A Food Retail-Based Intervention on Food Security and Consumption


Abstract
:
1. Introduction
1.1. Health and the Built Environment
1.2. Food Environments and Diet/Diet-Related Disease
1.3. “Food Desert” Discourse
“…declining food access can be understood critically through an analysis of the time- and place-specific nature of capital, including its uneven penetration in local economies, the extent of its concentration and consolidation, and its impact on the local built environment”.(p. 2) [20]
1.4. Innovative Study Designs in Food Environments Research
2. Experimental Section
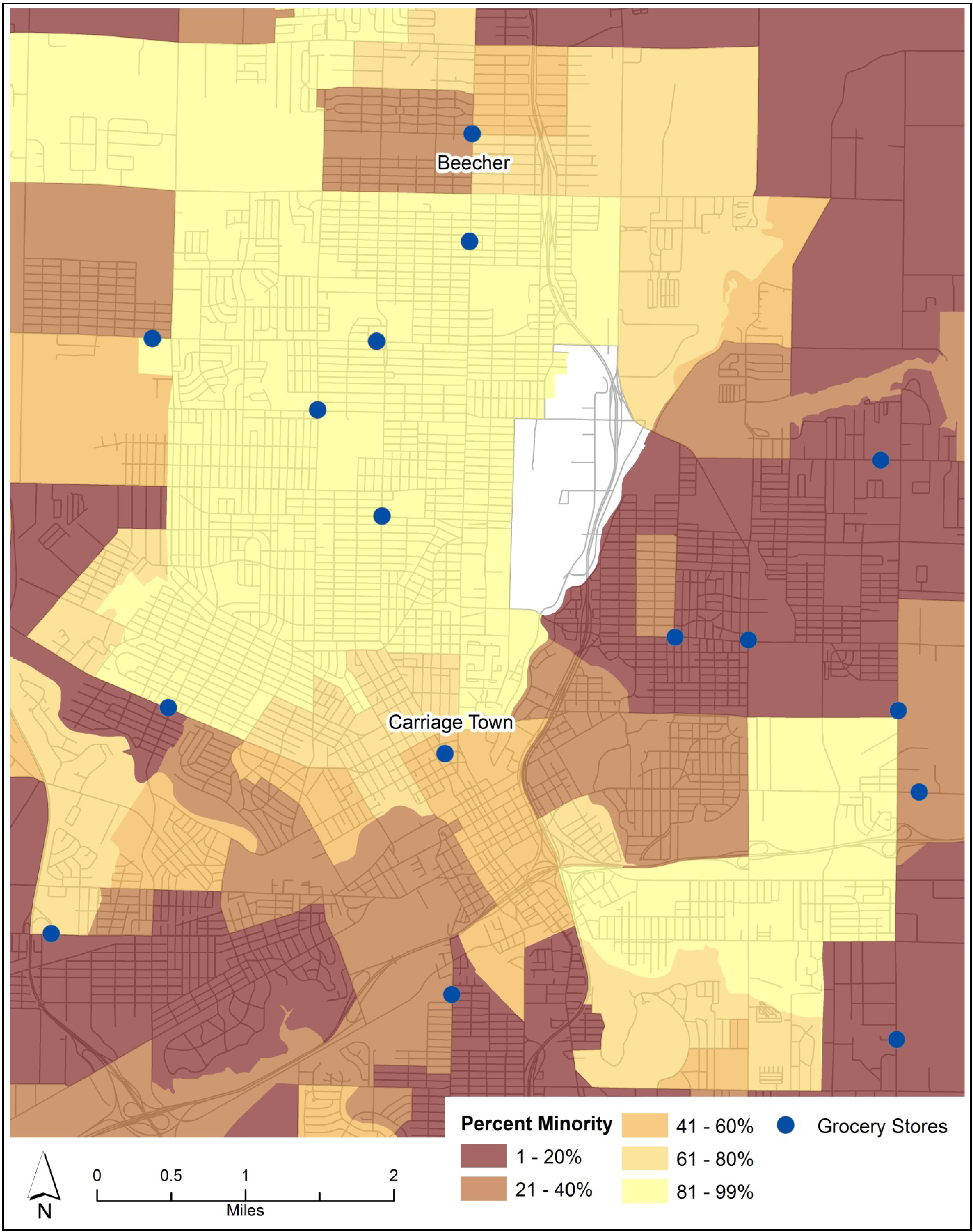
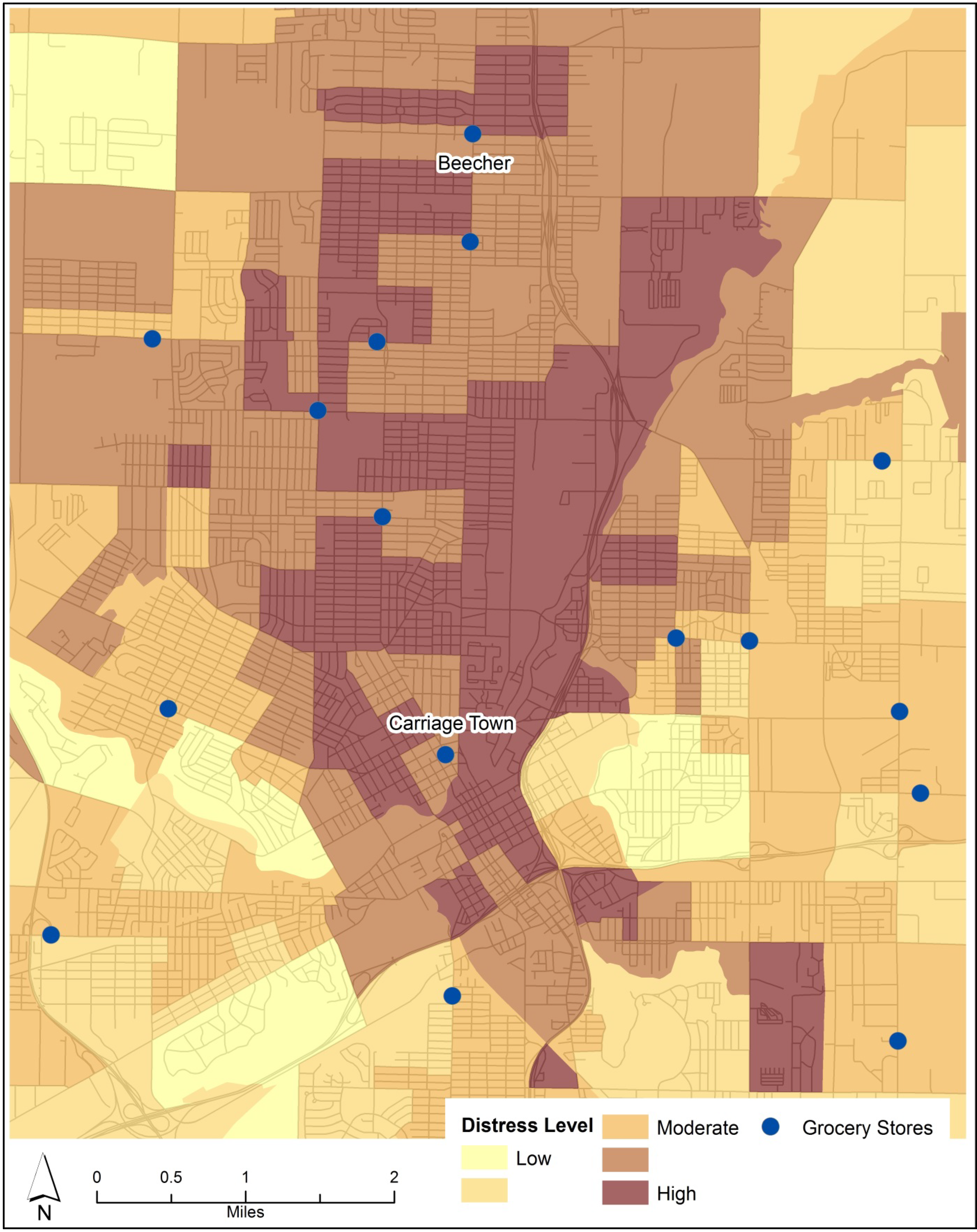
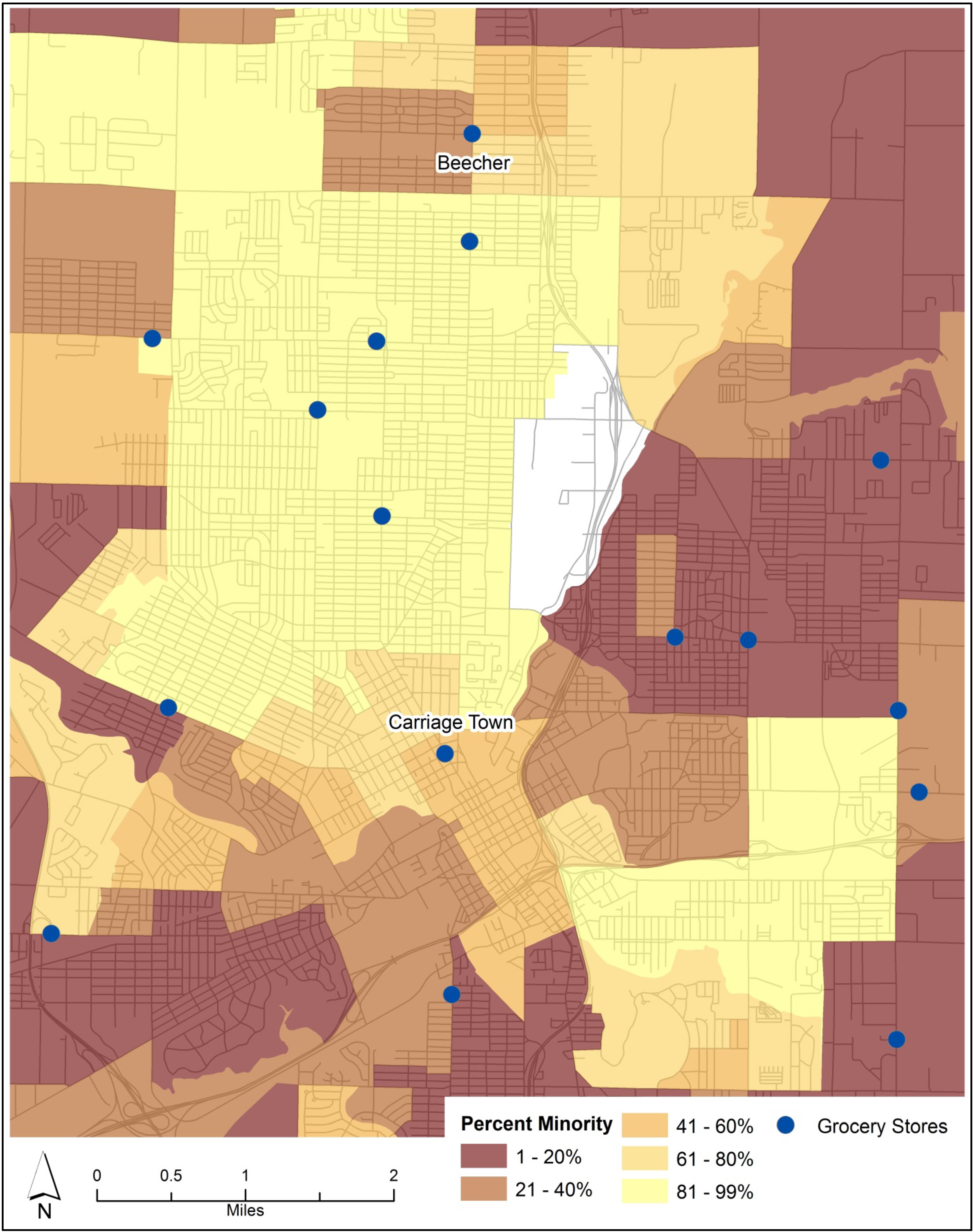
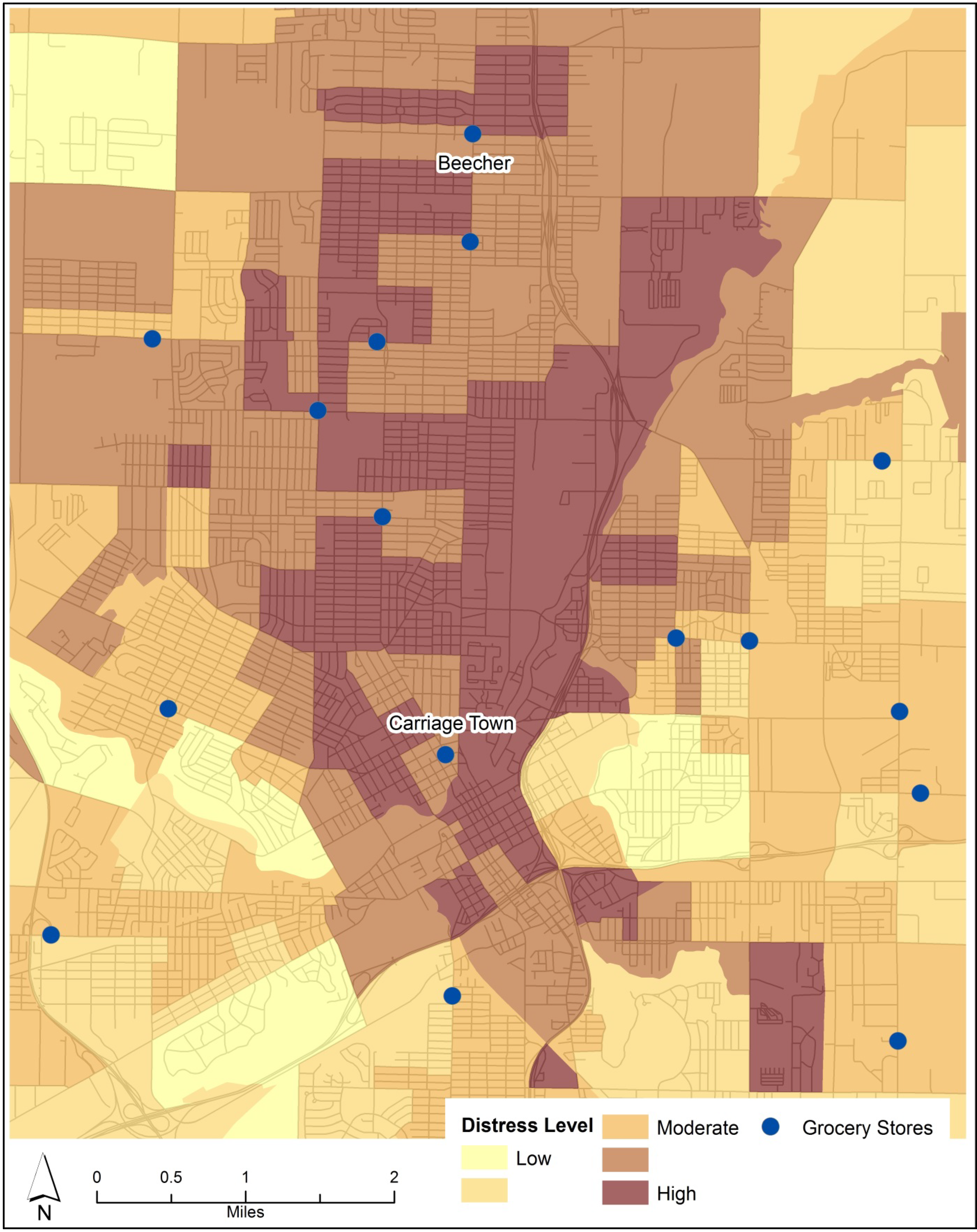
2.1. Study Area
2.2. Methods
3. Results and Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Average Age | % Female Respondents | % Black Respondents | % No High School Diploma | % Income < $20,000 | % Food Insecure | Servings of Fruits & Veg / Day | % Adequate F&V Consumption | % Overweight or Obese | Average BMI | % Excellent or Very Good Health | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alaimo (2008) (n = 766) | 44 | 52 | 49 | 13 | n/a | n/a | 4.0 | 20 | 68 | n/a | 38 |
| STYH CS (2009) (n = 736) | 47 | 73 | 53 | n/a | 67 | n/a | 4.0 | 18 | 71 | 29.3 | 37 |
| Phase 1 - 2009 (n = 186) | 56 | 73 | 60 | 23 | 75 | 32 | 2.5 | 7 | 72 | 29.5 | 32 |
| Phase 2 - 2011 (n = 166) | 53 | 62 | 61 | 17 | 60 | 37 | 2.8 | 9 | 72 | 29.5 | 40 |
| Carriage Town 2009 (n = 100) | 56 | 65 | 65 | 18 | 65 | 27 | 2.6 | 10 | 69 | 29.5 | 34 |
| Carriage Town 2011 (n = 96) | 52 | 49 | 61 | 13 | 54 | 39 | 2.6 | 5 | 65 | 28.5 | 46 |
| Beecher 2009 (n = 86) | 57 | 82 | 56 | 28 | 85 | 36 | 2.5 | 3 | 74 | 29.5 | 30 |
| Beecher 2011 (n = 70) | 57 | 77 | 61 | 24 | 70 | 34 | 2.9 | 14 | 82 | 31.1 | 31 |
| Food Secure (n = 226) | 57 | 67 | 51 | 19 | 65 | n/a | 2.6 | 9 | 70 | 29.5 | 43 |
| Food Insecure (n = 118) | 50 | 69 | 63 | 22 | 82 | n/a | 2.6 | 7 | 75 | 29.5 | 25 |
| Total | 55 | 67 | 61 | 20 | 67 | 34 | 2.8 | 8 | 72 | 29.5 | 37 |
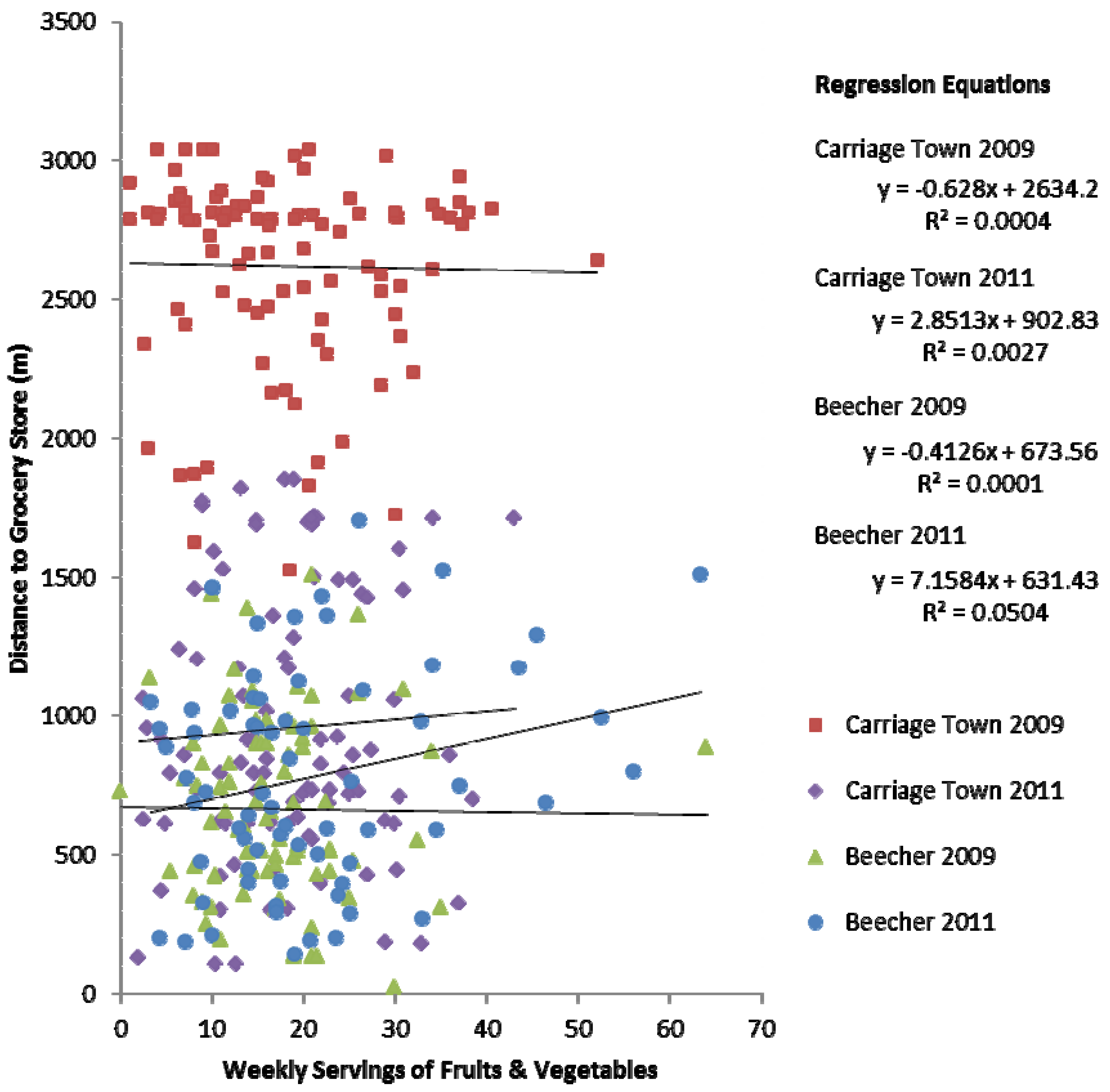
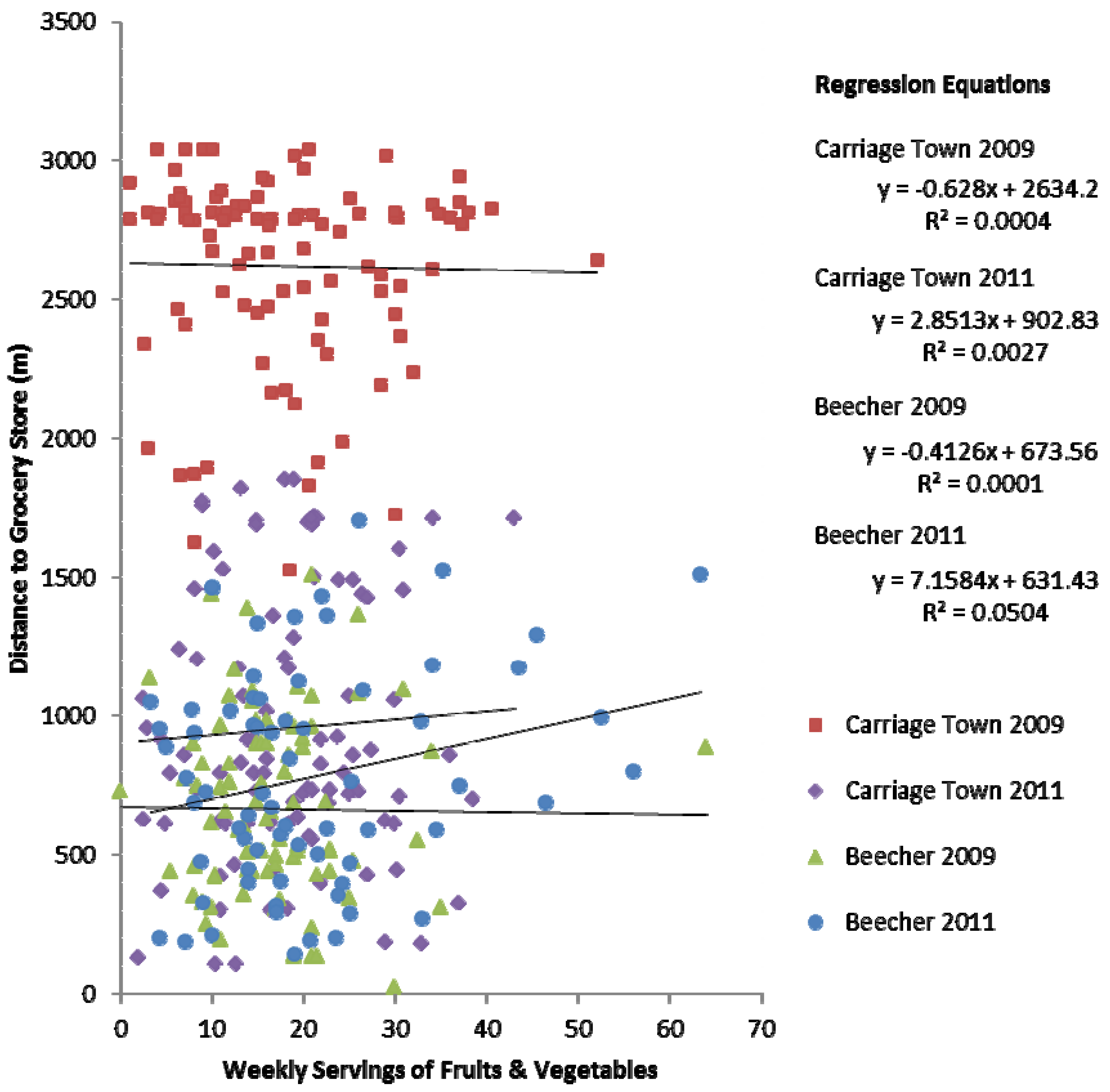
3.1. Regression Analysis
| Fruit & Vegetable Consumption | Food Security | Car Ownership | Self-Reported Health | Gender | Educational Attainment | Household Income | |
|---|---|---|---|---|---|---|---|
| * Correlation is significant at the .05 level (2-tailed) | |||||||
| ** Correlation is significant at the .01 level (2-tailed) | |||||||
| TFV | FS | MV | HLTH | GEND | EDU | INC | |
| TFV | 1 | ||||||
| FS | −0.012 | 1 | |||||
| MV | −0.081 | −0.128 | 1 | ||||
| HLTH | −0.102 | 0.248** | −0.208** | 1 | |||
| GEND | 0.082 | 0.019 | −0.091 | 0.052 | 1 | ||
| EDU | 0.125* | −0.074 | 0.160* | −0.208** | 0.019 | 1 | |
| INC | 0.129* | −0.143* | 0.048 | −0.219** | −0.068 | 0.311** | 1 |
| BMI | −0.095 | 0.000 | −0.201* | 0.270** | 0.041 | −0.034 | −0.043 |
| SM | 0.008 | −0.131* | 0.235** | 0.042 | −0.074 | 0.097 | 0.045 |
| NF | 0.052 | −0.120* | 0.173* | 0.004 | −0.078 | 0.126* | 0.162** |
| CON1 | −0.025 | 0.018 | 0.014 | −0.076 | −0.064 | 0.170** | 0.174** |
| CON2 | −0.086 | 0.034 | 0.023 | −0.019 | −0.071 | 0.043 | 0.003 |
| CON3 | −0.072 | 0.040 | −0.005 | −0.158** | −0.181** | 0.021 | 0.185** |
| IMP | −0.247** | 0.047 | 0.022 | 0.318** | −0.122* | −.184** | −0.168** |
| Age | −0.054 | 0.174** | 0.157* | −0.057 | −0.109* | 0.260** | 0.097 |
| BMI | SM | NF | CON1 | CON2 | CON3 | IMP | |
| BMI | 1 | ||||||
| SM | −0.009 | 1 | |||||
| NF | 0.003 | 0.624** | 1 | ||||
| CON1 | −0.086 | −0.060 | -0.036 | 1 | |||
| CON2 | −0.02 | −0.168** | -0.129* | 0.319** | 1 | ||
| CON3 | −0.084 | −0.113* | -0.124* | 0.233** | 0.200** | 1 | |
| IMP | 0.137* | 0.013 | -0.018 | −0.213** | -0.108* | -0.144** | 1 |
| Age | −0.015 | 0.006 | -0.011 | 0.077 | 0.203** | 0.098 | −0.059 |
3.2. Food Security
3.3. Food Consumption
3.4. Store Switching and Mobility
3.5. Discussion
3.6. Research Limitations
4. Conclusions
Acknowledgments
Conflict of Interest
References
- Mokdad, A.H.; Ford, E.S.; Bowman, B.A.; Dietz, W.H.; Vinicor, F.; Bales, V.S.; Marks, J.S. Prevalance of Obesity, Diabetes, and Obesity-Related Health Risk Factors, 2001. J. Am. Med. Assoc. 2003, 289, 76–79. [Google Scholar] [CrossRef]
- Roberts, P. The End of Food; Houghton Mifflin: New York, NY, USA, 2008. [Google Scholar]
- Kortt, M.A.; Langley, P.C.; Cox, E.R. A Review of Cost-of-Illness Studies on Obesity. Clin. Ther. 1998, 20, 772–779. [Google Scholar] [CrossRef]
- Hammond, R.A.; Levine, R. The economic impact of obesity in the United States. Diabetes Metab. Syndr. Obes. Target Ther. 2010, 3, 285–295. [Google Scholar] [CrossRef]
- Lytle, L.A. Measuring the Food Environment: State of the Science. Am. J. Prev. Med. 2009, 36, 134–144. [Google Scholar] [CrossRef]
- Reidpath, D.D.; Burns, C.; Garrard, J.; Mahoney, M.; Townsend, M. An ecological study of the relationship between social and environmental determinants of obesity. Health Place 2002, 8, 141–145. [Google Scholar]
- Robert, S.A.; Reither, E.N. A multilevel analysis of race, community disadvantage, and body mass index among adults in the US. Soc. Sci. Med. 2004, 59, 2421–2434. [Google Scholar] [CrossRef]
- Latham, J.; Moffat, T. Determinants of variation in food cost and availability in two socioeconomically contrasting neighbourhoods of Hamilton, Ontario, Canada. Health Place 2007, 13, 273–287. [Google Scholar] [CrossRef]
- Burns, C.M.; Inglis, A.D. Measuring food access in Melbourne: Access to healthy and fast foods by car, bus and foot in an urban municipality in Melbourne. Health Place 2007, 13, 877–885. [Google Scholar] [CrossRef]
- Ball, K.; Timperio, A.; Crawford, D. Neighbourhood socioeconomic inequalities in food access and affordability. Health Place 2009, 15, 578–585. [Google Scholar] [CrossRef]
- Smoyer-Tomic, K.E.; Spence, J.C.; Amrhein, C. Food Deserts in the Prairies? Supermarket Accessibility and Neighborhood Need in Edmonton, Canada. Prof. Geogr. 2006, 58, 307–326. [Google Scholar] [CrossRef]
- Chung, C.; Myers, S. Do the Poor Pay More for Food? An Analysis of Grocery Store Availability and Food Price Disparities. J. Consum. Aff. 1999, 33, 276–296. [Google Scholar] [CrossRef]
- Drewnowski, A.; Darmon, N. Food Choices and Diet Costs: An Economic Analysis. J. Nutr. 2005, 135, 900–904. [Google Scholar]
- Fraser, L.K.; Edwards, K.L. The association between the geography of fast food outlets and childhood obesity rates in Leeds, UK. Health Place 2010, 16, 1124–1128. [Google Scholar] [CrossRef]
- Morland, K.B.; Evenson, K.R. Obesity prevalence and the local food environment. Health Place 2009, 15, 491–495. [Google Scholar] [CrossRef]
- Pearce, J.; Hiscock, R.; Blakely, T.; Witten, K. A national study of the association between neighbourhood access to fast-food outlets and the diet and weight of local residents. Health Place 2009, 15, 193–197. [Google Scholar] [CrossRef]
- Kirkpatrick, S.I.; Tarasuk, V. Assessing the relevance of neighbourhood characteristics to the household food security of low-income Toronto families. Public Health Nutr. 2010, 13, 1139–1148. [Google Scholar] [CrossRef]
- United States Department of Health and Human Services: Healthy Food Financing Initiative. Available online: http://www.acf.hhs.gov/programs/ocs/resource/healthy-food-financing-initiative-0 (accessed on 5 January 2013).
- United States Department of Agriculture Economic Research Service: Food Access Research Atlas. Available online: http://www.ers.usda.gov/data-products/food-desert-locator.aspx (accessed on 5 January 2013).
- Bedore, M. Geographies of capital formation and rescaling: A historical-geographical approach to the food desert problem. Can. Geogr. 2013. [Google Scholar] [CrossRef]
- Donald, B. Food retail and access after the crash: Rethinking the food desert problem. J. Econ. Geogr. 2013. [Google Scholar] [CrossRef]
- Raja, S.; Ma, C.; Yadav, P. Beyond Food Deserts: Measuring and Mapping Racial Disparities in Neighborhood Food Environments. J. Plann. Educ. Res. 2008, 27, 469–482. [Google Scholar] [CrossRef]
- McEntee, J. Food Deserts: Contexts and Critiques of Contemporary Food Access Assessments; Centre for Business Relationships, Accountability, Sustainability and Society: Cardiff, Wales, UK, 2008. [Google Scholar]
- Coveney, J.; O’Dwyer, L.A. Effects of mobility and location on food access. Health Place 2009, 15, 45–55. [Google Scholar] [CrossRef]
- Petticrew, M.; Cummins, S.; Ferrell, C.; Findlay, A.; Higgins, C.; Hoy, C.; Kearns, A.; Sparks, L. Natural Experiments: an underused tool for public health? Public Health 2005, 119, 751–757. [Google Scholar] [CrossRef]
- Story, M.; Giles-Corti, B.; Yaroch, A.L.; Cummins, S.; Frank, L.D.; Huang, T.T-K.; Lewis, L.B. Work Group IV: Future Directions for Measures of the Food and Physical Activity Environments. Am. J. Prev. Med. 2009, 36, 182–188. [Google Scholar] [CrossRef]
- Fitzhugh, E.C.; Bassett, D.R., Jr.; Evans, M.F. Urban Trails and Physical Activity: A Natural Experiment. Am. J. Prev. Med. 2010, 39, 259–262. [Google Scholar] [CrossRef]
- MacDonald, J.M.; Stokes, R.J.; Cohen, D.A; Kofner, A.; Ridgeway, G.K. The Effect of Light Rail Transit on Body Mass Index and Physical Activity. Am. J. Prev. Med. 2010, 39, 105–112. [Google Scholar] [CrossRef]
- Kapinos, K.A.; Yakusheva, O. Environmental Influences on Young Adult Weight Gain: Evidence from a Natural Experiment. J. Adolescent Health 2011, 48, 52–58. [Google Scholar] [CrossRef]
- Wrigley, N.; Warm, D.; Margetts, B.; Whelan, A. Assessing the Impact of Improved Retail Access on Diet in a ‘Food Desert”: A Preliminary Report. Urban Studies 2002, 39, 2061–2082. [Google Scholar] [CrossRef]
- Cummins, S.; Petticrew, M.; Higgins, C.; Findlay, A.; Sparks, L. Large scale food retailing as an intervention for diet and health: quasi-experimental evaluation of a natural experiment. J. Epidemiol. Commun. H. 2005, 59, 1035–1040. [Google Scholar] [CrossRef]
- Cheadle, A.; Samuels, S.E.; Rauzon, S.; Yoshida, S.C.; Schwartz, P.M.; Boyle, M.; Beery, W.L.; Craypo, L.; Solomon, L. Approaches to Measuring the Extent and Impact of Environmental Change in Three California Community-Level Obesity Prevention Initiatives. Am. J. Public Health 2010, 100, 2129–2136. [Google Scholar] [CrossRef]
- Bickel, G.; Nord, M.; Price, C.; Hamilton, W.; Cook, J. Guide to Measuring Household Food Security; United States Department of Agriculture: Washington, DC, USA, 2000.
- Dixon, J.; Omwega, A.M.; Friel, S.; Burns, C.; Donati, K.; Carlisle, R. The Health Equity Dimensions of Urban Food Systems. J. Urban Health 2007, 84, 118–129. [Google Scholar] [CrossRef]
- Kendall, A.; Olson, C.M.; Frongillo, E.A. Relationship of hunger and food insecurity to food availability and consumption. J. Am. Diet. Assoc. 1996, 96, 1019–1024. [Google Scholar] [CrossRef]
- Chang-Hee, C.B.; Richardson, H.W. Urban Sprawl in Western Europe and the United States; Ashgate: Burlington, VT, USA, 2004. [Google Scholar]
- Bassett, D.R., Jr.; Pucher, J.; Buehler, R.; Thompson, D.L.; Crouter, S.E. Walking, Cycling, and Obesity Rates in Europe, North America, and Australia. J. Phys. Activ. Health 2008, 5, 795–814. [Google Scholar]
- Jacobs, A.J. The impacts of variations in development context on employment growth: A comparison of central cities in Michigan and Ontario, 1980–2006. Econ. Dev. Q. 2009, 23, 351–371. [Google Scholar] [CrossRef]
- Ladislas Segoe and Associates, and Associates. In Comprehensive Master Plan of Flint, Michigan, and Environs; Ladislas Segoe and Associates: Cincinnati, OH, USA, 1960.
- US Census Bureau: Census 2010. Available online: http://2010.census.gov/2010census/ (accessed on 11 November 2012).
- Sadler, R.C.; Gilliland, J.A.; Arku, G. Community Development and the Influence of New Food Retail Sources on the Price and Availability of Nutritious Food. J. Urban Aff. 2012. [Google Scholar] [CrossRef]
- Michigan Department of Community Health, Preliminary Health Indicators and Risk Estimates by Community Health Assessment Regions & Local Health Departments: Michigan Behavioral Risk Factor Survey 2008–2010 Combined. Lansing, MI, USA, 2011.
- Speak to Your Health Community Survey; Prevention Research Center of Michigan: Ann Arbor, MI, USA, 2009.
- Alaimo, K.; Packnett, E.; Miles, R.A.; Kruger, D.J. Fruit and Vegetable Intake among Urban Community Gardens. J. Nutr. Educ. Behav. 2008, 40, 94–101. [Google Scholar] [CrossRef]
- United States Department of Agriculture: Dietary Guidelines for Americans 2010. Available online: http://www.cnpp.usda.gov/dgas2010-policydocument.htm (accessed on 5 January 2013).
- Pampalon, R.; Hamel, D.; Gamache, P.; Raymond, G. A deprivation index for health planning in Canada. Chronic Dis. Can. 2010, 29, 178–191. [Google Scholar]
- US Census Bureau. Census 2010 Census Block Group Data. Available online: http://www.census.gov/geo/www/cob/bg2010.html (accessed on 11 November 2012).
- Franco, M.; Diez-Roux, A.V.; Nettleton, J.A.; Lazo, M.; Brancati, F.; Cabellero, B.; Glass, T.; Moore, L.V. Availability of healthy foods and dietary patterns: The multi-ethnic study of atherosclerosis. Am. J. Clin. Nutrit. 2009, 89, 897–904. [Google Scholar] [CrossRef]
- Hider, P. Environmental interventions to reduce energy intake or density: A critical appraisal of the literature. In New Zealand Health Technology Assessment Report; Department of Public Health and General Practice, Christchurch School of Medicine: Christchurch, New Zealand, 2001; Volume 4, Issue 2. [Google Scholar]
- Centers for Disease Control and Prevention (CDC), Behavioral Risk Factor Surveillance System Survey Questionnaire; US Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2009.
- Thompson, F.E.; Subar, A.F.; Smith, A.F.; Midthune, D.; Radimer, K.L.; Kahle, L.L.; Kipnis, V. Fruit and vegetable assessment: Performance of 2 new short instruments and a food frequency questionnaire. J. Am. Diet. Assoc. 2002, 102, 1764–1772. [Google Scholar] [CrossRef]
- Longley, K. Housing website says Flint had highest home turnover rate in January. Flint Journal. 22 February 2011. Available online: http://www.mlive.com/news/flint/index.ssf/2011/02/housing_website_report_says_fl.html (accessed on 11 November 2012).
- Sadler, R.C.; Gilliland, J.A.; Arku, G. An application of the edge effect in measuring accessibility to multiple food retailer types in rural Southwestern Ontario, Canada. Int. J. Health Geogr. 2011, 10. [Google Scholar] [CrossRef]
- NYCEDC. Food Retail Expansion to Support Health (FRESH). Available online: http://www.nycedc.com/financingincentives/taxexemptions/fresh/Pages/fresh.aspx (accessed on 11 November 2012).
- French, S.; Harnack, L.; Jeffery, R. Fast food restaurant use among women in the Pound of Prevention study: dietary, behavioral and demographic correlates. Int. J. Obesity 2000, 24, 1353–1359. [Google Scholar] [CrossRef]
- LISC-Flint (Local Initiatives Support Corporation-Flint), Witherbee’s Project Information; Flint: MI, USA, 2007.
- Turner, K. Witherbee’s market struggled to keep up with bills, co-owner blames bad economy for woes. Flint Journal 2011. [Google Scholar]
- Nestle, M. Food Politics: How the Food Industry Influences Nutrition and Health; University of California Press: Los Angeles, CA, USA, 2003. [Google Scholar]
- Thaler, R.H.; Sunstein, C.R. Libertarian Paternalism. Am. Econ. Rev. 2003, 93, 175–179. [Google Scholar] [CrossRef]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating Healthy Food and Eating Environments: Policy and Environmental Approaches. Annu. Rev. Publ. Health 2008, 29, 253–272. [Google Scholar] [CrossRef]
- Schafer-Elinder, L.; Jannson, M. Obesogenic environments—Aspects on measurement and indicators. Public Health Nutr. 2008, 12, 307–315. [Google Scholar]
- Algazy, J.; Gipstein, S.; Riahi, F.; Tryon, K. Why governments must lead the fight against obesity. McKinsey Quarterly 2010, October, 1–19. [Google Scholar]
- Winne, M. Community Food Security: Promoting Food Security and Building Healthy Food Systems; Community Food Security Coalition: Venice, CA, USA, 2005. [Google Scholar]
- Edible Flint. Home Page. Available online: http://www.edibleflint.org/ (accessed on 22 August 2012).
- Sadler, R.C.; Clark, M.; Gilliland, J. An economic impact comparative analysis of farmers’ markets in Michigan and Ontario. J. Agric. Food Syst. Community Dev. 2013, 3, 61–81. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Sadler, R.C.; Gilliland, J.A.; Arku, G. A Food Retail-Based Intervention on Food Security and Consumption. Int. J. Environ. Res. Public Health 2013, 10, 3325-3346. https://doi.org/10.3390/ijerph10083325
Sadler RC, Gilliland JA, Arku G. A Food Retail-Based Intervention on Food Security and Consumption. International Journal of Environmental Research and Public Health. 2013; 10(8):3325-3346. https://doi.org/10.3390/ijerph10083325
Chicago/Turabian StyleSadler, Richard C., Jason A. Gilliland, and Godwin Arku. 2013. "A Food Retail-Based Intervention on Food Security and Consumption" International Journal of Environmental Research and Public Health 10, no. 8: 3325-3346. https://doi.org/10.3390/ijerph10083325