Impact of Traumatic Dental Injury on the Quality of Life of Brazilian Preschool Children

Abstract
:1. Introduction
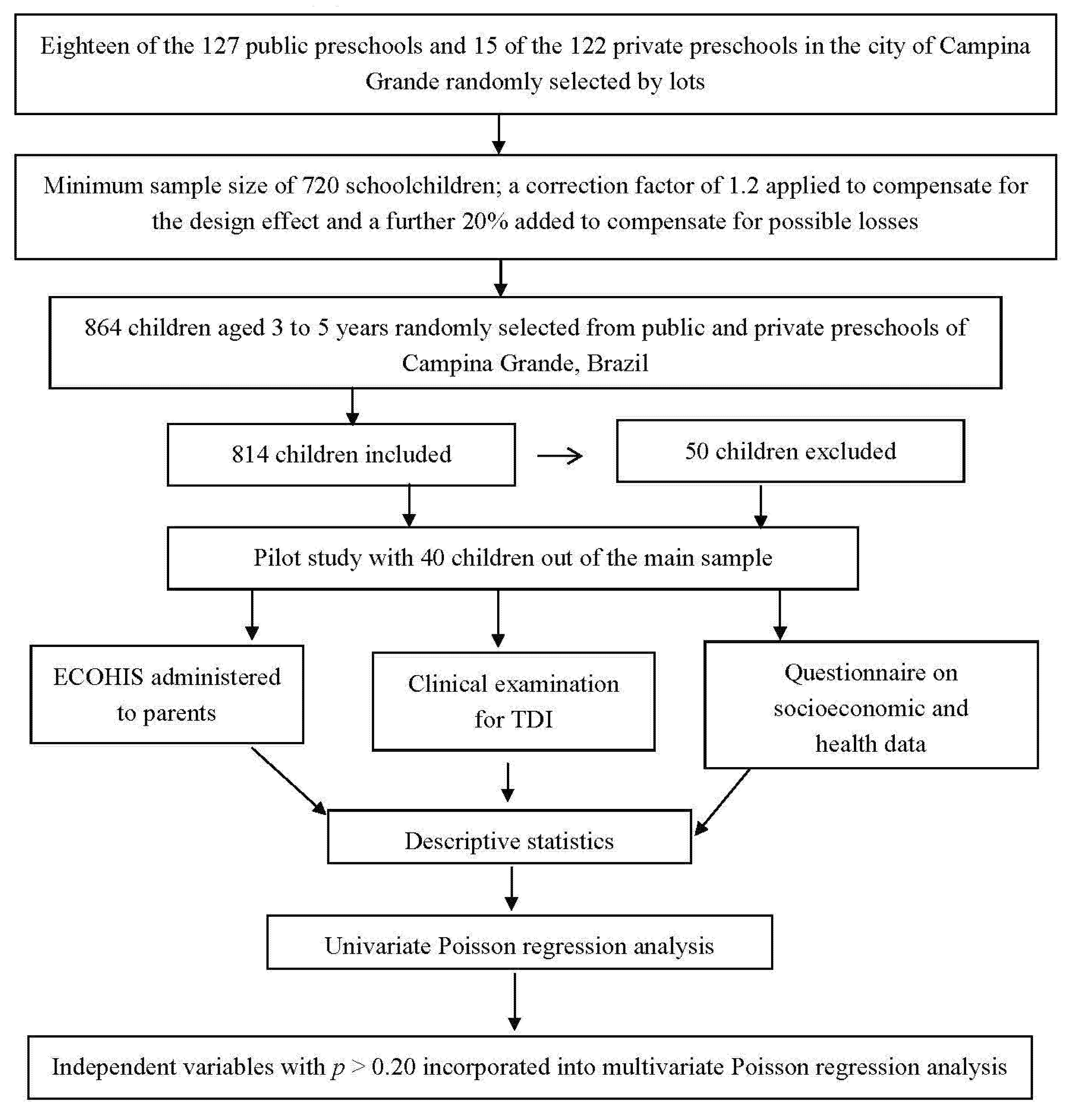
2. Methods
2.1. Sample Characteristics
2.2. Eligibility Criteria
2.3. Training and Calibration Exercise
2.4. Pilot Study
2.5. Non-Clinical Data Collection
2.6. Clinical Data Collection
2.7. Statistical Analysis
2.8. Ethical Considerations

3. Results

{kind=link}
| Variable | Frequency | |
|---|---|---|
| N | % | |
| • Gender of child | ||
| Female | 392 | 48.2 |
| Male | 422 | 51.8 |
| • Number of residents in home | ||
| <to 6 residents | 674 | 84.6 |
| 6 or more residents | 123 | 15.4 |
| • Household income | ||
| >3 times the minimum wage | 144 | 18.5 |
| ≤3 times the minimum wage | 634 | 81.5 |
| • Parent/caregiver’s schooling | ||
| >8 years of study | 437 | 54.0 |
| ≤8 years of study | 373 | 46.0 |
| • Parent/caregiver’s assessment of child’s oral health | ||
| Good | 759 | 93.4 |
| Poor | 54 | 6.6 |
| • Parent/caregiver’s assessment of child’s general health | ||
| Good | 801 | 99.0 |
| Poor | 8 | 1.0 |
| • TDI | ||
| Yes | 281 | 34.6 |
| No | 533 | 65.4 |
| • Type of TDI | ||
| None | 533 | 65.4 |
| Tooth discoloration | 91 | 11.2 |
| Enamel fracture | 138 | 17.0 |
| Enamel + dentin fracture | 39 | 4.8 |
| Luxation | 9 | 1.1 |
| Avulsion | 4 | 0.5 |
| • Number of teeth affected by TDI | ||
| 2 or more teeth | 104 | 12.8 |
| 1 tooth | 177 | 21.7 |
| None | 533 | 65.5 |
| • History of toothache | ||
| Yes | 71 | 36.6 |
| No | 123 | 63.4 |
| • History of dental visits | ||
| Yes | 196 | 24.2 |
| No | 614 | 75.8 |
| • Type of preschool | ||
| Public | 438 | 53.8 |
| Private | 376 | 46.2 |
| ECOHIS | ||||
|---|---|---|---|---|
| Domains, Items | SCORE Mean ± DP | Minimum–Maximum | n (%) Don’t Know | n (%) Prevalence of impact |
| • Child Impact | 2.21 ± 4.18 | 0–31 | - | 31.1% |
| Related to pain | 0.58 ± 0.979 | 0–4 | 14 (1.7%) | 176 (21.6%) |
| Had difficulty drinking hot or cold beverages | 0.35 ± 0.816 | 0–4 | 10 (1.2%) | 101 (12.4%) |
| Had difficulty eating some foods | 0.35 ± 0.830 | 0–4 | 11 (1.4%) | 103 (12.5%) |
| Had difficulty pronouncing words | 0.21 ± 0.707 | 0–4 | 25 (3.1%) | 59 (7.2%) |
| Missed preschool, daycare or school | 0.12 ± 0.466 | 0–3 | - | 29 (3.6%) |
| Had trouble sleeping | 0.17 ± 0.596 | 0–4 | 8 (1.0%) | 45 (5.5%) |
| Been irritable or frustrated | 0.29 ± 0.745 | 0–4 | 8 (1.0%) | 85 (10.4%) |
| Avoided smiling or laughing | 0.08 ± 0.395 | 0–4 | 10 (1.2%) | 18 (2.2%) |
| Avoided talking | 0.08 ± 0.00 | 0–4 | 9 (1.1%) | 19 (2.3%) |
| • Family Impact | 1.13 ± 2.167 | 0–14 | 24.7% | |
| Been upset | 0.39 ± 0.902 | 0–4 | 11 (1.4%) | 114 (14.0%) |
| Felt guilty | 0.46 ± 0.938 | 0–4 | 11 (1.4%) | 141 (17.3%) |
| Taken time off work | 0.16 ± 0.564 | 0–4 | 8 (1.0%) | 47 (5.8%) |
| Financial impact | 0.14 ± 0.560 | 0–4 | 9 (1.1%) | 41 (5.0%) |
| ECOHIS | TDI | ||||||
|---|---|---|---|---|---|---|---|
| Yes | No | Total | p-value | ||||
| Domains, Items | N | % | N | % | N | % | |
| • Child Impact | |||||||
| No impact | 185 | (33.0) | 376 | (67.0) | 561 | (68.9) | 0.45 |
| Impact | 92 | (36.4) | 161 | (63.6) | 253 | (31.1) | |
| • Symptoms Domain | |||||||
| Related to Pain | |||||||
| No impact | 218 | (34.2) | 420 | (65.8) | 638 | (78.4) | 0.873 |
| Impact | 59 | (33.5) | 117 | (66.5) | 176 | (21.6) | |
| • Function Domain | |||||||
| Had difficulty drinking hot or cold beverages | |||||||
| No impact | 236 | (33.6) | 467 | (66.4) | 703 | (87.4) | 0.543 |
| Impact | 37 | (36.6) | 64 | (63.4) | 101 | (12.6) | |
| Had difficulty eating some food | |||||||
| No impact | 235 | (33.5) | 466 | (66.5) | 462 | (81.9) | 0.724 |
| Impact | 36 | (35.3) | 66 | (64.7) | 102 | (18.1) | |
| Had difficulty pronouncing words | |||||||
| No impact | 239 | (32.7) | 491 | (67.3) | 730 | (92.5) | 0.213 |
| Impact | 24 | (40.7) | 35 | (59.3) | 59 | (7.5) | |
| Missing preschool | |||||||
| No impact | 266 | (33.9) | 519 | (66.1) | 785 | (96.4) | 0.652 |
| Impact | 11 | (37.9) | 18 | (62.1) | 29 | (3.6) | |
| • Psychological Domain | |||||||
| Had trouble sleeping | |||||||
| No impact | 257 | (33.8) | 504 | (66.2) | 761 | (94.4) | 0.952 |
| Impact | 15 | (33.3) | 30 | (66.7) | 45 | (5.6) | |
| Been irritable or frustrated | |||||||
| No impact | 244 | (33.8) | 477 | (66.2) | 721 | (95.7) | 0.959 |
| Impact | 29 | (34.1) | 56 | (65.9) | 32 | (4.3) | |
| • Self-image/Social Interaction Domain | |||||||
| Avoided smiling or laughing | |||||||
| No impact | 264 | (63.6) | 522 | (66.4) | 786 | (97.8) | 0.336 |
| Impact | 8 | (44.8) | 10 | (55.6) | 18 | (2.2) | |
| Avoided talked | |||||||
| No impact | 265 | (33.7) | 521 | (66.3) | 786 | (97.7) | 0.445 |
| Impact | 8 | (42.1) | 11 | (57.9) | 19 | (2.3) | |
| Family Impact | |||||||
| No impact | 205 | (33.7) | 403 | (66.3) | 608 | (75.1) | 0.874 |
| Impact | 69 | (34.3) | 132 | (65.7) | 201 | (24.9) | |
| • Distress Domain | |||||||
| Been upset | |||||||
| No impact | 229 | (33.2) | 460 | (66.8) | 689 | (85.8) | 0.349 |
| Impact | 43 | (37.7) | 71 | (62.3) | 114 | (14.2) | |
| Felt guilty | |||||||
| No impact | 227 | (34.3) | 435 | (65.7) | 662 | (82.4) | 0.705 |
| Impact | 46 | (32.6) | 95 | (67.4) | 141 | (17.6) | |
| • Family Function Domain | |||||||
| Taken time off work | |||||||
| No impact | 256 | (33.7) | 503 | (66.3) | 759 | (94.2) | 0.521 |
| Impact | 18 | (38.3) | 29 | (61.7) | 47 | (5.8) | |
| Financial Impact | |||||||
| No impact | 260 | (34.0) | 504 | (66.0) | 764 | (94.9) | 0.759 |
| Impact | 13 | (31.7) | 28 | (68.3) | 41 | (5.1) | |
| Variable | Impact on child’s QoL | Bivariate | Multivariate | |||
|---|---|---|---|---|---|---|
| Present | Absent | Unadjusted prevalence ratio | Adjusted prevalence ratio | |||
| n (%) | n (%) | p-value | (95% CI) | p-value | (95% CI) | |
| • Gender of child | ||||||
| Male | 131 (31.0) | 291 (69.0) | 1.00 | - | - | |
| Female | 122 (31.1) | 270 (68.9) | 0.980 | 1.003 (0.817–1.230) | - | - |
| • Mother’s schooling | ||||||
| >8 years of study | 113 (25.9) | 324 (74.1) | 1.00 | - | - | |
| ≤8 years of study | 139 (37.3) | 234 (62.7) | 0.001 | 1.441 (1.173–1.771) | - | - |
| • Monthly household income | ||||||
| >3 times the minimum wage | 29 (20.1) | 115 (79.9) | 1.00 | - | - | |
| ≤3 times the minimum wage | 219 (34.5) | 415 (65.5) | 0.020 | 1.715 (1.218–2.416) | - | - |
| • N° of residents in home | ||||||
| <6 | 199 (29.5) | 475 (70.5) | 1.00 | - | - | |
| ≥6 | 50 (40.7) | 73 (59.3) | 0.010 | 1.377 (1.079–1.756) | - | - |
| • Type of school | ||||||
| Public | 153 (34.9) | 285 (65.1) | 1.00 | - | - | |
| Private | 100 (26.6) | 276 (73.4) | 0.011 | 1.313 (1.064–1.622) | - | - |
| • Caregiver’s perception of child’s general health | ||||||
| Good | 247 (30.8) | 554 (69.2) | 1.00 | - | ||
| Poor | 6 (75.0) | 2 (25.0) | 0.001 | 2.432 (1.609–3.677) | - | - |
| • Caregiver’s perception of child’s oral health | ||||||
| Good | 205 (27.0) | 554 (73.0) | 1.00 | 1.00 | ||
| Poor | 48 (88.9) | 6 (11.1) | 0.001 | 2.432 (1.609–3.677) | 0.23 | 1.210 (1.027-1.426) |
| • TDI | ||||||
| Yes | 95 (33.8) | 186 (66.2) | 1.00 | - | - | |
| No | 158 (29.6) | 357 (70.4) | 0.342 | 1.108 (0.897–1.368) | - | - |
| • Type of trauma | ||||||
| Avulsion/Luxation | 6 (46.2) | 7 (53.8) | 0.139 | 1.572 (0.864–2.861) | - | - |
| Discoloration | 37 (40.7) | 54 (59.3) | 0.020 | 1385 (1.052–1.822) | - | - |
| Enamel + dentin fracture | 13 (33.3) | 26 (66.7) | 0.588 | 1.135 (0.717–1.797) | - | - |
| Enamel fracture or no trauma | 197 (29.4) | 474 (70.6) | 1.00 | - | - | |
| • Number of teeth with trauma | ||||||
| None | 158 (29.6) | 375 (70.4) | 1.00 | - | - | |
| One | 52 (29.4) | 125 (70.6) | 0.947 | 0.991 (0.762–1.289) | - | - |
| Two or more | 43 (41.3) | 61 (58.7) | 0.013 | 1.395 (1.072–1.816) | - | - |
| • Dental caries | ||||||
| No | 45 (16.1) | 235 (83.9) | <0.001 | 2.424 (1.817–3.232) | - | - |
| Yes | 208 (39.0) | 326 (61.0) | 1.00 | - | - | |
| • Malocclusion | ||||||
| No | 80 (28.6) | 200 (71.4) | 1.00 | - | - | |
| Yes | 173 (32.4) | 361 (67.6) | 0.267 | 1.134 (0.908–1.416) | - | - |
| • History of toothache | ||||||
| No | 15 (12.2) | 108 (87.8) | - | 1.00 | - | 1.00 |
| Yes | 62 (87.3) | 9 (12.7) | 0.001 | 7.161 (4.420–11.600) | 0.001 | 4.997 (2.943-8.483) |
| • History of visits to dentist | ||||||
| No | 173 (28.2) | 441 (71.8) | 1.00 | - | - | |
| Yes | 78 (39.8) | 118 (60.2) | 0.002 | 1.412 (1.41–1.749) | - | - |
| Variable | Impact on family’s QoL | Bivariate | Multivariate | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Present | Absent | Unadjusted prevalence ratio | Adjusted prevalence ratio | |||||||
| n (%) | n (%) | p-value | (95% CI) | p-value | (95% CI) | |||||
| • Gender of child | ||||||||||
| Male | 94 (24.2) | 294 (75.8) | 1.00 | - | - | |||||
| Female | 107 (25.4) | 314 (74.6) | 0.696 | 1.049 (0.825–1.334) | - | - | ||||
| • Mother’s schooling | ||||||||||
| >8 years of study | 97 (22.3) | 338 (77.7) | 1.00 | - | - | |||||
| ≤8 years of study | 103 (27.8) | 267 (72,2) | 0,070 | 1.248 (0.982–1.587) | - | - | ||||
| • Monthly household income | ||||||||||
| >3 times the minimum wage | 31 (21.5) | 113 (78.5) | 1.00 | - | - | |||||
| ≤3 times the minimum wage | 165 (26.2) | 464 (73.8) | 0.252 | 1.219 (0.869–1.709) | - | - | ||||
| • N° of residents in home | ||||||||||
| <6 | 160 (23.9) | 510 (76.1) | 1.00 | - | - | |||||
| ≥6 | 38 (30.9) | 85 (69.1) | 0.089 | 1.294 (0.961–1.741) | - | - | ||||
| • Type of school | ||||||||||
| Public | 85 (22.8) | 287 (77.2) | 1.00 | - | - | |||||
| Private | 116 (26.5) | 321 (73.5) | 0.227 | 1.162 (0.911–1.482) | - | - | ||||
| • Caregiver’s perception of child’s general health | ||||||||||
| Good | 194 (24.4) | 602 (75.6) | 1.00 | - | - | |||||
| Poor | 5 (62.5) | 3 (37.5) | 0.001 | 2.564 (1.479–4.447) | - | - | ||||
| • Caregiver’s perception of child’s oral health | ||||||||||
| Good | 161 (21.4) | 593 (78.6) | 1.00 | - | - | |||||
| Poor | 40 (74.1) | 14 (25.9) | 0.001 | 3.469 (2.815–4.275) | - | - | ||||
| • TDI | ||||||||||
| Yes | 131 (24.7) | 400 (75.3) | 1.00 | - | - | |||||
| No | 70 (25.2) | 208 (74.8) | 0.874 | 1.121 (0.793–1.313) | - | |||||
| • Type of trauma | ||||||||||
| Avulsion/Luxation | 5 (38.5) | 8 (61.5) | 0.185 | 1.606 (0.797–3.236) | - | - | ||||
| Discoloration | 28 (31.5) | 61 (68.5) | 0.111 | 1.313 (0.939–1.836) | - | - | ||||
| Enamel + dentin fracture | 8 (20.5) | 31 (79.5) | 0.631 | 0.856 (0.455–1.612) | - | - | ||||
| Enamel fracture or no trauma | 160 (24.0) | 508 (76.0) | 1.00 | - | - | |||||
| • Number of teeth with trauma | ||||||||||
| None | 131 (24.7) | 400 (75.3) | 1.00 | - | - | |||||
| One | 40 (23.0) | 134 (77.0) | 0.655 | 0.932 (0.683–1.270) | - | - | ||||
| Two or more | 30 (28.8) | 74 (71.2) | 0.362 | 1.169 (0.835–1.637) | - | - | ||||
| • Dental caries | ||||||||||
| No | 34 (12.3) | 243 (87.7) | <0.001 | 2.557 (1.822–3.589) | 0.022 | 2.305 (1.130–4.702) | ||||
| Yes | 167 (31.4) | 365 (68.6) | 1.00 | - | 1.00 | |||||
| • Malocclusion | ||||||||||
| No | 61 (22.0) | 216 (78.0) | 1.00 | - | - | |||||
| Yes | 140 (26.3) | 392 (73.7) | 0.185 | 1.195 (0.918–1.555) | - | - | ||||
| • History of toothache | ||||||||||
| No | 22 (18.0) | 100 (82.0) | - | 1.00 | 1.00 | |||||
| Yes | 48 (67.6) | 23 (32.4) | 0.001 | 3.749 (2.485–5.656) | 0.001 | 2.791 (1.801–4.325) | ||||
| • History of visits to dentist | ||||||||||
| No | 129 (21.1) | 481 (78.9) | 1.00 | - | - | |||||
| Yes | 71 (36.4) | 124 (63.6) | 0.001 | 1.772 (1.354–2.190) | - | - | ||||
4. Discussion
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Paula, J.S.; Leite, I.C.; Almeida, A.B.; Ambrosano, G.M.; Pereira, A.C.; Mialhe, F.L. The influence of oral health conditions, socioeconomic status and home environment factors on schoolchildren’s self-perception of quality of life. Health Qual. Life Outcomes 2012, 10, 6–13. [Google Scholar] [CrossRef]
- Barbosa, T.S.; Gavião, M.B. Oral health-related quality of life in children: Part II. Effects of clinical oral health status. A systematic review. Int. J. Dent. Hyg. 2008, 6, 100–107. [Google Scholar] [CrossRef]
- Bendo, C.B.; Paiva, S.M.; Torres, C.T.; Oliveira, A.C.; Goursand, D.; Pordeus, I.A. Association between treated/untreated traumatic dental injuries and impact on quality of life of Brazilian schoolchildren. Health Qual. Life Outcomes 2010, 114, 1–8. [Google Scholar]
- Nurelhuda, N.M.; Ahmed, M.F.; Trovik, T.A.; Astrom, A.N. Evaluation of oral health-related quality of life among Sudanese schoolchildren using Child-OIDO inventory. Health Qual. Life Outcomes 2010, 8, 152. [Google Scholar] [CrossRef]
- Abanto, J.; Carvalho, T.S.; Mendes, F.M.; Wanderley, M.T.; Bönecker, M.; Raggio, D.P. Impact of oral diseases and disorders on oral health-related quality of life of preschool children. Community Dent. Oral Epidemiol. 2011, 39, 105–114. [Google Scholar] [CrossRef]
- Pahel, B.T.; Rozier, R.G.; Salde, G.D. Parental perceptions of children’s oral health: The Early Childhood Oral Health Impact Scale (ECohis). Health Qual. Life Outcomes 2007, 5, 6. [Google Scholar] [CrossRef]
- Wong, H.M.; McGrath, C.P.; King, N.M. Rasch validation of the early childhood oral health impact scale. Community Dent. Oral Epidemiol. 2011, 39, 449–457. [Google Scholar] [CrossRef]
- Scarpelli, A.C.; Oliveira, B.H.; Tesch, F.C.; Leão, A.T.; Pordeus, I.A.; Paiva, S.M. Psychometric properties of the Brazilian version of the Early Childhood Oral Health Impact Scale (B-ECOHIS). BMC Oral Health 2011, 11, 19. [Google Scholar] [CrossRef]
- Talekar, B.S.; Rozier, R.G.; Slade, G.D.; Ennett, S.T. Parental perceptions of their preschool-aged children’s oral health. J. Am. Dent. Assoc. 2005, 136, 364–372. [Google Scholar]
- Sgan-Cohen, H.D.; Megnagi, G.; Jacobi, Y. Dental trauma and its association with anatomic, behavioral, and social variables among fifth and sixth grade schoolchildren in Jerusalem. Community Dent. Oral Epidemiol. 2005, 33, 174–180. [Google Scholar] [CrossRef]
- Kramer, P.F.; Zembruski, C.; Ferreira, S.H.; Feldens, C.A. Traumatic dental injuries in Brazilian preschool children. Dent. Traumatol. 2003, 19, 299–303. [Google Scholar]
- Granville-Garcia, A.F.; de Menezes, V.A.; de Lira, P.I. Dental trauma and associated factors in Brazilian preschoolers. Dent. Traumatol. 2006, 22, 318–322. [Google Scholar] [CrossRef]
- Robson, F.; Ramos-Jorge, M.L.; Bendo, C.B.; Vale, M.P.; Paiva, S.M.; Pordeus, I.A. Prevalence and determining factors of traumatic injuries to primary teeth in preschool children. Dent. Traumatol. 2009, 25, 118–122. [Google Scholar] [CrossRef]
- Granville-Garcia, A.F.; Vieira, I.T.; Siqueira, M.J.; de Menezes, V.A.; Cavalcanti, A.L. Traumatic dental injuries and associated factors among Brazilian preschool children aged 1–5 years. Acta Odontol. Latinoam. 2010, 23, 47–52. [Google Scholar]
- Viegas, C.M.; Scarpelli, A.C.; Carvalho, A.C.; Ferreira, F.M.; Pordeus, I.A.; Paiva, S.M. Predisposing factors for traumatic dental injuries in Brazilian preschool children. Eur. Arch. Paediatr. Dent. 2010, 11, 59–65. [Google Scholar] [CrossRef]
- Ferreira, J.M.; Andrade, E.M.F.; Katz, C.R.; Rosenblatt, A. Prevalence of dental trauma in deciduous teeth of Brazilian children. Dent. Traumatol. 2009, 25, 219–223. [Google Scholar]
- Aldrigui, J.M.; Abanto, J.; Carvalho, T.S.; Mendes, F.M.; Wanderley, M.T.; Bönecker, M.; Raggio, D.P. Impact of traumatic dental injuries and malocclusions on quality of life of young children. Health Qual. Life Outcomes 2011, 24, 78. [Google Scholar] [CrossRef] [Green Version]
- Viegas, C.M.; Scarpelli, A.C.; Carvalho, A.C.; Ferreira, F.M.; Pordeus, I.A.; Paiva, S.M. Impact of traumatic dental injury on quality of life among Brazilian preschool children and their families. Pediatr. Dent. 2012, 36, 300–307. [Google Scholar]
- Brazilian Institute of Geography and Statistics (IBGE). First Results of the 2010 Census. Available online: http://www.censo2010.ibge.gov.br/dadosdivulgados/index.php?uf=25 (accessed on 3 August 2012).
- David, J.; Astrom, A.; Wang, N.J. Factors associated with traumatic dental injuries among 12-year-old schoolchildren in South India. Dent. Traumatol. 2009, 25, 500–505. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research, 1st ed.; Chapman and Hall: London, UK, 1991. [Google Scholar]
- Tesch, F.C.; Oliveira, B.H.; Leão, A. Semantic equivalence of the Brazilian version of the Early Chilhood Oral Health Impact Scale. Cad. Saúde Pública 2008, 24, 1897–1909. [Google Scholar]
- Tesch, F.C.; Oliveira, B.H.; Leão, A. Measuring the impact of oral health problems on children’s quality of life: Conceptual and methodological issues. Cad. Saúde Pública 2007, 23, 2555–2564. [Google Scholar] [CrossRef]
- Ardenghi, T.M.; Ferreira, F.V.; Piovesan, C.; Mendes, F.M. Age of first dental visit and predictors for oral healthcare utilisation in preschool children. Oral Health Prev. Dent. 2012, 10, 17–27. [Google Scholar]
- Burstone, C.J. Lip posture and its significance in treatment planning. Am. J. Orthod. 1967, 53, 262–284. [Google Scholar] [CrossRef]
- Grabowski, R.; Stahl, F.; Gaebel, M.; Kundt, G. Relationship between occlusal findings and orofacial myofunctional status in primary and mixed dentition. Part I: Prevalence of malocclusions. J. Orofac. Orthop. 2007, 68, 26–37. [Google Scholar] [CrossRef]
- World Health Organization. Dentition Status and Criteria for Diagnosis and Coding. WHO Oral Health Surveys Basic Methods, 4th ed.; WHO: Geneva, Switzerland, 1997; pp. 39–44. [Google Scholar]
- Andreasen, J.O.; Andreasen, F.M.; Andersson, L. Textbook and Color Atlas of Traumatic Injuries to the Teeth, 1st ed.; Munskgaard International Publishers: Copenhagen, Denmark, 2007. [Google Scholar]
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, A.; Sen, A.; Hasson, H. The International Caries Detection and Assessment System (ICDAS): An integrated system for measuring dental caries. Community Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef]
- Oliveira, A.C.; Paiva, S.M.; Campos, M.R.; Czeresnia, D. Factors associated with malocclusions in children and adolescents with Down syndrome. Am. J. Orthod. Dent. Facial Orthoped. 2008, 133, 486. [Google Scholar] [CrossRef]
- Foster, T.D.; Hamilton, M.C. Occlusion in the primary dentition. Study of children at 2 and one-half to 3 years of age. Br. Dent. J. 1969, 126, 76–79. [Google Scholar]
- Goursand, D.; Paiva, S.M.; Zarzar, P.M.; Ramos-Jorge, M.L.; Cornacchia, G.M.; Pordeus, I.A.; Allison, P.J. Cross-cultural adaptation of the Child Perceptions Questionnaire 11-14 (CPQ11-14) for the Brazilian Portuguese language. Health Qual. Life Outcomes 2008, 14, 6–12. [Google Scholar]
- Locker, D.; Jokovic, A.; Stephens, M.; Kenny, D.; Tompson, B.; Cuyatt, G. Family impact of child oral and oro-facial conditions. Community Dent. Oral Epidemiol. 2002, 30, 438–448. [Google Scholar] [CrossRef]
- Goettems, M.L.; Ardenghi, T.M.; Romano, A.R.; Demarco, F.F.; Torriani, D.D. Influence of maternal dental anxiety on oral health-related quality of life of preschool children. Qual. Life Res. 2011, 20, 951–959. [Google Scholar] [CrossRef]
- Abanto, J.; Paiva, S.M.; Raggio, D.P.; Celiberti, P.; Aldrigui, J.M.; Bönecker, M. The impact of dental caries and trauma in children on family quality of life. Community Dent. Oral Epidemiol. 2012, 40, 323–331. [Google Scholar]
- Wandera, M.; Kayondo, J.; Engebretsen, I.M.; Okullo, I.; Astrom, A.N. Factors associated with caregivers’ perception of children’s health and oral health status: A study of 6- to 36-month-olds in Uganda. Int. J. Paediatr. Dent. 2009, 19, 251–262. [Google Scholar] [CrossRef]
- Hetherington, E.M.; Parke, R.D.; Locke, V.O. Child Psychology: A Contemporary Viewpoint, 1st ed.; The McGraw-Hill Companies: New York, NY, USA, 1999. [Google Scholar]
- Jokovic, A.; Locker, D.; Stephens, M.; Kenny, D.; Tompson, B.; Guyat, G. Validity and reliability of a questionnaire for measuring child oral-health-related quality of life. J. Dent. Res. 2002, 81, 459–463. [Google Scholar] [CrossRef]
- Bernabé, E.; Oliveira, C.M.; Sheiham, A. Comparison of the discriminative ability of a generic and a condition-specific OHRQoL measure in adolescents with and without normative need for orthodontic treatment. Health Qual. Life Outcomes 2008, 6, 64. [Google Scholar] [CrossRef]
- Traebert, J.; Almeida, I.C.; Garghetti, C.; Marcenes, W. Prevalence, need for treatment and predisposing factors of trauma in the permanent dentition of schoolchildren 11–13 years of age. Cad. Saúde Pública 2004, 20, 403–410. [Google Scholar] [CrossRef]
- Kosmala-Anderson, J.; Wallace, L.M. Breastfeeding works: The role of employers in supporting women who wish to breastfeed and work in four organizations in England. J. Public Health Med. 2006, 28, 183–191. [Google Scholar]
- Camargo, M.B.; Barros, A.J.; Frazão, P.; Matijasevich, A.; Santos, I.S.; Peres, M.A.; Peres, K.G. Predictors of dental visits for routine check-ups and for the resolution of problems among preschool children. Rev. Saúde Pública 2012, 46, 87–97. [Google Scholar] [CrossRef]
- Escobar-Paucar, G.; Sosa-Palacio, C.; Burgos-Gil, L.M. Social representations of pregnant mothers in an urban community: Medellín, Colombia. Salud Pública Méx. 2010, 52, 46–51. [Google Scholar] [CrossRef]
- Arora, A.; Bedros, D.; Bhole, S.; Do, L.G.; Scott, J.; Blinkhorn, A.; Schwarz, E. Child and family health nurses’ experiences of oral health of preschool children: A qualitative approach. J. BMC Public Health 2012, 72, 149–155. [Google Scholar]
- Feldens, C.A.; Kramer, P.F.; Ferreira, S.H.; Spiguel, M.H.; Marquezan, M. Exploring factors associated with traumatic dental injuries in preschool children: A Poisson regression analysis. Dent. Traumatol. 2010, 26, 143–148. [Google Scholar] [CrossRef]
- Choi, S.C.; Park, J.H.; Pae, A.; Kim, J.R. Retrospective study on traumatic dental injuries in preschool children at Kyung Hee Dental Hospital, Seoul, South Korea. Dent. Traumatol. 2010, 26, 70–75. [Google Scholar] [CrossRef]
- Patel, R.R.; Tootla, R.; Inglehart, M.R. Does oral health self-perceptions parenteral ratings and video-based assessments of children’s smiles? Community Dent. Oral Epidemiol. 2007, 35, 44–52. [Google Scholar] [CrossRef]
- Goettems, M.L.; Azevedo, M.S.; Correa, M.B.; Costa, C.T.; Wendt, F.P.; Schuch, H.S.; Bonow, M.L.; Romano, A.R.; Torriani, D.D. Dental trauma occurrence and occlusal characteristics in Brazilian preschool children. Pediatr. Dent. 2012, 34, 104–107. [Google Scholar]
- Dandi, K.K.; Raom, E.V.; Margabandhu, S. Dental pain as a determinant of expressed need for dental care among 12-year-old school children in India. Indian J. Dent. Res. 2010, 22, 611. [Google Scholar] [CrossRef]
- Buunk-Werkhoven, A.B.; Dijkstra, A. Promoting oral hygiene behavior in recruits in the Dutch army. Mil. Med. 2009, 174, 971–976. [Google Scholar]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Siqueira, M.B.; Firmino, R.T.; Clementino, M.A.; Martins, C.C.; Granville-Garcia, A.F.; Paiva, S.M. Impact of Traumatic Dental Injury on the Quality of Life of Brazilian Preschool Children. Int. J. Environ. Res. Public Health 2013, 10, 6422-6441. https://doi.org/10.3390/ijerph10126422
Siqueira MB, Firmino RT, Clementino MA, Martins CC, Granville-Garcia AF, Paiva SM. Impact of Traumatic Dental Injury on the Quality of Life of Brazilian Preschool Children. International Journal of Environmental Research and Public Health. 2013; 10(12):6422-6441. https://doi.org/10.3390/ijerph10126422
Chicago/Turabian StyleSiqueira, Maria B., Ramon T. Firmino, Marayza A. Clementino, Carolina C. Martins, Ana F. Granville-Garcia, and Saul M. Paiva. 2013. "Impact of Traumatic Dental Injury on the Quality of Life of Brazilian Preschool Children" International Journal of Environmental Research and Public Health 10, no. 12: 6422-6441. https://doi.org/10.3390/ijerph10126422