IAServ: An Intelligent Home Care Web Services Platform in a Cloud for Aging-in-Place

Abstract
:
1. Introduction
2. Related Work
2.1. Ambient Intelligence (AmI)
2.2. AmI Applied in Care Services
2.3. Profiles and Personalized Services
2.4. Ontology-Based Approach for Knowledge Intensive Applications
2.5. Web Service Approach in Information Integration
3. IAServ Design and Architecture
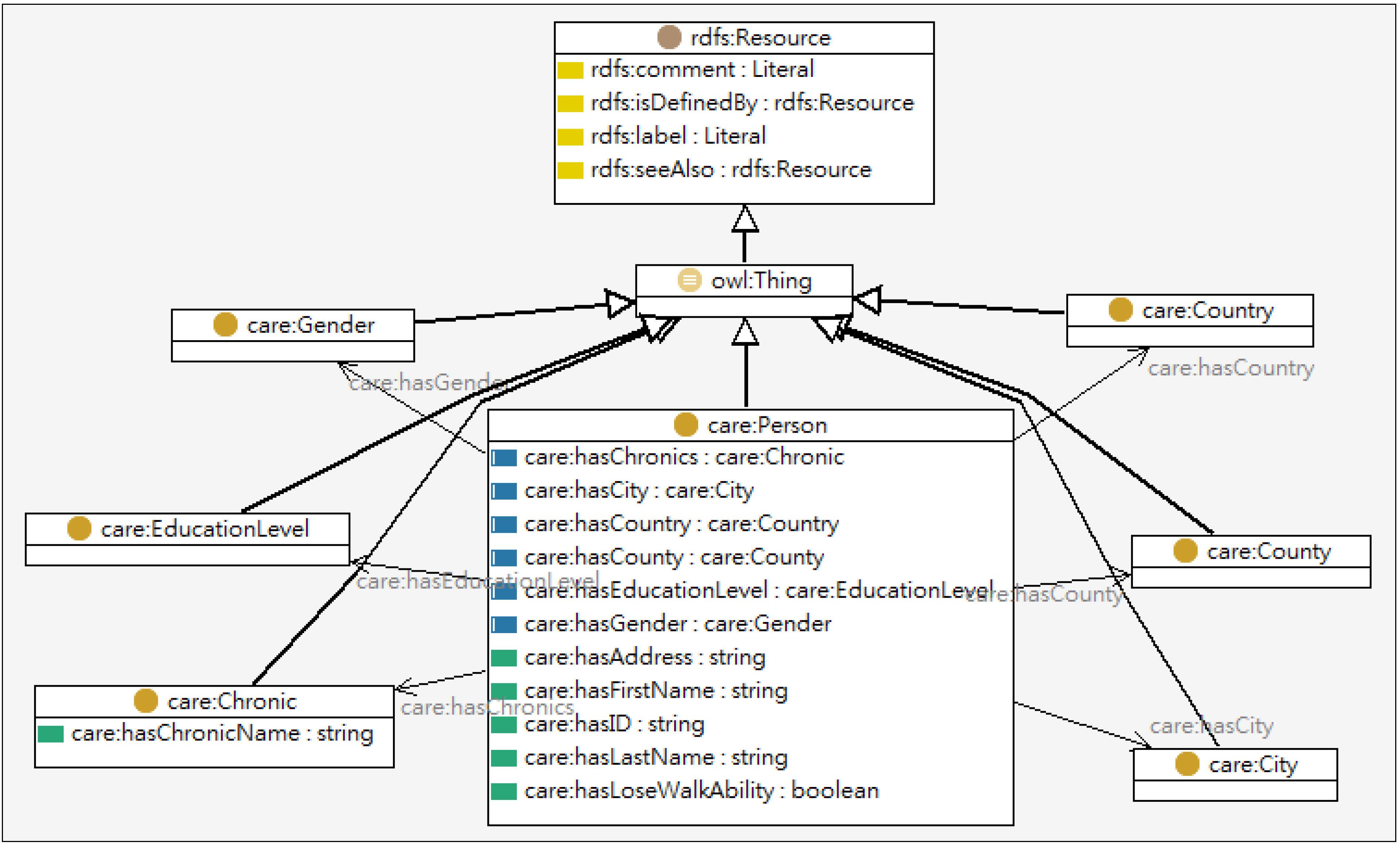
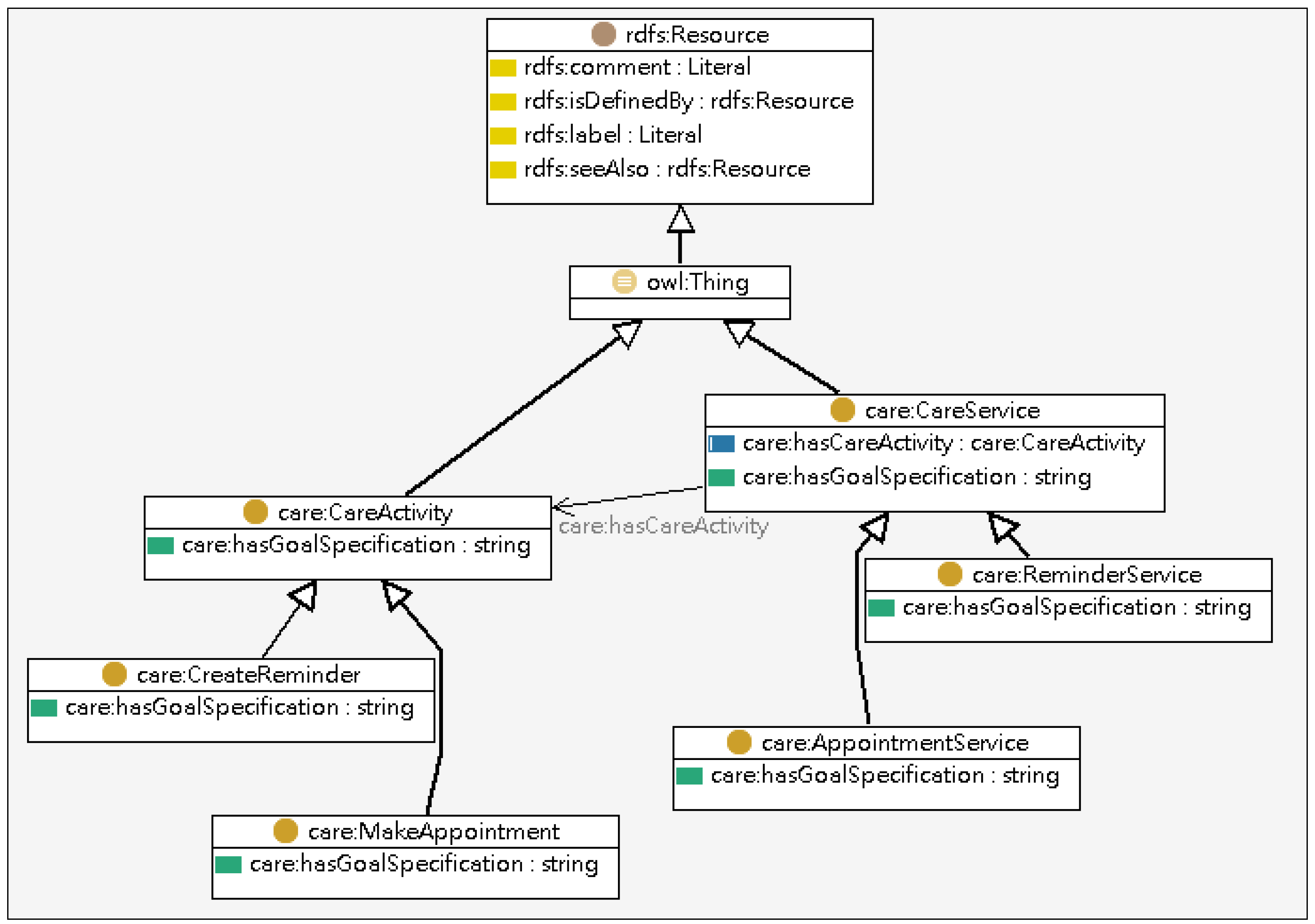
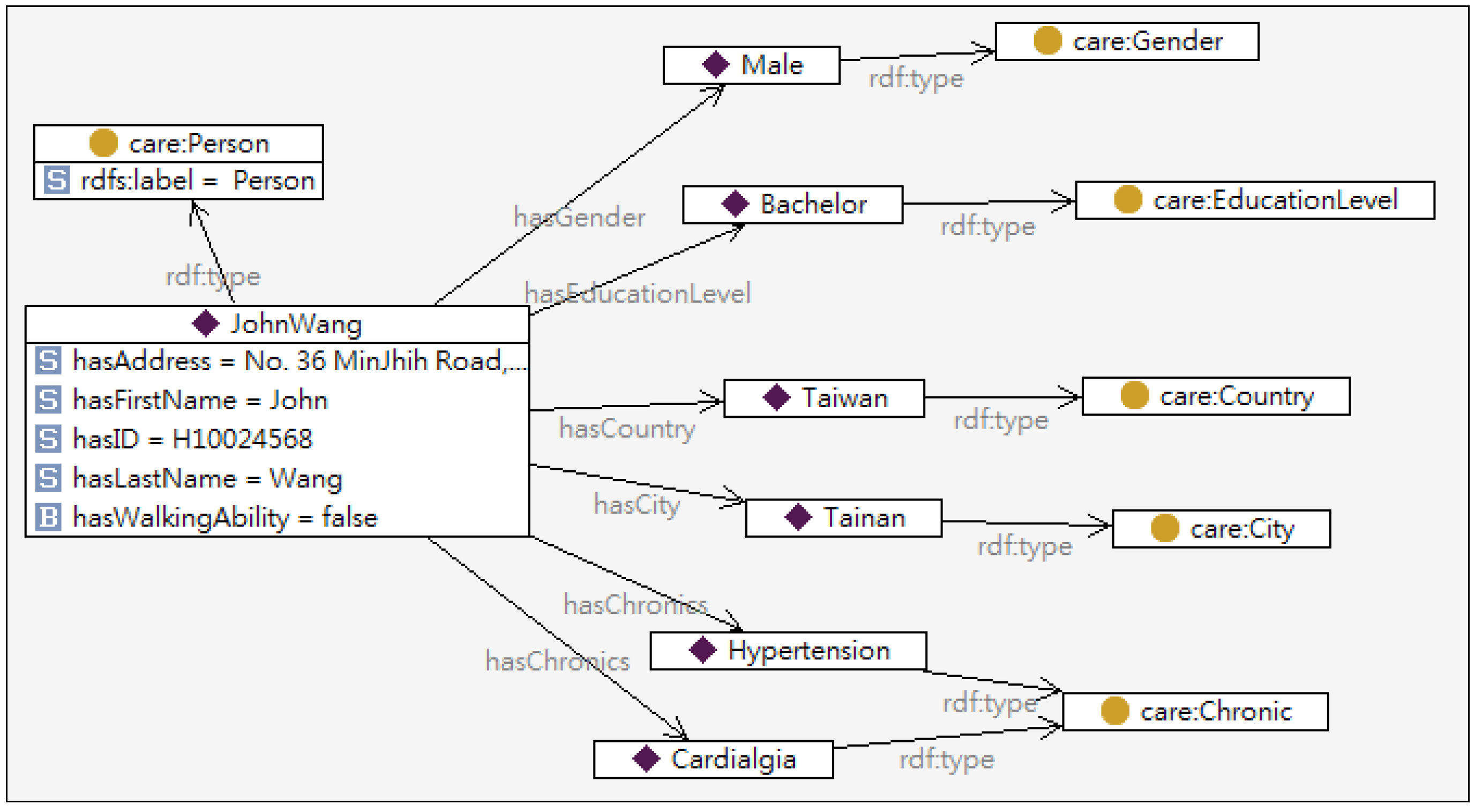
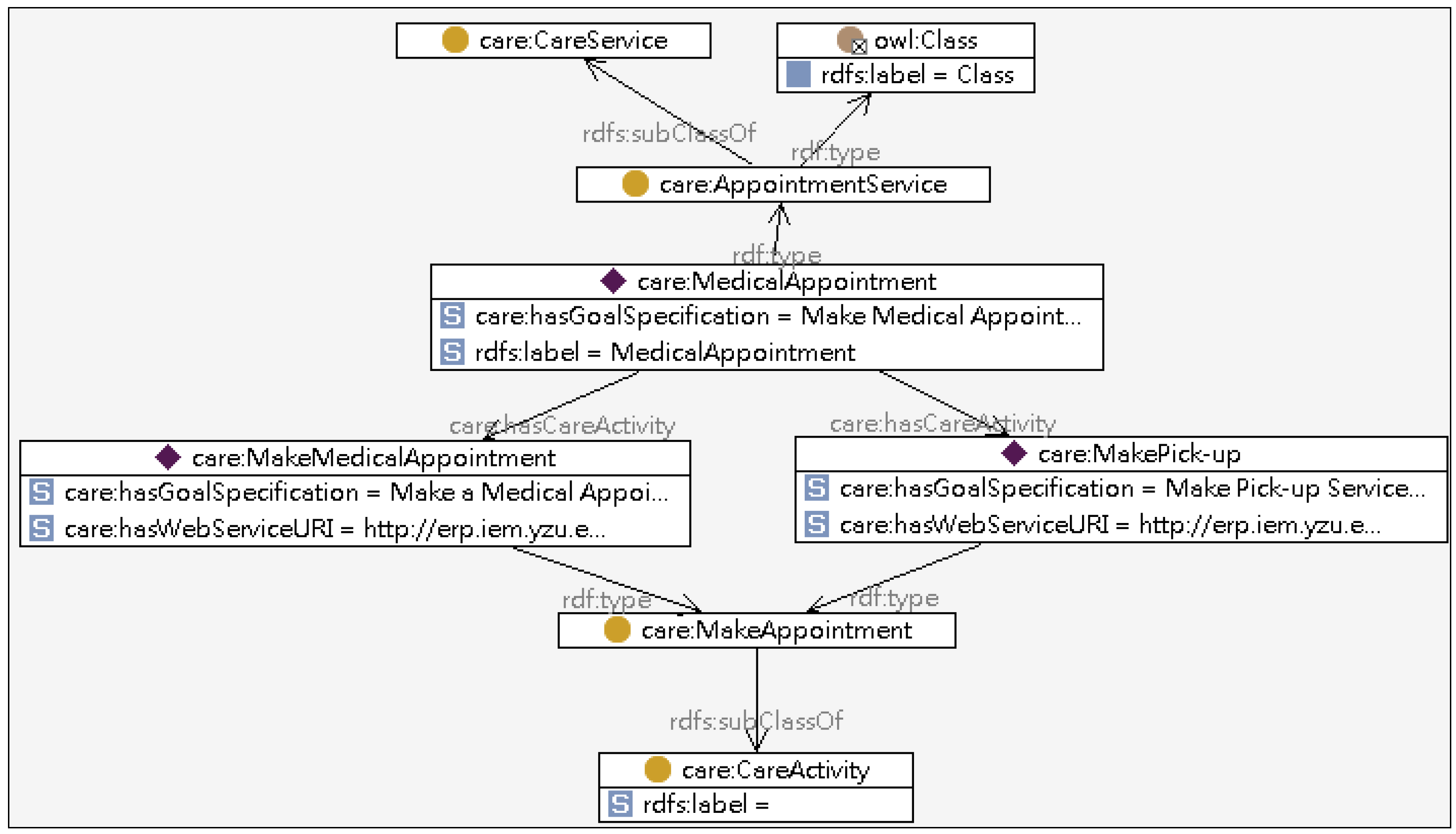
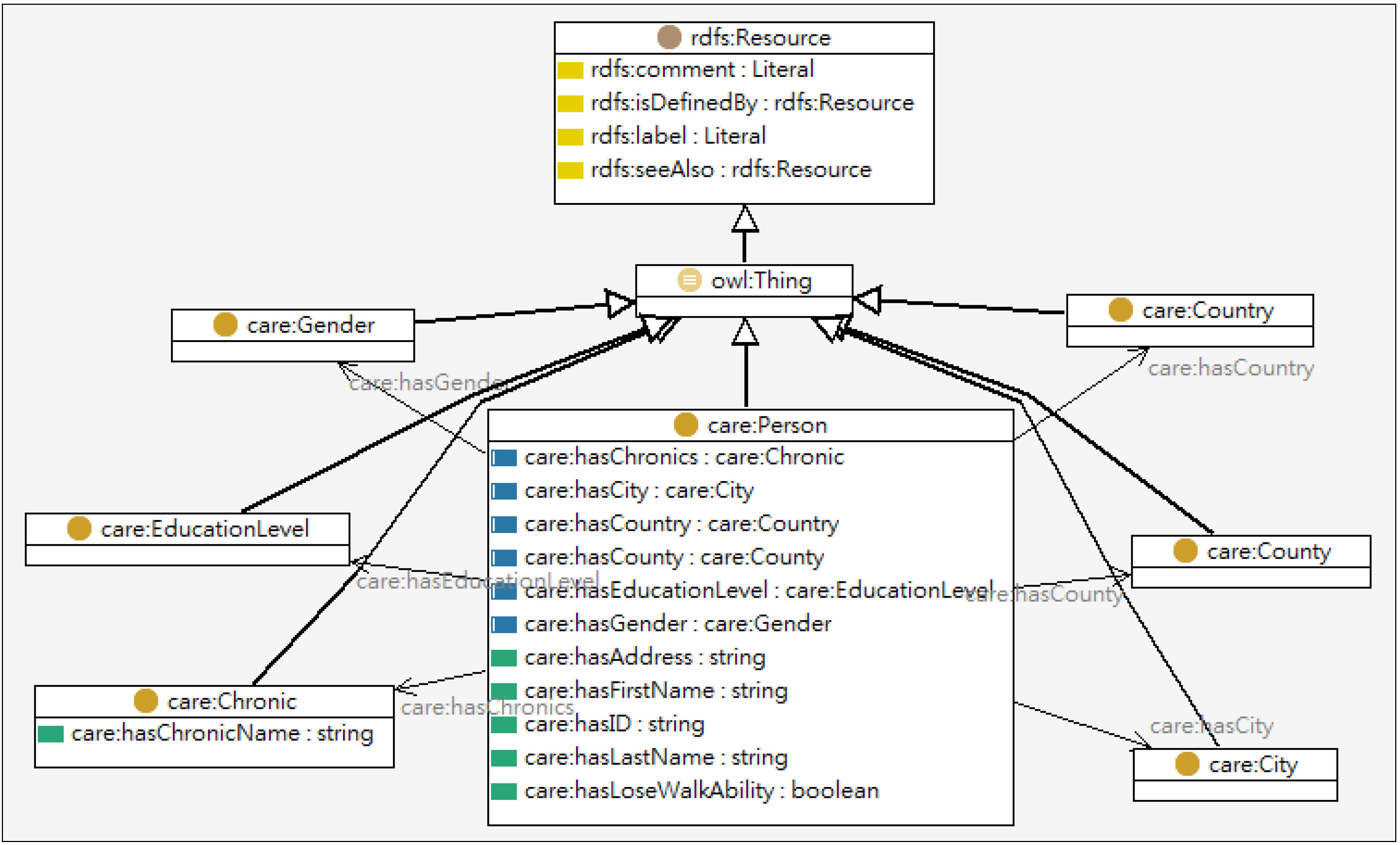
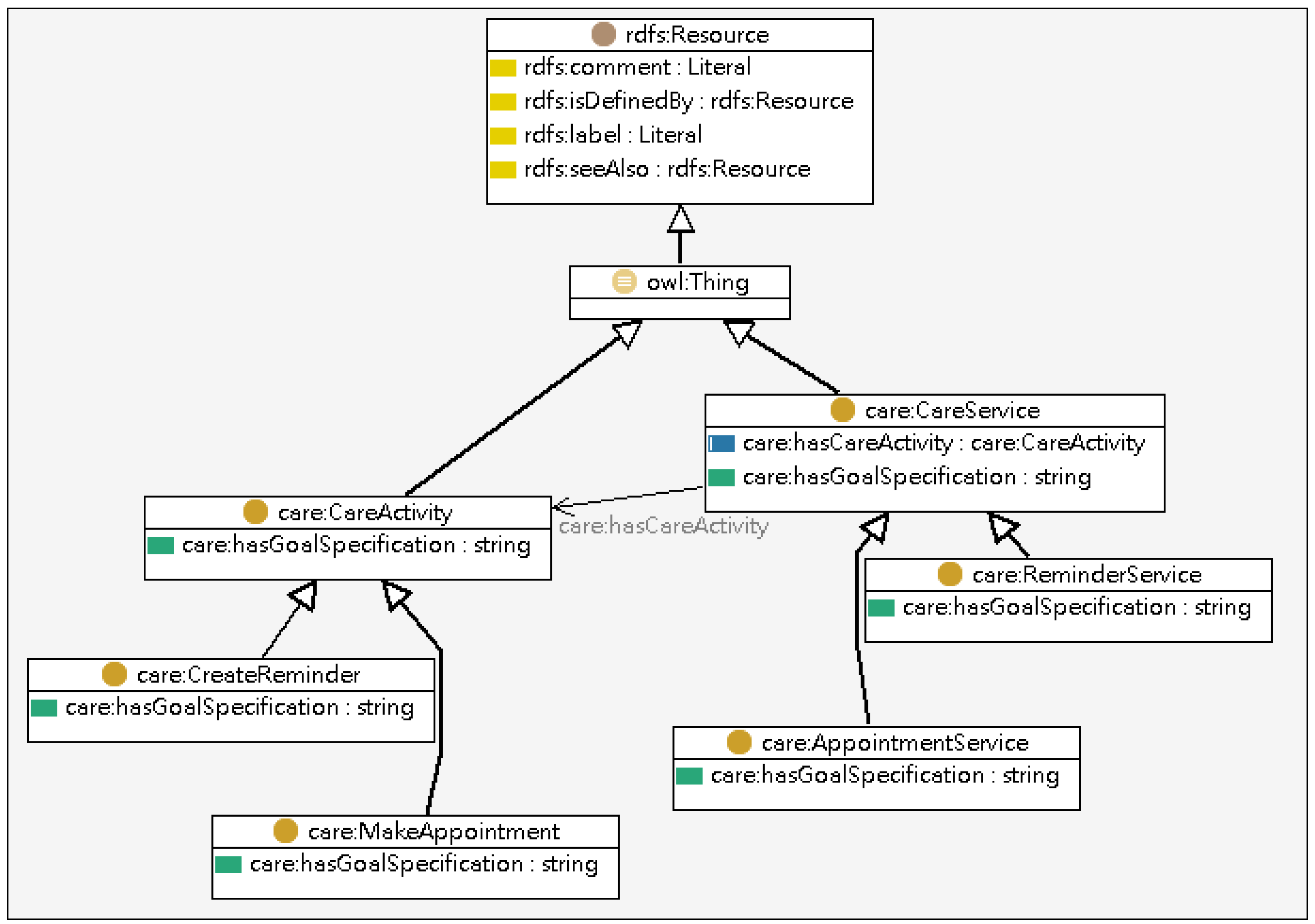
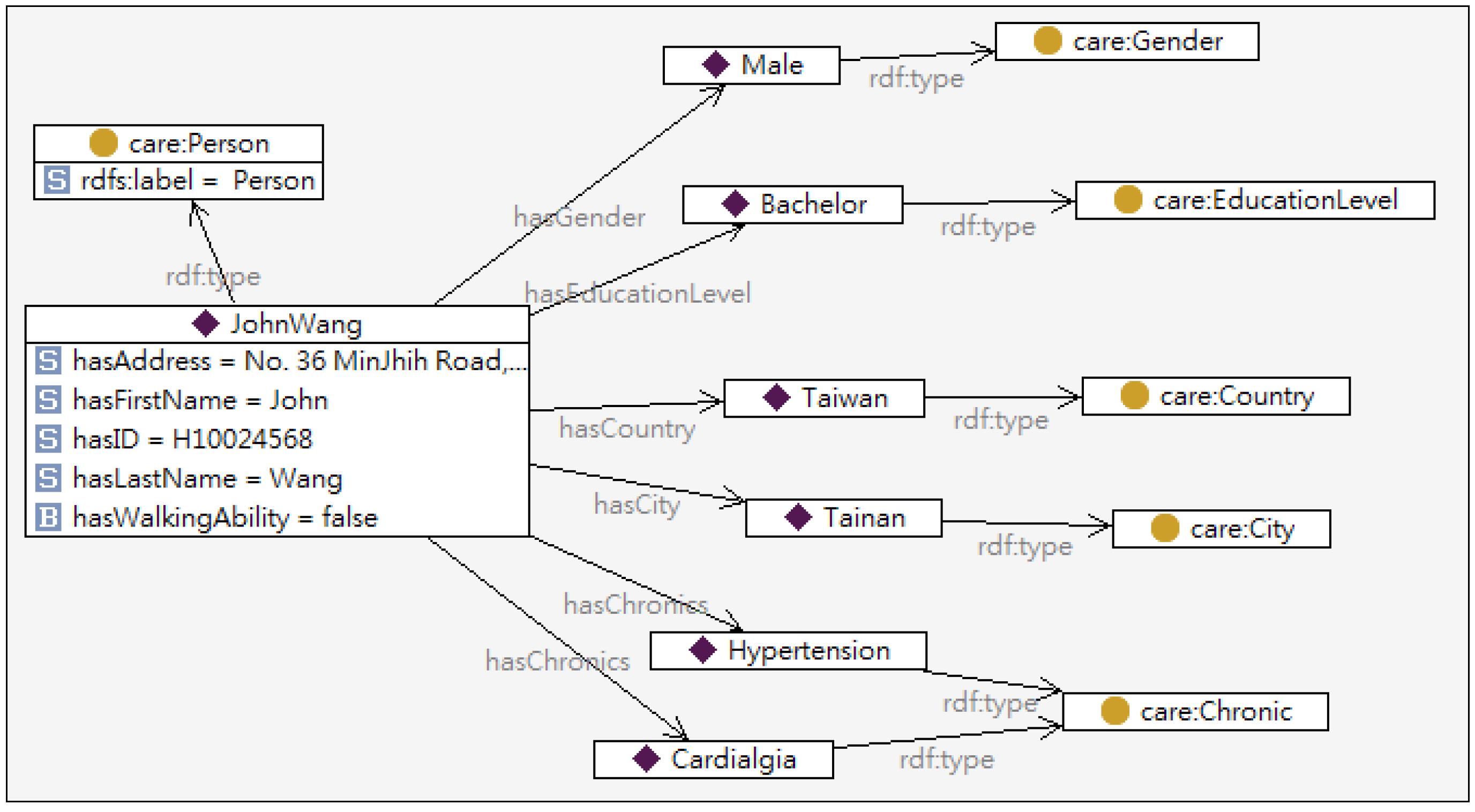
3.1. Knowledge Intensive Layer

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | Annotation |
|---|---|
| Person | Basic user information (e.g., name, sex, age, etc.) |
| Characteristics | General user characteristics (e.g., height, weight, etc.) |
| Ability | User abilities and disabilities, both mental and physical |
| Chronic Status | User diseases (e.g., hypertension, hemorrhagic stroke) |
| Living Conditions | Information relevant to the user’s residence |
| Contact | Other persons, with whom the person is related (e.g., including relatives, friends, co-workers) |
| Preferences | User preferences (e.g., love cats, prefer blue color, dislike classical music) |
| Interests | User hobby or work-related interests. For example, “interested in sports”, “interested in cooking” |
| Activity | User activities, hobby or work related |
| Education | User education issues, including for example university diplomas and languages |
| Profession | The user’s profession |
| Expertise | computer, Internet, mobile devices, etc. |
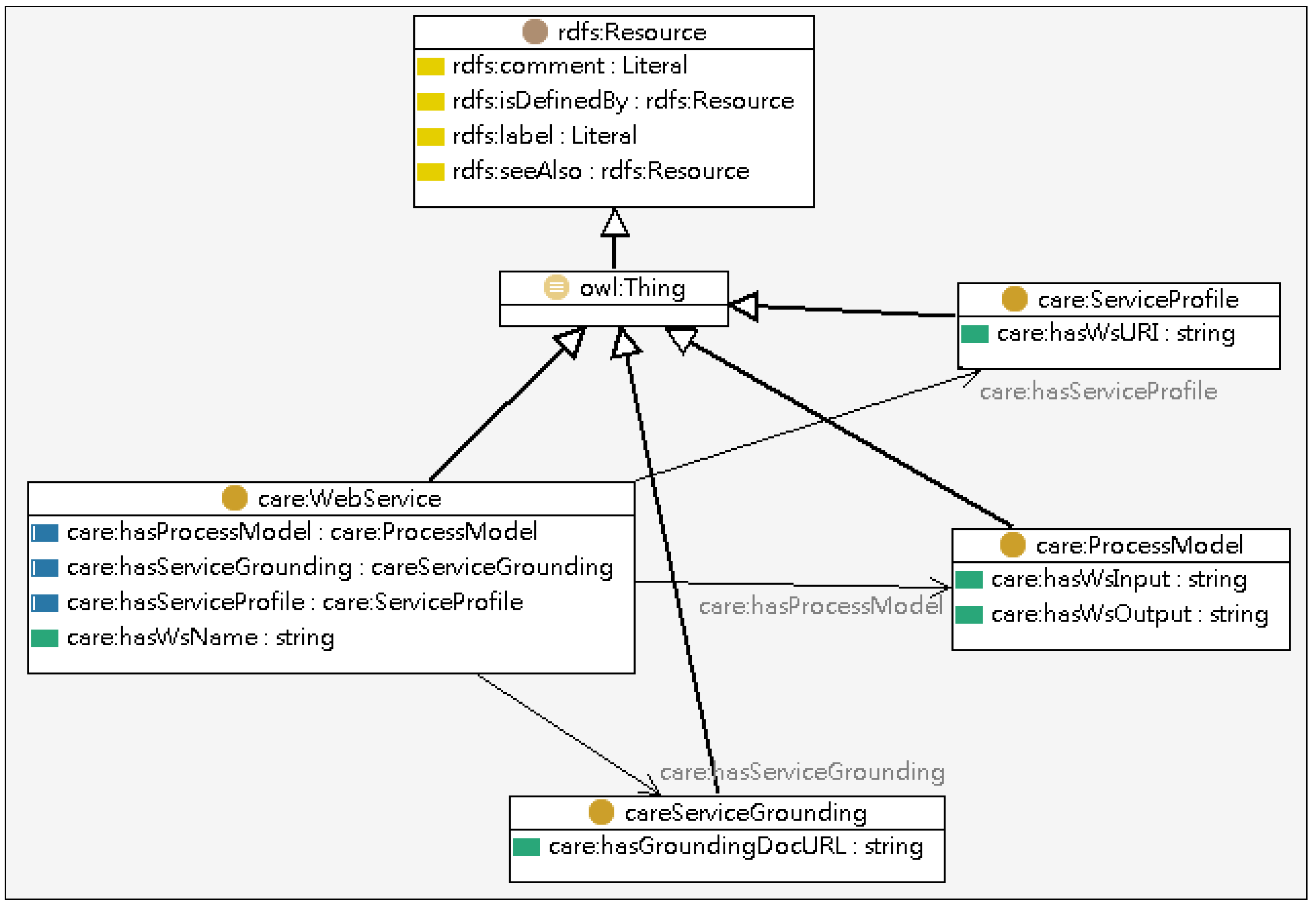
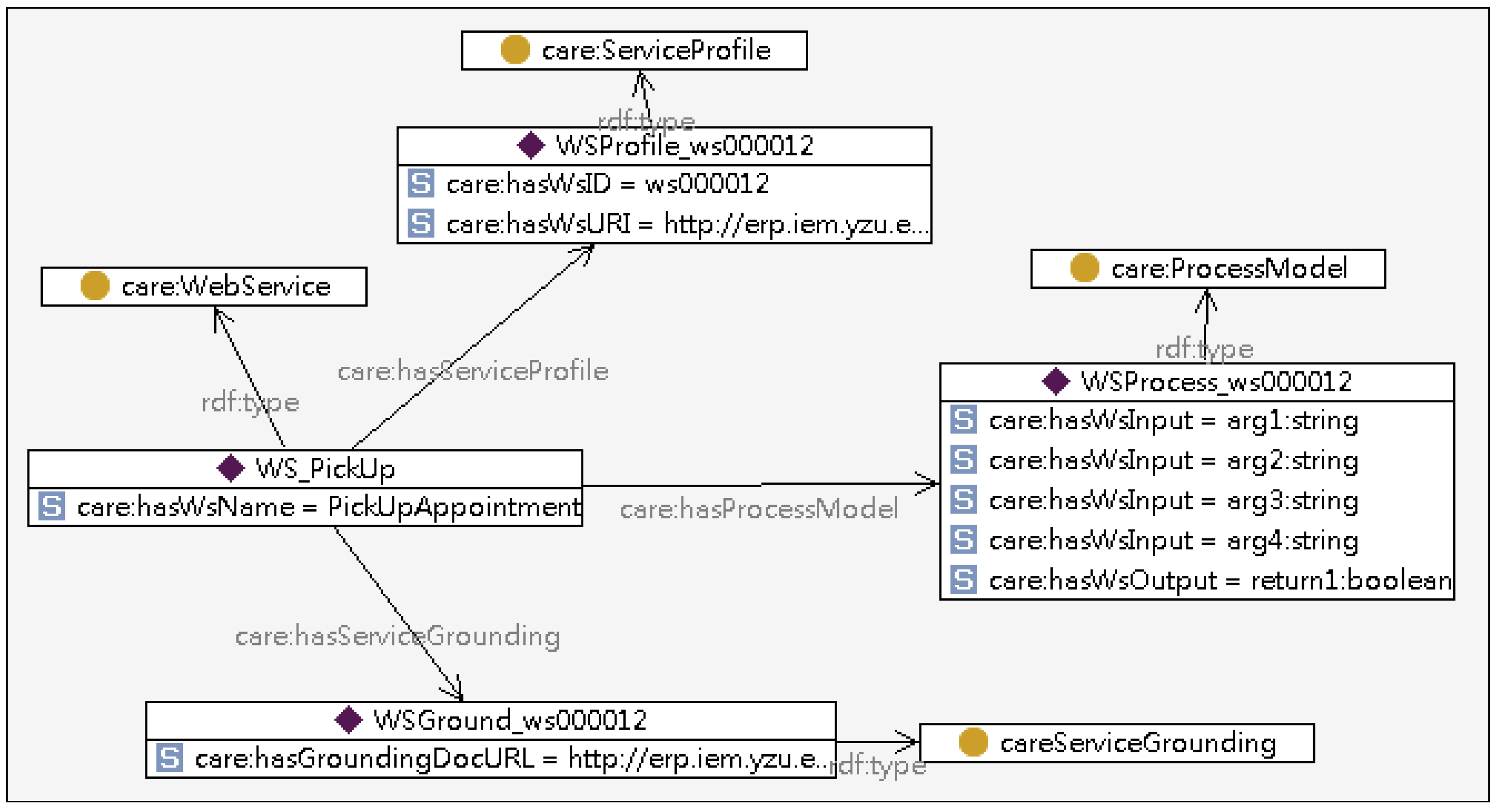
| Class | Description |
|---|---|
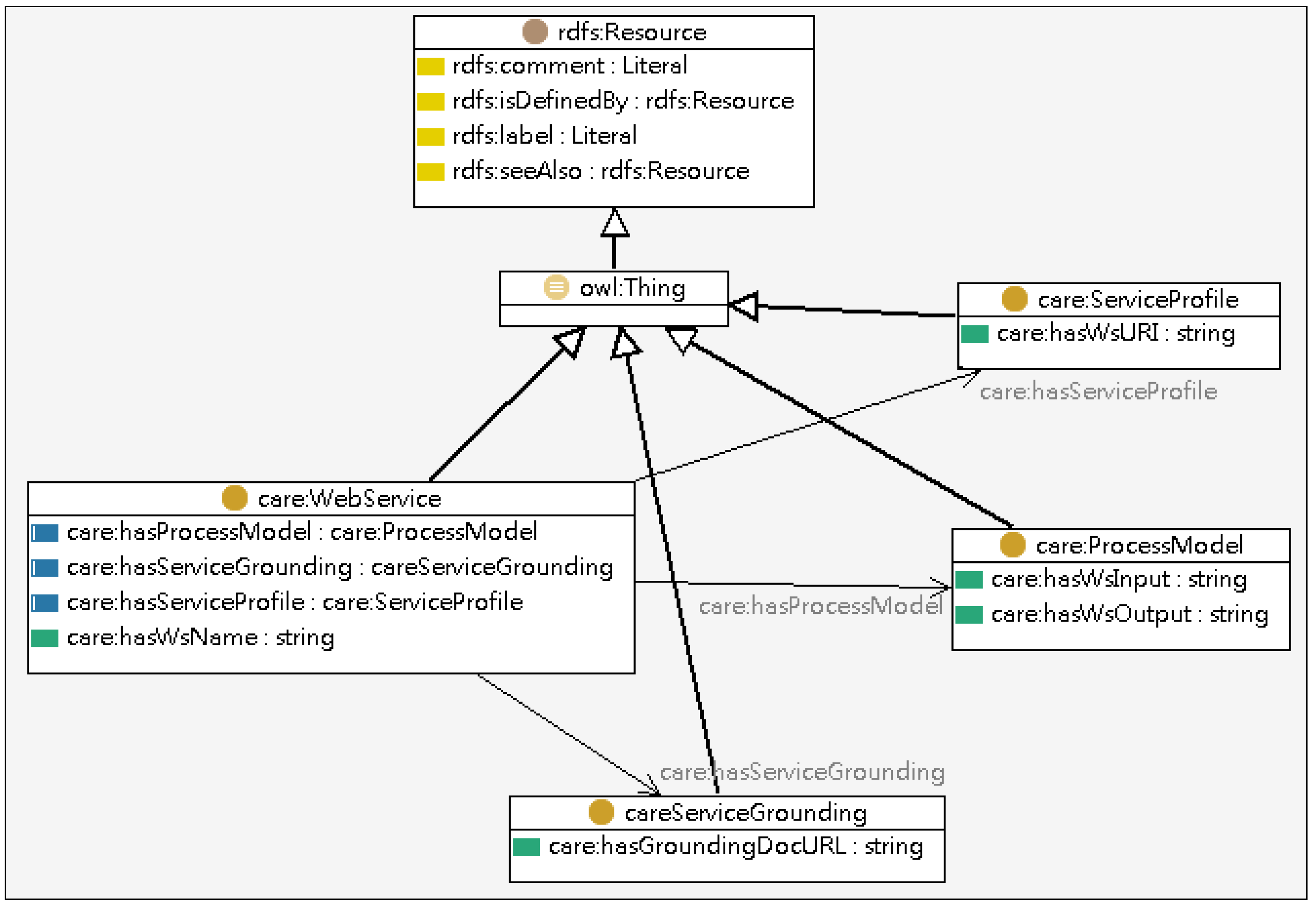
| Service Profile | Includes service name and parameter annotations. |
| Process Model | Includes information, including input (input type), output and local. |
| Service Grounding | Defined by WSDL (Web Services Definition Language) 2.0 operations. |
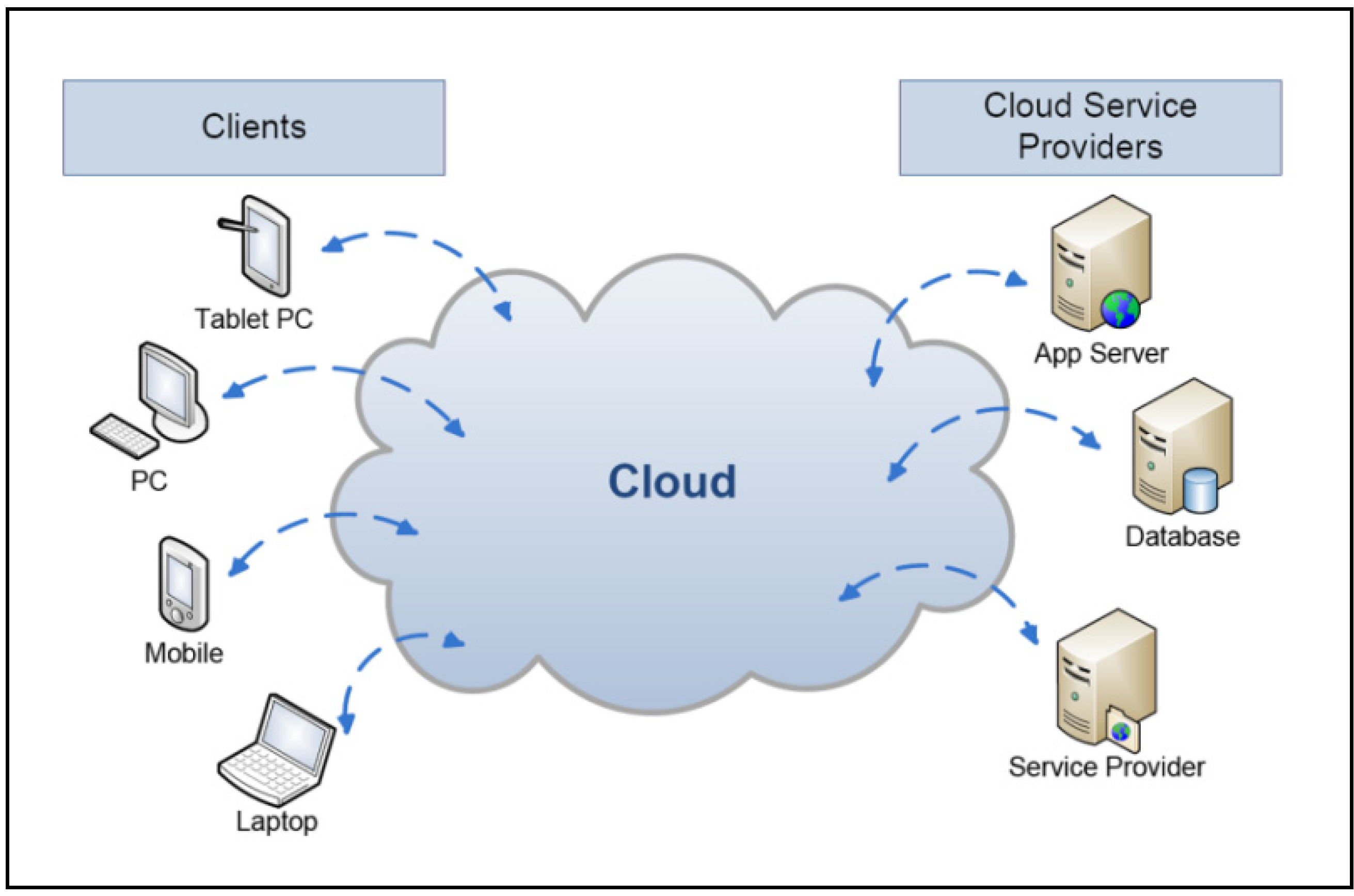
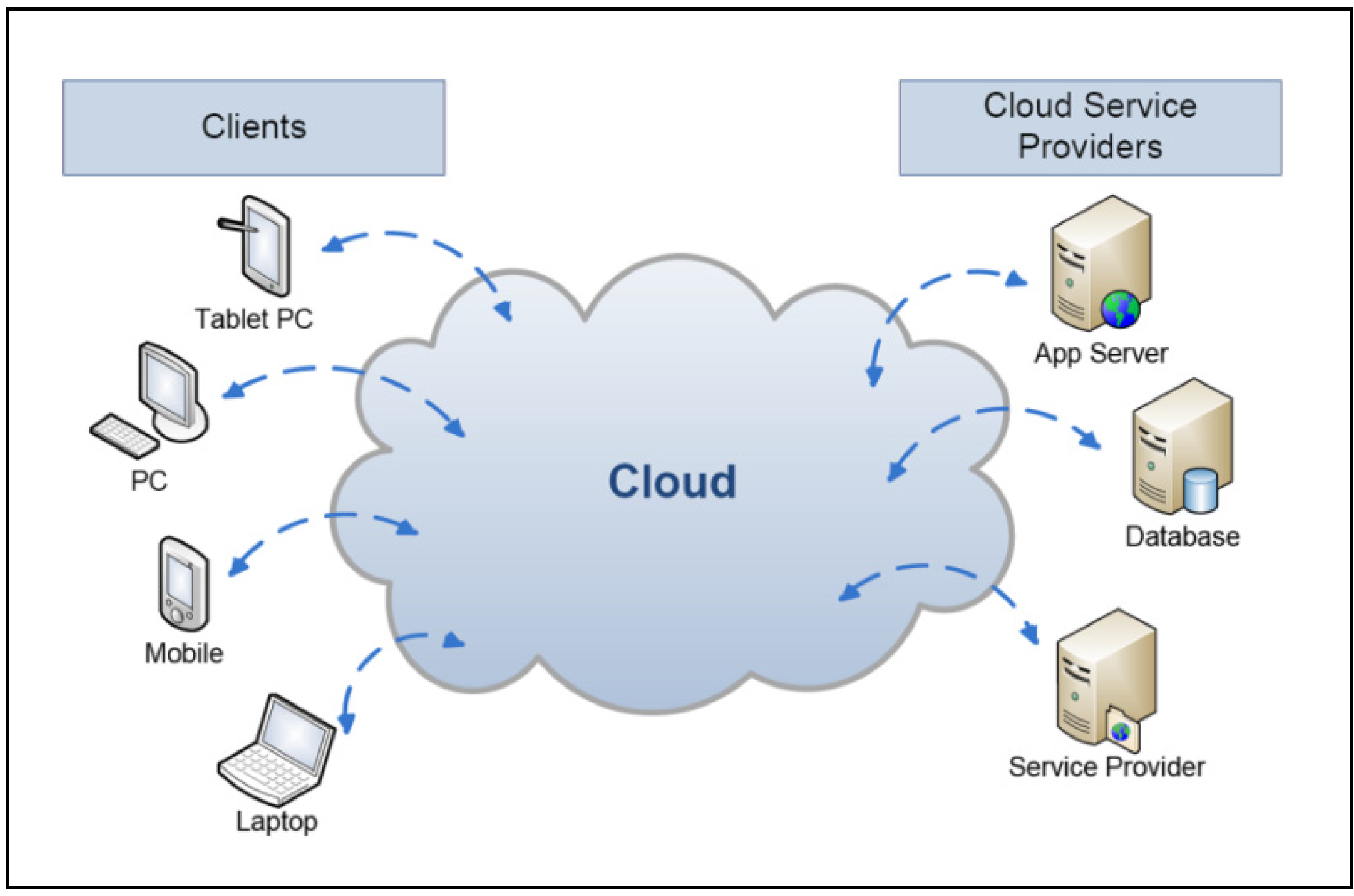
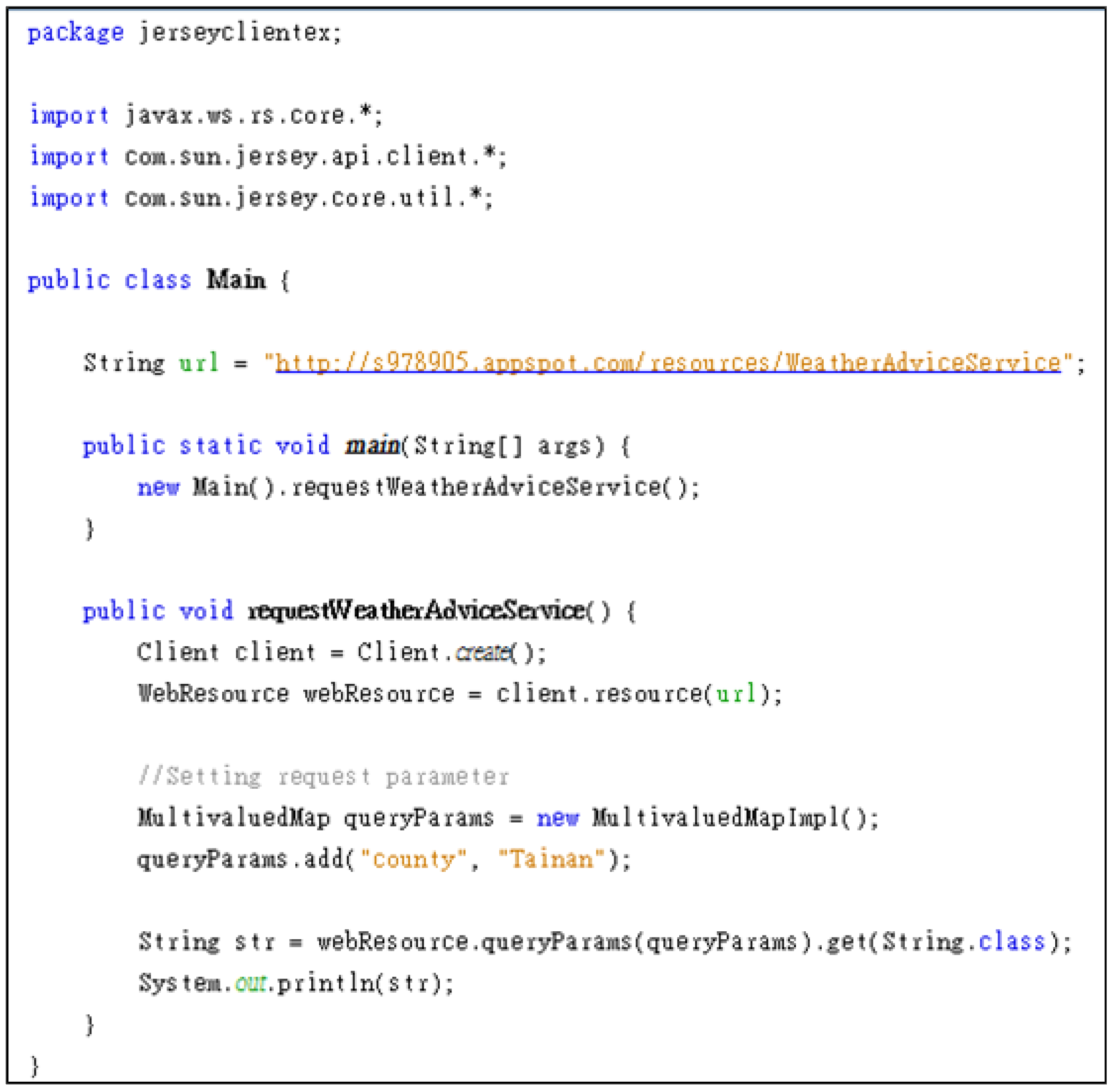
3.2. Web Service in the Cloud
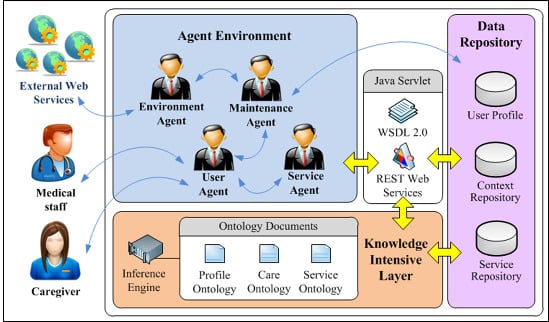
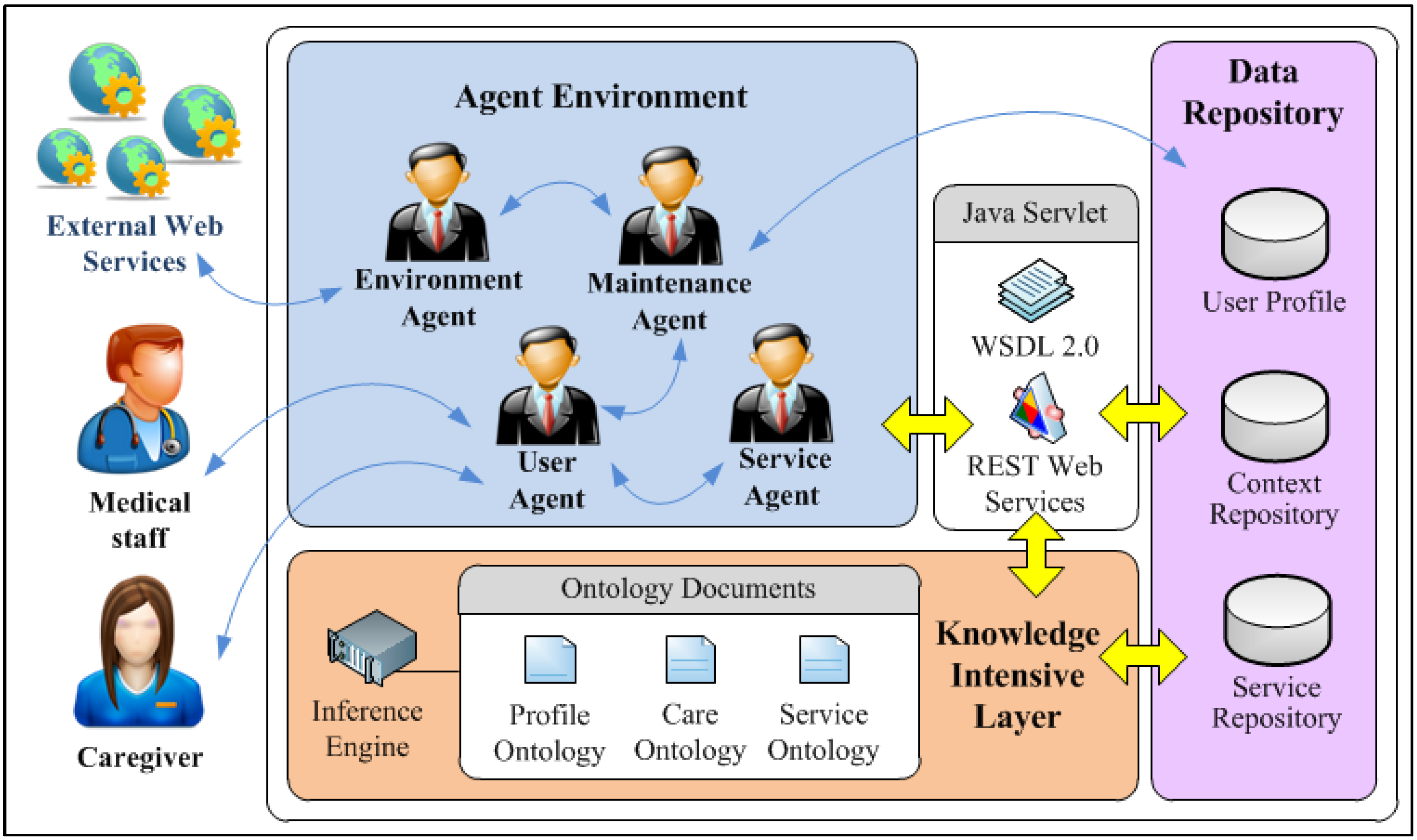
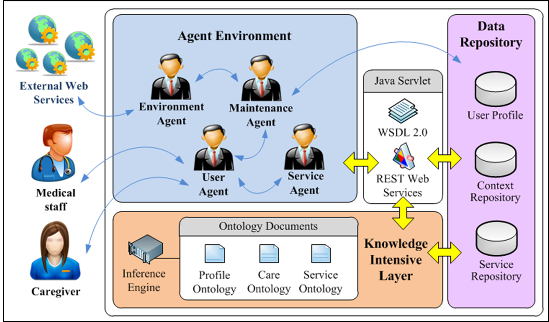
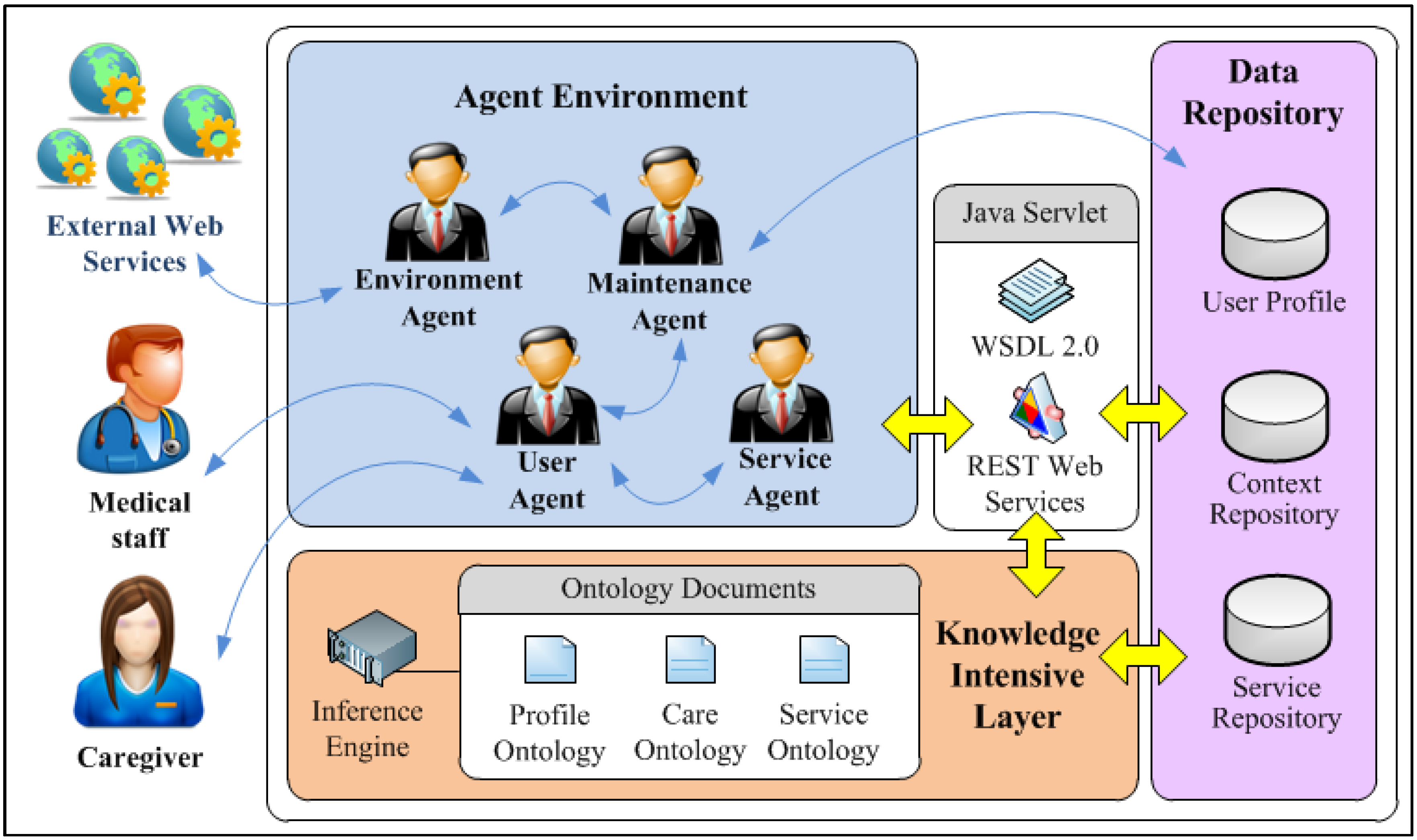
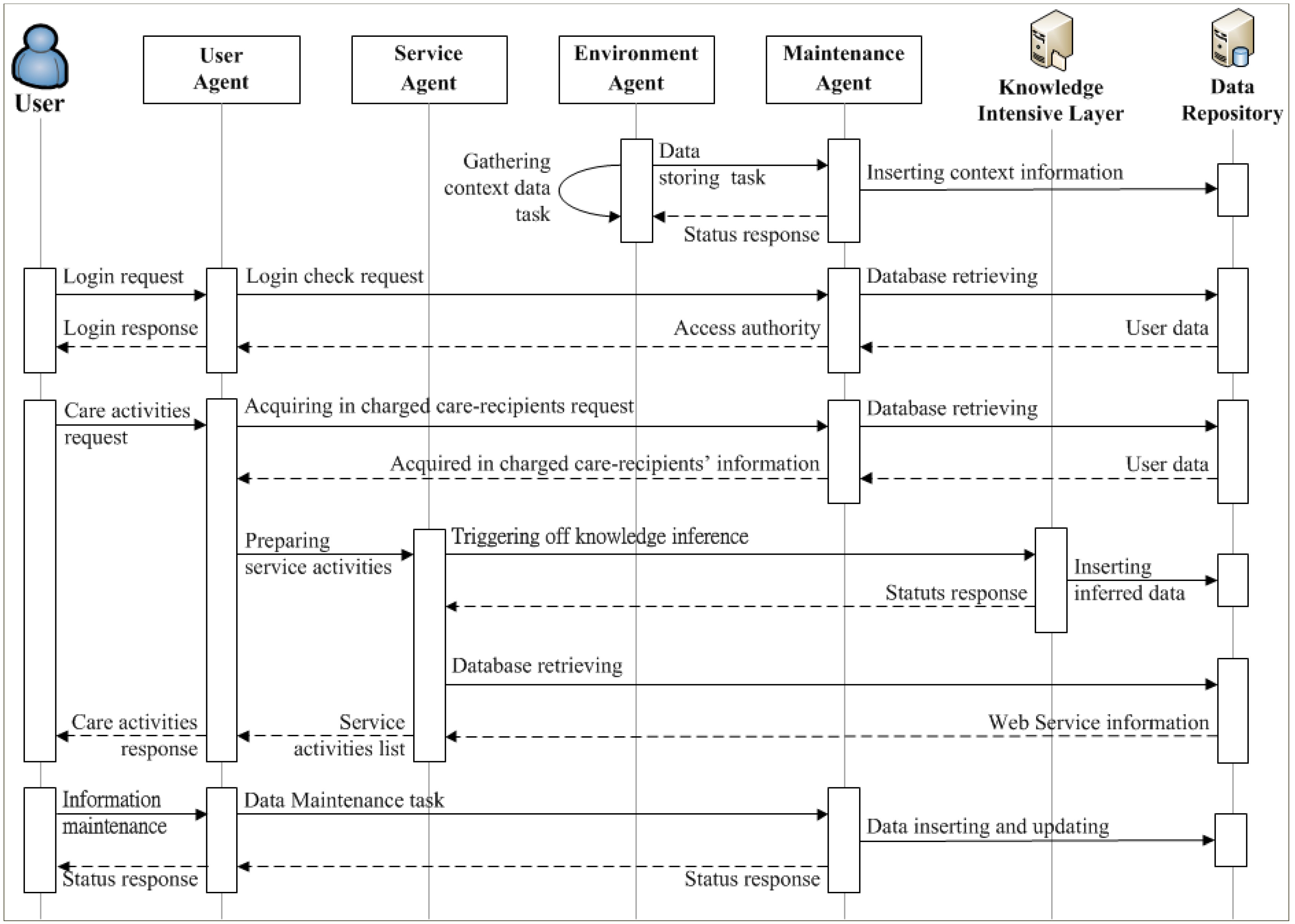
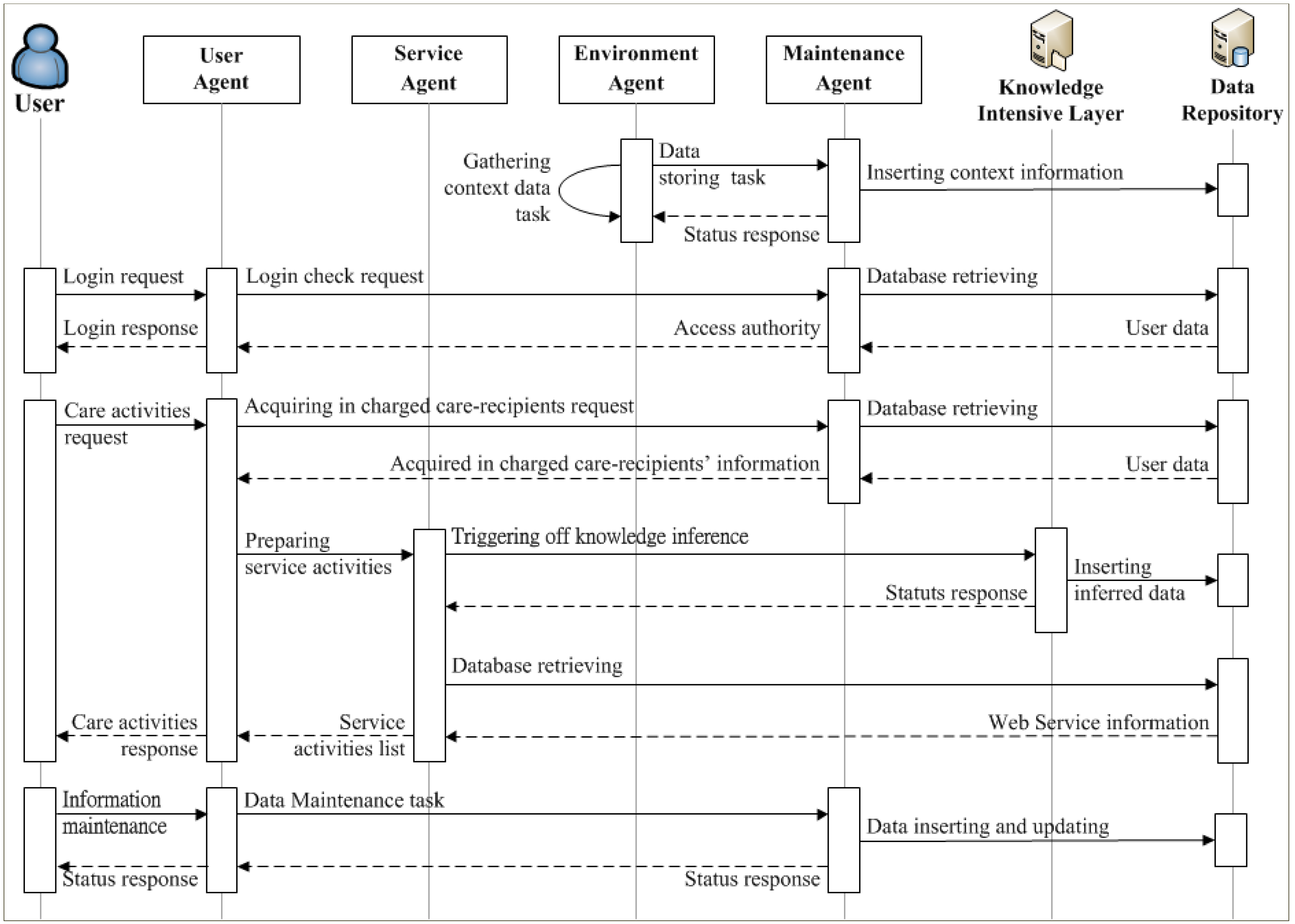
3.3. Agent Environment
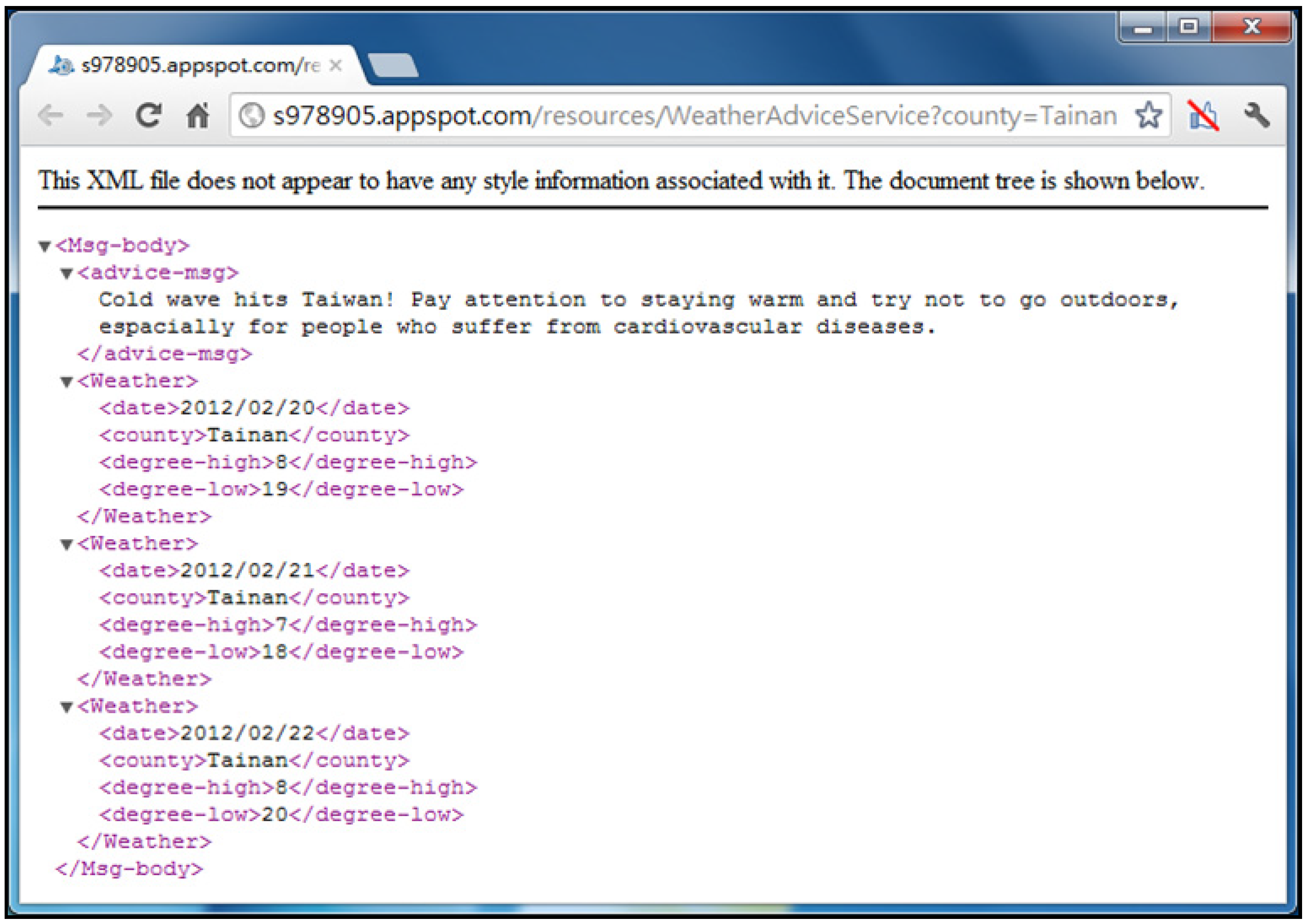
- Environment Agent: The Environment Agent is responsible for managing the environmental data (e.g., temperature, humidity, location, etc.). It works with the Context Repository and connects with the External Web Services to collect the environmental data from sources such as Yahoo! Weather [51], and stores the data into the Context Repository. When performing contextually relevant services, the Environment Agent offers the corresponding contextual data to the Service Agent for the provision of contextually-aware services.
- Service Agent: The Service Agent is designed to monitor the implementation of the personalized care plan. When it detects the scheduled care plan, it will use contextual data to prepare information from relevant web services and subsequently delegate task execution to the User Agent.
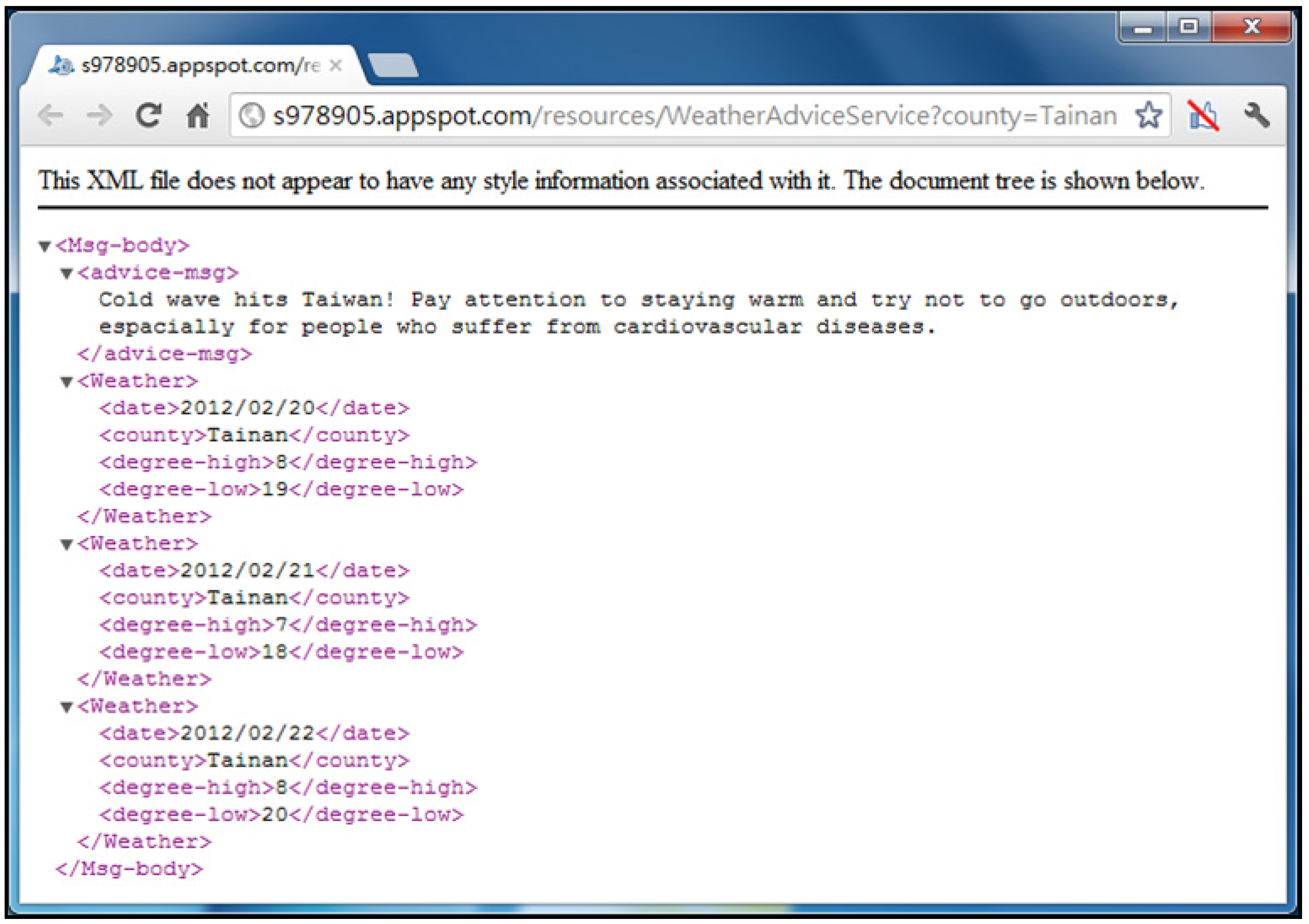
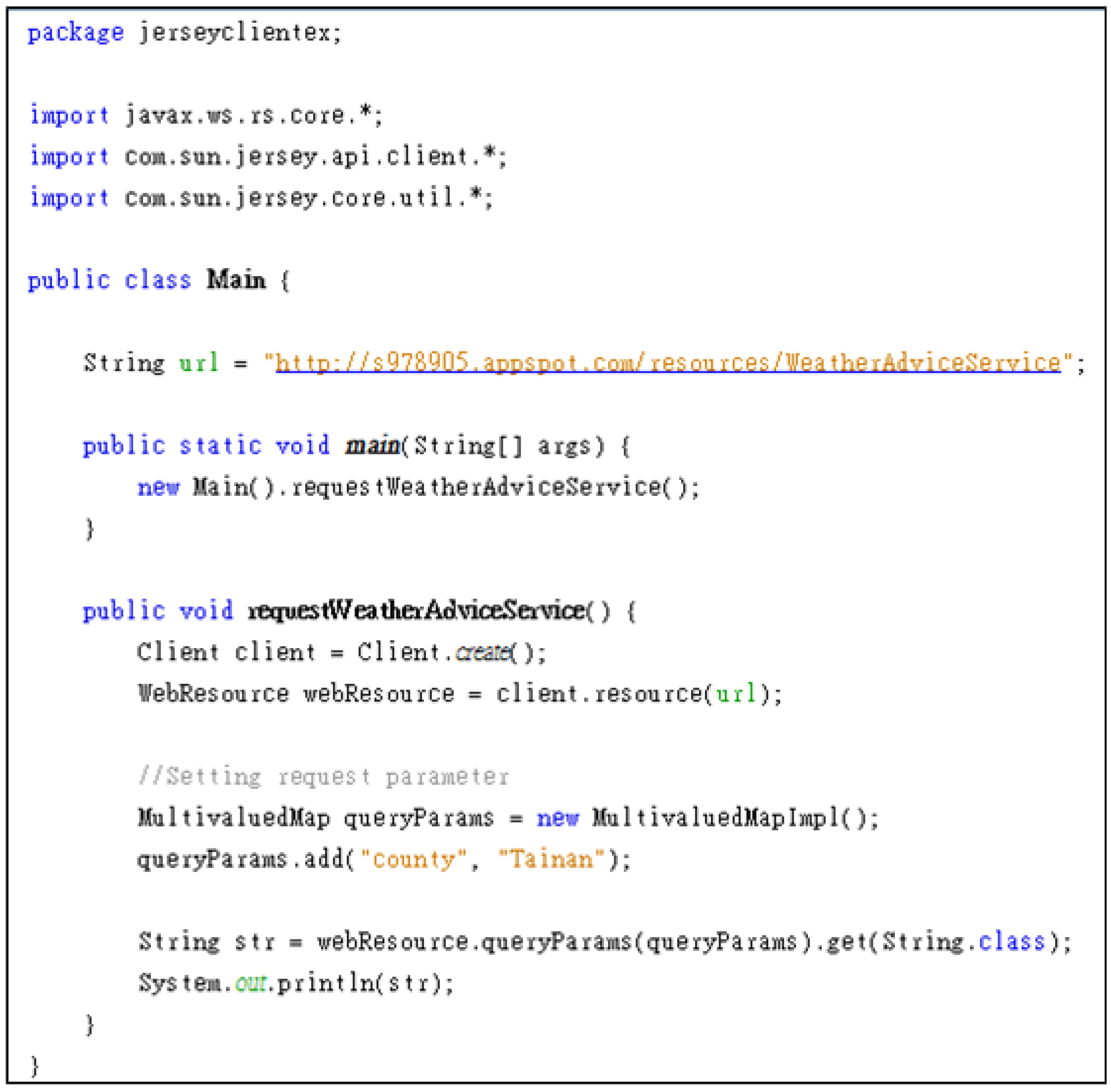
- User Agent: The User Agent is responsible for accessing the web service and performing the care services on behalf of patients when it receives tasks from the Service Agent. Following data provided by the Service Agent, the User Agent makes a request to the web service with the needed input data parameters via the HTTP protocol. The resulting information is then published to the user’s device by the User Agent to complete the care service.
- Maintenance Agent: Expert knowledge and patient conditions and experience may change over time. These changes can be accommodated appropriately in the ontologies through the Maintenance Agent. The Maintenance Agent plays an important role in dealing with the dynamic aspects of the health care environment. It allows experts to update the knowledge, instances, and rules encapsulated in the ontologies, as illustrated in Figure 10.
3.4. Data Repository
4. Implementation
4.1. Hardware and Software Configuration
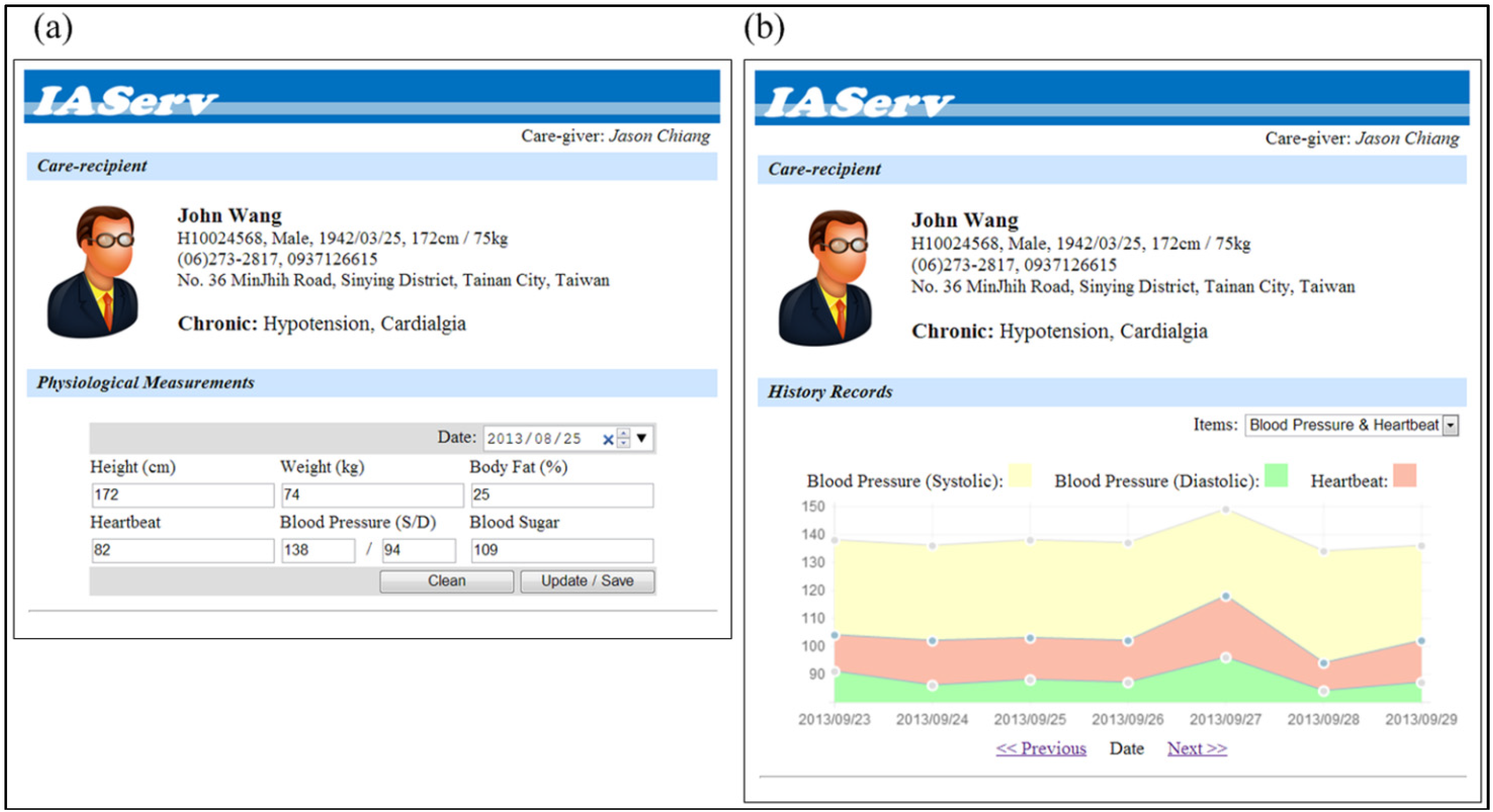
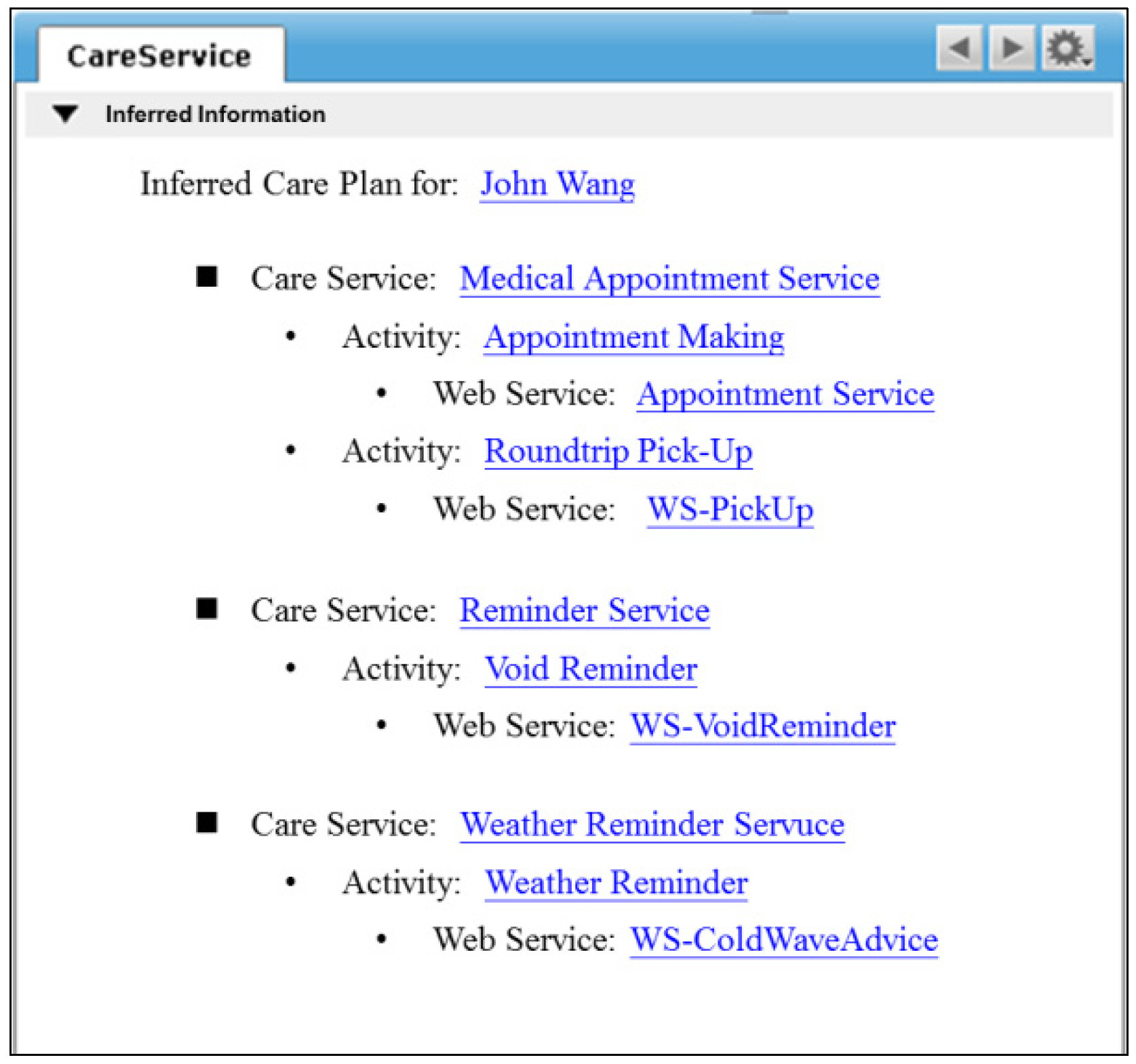
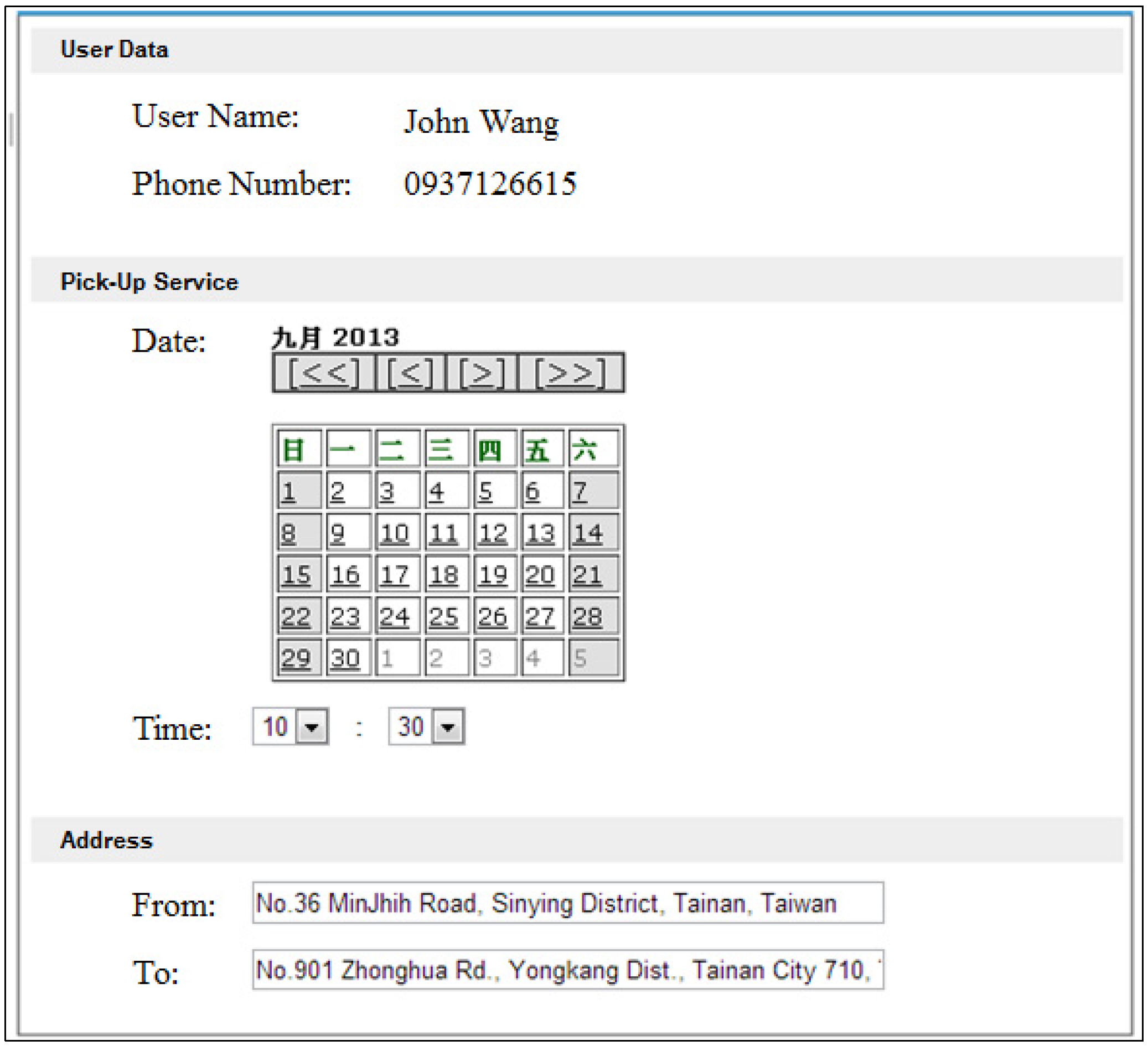
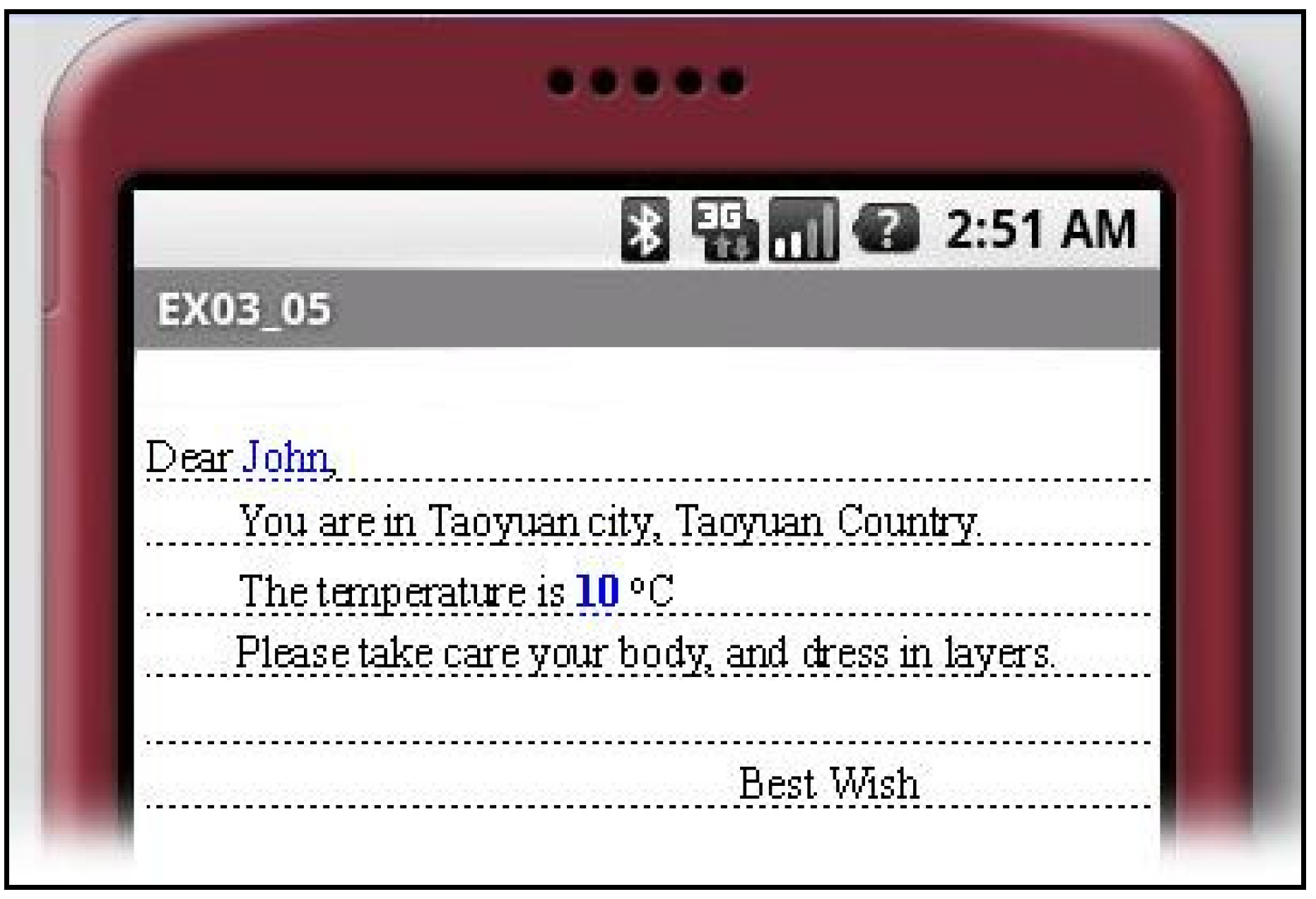
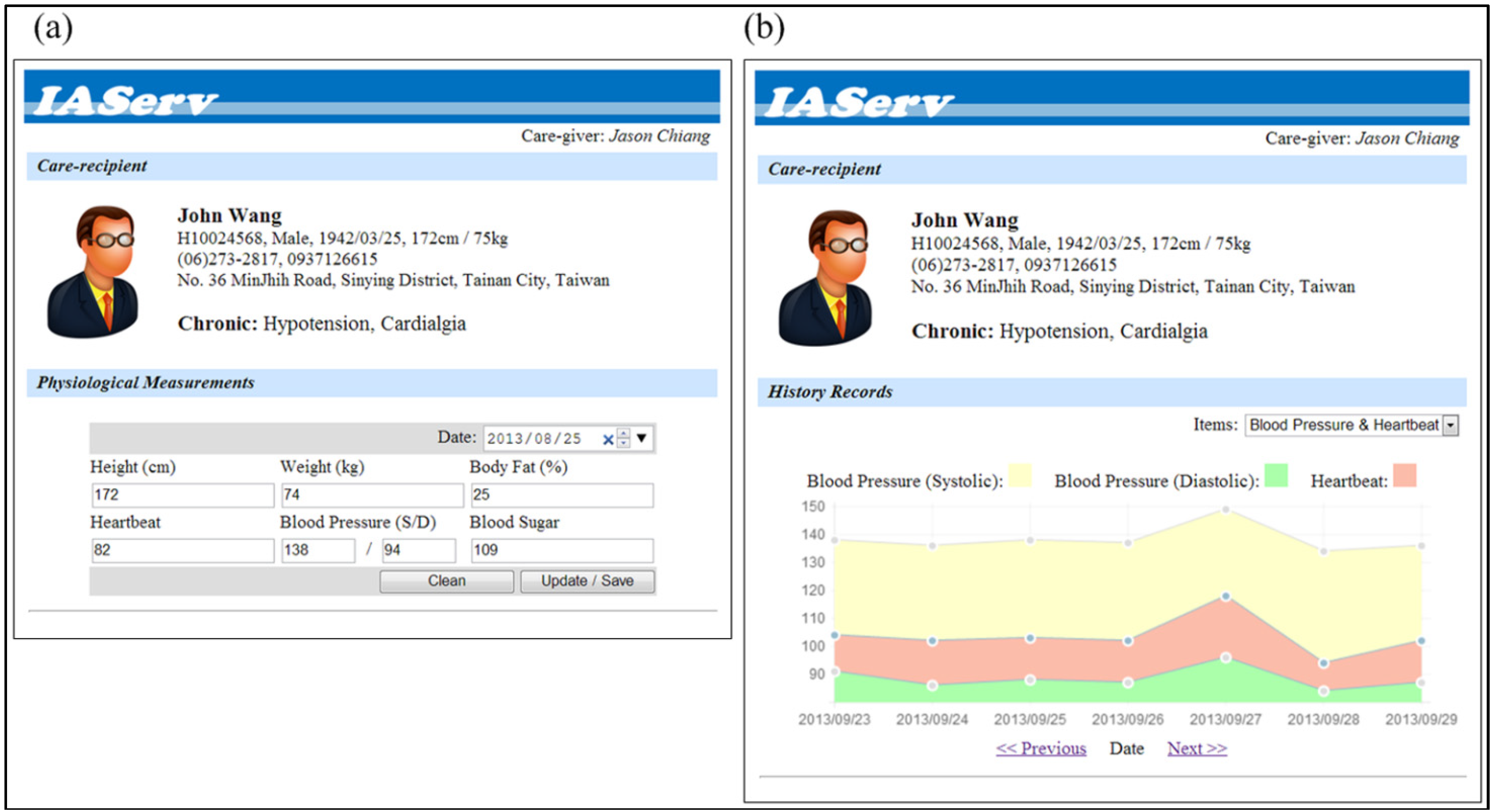
4.2. Usage Scenario and Demonstration


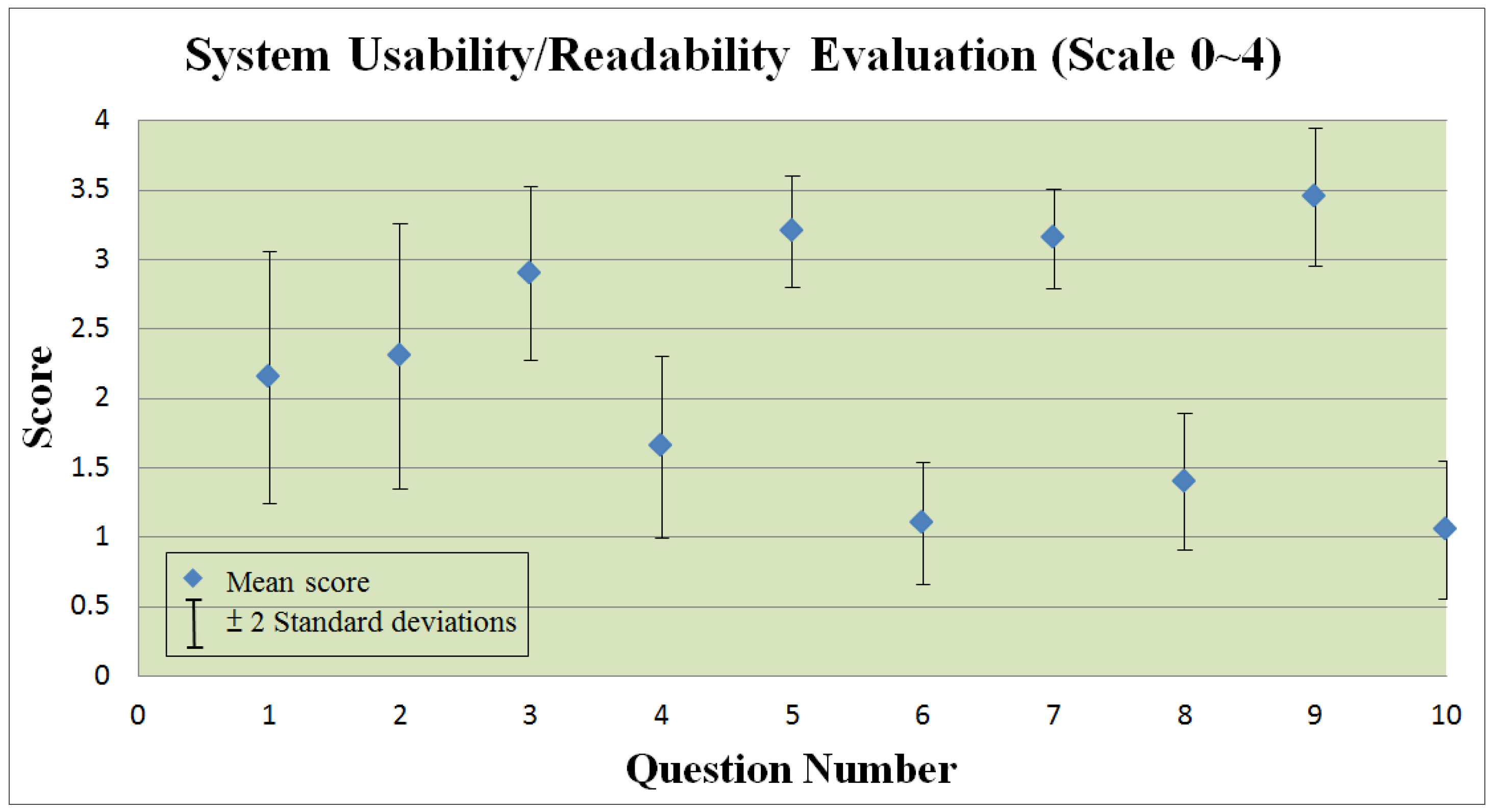
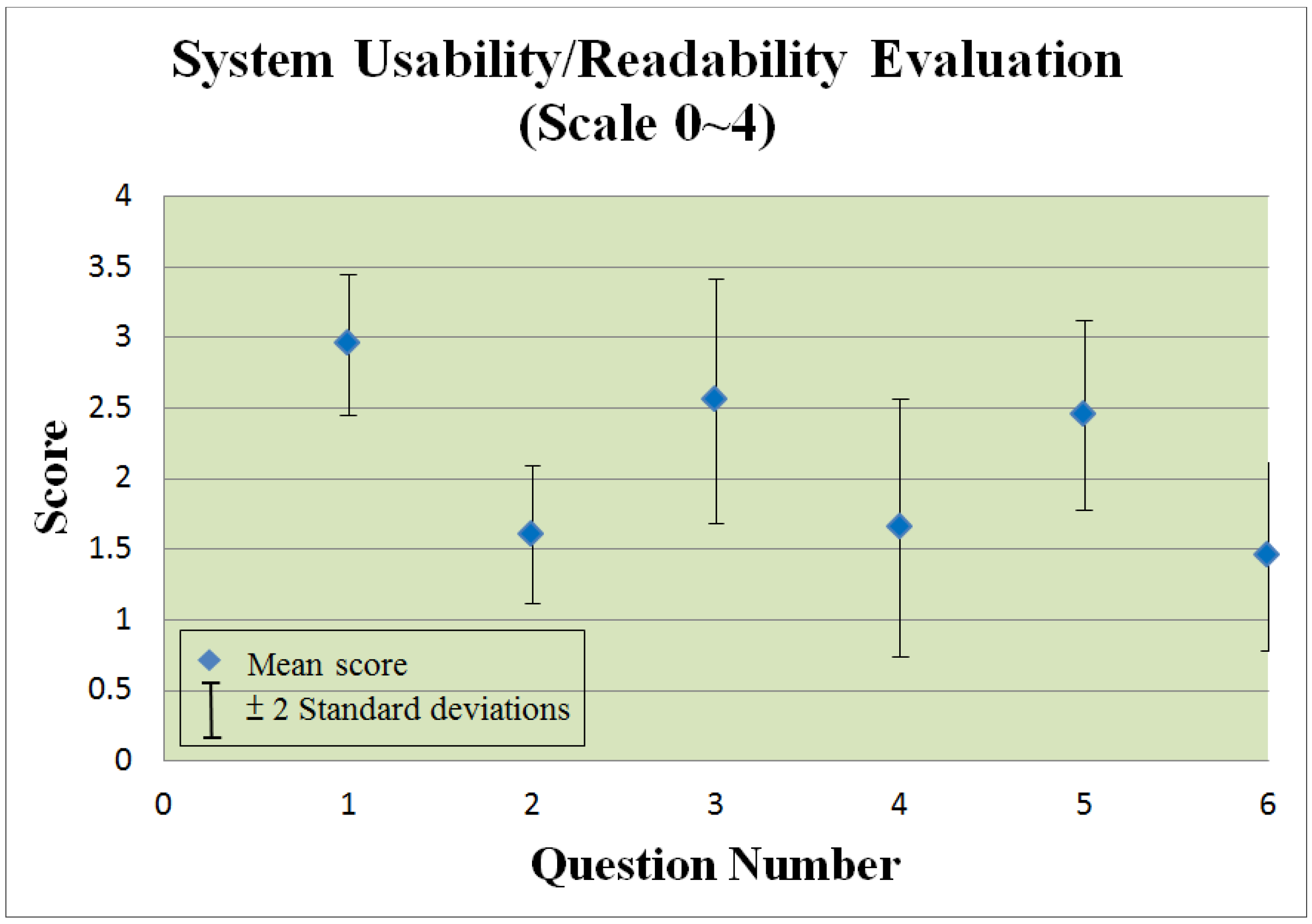
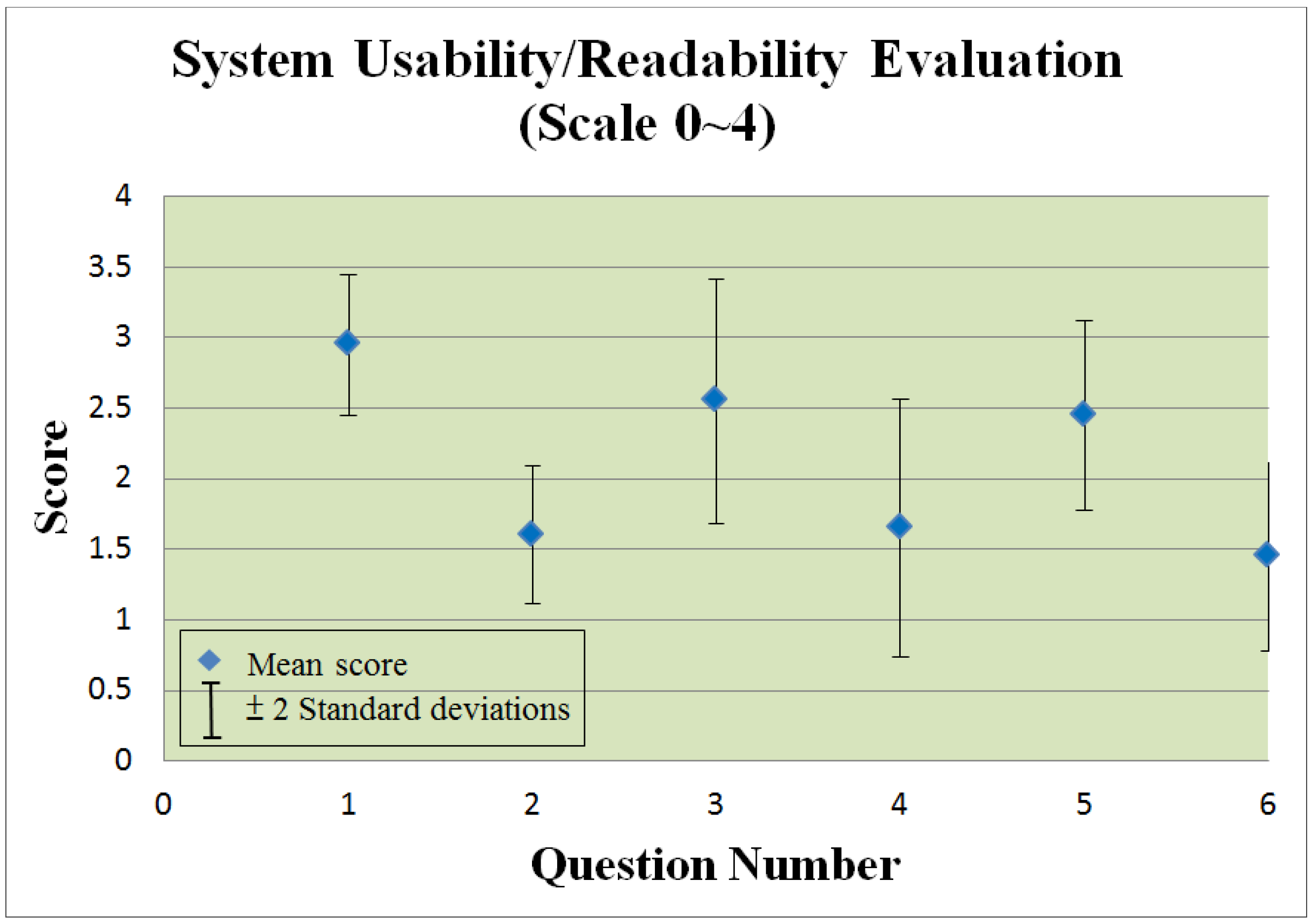
4.3. System Usability Evaluation
| Personal information | Number | % |
|---|---|---|
| Age | ||
| 20–30 | 4 | 20.0 |
| 30–40 | 13 | 65.0 |
| 40 or above | 3 | 15.0 |
| Total | 20 | 100.0 |
| Gender | ||
| Male | 8 | 40.0 |
| Female | 12 | 60.0 |
| Total | 20 | 100.0 |
| Service year | ||
| 1 or below | 6 | 30.0 |
| 1–3 | 7 | 35.0 |
| 3–5 | 6 | 30.0 |
| 5 or above | 1 | 5.0 |
| Total | 20 | 100.0 |
| Experience of using Internet | ||
| Yes | 15 | 75.0 |
| No | 5 | 25.0 |
| Total | 20 | 100.0 |
| Experience of using Smart Mobile Device | ||
| Yes | 11 | 55.0 |
| No | 9 | 45.0 |
| Total | 20 | 100.0 |
| Personal information | Number | % |
|---|---|---|
| Age | ||
| 45–55 | 10 | 50.0 |
| 55–65 | 8 | 40.0 |
| 65 or above | 2 | 10.0 |
| Total | 20 | 100.0 |
| Gender | ||
| Male | 8 | 40.0 |
| Female | 12 | 60.0 |
| Total | 20 | 100.0 |
| Patient with numbers of chronic disease | ||
| 0 | 4 | 20.0 |
| 1–2 | 11 | 55.0 |
| 3 or above | 5 | 25.0 |
| Total | 20 | 100.0 |
- IAServ was easy to use.
- I would need a technical person to assist me.
- IAServ is useful in providing better services to patients.
- IAServ wasn’t useful in improving service quality.
- IAServ significantly reducing the workload of care-givers.
- The system did not significantly assist care-givers.
- The features offered by IAServ are sufficient.
- The features offered by IAServ are insufficient.
- IAServ significantly contributes to improving the delivery of health care services.
- Care-givers won’t find IAServ isn’ helpful in serving patients.
- I would like to offer health care services using IAServ.
- I’m not interested in using the IAServ platform.
- The features offered by IAServ are sufficient.
- The features offered by IAServ are insufficient.
- IAServ was useful in helping to maintain my health.
- IAServ was useless for managing my health.
5. Concluding Remarks and Future Work
| Reference | Service domain | Ambient intelligence | Multi-agent system | Context-aware reasoning | Web services based architecture |
|---|---|---|---|---|---|
| Riva, 2003 [12] | Smart home environment | Yes | No | No | No |
| Su and Chiang, 2013 [20] | Home health care | Yes | Yes | Yes | No |
| Coronato et al., 2009 [21] | Smart hospital environment | No | No | Yes | No |
| Fraile et al., 2009 [22] | In-home Monitoring | Yes | Yes | Yes | No |
| Eslami et al., 2010 [27] | Care service tailoring | Yes | No | Yes | No |
| Chang et al., 2009 [28] | In-home Monitoring | Yes | No | No | No |
| Fenza et al., 2012 [23] | In-home Monitoring | Yes | Yes | Yes | No |
| IAServ | Home health care | Yes | Yes | Yes | Yes |
Conflicts of Interest
References
- Valls, A.; Gibert, K.; Sánchez, D.; Batet, M. Using ontologies for structuring organizational knowledge in Home Care assistance. Int. J. Med. Inform. 2010, 79, 370–387. [Google Scholar] [CrossRef]
- Fergenson, M. TigerPlace: An innovative ‘Aging in Place’ community. Am. J. Nurs. 2013, 113, 68–69. [Google Scholar] [CrossRef]
- Emily, A.G.; Andrew, S.; Amanda, J.L.; Joan, K.D. A conceptual framework for examining the promise of the NORC program and Village models to promote aging in place. J. Aging Stud. 2012, 26, 273–284. [Google Scholar] [CrossRef]
- Swan, M. Emerging patient-driven health care models: An examination of health social networks, consumer personalized medicine and quantified self-tracking. Int. J. Environ. Res. Public Health 2009, 6, 492–525. [Google Scholar] [CrossRef]
- Riaño, D.; Real, F.; Campana, F.; Ercolani, S.; Annicchiarico, R. An Ontology for the Care of the Elder at Home. In Artificial Intelligence in Medicine; Combi, C., Shahar, Y., Abu-Hanna, A., Eds.; Springer: Berlin, Germany, 2009; Volume 5651, pp. 235–239. [Google Scholar]
- Rosenberg, F.; Curbera, F.; Duftler, M.J.; Khalaf, R. Composing RESTful services and collaborative workflows: A lightweight approach. IEEE Internet Comput. 2008, 12, 24–31. [Google Scholar] [CrossRef]
- Maximilien, E.M.; Ranabahu, A.; Gomadam, K. An online platform for web APIs and service mashups. IEEE Internet Comput. 2008, 12, 32–43. [Google Scholar] [CrossRef]
- Konieczny, E.; Ashcraft, R.; Cunningham, D.; Maripuri, S. Establishing Presence within the Service-Oriented Environment. In Proceedings of the IEEE Aerospace Conference, McLean, VA, USA, 7–14 March 2009.
- Wang, Y.H.; Liao, J.C. Why or Why Not Service Oriented Architecture. In Proceedings of the 2009 IITA International Conference on Services Science, Management and Engineering, Washington, DC, USA, 11–12 July 2009.
- Kikhia, B. Acceptance of Ambient Intelligence (AmI) in Supporting Elderly People and People with Dementia. Ms.C. Thesis, Lulea University of Technology, Lulea, Sweden, 2008. [Google Scholar]
- Loenen, E.J. On the Role of Graspable Objects in the Ambient Intelligence Paradigm. In Proceedings of the Smart Objects Conference, Grenoble, France, 15–17 May 2003.
- Riva, G. Ambient intelligence in health care. Cyberpsychol. Behav. 2003, 6, 295–300. [Google Scholar] [CrossRef]
- Bieliková, M.; Krajcovic, T. Ambient Intelligence within a Home Environment. Available online: http://www.ercim.org/publication/Ercim_News/enw47/bielikova.html (accessed on 28 August 2013).
- Schmidt, A. Interactive Context-Aware Systems Interacting with Ambient Intelligence. In Ambient Intelligence; Riva, G., Vatalaro, F., Davide, F., Alcañiz, M., Eds.; IOS Press: Amsterdam, Nederland, 2005; pp. 159–178. [Google Scholar]
- Schilit, B.N.; Theimer, M.M. Disseminating active map information to mobile hosts. IEEE Netw. 1994, 8, 22–32. [Google Scholar] [CrossRef]
- Barkhuus, L. Context Information vs. Sensor Information: A Model for Categorizing Context in Context-Aware Mobile Computing. In Proceedings of the International Symposium on Collaborative Technologies and Systems, San Diego, CA, USA, 19–23 January 2003.
- Chen, H. An Intelligent Broker Architecture for Pervasive Context-Aware Systems. Ph.D. Thesis, University of Maryland, Baltimore, MD, USA, December 2004. [Google Scholar]
- Parupudi, G.; Evans, S.S.; Holtgrewe, B.J.; Reus, E.F. Context Aware Systems and Methods Utilizing Hierarchical Tree Structures. U.S. Patent 7743074, 29 June 2010. [Google Scholar]
- Bricon-Souf, N.; Newman, C.R. Context awareness in health care: A review. Int. J. Med. Inform. 2007, 76, 2–12. [Google Scholar] [CrossRef]
- Su, C.J.; Chiang, C.Y. Pervasive community care platform: Ambient Intelligence leveraging sensor networks and mobile agents. Int. J. Syst. Sci. 2013. [Google Scholar] [CrossRef]
- Coronato, A.; Esposito, M.; Pietro, G.D. A multimodal semantic location service for intelligent environments: An application for Smart Hospitals. Pers. Ubiquitous Comput. 2009, 13, 527–538. [Google Scholar] [CrossRef]
- Fraile, J.A.; Bajo, J.; Lancho, B.P.; Sanz, E. HoCa Home Care Multi-agent Architecture. In International Symposium on Distributed Computing and Artificial Intelligence; Corchado Rodríguez, J.M., Rodriguez, S., Llinas, J., Molina, J.M., Eds.; Springer-Verlag: Berlin/Heidelberg, Germany, 2009; Volume 50, pp. 52–61. [Google Scholar]
- Fenza, G.; Furno, D.; Loia, V. Hybrid approach for context-aware service discovery in healthcare domain. J. Comput. Syst. Sci. 2012, 78, 1232–1247. [Google Scholar] [CrossRef]
- Meulendijk, M.; van de Wijngaert, L.; Brinkkemper, S.; Leenstra, H. AmI in good care? Developing design principles for ambient intelligent domotics for elderly. Inform. Health Soc. Care 2011, 36, 75–88. [Google Scholar] [CrossRef]
- Gauch, S.; Speretta, M.; Chandramouli, A.; Micarelli, A. User Profiles for Personalized Information Access. In The Adaptive Web; Brusilovsky, P., Kobsa, A., Nejdl, W., Eds.; Springer-Verlag: Berlin/Heidelberg, Germany, 2007; pp. 54–89. [Google Scholar]
- Golemati, M.; Katifori, A.; Vassilakis, C.; Lepouras, G.; Halatsis, C. Creating an Ontology for the User Profile: Method and Applications. In Proceedings of the First International Conference on Research Challenges in Information Science, Ouarzazate, Morocco, 23–26 April 2007.
- Eslami, M.Z.; Zarghami, A.; Sapkota, B.; Sinderen, M. Service Tailoring: Towards Personalized Homecare Services. In Proceedings of the 4th International Workshop on Architectures, Concepts and Technologies for Service Oriented Computing (ACT4SOC), Athens, Greece, 23 July 2010.
- Chang, Y.K.; Yang, C.L.; Chang, C.P.; Chu, C.P. A Personalized Service Recommendation System in a Home-Care Environment. In Proceedings of the 15th International Conference on Distributed Multimedia Systems, San Francisco, CA, USA, 10–12 September 2009.
- Chang, X.; Sahin, A.; Terpenny, J. An ontology-based support for product conceptual design. Robot. Comput. Integr. Manuf. 2008, 24, 755–762. [Google Scholar] [CrossRef]
- Horridge, M.; Jupp, S.; Moulton, G.; Rector, A.; Stevens, R.; Wroe, C. A Practical Guide to Building OWL Ontologies Using the Protege 4 and CO-ODE Tools. Available online: http://owl.cs.manchester.ac.uk/tutorials/protegeowltutorial/resources/ProtegeOWLTutorialP4_v1_1.pdf (accessed on 28 August 2013).
- Juarez, J.M.; Riestra, T.; Campos, M.; Morales, A.; Palma, J.; Marin, R. Medical knowledge management for specific hospital departments. Expert Syst. Appl. 2009, 36, 12214–12224. [Google Scholar] [CrossRef]
- Kola, J.; Wheeldin, B.; Rector, A. Lessons in Building OWL Ontology Driven Applications: OCHWIZ—An Occupational Health Application. In Proceedings of the UK e-Science All Hands Conference, Nottingham, UK, 10–13 September 2007.
- Huang, M.J.; Chen, M.Y. Integrated design of the intelligent web-based Chinese Medical Diagnostic System (CMDS)—Systematic development for digestive health. Expert Syst. Appl. 2007, 32, 658–673. [Google Scholar] [CrossRef]
- Ángel, G.C.; Alejandro, R.; Mencke, M.; Miguel, G.B.J.; Colomo-Palacios, R. ODDIN: Ontology-driven differential diagnosis based on logical inference and probabilistic refinements. Expert Syst. Appl. 2010, 37, 2621–2628. [Google Scholar] [CrossRef]
- Alexandrou, D.A.; Skitsas, I.E.; Mentzas, G.N. A holistic environment for the design and execution of self-adaptive clinical pathways. IEEE Trans. Inf. Technol. Biomed. 2010, 15, 108–118. [Google Scholar] [CrossRef]
- Su, C.J.; Peng, C.W. Multi-agent ontology-based Web 2.0 platform for medical rehabilitation. Expert Syst. Appl. 2012, 39, 10311–10323. [Google Scholar] [CrossRef]
- Sirota, P.; Johnson, D.; Ghare, G.D.; Jain, T.; Geller, A.S. Using Configured Application Pricing to Determine End User Fees for Use of Invocable Services. U.S. Patent 7925554, 12 April 2011. [Google Scholar]
- Frederick, R.; Kakulapati, G.; Agrawal, A.; McCann, J.R., III. Providing an Invocable Composite Network Service Based on Multiple Other Invocable Constituent Network Services. U.S. Patent 2010. [Google Scholar]
- Thies, G.; Vossen, G. Web-Oriented Architectures: On the Impact of Web 2.0 on Service-Oriented Architectures. In Proceedings of the 3rd IEEE Asia-Pacific Services Computing Conference, Yilan, Taiwan, 9–12 December 2008.
- Szepielak, D.; Tumidajewicz, P.; Hagge, L. Integrating Information Systems Using Web Oriented Integration Architecture and RESTful Web Services. In Proceedings of the 6th IEEE World Congress on Services, Miami, FL, USA, 5–10 July 2010.
- Fielding, R.T.; Taylor, R.N. Principled design of the modern Web architecture. ACM Trans. Internet Technol. 2002, 2, 115–150. [Google Scholar] [CrossRef]
- Belimpasakis, P.; Moloney, S. A Platform for proving family oriented RESTful services hosted at home. IEEE Trans. Consum. Electr. 2009, 55, 690–698. [Google Scholar] [CrossRef]
- Dodero, J.M.; Ghiglione, E. ReST-based web access to learning design services. IEEE Trans. Learn. Technol. 2008, 1, 190–195. [Google Scholar] [CrossRef]
- Su, C.J.; Chiang, C.Y. Enabling successful Collaboration 2.0: A REST-based Web Service and Web 2.0 technology oriented information platform for collaborative product development. Comput. Ind. 2012, 63, 948–959. [Google Scholar] [CrossRef]
- JADE. Available online: http://jade.tilab.com/ (accessed on 28 August 2013).
- OWL-S: Semantic Markup for Web Services. Available online: http://www.w3.org/Submission/OWL-S (accessed on 28 August 2013).
- W3C, SPIN—Modeling Vocabulary. Available online: http://spinrdf.org/spin.html (accessed on 3 October 2013).
- Murty, J. Programming Amazone Web Service; O’Reilly Media: Sebastopol, CA, USA, 2008. [Google Scholar]
- Krishnan, S. Programming Windows Azure; O’Reilly Media: Sebastopol, CA, USA, 2010. [Google Scholar]
- Uploading Your Application. Google App Engine. Available online: https://developers.google.com/appengine/docs/java/gettingstarted/uploading (accessed on 28 August 2013).
- Yahoo Weather RSS Feed. Available online: http://developer.yahoo.com/weather (accessed on 28 August 2013).
- Jena—A Semantic Web Framework for Java. Available online: http://jena.sourceforge.net/index.html (accessed on 28 August 2013).
- TopBraid Composer. Available online: http://www.topquadrant.com/products/TB_Composer.html (accessed on 28 August 2013).
- SPIN Support in TopBraid. Available online: http://www.topquadrant.com/products/SPIN.html (accessed on 3 October 2013).
- Jih, W.; Hsu, J.Y.; Tsai, T. Context-Aware Service Integration for Elderly Care in a Smart Environment. In Proceedings of the AAAI Workshop on Modeling and Retrieval Context, Boston, MA, USA, 16–17 July 2006.
- Moreno, A.; Sanchez, D.; Isern, D. Security Measures in a Medical Multi-Agent System. In Artificial Intelligence Research and Development; Aguiló, I., Valverde, L., Escrig, M.T., Eds.; IOS Press: Amsterdam, Nederland, 2003; pp. 244–255. [Google Scholar]
- Burkle, A.; Essendorfer, B.; Hertel, A.; Muller, W.; Wieser, M. A Test Suite for the Evaluation of Mobile Agent Platform Security. In Proceedings of the IEEE/WIC/ACM International Conference on Intelligent Agent Technology, Hong Kong, China, 18–22 December 2006.
- Shakshuki, E.; Luo, Z.; Gong, J.; Chen, Q. Multi-Agent System for Security Service. In Proceedings of International Conference on Advanced Information Networking and Applications, Fukuoka, Japan, 29–31 March 2004.
- Wong, S.W.; Ng, K.W. Security Support for Mobile Grid Services Framework. In Proceedings of International Conference on Next Generation Web Services Practices, Seoul, Korea, 25–28 September 2006.
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Su, C.-J.; Chiang, C.-Y. IAServ: An Intelligent Home Care Web Services Platform in a Cloud for Aging-in-Place. Int. J. Environ. Res. Public Health 2013, 10, 6106-6130. https://doi.org/10.3390/ijerph10116106
Su C-J, Chiang C-Y. IAServ: An Intelligent Home Care Web Services Platform in a Cloud for Aging-in-Place. International Journal of Environmental Research and Public Health. 2013; 10(11):6106-6130. https://doi.org/10.3390/ijerph10116106
Chicago/Turabian StyleSu, Chuan-Jun, and Chang-Yu Chiang. 2013. "IAServ: An Intelligent Home Care Web Services Platform in a Cloud for Aging-in-Place" International Journal of Environmental Research and Public Health 10, no. 11: 6106-6130. https://doi.org/10.3390/ijerph10116106