Cancer Risk in Diagnostic Radiation Workers in Korea from 1996–2002

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
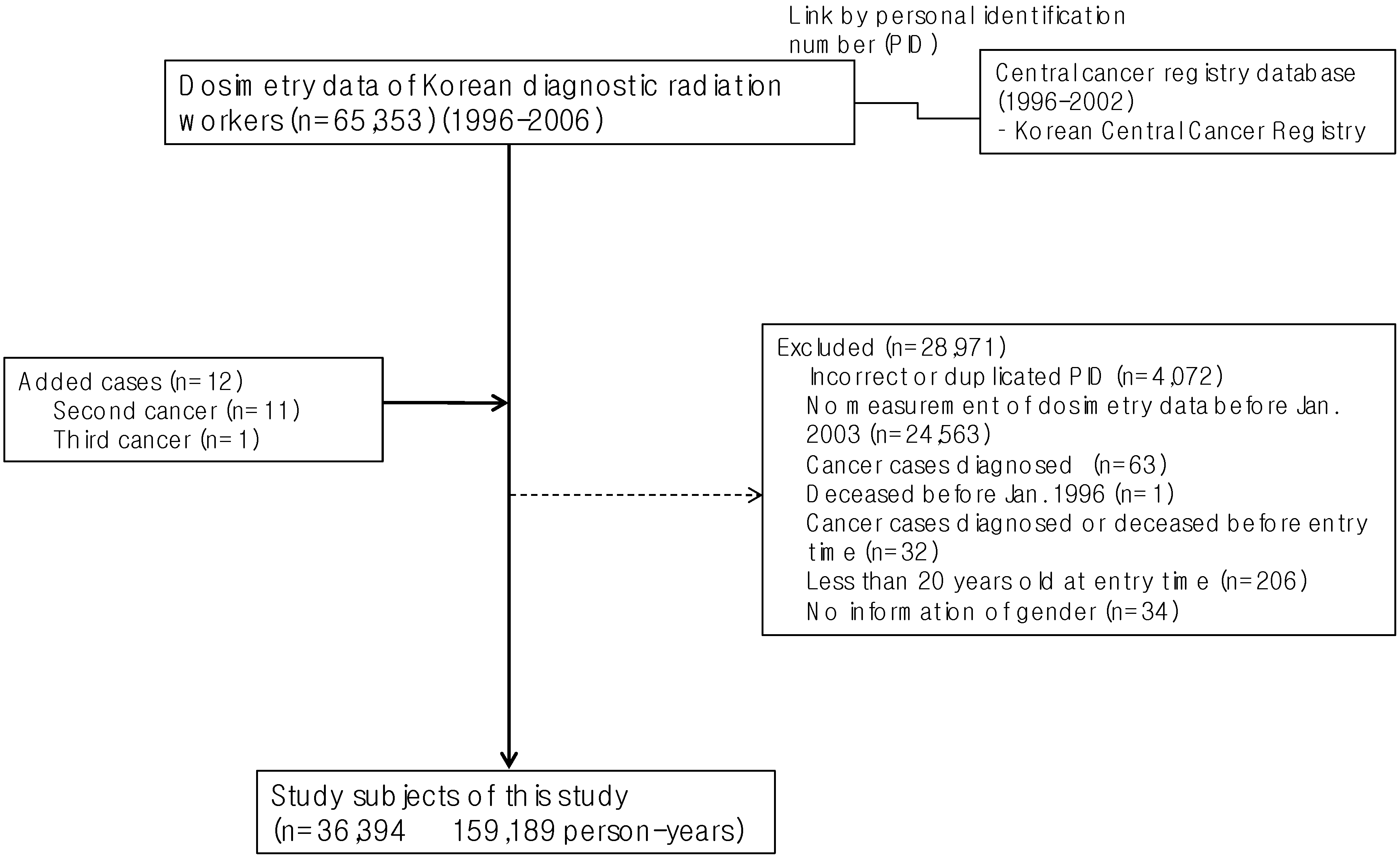
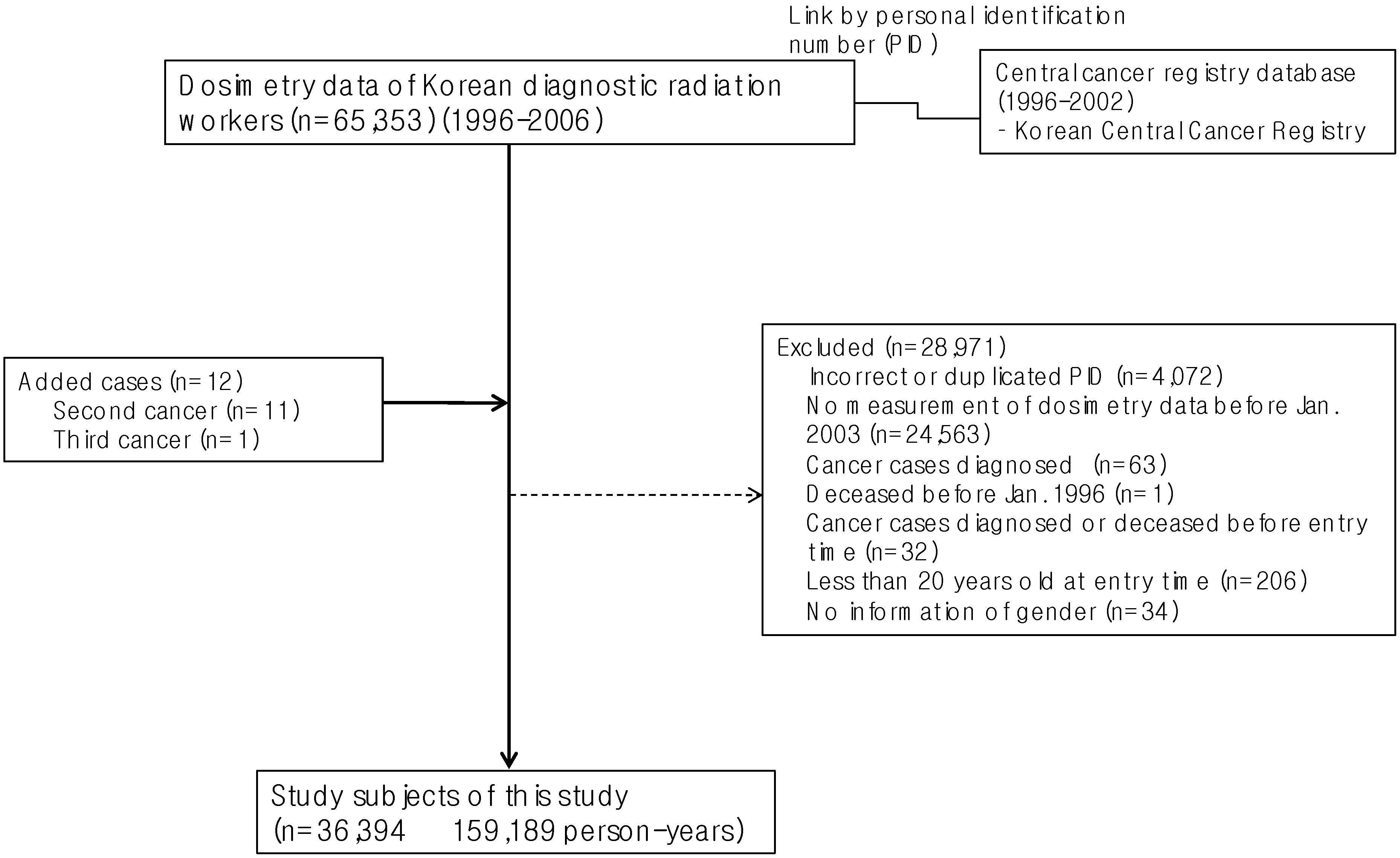
2.1. Study Subjects
2.2. Identification of Cancer Occurrence
2.3. Radiation Dose
2.4. Potential Confounding or Modifying Factors
2.5. Statistical Analysis
3. Results
3.1. Distribution of Radiation Effective Dose (1996–2002)
3.2. Standardized Incidence Rates (SIRs, 1999–2002)
3.3. Average Annual Effective Dose and Cancer Risk

{kind=link}
| N | Follow-up time (person-years) | Age at entry (years) | Average annual effective dose | Maximum annual effective dose | > 5 mSv/year | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Q1 | Median | Q3 | Q1 | Median | Q3 | N | % | ||||
| Male workers | ||||||||||||
| All | 25,022 | 114,339 | 34.11 (9.36) | 0.14 | 0.41 | 1.26 | 0.26 | 0.83 | 2.90 | 1,249 | 5.0 | |
| Radiologic technologists | 9,741 | 49,395 | 29.89 (6.75) | 0.52 | 1.17 | 2.70 | 1.04 | 2.49 | 5.61 | 828 | 8.5 | |
| Physicians | 2,700 | 9,865 | 36.80 (6.87) | 0.06 | 0.13 | 0.25 | 0.08 | 0.22 | 0.48 | 9 | 0.3 | |
| Dentists | 6,782 | 26,558 | 39.62 (8.78) | 0.10 | 0.23 | 0.59 | 0.14 | 0.38 | 1.17 | 147 | 2.2 | |
| Dental hygienists | 9 | 30 | 31.11 (7.51) | 0.04 | 0.09 | 0.17 | 0.08 | 0.12 | 0.22 | 0 | 0.0 | |
| Others | 5,790 | 28,491 | 33.50 (10.99) | 0.08 | 0.24 | 0.56 | 0.22 | 0.57 | 1.66 | 265 | 4.6 | |
| Female workers | ||||||||||||
| All | 11,372 | 44,850 | 27.16 (5.85) | 0.07 | 0.21 | 0.52 | 0.13 | 0.39 | 1.12 | 118 | 1.0 | |
| Radiologic technologists | 3,335 | 12,893 | 25.40 (4.87) | 0.21 | 0.47 | 0.98 | 0.33 | 0.77 | 2.00 | 48 | 1.4 | |
| Physicians | 624 | 2,114 | 32.27 (5.40) | 0.05 | 0.12 | 0.23 | 0.06 | 0.19 | 0.42 | 1 | 0.2 | |
| Dentists | 876 | 3,411 | 33.32 (6.19) | 0.12 | 0.30 | 0.68 | 0.17 | 0.50 | 1.62 | 9 | 1.0 | |
| Dental hygienists | 1,797 | 3,800 | 25.23 (3.76) | 0.04 | 0.12 | 0.25 | 0.05 | 0.14 | 0.35 | 0 | 0.0 | |
| Others | 4,740 | 22,632 | 27.31 (5.91) | 0.05 | 0.15 | 0.37 | 0.14 | 0.37 | 0.96 | 60 | 1.3 | |
| Cancer | Male (n = 24,942; 114,216 person-year) | Female (n = 11,360; 44,829 person-year) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| No. of cancer | SIR a | 95% CI | No. of cancer | SIR a | 95% CI | ||||
| Observed | Expected | Observed | Expected | ||||||
| All (C00-C97) | 110 | 297.13 | 0.37 | 0.30 to 0.44 | 32 | 57.05 | 0.56 | 0.37 to 0.76 | |
| Esophagus (C15) | 4 | 6.42 | 0.62 | 0.01 to 1.23 | 0 | 0.04 | - | - | |
| Stomach (C16) | 21 | 73.60 | 0.29 | 0.16 to 0.41 | 1 | 6.94 | 0.14 | −0.14 to 0.43 | |
| Colon and rectum (C18-C20) | 16 | 30.65 | 0.52 | 0.27 to 0.78 | 2 | 2.94 | 0.68 | −0.26 to 1.62 | |
| Liver (C22) | 15 | 58.25 | 0.26 | 0.13 to 0.39 | 1 | 1.56 | 0.64 | −0.61 to 1.90 | |
| Lung (C33-C34) | 7 | 38.22 | 0.18 | 0.05 to 0.32 | 0 | 1.33 | - | - | |
| Breast (C50) | 0 | 0.31 | - | - | 10 | 12.63 | 0.79 | 0.30 to 1.28 | |
| Bladder (C67) | 3 | 7.88 | 0.38 | −0.05 to 0.81 | 0 | 0.18 | - | - | |
| Brain (C70-C72) | 1 | 4.58 | 0.22 | −0.21 to 0.65 | 2 | 1.04 | 1.92 | −0.74 to 4.59 | |
| Thyroid (C73) | 7 | 4.82 | 1.45 | 0.38 to 2.53 | 9 | 9.27 | 0.97 | 0.34 to 1.61 | |
| Hodgkin (C81) | 1 | 0.63 | 1.58 | −1.51 to 4.67 | 0 | 0.17 | - | - | |
| Non-Hodgkin lymphoma (C82-C85, C96) | 2 | 8.35 | 0.24 | −0.09 to 0.57 | 0 | 1.24 | - | - | |
| Leukemia (C91-C95) | 4 | 6.91 | 0.58 | 0.01 to 1.15 | 1 | 1.73 | 0.58 | −0.56 to 1.71 | |
| All cancers excluding leukemia | 106 | 290.22 | 0.37 | 0.30 to 0.43 | 31 | 55.32 | 0.56 | 0.36 to 0.76 | |
| Total radiation related cancers b | 81 | 240.63 | 0.34 | 0.26 to 0.41 | 26 | 39.07 | 0.67 | 0.41 to 0.92 | |
| Total radiation related cancers excluding leukemia | 77 | 233.72 | 0.33 | 0.26 to 0.40 | 25 | 37.34 | 0.67 | 0.41 to 0.93 | |
| Cancer | Average of annual effective dose | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male (n = 25,022 114,339 person-years) | Female (n = 11,372 44,850 person-years) | ||||||||||||
| Q1-Q3 (n = 17,412) | Q4 (n = 7,610) | p-trend a | p-trend b | Q1-Q3 (n = 9,883) | Q4 (n = 1,489) | p-trend a | p-trend b | ||||||
| Case | Case | HR | 95% CI | Case | Case | HR | 95% CI | ||||||
| All (C00-C97) | 104 | 50 | 2.14 | 1.48–3.10 | <0.0001 | 0.01 | 25 | 13 | 4.43 | 2.17–9.04 | <0.0001 | 0.06 | |
| Esophagus (C15) | 5 | 1 | 1.78 | 0.21–15.27 | 0.68 | 0.84 | 0 | 0 | - | - | - | ||
| Stomach (C16) | 20 | 7 | 0.97 | 0.38–2.49 | 0.65 | 0.57 | 2 | 1 | 5.99 | 0.53–68.19 | 0.22 | 0.94 | |
| Colon and rectum (C18-C20) | 19 | 8 | 2.37 | 0.99–5.67 | 0.02 | 0.82 | 1 | 1 | 10.25 | 0.54–192.77 | 0.09 | 0.32 | |
| Liver (C22) | 17 | 6 | 1.99 | 0.73–5.42 | 0.10 | 0.83 | 1 | 0 | 0.00 | 0–Inf | <0.0001 | 0.96 | |
| Lung (C33-C34) | 7 | 3 | 2.89 | 0.70–11.96 | 0.14 | 0.26 | 0 | 0 | - | - | - | ||
| Breast (C50) | - | - | - | - | - | 7 | 3 | 3.34 | 0.78–14.32 | 0.06 | 0.59 | ||
| Bladder (C67) | 3 | 1 | 0.69 | 0.07–6.63 | 0.99 | 0.61 | 0 | 0 | - | - | |||
| Brain (C70-C72) | 1 | 1 | 5.59 | 0.35–90.42 | 0.19 | 0.08 | 1 | 1 | 17.38 | 1.05–287.80 | 0.04 | 0.40 | |
| Thyroid (C73) | 4 | 5 | 3.55 | 0.85–14.81 | 0.05 | 0.12 | 8 | 4 | 3.88 | 1.09–13.75 | 0.01 | 0.13 | |
| Hodgkin (C81) | 1 | 1 | 5.00 | 0–Inf | 0.21 | 0.91 | 0 | 0 | - | - | - | ||
| Non-Hodgkin (C82-C85, C96) | 2 | 1 | 0.63 | 0–Inf | 0.87 | 0.36 | 1 | 0 | 0.00 | 0–Inf | - | 0.93 | |
| Leukemia (C91-C95) | 3 | 1 | 3.48 | 0.36–34 | 0.32 | 0.80 | 1 | 0 | 0.00 | 0–Inf | 0.48 | 0.99 | |
| All cancers excluding leukemia | 101 | 49 | 2.11 | 1.45–3.08 | <0.0001 | 0.01 | 24 | 13 | 4.53 | 2.21–9.29 | <0.0001 | 0.06 | |
| Total radiation related cancers c | 82 | 35 | 1.95 | 1.27–3.00 | <0.0001 | 0.01 | 22 | 10 | 4.29 | 1.92–9.58 | <0.0001 | 0.06 | |
| Total radiation related cancers excluding leukemia | 79 | 34 | 1.91 | 1.23–2.96 | 0.0002 | 0.01 | 21 | 10 | 4.41 | 1.96–9.91 | <0.0001 | 0.06 | |
| Cancer | Experience of annual doses exceeding 5 mSv | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male (n = 25,022 114,339 person-years) | Female (n = 11,372 44,850 person-years) | ||||||||||||
| No (n = 23,773) | Yes (n = 1,249) | Frequency of experience c | No (n = 11,254) | Yes (n = 118) | Frequency of experience c | ||||||||
| Case | Case | HR a | 95% CI | HR b | 95% CI | Case | Case | HR a | 95% CI | HR b | 95% CI | ||
| All (C00-C97) | 147 | 7 | 0.80 | 0.37–1.72 | 0.79 | 0.43–1.45 | 37 | 1 | 1.20 | 0.16–9.05 | 1.05 | 0.17–6.39 | |
| Esophagus (C15) | 6 | 0 | 0.00 | 0–Inf | 0 | 0 | - | - | - | - | |||
| Stomach (C16) | 25 | 2 | 1.07 | 0.25–4.60 | 0.88 | 0.26–2.99 | 3 | 0 | |||||
| Colon and rectum (C18-C20) | 26 | 1 | 0.83 | 0.11–6.16 | 0.73 | 0.13–4.07 | 2 | 0 | |||||
| Liver (C22) | 22 | 1 | 0.90 | 0.12–6.78 | 0.77 | 0.14–4.23 | 1 | 0 | - | 1.04 | 0–Inf | ||
| Lung (C33-C34) | 10 | 0 | 0 | 0 | - | - | |||||||
| Breast (C50) | 0 | 0 | 10 | 0 | |||||||||
| Bladder (C67) | 4 | 0 | 0 | 0 | - | - | |||||||
| Brain (C70-C72) | 2 | 0 | 1 | 1 | 63.11 | 3.70–1075 | 13.2 | 1.80–96.76 | |||||
| Thyroid (C73) | 9 | 0 | 12 | 0 | |||||||||
| Hodgkin (C81) | 2 | 0 | 0 | 0 | |||||||||
| Non-Hodgkin (C82-C85, C96) | 3 | 0 | 1 | 0 | 1.02 | 0–Inf | |||||||
| Leukemia (C91-C95) | 3 | 1 | 11.75 | 1.08–128.2 | 4.67 | 0.30–71.66 | 1 | 0 | 0.90 | 0–Inf | |||
| All cancers excluding leukemia | 144 | 6 | 0.69 | 0.30–1.57 | 0.72 | 0.37–1.39 | 36 | 1 | 1.21 | 0.16–9.09 | 1.05 | 0.17–6.37 | |
| Total radiation related cancers d | 112 | 5 | 0.77 | 0.31–1.90 | 0.69 | 0.32–1.50 | 31 | 1 | 1.91 | 0.26–14.15 | 1.47 | 0.26–8.25 | |
| Total radiation related cancers excluding leukemia | 109 | 4 | 0.62 | 0.23–1.70 | 0.59 | 0.25–1.41 | 30 | 1 | 1.92 | 0.26–14.26 | 1.47 | 0.26–8.21 | |
3.4. Experience Exposed to more than 5 mSv/Year and Cancer Risk
4. Discussion
Acknowledgments
Conflict of Interest
References
- Yoshinaga, S.; Mabuchi, K.; Sigurdson, A.J.; Doody, M.M.; Ron, E. Cancer risks among radiologists and radiologic technologists: Review of epidemiologic studies. Radiology 2004, 233, 313–321. [Google Scholar] [CrossRef]
- Linet, M.S.; Freedman, D.M.; Mohan, A.K.; Doody, M.M.; Ron, E.; Mabuchi, K.; Alexander, B.H.; Sigurdson, A.; Hauptmann, M. Incidence of haematopoietic malignancies in US radiologic technologists. Occup. Environ. Med. 2005, 62, 861–867. [Google Scholar] [CrossRef]
- Lee, W.J.; Cha, E.S.; Ha, M.; Jin, Y.W.; Hwang, S.S.; Kong, K.A.; Lee, S.W.; Lee, H.K.; Lee, K.Y.; Kim, H.J. Occupational radiation doses among diagnostic radiation workers in South Korea, 1996–2006. Radiat. Prot. Dosimetry 2009, 136, 50–55. [Google Scholar] [CrossRef]
- UNSCEAR 2008 Report Vol. 1. Available online: www.unscear.org/unscear/en/publications/2008_1.html (accessed on 25 June 2012).
- Korea Food & Drug Administration. Annual Report of Individual Dosimetry of Medical Radiation Workers, Radiation Protection Series No. 20. 2008. Available online: www.kfda.go.kr/medicaldevice/index.do?nMenuCode=94&page=2&categoryCode1=86&page=2&mode=view&boardSeq=49608 (accessed on 8 November 2012).
- Korea Center for Cancer Registry. Annual Report of Cancer in Korea 2002. Report number 11744. Ministry of Health and Welfare 2007. Available online: http://ncc.re.kr/manage/manage03_033_view.jsp?bbsnum=88&hSelSearch=&hTxtKeyword=¤t_page=2&cd=null (accessed on 16 January 2012).
- Korea Food & Drug Administration. Construction of Cohort of Radiation Workers in Diagnostic Radiology. 2008. Available online: http://rnd.kfda.go.kr/documentReport/documentReportResult.do (accessed on 8 November 2012).
- National Committee of Nuclear Safety. Enforcement Regulations (No. 2) of Nuclear Safety Acts. Available online: www.kins.re.kr/information/inf_law02.asp?top_menu_id=1095&menu_id=1115 (accessed on 27 August 2012).
- Moyses, S.; Javier, N. Epidemiologybeyond the Basics, 1st ed; Jones and Bartlett Learning: Burlington, VT, USA, 2000; p. 272. [Google Scholar]
- Preston, D.L.; Ron, E.; Tokuoka, S.; Funamoto, S.; Nishi, N.; Soda, M.; Mabuchi, K.; Kodama, K. Solid cancer incidence in atomic bomb survivors: 1958–1998. Radiat. Res. 2007, 168, 1–64. [Google Scholar] [CrossRef]
- Korean Statistical information service (KOSIS). Available online: http://kosis.kr/ (accessed on 27 March 2011).
- McMichael, A.J. Standardized mortality ratios and the “healthy worker effect”: Scratching beneath the surfact. J. Occup. Med. 1976, 18, 165–168. [Google Scholar] [CrossRef]
- R Version 2.12.2© R Foundation. The R project for statistical computing. Available online: www.r-project.org (accessed on 25 February 2011).
- Douple, E.B.; Mabuchi, K.; Cullings, H.M.; Preston, D.L.; Kodama, K.; Shimizu, Y.; Fujiwara, S.; Shore, R.E. Long-term radiation-related health effects in a unique human population: Lessons learned from the atomic bomb survivors of Hiroshima and Nagasaki. Disaster Med. Public Health Prep. 2011, 5 Suppl. 1, S122–S133. [Google Scholar] [CrossRef]
- Sigurdson, A.J.; Doody, M.M.; Rao, R.S.; Freedman, D.M.; Alexander, B.H.; Hauptmann, M.; Mohan, A.K.; Yoshinaga, S.; Hill, D.A.; Tarone, R.; Mabuchi, K.; Ron, E.; Linet, M.S. Cancer incidence in the US radiologic technologists health study, 1983–1998. Cancer 2003, 97, 3080–3089. [Google Scholar] [CrossRef]
- UNSCEAR 2006 Report Vol. 1. Available online: www.unscear.org/unscear/en/publications/2006_1.html (accessed on 25 June 2012).
- Wenzl, T.B. Increased brain cancer risk in physicians with high radiation exposure. Radiology 2005, 235, 709–711. [Google Scholar] [CrossRef]
- Zabel, E.W.; Alexander, B.H.; Mongin, S.J.; Doody, M.M.; Sigurdson, A.J.; Linet, M.S.; Freedman, D.M.; Hauptmann, M.; Mabuchi, K.; Ron, E. Thyroid cancer and employment as a radiologic technologist. Int. J. Cancer 2006, 119, 1940–1945. [Google Scholar] [CrossRef]
- Jeong, M.; Jin, Y.W.; Yang, K.H.; Ahn, Y.O.; Cha, C.Y. Radiation exposure and cancer incidence in a cohort of nuclear power industry workers in the Republic of Korea, 1992–2005. Radiat. Environ. Biophys 2010, 49, 47–55. [Google Scholar] [CrossRef]
- Fornalski, K.W.; Dobrzyński, L. The Healthy worker effect and nuclear industry workers. Dose Resp. 2010, 8, 125–147. [Google Scholar] [CrossRef]
- Dauer, L.T.; Brooks, A.L.; Hoel, D.G.; Morgan, W.F.; Stram, D.; Tran, P. Review and evaluation of updated research on the health effects associated with low-dose ionising radiation. Radiat. Prot. Dosimetry 2010, 140, 103–136. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Choi, K.-H.; Ha, M.; Lee, W.J.; Hwang, S.-S.; Jeong, M.; Jin, Y.-W.; Kim, H.J.; Lee, K.-Y.; Lee, J.-E.; Kang, J.-W.; et al. Cancer Risk in Diagnostic Radiation Workers in Korea from 1996–2002. Int. J. Environ. Res. Public Health 2013, 10, 314-327. https://doi.org/10.3390/ijerph10010314
Choi K-H, Ha M, Lee WJ, Hwang S-S, Jeong M, Jin Y-W, Kim HJ, Lee K-Y, Lee J-E, Kang J-W, et al. Cancer Risk in Diagnostic Radiation Workers in Korea from 1996–2002. International Journal of Environmental Research and Public Health. 2013; 10(1):314-327. https://doi.org/10.3390/ijerph10010314
Chicago/Turabian StyleChoi, Kyung-Hwa, Mina Ha, Won Jin Lee, Seung-Sik Hwang, Meeseon Jeong, Young-Woo Jin, Hyeog Ju Kim, Kwang-Yong Lee, Jung-Eun Lee, Jong-Won Kang, and et al. 2013. "Cancer Risk in Diagnostic Radiation Workers in Korea from 1996–2002" International Journal of Environmental Research and Public Health 10, no. 1: 314-327. https://doi.org/10.3390/ijerph10010314