Lung Deposition Analyses of Inhaled Toxic Aerosols in Conventional and Less Harmful Cigarette Smoke: A Review


Abstract
:1. Introduction
2. Cigarette Toxicity and Vulnerable Population Groups
2.1. Toxicants and Carcinogens in Conventional Cigarette Smoke
2.2. Less Harmful Cigarette Products
2.2.1. Manufacture Approaches
2.2.2. Typical LHC Products
Non-Burning Cigarettes
Electrical Heated Cigarettes (EHCs)
E-Cigarettes
2.2.3. Potential Health Risks of LHC Products
- (a)
- (b)
- Unknown reactions between some components in newly designed filters (or other new additives) may lead to the production of carcinogens or other toxicants.

| Toxicants | Induced Cancer Type | Related Biomarkers |
|---|---|---|
| Acetaldehyde * | Lung, nasal | Leukocyte DNA adducts |
| Acrolein * | Lung | 3-HPMA in urine |
| Benzene * | Lung, leukemia | SPMA in urine |
| Benzo[a]pyrene * | Lung | 1-hydroxypyrene in urine |
| 1,3-Butadiene * | Lung, leukemia, liver | MHBMA in urine |
| Carbon monoxide * | N/A | Exhaled CO |
| NNK, NNN * | Lung, nasal, oral cavity, liver, oesophageal, pancreatic, cervical | NNAL and NNN in urine |
| PAH * | Lung, laryngeal, oral cavity, cervical | 1-HOP |
| Formaldehyde | Lung, nasal | Leukocyte DNA adducts |
| Nicotine * | N/A | Nicotine, cotinine, 3′-hydroxicotinine and other their glucuronides in urine |
| Nickel * | Lung, nasal | N/A |
2.3. Children as the Vulnerable Population Group
3. Studies of Toxic Aerosols from Inhaled Cigarette Smoke
3.1. Experimental and Clinical Investigations
3.1.1. Experimental Studies
- (1)
- Cigarette Smoke Extract Exposure (CSEE) systems, which collect the CSPs using filters, traps, etc. [77].
- (2)
- A smoking machine to generate and dilute mainstream smoke samples to the experimental chamber, e.g., Walton Smoking Machine (WSM), Borgwaldt RM20S® smoking machine, TE-10z smoking machine, etc. [40,78,80,81,82]. The simulated puffing conditions were based on the International Organization for Standardization (ISO).
- An exposure chamber where the smoke and cell cultures (i.e., tissues or physiological fluids samples) interacts with each other [27,78]. Additionally, for clinical study, a human exposure chamber may be applied [40]. It is necessary to carefully regulate the conditions in the chamber, in order to mimic the environment in vivo.
3.1.2. Clinical Investigations
3.2. Computational Fluid-Particle Dynamics (CF-PD) Simulation Models
- (1)
- Multiphase flow models with relevant physical and bio-chemical processes. Considering the computational costs and accuracies, the multiphase flow models widely used for simulating tobacco smoke aerosol transport and deposition in human respiratory systems are mostly within the Euler-Lagrange and Euler-Euler frameworks [12,13,97,101]. Specifically, different approaches employed for particulate phases or vapors are as follows:
- (a)
- Lagrangian approaches employing the point force-and-moment method for transport and deposition simulations of tobacco smoke particulate phases, i.e., particles and droplets [12]. These approaches provide direct descriptions of the particulate flow by tracking the motion of individual particulate entities. The transient airflow field can be solved independently in the Eulerian frame in case of dilute aerosol suspensions.
- (b)
- Eulerian approaches with enhanced mass transfer for vapors and nanoparticles (less than 50 nm in diameter) in tobacco smoke [13]. Solution of the enhanced mass transfer equation, i.e., Euler-Euler approach, considering inhaled material convection, diffusion, coagulation/aggregation, wall-flux deposition, etc.
- (2)
- Initial and boundary conditions. Initial and boundary conditions include realistic airflow waveforms as part of smoking behavior, initial particle distribution at the mouth inlet, physical/chemical characteristics of inhaled particles, droplets and vapors, rigid or moving lung airway-wall boundary conditions, lung airway-outlet boundary conditions, etc.
- (3)
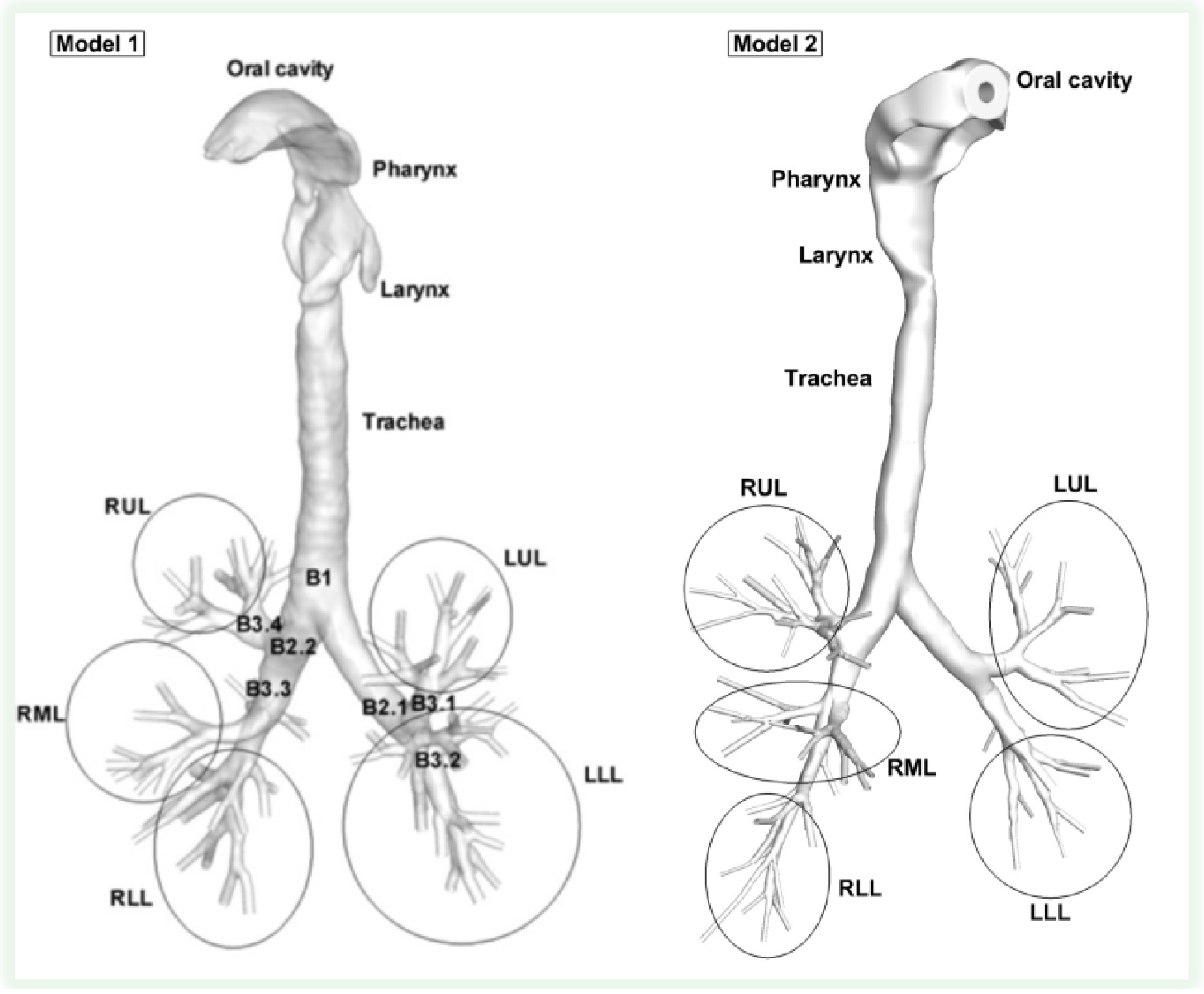
- Realistic human respiratory system geometries. Accurate and realistic human respiratory system models (see examples in Figure 1) compose the necessary precursor for experimental or computational airflow and particle transport/deposition analyses [100]. The human respiratory system ventilation path contains mouth, nose, pharynx, glottis, larynx, trachea, bronchi, bronchioles (including terminal bronchioles (Generation 16) and respiratory bronchioles (Generation 17–19)), and alveoli. Development of a subject-specific model for ventilation of a breathing lung can only be accomplished through multidisciplinary efforts that require expertise in medical imaging, airway geometric reconstruction, computational techniques, pulmonary physiology and medicine, and fluid mechanics [102].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
3.3. Semi-Empirical Models
3.4. Parameters and Mechanisms Influencing the Deposition of Toxicants and Carcinogens
3.4.1. Variability in Smoking Behavior
- 31 to 86 mL in puff volume.
- 0.9 to 3.0 s in puff duration.
- 18 to 64 s for inter-puff interval.
- 2,100 to 3,800 mL/min in puff flow rate.
- 8 to 16 puffs per cigarette.
| Cigarette | Smoking Condition | Puff Volume (mL) | Puff Duration (s) | Puff Frequency (min−1) |
|---|---|---|---|---|
| EHCSS-K6 | LOW4 | 40 | 1.2 | 4.0 |
| EHCSS-K3 | LOW | 40 | 1.2 | 2.0 |
| M6UK | LOW | 26 | 0.8 | 1.9 |
| M6J | LOW | 15 | 0.7 | 0.9 |
| PM1 | LOW | 29 | 0.9 | 3.6 |
| Lark1 | LOW | 29 | 0.9 | 3.0 |


3.4.2. Mechanisms Influencing Time-Evolution of Aerosol Size
Evaporation or Hygroscopic Growth Effect
- Group 1: Assuming that the droplet surface temperature is uniform and does not change with time.
- Group 2: Assuming that no temperature gradient and species mass fraction gradient exist inside the droplets, i.e., infinite thermal conductivity and mass diffusivity in the liquid phase.
- Group 3: Taking into account the temperature gradient and mass fraction gradient inside droplets without considering the recirculation inside droplets (Hill’s vortex) which would enhance the effective thermal conductivity of the liquid.
- Group 4: Based on the Group 3 conditions, taking into account the recirculation effect by introducing a correction factor to the liquid thermal conductivity.
- Group 5: Describing the recirculation effect by simulation of the internal vortex dynamics.
- Group 6: Full solution of the multi-phase Navier-Stokes equations.









Particle-Particle Interactions


- (1)
- The initial acceleration phase: the cloud accelerate to its maximum velocity, during which the particles circulate in a toroidal vortex (Hill’s vortex) inside the cloud, in a manner similar to the heavy fluid inside a droplet descending in a lighter fluid. Chaotic fluctuations due to the particle-particle and particle-flow interactions will cause some particles to start cross the boundary of the closed surfaces (see Figure 6(a)).
- (2)
- The torus shape phase: The initial spherical shape cloud gradually evolves into a flattened oblate shape and eventually a torus due to the “leaking” of particles and the toroidal circulation motion (see Figure 6(b)).The torus expands until it reaches a critical aspect ratio.
- (3)
- The break-up phase: After the torus expands to the critical aspect ratio, it becomes instable and the cloud start to break into two and further four smaller particle clouds (see Figure 6(c) and (d)).


Charged-Particle Effect
4. Conclusions and Future Directions
4.1. Summary
- Inter-subject variability in respiratory tract geometry;
- Air-particle inlet conditions; and
- Type and properties of inhaled toxic aerosol.
4.2. Future Directions for Experimental Studies
- (1)
- High-resolution puff-by-puff measuring techniques for dense tobacco smoke. Present techniques and devices (e.g., Scanning Mobility Particle Sizer (SMPS), Optical Particle Counters (OPC), and Aerodynamic Particle Sizer (APS)) for measuring particle diameter time-evolution dynamics and deposition efficiency require diluted aerosol suspensions; thus, any influence of coagulation in the original dense suspensions is diminished [87]. Specifically, because most of the measurement techniques are low-time resolution, so that in order to capture aerosol particulate evolution, the high number concentration of the tobacco smoke need to be diluted [86]. Hence, high-time resolved, puff-by-puff measuring techniques have to be developed, and future work should focus on improving real-time quantitative measurements of key toxicants and nicotine inhaled and exhaled. This will allow improved estimates of regional depositions of toxic chemical species and particles to better improve dosimetry and quantitative risk assessment.
- (2)
- Pathological Biomarkers and Mechanisms. Although the causal relationship between smoking and several diseases has been well established, there is still little understanding of the underlying mechanisms. Furthermore, the health impact of the release of the volatile organic compounds from the “e-juice” and the release of e-cigarette particulate phase into the indoor environment are still mostly unknown [66]. Although many carcinogen biomarkers have been identified, difficulties exist in tracking them in the human lung airways and beyond. For example, amounts of strong carcinogens [31] are very limited per cigarette (i.e., 1–200 ng per cigarette). Therefore, available biomarkers need to be identified for further investigations.
4.3. Future Directions for CF-PD Simulations
- (1)
- Accurate Image Processing: Currently, 100% accurate realistic 3-D imaging and modeling of the entire human respiratory system is unrealistic for several reasons: (a) the resolution of CT/MRI is not sufficiently high to capture lung airway geometries on a small scale, i.e., airways exceeding generation 6 (G6); (b) the lung consists of 223 airways plus millions of alveoli; (c) in vivo measurements are difficult because the whole respiratory system geometry is time dependent according to the human respiratory movements [137]. Accurate and high-resolution image processing techniques of the future will be the cornerstone of CF-PD simulations of the transport and deposition of toxicants and carcinogens in the whole human respiratory system.
- (2)
- Realistic smoking inlet conditions. Most CF-PD simulations assumed that the aerosols are directly inhaled into the lung (e.g., without considering the closing of the soft palate during puffing). Thus, the following three steps of smoking, i.e., mouth hold, inhalation and exhalation must be accurately modeled due to their strong influences on aerosol size evolution [26,85]. Furthermore, the puffing strength is not constant during the consumption of one cigarette [11], i.e., it increases as the puff number increases.
- (3)
- Time-evolved aerosol size distribution release at the mouth inlet. Presently, assumed aerosol-size distributions at the mouth inlet, employed as boundary conditions for CF-PD simulations, are not time-developed. As it is evident from experiments, most smoke constituents feature a continuous increase from the first puff to the last puff. Also, for e-cigarettes (e.g., NJOY®), the aerosol concentration decreases rapidly as the puff number increases during smoking [11]. Furthermore, the transport of droplets probably suffers coalescence which would break the assumption of monodisperse particles. In this case the microscopic mechanism that lead to droplet coalescence need to be investigated and incorporated in the model, as well as the resulted polydisperse distribution. For accurate numerical prediction of the deposition patterns, time-evolved aerosol-size distributions of CSPs based on accurate experimental measurements are necessary.
- (4)
- Fluid-Structure Interaction. The assumption of rigid walls is a potentially misleading approximation considering that moving lung airway walls will influence the airflow characteristics and hence airflow-particle interaction in the near-wall region, thereby altering the deposition patterns of the particles. Thus, fluid-structure interaction (FSI) analysis should be introduced for the solution of airflow quantities (i.e., velocity, pressure and shear stress) impacted by continuously deforming geometries (i.e., near-mesh displacement and velocity), as well as the influence on the local DE of CSPs.
- (5)
- Coupled Droplet-Vapor Interaction. Currently, the vaporization of droplets with toxicants and vapor transport are uncoupled [62,63]. That is, except for water, the realistic vapor concentrations are ignored for the vaporization of officially identified toxicants in CSPs, while the vaporization mass is not considered in the mass transfer equation either. However, for more accurate modeling, the effect of coupled vaporization and vapor transfer should be investigated. Thus, the local vaporized mass of the objective toxicant has to be added to its vapor transport equation as a source term, while realistic vapor concentrations have to be employed in simulating the vaporization of species. In addition, the local and segmental mass loss due to wall deposition should be considered.
- (6)
- Nanoparticles/vapors in Tobacco Smoke. During the smoking of tobacco, some constituents on the nano-scale penetrate the pulmonary alveoli and enter via lymph and/or blood circulation other organs [138]. Thus, a realistic and accurate multi-compartment model for deposited constituent mass transfer into systemic regions is a valuable and cost-effective tool for toxicologists and others to establish dose-response-effect relationships and generate new physical insight and reliable, quantitative data sets [14,15].
- (7)
- Particle Shape Effect. The filters of typical commercial cigarettes contain microscopic, needle-shaped shards of glass wool (like fiberglass insulation) which escape into the mouth and throat, and then lodge with tobacco tar in the lung tissue, surrounding the alveoli and lead to COPD, emphysema and eventually lung cancer. Numerous studies have demonstrated that the fiber aspect ratios as well as fiber durability are critical factors involved in pathogenicity [97]. Therefore, it is important to extend CF-PD modeling and accurately describe the orientation and transport of inhaled glass fibers.
Abbreviations
| 1-HOP | 1-Hydroxypyrene |
| 3-HPMA | 3-Hydroxypropylmercapturic Acid |
| APS | Aerodynamic Particle Sizer |
| CF-PD | Computational Fluid-Particle Dynamics |
| COPD | Chronic Obstructive Pulmonary Disease |
| CMD | Count Median Diameter |
| CORESTA | Cooperation Centre for Scientific Research Relative to Tobacco |
| CSEE | Cigarette Smoke Extract Exposure |
| CSP | Cigarette Smoke Particles |
| DE | Deposition Efficiency |
| DEM | Discrete Element Method |
| e-cigs | Electronic Cigarettes |
| EHC | Electronic Heating Cigarettes |
| ENDS | Electronic Nicotine Delivery Systems |
| ETS | Environmental Tobacco Smoke |
| FTC | Federal Trade Commission |
| FSI | Fluid-Structure Interaction |
| ISO | International Organization for Standardization |
| LDE | Local Deposition Efficiency |
| LHC | Less Harmful Cigarettes |
| LLL | Left Lower Lung |
| LUL | Left Upper Lung |
| LUDEP | Lung Dose Evaluation Program |
| MHBMA | Monohydroxy-3-Butenyl Mercapturic Acids |
| MPPD | Multiple Path Particle Dosimetry |
| MS | Mainstream Smoke |
| NNAL | 4-(Methylnitrosamino)-1-(3-Pyridyl)-1-Butanol |
| NNK | 4-(Methylnitrosamino)-1-(3-Pyridyl)-1-Butanone |
| NNN | N'-Nitrosonornicotine |
| OPC | Optical Particle Counters |
| PAH | Polycyclic Aromatic Hydrocarbons |
| PG | Propylene Glycol |
| PREP | Potential Reduced Exposure Product |
| PTR-MS | Proton-Transfer-Reaction Mass Spectrometry |
| RH | Relative Humidity |
| RLL | Right Lower Lung |
| RML | Right Middle Lung |
| RUL | Right Upper Lung |
| SC | Safer Cigarettes |
| SD | Standard Deviation |
| SHS | Second-hand Smoke |
| SMPS | Scanning Mobility Particle Sizer |
| SPMA | S-Phenylmercapturic Acid |
| TDE | Total Deposition Efficiency |
| THR | Tobacco Harm Reduction |
| TPM | Total Particulate Matter |
| TSNA | Tobacco Specific Nitrosamines |
| WSE | Whole Smoke Exposure |
| WSM | Walton Smoking Machine |
Acknowledgements
Conflicts of Interest
References
- Ingebrethsen, B.J. Evolution of the particle size distribution of mainstream cigarette smoke during a puff. Aerosol Sci. Technol. 1986, 5, 423–433. [Google Scholar] [CrossRef]
- Ingebrethsen, B.J.; Alderman, S.L.; Ademe, B. Coagulation of mainstream cigarette smoke in the mouth during puffing and inhalation. Aerosol Sci. Technol. 2011, 45, 1422–1428. [Google Scholar] [CrossRef]
- Patskan, G.; Reininghaus, W. Toxicological evaluation of an electrically heated cigarette. Part 1: Overview of technical concepts and summary of findings. J. Appl. Toxicol. 2003, 23, 323–328. [Google Scholar] [CrossRef]
- Rodgman, A.; Perfetti, T.A. The Chemical Components of Tobacco and Tobacco Smoke; CRC press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Fowles, J.; Dybing, E. Application of toxicological risk assessment principles to the chemical constituents of cigarette smoke. Tob. Control 2003, 12, 424–430. [Google Scholar] [CrossRef]
- FDA harmful and potentially harmful constituents in tobacco products and tobacco smoke. Establ. List Fed. Register 2012, 77, 20034–20037.
- Church, T.R.; Anderson, K.E.; Caporaso, N.E.; Geisser, M.S.; Le, C.T.; Zhang, Y.; Benoit, A.R.; Carmella, S.G.; Hecht, S.S. A prospectively measured serum biomarker for a tobacco-specific carcinogen and lung cancer in smokers. Cancer Epidemiol. Biomark. Prev. 2009, 18, 260–266. [Google Scholar] [CrossRef]
- Goniewicz, M.Ł.; Czogała, J.; Kośmider, L.; Koszowski, B.; Zielińska-Danch, W.; Sobczak, A. Exposure to carbon monoxide from second-hand tobacco smoke in Polish pubs. Cent. Eur. J. Public Health 2009, 17, 220–222. [Google Scholar]
- Al-Sayed, E.M.; Abrahim, K.S. Second-hand tobacco smoke and children. Toxicol. Ind. Health 2012, 5. [Google Scholar] [CrossRef]
- Yang, G. Marketing ‘less harmful, low-tar’ cigarettes is a key strategy of the industry to counter tobacco control in China. Tob. Control 2013. [Google Scholar] [CrossRef]
- Trtchounian, A.; Williams, M.; Talbot, P. Conventional and electronic cigarettes (e-cigarettes) have different smoking characteristics. Nicotine Tob. Res. 2010, 12, 905–912. [Google Scholar] [CrossRef]
- Zhang, Z.; Kleinstreuer, C.; Hyun, S. Size-change and deposition of conventional and composite cigarette smoke particles during inhalation in a subject-specific airway model. J. Aerosol Sci. 2012, 46, 34–52. [Google Scholar] [CrossRef]
- Zhang, Z.; Kleinstreuer, C.; Feng, Y. Vapor deposition during cigarette smoke inhalation in a subject-specific human airway model. J. Aerosol Sci. 2012, 50, 40–60. [Google Scholar]
- Kolanjiyil, A.V.; Kleinstreuer, C. Nanoparticle mass transfer from lung airways to systemic regions—Part I: Lung aerosol dynamics. J. Biomech. Eng. ASME 2013, in press. [Google Scholar]
- Kolanjiyil, A.V.; Kleinstreuer, C. Nanoparticle mass transfer from lung airways to systemic regions—Part II: Multi-compartmental modeling. J. Biomech. Eng. ASME 2013, in press. [Google Scholar]
- Polosa, R.; Thomson, N.C. Smoking and asthma: Dangerous liaisons. Eur. Respir. J. 2013, 41, 716–726. [Google Scholar] [CrossRef]
- Goldklang, M.P.; Marks, S.M.; D’Armiento, J.M. Second hand smoke and COPD: Lessons from animal studies. Front. Physiol. 2013, 4, 1–8. [Google Scholar]
- Vestbo, J.; Edwards, L.D.; Scanlon, P.D.; Yates, J.C.; Agusti, A.; Bakke, P.; Calverley, P.M.; Celli, B.; Coxson, H.O.; Crim, C. Changes in forced expiratory volume in 1 second over time in COPD. N. Engl. J. Med. 2011, 365, 1184–1192. [Google Scholar] [CrossRef]
- Chalouhi, N.; Ali, M.S.; Starke, R.M.; Jabbour, P.M.; Tjoumakaris, S.I.; Gonzalez, L.F.; Rosenwasser, R.H.; Koch, W.J.; Dumont, A.S. Cigarette smoke and inflammation: Role in cerebral aneurysm formation and rupture. Mediat. Inflamm. 2012, 2012, 271582:1–271582:12. [Google Scholar]
- Huxley, R.R.; Woodward, M. Cigarette smoking as a risk factor for coronary heart disease in women compared with men: A systematic review and meta-analysis of prospective cohort studies. Lancet 2011, 378, 1297–1305. [Google Scholar] [CrossRef]
- Barua, R.S.; Ambrose, J.A. Mechanisms of coronary thrombosis in cigarette smoke exposure. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1460–1467. [Google Scholar] [CrossRef]
- Csordas, A.; Bernhard, D. The biology behind the atherothrombotic effects of cigarette smoke. Nat. Rev. Cardiol. 2012, 10, 219–230. [Google Scholar] [CrossRef]
- Reynolds, P. Smoking and breast cancer. J. Mammary Gland Biol. Neoplasia 2013, 18, 15–23. [Google Scholar] [CrossRef]
- Xue, F.; Willett, W.C.; Rosner, B.A.; Hankinson, S.E.; Michels, K.B. Cigarette smoking and the incidence of breast cancer. Arch. Intern. Med. 2011, 171, 125–133. [Google Scholar] [CrossRef]
- Anderson, L.N.; Cotterchio, M.; Mirea, L.; Ozcelik, H.; Kreiger, N. Passive cigarette smoke exposure during various periods of life, genetic variants, and breast cancer risk among never smokers. Am. J. Epidemiol. 2012, 175, 289–301. [Google Scholar] [CrossRef]
- McAughey, J.; Adam, T.; McGrath, C.; Mocker, C.; Zimmermann, R. Simultaneous On-Line Size and Chemical Analysis of Gas Phase and Particulate Phase of Mainstream Tobacco Smoke. J. Phys. Conf. Ser. 2009, 151. [Google Scholar] [CrossRef]
- Narkowicz, S.; Polkowska, Ż.; Kiełbratowska, B.; Namieśnik, J. Environmental tobacco smoke: Exposure, health effects, and analysis. Crit. Rev. Environ. Sci. 2013, 43, 121–161. [Google Scholar] [CrossRef]
- Haustein, K.; Groneberg, D. Tobacco or Health? Springer: New York, NY, USA, 2010. [Google Scholar]
- Piadé, J.; Wajrock, S.; Jaccard, G.; Janeke, G. Formation of mainstream cigarette smoke constituents prioritized by the World Health Organization-yield patterns observed in market surveys, clustering and inverse correlations. Food Chem. Toxicol. 2013, 55, 329–347. [Google Scholar] [CrossRef]
- Burns, D.; Dybing, E.; Gray, N.; Hecht, S.; Anderson, C.; Sanner, T.; O’Connor, R.; Djordjevic, M.; Dresler, C.; Hainaut, P. Mandated lowering of toxicants in cigarette smoke: A description of the World Health Organization TobReg proposal. Tob. Control 2008, 17, 132–141. [Google Scholar] [CrossRef]
- Hecht, S.S.; Yuan, J.; Hatsukami, D. Applying tobacco carcinogen and toxicant biomarkers in product regulation and cancer prevention. Chem. Res. Toxicol. 2010, 23, 1001–1008. [Google Scholar] [CrossRef]
- Borgerding, M.; Klus, H. Analysis of complex mixtures—Cigarette smoke. Exp. Toxicol. Pathol. 2005, 57, 43–73. [Google Scholar] [CrossRef]
- Sureda, X.; Fernández, E.; López, M.J.; Nebot, M. Second-hand tobacco smoke exposure in open and semi-open settings: A systematic review. Environ. Health Perspect. 2013, 121, 766–773. [Google Scholar] [CrossRef] [Green Version]
- Jones, L.L.; Hassanien, A.; Cook, D.G.; Britton, J.; Leonardi-Bee, J. Parental smoking and the risk of middle ear disease in children: A systematic review and meta-analysis. Arch. Pediatr. Adolesc. Med. 2012, 166, 18–27. [Google Scholar] [CrossRef]
- Apostolou, A.; Garcia-Esquinas, E.; Fadrowski, J.J.; McLain, P.; Weaver, V.M.; Navas-Acien, A. Secondhand tobacco smoke: A source of lead exposure in US children and adolescents. J. Inf. 2012, 102, 714–722. [Google Scholar]
- Valenti, V.E.; Vanderlei, L.C.M.; Ferreira, C.; Fonseca, F.L.; Oliveira, F.R.; Sousa, F.H.; Rodrigues, L.M.; Monteiro, C.B.; Adami, F.; Wajnsztejn, R. Sidestream cigarette smoke and cardiac autonomic regulation. Int. Arch. Med. 2013, 6, 11. [Google Scholar] [CrossRef]
- Flouris, A.D.; Vardavas, C.I.; Metsios, G.S.; Tsatsakis, A.M.; Koutedakis, Y. Biological evidence for the acute health effects of secondhand smoke exposure. Am. J. Physiol. Lung Cell. Mol. Physiol. 2010, 298, L3–L12. [Google Scholar] [CrossRef]
- Jefferis, B.; Lawlor, D.; Ebrahim, S.; Wannamethee, S.; Feyerabend, C.; Doig, M.; McMeekin, L.; Cook, D.; Whincup, P. Cotinine-assessed second-hand smoke exposure and risk of cardiovascular disease in older adults. Heart 2010, 96, 854–859. [Google Scholar] [CrossRef]
- Schick, S.; Glantz, S. Philip Morris toxicological experiments with fresh sidestream smoke: More toxic than mainstream smoke. Tob. Control 2005, 14, 396–404. [Google Scholar] [CrossRef]
- Schick, S.F.; Farraro, K.F.; Fang, J.; Nasir, S.; Kim, J.; Lucas, D.; Wong, H.; Balmes, J.; Giles, D.K.; Jenkins, B. An apparatus for generating aged cigarette smoke for controlled human exposure studies. Aerosol Sci. Technol. 2012, 46, 1246–1255. [Google Scholar] [CrossRef]
- Schick, S.; Glantz, S.A. Sidestream cigarette smoke toxicity increases with aging and exposure duration. Tob. Control 2006, 15, 424–429. [Google Scholar] [CrossRef]
- Wayne, G.F. Potential reduced exposure products (PREPs) in industry trial testimony. Tob. Control 2006, 15, iv90–iv97. [Google Scholar] [CrossRef]
- Lippi, G.; Mattiuzzi, C.; Thun, M.; Carter, B.; Feskanich, D. Smoking-related mortality in the United States. N. Engl. J. Med. 2013, 368, 1752–1752. [Google Scholar] [CrossRef]
- Givel, M.S. In search of the less hazardous cigarette. Int. J. Health Serv. 2011, 41, 77–94. [Google Scholar] [CrossRef]
- Meckley, D.R.; Hayes, J.R.; van Kampen, K.; Ayres, P.H.; Mosberg, A.T.; Swauger, J.E. Comparative study of smoke condensates from 1R4F cigarettes that burn tobacco versus ECLIPSE cigarettes that primarily heat tobacco in the SENCAR mouse dermal tumor promotion assay. Food Chem. Toxicol. 2004, 42, 851–863. [Google Scholar] [CrossRef]
- Stabbert, R.; Voncken, P.; Rustemeier, K.; Haussmann, H.; Roemer, E.; Schaffernicht, H.; Patskan, G. Toxicological evaluation of an electrically heated cigarette. Part 2: Chemical composition of mainstream smoke. J. Appl. Toxicol. 2003, 23, 329–339. [Google Scholar] [CrossRef]
- Felter, J.L.; Lee, R.E.; Solanky, A.; Blake, C.; Davis, P.; Sharpe, D.E.; Watson, M.E.; Ripley, R.L.; Stevenson, B.W.; Crowe, W.J. Electrically Heated Cigarette Smoking System with Internal Manifolding for Puff Detection. European Patent No. EP 1558098, 2 January 2013. [Google Scholar]
- Adkison, S.E.; O’Connor, R.J.; Bansal-Travers, M.; Hyland, A.; Borland, R.; Yong, H.; Cummings, K.M.; McNeill, A.; Thrasher, J.F.; Hammond, D. Electronic nicotine delivery systems: International tobacco control four-country survey. Am. J. Prev. Med. 2013, 44, 207–215. [Google Scholar] [CrossRef]
- Electronic Nicotine Delivery Systems (ENDS)/E-Cigarettes Briefing; ASH Scotland: Scotland, UK, 2012; pp. 1–13.
- Laugesen, M. Safety Report on the Ruyan® E-Cigarette Cartridge and Inhaled Aerosol; Health New Zealand Ltd.: Christchurch, New Zealand, 2008; pp. 1–28. [Google Scholar]
- Zheng, J.; Zheng, Z. Preparation Method of E-Cigarette Liquid. European Patent No. EP 2543265, 9 January 2013. [Google Scholar]
- Williams, M.; Villarreal, A.; Bozhilov, K.; Lin, S.; Talbot, P. Metal and silicate particles including nanoparticles are present in electronic cigarette cartomizer fluid and aerosol. PloS One 2013, 8. [Google Scholar] [CrossRef]
- Series, R. Electronic cigarettes—An overview. Tob. Prev. Tob. Control 2013, 19, 1–39. [Google Scholar]
- Hatsukami, D.K.; Kotlyar, M.; Hertsgaard, L.A.; Zhang, Y.; Carmella, S.G.; Jensen, J.A.; Allen, S.S.; Shields, P.G.; Murphy, S.E.; Stepanov, I. Reduced nicotine content cigarettes: Effects on toxicant exposure, dependence and cessation. Addiction 2010, 105, 343–355. [Google Scholar] [CrossRef]
- Warner, K.E. Will the next generation of “safer” cigarettes be safer? J. Pediatr. Hematol.Oncol. 2005, 27, 543–550. [Google Scholar] [CrossRef]
- McNeill, A.; Munafò, M.R. Reducing harm from tobacco use. J. Psychopharmacol. 2013, 27, 13–18. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Henningfield, J.E. Reducing the nicotine content to make cigarettes less addictive. Tob. Control 2013, 22, i14–i17. [Google Scholar] [CrossRef]
- Brooks, D.R.; Austin, J.H.; Heelan, R.T.; Ginsberg, M.S.; Shin, V.; Olson, S.H.; Muscat, J.E.; Stellman, S.D. Influence of type of cigarette on peripheral versus central lung cancer. Cancer Epidemiol. Biomark. Prev. 2005, 14, 576–581. [Google Scholar] [CrossRef]
- Laugesen, M.; Fowles, J. Marlboro ultrasmooth: A potentially reduced exposure cigarette? Tob. Control 2006, 15, 430–435. [Google Scholar] [CrossRef]
- Chen, J.; Higby, R.; Tian, D.; Tan, D.; Johnson, M.D.; Xiao, Y.; Kellar, K.J.; Feng, S.; Shields, P.G. Toxicological analysis of low-nicotine and nicotine-free cigarettes. Toxicology 2008, 249, 194–203. [Google Scholar] [CrossRef]
- Lin, S.; Fonteno, S.; Weng, J.; Talbot, P. Comparison of the toxicity of smoke from conventional and harm reduction cigarettes using human embryonic stem cells. Toxicol. Sci. 2010, 118, 202–212. [Google Scholar] [CrossRef]
- Lin, S.; Tran, V.; Talbot, P. Comparison of toxicity of smoke from traditional and harm-reduction cigarettes using mouse embryonic stem cells as a novel model for preimplantation development. Hum. Reprod. 2009, 24, 386–397. [Google Scholar] [CrossRef]
- Gan, Q.; Yang, J.; Yang, G.; Goniewicz, M.; Benowitz, N.L.; Glantz, S.A. Chinese “herbal” cigarettes are as carcinogenic and addictive as regular cigarettes. Cancer Epidemiol. Biomark. Prev. 2009, 18, 3497–3501. [Google Scholar] [CrossRef]
- McCauley, L.; Markin, C.; Hosmer, D. An unexpected consequence of electronic cigarette useunforeseen risk of electronic cigarette use. CHEST J. 2012, 141, 1110–1113. [Google Scholar] [CrossRef]
- Chen, I. FDA summary of adverse events on electronic cigarettes. Nicotine Tob. Res. 2013, 15, 615–616. [Google Scholar] [CrossRef]
- Schripp, T.; Markewitz, D.; Uhde, E.; Salthammer, T. Does e-cigarette consumption cause passive vaping? Indoor Air 2013, 23, 25–31. [Google Scholar] [CrossRef]
- Hecht, S.S. Cigarette smoking and lung cancer: Chemical mechanisms and approaches to prevention. Lancet Oncol. 2002, 3, 461–469. [Google Scholar] [CrossRef]
- Hecht, S.S. Tobacco carcinogens, their biomarkers and tobacco-induced cancer. Nat. Rev. Cancer 2003, 3, 733–744. [Google Scholar] [CrossRef]
- Feng, Z.; Hu, W.; Hu, Y.; Tang, M. Acrolein is a major cigarette-related lung cancer agent: Preferential binding at p53 mutational hotspots and inhibition of DNA repair. Proc. Natl. Acad. Sci. USA 2006, 103, 15404–15409. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Kimmel, C.A.; Correa, A.; Eskenazi, B. Children’s health and the environment: Public health issues and challenges for risk assessment. Environ. Health Perspect. 2004, 112, 257–265. [Google Scholar]
- Landrigan, P.J.; Garg, A. Chronic effects of toxic environmental exposures on children’s health. Clin. Toxicol. 2002, 40, 449–456. [Google Scholar] [CrossRef]
- Knudsen, T.B.; Kleinstreuer, N.C. Disruption of embryonic vascular development in predictive toxicology. Birth Defects Res. Part C 2011, 93, 312–323. [Google Scholar] [CrossRef]
- Proietti, E.; Röösli, M.; Frey, U.; Latzin, P. Air pollution during pregnancy and neonatal outcome: A review. J. Aerosol Med. Pulm. Drug Deliv. 2012, 26, 9–23. [Google Scholar]
- Kit, B.K.; Simon, A.E.; Brody, D.J.; Akinbami, L.J. US prevalence and trends in tobacco smoke exposure among children and adolescents with asthma. Pediatrics 2013, 131, 407–414. [Google Scholar]
- Lardi, E.; Ott, C.; Schulzki, T.; Kuhn, M.; Bonetti, P.; Reinhart, W. Acute effects of short-term exposure to second-hand smoke on induced platelet aggregation. Clin. Hemorheol. Microcirc. 2010, 45, 359–364. [Google Scholar]
- Argacha, J.; Fontaine, D.; Adamopoulos, D.; Ajose, A.; van de Borne, P.; Fontaine, J.; Berkenboom, G. Acute effect of sidestream cigarette smoke extract on vascular endothelial function. J. Cardiovasc. Pharmacol. 2008, 52, 262–267. [Google Scholar] [CrossRef]
- Johnson, M.D.; Schilz, J.; Djordjevic, M.V.; Rice, J.R.; Shields, P.G. Evaluation of in vitro assays for assessing the toxicity of cigarette smoke and smokeless tobacco. Cancer Epidemiol. Biomark. Prev. 2009, 18, 3263–3304. [Google Scholar] [CrossRef]
- Adamson, J.; Hughes, S.; Azzopardi, D.; McAughey, J.; Gaça, M.D. Real-time assessment of cigarette smoke particle deposition in vitro. Chem. Cent. J. 2012, 6, 1–11. [Google Scholar] [CrossRef]
- Pezzulo, A.A.; Starner, T.D.; Scheetz, T.E.; Traver, G.L.; Tilley, A.E.; Harvey, B.; Crystal, R.G.; McCray, P.B.; Zabner, J. The air-liquid interface and use of primary cell cultures are important to recapitulate the transcriptional profile of in vivo airway epithelia. Am. J. Physiol. Lung Cell. Mol. Physiol. 2011, 300, L25–L31. [Google Scholar] [CrossRef]
- Kaur, N.; Lacasse, M.; Roy, J.; Cabral, J.; Adamson, J.; Errington, G.; Waldron, K.C.; Gaça, M.; Morin, A. Evaluation of precision and accuracy of the Borgwaldt RM20S® smoking machine designed for in vitro exposure. Inhal. Toxicol. 2010, 22, 1174–1183. [Google Scholar] [CrossRef]
- Gordon, S.; Brinkman, M.; Meng, R.; Anderson, G.; Chuang, J.; Kroeger, R.; Reyes, I.; Clark, P. Effect of cigarette menthol content on mainstream smoke emissions. Chem. Res. Toxicol. 2011, 24, 1744–1753. [Google Scholar] [CrossRef]
- Zhang, Y.; Sumner, W.; Chen, D. In vitro particle size distributions in electronic and conventional cigarette aerosols suggest comparable deposition patterns. Nicotine Tob. Res. 2013, 15, 501–508. [Google Scholar] [CrossRef]
- Morawska, L.; Hofmann, W.; Hitchins-Loveday, J.; Swanson, C.; Mengersen, K. Experimental study of the deposition of combustion aerosols in the human respiratory tract. J. Aerosol Sci. 2005, 36, 939–957. [Google Scholar] [CrossRef] [Green Version]
- Sahu, S.; Tiwari, M.; Bhangare, R.; Pandit, G. Particle size distribution of mainstream and exhaled cigarette smoke and predictive deposition in human respiratory tract. Aerosol Air Q. Res. 2013, 13, 324–332. [Google Scholar]
- McGrath, C.; Warren, N.; Biggs, P.; McAughey, J. Real-time measurement of inhaled and exhaled cigarette smoke: Implications for dose. J. Phys. Conf. Ser. 2009, 151. [Google Scholar] [CrossRef]
- Van Dijk, W.D.; Heijdra, Y.; Lenders, J.W.; Klerx, W.; Akkermans, R.; van der Pouw, A.; van Weel, C.; Scheepers, P.T.; Schermer, T.R. Cigarette smoke retention and bronchodilation in patients with COPD. A controlled randomized trial. Respir. Med. 2012, 107, 112–119. [Google Scholar]
- Yu, L.; Dzikovski, B.G.; Freed, J.H. A protocol for detecting and scavenging gas-phase free radicals in mainstream cigarette smoke. J. Vis. Exp. 2012, 59. [Google Scholar] [CrossRef]
- Roemer, E.; Schramke, H.; Weiler, H.; Buettner, A.; Kausche, S.; Weber, S.; Berges, A.; Stueber, M.; Muench, M.; Trelles-Sticken, E. Mainstream smoke chemistry and in vitro and in vivo toxicity of the reference cigarettes 3R4F and 2R4F. Beiträge zur Tabakforschung International 2012, 25, 316–335. [Google Scholar]
- Goniewicz, M.L.; Knysak, J.; Gawron, M.; Kosmider, L.; Sobczak, A.; Kurek, J.; Prokopowicz, A.; Jablonska-Czapla, M.; Rosik-Dulewska, C.; Havel, C. Levels of selected carcinogens and toxicants in vapour from electronic cigarettes. Tob. Control 2013, in press. [Google Scholar]
- Zenzen, V.; Diekmann, J.; Gerstenberg, B.; Weber, S.; Wittke, S.; Schorp, M.K. Reduced exposure evaluation of an Electrically Heated Cigarette Smoking System. Part 2: Smoke chemistry and in vitro toxicological evaluation using smoking regimens reflecting human puffing behavior. Regul. Toxicol. Pharmacol. 2012, 64, S11–S34. [Google Scholar] [CrossRef]
- Charles, F.; Krautter, G.R.; Mariner, D.C. Post-puff respiration measures on smokers of different tar yield cigarettes. Inhal. Toxicol. 2009, 21, 712–718. [Google Scholar] [CrossRef]
- Alfi, M.; Talbot, P. Health-related effects reported by electronic cigarette users in online forums. J. Med. Internet Res. 2013, 15. [Google Scholar] [CrossRef]
- Finlay, W.H.; Martin, A.R. Recent advances in predictive understanding of respiratory tract deposition. J. Aerosol Med. Pulm. Drug Deliv. 2008, 21, 189–206. [Google Scholar] [CrossRef]
- Schorp, M.K.; Tricker, A.R.; Dempsey, R. Reduced exposure evaluation of an Electrically Heated Cigarette Smoking System. Part 1: Non-clinical and clinical insights. Regul. Toxicol. Pharmacol. 2012, 64, S1–S10. [Google Scholar] [CrossRef]
- Dickens, C.; McGrath, C.; Warren, N.; Biggs, P.; McAughey, J. Puffing and inhalation behaviour in cigarette smoking: Implications for particle diameter and dose. J. Phys. Conf. Ser. 2009, 151. [Google Scholar] [CrossRef]
- Hofmann, W. Modelling inhaled particle deposition in the human lung—A review. J. Aerosol Sci. 2011, 42, 693–724. [Google Scholar] [CrossRef]
- Kleinstreuer, C.; Feng, Y. Computational analysis of non-spherical particle transport and deposition in shear flow with application to lung aerosol dynamics—A review. J. Biomech. Eng. 2013, 135. [Google Scholar] [CrossRef]
- Sosnowski, T.R. Importance of airway geometry and respiratory parameters variability for particle deposition in the human respiratory tract. J. Thorac. Dis. 2011, 3, 153–155. [Google Scholar]
- Rostami, A.A. Computational modeling of aerosol deposition in respiratory tract: A review. Inhal. Toxicol. 2009, 21, 262–290. [Google Scholar] [CrossRef]
- Kleinstreuer, C.; Zhang, Z. Airflow and particle transport in the human respiratory system. Annu. Rev. Fluid Mech. 2010, 42, 301–334. [Google Scholar] [CrossRef]
- Kleinstreuer, C. Two-Phase Flow: Theory and Applications; Taylor & Francis Group: New York, NY, USA, 2003. [Google Scholar]
- Tawhai, M.H.; Hunter, P.; Tschirren, J.; Reinhardt, J.; McLennan, G.; Hoffman, E.A. CT-based geometry analysis and finite element models of the human and ovine bronchial tree. J. Appl. Physiol. 2004, 97, 2310–2321. [Google Scholar] [CrossRef]
- Longest, P.W.; Tian, G.; Walenga, R.L.; Hindle, M. Comparing MDI and DPI aerosol deposition using in vitro experiments and a new stochastic individual path (SIP) model of the conducting airways. Pharm. Res. 2012, 29, 1670–1688. [Google Scholar] [CrossRef]
- Li, Z. Particle deposition in oral-tracheal airway models with very low inhalation profiles. J. Bionic Eng. 2012, 9, 252–261. [Google Scholar] [CrossRef]
- Longest, P.W.; Xi, J. Condensational growth may contribute to the enhanced deposition of cigarette smoke particles in the upper respiratory tract. Aerosol Sci. Technol. 2008, 42, 579–602. [Google Scholar] [CrossRef]
- Solomon, P.A.; Gehr, P.; Bennett, D.H.; Phalen, R.F.; Méndez, L.B.; Rothen-Rutishauser, B.; Clift, M.; Brandenberger, C.; Mühlfeld, C. Macroscopic to microscopic scales of particle dosimetry: From source to fate in the body. Air Q. Atmosphere Health 2012, 5, 169–187. [Google Scholar] [CrossRef]
- Jarvis, N.; Birchall, A.; James, A.; Bailey, M.; Dorrian, M. LUDEP 2.0: Personal computer program for calculating internal doses using the ICRP Publication 66 respiratory tract model; Technical Report NRPB-SR287; NRPB: Chilton, UK, 1996. [Google Scholar]
- Kane, D.B.; Asgharian, B.; Price, O.T.; Rostami, A.; Oldham, M.J. Effect of smoking parameters on the particle size distribution and predicted airway deposition of mainstream cigarette smoke. Inhal. Toxicol. 2010, 22, 199–209. [Google Scholar] [CrossRef]
- Anjilvel, S.; Asgharian, B. A multiple-path model of particle deposition in the rat lung. Toxicol. Sci. 1995, 28, 41–50. [Google Scholar] [CrossRef]
- Robinson, R.; Yu, C. Coagulation of cigarette smoke particles. J. Aerosol Sci. 1999, 30, 533–548. [Google Scholar] [CrossRef]
- Bernstein, D.M. A review of the influence of particle size, puff volume, and inhalation pattern on the deposition of cigarette smoke particles in the respiratory tract. Inhal. Toxicol. 2004, 16, 675–689. [Google Scholar] [CrossRef]
- Hicks, J.; Pritchard, J.; Black, A.; Megaw, W. Experimental evaluation of aerosol growth in the human respiratory tract. In Aerosols: Formation and Reactivity; Berlin Pergamon Press: Oxford, UK, 1986; pp. 244–247. [Google Scholar]
- Li, W.; Hopke, P. Initial size distributions and hygroscopicity of indoor combustion aerosol particles. Aerosol Sci. Technol. 1993, 19, 305–316. [Google Scholar] [CrossRef]
- Robinson, R.J.; Yu, C. Deposition of cigarette smoke particles in the human respiratory tract. Aerosol Sci. Technol. 2001, 34, 202–215. [Google Scholar] [CrossRef]
- Tang, X.; Zheng, Z.; Jung, H.S.; Asa-Awuku, A. The effects of mainstream and sidestream environmental tobacco smoke composition for enhanced condensational droplet growth by water vapor. Aerosol Sci. Technol. 2012, 46, 760–766. [Google Scholar] [CrossRef]
- Sazhin, S.; Kristyadi, T.; Abdelghaffar, W.; Heikal, M. Models for fuel droplet heating and evaporation: Comparative analysis. Fuel 2006, 85, 1613–1630. [Google Scholar] [CrossRef]
- Kim, J.W.; Xi, J.; Si, X.A. Dynamic growth and deposition of hygroscopic aerosols in the nasal airway of a 5-year-old child. Int. J. Numer. Methods Biomed. Eng. 2013, 29, 17–39. [Google Scholar] [CrossRef]
- Sazhin, S.; Xie, J.; Shishkova, I.; Elwardany, A.; Heikal, M. A kinetic model of droplet heating and evaporation: Effects of inelastic collisions and a non-unity evaporation coefficient. Int. J. Heat Mass Transfer 2013, 56, 525–537. [Google Scholar] [CrossRef] [Green Version]
- Vesala, T.; Kulmala, M.; Rudolf, R.; Vrtala, A.; Wagner, P.E. Models for condensational growth and evaporation of binary aerosol particles. J. Aerosol Sci. 1997, 28, 565–598. [Google Scholar] [CrossRef]
- Finlay, W. The Mechanics of Inhaled Pharmaceutical Aerosols: An Introduction; Academic Press: London, UK, 2001. [Google Scholar]
- Robinson, R.J. Carcinogen specific dosimetry model for passive smokers of various ages. Sci. Total Environ. 2005, 338, 201–212. [Google Scholar] [CrossRef]
- Park, J.; Metzger, B.; Guazzelli, É.; Butler, J.E. A cloud of rigid fibres sedimenting in a viscous fluid. J. Fluid Mech. 2010, 648, 351–362. [Google Scholar] [CrossRef]
- Sadlej, K.; Wajnryb, E.; Ekiel-Jeżewska, M.L. Hydrodynamic interactions suppress deformation of suspension drops in Poiseuille flow. J. Chem. Phys. 2010, 133. [Google Scholar] [CrossRef]
- Pignatel, F.; Nicolas, M.; Guazzelli, E. A falling cloud of particles at a small but finite Reynolds number. J. Fluid Mech. 2011, 671, 34–51. [Google Scholar] [CrossRef]
- Guazzelli, E. A Physical Introduction to Suspension Dynamics; Cambridge University Press: New York, NY, USA, 2011; Volume 45. [Google Scholar]
- Lai, A.C.; Zhao, B.; Law, A.W.; Adams, E.E. Two-phase modeling of sediment clouds. Environ. Fluid Mech. 2013. [Google Scholar] [CrossRef]
- Hinds, W. Aerosol Technology: Properties, Behavior, and Measurements of Aerosol Particles; Wiley-Interscience: New York, NY, USA, 1982. [Google Scholar]
- Hinds, W.C. Aerosol Technology: Properties, Behavior, and Measurement of Airborne Particles; Wiley-Interscience: New York, NY, USA, 2012. [Google Scholar]
- Broday, D.M.; Robinson, R. Application of cloud dynamics to dosimetry of cigarette smoke particles in the lungs. Aerosol. Sci. Technol. 2003, 37, 510–527. [Google Scholar] [CrossRef]
- Martonen, T.; Musante, C. Importance of cloud motion on cigarette smoke deposition in lung airways. Inhal. Toxicol. 2000, 12, 261–280. [Google Scholar] [CrossRef]
- Asgharian, B.; Price, O.T.; Dickens, C.; McAughey, J. Coagulation and Deposition of Cigarette Smoke Particles in the Human Lung. In Presented at American Association for Aerosol Research, Oregon Convention Center, Portland, OR, USA, 2010.
- Friedlander, S.K. Smoke, Dust, and Haze; Oxford University Press: New York, NY, USA, 2000; Volume 198. [Google Scholar]
- Rim, D.; Green, M.; Wallace, L.; Persily, A.; Choi, J. Evolution of ultrafine particle size distributions following indoor episodic releases: Relative importance of coagulation, deposition and ventilation. Aerosol Sci. Technol. 2012, 46, 494–503. [Google Scholar] [CrossRef]
- Keith, C. Particle size studies on tobacco smoke. Beitrage Zur Tabakforschung Int. 1982, 11, 123. [Google Scholar]
- Yu, M.; Koivisto, A.J.; Hämeri, K.; Seipenbusch, M. Size Dependence of the Ratio of Aerosol Coagulation to Deposition Rates for Indoor Aerosols. Aerosol Sci. Technol. 2012, 47, 427–434. [Google Scholar]
- Koolpiruck, D.; Prakoonwit, S.; Balachandran, W. Numerical modeling of inhaled charged aerosol deposition in human airways. Ind. Appl. IEEE Trans. 2004, 40, 1239–1248. [Google Scholar] [CrossRef]
- Wu, G.; Wang, Q.; Lian, J.; Shen, D. Reconstruction of 4D-CT from A Single Free-Breathing 3D-CT by Spatial-Temporal Image Registration; Information Processing in Medical Imaging; Springer: New York, NY, USA, 2011; pp. 686–698. [Google Scholar]
- Shang, S.; Ordway, D.; Henao-Tamayo, M.; Bai, X.; Oberley-Deegan, R.; Shanley, C.; Orme, I.M.; Case, S.; Minor, M.; Ackart, D. Cigarette smoke increases susceptibility to tuberculosis—Evidence from in vivo and in vitro models. J. Infect. Dis. 2011, 203, 1240–1248. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kleinstreuer, C.; Feng, Y. Lung Deposition Analyses of Inhaled Toxic Aerosols in Conventional and Less Harmful Cigarette Smoke: A Review. Int. J. Environ. Res. Public Health 2013, 10, 4454-4485. https://doi.org/10.3390/ijerph10094454
Kleinstreuer C, Feng Y. Lung Deposition Analyses of Inhaled Toxic Aerosols in Conventional and Less Harmful Cigarette Smoke: A Review. International Journal of Environmental Research and Public Health. 2013; 10(9):4454-4485. https://doi.org/10.3390/ijerph10094454
Chicago/Turabian StyleKleinstreuer, Clement, and Yu Feng. 2013. "Lung Deposition Analyses of Inhaled Toxic Aerosols in Conventional and Less Harmful Cigarette Smoke: A Review" International Journal of Environmental Research and Public Health 10, no. 9: 4454-4485. https://doi.org/10.3390/ijerph10094454