenic in urine than they had consumed through drinking water. This clearly indicated that there could be more than one source of arsenic contamination than drinking water. The average level of arsenic in the urine of the patients was 234.6 ± 311.5 μg/L while the median value was 129.7 μg/L and the levels varied from 20.0 – 1764.0 μg/L. Statistical analysis showed the levels of arsenic in the drinking water and urine samples of the patients was positively correlated at 1% level.
Table 1.
Clinical symptoms and complications in arsenicosis patients in relation to the duration of arsenic exposure
Table 1.
Clinical symptoms and complications in arsenicosis patients in relation to the duration of arsenic exposure
| Clinical symptoms (based on skin lesions and appearance) | Number of patients | Duration of arsenic exposure (years) | Number of patients with complications (most having more than one) |
|---|
| Asthma, bronchitis, cough | Gastric and abdominal pain | Weakness, headache, palpitation | Pain in limbs, knee, backache | Frequent fever, cold | Itchy rash, burning, tingling | Anaemia |
|---|
| (i) Melanosis (black and/ white pigmentation on skin) | 21 | 5.6 ± 4.1 | 8 | 13 | 8 | 4 | 6 | 5 | 8 |
| (ii) Melanosis, keratosis, rough and mottled skin | 53 | 7.2 ± 4.7 | 40 | 30 | 13 | 9 | 7 | 14 | 15 |
| (iii) Melanosis, keratosis on palms and soles with and without cracks, nodule formation | 23 | 8.6 ± 5.4 | 11 | 15 | 11 | 4 | 6 | 6 | 4 |
| (iv) Melanosis, keratosis, severe skin irritation, lump formation on feet | 18 | 9.7 ± 6.6 | 10 | 10 | 6 | 3 | 1 | 7 | 3 |
| Total (%) | 115 | | 69 (60%) | 68 (59%) | 38 (33%) | 20 (17%) | 20 (17%) | 32 (28%) | 30 (26%) |
Food Intake, Calorie Consumption and Anthropometric Data of the Study Subjects
The quality and quantity of food intake, calorie consumption, and anthropometric data of the patients showed that most of them were of poor health. The patients usually took rice with vegetables, potatoes and/or pulse everyday. They could manage to eat meat / fish once or twice a week. However, about 44% of the patients could eat meat / fish every day. The mean calorie consumption values were 1980 Kcal/day and 1850 Kcal/day for male and female patients, respectively. On the other hand, the quality and quantity of food intake by the control subjects were slightly improved and the mean calorie consumption values were 2100 Kcal/day and 1960 Kcal/day for males and females, respectively. The male patients had an average height of 1.67 meters (range: 1.47 – 1.85) and body weight of 54.4 Kg (range: 36.0–70.0); while the females had an average height of 1.49 meters (range: 1.27 – 1.82) and body weight of 48.3 Kg (range: 36.0 – 68.0). The control males had an average height of 1.70 meters (range: 1.55 – 1.82), body weight of 63.2 ± 8.0 Kg (range: 47 – 86) and body mass index (BMI) of 22.0 ± 2.3. The control females had an average height of 1.60 meters (range: 1.50– 1.68), body weight of 54.1 ± 7.8 Kg (range: 44 – 67) and BMI of 21.2 ± 2.5.
Nutritional Profile of Arsenicosis Patients
The nutritional profile of the arsenicosis patients was evaluated based on their BMI. The male patients had an average BMI of 20.4 (range: 15.7 – 26.4), and that of the female patients was 21.4 (range: 16.2 – 31.5). The male and female patients were further divided into underweight (malnourished, BMI: < 18.5), normal weight (BMI: 18.5 – 24.9), and overweight (BMI: 25.0 – above) and their nutritional statuses were determined. The results are shown in
Table 2. It was found that about 28% of the patients were underweight (malnourished) compared to 15% of the controls. The results showed kilocalorie consumed per kilogram body weight (Kcal/Kg) was highly significantly different between the female patients of different nutritional groups (
p < 0.0001); but was significantly different only between the underweight and overweight male patients (
p < 0.05). On the other hand, nutritional status of the male patients was directly related to the monthly income of the family; whereas data of the female patients did not show this correlation.
Relationship between Clinical Complications of Toxicity and Nutritional Status
To find out whether nutritional status played any role in the development of the toxic effects of arsenic, incidences of the different categories of arsenicosis were compared between the underweight, normal weight, and overweight patients (
Table 3). The clinical symptoms that were evaluated were as described in the text and
Table 1. The results showed that the severe symptoms of types (iii) and (iv) were absent in the overweight (well nourished) patients; whereas those were present in 9 out of 32 (about 28%) of the underweight (malnourished) patients. Further, some of the overweight patients suffered from toxicity for more than 10 years; still their clinical symptoms were not severe.
Evaluation of Blood Type and Total WBC Count
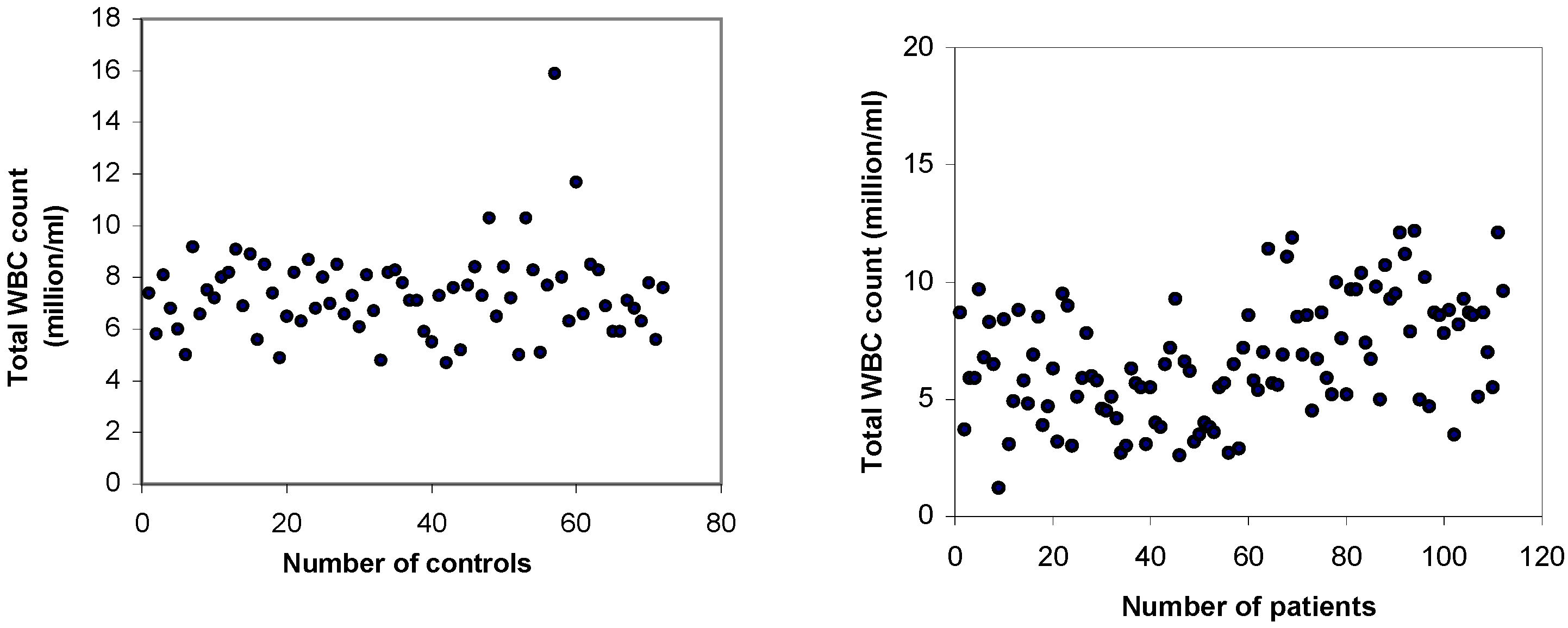
The blood type data of the patients showed that 35% had O group, 31% had A group, 24% had B group, and 10% had AB group. On the other hand, the control subjects showed 27% had O group, 25% had A group, 37% had B group, and 11% had AB group. The blood group data showed O and A type blood were more common among the arsenicosis patients (pooled: 66%) than the unexposed controls (pooled: 52%). The total counts of the WBC in the patients and control subjects are shown in Fig. 1. It was found that the total WBC count in about 26% of the patients was ≤ 5 X 106 cells/mL, while 16% had leukopenia. Although leukocytosis was observed in about 4% of the cases, the whole population of patients showed an average WBC count of 6.71 ± 2.51 X 106 cells/mL compared to 7.34 ± 1.70 X 106 cells/mL in the control subjects. Statistical analysis showed the total WBC count in the arsenic patients was significantly lower than the control, unexposed subjects.
Assessment of WBC Counts in Relation to Nutritional Status
Assessment of WBC counts in relation to nutritional statuses of the patients is shown in
Table 4. The results showed that nutritional status was directly related to the WBC counts in the female patients who had low WBC counts than the males within the same nutritional group. Of the total 18 patients identified with leukopenia, about 78% of them were females (not shown in Table). Further, about 44% of the total patients with leukopenia belonged to the underweight nutritional group.
Comparison of Differential Counts
The differential counts of WBC in the patients and control subjects are shown in
Table 5. It was observed that about 26% of the patients showed neutropenia, having less than 50% neutrophils in the peripheral blood (normal range: 50 - 70%). This low neutrophil count was not compensated by elevated eosinophil or basophil counts. Further, the lymphocyte count showed high values in many patients (normal range: 20 - 40%); and 45 of them had more than 40% lymphocytes, of which 13 had ≥ 50% of the leukocytes belonged to this type. However, the whole population data showed none of the leukocytes in the patients varied significantly compared to that in the controls. The average neutrophil count in the neutropenic patients was 44.8 ± 3.7%, lymphocyte count 48.7 ± 4.4%, levels of arsenic in water and urine samples of 236.9 ± 248.3 μg/L and 195.9 ± 197.7μg/L respectively, and duration of arsenic exposure for 8.4 ± 5.9 yrs. These findings suggest that chronic exposure to high levels of arsenic in drinking water may cause neutropenia and lymphocytosis.
Discussion
This study has been conducted in an attempt to quantify whether nutritional status plays any role in the prevalence of chronic arsenic toxicity. Almost every physiological system in the human including the respiratory, immune, gastrointestinal, genitourinary, reproductive, and nervous systems have been reported to be adversely affected by prolonged exposure to high doses of arsenic [
7,
17,
18]. There has been a significant dose-response relationship between skin cancer prevalence and chronic arsenic exposure as indexed by duration of consumption of high-arsenic artesian well water, average exposure, and cumulative exposure among residents of Taiwanese villages [
19]. In these people, under nourishment due to a high consumption of dried sweet potato as a staple food has been found to be significantly associated with an increased prevalence of arsenic induced skin cancer. An epidemiological study conducted in West Bengal, India showed male gender and malnutrition correlated with increased prevalence of skin manifestations in arsenic exposed population [
20]. In a recent study, an association between nutritional status and chronic exposure to arsenic has been reported among Bangladeshi patients [
21].
Table 2.
Nutritional status of arsenicosis patients
Table 2.
Nutritional status of arsenicosis patients
| Nutritional status | BMI | Body weight (Kg) | Kcal/Kg | Kcal/day | Monthly family income (Taka) |
|---|
| Underweight: | | | | | |
| Male (n = 14) | 17.5 ± 0.9 | 50.6 ± 3.6 | 36.8 ± 3.5 | 1853 ± 181 | 4060 ± 2280 |
| Female (n = 18) | 17.8 ± 0.6 | 43.4 ± 4.7 | 44.6 ± 4.9 | 1810 ± 110 | 4970 ± 2880 |
| Normal weight: | | | | | |
| Male (n = 18) | 21.4 ± 2.0 | 58.3 ± 7.7 | 35.0 ± 5.0 | 1986 ± 97 | 5110 ± 3376 |
| Female (n = 48) | 21.2 ± 1.9 | 48.7 ± 6.8 | 38.6 ± 4.2 | 1842 ± 142 | 4115 ± 2530 |
| Overweight: | | | | | |
| Male (n = 04) | 25.8 ± 0.2 | 68.5 ± 1.5 | 32.0 ± 2.0 | 2104 ± 96 | 5250 ± 870 |
| Female (n = 13) | 26.9 ± 1.9 | 59.1 ± 7.3 | 31.6 ± 4.6 | 1884 ± 294 | 4300 ± 2440 |
Table 3.
Relationship between clinical symptoms of arsenic toxicity and nutritional status of patients
Table 3.
Relationship between clinical symptoms of arsenic toxicity and nutritional status of patients
| Nutritional status of the patients | Number of patients with clinical symptoms |
|---|
| i) Melanosis (black and/white pigmentation on skin) | ii) Melanosis, keratosis, rough and mottled skin | (iii) Melanosis, keratosis on palms and soles with and without cracks, nodule formation | (iv) Melanosis, keratosis, severe skin irritation, lump formation on feet |
|---|
Underweight
(n = 32) | 7 | 16 | 8 | 1 |
Normal weight
(n = 66) | 9 | 25 | 15 | 17 |
Overweight
(n = 17) | 6 | 11 | _ | _ |
Figure 1.
Comparison of the total white blood cell (WBC) counts in control subjects (n = 74) and arsenic patients (n = 115). Leukopenia (< 4 million cells/mL) had been found in 18 (16%) of the patients suffering from arsenic toxicity. The average WBC count in the patients was 6.71 ± 2.51 X 106 cells/mL compared to 7.34 ± 1.70 X 106 cells/mL in the controls, suggesting the patients had significantly lower WBC counts than the control subjects (p = < 0.05).
Figure 1.
Comparison of the total white blood cell (WBC) counts in control subjects (n = 74) and arsenic patients (n = 115). Leukopenia (< 4 million cells/mL) had been found in 18 (16%) of the patients suffering from arsenic toxicity. The average WBC count in the patients was 6.71 ± 2.51 X 106 cells/mL compared to 7.34 ± 1.70 X 106 cells/mL in the controls, suggesting the patients had significantly lower WBC counts than the control subjects (p = < 0.05).
Table 4.
Assessment of WBC counts in relation to the nutritional status of patients
Table 4.
Assessment of WBC counts in relation to the nutritional status of patients
| Nutritional status | Total WBC counts: (Mean ± S.D) X 106 cells/mL | Total patients with leukopenia
n = 18 |
|---|
Female patients
n = 79 | Male patients
n = 36 | Total patients
n = 115 |
|---|
| Underweight | 5.74 ± 2.27
n = 18 | 7.21 ± 3.32
n = 14 | 6.38 ± 2.83
n = 32 | 8 (44%) |
| Normal weight | 6.80 ± 2.34
n = 48 | 7.12 ± 2.17
n = 18 | 6.89 ± 2.28
n = 66 | 7 (39%) |
| Overweight | 6.38 ± 2.80
n = 13 | 7.10 ± 2.12
n = 04 | 6.55 ± 2.62
n = 17 | 3 (17%) |
Table 5.
Differential counts of WBC in the arsenic patients and control subjects
Table 5.
Differential counts of WBC in the arsenic patients and control subjects
| Study subjects | Percentage of white blood cells: Mean ± SD
( Range) |
|---|
| Neutrophils | Lymphocytes | Monocytes | Eosinophils | Basophils |
|---|
Patients
n = 115 | 56.9 ± 10.0
(32.0 – 79.0) | 37.4 ± 9.7
(17.0 – 58.0) | 2.8 ± 1.5
(0 – 7.0) | 1.6 ± 1.7
(0 – 11.0) | 1.2 ± 1.3
(0 – 7.0) |
Controls
n = 74 | 58.4 ± 6.8
(44.8 – 76.2) | 36.3 ± 6.2
(22.6 – 48.8) | 2.6 ± 1.6
(0.4 – 10.0) | 1.6 ± 1.3
(0 – 6.0) | 1.2 ± 1.6
(0 – 10.0) |
In this study, skin manifestations have been found as the prime and common features of arsenic toxicity that has been considered as definite exposure [
22]. We found a significant direct relationship between the concentrations of arsenic in water to that in urine. The duration of exposure has been found directly related to the severity of clinical disease. Similar dose-response relationships have been reported in long-term arsenic exposure with ischemic heart disease mortality in Taiwan [
23], and with skin lesions in Bangladesh [
3].
The calorie consumption per day values indicated that the patients have been nutritionally compromised and represented the common lower-middle class Bangladeshi populations; the control subjects from the same area showed similar data but have been in relatively better shape. BMI of the patients has been found inversely related to the duration of toxicity. Assessment of nutritional status in terms of BMI, calorie consumption per day and body weight has shown to have an inverse relationship to the clinical symptoms of arsenic toxicity. Our observations suggested that the underweight (malnourished) patients have been more prone than the overweight ones in developing the severe clinical symptoms of arsenicosis. Although BMI of the male patients has been lower than the females, we have not found an association of male gender with increased prevalence of arsenic-related clinical complications as has been reported [
3].
About 60% of our patients suffered from respiratory problems including asthma, bronchitis and cough. Prevalence of respiratory effects has been reported in a study conducted in West Bengal, India [
24], and in Bangladesh [
22]. In our study, some patients have had more than one arsenic-related complication as about 59% of them reported of having gastric and abdominal pain. About one third of the patients complained of weakness, headache and palpitation. These observations lead to the possibility that the respiratory and gastrointestinal systems are preferentially selected than other organs in human arsenic toxicity. Another observation of this study has been that since the study area located in the arsenic endemic region where the farmers use ground water for irrigation, and high concentration of arsenic present in these water might increase arsenic content of the paddy fields and ultimately contaminate nearby ponds, canals and other water bodies from where the residents collect water for cooking. Thus cooking rice and other foods in contaminated water might explain the reason for about 42% of the patients excreting more arsenic in urine than they have consumed through drinking water.
The effect of inorganic arsenic on human erythrocyte morphology has been studied in an
in vitro model and found changes in membrane integrity and deformability that could contribute to micro vascular occlusion and related peripheral vascular effects in chronic arsenic exposure [
25]. Rodent models of arsenic exposure have also demonstrated disturbances in heme biosynthesis, characterized particularly by an increased urinary uroporphyrin excretion [
26,
27]. These observations explain the possible reason for 26% of our patients suffering from anaemia, also reported by previous workers [
8,
9]. However, we have seen a far higher prevalence of anaemia in the female patients than males, 26 out of 30; 14 of these female patients represented the underweight nutritional group. Accounts of leukopenia due to neutropenia or lymphopenia, and relative eosinophilia have been reported in some of the early studies [
28,
29]. However, we have seen neutropenia among 26% of the patients, incidences of lymphopenia and eosinophilia have been insignificant; instead, we report lymphocytosis in 40% of the patients. Neutropenia and lymphocytosis have been found associated with chronic exposure to high levels of arsenic in drinking water. Conditions of neutropenia may indicate persistent infection in the patients, possibly due to arsenical skin lesions. Further, arsenic-toxicity induced lymphocytosis may modulate the immune response of the patients.
The majority of our patients have come from very poor socioeconomic class with about 56% unable to eat animal protein (meat / fish) everyday. Poor nutritional status of the patients may increase arsenic retention in the body and thus lead to severity of clinical complications. Patients with protein-energy malnutrition have inadequate supply of methionine from dietary sources, and studies in rabbits have shown low amount of methionine or protein in the diet decreased methylation of inorganic arsenic [
30]; and deficiency of other dietary trace elements including zinc and selenium [
31] may lead to arsenic accumulation and contribute to the toxic effects in the body. A recent study has shown that low intake of calcium, animal protein, folate and dietary fiber may increase susceptibility to arsenic-caused skin lesions [
32]. Moreover, apart from the poor nutritional status, peoples in Bangladesh have greater daily intake of water (and thus consume more arsenic) than those living in other parts of the world that are not tropical, and thereby suffer from the adverse effects of arsenic toxicity.


{kind=link}
