Was Mandatory Quarantine Necessary in China for Controlling the 2009 H1N1 Pandemic?



Abstract
:1. Introduction
2. Methods
2.1. The SEIR Model


2.2. Determination of Model Parameters
3. Results
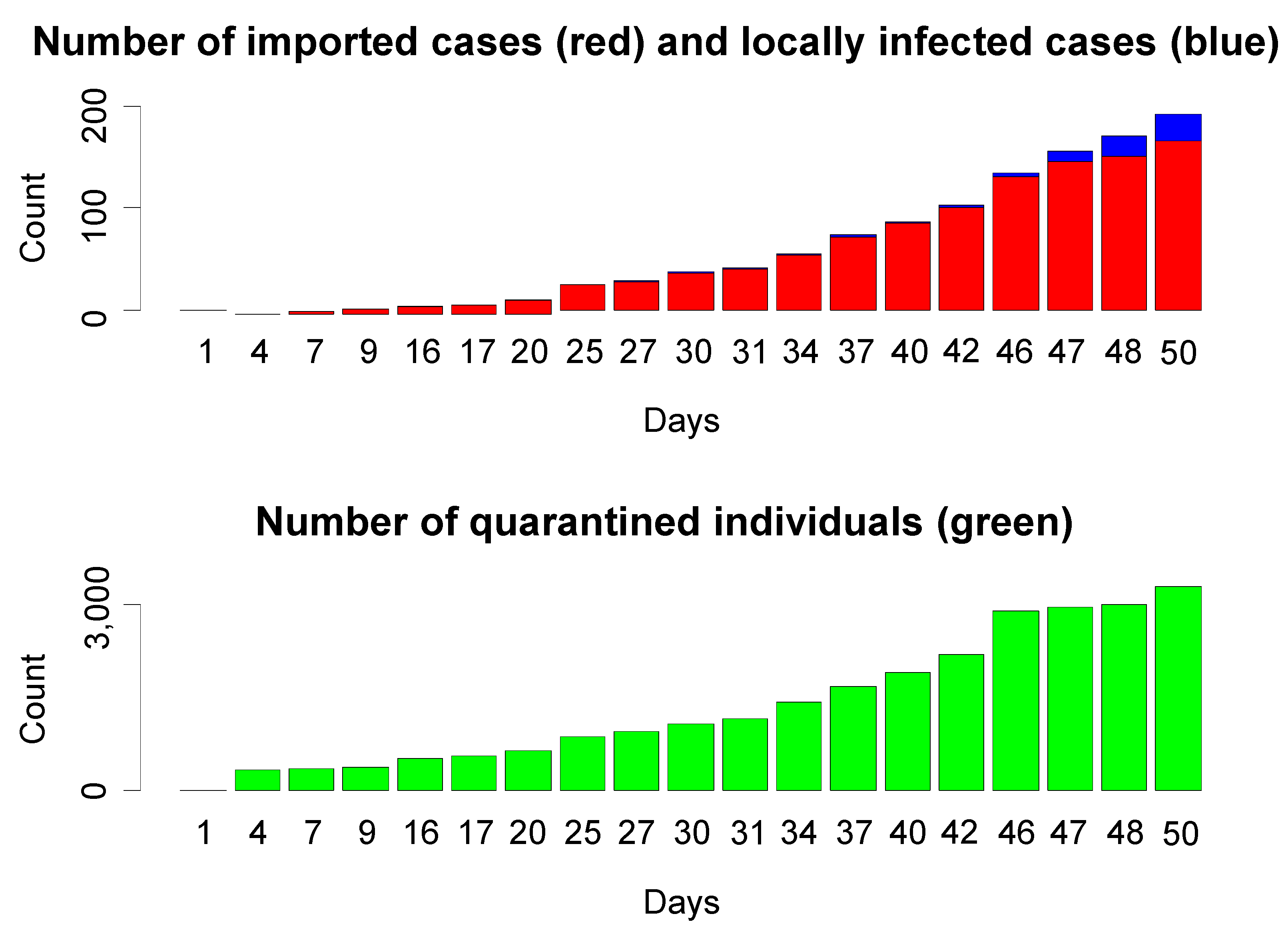
3.1. Summary of 2009 H1N1 Pandemic Infection and Control in Beijing and Mainland China

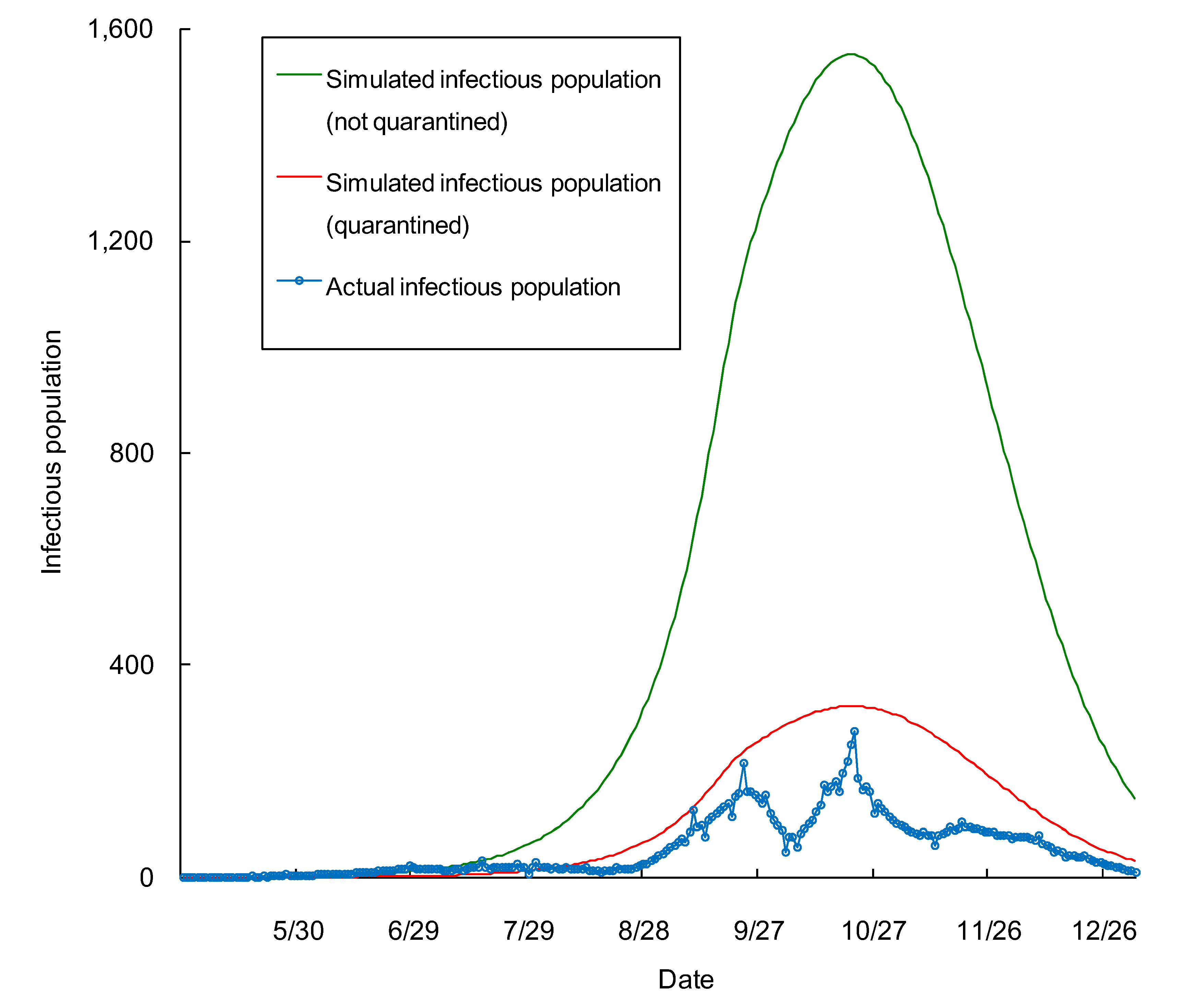
3.2. Effectiveness of Quarantine in Beijing


{kind=link}
{kind=link}
| Scenario 1: nobody was quarantined | ||||
|---|---|---|---|---|
| Quarantined individuals | Cost per capita (US$) | Cost (US$) | Memo | |
| Tracking | 3,279 | 120 | 3.93E+05 | an ambulance with three staff |
| Accommodations | 3,279 | 70 × 7 days | 1.61E+06 | seven days in a three star hotel |
| Medical check | 3,279 | 50 | 1.64E+05 | |
| Infected individuals | Cost per capita (US$) | Cost (US$) | Memo | |
| Medical check | 26,622/3.38 * = 7876 | 50 | 3.94E+05 | simulated intensity/duration |
| Total | 2.56E+06 | |||
| Scenarios 2: close contactors were quarantined during the period from 16 May to 8 July 2009 | ||||
| Infected individuals | Cost per capita (US$) | Cost (US$) | Memo | |
| Medical check | 128,004/3.38 * = 37,871 | 50 | 1.89E+06 | simulated intensity/duration |
| Total | 1.89E+06 | |||
4. Discussion
5. Conclusions
Acknowledgements
Conflicts of Interest
References
- Glasser, J.W.; Hupert, N.; McCauley, M.M.; Hatchett, R. Modeling and public health emergency responses: Lessons from SARS. Epidemics 2011, 3, 32–37. [Google Scholar] [CrossRef]
- Layne, S.P.; Monto, A.S.; Taubenberger, J.K. Pandemic influenza: An inconvenient mutation. Science 2009, 323, 1560–1561. [Google Scholar] [CrossRef]
- Fraser, C.; Donnelly, C.A.; Cauchemez, S.; Hanage, W.P.; van Kerkhove, M.D.; Hollingsworth, T.D.; Griffin, J.; Baggaley, R.F.; Jenkins, H.E.; Lyons, E.J.; et al. Pandemic potential of a strain of influenza A (H1N1): Early findings. Science 2009, 324, 1557–1561. [Google Scholar] [CrossRef]
- WHO World now at the Start of 2009 Influenza Pandemic. Statement to the Press by WHO Director-General Dr Margaret Chan. Available online: http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/en/index.html (accessed on 14 June 2009).
- WHO H1N1 in Post-Pandemic Period. Available online: http://www.who.int/mediacentre/news/statements/2010/h1n1_vpc_20100810/en/index.html (accessed on 10 August 2010).
- WHO Pandemic (H1N1) 2009—Update 112. Available online: http://www.who.int/csr/don/2010_08_06/en/index.html (accessed on 1 August 2011).
- Li, X.; Tian, H.; Lai, D.; Zhang, Z. Validation of the gravity model in predicting the global spread of Influenza. Int. J. Env. Res. Public Health 2011, 8, 3134–3143. [Google Scholar] [CrossRef]
- Velasco, R.P.; Praditsitthikorn, N.; Wichmann, K.; Mohara, A.; Kotirum, S.; Tantivess, S.; Vallenas, C.; Harmanci, H.; Teerawattananon, Y. Systematic review of economic evaluations of preparedness strategies and interventions against influenza pandemics. PloS One 2012, 7, e30333. [Google Scholar] [CrossRef]
- Temte, J.L. Basic rules of influenza: How to combat the H1N1 influenza (Swine Flu) virus. Am. Fam. Physician 2009, 79, 938–939. [Google Scholar]
- Tang, S.; Xiao, Y.; Yuan, L.; Cheke, R.A.; Wu, J. Campus quarantine (Fengxiao) for curbing emergent infectious diseases: Lessons from mitigating A/H1N1 in Xi’an, China. J. Theor. Biol. 2012, 295, 47–58. [Google Scholar] [CrossRef]
- Pang, X.; Yang, P.; Li, S.; Zhang, L.; Tian, L.; Li, Y.; Liu, B.; Zhang, Y.; Liu, B.; Huang, R.; et al. Pandemic (H1N1) 2009 among quarantined close contacts, Beijing, People’s Republic of China. Emerg. Infect. Dis. 2011, 17, 1824–1830. [Google Scholar] [CrossRef]
- Tang, S.; Xiao, Y.; Yang, Y.; Zhou, Y.; Wu, J.; Ma, Z. Community-based measures for mitigating the 2009 H1N1 pandemic in China. PloS One 2011, 5, e10911. [Google Scholar] [CrossRef]
- Mei, S.; van de Vijver, D.; Xuan, L.; Zhu, Y.; Sloot, P.M.A. Quantitatively evaluating interventions in the influenza a (H1N1) epidemic on china campus grounded on individual-based simulations. ProcediaComput. Sci. 2010, 1, 1669–1676. [Google Scholar]
- Liang, W.; Feng, L.; Xu, C.; Xiang, N.; Zhang, Y.; Shu, Y.; Wang, H.; Luo, H.; Yu, H.; Liang, X.; et al. Response to the first wave of pandemic (H1N1) 2009: Experiences and lessons learnt from China. Public Health 2012, 126, 427–436. [Google Scholar] [CrossRef]
- Ministry of Health of China. A Suspicious Case of Influenza A (H1N1) in Sichuan Province. Available online: http://www.gov.cn/gzdt/2009-05/10/content_1310043.htm (accessed on 10 August 2010).
- Ministry of Health of China. Notification on Further Improving the Prevention and Control of Influenza A H1N1. Available online: http://www.gov.cn/gzdt/2009-07/08/content_1360236.htm (accessed on 10 August 2010).
- Castillo, E.E.; Ang, A. Mexico Decries China’s Quarantine of Its Citizens. Huffington Post. Available online: http://www.huffingtonpost.com/huff-wires/20090504/as-china-mexico-swine-flu/ (accessed on 17 September 2013).
- WHO Statement made at the Secretary-General’s briefing to the United Nations General Assembly on the H1N1 Influenza Situation. Available online: http://www.who.int/dg/speeches/2009/influenza_a_h1n1_situation_20090504/en/index.html (accessed on 4 May 2009).
- Shetty, P. Preparation for a pandemic: Influenza A H1N1. Lancet Infect. Dis. 2009, 9, 339–340. [Google Scholar] [CrossRef]
- Van Kerkhove, M.D.; Asikainen, T.; Becker, N.G.; Bjorge, S.; Desenclos, J.C.; dos Santos, T.; Fraser, C.; Leung, G.M.; Lipsitch, M.; Longini, I.M.; et al. Studies needed to address public health challenges of the 2009 H1N1 influenza pandemic: Insights from modeling. PloS Med. 2010, 7, e1000275. [Google Scholar] [CrossRef]
- Kamigaki, T.; Oshitani, H. Influenza pandemic preparedness and severity assessment of pandemic (H1N1) 2009 in South-east Asia. Public Health 2010, 124, 5–9. [Google Scholar] [CrossRef]
- Hayden, E.C. The turbulent history of the A(H1N1) virus. Nature 2009, 459, 14–15. [Google Scholar] [CrossRef]
- Tarantola, D.; Amon, J.; Zwi, A.; Gruskin, S.; Gostin, L. H1N1, public health security, bioethics, and human rights. Lancet 2009, 373, 2107–2108. [Google Scholar]
- Doyle, A.; Bonmarin, I.; Levy-Bruhl, D.; le Strat, Y.; Desenclos, J.C. Influenza pandemic preparedness in France: Modelling the impact of interventions. J. Epidemiol. Commun. Health 2006, 60, 399–404. [Google Scholar] [CrossRef]
- Waterer, G.W.; Hui, D.S.; Jenkins, C.R. Public health management of pandemic (H1N1) 2009 infection in Australia: A failure! Respirology 2010, 15, 51–56. [Google Scholar] [CrossRef]
- Zhang, J.; Xiao, Y. Modeling strategies for controlling H1N1 outbreaks in China. Int. J. Biomath. 2012, 5, 1250017. [Google Scholar] [CrossRef]
- Hethcote, H.W. The mathematics of infectious diseases. Siam Rev. 2000, 42, 599–653. [Google Scholar] [CrossRef]
- Fang, L.-Q.; Wang, L.-P.; de Vlas, S.J.; Liang, S.; Tong, S.-L.; Li, Y.-L.; Li, Y.-P.; Qian, Q.; Yang, H.; Zhou, M.-G.; et al. Distribution and risk factors of 2009 pandemic influenza A (H1N1) in mainland china. Am. J. Epidemiol. 2012, 175, 890–897. [Google Scholar] [CrossRef]
- Tuite, A.R.; Greer, A.L.; Whelan, M.; Winter, A.-L.; Lee, B.; Yan, P.; Wu, J.; Moghadas, S.; Buckeridge, D.; Pourbohloul, B.; et al. Estimated epidemiologic parameters and morbidity associated with pandemic H1N1 influenza. CMAJ Can. Med. Assoc. J. 2010, 182, 131–136. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention (China). China Adjusts and Improves Prevention and Control Against Influenza A (H1N1). Available online: http://www.chinacdc.net.cn/n272442/n272530/n273736/n273781/n4624704/n4624713/32164.html (accessed on 19 March 2010).
- Simonov, E.A.; Dahmer, T.D. Amur-Heilong River Basin Reader; Ecosystems Ltd.: Hong Kong, China, 2008. [Google Scholar]
- Ministry of Health of China. News Release Conference on Prevention and Control of Influenza A H1N1. Available online: http://www.china.com.cn/zhibo/2010-01/04/content_19174002.htm (accessed on 19 March 2010).
- Center for Disease Control and Prevention (Beijing), Status Report on Pandemic (H1N1) 2009 in Beijing; Publisher: Beijing, China, 2009.
- Szucs, T.D.; Nichol, K.; Meltzer, M.; Hak, E.; Chancelor, J.; Ammon, C. Economic and social impact of epidemic and pandemic influenza. Vaccine 2006, 24, 6776–6778. [Google Scholar]
- Keogh-Brown, M.R.; Smith, R.D. The economic impact of SARS: How does the reality match the predictions? Health Policy 2008, 88, 110–120. [Google Scholar] [CrossRef]
- Sato, H.; Nakada, H.; Yamaguchi, R.; Imoto, S.; Miyano, S.; Kami, M. When should we intervene to control the 2009 influenza A(H1N1) pandemic? Eur. Surveill. 2010, 15. pii=19455. [Google Scholar]
- Miyaki, K.; Sakurazawa, H.; Mikurube, H.; Nishizaka, M.; Ando, H.; Song, Y.; Shimbo, T. An effective quarantine measure reduced the total incidence of influenza a H1N1 in the workplace: Another way to control the H1N1 flu pandemic. J. Occup. Health 2011, 53, 287–292. [Google Scholar] [CrossRef]
- Tay, J.; Ng, Y.F.; Cutter, J.; James, L. Influenza A (H1N1–2009) pandemic in Singapore—public health control measures implemented and lessons learnt. Ann. Acad. Med. Singap. 2010, 39, 313–324. [Google Scholar]
- Lee, D.H.; Shin, S.S.; Jun, B.Y.; Lee, J.K. National level response to pandemic (H1N1) 2009. J. Prev. Med. Public Health 2010, 43, 99–104. [Google Scholar] [CrossRef]
- Balasegaram, S.; Glasswell, A.; Cleary, V.; Turbitt, D.; McCloskey, B. From containment to community: Trigger points from the London pandemic (H1N1) 2009 influenza incident response. Public Health 2011, 125, 72–78. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Li, X.; Geng, W.; Tian, H.; Lai, D. Was Mandatory Quarantine Necessary in China for Controlling the 2009 H1N1 Pandemic? Int. J. Environ. Res. Public Health 2013, 10, 4690-4700. https://doi.org/10.3390/ijerph10104690
Li X, Geng W, Tian H, Lai D. Was Mandatory Quarantine Necessary in China for Controlling the 2009 H1N1 Pandemic? International Journal of Environmental Research and Public Health. 2013; 10(10):4690-4700. https://doi.org/10.3390/ijerph10104690
Chicago/Turabian StyleLi, Xinhai, Wenjun Geng, Huidong Tian, and Dejian Lai. 2013. "Was Mandatory Quarantine Necessary in China for Controlling the 2009 H1N1 Pandemic?" International Journal of Environmental Research and Public Health 10, no. 10: 4690-4700. https://doi.org/10.3390/ijerph10104690